Metastatic prostate carcinoma. Lee Say Bob July 2017
|
|
|
- Cornelia Cecilia Wilkins
- 6 years ago
- Views:
Transcription
1 Metastatic prostate carcinoma Lee Say Bob July 2017
2 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history of CVD with a cardiac stent inserted 2 years ago and is on Aspirin. Discuss management options: Antiandrogen vs LHRH analog vs LHRH antagonist
3 Hormonal therapy Androgen deprivation (ADT) can be achieved by suppressing the secretion of testicular androgens Medical castration Surgical castration inhibiting the action of circulating androgens at the level of their receptor. Complete androgen blockade (CAB)
4 LHRH agonists Long-acting LHRH agonists are currently the main forms of ADT. Delivered as depot injections on a 1-, 2-, 3-, 6-monthly, or yearly basis. After the first injection induce a transient rise in LH and FSH leading to the testosterone surge or flare-up phenomenon, which starts 2 to 3 days after administration and lasts for 1w.
5 LHRH agonists MOA: Stimulation of LHRH receptors in the pituitary produces an initial increase in LH and FSH, which causes an initial increase in testosterone. Further LHRH agonism suppresses LH and FSH secretion, resulting in a decrease in testosterone. Eg: Leuprolide (Lupron, Eligard) Histrelin (Vantas) Goserelin (Zoladex) Triptorelin (Trelstar) A castration level - within 2 to 4 weeks.
6 Flare-up phenomenon The flare-up phenomenon might lead to detrimental clinical effects (the clinical flare) such as increased bone pain acute BOO obstructive renal failure spinal cord compression cardiovascular death due to hypercoagulation status. Pts at risk are usually those with high-volume symptomatic bony disease
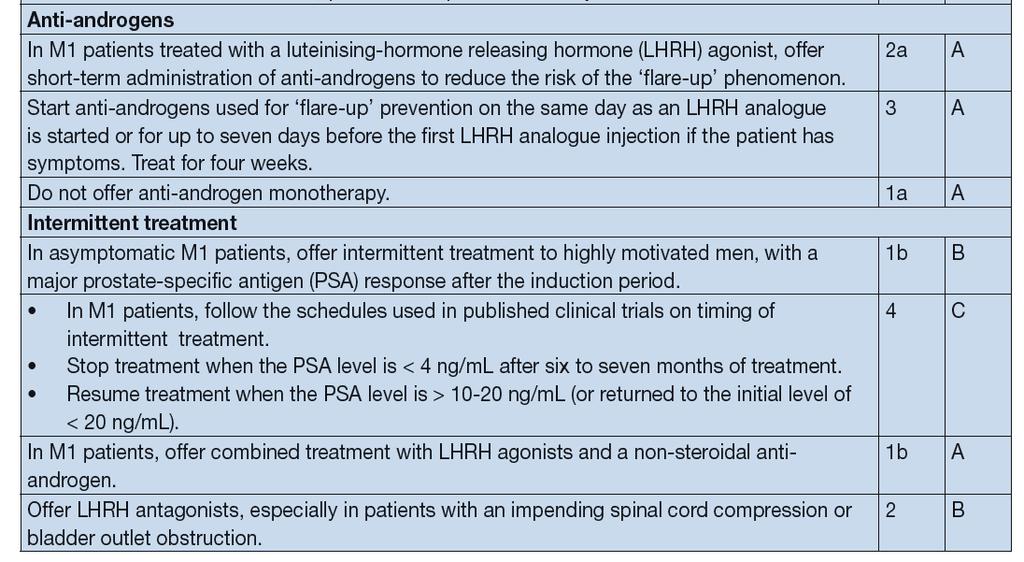
7 Prevention of flare-up Concomitant therapy with an anti-androgen decreases the incidence of clinical flare, but does not completely remove the risk. Prevention of flare-up is important in symptomatic patients or when a clinical flare might lead to severe complications. Anti-androgen therapy is usually continued for 4 weeks.
8 LHRH antagonists Bind to LHRH receptors, leading to a rapid decrease in LH, FSH and testosterone levels without any flare. The practical shortcoming of these compounds is the lack of a long-acting depot formulation with only monthly formulations being available.
9 LHRH antagonists Degarelix is an LHRH antagonist 240 mg in the first month Followed by monthly injections of 80 mg Castrate level at day 3. Its definitive superiority over the LHRH analogues remains to be proven. AST, ALT and GGT increased in 10% of pts. Injection site irritation (40%) vs LHRH agonists (3%).
10 Morbidity from Medical or Surgical Castration S/e from castration increases with the duration of tx Changes in body habitus (gynecomastia, testicular atrophy, loss of muscle mass, weight gain, increased subcut fat) Adverse lipid profile Diabetes (insulin resistance) CVD Anaemia (normocytic) Fatigue Osteoporosis Periodontal disease Sexual dysfunction Infertility Hot flashes Cognitive deficits
11 Anti-androgens Classified accd to their chemical structure as: steroidal cyproterone acetate (CPA) megestrol acetate medroxyprogesterone acetate non-steroidal/pure nilutamide flutamide bicalutamide
12 Anti-androgens MOA: Compete with androgens at the receptor level. This is the sole action of non-steroidal antiandrogens and leads to an unchanged or slightly elevated testosterone level. Steroidal antiandrogens have progestational properties leading to central inhibition by crossing the BBB.
13 Non-steroidal anti-androgens Non-steroidal anti-androgen monotherapy does not suppress testosterone secretion and it is claimed that libido, overall physical performance and bone mineral density (BMD) are frequently preserved. Non-androgen pharmacological s/e differ between agents, with bicalutamide showing a more favourable safety and tolerability profile than flutamide and nilutamide. Potential liver toxicity (occasionally fatal), requiring regular monitoring of pts liver enzymes.
14 CAB Monotherapy IAD vs Continuous ADT Immediate vs delayed ADT Hormonal tx combined with chemo
15 Combination therapies (CAB) The largest RCT in 1,286 M1b pts found no difference between surgical castration with or w/o flutamide. However, results with other anti-androgens or castration modalities have differed and SRs have shown that CAB using a non-steroidal anti-androgen (NSAA) appears to provide a small survival advantage (< 5%) vs. monotherapy (surgical castration or LHRH agonists) beyond 5 years of survival but this minimal advantage in a small subset of pts must be balanced against the increased s/e a/w long-term use of NSAAs.
16 Non-steroidal anti-androgen monotherapy Based on a Cochrane SR comparing NSAA monotherapy to castration (either medical or surgical), NSAA was considered to be less effective in terms of OS clinical progression treatment failure and treatment discontinuation due to adverse events. The evidence quality of the studies included in this review was rated as moderate.
17 Intermittent versus continuous androgen deprivation therapy 3 independent reviews and 2 meta-analyses, looked at the clinical efficacy of IAD therapy included 8 RCTs of which only 3 were conducted in pts with exclusively M1 disease. 5 remaining trials included different pt groups, mainly locally advanced and metastatic pts relapsing. SWOG 9346 is the largest trial conducted in M1b patients. Out of 3,040 selected pts, only 1,535 were randomised based on the inclusion criteria set. At best, only 50% of M1b pts might be candidates for IAD, i.e. the best PSA responders.
18 IAD None of the trials addressing M1 pts only showed a survival benefit, but there was a trend favouring continuous treatment for OS and PFS. Trend favouring IAD in terms of QoL, esp regarding tx-related s/e, such as hot flushes. In some cohorts the negative impact on sexual function was less pronounced Other possible long-term benefits of IAD include bone protection and a protective effect against metabolic syndrome.
19 IAD No benefit observed for the endocrine, psychiatric, sexual and neurological s/e based on a detailed analysis from the SWOG 9346 trial. Testosterone recovery was observed in most studies leading to intermittent castration. Must only be considered as an option in a well-informed patient bothered by significant s/e and willing to avoid them.
20 IAD The PSA threshold at which ADT must be stopped or resumed still needs to be defined in prospective studies. Consensus amongst authors on some statements: IAD is based on intermittent castration; therefore, only drugs leading to castration are suitable. LHRH antagonist might be a valid alternative to an agonist. The induction cycle cannot be longer than 9 months, otherwise testosterone recovery is unlikely.
21
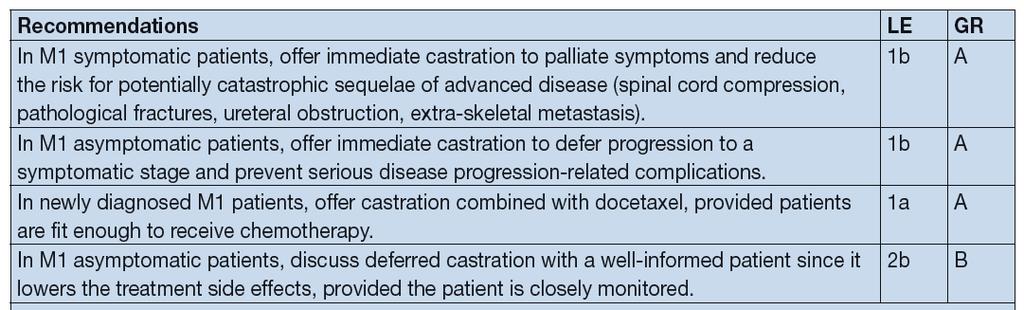
22 Immediate versus deferred ADT In symptomatic pts, immediate tx is mandatory. Controversy exists for asymptomatic metastatic pts due to the lack of quality studies. A Cochrane review extracted 4 good-quality RCTs: VACURG I trial VACURG II trial MRC trial ECOG 7887 study All of these studies were conducted in the pre-psa era and included pts with advanced PCa, who had received early vs. deferred ADT, either as primary therapy or as adjuvant therapy after RP. No improvement in OS was observed in the M1a/b population, although early ADT significantly reduced disease progression and assc cx.
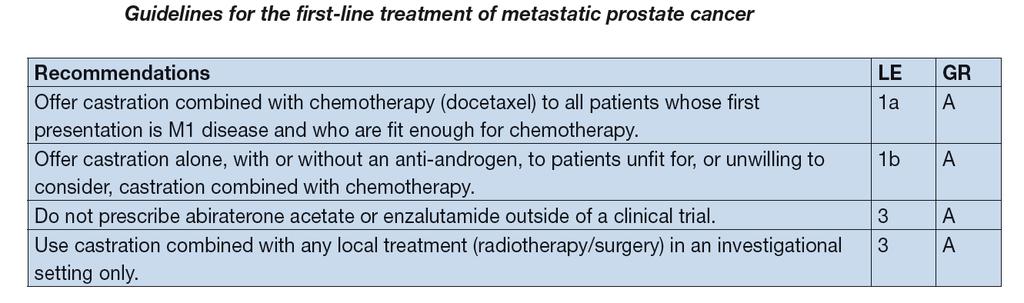
23 Hormonal treatment combined with chemotherapy 3 large RCT were conducted. GETUG 15 trial CHAARTED STAMPEDE All trials compared ADT alone as the standard of care with ADT combined with immediate docetaxel (75 mg/sqm, every 3w) (within 3 mths of ADT initiation). The primary objective in all three studies was OS. >> Upfront docetaxel combined with ADT should be considered as a new standard in men presenting with metastases at 1 st presentation, provided they are fit enough to receive the drug
24 EAU 2017
25 EAU 2017
26 Conclusion A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history of CVD with a cardiac stent inserted 2 years ago and is on Aspirin. Options LHRH antagonist LHRH agonist + antiandrogen (4 weeks) Bilateral orchidectomy Chemotherapy
27 Summary There is no level 1 evidence for, or against, a specific type of ADT, whether orchiectomy, an LHRH analogue or antagonist, except in patients with impending spinal cord compression for whom either a bilateral orchidectomy, or an LHRH antagonist are the preferred options.
28 Thank You
29 Primary ADT has been the standard of care for over 50 years. There is no level 1 evidence for, or against, a specific type of ADT, whether orchiectomy, an LHRH analogue or antagonist, except in patients with impending spinal cord compression for whom either a bilateral orchidectomy, or an LHRH antagonist are the preferred options.
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Androgen Deprivation Therapy Its impact and the nursing role. Jane Thacker Uro-Oncology Nurse Specialist
 Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer
 Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
2. The effectiveness of combined androgen blockade versus monotherapy.
 Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
Clinical Policy: Enzalutamide (Xtandi) Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19
 Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19") Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline
 Treatment Guideline") Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Hormonotherapy of advanced prostate cancer
 Annals of Oncology 16 (Supplement 4): iv80 iv84, 2005 doi:10.1093/annonc/mdi913 Hormonotherapy of advanced prostate cancer P. Pronzato & M. Rondini Department of Oncology, Felettino Hospital, La Spezia,
Annals of Oncology 16 (Supplement 4): iv80 iv84, 2005 doi:10.1093/annonc/mdi913 Hormonotherapy of advanced prostate cancer P. Pronzato & M. Rondini Department of Oncology, Felettino Hospital, La Spezia,
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
The Current State of Hormonal Therapy for Prostate Cancer
 The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Intermittent Androgen Suppression - A standard of care or a good second choice?
 Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
reviews LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate therapy
 reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG. (goserelin)
") ONC.000-092-861.10.0 PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG (goserelin) Name of the medicinal product Zoladex LA 10.8mg depot Qualitative and quantitative composition Goserelin acetate (equivalent to 10.8
ONC.000-092-861.10.0 PACKAGE LEAFLET TEXT ZOLADEX LA 10.8MG (goserelin) Name of the medicinal product Zoladex LA 10.8mg depot Qualitative and quantitative composition Goserelin acetate (equivalent to 10.8
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
M0BCore Safety Profile. Active substance: Triptorelin Pharmaceutical form(s)/strength: 0,1 mg P-RMS: DE/H/PSUR/0038/002 Date of FAR:
/strength: 0,1 mg P-RMS: DE/H/PSUR/0038/002 Date of FAR:") M0BCore Safety Profile Active substance: Triptorelin Pharmaceutical form(s)/strength: 0,1 mg P-RMS: DE/H/PSUR/0038/002 Date of FAR: 26.05.2014 4.3 Contraindications Hypersensitivity to GnRH, its analogues
M0BCore Safety Profile Active substance: Triptorelin Pharmaceutical form(s)/strength: 0,1 mg P-RMS: DE/H/PSUR/0038/002 Date of FAR: 26.05.2014 4.3 Contraindications Hypersensitivity to GnRH, its analogues
Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels?
 ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
Marketing Authorisation Holder Applicant Invented name. Route of administration. Content (concentration) Member State. l form
 Member State. l form") ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
Metasta&c prostate cancer. Walid Obeid PGY IV SGHUMC
 Metasta&c prostate cancer Walid Obeid PGY IV SGHUMC Defini&on Stage IV prostate cancer : is defined by the American Joint CommiEee on Cancer's TNM classifica&on system: T4, N0, M0, any prostate- specific
Metasta&c prostate cancer Walid Obeid PGY IV SGHUMC Defini&on Stage IV prostate cancer : is defined by the American Joint CommiEee on Cancer's TNM classifica&on system: T4, N0, M0, any prostate- specific
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Final Appraisal Report. Ferring Pharmaceuticals Ltd. Advice No: 2109 December Recommendation of AWMSG
 Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer
 agonists in prostate cancer") B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer
 induction and maintenance for advanced hormone-dependent prostate cancer") LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent prostate cancer Degarelix (Firmagon) induction and maintenance for advanced hormone-dependent
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol
 Analogs Drug Class Prior Authorization Protocol") Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been
Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been
Manipulating Hormones: Androgen Suppression in Prostate Cancer Patients
 Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
FIRMAGON/DEGARELIX. Compiled by Charles (Chuck) Maack Prostate Cancer Activist/Mentor
 Maack Prostate Cancer Activist/Mentor") FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Androgen deprivation therapy: New concepts. Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto
 Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Drug Class Monograph
 Drug Class Monograph Class: Gonadotropin Releasing Hormone (GnRH) Analogs Drugs: Eligard (leuprolide acetate), Firmagon (degarelix), Lupaneta Pack (leuprolide acetate and norethindrone), Lupron Depot (leuprolide
Drug Class Monograph Class: Gonadotropin Releasing Hormone (GnRH) Analogs Drugs: Eligard (leuprolide acetate), Firmagon (degarelix), Lupaneta Pack (leuprolide acetate and norethindrone), Lupron Depot (leuprolide
Androgen Deprivation Therapy (ADT) Following Recurring Prostate Cancer Or When Androgen Deprivation Becomes The Necessary Therapy
 Following Recurring Prostate Cancer Or When Androgen Deprivation Becomes The Necessary Therapy") Androgen Deprivation Therapy (ADT) Following Recurring Prostate Cancer Or When Androgen Deprivation Becomes The Necessary Therapy By Prostate Cancer Patient and Activist/Mentor Charles (Chuck) Maack with
Androgen Deprivation Therapy (ADT) Following Recurring Prostate Cancer Or When Androgen Deprivation Becomes The Necessary Therapy By Prostate Cancer Patient and Activist/Mentor Charles (Chuck) Maack with
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer
 Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer www.nshealth.ca Hormone Therapy for Prostate Cancer What is the prostate? The prostate is one of the male sex glands. It makes seminal fluid
Patient & Family Guide 2015 Hormone Therapy for Prostate Cancer www.nshealth.ca Hormone Therapy for Prostate Cancer What is the prostate? The prostate is one of the male sex glands. It makes seminal fluid
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Radiation Therapy. External Beam Radiation Therapy
 Radiation Therapy Radiation therapy is a non-invasive treatment for prostate cancer that uses x-rays or gamma-rays to eradicate prostate cancer cells. There are several forms of radiation therapy that
Radiation Therapy Radiation therapy is a non-invasive treatment for prostate cancer that uses x-rays or gamma-rays to eradicate prostate cancer cells. There are several forms of radiation therapy that
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS
 UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
Community care of Prostate Cancer. Shaun Costello Southern Cancer Network
 Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Hormone therapy for prostate cancer
 The Clatterbridge Cancer Centre NHS Foundation Trust Hormone therapy for prostate cancer General information A guide for patients and carers Contents What is hormone therapy?... 1 How does hormone therapy
The Clatterbridge Cancer Centre NHS Foundation Trust Hormone therapy for prostate cancer General information A guide for patients and carers Contents What is hormone therapy?... 1 How does hormone therapy
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
Prostate Cancer Case Study 2. Medical Student Case-Based Learning
 Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Challenges in the management of metastatic prostate cancer
 Oncology 323 Challenges in the management of metastatic prostate cancer A significant number of men with prostate cancer will be elderly. Although some of the issues they face will be the same as their
Oncology 323 Challenges in the management of metastatic prostate cancer A significant number of men with prostate cancer will be elderly. Although some of the issues they face will be the same as their
Cost-effectiveness of androgen suppression therapies in advanced prostate cancer Bayoumi A M, Brown A D, Garber A M
 Cost-effectiveness of androgen suppression therapies in advanced prostate cancer Bayoumi A M, Brown A D, Garber A M Record Status This is a critical abstract of an economic evaluation that meets the criteria
Cost-effectiveness of androgen suppression therapies in advanced prostate cancer Bayoumi A M, Brown A D, Garber A M Record Status This is a critical abstract of an economic evaluation that meets the criteria
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Suthan Chanthawong. B. Pharm, BCP, BCOP. Faculty of Pharmaceutical Sciences, Khon Kaen University
 Suthan Chanthawong B. Pharm, BCP, BCOP Faculty of Pharmaceutical Sciences, Khon Kaen University Objectives 1) Outline appropriate screening and prevention strategy. 2) Describe appropriate patient-specific
Suthan Chanthawong B. Pharm, BCP, BCOP Faculty of Pharmaceutical Sciences, Khon Kaen University Objectives 1) Outline appropriate screening and prevention strategy. 2) Describe appropriate patient-specific
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE
 mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
J Clin Oncol 25: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 25 NUMBER 12 APRIL 20 2007 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Initial Hormonal Management of Androgen-Sensitive Metastatic, Recurrent, or Progressive Prostate Cancer:
VOLUME 25 NUMBER 12 APRIL 20 2007 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Initial Hormonal Management of Androgen-Sensitive Metastatic, Recurrent, or Progressive Prostate Cancer:
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
פ א ר מ ה P H A R x M A
 פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh)
") Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh) Specialist: Please complete the Shared Care letter sending a request to GP (see bottom of the page) April 2013 GP: Please indicate
Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh) Specialist: Please complete the Shared Care letter sending a request to GP (see bottom of the page) April 2013 GP: Please indicate
A Layperson's Guide to Endocrine (Hormone) Therapy
 Therapy") A Layperson's Guide to Endocrine (Hormone) Therapy What we will cover What is the endocrine system Basic definition of endocrine therapy Classes of endocrine drugs How you can utilise endocrine therapy
A Layperson's Guide to Endocrine (Hormone) Therapy What we will cover What is the endocrine system Basic definition of endocrine therapy Classes of endocrine drugs How you can utilise endocrine therapy
Androgen Deprivation Therapy A Question of Timing
 Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Review of Polish and international guidelines on hormonal therapy in localized prostate cancer
 Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
 QoL compared with ADT plus placebo. perc considered this to be reasonable in the nmcrpc setting, where patients QoL is expected to be relatively high and stable. perc discussed that there is a net clinical
QoL compared with ADT plus placebo. perc considered this to be reasonable in the nmcrpc setting, where patients QoL is expected to be relatively high and stable. perc discussed that there is a net clinical
Mr PHIP No. 5 Hormone treatment for prostate cancer
 Mr PHIP No. 5 Hormone treatment for prostate cancer Mr Phip Hormone treatment controls cancer growth by reducing the effects of male hormones. Mr Phip No. 5 / Key points cancer cells require male hormone
Mr PHIP No. 5 Hormone treatment for prostate cancer Mr Phip Hormone treatment controls cancer growth by reducing the effects of male hormones. Mr Phip No. 5 / Key points cancer cells require male hormone
Prostate cancer is now the most
 : a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
: a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment
 Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
LUNCH AND LEARN. April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology
 LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers