Impact of immunostaining of pulmonary and mediastinal cytology
|
|
|
- Roxanne Chapman
- 5 years ago
- Views:
Transcription
1 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014
2 Disclaimer Pfizer: Honorarium-Advisory Board and Education Events AstraZeneca: Honorarium-Advisory Board Roche: Honorarium Click View then Header and Footer to change this footer
3 OBJECTIVES To understand the limitations of cytomorphological features in achieving the specific diagnosis To know the role of ancillary studies in cytological diagnoses of lung and mediastinal neoplasms To understand the implications of delivering information of specific cellular differentiation in lung cancer oncology practice
 Squamous cell carcinoma (25%- 30%) Atypical carcinoid SCLC (5%-10%) Metastatic (Mostly), multiple 1 Pleural (3) Adenocarcinoma (rare)")
4 Lung Tumours Central (1) Squamous cell Carcinoma (70%- 75%) Small cell Carcinoma (90%-95%) Adenocarcinoma (5%-10%) Typical carcinoid Peripheral (2) Adenocarcinoma (80%) Squamous cell carcinoma (25%- 30%) Atypical carcinoid SCLC (5%-10%) Metastatic (Mostly), multiple 1 Pleural (3) Adenocarcinoma (rare) Mesothelioma 3 2
5 TRENDING CYTOLOGY Molecular era: Shift in oncology practice and expectations Diagnostic pathway: less invasive, cost effective, reliable, optimal Cytomorphological features: Reliability for specific cellular differentiation Ancillary studies: Knowledge and interpretation skills Cytology Radiology Correlation: Understanding and integration Ground glass, spiculated, circumscribed Solid, cavitary, consolidation Solitary, multiple, location Specific diagnoses: Translations and implications
6 CYTOLOGY: IMPLICATIONS Standard chemotherapy ADC more responsive to Gemcitabine + Docetaxel Non-ADC more responsive to Cisplatin + Docetaxel Targeted chemotherapies VEGF inhibitor (i.e Bevacizumab): Contraindicated in SQCC - EGFR mutation (i.e. Erlotinib, Gefitinib): Adenocarcinoma (race, age, gender, smoking status) - ALK gene-rearrangement (i.e. Crizotinib): Adenocarcinoma - ROS gene-rearrangement (i.e. Crizotinib): Adenocarcinoma Predictor and prognostic markers Type of adenocarcinomas have higher frequency of gene aberrations (mucinous and signet ring for ALK gene) Patient management: Response and outcome Patient quality of life: Therapy administration and toxicity

7 CYTOLOGY: EVOLUTION Sekhon et al. Thorac Surg Clin. 2013;23:163-78
8 CYTOLOGICAL AND SMALL BIOPSY DIAGNOSIS Adenocarcinoma: features suggestive of lepidic growth pattern (note: invasive component cannot be excluded) 2004 WHO AND 2011 ADENOCARCINOMA CLASSIFICATION Non-mucinous AIS(<3 cm), MIS(<3 cm with <0.5 cm invasion) and lepidic predominant (>3 cm) Mucinous adenocarcinoma (Describe pattern if identifiable) Mucinous AIS, MISand predominant pattern (lepidic, acinar, papillary, micropapillary, solid) Adenocarcinoma: features suggestive of identifiable growth pattern Adenocarcinoma with fetal pattern Adenocarcinoma with colloid pattern Adenocarcinoma (pattern) with signet ring or clear cell features Non-small carcinoma, favour adenocarcinoma (immunophenotypically consistent with adenocarcinoma) Squamous cell carcinoma (morphologically squamous cell differentiation present) Non-small carcinoma, favour squamous cell carcinoma (immunophenotypically consistent with squamous cell carcinoma) Predominant growth pattern (acinar, papillary, micropapillary and solid) Fetal Adenocarcinoma 8Mucinous or colloid adenocarcinoma Signet ring or clear cell adenocarcinoma Mostly solid pattern Squamous cell carcinoma (papillary, clear cell, small cell, basiloid variants) Squamous cell carcinoma
 Non-small cell carcinoma with neuroendocrine morphology (positive NE stains) Non-small cell carcinoma with neuroendocrine morphology (negative NE stains) Note: LCNEC suspected but")
9 CYTOLOGICAL AND SMALL Bx DIAGNOSIS Small cell carcinoma Non-small cell carcinoma, not otherwise specified (NOS) (no clear immunohistochemical profile to favour adenocarcinoma or squamous cell carcinoma) Non-small cell carcinoma with neuroendocrine morphology (positive NE stains) Non-small cell carcinoma with neuroendocrine morphology (negative NE stains) Note: LCNEC suspected but immunohistochemical stains (IHC) failed to demonstrate NE differentiation 1. Non-small cell carcinoma with squamous and adenocarcinoma morphology 2. Non-small cell carcinoma, NOS (IHC demonstrates squamous cell and adenocarcinoma differentiation) Comment: It could represent adenosquamous carcinoma 2004 WHO AND 2011 ADENOCARCINOMA CLASSIFICATION Small cell carcinoma Large cell carcinoma Large cell neuroendocrine carcinoma (LCNEC) Large cell carcinoma with NE morphology (LCNEC) Adenosquamous carcinoma Poorly differentiated non-small cell carcinoma with spindle and/or giant cell carcinoma (mention if squamous cell or adenocarcinoma differentiation present) Sarcomatoid carcinoma Travis W et al. J Thorac Oncol. 2011;6:244-85
10 CYTOLOGY: TISSUE ISSUE EBUS (lymph nodes for staging, central tumours, mediastinal tumours) EUS (lymph nodes not accessible with EBUS) Image-guided FNA (lung, pleural, chest wall, mediastinal tumours) Bronchial brush and wash Broncho-alveolar lavage Effusions Adequate specimen is the key!!!!


")
11 FNA Requisition and ROSE Two extra passes submitted in formalin for cell block after establishing rapid on site adequacy (ROSE)

12 LUNG CYTOLOGY: FNA Sekhon et al. Thorac Surg Clin. 2013;23:163-78

13 ADC and SQCC Smear CB


14 Squamous cell carcinoma Smear CB CK5/6 P40
15 Adenocarcinoma Smear CB TTF-1 Surfactant-A
16 NSCLC: Cytology +/- IHC IHC is not 100% sensitive and specific Ancillary studies!!! SQCC: p40/p63+, CK5/6+, CK7+/-, TTF-1- ADC: p40/p63-, CK5/6-, CK7+, TTF-1+/- Diagnosis of SQCC and ADC ( and ) (R. Ocque et al., Am J Clin Pathol. 2011; 136:81-7) Cytomorphology alone: 75.1% vs 40.7% Increase in IHC use: 11% to 89% vs 14.1% to 85.9% Increase in diagnostic accuracy: ADC: 56% -> 83.2 SQCC : 77% -> 74%

17 ?: Case 1 Case 2

18 Dual IHC: Case 1 Adenocarcinoma TTF-1 + Napsin P63 + CK5/6 TTF-1 + Napsin



19 Dual IHC: Case 2 Squamous cell Carcinoma P63 + CK5/6 TTF-1 + Napsin P63 + CK5/6
20 Utility of IHC in NSCLC Immunostains Adenocarcinoma Squamous cell carcinoma TTF % 6% Napsin-A 84% 21% Surfactant-A 54% 2% P40/p63 0% / 23-32% 96%/ 97% CK5/ % 93% Dual stains help conserve tissue for molecular tests


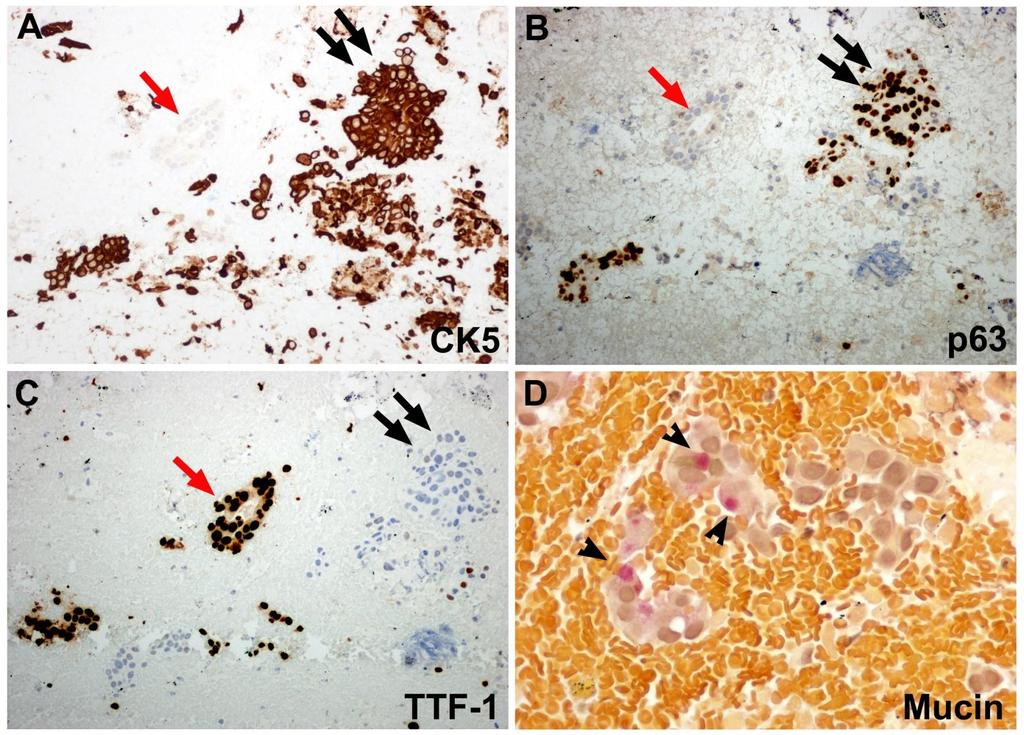
21 CYTOLOGY: IHC Panel (Canadian consensus recommendations, 2011) H&E TTF-1 p63/p40 CK5 ADC SQCC Mucin stains: Only 30% ADC contain mucin vacuoles
22 CYTOLOGY: NSCLC IHC Diffuse TTF-1 staining more specific for adenocarcinoma Minimal overlap between TTF-1 and p63+ck5/6 (Rekhtman et al., Mod Pathol. 2011; 24: ) Small number of adenocarcinomas are positive for p63, CK5/6 and 34BE12 34BE12 is not a good marker for squamous cell as P63- P63+ P63++ TTF-1++ ADC (84% any) ADC ADC TTF-1+ ADC ADC (6%) SQCC (3%) TTF-1- ADC (10%) INDET (1% + CK5/6 SQCC) SQCC (96%) (Rekhtman et al., Mod Pathol. 2011; 24: )

23 Case 3 65 yrs old gentleman, smoker (44 pack yrs) 7.1 x 5.9 cm mass in the left upper lobe, previously 5.8 x 5.3 cm; 1.7 x 2.0 cm mass in the left lower lobe Multiple granulomas are seen bilaterally Multiple enlarged lymph nodes Right hilar: 2.9 x 2.8 cm 6 cm mass in stomach assumed as GIST, YTD PH: Melanoma resected 10 yrs ago 2 MIs, stenting, cardiomegaly, CHF


24 Case 3: FNA Ddx: Sarcomatoid SQCC, melanoma, sarcoma


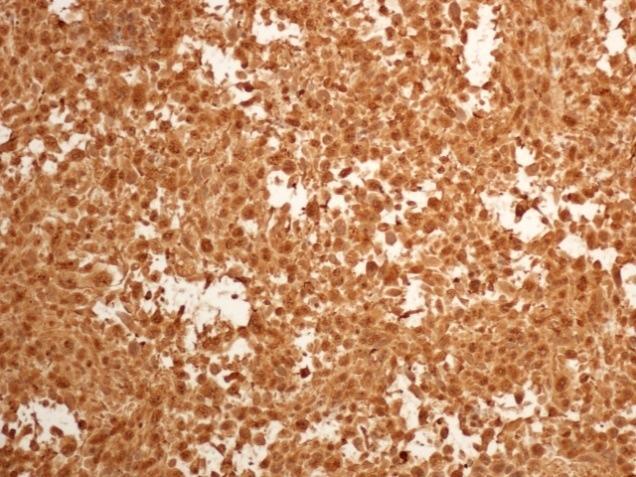
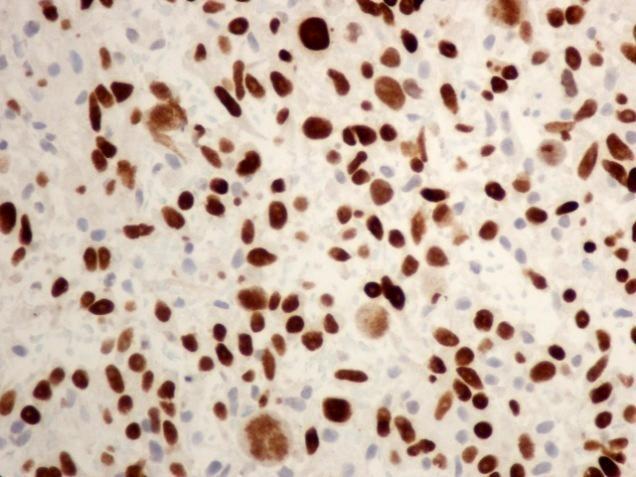
25 Sarcomatoid carcinoma CK7 Vim TTF-1 p40
26 Adeno-squamous

27 FNA LUNG MASS: ALK At least 50 countable tumour cells are required for FISH
28 IHC: SPECIFIC DIAGNOSIS 25% of NSCLC are poorly differentiated 70% of NSCLC cases are non-resectable Any mediastinal lymph node positive (N2, levels 1-9) Greater than 4 cm (ECOG score, chemo) Multiple tumours Clinical stage T3a and above: Invasion into chest wall, mediastinum and invasion into the other structures Distant metastasis Molecular testing? All cases except pure squamous cell carcinoma, pure small cell carcinoma, pure neuroendocrine carcinomas (including carcinoids) All cases where adenocarcinoma component cannot be excluded including in squamous or small cell with appropriate clinical criteria
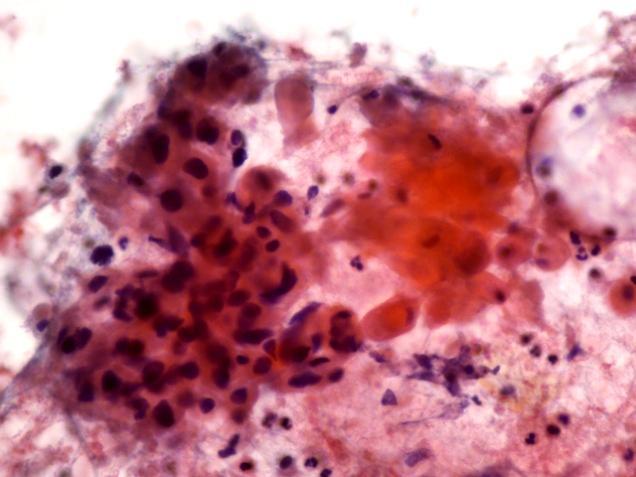
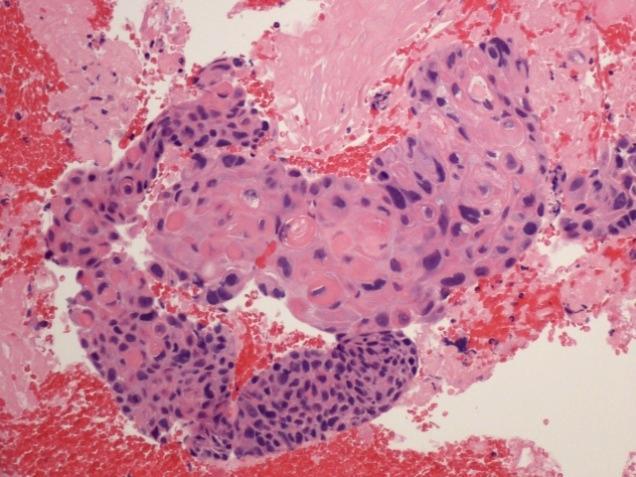
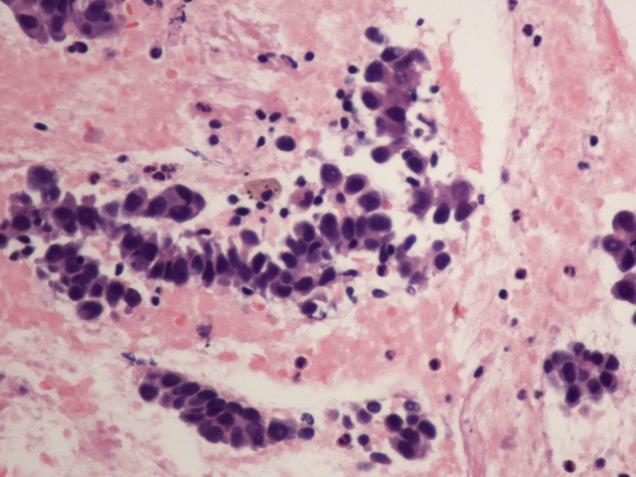
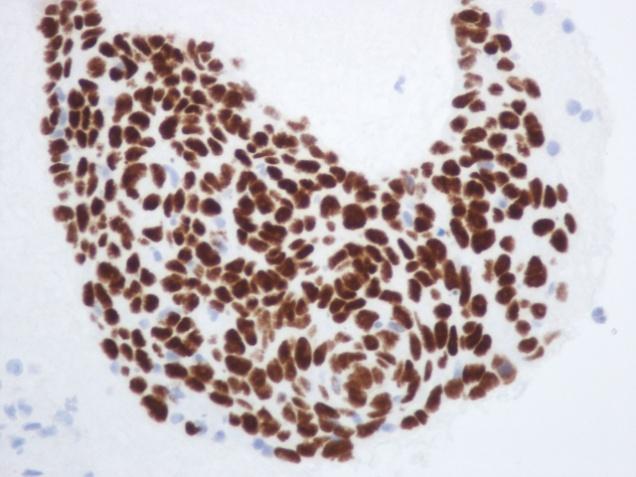
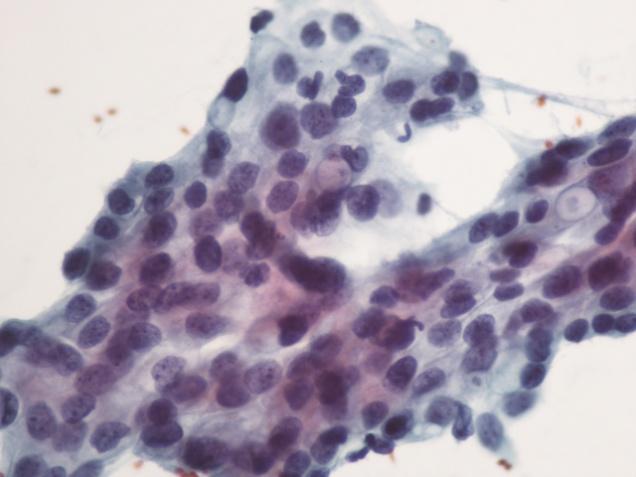
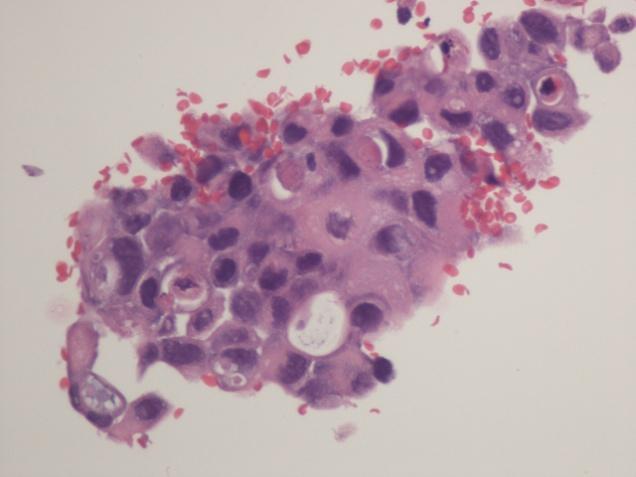
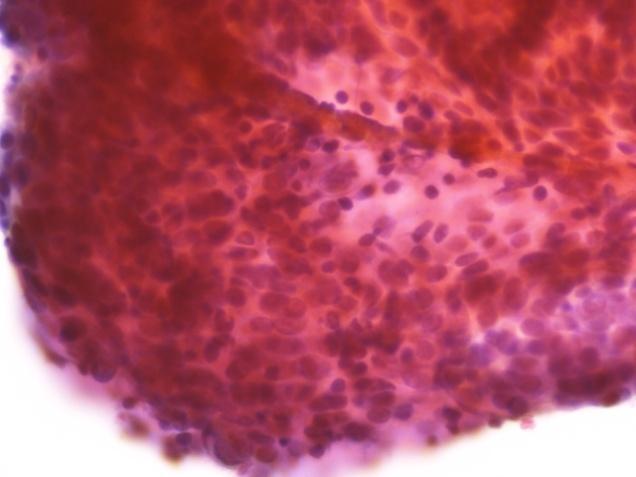
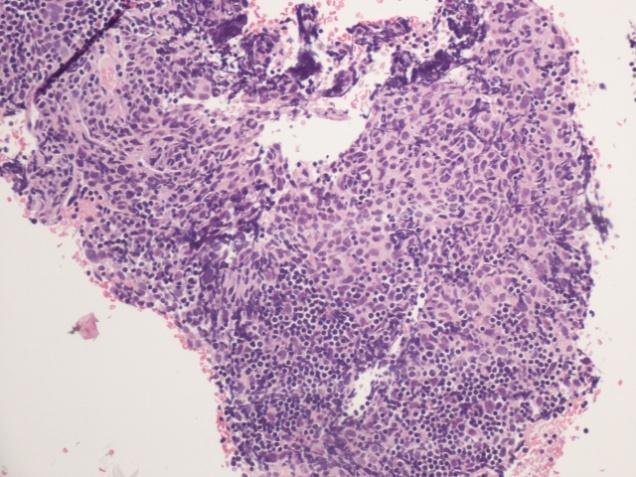
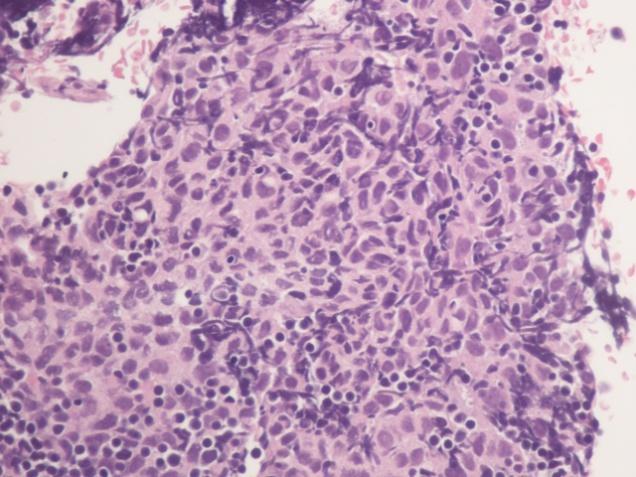
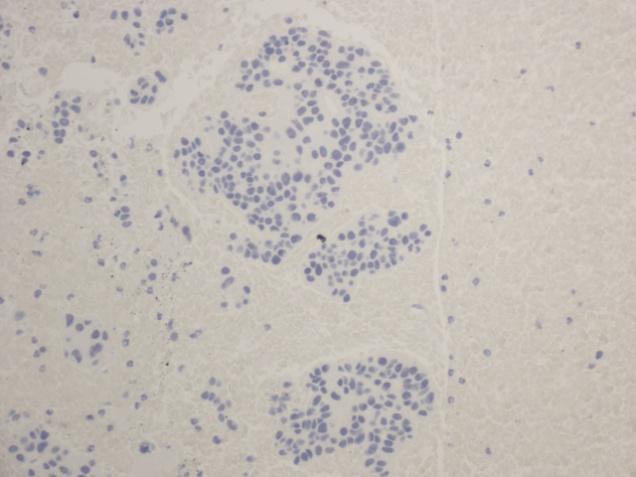
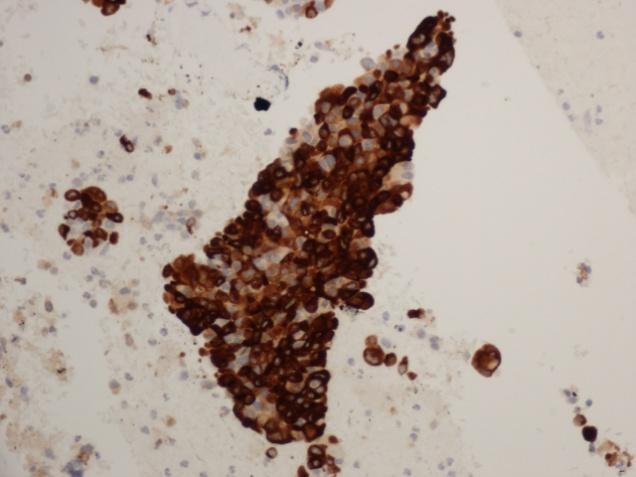
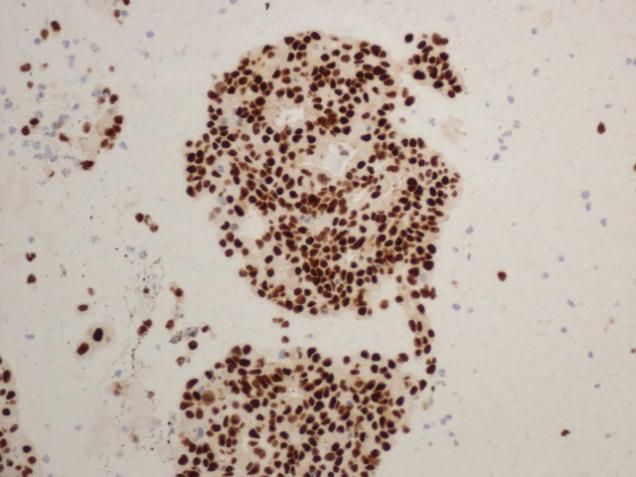
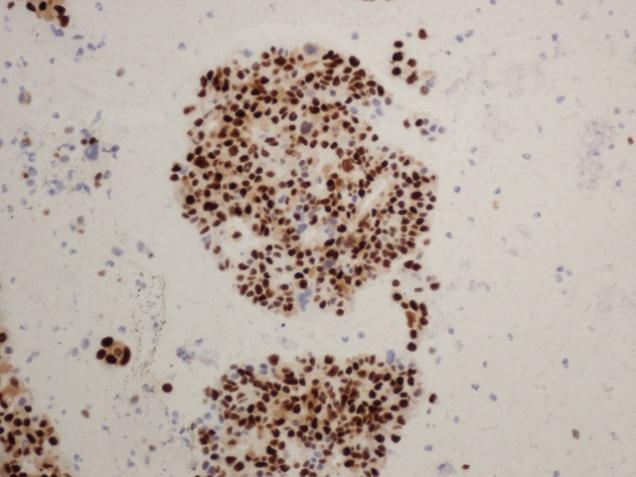
29 Case 4: NEUROENDOCRINE TUMOURS 55 year man, non-smoker Presented with a non-resolving productive cough for three months Abnormal chest X-ray followed by CT showed left lung, central mass (4.2 x 4.0 cm), circumscribed, partially occluding the main bronchus Consolidation of upper lobe Fine needle aspirate performed

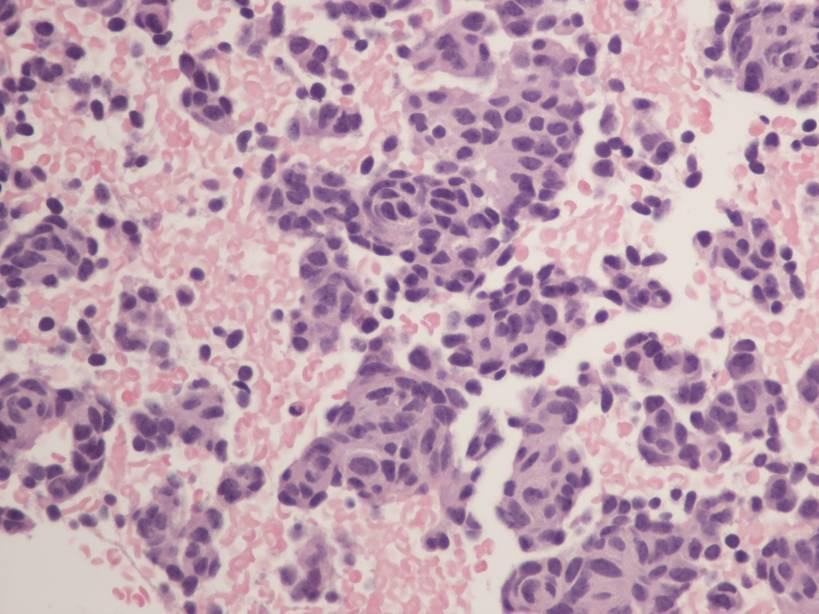
30 Case 4: FNA LUL MASS



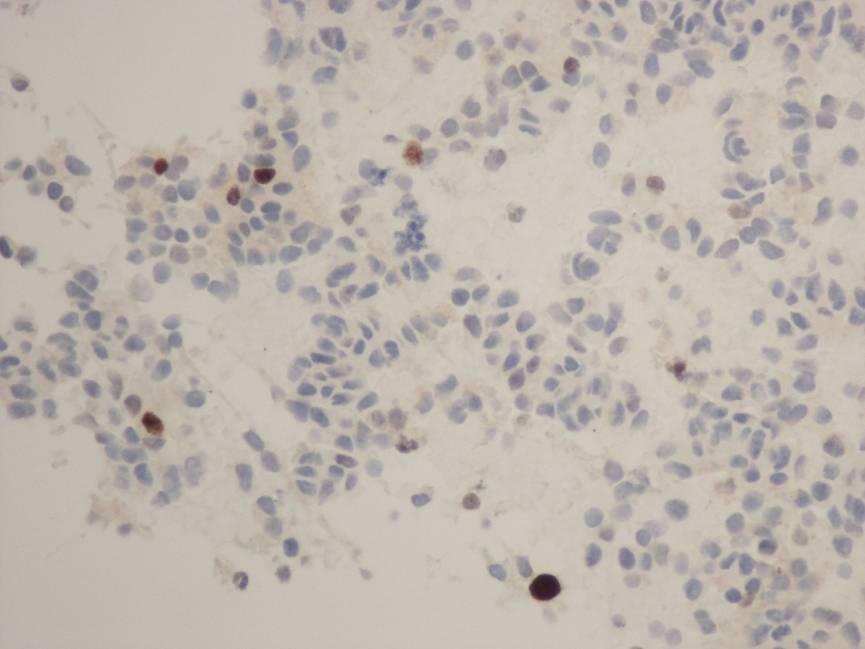
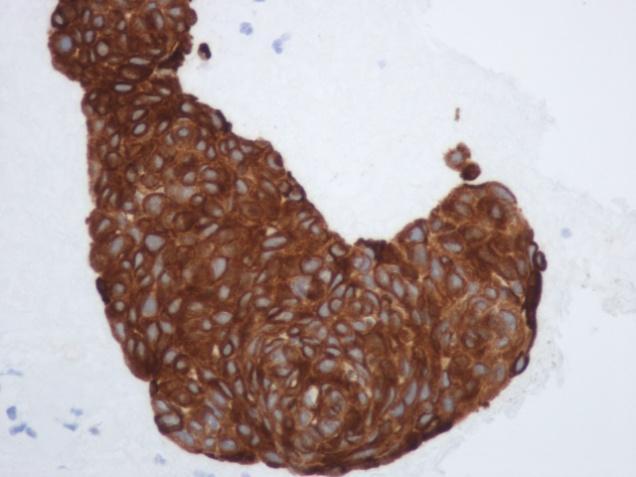
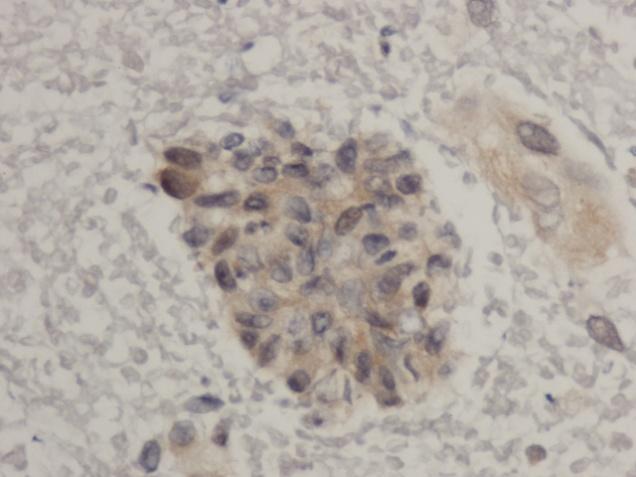
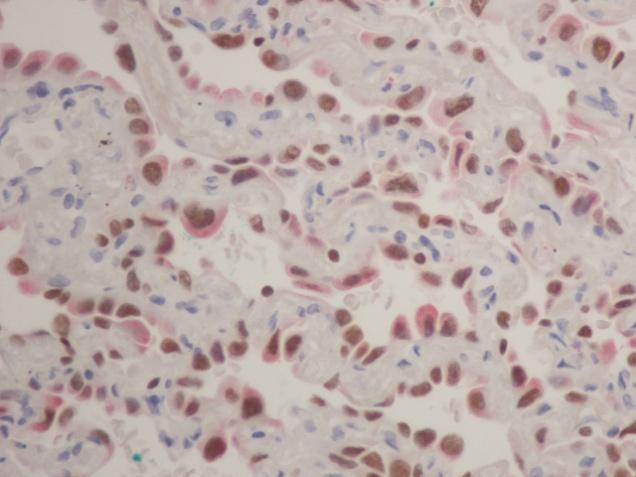
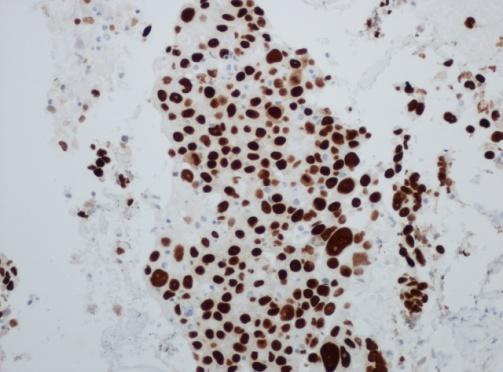
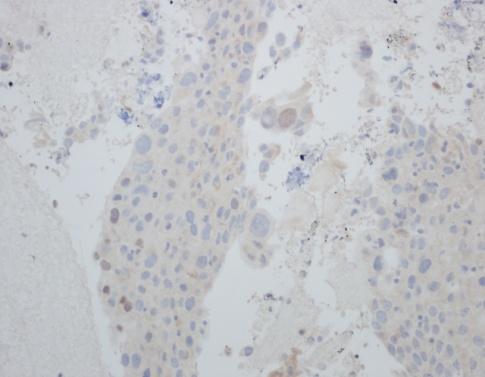
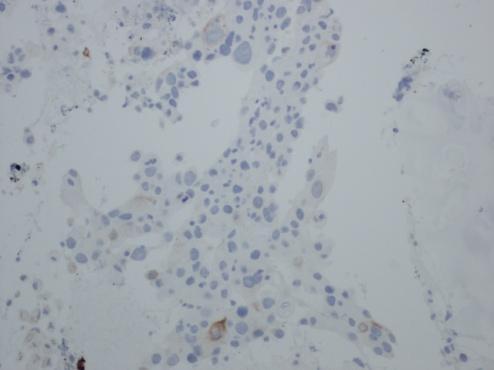
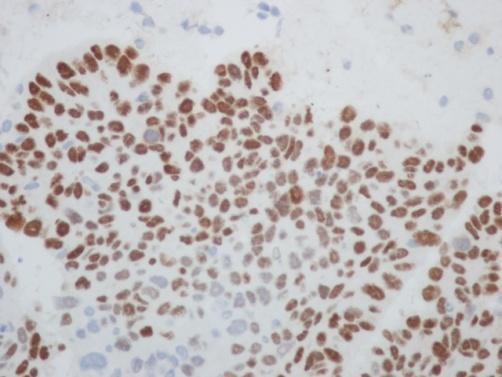
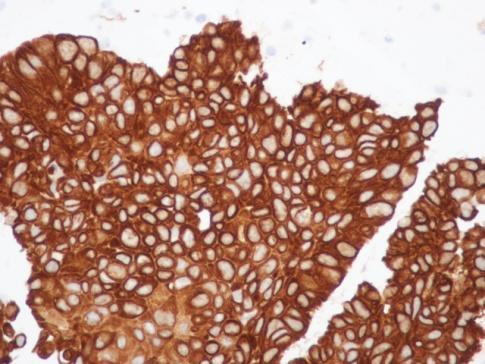
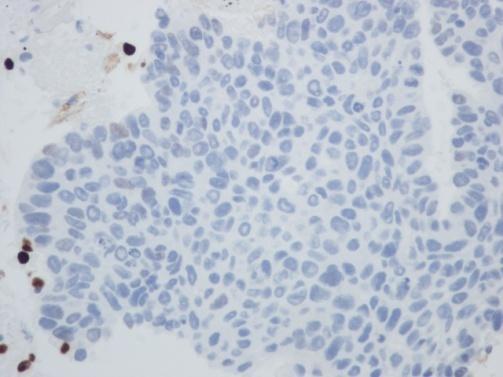
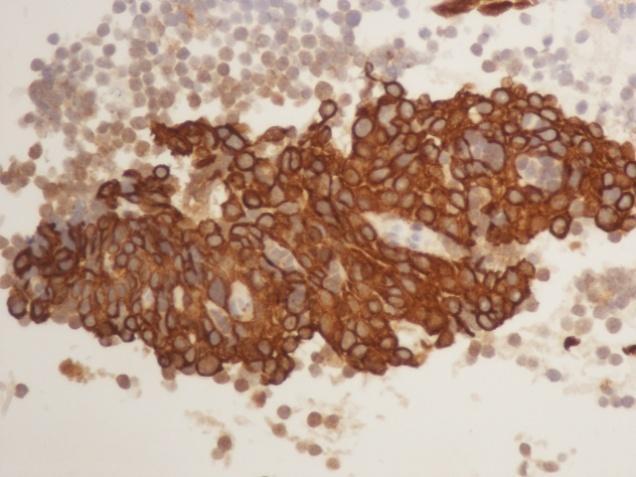
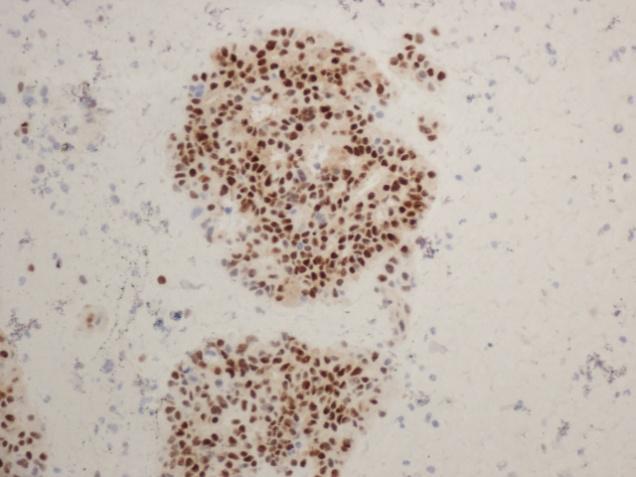
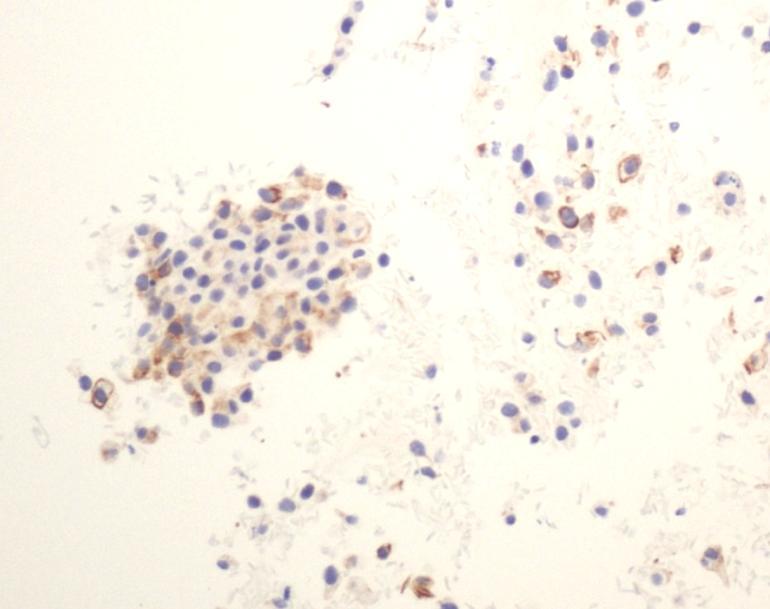
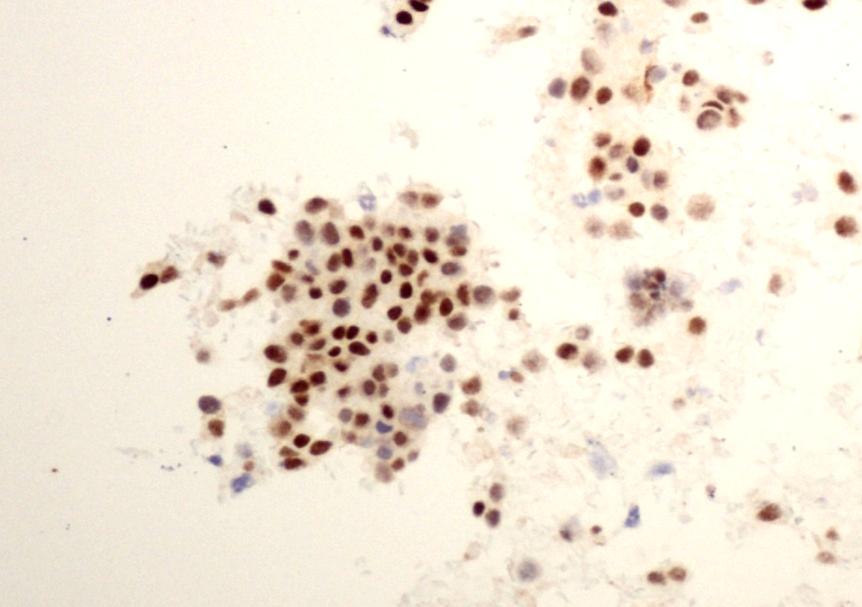
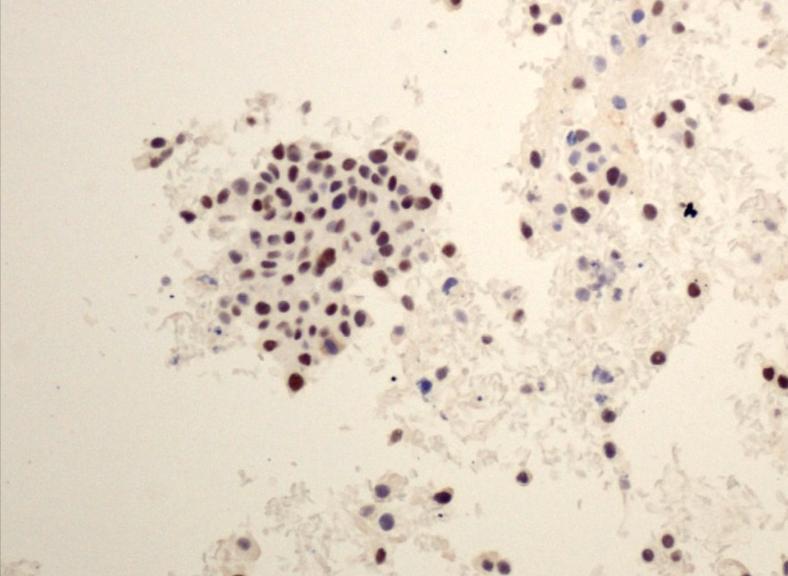
31 Case 4: FNA LUL, IHC- TYPICAL CARCINOID AE1/AE3 TTF-1 Synaptophysin Ki-67


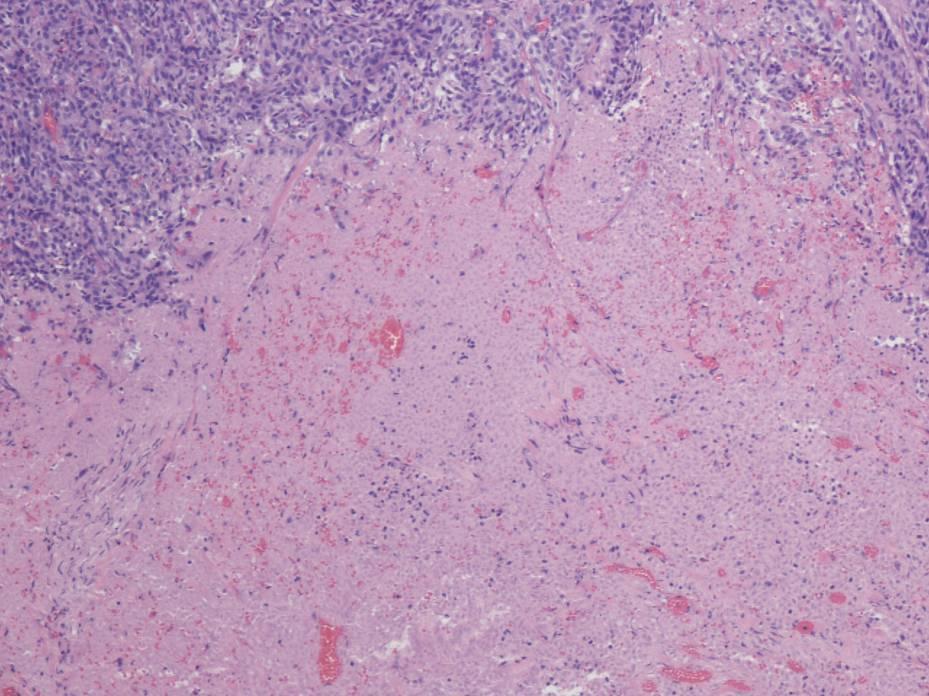
32 Pneumonectomy: ATYPICAL CARCINOID


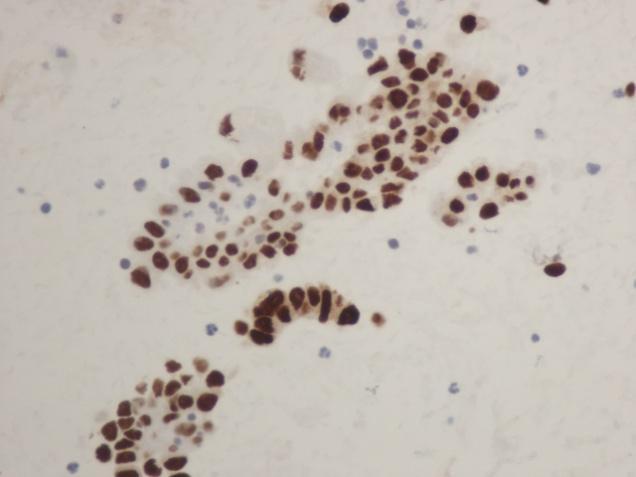
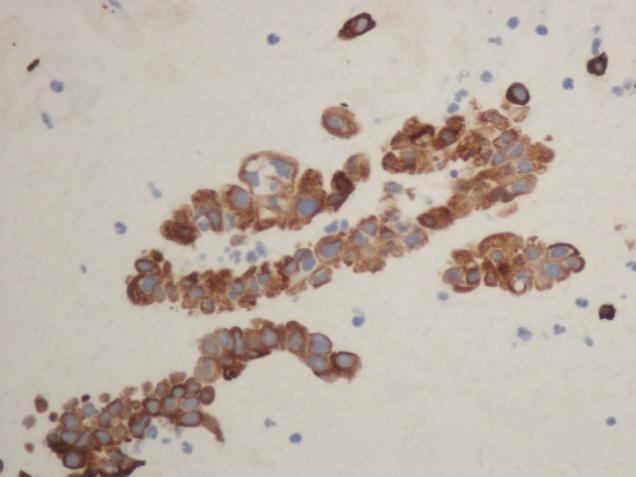
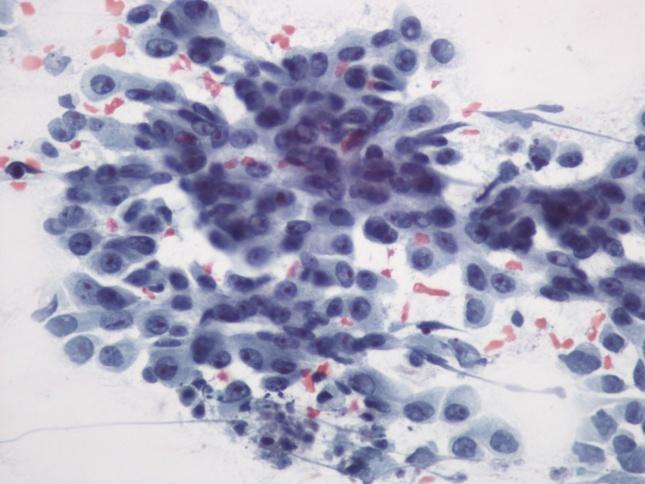
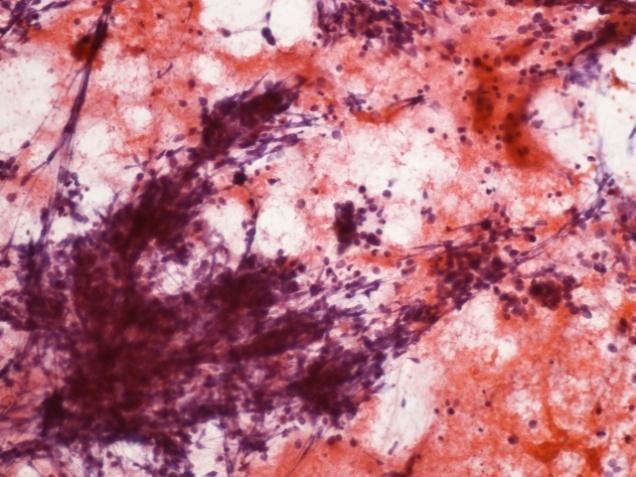
33 Case 5: Station 7 Lymph node: FNA 51 yrs woman, 48 pack yrs smoker Ill-defined central mass with bronchial thickening 21 kg weight loss over 3 months, fatigued, lethargic Multiple mediastinal lymph nodes enlarged, FNA performed


34 Case 5: Station 7 Lymph node: FNA


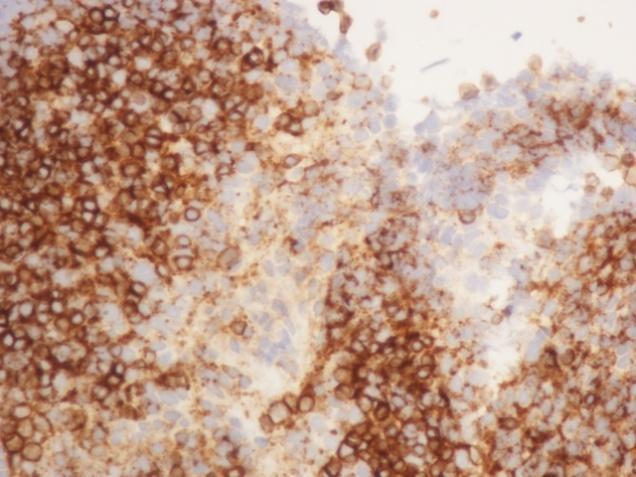
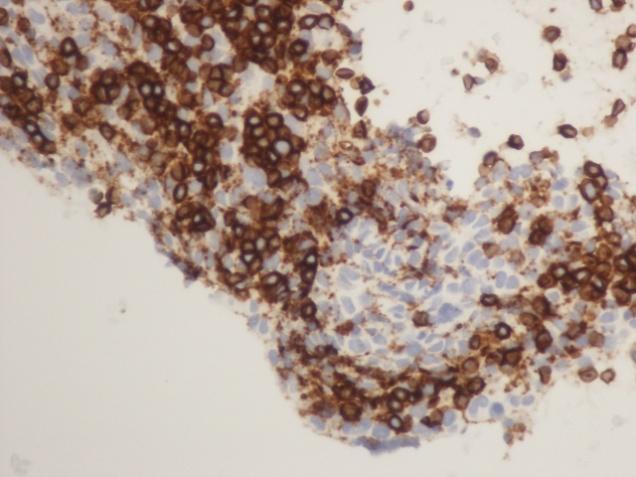
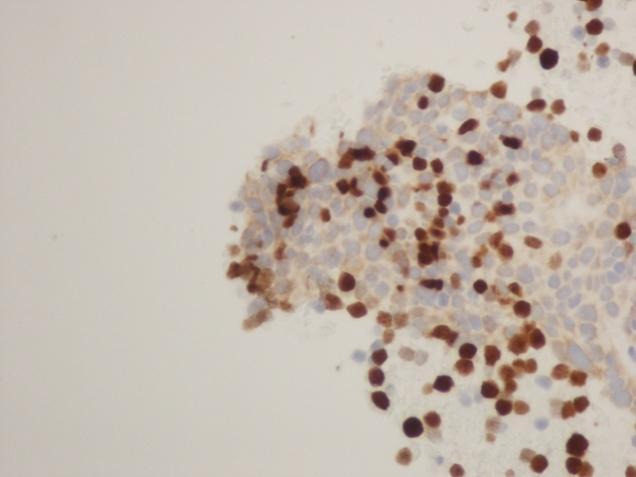
35 Case 5: Station 7 Lymph node: IHC AE1/AE3 Ki-67 Dx: Small cell carcinoma


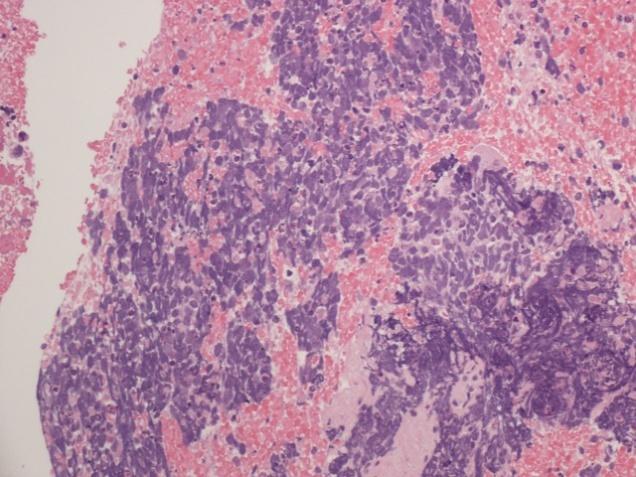
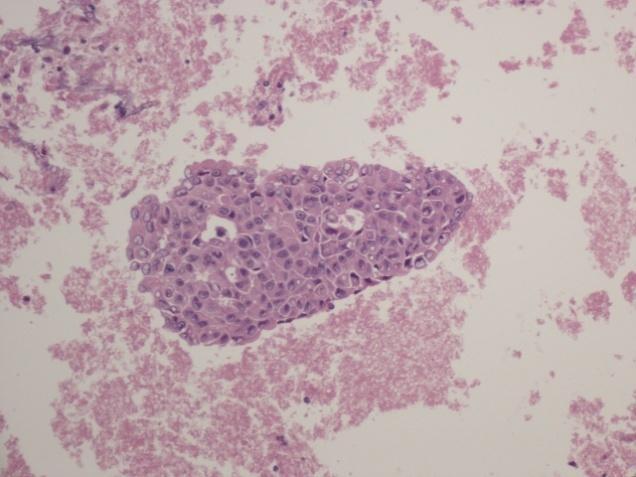
36 Case 6: Combined Small cell and ADC



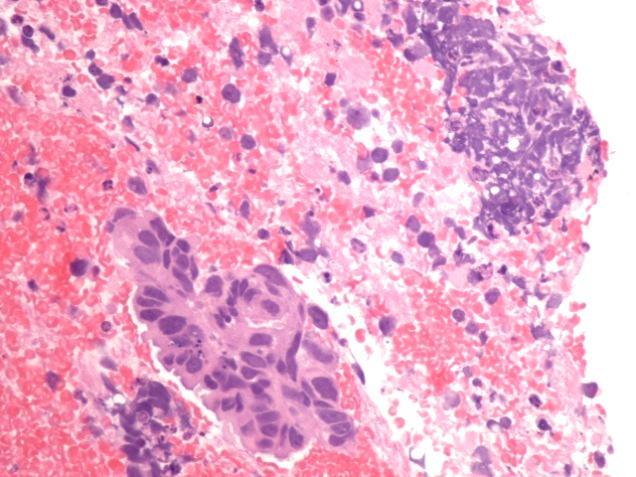
37 Case 6: Combined Small cell and ADC CB Syn CD56 TTF-1
38 IHC: NEUROENDOCRINE TUMOURS Antibodies TC AC SCLC LCNEC NSCLC Synaptophysin Focal <20% CD Focal <20% Chromo + + +/- + - TTF-1 +/- +/- + +/- AD+/SQ- PANCK + + Dot-like + + Ki % (~2%) 5-20% (~10%) >25% (~70%) >25% (~40%) Variable Modified from Rekhtman N. Arch Pathol Lab Med.2010;134: )
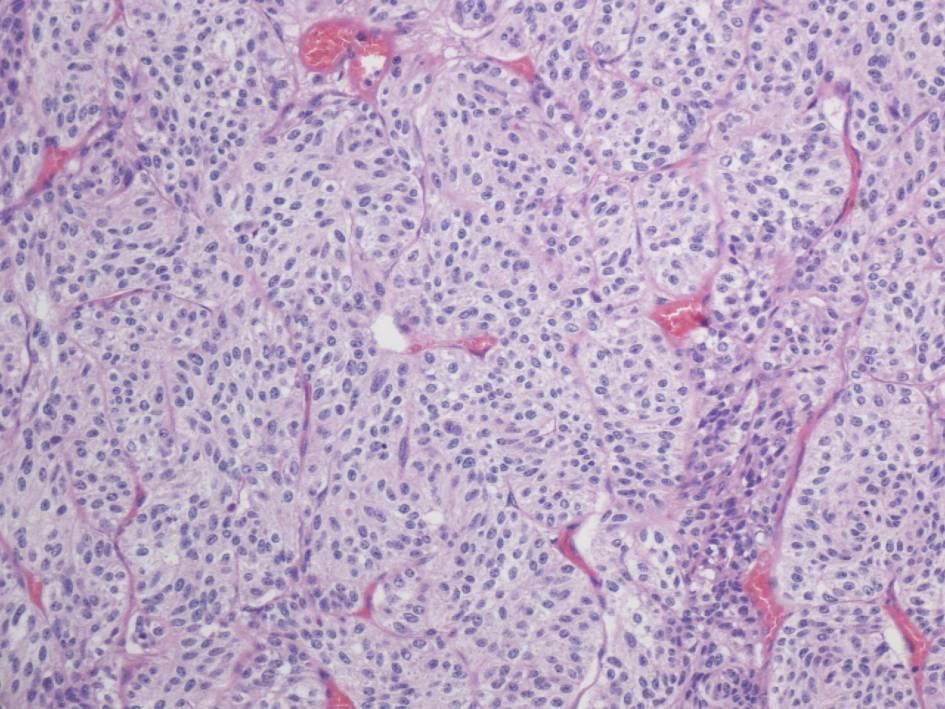
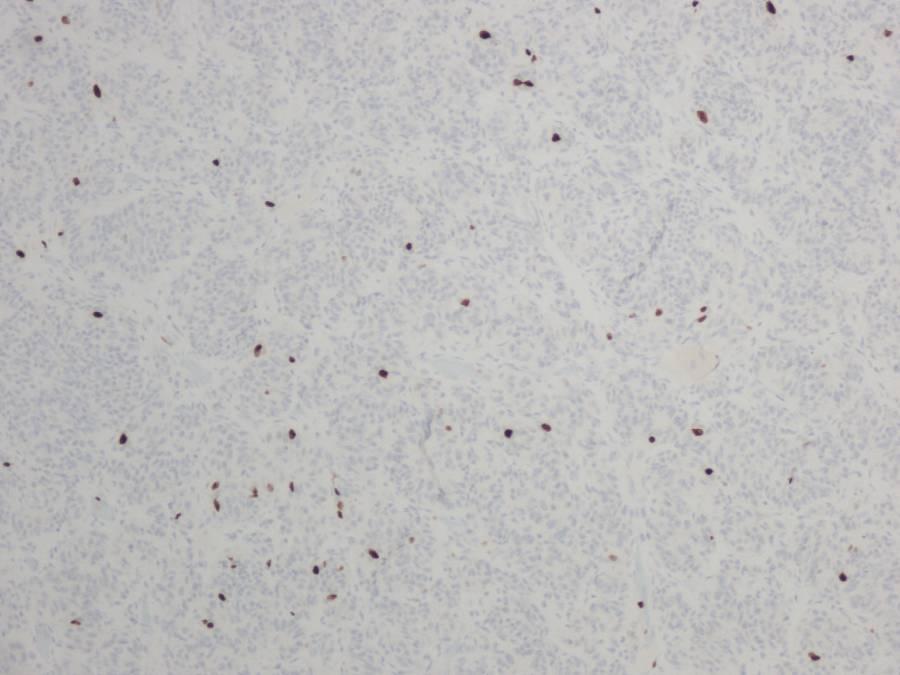
39 Case 7 58 year old man, smoker, AA, DA Cough for 1 month slowly resolved with antibiotics CT finding: Incidental, 2.3 x 2.2 cm cirumscribed, left upper lobe mass followed for three months with small increase in size No symptoms CT-Guided FNA performed

40 Case 7: LUNG MASS
41 INTRAPULMONARY B2 THYMOMA PAN-CK CD99 CD1a TdT




42 MEDIASTINAL MASS: TYPE A THYMOMA Thymoma and carcinoma Thyroid carcinoma Teratoma and other germ cell tumours T-cell lymphoma Tumour metastasis PAN-CK TdT
43 Case 8 58 yrs female, non-smoker 1.2 cm right middle lobe lesion, circumscribed, paracentral 4R lymph node enlarged 1.5 cm History: Colon Carcinoma 2012, Breast Ca 1999 EBUS of 4R


44 Case 8: FNA: EBUS 4R Lymph node TTF-1
45 Case 8: Metastatic Breast Ca Mammaglobin GATA3 ER PR

46 LUL MASS: Clear cell renal carcinoma Sekhon et al. Thorac Surg Clin. 2013;23:163-78

47 RUL MASS: UCC metastasis CK7 CK20 GATA-3 p63
48 Common metastasis: IHC Profile IHC Lung Colon Breast Thyroid UCC CK CK /- TTF CDX ER Mammaglobin GATA PAX Thyroglobulin




49 Test Case: Question 67 yrs old gentleman, current smoker, laryngeal squamous cell carcinoma 5 years ago, presented with a paracentral, circumscribed, 5.5 cm mass with N2 nodes positive for metastasis. FNA was done and immunostains performed showed the following profile: CK5 p40 CK7 TTF-1
50 Question: 1. Treatment with Bevacizumab is contra-indicated in this patient 2. ALK stain to determine ALK gene-rearrangement and EGFR mutation analysis should be performed for treatment with Gefitinib or Crizotinib 3. This neuroendocrine carcinoma and the patient would need radiation therapy and surgery 4. This is metastasis from the laryngeal carcinoma
51 Question: Answer 1. Treatment with Bevacizumab is contra-indicated in this patient 2. ALK stain to determine ALK gene-rearrangement and EGFR mutation analysis should be performed for treatment with Gefitinib or Crizotinib 3. This neuroendocrine carcinoma and the patient would need radiation therapy and surgery 4. This is metastasis from the laryngeal carcinoma

52
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE. Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University
 EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Ground Glass Opacities
 Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES)
") SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP
 Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University Pulmonary Pathologist and Cytopathologist, QEII HSC Senior Scientist, Beatrice Hunter Cancer
Lung Cancer Update on Pathology Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University Pulmonary Pathologist and Cytopathologist, QEII HSC Senior Scientist, Beatrice Hunter Cancer
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
5/1/2009. Squamous Dysplasia/CIS AAH DIPNECH. Adenocarcinoma
 Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Lung/Thoracic Neoplasms. Manish Powari
 Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens
 is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens") Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Insulinoma-associated protein (INSM1) is a sensitive and specific marker for lung neuroendocrine tumors in cytologic and surgical specimens Kartik Viswanathan, M.D., Ph.D New York Presbyterian - Weill
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas
 Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Diagnostic & Predictive Immunohistochemistry in Lung Carcinomas Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Associate Professor, Harvard Medical School Boston, MA Disclosures
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
EBUS-TBNA Diagnosis and Staging of Lung Cancer
 EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center
 The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings
 CASE REPORT Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings Makoto Nagashima 1, Ayako Moriyama 1, Yasuo
CASE REPORT Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings Makoto Nagashima 1, Ayako Moriyama 1, Yasuo
Cytology and the Investigation of Carcinoma of Unknown Primary (CUP) Dr Anna Green ST5, St Thomas Hospital London, UK
 Dr Anna Green ST5, St Thomas Hospital London, UK") Cytology and the Investigation of Carcinoma of Unknown Primary (CUP) Dr Anna Green ST5, St Thomas Hospital London, UK Objectives Introduction to CUP Our experience of cytology and CUP Role of Cytology
Cytology and the Investigation of Carcinoma of Unknown Primary (CUP) Dr Anna Green ST5, St Thomas Hospital London, UK Objectives Introduction to CUP Our experience of cytology and CUP Role of Cytology
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Case Studies. Ravi Salgia, MD, PhD
 Case Studies Ravi Salgia, MD, PhD Professor and Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Associate Director for Clinical Sciences Research City of Hope 04-21-2018 Objectives
Case Studies Ravi Salgia, MD, PhD Professor and Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Associate Director for Clinical Sciences Research City of Hope 04-21-2018 Objectives
Minimally invasive adenocarcinoma. 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS)
") Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Utility of small biopsies for diagnosis of lung nodules: doing more with less
 & 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
& 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Tumor Board Discussions: Case 1
 Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
CYTOPATHOLOGIC AND MOLECULAR DIAGNOSTIC ISSUES IN LUNG CYTOPATHOLOGY
 COMPANION MEETING Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory CYTOPATHOLOGIC AND MOLECULAR DIAGNOSTIC ISSUES IN LUNG CYTOPATHOLOGY Prof. Fernando Schmitt
COMPANION MEETING Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory CYTOPATHOLOGIC AND MOLECULAR DIAGNOSTIC ISSUES IN LUNG CYTOPATHOLOGY Prof. Fernando Schmitt
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
Neuroendocrine neoplasms of the lung
 Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Neuroendocrine neoplasms of the lung M Papotti, L Righi, & M Volante University of Turin at San Luigi Hospital TORINO NETs OF THE LUNG Menu - Spectrum of NE lung tumors - CARCINOID TUMORS - SCLC /LCNEC
Accuracy of cell typing in nonsmall cell lung cancer by EBUS/EUS FNA cytological samples
 Eur Respir J 2011; 38: 911 917 DOI: 10.1183/09031936.00176410 CopyrightßERS 2011 Accuracy of cell typing in nonsmall cell lung cancer by EBUS/EUS FNA cytological samples W.A.H. Wallace* and D.M. Rassl
Eur Respir J 2011; 38: 911 917 DOI: 10.1183/09031936.00176410 CopyrightßERS 2011 Accuracy of cell typing in nonsmall cell lung cancer by EBUS/EUS FNA cytological samples W.A.H. Wallace* and D.M. Rassl
Historical Note 5/2/2017. Advances in Lung Cancer Cytohistology. Purpose of FNA in Patients with Lung Cancer
 Advances in Lung Cancer Cytohistology Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Purpose of FNA in Patients
Advances in Lung Cancer Cytohistology Martha Bishop Pitman, M.D. Director, Cytopathology Massachusetts General Hospital Professor of Pathology Harvard Medical School Boston, MA Purpose of FNA in Patients
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
Lecture Goals. Lung (Bronchogenic) Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic
 Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic") Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
What I Learned from 3 Cases and 3 Antibodies
 What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
Cool Stains for Hot Diagnoses in Thoracic Pathology
 Cool Stains for Hot Diagnoses in Thoracic Pathology Anja C. Roden, M.D. Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA No disclosures Disclosure Learning Objectives Know
Cool Stains for Hot Diagnoses in Thoracic Pathology Anja C. Roden, M.D. Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, USA No disclosures Disclosure Learning Objectives Know
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
Applying Genomics to Cancer 21 st September The Frequency of EGFR mutations in Lung Adenocarcinoma: The Cardiff Experience
 Applying Genomics to Cancer 21 st September 2015 The Frequency of EGFR mutations in Lung Adenocarcinoma: The Cardiff Experience Aled Daniels R Butler, R Attanoos, H Davies University Hospital of Wales
Applying Genomics to Cancer 21 st September 2015 The Frequency of EGFR mutations in Lung Adenocarcinoma: The Cardiff Experience Aled Daniels R Butler, R Attanoos, H Davies University Hospital of Wales
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
A nonresponding small cell lung cancer combined with adenocarcinoma
 Case Report A nonresponding small cell lung cancer combined with adenocarcinoma Hongyang Lu 1,2, Shifeng Yang 3 1 Zhejiang Key Laboratory of Diagnosis & Treatment Technology on Thoracic Oncology (Lung
Case Report A nonresponding small cell lung cancer combined with adenocarcinoma Hongyang Lu 1,2, Shifeng Yang 3 1 Zhejiang Key Laboratory of Diagnosis & Treatment Technology on Thoracic Oncology (Lung
CME/SAM. Rebecca Ocque, MD, Naobumi Tochigi, MD, N. Paul Ohori, MD, and Sanja Dacic, MD, PhD. Abstract
 Anatomic Pathology / Lung Carcinoma Classification Usefulness of Immunohistochemical and Histochemical Studies in the Classification of Lung Adenocarcinoma and Squamous Cell Carcinoma in Cytologic Specimens
Anatomic Pathology / Lung Carcinoma Classification Usefulness of Immunohistochemical and Histochemical Studies in the Classification of Lung Adenocarcinoma and Squamous Cell Carcinoma in Cytologic Specimens
The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer
 The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School & Aberdeen Royal Infirmary, UK The management
The role of the Pathologist in the diagnosis and biomarker profiling of Lung Cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School & Aberdeen Royal Infirmary, UK The management
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS
 THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Mediastinal Mysteries: What can be solved with EBUS?
 Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Serous Effusions. Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland
 Serous Effusions Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Serous membrane Body cavities: Pleural Pericardial Peritoneal Effusion = Excess of fluid 80% Benign 20% Malignant
Serous Effusions Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Serous membrane Body cavities: Pleural Pericardial Peritoneal Effusion = Excess of fluid 80% Benign 20% Malignant
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as