Diagnosis and Management of Chronic Myeloid Leukaemia
|
|
|
- Miranda Miller
- 6 years ago
- Views:
Transcription
1 Diagnosis and Management of Chronic Myeloid Leukaemia Dr Simon Watt Dr Katherine O Neill Dr Fiona Dignan Written July 2017 Prof Tim Somervaille Review July
2 Table of Contents 1.0 Introduction Investigation and diagnosis Assessment of disease status Prognostic Scoring Systems Management of chronic phase CML Management of advanced phase disease Monitoring of patients on TKIs Treatment failure or intolerance on 1 st line TKIs Discontinuing TKIs Pregnancy References Appendix 1 Prognostic Scoring Systems.. 14 Appendix 2 Data on comparative trials of imatinib versus second generation TKIs..15 Appendix 3 Further data on TKI discontinuation trials Appendix 4 Request form for BCR ABL mutation analysis (Birmingham)
3 1.0 Introduction CML occurs with an incidence of approximately in /year. More recent studies estimate survival rates for CML at approximately 90% at 5 years. Mortality rates have decreased by ~70% in the UK since the early 1970s. This is largely due to the introduction of tyrosine kinase inhibitors (TKIs) which have revolutionised therapy for CML. However TKIs present challenges in terms of monitoring, toxicity and discussions regarding withdrawing treatment. 2.0 Investigation and Diagnosis All new patients presenting with CML should have the following examinations and investigations:- Examination Full clinical examination including documentation of spleen and liver size below the costal margin Check for retinal haemorrhages Check for priapism (males) & any other signs of vascular stasis Blood Tests Full blood count with manual differential Routine biochemistry including U&E, LFTs, alb, calcium, LDH and urate Peripheral blood for RT-PCR for identification of BCR-ABL transcript. This must be performed even if diagnosis has been confirmed by FISH/G banding as it is used as a baseline for monitoring treatment. Virology including Hepatitis B & C, HIV Bone Marrow Aspirate (+/- trephine) Differential analysis, including blast percentage Chromosome banding analysis/cytogenetics for G banding and FISH for BCR-ABL Consider immunophenotyping where morphology suggests elevated blast percentage Cytogenetic analysis and FISH are performed by the Cytogenetics Laboratory at The Christie NHS Foundation Trust. RT-PCR for BCR-ABL can be performed on 10 ml EDTAanticoagulated blood sent by first class post to Molecular Genetics Lab, Department of Haematology, CMFT ( ). If allogeneic HSCT is being considered: HLA typing of patient and siblings. Consider volunteer unrelated donor (VUD) search. Where possible, register the patient with local/regional CML patient registry- see 3
4 3.0 Assessment of disease status WHO criteria (2008) ELN criteria (2013) Chronic phase Blasts <10% in bone marrow and peripheral blood; Peripheral blood basophils <20%; Absence of other criteria of accelerated phase or blast crisis Accelerated Phase Blasts in blood or marrow 10 19% Basophils in blood 20% Persistent thrombocytopenia (< /L) unrelated to therapy CCA (clonal chromosomal abnormalities)/ph+ (i.e. cytogenetic evolution) on treatment Thrombocytosis (> /L) unresponsive to therapy. Increasing spleen size and increasing WBC count unresponsive to therapy Blast crisis Blasts in blood or marrow 20% Extramedullary blast proliferation, spleen excluded Large foci or clusters of blasts in the bone marrow biopsy Blasts in blood or marrow 15 29%, or blasts plus promyelocytes in blood or marrow >30%, with blasts <30% Basophils in blood 20% Persistent thrombocytopenia (< /L) unrelated to therapy Clonal chromosome abnormalities in Ph+ cells (CCA/Ph+) on treatment Blasts in blood or marrow 30% Extramedullary blast proliferation, spleen excluded (e.g. chloroma) Should blast transformation of CML be considered, it is important to determine by morphology and immunophenotyping of the blood and marrow whether the transformation is myeloid (approx. 70%) or lymphoid (approx. 30%). 4.0 Prognostic Scoring Systems It may be helpful for patients in the chronic phase to have a prognostic score (e.g. HASFORD, SOKAL and EUTOS) calculated at baseline. These are listed in Appendix Management of chronic phase CML (a) Leukapheresis Leukapheresis should be considered as an urgent approach to reduce the white cell count rapidly if there are signs of leukostasis (e.g. deteriorating level of consciousness, papilloedema, retinal venous engorgement/haemorrhages or priapism). If a patient is likely to require leukapheresis, early discussion with a centre offering this facility is advisable (i.e. The Christie or Manchester Royal Infirmary). (b) Hydroxycarbamide If active treatment to bring down the white cell count prior to starting tyrosine kinase inhibition is required while confirmation of diagnosis is awaited, hydroxycarbamide (hydroxyurea) is recommended at a dose of 1g to 6g a day in divided doses depending on clinical need. It is 4
5 usually well tolerated, although gastrointestinal symptoms may occur, particularly with higher doses. Renal and hepatic function should be monitored before and during treatment and the initial dose should be reduced by 50% if egfr is <60 ml/min. In patients with elevated white cell counts, allopurinol 300 mg/day (reduced in renal and hepatic impairment) should be given and an adequate intake of fluids maintained. (c) Definitive treatments All patients should be discussed in the relevant Haematology MDT. If available and deemed suitable, patients should be considered for a clinical trial. Patients not wishing to enrol/ineligible for clinical trials should be offered a tyrosine kinase inhibitor (TKI) as first line therapy. NICE Guidelines (TA426, December 2016) recommend the use of imatinib, dasatinib or nilotinib for untreated, chronic-phase Philadelphia-chromosome-positive chronic myeloid leukaemia in adults. NICE does not currently provide guidance over which should be used as first line, providing the company provides the drug within the discount agreed in the relevant patient access scheme. Generic imatinib is recommended as the first choice TKI due to the significant current cost differential and lack of proven mortality benefit versus any of the second generation TKIs. Guideline prices (access date , BNF) are ~ 2500 p.a. for generic imatinib versus ~ 18,000 p.a. for either nilotinib or dasatinib (with agreed NHS discount). Recommended doses with TKI therapy are: Imatinib: 400mg OD in the chronic phase (may be increased to 600mg/day) Dasatanib: 100mg OD Nilotinib: 300mg BD While the second generation TKIs nilotinib and dasatinib induce deeper and more rapid molecular responses than imatinib, this has not to date been demonstrated to translate into improved clinical outcomes including survival. Furthermore, second generation TKIs are frequently associated with more deleterious ADRs which may represent an important consideration for some patients. For example, dasatinib is associated with pleural effusion in 19% of patients over 5 years compared to 1% of patients treated with imatinib (data from SPIRIT2). Likewise, nilotinib is associated with elevations in blood cholesterol and glucose and an increased frequency of cardiovascular events, including ischaemic heart disease, ischaemic cerebrovascular disease and peripheral vascular disease (by comparison with patients treated with imatinib). In view of the elevated cardiovascular risk associated with nilotinib it is recommended that all patients starting the drug have a Q-risk score calculated and glucose, blood pressure and lipid profile monitored. An ECG as well as tests for amylase and thyroid function tests should be performed at baseline. First line use of second generation TKIs should be limited to clinical situations where a faster and deeper molecular response is deemed essential, for example in high risk patients (e.g. from prognostic scoring) or in those presenting in accelerated phase. Patient co-morbidities and side effect profiles are further important considerations. For example, elderly patients are more likely to develop pleural effusions on dasatinib, and use of nilotinib in patients with established cardiovascular disease should be carefully considered. Further details supporting these recommendations may be found in Appendix 2. 5
6 Specific side effect profiles of the TKIs This is not an exhaustive list. Please see the BNF or for further specific details. Imatinib Dasatinib Nilotinib GI side effects: nausea, Pleural effusion Adverse cardiac events diarrhoea. Dyspnoea including ischaemic heart Fluid retention Thrombocytopenia disease, cerebrovascular Cramps Pulmonary hypertension events and peripheral vascular disease. Hypertension QT interval prolongation Hypercholesterolaemia Hyperglycaemia Thyrotoxicosis 6.0 Management of advanced phase disease Advanced disease comprises accelerated phase (AP) and blast crisis (BC). Some patients may present in AP or BC, however the majority progress to BC following TKI failure. Patients presenting in AP are typically responsive and should be treated with TKIs, preferably with the more potent second generation TKIs according to Baccarani et al. (2015). They should be considered for allogeneic stem cell transplantation (SCT) if they fail to achieve an optimal response. Patients presenting in BC are also responsive to TKIs, although the risk of relapse is high and thus all should be considered for allogeneic SCT (Baccarani et al., 2015). Mutational analysis is recommended in AP and BC either prior to treatment or at any point during treatment when the trajectory of the molecular response appears sub-optimal. In CP it is likewise appropriate when the trajectory of the molecular response is sub-optimal. NICE guidelines (2016) Endorse the use of higher doses of imatinib (600mg OD which may be increased up to 800mg daily, given as 400mg BD) for:- o Patients who present in accelerated phase or blast-crisis o Patients who present in chronic phase and progress to the accelerated phase or blast crisis phase if they have not received imatinib before. High dose imatinib is not recommended for treating Philadelphia-chromosomepositive chronic myeloid leukaemia in adults whose disease is imatinib-resistant. Dasatinib and nilotinib may be used to treat accelerated phase CML in adults if they cannot have imatinib, are imatinib resistant and if companies provide the drugs with the agreed discounts. Doses recommended in accelerated phase or blast crisis (BNF):- Imatinib: 600mg OD increased if necessary to max 800mg daily in two divided doses Dasatinib: 140mg OD increased if necessary to 180mg OD Nilotinib: 400mg BD 6
7 Chemotherapy maybe required before allogeneic SCT to control disease. This would usually be an AML induction regime for patients in myeloid blast crisis and an ALL induction regimen for patients in lymphoid blast crisis. 7.0 Monitoring of patients on TKIs Monitoring of treatment is generally divided into haematological, cytogenetic and molecular response. Definitions are as follows:- Complete Haematological Response: Platelet count <450; WBC <10; no immature myeloid lineage cells in PB; basophils <5%; no palpable spleen The first goal of treatment is to achieve a normal blood count and resolution of splenomegaly. This is the definition of a complete haematological response (CHR) and is achieved in at least 95% of patients with any of the three licensed TKIs (imatinib, dasatinib and nilotinib) within 6 weeks. Complete Cytogenetic Response (CCyR) No Ph+ve metaphases or <1% Bcr:Abl +ve nuclei when 200 nuclei analysed The second goal of treatment is to achieve clearance of the Ph chromosome from the marrow. This should be assessed by G banding through analysis of at least 20 metaphases. FISH should only be used for assessment of CCyR when <1% of nuclei are positive and at least 200 nuclei have been assessed. Cytogenetic response can be classified as:- Ph positive marrow metaphases (%) Designation 0 Complete cytogenetic response (CCyR) 1-35 Partial cytogenetic response (PCyR) Minor cytogenetic response >95 None Complete Molecular Response This is assessed by RQ-PCR of a peripheral blood sample and is expressed according to the International Scale (IS) as the ratio of BCR:ABL1 (leukaemic) transcripts to ABL1 (normal) transcripts. It is reported as BCR-ABL1:ABL1 ratio (%) on a log scale as a reduction below the standard baseline. A BCR-ABL1:ABL1 ratio of <0.1% corresponds to a major molecular response (MMR). The depth of molecular response can then be further classified as below:- BCR:ABL1% Log reduction Depth of response MMR (MR 3.0) MR MR MR5.0 7
8 Patients with no detectable transcripts should be referred to as having molecularly undetectable leukaemia. ELN (European Leukaemia Network) recommendations (2013) Monitoring can be performed using a molecular or cytogenetic test or both depending on laboratory facilities. Wherever possible both are recommended until a MMR and CCyR has been achieved. Then RQ-PCR may be sufficient. Molecular testing:- RQ-PCR should be performed every 3 months until an MMR is attained, then every 3-6 months. Levels may vary over time, partly due to laboratory techniques. However, if transcript levels have increased >5-fold in a single follow up then the test should be repeated at a shorter time interval and patients should be questioned about compliance. Cytogenetics:- Must be performed by CBA (chromosome banding analysis) of marrow cell metaphases, counting at least 20 metaphases at 3, 6 and 12 months until a CCyR is achieved and then every 12 months. CBA can be substituted by FISH of peripheral blood cells only when a CCyR has been achieved. Warning In case of warning, it is recommended to repeat all tests, cytogenetic and molecular more frequently, even monthly. Treatment failure/progression to AP or BC Cytogenetics of marrow cell metaphases, PCR and mutational analyses should be performed. Dysplastic morphology/myelodysplasia If dysplastic morphology or other features of myelodysplasia develop, histopathologic and cytogenetic studies of bone marrow are recommended. In practice, it may be unrealistic and undesirable to the patient to perform bone marrow cytogenetic assessment as frequently as is recommended above and thus flexibility may be exercised. Many physicians may choose to delay BM cytogenetic assessment to 6 months to improve the likelihood of documenting a CCyR. However, all patients must have at least one BM cytogenetics documenting a CCyR. Several groups have shown that the threshold of complete cytogenetic response correlates very well with a BCR-ABL1/ABL1 ratio of 1%; molecular monitoring alone may therefore be adequate for patients who decline a marrow examination for CCR assessment at 12+ months of treatment. Many patients may elect to be monitored with RQ-PCR only, although the gold standard remains annual BM cytogenetics. 8
9 Summary of suggested monitoring Test FBC Bone marrow for cytogenetics/fish RQ-PCR on peripheral blood Frequency 2 weekly until CHR then 3 monthly 3, 6 and 12 months. Once patients have achieved a CCyR a repeat should be considered every 12 months. Consideration could be given to peripheral blood FISH for patients in known CCyR 3 monthly. ELN recommend that this should be done indefinitely, providing this is an informative test at presentation. 8.0 Treatment failure or intolerance on 1 st line TKIs The following table is adapted from the European Leukemia Net (Baccarani et al, 2013) guidelines which updated the previous 2009 guidelines. Failure necessitates a change in treatment because the impaired response means that the patient is at a significant risk of progression and death. Warning is an intermediate category. It is acknowledged by the authors that there is no solid data to make specific recommendations on how the treatment should be changed to improve the response. Definition of the response to TKIs (any TKI) as first line treatment. N.B. Definitions are the same for patients in CP, AP and BC and apply also to second line treatment, when first line treatment was changed due to intolerance. Optimal Warning Failure Baseline N/A High risk or N/A CCA/Ph+, major route 3 months BCR-ABL1:ABL1 ratio BCR:ABL1:ABL1 ratio Non CHR 10% Ph+ 35% >10% Ph % Ph+>95% 6 months BCR:ABL1:ABL1 ratio <1% Ph+ 0 (CCyR) 12 months BCR-ABL1:ABL1 ratio 0.1% (MMR) Then, and at any time BCR:ABL1:ABL1 0.1% CCA: Clonal chromosome abnormalities Major route: High risk score + CCA/Ph+ ratio BCR:ABL1:ABL1 ratio 1-10% Ph+ 1-35% BCR-ABL1:ABL1 ratio 0.1-1% CCA/Ph-(-7, or 7q-) BCR-ABL1:ABL1 >10% Ph+ >35% BCR-ABL1:ABL1 >1% Ph+>0 ratio ratio Loss of CHR Loss of CCyR Confirmed loss of MMR Mutations CCA/Ph+ 9
10 Definition of response to second line therapy in the case of failure of imatinib N.b. Definitions based primarily on data for nilotinib and dasatinib but can also be used provisionally for bosutinib and ponatinib until more data are available. Optimal Warning Failure Baseline N/A No CHR or loss of CHR on imatinib Or lack of CyR to first line TKI Or high risk N/A 3 months BCR:ABL1:ABL1 ratio BCR:ABL1:ABL1 ratio No CHR 10% Ph+<65% >10% Ph % Ph+>95% Or 6 months BCR:ABL1:ABL1 ratio 10% Ph <35% 12 months BCR-ABL1:ABL1 ratio <1% Ph+ 0 (CCyR) Then,and any time at BCR-ABL1:ABL1 0.1% ratio New mutations Ph % BCR-ABL1:ABL1 ratio >10% Ph+ >65% new mutations BCR-ABL1:ABL1 ratio 1-10% And/or Ph+ 1-35% CCA/Ph-(-7, or 7q-) Or BCR:ABL1 >0.1% BCR-ABL1:ABL1 >10% Ph+>35% new mutations Loss of CHR Loss of CCyR or PCyR Confirmed loss of MMR New mutations CCA/Ph+ ratio Treatment Recommendations in the Case of Treatment Failure Based on NICE guidelines 2016 and Review of ELN Recommendations (Baccarani et al., 2015). First line Imatinib Treatment failure (including intolerance) Mutation analysis Second line Dasatinib Nilotinib N.b. High dose imatinib (i.e.600/800mg) is not recommended in imatinib-reistant disease Third line Nilotinib Dasatinib Bosutinib If nilotinib/dasatinib not appropriate. Ponatinib If T315I mutation present Consider SCT There are no direct comparisons of second line therapies in the literature. Choice should be guided by patient characteristics, including comorbidities and sensitivity to the side effect profile of the various TKIs, combined with the results of mutation analysis. 10
11 BCR-ABL1 kinase point mutations are present in approximately 50% of patients with treatment failure and progression. Over 80 amino acid substitutions have been associated with resistance to imatinib. Dasatinib and nilotinib resistance are associated with a smaller spectrum of mutations. The T315I mutation is associated with resistance to all TKIs with the exception of ponatinib. NICE is due to publish guidelines in June 2017 which provisionally authorises use of ponatinib in chronic, accelerated or blast phase CML when the T315I mutation is present. Mutation analysis is performed at West Midlands Regional Genetics Laboratory in Birmingham. Please send sample with the completed form (appendix 4) either directly to Birmingham or via the Molecular Diagnostics Center at CMFT. A list of mutations and information regarding sensitivity to TKIs is presented here: Hochhaus A, Ernst T, Eigendorff E, La Rosee P. Causes of resistance and treatment choices of second and third line treatment in chronic myelogenous leukaemia patients. Ann Haematol: 94: Discontinuing TKIs Most international guidelines recommend that patients who are responding optimally to TKI therapy should continue on treatment indefinitely. Discontinuation of TKI following a prolonged period of molecularly undetectable disease (e.g. 2 yrs) is currently under investigation in clinical trials. Where there are strong reasons to consider discontinuation of TKI the following points arising from studies to date should be considered: 1. Should only be considered in patients with molecularly undetectable leukaemia for > 2 years 2. Most relapses occur within 6 months of stopping TKIs and most patients failing a treatment free period do so with an exponential increase in BCR-ABL, rising approximately 1 log per month. Thus close monitoring, with high quality and timely RQ-PCR, particularly during the first 6 months is essential. 3. For patients remaining in treatment-free response beyond the first 6 months, the risk of relapse is lower, and less frequent testing, e.g., every 2 to 3 months, may be sufficient. 4. The question of how long to continue monitoring is more difficult to answer. The latest reported loss of TFR was at 42 months, and thus long term monitoring is necessary. Further information may be found in Appendix Pregnancy Patients taking TKIs should be advised to use barrier methods of contraception and to avoid pregnancy (males and females). Patients who wish to become pregnant (or father a child) should have careful pre-pregnancy planning and counselling about feasibility and relative risk. Given the specialist management required, patients should be discussed on a case by case basis with regional or national experts with experience in this area. 11
12 11.0 References Abstracts and notes on CML presentations. ASH 2014 San Francisco. Steve O Brien, Newcastle University Baccarani M, Castagnietti F, Gugliotta G, & Rosti G. A review of the European LeukaemiaNet recommendations for the management of CML. Ann Haematol : Baccarani M, Cortes J, Pane F, et al. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol. 2009: 27(35): Baccarani M, Deininger MW, Rosti G, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia. Blood. 2013;122(6): Baccarani M, Pileri S, Steegmann J L, et al. Chronic myeloid leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol.2012; 23 (Suppl 7): vii72-vii77 Hasford J, Baccarani M, Hoffmann V, et al. Predicting complete cytogenetic response and subsequent progression-free survival in 2060 patients with CML on imatinib treatment: the EUTOS score. Blood. 2011;118(3): Hasford J, Pfirrmann M, Hehlmann R, et al. Writing Committee for the Collaborative CML Prognostic Factors Project Group. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. J Natl Cancer Inst. 1998;90(11): Hochhaus A, Saglio G, Hughes TP, et al. Long-term benefits and risks of frontline nilotinib vs imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia ;30(5): Hughes TP, Ross DM. Moving treatment free remission into mainstream clinical practice in CML. Blood. 2016;128(1): Kantarjian H, Shah NP, Hochhaus A, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362(24): Larson RA, Hochhaus A, Hughes TP, et al. Nilotinib vs imatinib in patients with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase: ENESTnd 3-year follow-up. Leukemia. 2012;26(10): Mahon FX, Réa D, Guilhot J. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: the prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010;11(11): NICE Guidelines: Mahon FX, Richter J, Guilhot J, et al.. Interim Analysis of a Pan European Stop Tyrosine Kinase Inhibitor Trial in Chronic Myeloid Leukemia : The EURO-SKI study. Blood. 2014; 124:
13 Saglio G, Kim DW, Issaragrisil S,et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N Engl J Med. 2010;362(24): Sokal JE, Cox EB, Baccarani M, et al. Prognostic discrimination in good-risk chronic granulocytic leukemia. Blood. 1984; 63(4): Sung-Eun L, Soo Young C, Hye-Young S, et al. Imatinib withdrawal syndrome and longer duration of imatinib have a close association with a lower molecular relapse after treatment discontinuation: the KID study. Haematologica. 2016; 101(6): Vardiman JW, Melo JV, Baccarani M, Thiele J. Chronic myelogenous leukemia, BCR-ABL1 positive. In Swerdlowsh. et al (eds), WHO Classification of Tumours of Hematopoietic and Lymphoid Tissues. Lyon: IARC 2008;
14 Appendix 1 - Prognostic Scoring Systems It may be helpful for patients in the chronic phase to have a prognostic score (e.g. HASFORD, SOKAL and EUTOS) calculated at baseline. These are listed in Appendix 1. N.B. Spleen is measured by manual palpation and expressed as maximum distance below costal margin. Sokal score = Exp[ (age 43.4 years) (spleen size 7.51) ([platelets/700] ) (blasts 2.1)] Low risk <0.8 Intermediate risk High risk >1.2 Hasford score = ( age [0 when age <50 years; otherwise 1] + (0.042 spleen size (cm below costal margin)) + ( blasts [%]) +( eosinophils [%]) + ( basophils [0 when basophils <3%;otherwise 1]) + ( platelet count [0 when platelets<1500 per μl; otherwise 1]) 1000 Low risk <780 Intermediate risk High risk >1480 Eutos score= (Spleen (cm beneath costal margin) x4) + (basophils (% of PB leukocytes) x 7) Low risk 87; High risk >87 For online calculators see:- Hasford and Sokal: Eutos: 14
15 Appendix 2 Data on comparative trials of imatinib versus second generation TKIs The SPIRIT 2 trial (unpublished, provisional results from abstracts and notes on CML presentations, ASH 2014) randomised 814 participants with newly diagnosed CML to treatment with either imatinib or dasatinib. Provisional results suggest MR3 (major molecular response) rate at one year was 58.4% with dasatinib compared to 43.1% with imatinib (p<0.001) however there was no difference in disease progression or overall survival. Furthermore dasatinib was associated with pleural effusion in 19.0% of patients over 5 years (16.9% of which required a chest drain) compared to only 0.7% of patients treated with imatinib. Dasatinib was also associated with higher rates of thrombocytopenia and significantly higher rates of dyspnoea in the absence of pleural effusion, compared to imatinib. Similarly Kantarjian et al (2010) (DASISION study) demonstrated superiority of dasatinib versus imatinib for complete cytogenetic response (cccyr) (77% vs. 66%, P = 0.007) and major molecular response(mmr) (46% vs. 28%, P<0.0001)in 519 randomised patients at 12 months. Differences between cccyr and MMR remained at 5 year follow up, however overall five-year progression-free survival (PFS) and overall survival (OS) rates were similar across treatment arms (PFS: 85% -dasatinib, 86%-imatinib); OS: 91%- dasatinib, 90%-imatinib). As above, thrombocytopenia and pleural effusion occurred more commonly with dasatinib, however imatinib was more commonly associated with other adverse side effects including fluid retention, nausea, vomiting and muscle inflammation. The ENESTnd study (Saglio et al., 2010) randomly assigned 846 participants with newly diagnosed CML to nilotinib 300 mg or 400mg BD versus imatinib 400 mg OD. They established a significantly higher rate of CCyR with nilotinib after 1 and 2 years (80% vs 65%, and 87% vs 77%), and a significantly higher rate of MMR with nilotinib after 1 year (50% vs 27%) and 3 years. Molecular response rates continued to be superior at 5 year follow up (Hochhaus et al.,2016) with 54% of patients in the nilitonib 300mg BD arm achieving a MR4.5 versus 31% of patients in the imatinib arm. However, rates of progression free survival and overall survival at 5 years for standard dose nilotinib (300mg BD) versus imatinib were not significantly different (PFS: nilotinib- 92.2% versus imatinib- 91.0%, p = 0.68; OS: nilotinib 93.7% versus imatinib 91.7%, p = 0.48). Nilotinib was associated with elevations in blood cholesterol and glucose and an increased frequency of cardiovascular events, including ischaemic heart disease, ischaemic cerebrovascular disease and peripheral vascular disease. 15
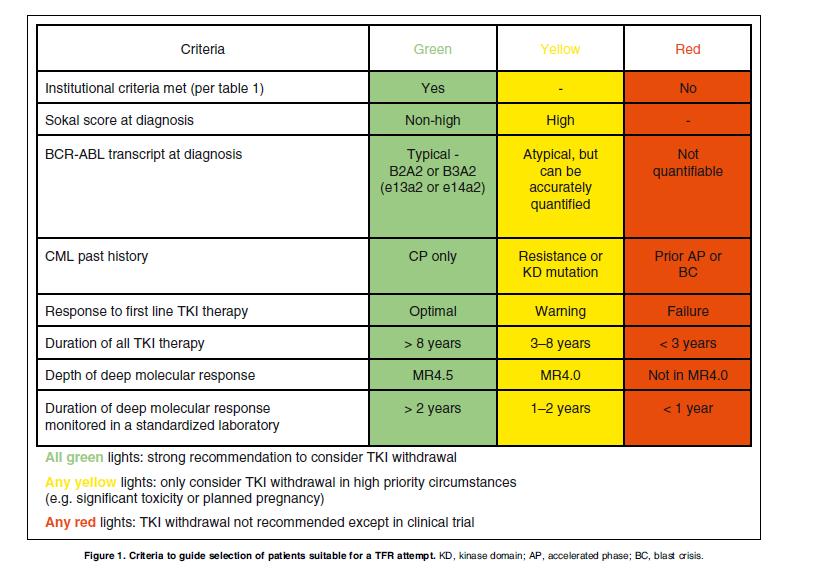
16 Appendix 3 Further data on TKI discontinuation trials The EURO-SKI study (European Stop Tyrosine Kinase Inhibitor Trial in Chronic Myeloid Leukemia) is the largest study of its kind to date, recruiting 821 patients with CML from 11 European Countries. Final results are awaited, however an interim analysis of 200 patients was conducted in 2014 (Mahon et al., 2014). Eligibility criteria included: confirmed deep molecular response (MR4, BCR-ABL <0.01%) for at least one year; and on TKI treatment for at least 3 years. The majority of patients (97%) were taking imatinib. The median duration of TKI therapy was 8 years. Recurrence of CML, defined as loss of MMR, was observed in 47% of patients treated <8 years, compared to 26% of patients treated for >8 years (p= 0.005). Furthermore, initial data suggested that longer durations of MR4 were associated with a significantly reduced risk of remission. 46% of patients in MR4 <5 years lost MMR within 6 months compared to 32% of patients in MR4 >5 years. TKI cessation was well tolerated, although a significant number of participants were noted to experience myalgia in the weeks following cessation. Hughes and Ross (2016) review the evidence for cessation of TKIs in CML and attempt to establish criteria for the safe cessation of TKIs. They summarise the results of key studies to date. The STIM study (Mahon et al., 2010) evaluated 100 patients on imatinib with MR5.0 for at least 2 years. At 12 months 61% of patients had relapsed. However, all patients who relapsed responded well to the re-introduction of imatinib. The trigger to resume TKI was a loss of UMRD (undetectable minimal residual disease, roughly equivalent to MR4.5). Similar results were reported in the TWISTER study (Australasian Leukaemia & Lymphoma group Trial of Withdrawing Imatinib in Stable Remission), where 47.1% of patients achieved treatment free remission (TFR) after 24 months after achieving UMRD on imatinib for at least 2 years. Both studies reported higher treatment free remission rates in Sokal low risk patients. Both studies also reported that most patients regained UMRD within 3 to 6 months of restarting imatinib treatment in response to a rather conservative RQ-PCR defined trigger. Studies with less conservative triggers for resuming TKI have reported even higher treatment free remission rates, for example the KIDS study (Korean Imatinib Discontinuation Study)(Lee et al, 2016) used loss of MMR as a trigger for resuming TKIs and found that 59% of the 90 patients remained in TFR at 2 years. The authors conclude that the safety data from the TFR studies reported to date is sufficiently reassuring to offer all eligible patients a supervised test of TKI withdrawal and have devised criteria to guide when discontinuation of TKI might be appropriate, see table below:- 16
17 17

18 Appendix 4 Request form for BCR-ABL Mutation Analysis (Birmingham) 18
Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012
 Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012 Dr Simon Watt Dr Shiva Natarajan 1.0 Introduction The landscape in chronic myeloid leukaemia (CML) has changed dramatically
Greater Manchester and Cheshire Cancer Network Chronic Myeloid Leukaemia v3 2012 Dr Simon Watt Dr Shiva Natarajan 1.0 Introduction The landscape in chronic myeloid leukaemia (CML) has changed dramatically
The BCR-ABL1 fusion. Epidemiology. At the center of advances in hematology and molecular medicine
 At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
Chronic Myeloid Leukaemia Guidelines
 Chronic Myeloid Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Heather Oakervee, Bart s Health NHST Date of issue: 12.03.2015 Version number:v1.0 These
Chronic Myeloid Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Heather Oakervee, Bart s Health NHST Date of issue: 12.03.2015 Version number:v1.0 These
A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable.
 1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
1 Case 1 A 34-year old women came because of abdominal discomfort. Vital sign was stable. Spleen tip was palpable. CBC and bone marrow aspiration and biopsy were done. Chromosome study showed she had t(9;22)
CML and Future Perspective. Hani Al-Hashmi, MD
 CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
CML and Future Perspective Hani Al-Hashmi, MD Objectives Learning from CML history Outcome of interest to clinician Patient and community interest!! Learning from CML history Survival Probability (All
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway. Chronic Myeloid Leukaemia
 Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute
 Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
Stopping TKI s in CML- Are we There Yet? Joseph O. Moore, MD Duke Cancer Institute Natural History of CML Accumulation of immature myeloid cells New cytogenetic changes Chronic Phase Accelerated Phase
ELN Recommendations on treatment choice and response. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
ELN Recommendations on treatment choice and response Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy ELN 2013 Response to Front-line Treatment Baseline 3 months 6 months OPTIMAL
Chronic Myeloid Leukaemia
 Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
Chronic Myeloid Leukaemia Molecular Response: What is really important? Jeff Szer The Royal Melbourne Hospital PROBABILITY, % PROBABILITY OF SURVIVAL AFTER MYELOABLATIVE TRANSPLANTS FOR CML IN CHRONIC
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML. GIUSEPPE SAGLIO, MD University of Torino, Italy
 Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
Role of Second Generation Tyrosine Kinase Inhibitors in Newly Diagnosed CML GIUSEPPE SAGLIO, MD University of Torino, Italy Outcome in 282 Patients Treated with Imatinib First Line in Hammersmith Hospital
The concept of TFR (Treatment Free Remission) in CML
 in CML") The concept of TFR (Treatment Free Remission) in CML Giuseppe Saglio University of Turin, Italy What can we expect today on long-term therapy with TKIs in CML? German CML study IV Relative and overall
The concept of TFR (Treatment Free Remission) in CML Giuseppe Saglio University of Turin, Italy What can we expect today on long-term therapy with TKIs in CML? German CML study IV Relative and overall
Guidelines and real World: Management of CML in chronic and advanced phases. Carolina Pavlovsky. FUNDALEU May 2017 Frankfurt
 Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
Guidelines and real World: Management of CML in chronic and advanced phases Carolina Pavlovsky. FUNDALEU 26-28 May 217 Frankfurt Some Issues in CML 217 First Line treatment: Imatinib vs 2nd generation
HOW I TREAT CML. 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek,
 HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
HOW I TREAT CML 4. KONGRES HEMATOLOGOV IN TRANSFUZIOLOGOV SLOVENIJE Z MEDNARODNO UDELEŽBO Terme Olimia, Podčetrtek, 12. - 14. april, 2012 Gianantonio Rosti Dpt of Hematology and Oncological Sciences S.
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD
 10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
10 YEARS EXPERIENCE OF TYROSINE KINASE INHIBITOR THERAPY FOR CML IN OXFORD Dalia Khan 1, Noemi Roy 1, Vasha Bari 1, Grant Vallance 1, Helene Dreau 1, Timothy Littlewood 1, Andrew Peniket 1, Paresh Vyas
Oxford Style Debate on STOPPING Treatment.
 Oxford Style Debate on STOPPING Treatment. This house believes that there are good reasons NOT to stop CML treatment. It should be done within clinical trials, OR only in expert centers where frequent,
Oxford Style Debate on STOPPING Treatment. This house believes that there are good reasons NOT to stop CML treatment. It should be done within clinical trials, OR only in expert centers where frequent,
Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN!
 Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN! Dragana Milojković The Hammersmith Hospital, London, UK Leukemic burden Current Aim of TKI therapy Molecular
Stopping Treatment in CML and dose reduction in clinical practice: Can we do it safely? YES WE CAN! Dragana Milojković The Hammersmith Hospital, London, UK Leukemic burden Current Aim of TKI therapy Molecular
Guideline for the Management of Patients with Chronic Myeloid Leukaemia (CML)
") Guideline for the Management of Patients with Chronic Myeloid Leukaemia (CML) Version History Version Summary of change Date Issued 3.0 Approved by Doug Wulff on behalf of the Governance 14.11.08 Committee
Guideline for the Management of Patients with Chronic Myeloid Leukaemia (CML) Version History Version Summary of change Date Issued 3.0 Approved by Doug Wulff on behalf of the Governance 14.11.08 Committee
CML TREATMENT GUIDELINES
 CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
CML TREATMENT GUIDELINES INITIAL INVESTIGATION Propose enrolment in the CML Registry of the CML-MPN Quebec Research Group. Medical history : Question for cardio-respiratory disorders, diabetes, pancreatitis,
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body
 Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
Chronic Myeloid Leukemia A Disease of Young at Heart but Not of Body Jeffrey H Lipton, PhD MD FRCPC Staff Physician, Princess Margaret Cancer Centre Professor of Medicine University of Toronto POGO November,
2 nd Generation TKI Frontline Therapy in CML
 2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
2 nd Generation TKI Frontline Therapy in CML Elias Jabbour, M.D. April 212 New York Frontline Therapy of CML in 212 - imatinib 4 mg daily - nilotinib 3 mg BID - dasatinib 1 mg daily Second / third line
CML: Living with a Chronic Disease
 CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
CML: Living with a Chronic Disease Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia M. D. Anderson Cancer Center Houston, Texas Survival in Early Chronic Phase CML TKI Interferon Chemotherapy
Blast Phase Chronic Myelogenous Leukemia
 Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
Blast Phase Chronic Myelogenous Leukemia Benjamin Powers, MD; and Suman Kambhampati, MD The dramatic improvement in survival with tyrosine kinase inhibitors has not been demonstrated in the advanced blast
EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA
 EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA SAN DIEGO, 11 DECEMBER 2011 AMSTERDAM, 14 JUNE 2012 BALTIMORE, 20 SEPTEMBER 2012 ATLANTA, 6 DECEMBER 2012 ELN, CML Panel Jane Apperley
EUROPEAN LEUKEMIANET RECOMMENDATIONS FOR CHRONIC MYELOID LEUKEMIA SAN DIEGO, 11 DECEMBER 2011 AMSTERDAM, 14 JUNE 2012 BALTIMORE, 20 SEPTEMBER 2012 ATLANTA, 6 DECEMBER 2012 ELN, CML Panel Jane Apperley
How I treat high risck CML
 Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria:
Torino, September 14, 2018 How I treat high risck CML Patrizia Pregno Hematology Dept. Citta della Salute e della Scienza Torino Disclosures Advisory Board: Novartis, Pfizer, Incyte Speaker Honoraria:
t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case
(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case") CHRONIC MYELOID LEUKAEMIA Diagnostic Criteria Chronic phase CML t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case Maximally cellular marrow
CHRONIC MYELOID LEUKAEMIA Diagnostic Criteria Chronic phase CML t(9;22)(q34;q11) as part of a single or complex translocation, or BCR-ABL transcripts must be present in every case Maximally cellular marrow
2nd generation TKIs to first line therapy
 New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
New Horizons 2011 Newly diagnosed CML moving 2nd generation TKIs to first line therapy Gianantonio Rosti Dept. Of Hematology and Oncology St. Orsola-Malpighi University Hospital Bologna (Italy) GIMEMA
RESEARCH ARTICLE. Introduction. Methods Wiley Periodicals, Inc.
 BCR/ABL level at 6 months identifies good risk CML subgroup after failing early molecular response at 3 months following imatinib therapy for CML in chronic phase AJH Dennis (Dong Hwan) Kim, 1 * Nada Hamad,
BCR/ABL level at 6 months identifies good risk CML subgroup after failing early molecular response at 3 months following imatinib therapy for CML in chronic phase AJH Dennis (Dong Hwan) Kim, 1 * Nada Hamad,
TREATMENT INTENT Disease modification- see European LeukemiaNet (ELN) 2013 guidelines for treatment goals.
 2013 guidelines for treatment goals.") BOSUTINIB INDICATION Licensed / NICE TA401 (BLUETEQ required) The treatment of adult patients with chronic, accelerated and blast phase Philadelphia chromosome positive chronic myeloid leukaemia (Ph+ CML)
BOSUTINIB INDICATION Licensed / NICE TA401 (BLUETEQ required) The treatment of adult patients with chronic, accelerated and blast phase Philadelphia chromosome positive chronic myeloid leukaemia (Ph+ CML)
Welcome and Introductions
 Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
Living with Chronic Myeloid Leukemia Welcome and Introductions Living with Chronic Myeloid Leukemia Living with Chronic Myeloid Leukemia (CML) Neil P. Shah, MD, PhD Edward S. Ageno Distinguished Professor
NCCP Chemotherapy Protocol. Bosutinib Monotherapy
 Bosutinib Monotherapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase (CP), accelerated phase (AP), and blast phase (BP) Philadelphia chromosome positive chronic myelogenous
Bosutinib Monotherapy INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase (CP), accelerated phase (AP), and blast phase (BP) Philadelphia chromosome positive chronic myelogenous
Milestones and Monitoring
 Curr Hematol Malig Rep (2015) 10:167 172 DOI 10.1007/s11899-015-0258-1 CHRONIC MYELOID LEUKEMIAS (E JABBOUR, SECTION EDITOR) Milestones and Monitoring Alessandro Morotti 1 & Carmen Fava 1 & Giuseppe Saglio
Curr Hematol Malig Rep (2015) 10:167 172 DOI 10.1007/s11899-015-0258-1 CHRONIC MYELOID LEUKEMIAS (E JABBOUR, SECTION EDITOR) Milestones and Monitoring Alessandro Morotti 1 & Carmen Fava 1 & Giuseppe Saglio
CML David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML Current treatment options for CML
 1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
1 CML 2012 LLS Jan 26, 2012 David L Porter, MD University of Pennsylvania Medical Center Abramson Cancer Center CML 2012 Current treatment options for CML patients Emerging therapies for CML treatment
Chronic myeloid leukemia (CML) Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University
 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University") Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
Chronic myeloid leukemia (CML) 1 Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University Hematologic malignancies CML ALL AML 2 CML CD34+ results from an acquired mutation that affects hematopoietic
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019
 Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
Starting & stopping therapy in Chronic Myeloid Leukemia: What more is needed? Richard A. Larson, MD University of Chicago March 2019 Disclosures Richard A. Larson, MD Research funding to the University
CML Clinical Case Scenario
 CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
CML Clinical Case Scenario Neil Shah, MD, PhD Edward S. Ageno Distinguished Professor in Hematology/Oncology Leader, Hematopoietic Malignancies Program Helen Diller Family Comprehensive Cancer Center at
Juan Luis Steegmann Hospital de la Princesa. Madrid. JL Steegmann
 Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
Juan Luis Steegmann Hospital de la Princesa. Madrid. Juan Luis Steegmann Hospital de la Princesa. Madrid No rush,at least in Chronic Phase Blast Phase*: SCT asap, after restablishing CP with TKI Accelerated
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane
 La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
La terapia della LMC: è possibile guarire senza trapianto? Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival And QoL comparable
Treatment free remission in CML: from the concept to practice. François-Xavier Mahon. Cancer Center Bordeaux Université Bordeaux, France
 Treatment free remission in CML: from the concept to practice François-Xavier Mahon Cancer Center Bordeaux Université Bordeaux, France CML is a model 1960 1970 1980 1990 2000 2010 Philadelphia chromosome
Treatment free remission in CML: from the concept to practice François-Xavier Mahon Cancer Center Bordeaux Université Bordeaux, France CML is a model 1960 1970 1980 1990 2000 2010 Philadelphia chromosome
Research Article The Hasford Score May Predict Molecular Response in Chronic Myeloid Leukemia Patients: A Single Institution Experience
 Disease Markers Volume 216, Article ID 7531472, 5 pages http://dx.doi.org/1.1155/216/7531472 Research Article The Hasford Score May Predict Molecular Response in Chronic Myeloid Leukemia Patients: A Single
Disease Markers Volume 216, Article ID 7531472, 5 pages http://dx.doi.org/1.1155/216/7531472 Research Article The Hasford Score May Predict Molecular Response in Chronic Myeloid Leukemia Patients: A Single
Contemporary and Future Approaches in CML. Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D.
 Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
Contemporary and Future Approaches in CML Emory Meeting; Sea Island August 2014 Hagop Kantarjian, M.D. 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR
 What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
What is the optimal management strategy for younger CP-CML patients with matched, related donors who fail to achieve CCyR after 18 months of imatinib? Second generation TKIs as a bridge to allogeneic SCT
Does Generic Imatinib Change the Treatment Approach in CML?
 Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
Does Generic Imatinib Change the Treatment Approach in CML? Jerald P. Radich, MD Fred Hutchinson Cancer Research Center/ Seattle Cancer Care Alliance NCCN.org For Clinicians NCCN.org/patients For Patients
The speaker has no financial relationships with a commercial interest to disclose and no conflicts of interest to resolve.
 Hana Safah MD Professor of Medicine Tulane University School of Medicine Director of the SCT program, Tulane Medical Center The speaker has no financial relationships with a commercial interest to disclose
Hana Safah MD Professor of Medicine Tulane University School of Medicine Director of the SCT program, Tulane Medical Center The speaker has no financial relationships with a commercial interest to disclose
Allogeneic SCT for. 1st TKI. Vienna Austria. Dr. Eduardo Olavarría Complejo Hospitalario de Navarra
 The International Congress on Controversies in Stem Cell Transplantation and Cellular Therapies (COSTEM) Berlin, Germany September 8-11, 2011 Vienna Austria Allogeneic SCT for CML Allogeneic after failure
The International Congress on Controversies in Stem Cell Transplantation and Cellular Therapies (COSTEM) Berlin, Germany September 8-11, 2011 Vienna Austria Allogeneic SCT for CML Allogeneic after failure
C Longer follow up on IRIS data
 hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
hronic Myeloid Leukemia Drs. Rena Buckstein, Mervat Mahrous & Eugenia Piliotis with input from Dr. J. Lipton (PMH) Updated August 2008* Updates: C Longer follow up on IRIS data Guidelines for monitoring
MRD in CML (BCR-ABL1)
") MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
MRD in CML (BCR-ABL1) Moleculaire Biologie en Cytometrie cursus Barbara Denys LAbo Hematologie UZ Gent 6 mei 2011 2008 Universitair Ziekenhuis Gent 1 Myeloproliferative Neoplasms o WHO classification 2008:
NEW DRUGS IN HEMATOLOGY
 NEW DRUGS IN HEMATOLOGY BOLOGNA, 15-17 April 2013 TYROSINE KINASE INHIBITORS IN CHRONIC MYELOID LEUKEMIA MICHELE BACCARANI michele.baccarani@unibo.it Historic Development of CML Therapy Palliative Therapy
NEW DRUGS IN HEMATOLOGY BOLOGNA, 15-17 April 2013 TYROSINE KINASE INHIBITORS IN CHRONIC MYELOID LEUKEMIA MICHELE BACCARANI michele.baccarani@unibo.it Historic Development of CML Therapy Palliative Therapy
Chronic myeloid leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
 clinical practice guidelines Annals of Oncology 23 (Supplement 7): vii72 vii77, 2012 doi:10.1093/annonc/mds228 Chronic myeloid leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
clinical practice guidelines Annals of Oncology 23 (Supplement 7): vii72 vii77, 2012 doi:10.1093/annonc/mds228 Chronic myeloid leukemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
CML: definition. CML epidemiology. CML diagnosis. CML: peripheralbloodsmear. Cytogenetic abnormality of CML
 MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
MolecularDiagnostic.be Third Scientific Meeting Molecular Diagnostics.be t(9;22) CML: definition Management of CML patients treated with TKI: the place of molecular monitoring Antwerp, December 13 th 11
Low doses of tyrosine kinase inhibitors in CML
 CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
CML Horizons Conference Warsaw 4-6 May 2018 Low doses of tyrosine kinase inhibitors in CML Delphine Rea, MD, PhD Pôle Hématologie Oncologie Radiothérapie INSERM UMR-1160 Centre Hospitalo-Universitaire
Is there a best TKI for chronic phase CML?
 MANAGING TYPICAL AND ATYPICAL CHRONIC MYELOID LEUKEMIA Is there a best TKI for chronic phase CML? Richard A. Larson 1 1 Section of Hematology/Oncology, Department of Medicine, and Comprehensive Cancer
MANAGING TYPICAL AND ATYPICAL CHRONIC MYELOID LEUKEMIA Is there a best TKI for chronic phase CML? Richard A. Larson 1 1 Section of Hematology/Oncology, Department of Medicine, and Comprehensive Cancer
NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT.
 NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT Michele.baccarani@unibo.it Michele BACCARANI, MD Professor of Hematology at the Universities of Trieste,
NEW DRUGS IN HEMATOLOGY Bologna, 9-11 May 2016 CHRONIC MYELOID LEUKEMIA STATUS OF THE ART OF TREATMENT Michele.baccarani@unibo.it Michele BACCARANI, MD Professor of Hematology at the Universities of Trieste,
DAVID S. SNYDER, M.D.
 CML UPDATE 2019 DAVID S. SNYDER, M.D. MARCH 21,2019 Click to edit Master Presentation Date Disclosures I do not have anything to disclose 2001 2016 Loss in expectation of life of patients with chronic
CML UPDATE 2019 DAVID S. SNYDER, M.D. MARCH 21,2019 Click to edit Master Presentation Date Disclosures I do not have anything to disclose 2001 2016 Loss in expectation of life of patients with chronic
Venice Meeting Highlights: Key lessons. Conclusions Michele Baccarani Rüdiger Hehlmann
 Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
Venice Meeting Highlights: Key lessons Conclusions Michele Baccarani Rüdiger Hehlmann CML therapy in the imatinib era CML prognosis has improved dramatically Cellular and molecular biology studies help
Imatinib & Ponatinib. Two ends of the spectrum in 2016s reality
 Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
Imatinib & Ponatinib Two ends of the spectrum in 2016s reality CML 2016 Benefits & risks Steve O Brien CML Horizons, May 2016 Disclosures Research funding, participation in company trial, speaker, consultant,
Accepted Manuscript. Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors. Pradnya Chopade, Luke P.
 Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
Accepted Manuscript Improving Outcomes in Chronic Myeloid Leukemia Over Time in the Era of Tyrosine Kinase Inhibitors Pradnya Chopade, Luke P. Akard PII: S2152-2650(18)30343-4 DOI: 10.1016/j.clml.2018.06.029
Cancer Biology 2016;6(1) Imatinib Mesylate Effectiveness in Chronic Myeloid Leukemia patients in Upper Egypt. Mervat M.
 Imatinib Mesylate Effectiveness in Chronic Myeloid Leukemia patients in Upper Egypt. Mervat M.") Imatinib Mesylate Effectiveness in Chronic Myeloid Leukemia patients in Upper Egypt Mervat M. Omar Department of Oncology, Assuit University Hospital, Assuit, Egypt drmervatomar@yahoo.com Abstract: Background
Imatinib Mesylate Effectiveness in Chronic Myeloid Leukemia patients in Upper Egypt Mervat M. Omar Department of Oncology, Assuit University Hospital, Assuit, Egypt drmervatomar@yahoo.com Abstract: Background
NCCP Chemotherapy Protocol. Ponatinib Therapy
 INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant
INDICATIONS FOR USE: INDICATION Treatment of adult patients with chronic phase, accelerated phase, or blast phase chronic myeloid leukaemia (CML) who are resistant to dasatinib or nilotinib; who are intolerant
History of CML Treatment
 History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
History of CML Treatment Eduardo Olavarria No conflict of interest Lisbon, 20th March 2018 #EBMT18 www.ebmt.or What is CML? The mystery of chronic myeloid leukaemia Chronic myeloid leukaemia Often diagnosed
Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus
 Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus Frankfurt I 27.5.2017 Aims of CML Therapy Leukemia cells >10 12 CHR 10
Stopping treatment how much we understand about mechanisms to stop successfully today, and where are the limits? Andreas Hochhaus Frankfurt I 27.5.2017 Aims of CML Therapy Leukemia cells >10 12 CHR 10
1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with
 1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with both Nilotinib and Dasatinib. Nilotinib for the cardio
1 Educational session salient points. Tim Hughes, Vivian Oehler and Rick Van Etten. Tim - Imatinib is a less toxic drug than what we are seeing with both Nilotinib and Dasatinib. Nilotinib for the cardio
Executive summary Overview
 Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
Executive summary Overview In this appraisal, we have demonstrated that dasatinib is clinically more effective, as well as more cost effective, than imatinib, the current standard of care. In the pivotal
Taiwan Guidelines for the Management of Chronic Myeloid Leukemia
 Taiwan Guidelines for the Management of Chronic Myeloid Leukemia Taiwan CML Study Group Coordinator: Lee-Yung Shih 2013/11/30 1 Contents Initial work-up at diagnosis and define baseline prognostic factors
Taiwan Guidelines for the Management of Chronic Myeloid Leukemia Taiwan CML Study Group Coordinator: Lee-Yung Shih 2013/11/30 1 Contents Initial work-up at diagnosis and define baseline prognostic factors
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms
 Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
Clinical Guidelines for Leukaemia and other Myeloid Disorders Myeloproliferative Neoplasms Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1
Form 2012 R3.0: Chronic Myelogenous Leukemia (CML) Pre-Infusion Data
 Pre-Infusion Data") Form 2012 R3.0: Chronic Myelogeus Leukemia (CML) Pre-Infusion Data Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Research ID: Event date: - - HCT type: (check all that apply)
Form 2012 R3.0: Chronic Myelogeus Leukemia (CML) Pre-Infusion Data Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Research ID: Event date: - - HCT type: (check all that apply)
What is New in CML in Hagop Kantarjian, M.D. February 2011
 What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
What is New in CML in 2011 Hagop Kantarjian, M.D. February 2011 1 CML. Historical vs. Modern Perspective Parameter Historical Modern Course Fatal Indolent Prognosis Poor Excellent 10-yr survival 10% 84-90%
Contemporary and Future Approaches in Management of CML. Disclosures
 Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
Winship Cancer Institute of Emory University Contemporary and Future Approaches in Management of CML Hagop Kantarjian, MD Chairman and Professor, Department of Leukemia University of Texas M. D. Anderson
SESSION III: Chronic myeloid leukemia PONATINIB. Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy
 SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
SESSION III: Chronic myeloid leukemia PONATINIB Gianantonio Rosti, MD, Department of Hematology, University of Bologna, Italy Ponatinib A Pan-BCR-ABL Inhibitor Rationally designed inhibitor of BCR- ABL
An update on imatinib mesylate therapy in chronic myeloid leukaemia patients in a teaching hospital in Malaysia
 Singapore Med J 2012; 53(1) : 57 An update on imatinib mesylate therapy in chronic myeloid leukaemia patients in a teaching hospital in Malaysia Bee PC 1, MD, MMed, Gan GG 1, MBBS, FRCP, Tai YT 1, MBBS,
Singapore Med J 2012; 53(1) : 57 An update on imatinib mesylate therapy in chronic myeloid leukaemia patients in a teaching hospital in Malaysia Bee PC 1, MD, MMed, Gan GG 1, MBBS, FRCP, Tai YT 1, MBBS,
I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica. Fabrizio Pane
 I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival
I nuovi guariti? La malattia minima residua nella leucemia mieloide cronica Fabrizio Pane What could be the concept of Cure in CML? Sustained DMR with or without TKI therapy And 100% CML-related survival
Abstract. Research. Keywords: CML, Sokal score, Euro score, EUTOS score. Published: 06/10/2016 Received: 29/05/2016
 Prognostic and predictive implications of Sokal, Euro and eutos scores in chronic myeloid leukaemia in the imatinib era experience from a tertiary oncology centre in Southern India Lakshmaiah Chinnagiriyappa
Prognostic and predictive implications of Sokal, Euro and eutos scores in chronic myeloid leukaemia in the imatinib era experience from a tertiary oncology centre in Southern India Lakshmaiah Chinnagiriyappa
Pan-London Haemato-Oncology Clinical Guidelines. Acute Leukaemias and Myeloid Neoplasms Part 3: Chronic Myeloid Leukaemia
 Pan-London Haemato-Oncology Clinical Guidelines Acute Leukaemias and Myeloid Neoplasms Part 3: Chronic Myeloid Leukaemia September 2018 CONTENTS Contents 1 Introduction... 3 2 Referral Pathways from Primary
Pan-London Haemato-Oncology Clinical Guidelines Acute Leukaemias and Myeloid Neoplasms Part 3: Chronic Myeloid Leukaemia September 2018 CONTENTS Contents 1 Introduction... 3 2 Referral Pathways from Primary
Management of CML in blast crisis. Lymphoma Tumor Board November 27, 2015
 Management of CML in blast crisis Lymphoma Tumor Board November 27, 2015 Chronic Phase CML - 2. Peter Maslak, ASH Image Bank 2011; 2011-2455 Copyright 2011 American Society of Hematology. Copyright restrictions
Management of CML in blast crisis Lymphoma Tumor Board November 27, 2015 Chronic Phase CML - 2. Peter Maslak, ASH Image Bank 2011; 2011-2455 Copyright 2011 American Society of Hematology. Copyright restrictions
Hematologic and cytogenetic responses of Imatinib Mesylate and significance of Sokal score in chronic myeloid leukemia patients
 ORIGINAL ALBANIAN MEDICAL RESEARCH JOURNAL Hematologic and cytogenetic responses of Imatinib Mesylate and significance of Sokal score in chronic myeloid leukemia patients Dorina Roko 1, Anila Babameto-Laku
ORIGINAL ALBANIAN MEDICAL RESEARCH JOURNAL Hematologic and cytogenetic responses of Imatinib Mesylate and significance of Sokal score in chronic myeloid leukemia patients Dorina Roko 1, Anila Babameto-Laku
CML UPDATE 2018 DAVID S. SNYDER, M.D. MARCH
 CML UPDATE 2018 DAVID S. SNYDER, M.D. MARCH 15, 2018 Click to edit Master Presentation Date DISCLOSURES I have nothing to disclose 2001 2016 Loss in expectation of life of patients with chronic myeloid
CML UPDATE 2018 DAVID S. SNYDER, M.D. MARCH 15, 2018 Click to edit Master Presentation Date DISCLOSURES I have nothing to disclose 2001 2016 Loss in expectation of life of patients with chronic myeloid
1794 Updating Long-Term Outcome of Intermittent Imatinib. (INTERIM) Treatment in Elderly Patients with Ph+-CML
 Treatment in Elderly Patients with Ph+-CML") 738 What Is the Most Cost-Effective Strategy for Treating Newly Diagnosed Chronic Phase Chronic Myeloid Leukaemia (CML) after Imatinib Loses Patent Exclusivity? https://ash.confex.com/ash/2014/webprogram/paper71699.html
738 What Is the Most Cost-Effective Strategy for Treating Newly Diagnosed Chronic Phase Chronic Myeloid Leukaemia (CML) after Imatinib Loses Patent Exclusivity? https://ash.confex.com/ash/2014/webprogram/paper71699.html
Bosulif. Bosulif (bosutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib
 BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
BCCA Protocol Summary for Treatment of Chronic Myeloid Leukemia and Ph+ Acute Lymphoblastic Leukemia Using PONAtinib Protocol Code Tumour Group Contact Physician ULKCMLP Leukemia Dr. Donna Forrest ELIGIBILITY:
CML: Yesterday, Today and Tomorrow. Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center
 CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
CML: Yesterday, Today and Tomorrow Jorge Cortes, MD Chief CML Section Department of Leukemia The University of Texas, M.D. Anderson Cancer Center Five Years of Signal Transduction Inhibition The Beginning
Technology appraisal guidance Published: 24 August 2016 nice.org.uk/guidance/ta401
 Bosutinib for previously treated chronic myeloid leukaemia Technology appraisal guidance Published: 24 August 2016 nice.org.uk/guidance/ta401 NICE 2018. All rights reserved. Subject to Notice of rights
Bosutinib for previously treated chronic myeloid leukaemia Technology appraisal guidance Published: 24 August 2016 nice.org.uk/guidance/ta401 NICE 2018. All rights reserved. Subject to Notice of rights
Implementation of Management Guidelines
 Implementation of Management Guidelines For Chronic Myeloid Leukemia Perspectives in the United States David Rizzieri, MD; and Joseph O. Moore, MD ABSTRACT Clinical practice guidelines are developed to
Implementation of Management Guidelines For Chronic Myeloid Leukemia Perspectives in the United States David Rizzieri, MD; and Joseph O. Moore, MD ABSTRACT Clinical practice guidelines are developed to
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping?
 Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
Discontinuation of Tyrosine Kinase Inhibitors in Chronic Myeloid Leukemia: What s Stopping us from Stopping? David Pham, PharmD PGY2 Hematology/Oncology Pharmacy Resident South Texas VA Health Care System
Post ASH Actualités LMC
 Post ASH 2014 - Actualités LMC Actualités de première ligne LMC PC ENESTnd (6 ans) Dasision (5 ans) EPIC Spirit France (5 ans) Spirit 2 UK (5 ans) ENESTnd: Mise à jour à 6 ans Design = 846 ults with wly
Post ASH 2014 - Actualités LMC Actualités de première ligne LMC PC ENESTnd (6 ans) Dasision (5 ans) EPIC Spirit France (5 ans) Spirit 2 UK (5 ans) ENESTnd: Mise à jour à 6 ans Design = 846 ults with wly
IRIS 8-Year Update. Management of TKI Resistance Will KD mutations matter? Sustained CCyR on study. 37% Unacceptable Outcome 17% 53% 15%
 Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
Management of TKI Resistance Will KD mutations matter? IRIS 8-Year Update 17% 53% 5% 15% 37% Unacceptable Outcome No CCyR Lost CCyR CCyR Other 3% 7% Safety Lost-regained CCyR Sustained CCyR on study Deininger
CML Update 2016 Arthur 2016
 CML Update 2016 Chronic Myeloid Leukemia Splenomegaly CML (3 phase disease) Increased white cells Malignant proliferation of myeloid white cells Initially mature cells a) chronic phase of disease Evolution
CML Update 2016 Chronic Myeloid Leukemia Splenomegaly CML (3 phase disease) Increased white cells Malignant proliferation of myeloid white cells Initially mature cells a) chronic phase of disease Evolution
Molecular monitoring of CML patients
 EHA, Education Session, CML Stockholm, 14 June 2013 Molecular monitoring of CML patients Martin C. Müller Medical Faculty Mannheim Ruprecht-Karls-University Heidelberg Mannheim, Germany Disclosures Research
EHA, Education Session, CML Stockholm, 14 June 2013 Molecular monitoring of CML patients Martin C. Müller Medical Faculty Mannheim Ruprecht-Karls-University Heidelberg Mannheim, Germany Disclosures Research
When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany
 When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany Chromosome 22 Chromosome 9 e1 1b m-bcr M-bcr e1 e2 b1 b5 5 3 BCR ABL 5 3 1a a2 a3 μ -bcr e19 a11 e1a2 b2a2 b3a2 e19a2 p190 bcr-abl
When to change therapy? Andreas Hochhaus Universitätsklinikum Jena, Germany Chromosome 22 Chromosome 9 e1 1b m-bcr M-bcr e1 e2 b1 b5 5 3 BCR ABL 5 3 1a a2 a3 μ -bcr e19 a11 e1a2 b2a2 b3a2 e19a2 p190 bcr-abl
Talpaz M. et al. Dasatinib in Imatinib-resistant Philadelphia chromosomepositive leukemias. N Engl J Med (2006) 354;24:
 354;24:") References Sprycel Talpaz M. et al. Dasatinib in Imatinib-resistant Philadelphia chromosomepositive leukemias. N Engl J Med (2006) 354;24:2531-2541. National Comprehensive Cancer Network. Clinical Practice
References Sprycel Talpaz M. et al. Dasatinib in Imatinib-resistant Philadelphia chromosomepositive leukemias. N Engl J Med (2006) 354;24:2531-2541. National Comprehensive Cancer Network. Clinical Practice
The legally binding text is the original French version
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 March 2007 SPRYCEL 20 mg, film-coated tablet, blister (377 637-9) SPRYCEL 20 mg, film-coated tablet, bottle (377
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 March 2007 SPRYCEL 20 mg, film-coated tablet, blister (377 637-9) SPRYCEL 20 mg, film-coated tablet, bottle (377
New drugs in first-line therapy
 New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
New drugs in first-line therapy Gianantonio Rosti Dept of Hematology and Oncology Seràgnoli, Bologna University (Italy) GIMEMA (Gruppo Italiano Malattie Ematologiche dell Adulto) CML WORKING PARTY IRIS
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 1.2015 NCCN.org Continue Version 1.2015, 08/28/14 National Comprehensive Cancer Network, Inc. 2014,
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML
 Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
Molecular Detection of BCR/ABL1 for the Diagnosis and Monitoring of CML Imran Mirza, MD, MS, FRCPC Pathology & Laboratory Medicine Institute Sheikh Khalifa Medical City, Abu Dhabi, UAE. imirza@skmc.ae
Patient With Chronic Myeloid Leukemia in Complete Cytogenetic Response: What Does It Mean, and What Does One Do Next?
 VOLUME 32 NUMBER 5 FEBRUARY 10 2014 JOURNAL OF CLINICAL ONCOLOGY ONCOLOGY GRAND ROUNDS Patient With Chronic Myeloid Leukemia in Complete Cytogenetic Response: What Does It Mean, and What Does One Do Next?
VOLUME 32 NUMBER 5 FEBRUARY 10 2014 JOURNAL OF CLINICAL ONCOLOGY ONCOLOGY GRAND ROUNDS Patient With Chronic Myeloid Leukemia in Complete Cytogenetic Response: What Does It Mean, and What Does One Do Next?
CML: Role of combination treatments, Interferon and immunotherapy in CML
 CML: 2017 Role of combination treatments, Interferon and immunotherapy in CML Andreas Burchert Philipps Universität Marburg Universitätsklinikum Gießen und Marburg GmbH Key Developments that will Change
CML: 2017 Role of combination treatments, Interferon and immunotherapy in CML Andreas Burchert Philipps Universität Marburg Universitätsklinikum Gießen und Marburg GmbH Key Developments that will Change
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA.
 A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
A COMPARATIVE EFFECTIVENESS ANALYSIS OF PATIENTS NEWLY INITIATING TYROSINE KINASE INHIBITOR THERAPY FOR CHRONIC MYELOID LEUKEMIA Melea Ward A dissertation submitted to the faculty of the University of
AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA.
 AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA Michele.Baccarani@unibo.it EUROPEAN LEUKEMIANET 2013 (Blood 2013;122:885 892). RESPONSE
AGGIORNAMENTI IN EMATOLOGIA Faenza, 7 Giugno 2018 LMC: ALGORITMI TERAPEUTICI ATTUALI E IL PROBLEMA DELLA RESISTENZA Michele.Baccarani@unibo.it EUROPEAN LEUKEMIANET 2013 (Blood 2013;122:885 892). RESPONSE
Treatment and Survival in Patients with Chronic Myeloid Leukemia in a Chronic Phase in the West of Iran
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.17.7555 RESEARCH ARTICLE Treatment and Survival in Patients with Chronic Myeloid Leukemia in a Chronic Phase in the West of Iran Mehrdad Payandeh 1&, Masoud
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.17.7555 RESEARCH ARTICLE Treatment and Survival in Patients with Chronic Myeloid Leukemia in a Chronic Phase in the West of Iran Mehrdad Payandeh 1&, Masoud
Technology appraisal guidance Published: 21 December 2016 nice.org.uk/guidance/ta426
 Dasatinib, nilotinib and imatinib for untreated chronic myeloid leukaemia Technology appraisal guidance Published: 21 December 2016 nice.org.uk/guidance/ta426 NICE 2017. All rights reserved. Subject to
Dasatinib, nilotinib and imatinib for untreated chronic myeloid leukaemia Technology appraisal guidance Published: 21 December 2016 nice.org.uk/guidance/ta426 NICE 2017. All rights reserved. Subject to
What is New in CML Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas
 What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
What is New in CML 2018 Jorge Cortes, MD Chief, CML and AML Sections Department of Leukemia MD Anderson Cancer Center Houston, Texas Final Results CML-IV Molecular Response with Imatinib 1538 pts newly
Chronic Myelogenous Leukemia
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Chronic Myelogenous Leukemia Version 3.2014 NCCN.org Continue Version 3.2014, 01/15/14 National Comprehensive Cancer Network, Inc. 2014,