Hormone-Independent Metastatic Breast Cancer
|
|
|
- Shanon Adams
- 6 years ago
- Views:
Transcription
1 Hormone-Independent Metastatic Breast Cancer Alison Stopeck, M.D. Director, Clinical Breast Cancer Program Arizona Cancer Center University of Arizona Tucson, AZ
2 Discussion Points Heterogeneity of hormone resistant breast cancers Triple negative HR positive disease resistant to hormonal therapies Goals of treatment To prolong life Maintain QOL Palliate symptoms Optimally balance the benefits and toxicities of therapy
3 Improvements in OS in MBC -Population based study from British Columbia -Compared survival in pts with first diagnosis of MBC in 4 time cohort Ref: Chia et al. Cancer 2007;110: Year of Diagnosis OS (days) HR P <.001
4 11 ECOG adjuvant chemotherapy trials from ,785 patients, of whom 3447 (25%) had distant recurrence Median OS after recurrence was 20 months Improvement in OS seen only in those pts with short DRFI (?trastuzumab effect) Shorter DRFI, ER neg, # positive LNs, and black race associated with inferior survival after relapse NOT year of recurrence DRFI </= 3 years p=0.04 DRFI > 3 years p=0.47 Ref: AJ Tevaarwerk et al. Cancer 2013:119:1140-8
 Only use of adjuvant chemotherapy was statistically correlated? Improvements in DFS are more weighted towards a reduction in LR rather distant met recurrences Ref: Bouganim et al.")
5 Patterns of Recurrence in ESBC 1/90 thru 3/11 53 RCTs and > 86,000 pts Proportion of Loco-regional recurrences has decreased from 30% to 15% (P<0.001) Only use of adjuvant chemotherapy was statistically correlated? Improvements in DFS are more weighted towards a reduction in LR rather distant met recurrences Ref: Bouganim et al. Breast Cancer Res Treat 2013; 139:
6 Caveats of Data Perils of Phase II studies Do not necessarily translate into positive phase III trials Choice of endpoints PFS vs OS Obtain FDA approval
7 God speaks to oncologists with large, randomized phase III trials The devil speaks with small single institution phase II trials Paraphrasing George W. Sledge, M.D.
8 Surrogate Endpoints for Overall Survival in Metastatic Breast Cancer R 2 =0.96 R 2 =0.48 Excellent correlation between RR and PFS Poor correlation between PFS and OS Ref: Burzykowski T et al. JCO 2008;26:
9 Determinants of Therapy Understand the drivers of the tumor Great targets Estrogen Receptor Her 2 Receptor Triple Negative No proven target Heterogeneity
 Amir E et al.")
10 Changes in ER, PgR, and HER2 between the original primary and metastasis Heterogeneity within the original tumor and metastatic sites ( ) Amir E et al. JCO 2012;30:
11 Survival By Discordance No compromise in outcome No discordance in TN Loss of PR associated with worse TTP with HT Re-analysis primary tumors, discordance rates (ER 6%, PR 12%, HER2 4%) Avoid Bone Bx (lowest yield at 64%) Lead to changes in Rx in 14% (1 in 7) Amir E et al. JCO 2012;30:
12 Intrinsic Subtypes (Perou and Sorlie) Luminal A Luminal B ERBB2+ Basal Normal Triple Negative Tumors BL1 BL2 IM M MSL LAR BL1= basal-like 1 BL2 = basal-like 2 IM = immunomodulatory M = mesenchymal MSL = mesenchymal stem-like LAR = luminal androgen receptor Ref: Sorlie et al. PNAS 2001; 98;10869 Lehmann BD et al. J Clin Invest 2011;121:2750
13 Triple Negative Subtype as a Determinant of Therapy TN Subtype Chararacteristics Targeted Therapy Basal like-1 Basal like-2 Immunomodulary (IM) Mesenchymal (M) Mesenchymal stem-like (MSL) Luminal androgen receptor (LAR) BRCA, HRD Highest pcr rates ~BL1, but EGF, MET, IGFR1 immune cell signaling, NFKB, JAK/STAT, TNF Medullary EMT, TGF-B, Src Metaplastic cancer Angiogenesis: VEGFR2, PDGF, EGFR Androgen receptor and other hormone pathways Platinums PARP inhibitors EGFR inhibitors Anti-PD-1, PD-L1, CTLA- 4 antibodies JAK 2 inhibitors Dasatinib, Sarcoma regimens (Doxil, Temsirolimus, Bev 42% RR in 12 pts) 1 Anti-angiogenics Bicalutamide, abiraterone, enzalutamide, mtor i (ref: Moroney et al. CCR 2012: 18:5796)
14 PARP Inhibitors in BRCA Associated Breast Cancer Agent Dose ORR PFS (mo) Germline BRCA Olaparib 400mg BID 100mg BID Veliparib 40mg BID + TMZ 11/27 (41%) 6/22 (22%) 17% (all) 37.5% (BRCA +) 5.7 mo ( ) 1.9 mo 5.5 mo Toxicities 100% Fatigue, nausea, vomiting, anemia 23 TN + 8 BRCA Expansion 3.5 mo 21 BRCA Myelosuppresion Ref:Tutt et al. Lancet 2010;376:235. Isakoff et al. ASCO 2010abstract
15 PARP Inhibitors and BRCA Disease Olaparib 400mg BID No responses in TN without BRCA germline mutations SD in 38% of BRCA carriers of which ~50% were TN Major toxicities: Fatigue, nausea, vomiting, decreased appetite Ref: KA Gelmon et al. Lancet Oncology 2011;12:
16 Targeting EGFR EGFR overexpressed in TNBC Correlate with BL subtype BL subtype often have defects in DNA repair genes and thus may be particularly sensitive to DNA damaging agents such as platinums
17 Cetuximab in TN MBC Stage IV TNBC < 1 prior Rx for MBC 2:1 Cisplatin 75mg/m2 D1 q 3 weeks + Cetuximab 400mg/m2 load followed by 250mg/m2 weekly N = cycles Cisplatin Maintenance Cetuximab Cisplatin 75mg/m2 D1 q 3 weeks N = 58 Median age: 52 years 1st line: 73% Baselga J et al. JCO 2013;31:
18 Baselga J et al. JCO 2013;31: ORR: 20% vs 10%
19 Randomized Trials of Cetuximab in Triple Negative Metastatic Breast Cancer Author N Treatment Arms ORR Carey et al TBCRC Cetuximab Cet/carbo Carboplatin + cetuximab 6% 17% Median PFS 1.4 mo. 2.1 mo. Baselga et al BALI Cisplatin Cisplatin + cetuximab 10% 20% 1.5 mo. 3.7 mo. (p=0.03) O Shaughnessy et al 154 Irinotecan + carbo cetuximab Irinotecan + carbo + cetuximab 28% 33% 4.5 mo. 4.7 mo. Carey et al. J Clin Onc 2012; 30: Baselga J et al. JCO 2013;31: O Shaughnessy et al. Proc SABCS 2008; Abstract 308.
20 EGFR Inhibitors in TN Disappointing results with cetuximab ORR 5-10% as single agent in unselected TN patients Small molecule inhibitors (TKIs) Single agent trials Erlotinib RR 3% Gefitinib RR 0%
21 Disappointing Results with EGFR inhibitors: Cetuximab Erlotinib Gefitinib Another Hypothesis EGFR on Breast Cancer Cell Surface Signaling through receptor MUC-1 Translocation to nucleus Nonessential pathway of cell growth? Refs: Schroeder, MUC1 regulates nuclear localization and function of the epidermal growth factor receptor, J Cell Sci., 2010 Schroeder, Cancer Res, 2007 EGFR interacts with DNA/ promoters of cell cycling genes (Cyclin D1) Cell Growth and Cancer Progression

22 - MB-MDA-468 (TN breast cancer cell line) - EGFR = green staining - Presence of EGF and MUC-1 EGFR translocates to the nucleus - In presence of EGF and sirna to MUC-1 no EGFR in the nucleus, but instead trapped at the nuclear membrane Inhibition of cell growth
23 Targeting Angiogenesis TNBC have higher levels of VEGF compared to ER+ BC Mutated p53 associated with increased plasma and intratumoral levels of VEGF and BL subtypes Wildtype p53 increases levels of the natural inhibitor of angiogenesis, thrombospondin-1
24 Meta-analysis of First-line Bevacizumab Plus Chemotherapy Trials E2100, AVADO, RIBBON-1 trials N = 2447 TN subgroup = 621 pts All Patients (N = 2447) Triple Negative Patients (N = 621) Chemo Chemo + Bev HR P Chemo Chemo + Bev HR P ORR 32% 49% < % 42% <.0001 PFS (mo) ( ) ( ) <.0001 OS year survival 77% 82% 65% 71%.11 Miles D W et al. Ann Oncol 2013;1-8
25 Phase III RIBBON 2 Trial of Chemotherapy/ Bevacizumab in Second-line HER2-Negative MBC Inclusion criteria: 1 prior chemotherapy Exclusion criteria: > 1 cytotoxic regimen for MBC HER2 + Prior VEGFtargeted therapy R A N D O M I Z E (n = 684) 2:1 Chemotherapy (taxane*, gemcitabine, vinorelbine, or capecitabine) Bevacizumab 10 mg/kg q 2 weeks or 15 mg/kg q 3 weeks Chemotherapy (taxane*, gemcitabine, vinorelbine, or capecitabine Placebo q 2 weeks or q 3 weeks * RIBBON 2 allows docetaxel, paclitaxel, or albumin-bound paclitaxel. PD PD Primary endpoint: progression-free survival Chemotherapy regimen is determined by investigator prior to randomization. Brufsky et al. JCO 2011;29:
26 RIBBON 2: Efficacy Overall Response Rate Median Progression-Free Survival Median Overall Survival (Interim) Chemotherapy/ Placebo Chemotherapy/ Bevacizumab 29.6% 39.5% P =.0193 (n = 225) (n = 459) 5.1 months 7.2 months HR 0.78 (95% CI, ); P = months 18 months HR 0.90 (95% CI, ); P =.3741 Chemotherapy: taxanes (44%), gemcitabine (23%), capecitabine (21%), vinorelbine (11%) Duration of response was similar with or without bevacizumab (7.3 months vs. 7.5 months). Brufsky et al. SABCS 2009; abstract 42.
27 RIBBON-2 TN Subset -N =159 pts (23%) -Majority received taxane chemotherapy Brufsky et al. Breast Cancer Res Treat 2012; 133: 1067 Chemo+ Bev N = 112 Chemo alone N = 47 PFS (months) HR (CI) ( ) P value OS (months) HR (CI) ( ) P value
28 Predictive Biomarker For Antiangiogenic Therapy AVADO Trial Biomarker Discovery Extensive Search for a predictive biomarker Plasma: VEGF-A 121, VEGFR-1, VEGFR-2, E-selectin, VCAM, ICAM-1 Tumor: (IHC and qrt-pcr) VEGF-A, VEGF-C, VEGF-D VEGFR-2, VEGFR-3 Placental Growth Factor Neuropilin-1 Germline DNA for SNPs in VEGF pathway No formal P-value testing for multiple comparisons
29 AVADO Trial Biomarker Discovery Plasma VEGF-A, VEGFR-2 Genentech developed ELISA that preferentially measure VEGF 121
 Hormonal status (ER +/-) Paclitaxel 90mg/m2 weekly x 3 q4 weeks / Placebo 10 mg/kg q2w Co-Primary Endpoints: PFS (All Patients), PFS (VEGF high subset) Secondary Endpoints:")
30 R A N D O M I Z E D Confirmatory Study Schema: MERiDiAN MBC, HER2-Negative Chemo-naïve N=480 Paclitaxel 90 mg/m2 weekly x 3 q4 weeks / Bevacizumab 10 mg/kg q2w Stratification VEGF-A (low/high) Adjuvant therapy (yes/no) Hormonal status (ER +/-) Paclitaxel 90mg/m2 weekly x 3 q4 weeks / Placebo 10 mg/kg q2w Co-Primary Endpoints: PFS (All Patients), PFS (VEGF high subset) Secondary Endpoints: OS; ORR; Symptoms/QoL; Safety
31 Anti-Androgen therapy in LAR Triple Negative Subtype PFS on oral daily bicalutamide 150 mg Clinical benefit rate of 19% All ER/PR Negative -Majority HER2 neg -12% TN had > 10% AR expression by IHC -92% postmenopausal -Median age 66 yrs -Recur late (> 3 years) -Metastatic sites nodal, soft tissue, bone -All responders had AR > 20% -90% Gucalp A et al. Clin Cancer Res 2013;19:
 Validated MOA (microtubule inhibitor or DNA damaging) Linker: Stable in plasma Labile once internalized")
32 Antibody-Drug Conjugates Antibody: Specificity for tumor Abundant expression of target on tumor cell surface Rapid internalization of Ab Target recognition unaltered compared with naked Ab Drug: Highly potent antitumor agent (MMAE or Maytansine) Validated MOA (microtubule inhibitor or DNA damaging) Linker: Stable in plasma Labile once internalized
33 CDX-011 (Glembatumumab) EMERGE Trial Fully human monoclonal antibody that targets GPNMB linked to MMAE (dolastatin-like tubulin inhibitor) GPNMB overexpressed in ~40-75% of breast cancer expressed on both tumor cells and stromal cells Increased expression on TN associated with poor prognosis
![EMERGE: Randomized Phase II Study Endpoints: overall response rate [primary], progression-free survival, duration of response, safety, PK/PD Planned sample size = 120 Locally advanced or metastatic,](/docs-images/76/74220168/images/34-0.jpg "GPNMB+ breast cancer Refractory/resistant to approved therapies (taxane, anthracycline, capecitabine; and if HER2+, trastuzumab and lapatinib) 2-7 prior lines of cytotoxic chemotherapy for advanced")
34 EMERGE: Randomized Phase II Study Endpoints: overall response rate [primary], progression-free survival, duration of response, safety, PK/PD Planned sample size = 120 Locally advanced or metastatic, GPNMB+ breast cancer Refractory/resistant to approved therapies (taxane, anthracycline, capecitabine; and if HER2+, trastuzumab and lapatinib) 2-7 prior lines of cytotoxic chemotherapy for advanced disease Progression within 6 months of last regimen CDX-011 (1.88 mg/kg, 90 minute IV infusion, once every three weeks) Randomization (2:1) PD Cross-over to CDX-011 permitted upon centrally confirmed PD and continued eligibility Investigator s Choice single-agent chemotherapy (IC) Yardley et al. SABCS 2012
35 Progression-Free Survival (PFS) and Overall Survival (OS) All Patients TN High GPNMB TN and High GPNMB CDX-011 IC CDX-011 IC CDX-011 IC CDX-011 IC Median PFS (months) P= P= P= P=0.008* (n=96) (n=41) (n=31) (n=11) (n=27) (n=11) (n=12) (n=6) Median OS (months) P= P= P= P=0.003* (n=81) (n=41) (n=28) (n=11) (n=22) (n=11) (n=10) (n=6) High GPNMB > 25% tumor cell expression 35
36 Diagnosing the Molecular Subtype Does Not Direct Therapy Understand the patient s disease course Determine type and number of prior therapies Is the cancer hormone-resistant? After 3-4 endocrine agents unlikely to gain further benefit Hormone receptor positive disease recurrence within a short DFI Know the disease-free interval Hormone receptor positive < 2 years = short DFI Was the adjuvant chemotherapy < 1 year or > 2 years prior to metastasis? Recurrence > 2 years cancer may be responsive to same drugs Recurrence < 1 year resistant to adjuvant therapy treatment Patient s PFS and co-morbidities


37 Predicting Resistance to Hormone Therapies: Oncotype RS in de novo Metastatic Disease 128 patients with de novo MBC or MBC within 3 months of surgery Treatment as per Physician Follow For PFS and OS Biopsy Obtain Objective: To determine whether the 21- gene RS provides clinically meaningful information in pts with de novo stage IV breast cancer enrolled in TBCRC 013. King et al. ASCO 2013
38 % progression free Time to First Progression by Risk Group Recurrence Score result <18 Recurrence Score result Recurrence Score result 31 King et al. ASCO Median time to progression, months Recurrence Score result <18 months Recurrence Score result Recurrence Score result 31 Log rank, p All pts (n=102) 32 (16-NR) 20 (15-NR) 15 (9-21) ER+ (n=86) 32 (16-NR) 20 (15-NR) 15 (9-25) ER+HER2- (n=70) 32 (16-NR) 20 (15-NR) 15 (9-26) 0.013
39 % alive with disease Two Year Overall Survival by Risk Group Recurrence Score result <18 Recurrence Score result Recurrence Score result 31 King et al. ASCO Two Year Overall Survival, % Recurrence Score result <18 Recurrence Score result Recurrence Score result 31 Log rank, p All pts (n=102) 100 (78-100) 100 (78-100) 80 (69-93) ER+ (n=86) 100 (78-100) 100 (78-100) 77 (64-94) ER+HER2- (n=70) 100 (78-100) 100 (75-100) 69 (51-93) 0.001
40 21-gene Recurrence Score Independently prognostic for both time to progression and 2 yr OS in ER+ HER2- de novo stage IV breast cancer High RS ( 31) may be a surrogate for relative endocrine resistance in metastatic disease Hypothesis: RS 31 can be used to select patients with ER+ HER2- de novo stage IV breast cancer who may benefit from first line chemotherapy A randomized trial to address this hypothesis is warranted.
41 Single Agent vs Combination Chemotherapy Is More Really Better? Combinations regimens: Typically have higher response rates, time to progression, and progression free survival Toxicity is usually higher Cost higher Overall survival benefit not often achieved, due to crossover to other treatment arm True synergistic interaction that may have the potential to increase survival
42 Doxorubicin vs Paclitaxel vs Doxorubicin/Paclitaxel in Metastatic Breast Cancer E1193 trial 739 patients, first-line therapy for metastatic breast cancer Randomization to 3 arms: 1) Doxorubicin 60mg/m 2, q3 weeks 2) Paclitaxel 175mg/m 2 over 24 hours, q3 weeks 3) Doxorubicin 50mg/m 2, Paclitaxel 150mg/m 2 over 24 hours, q3 weeks plus G- CSF Sledge, G. et al. JCO 21: (2003)
43 E1193 Trial Large published randomized trial comparing single agent to combination therapy in 1 st line MBC patients Used Modern age therapies Cross-over mandated at time of progression Phase III, cooperative setting Sledge, G. et al. JCO 21: (2003)
44 Results E1193 Response (CR + PR) Median TTF (Months) Median Survival (Months) DOX Paclitaxel Dox/Pac Sledge, G. et al. JCO 21: (2003)
45 Pivotal RCT Used for Approval of Agents 2000 to 2011 Study Design PFS HR mos OS HR mos Ratio PFS/ OS Gemcitabine/Paclitaxel vs Pac / / Ixabepilone/Cape vs Capecitabine / / Cape/Docetaxel vs Docetaxel / / Nab-paclitaxel vs paclitaxel / / Ref: Ocana et al. CCR 2013:19:
46 Capecitabine +/- Ixabepilone 048 (N=1221) 046 (N=752) Dosereduced I+C=609 C=612 I+C=375 C=377 I+C > 4 cycles N = 566 Primary Outcome OS PFS ORR (%) v PFS mo v. 7.0 HR P value (CI) ( ) OS mo HR P value HR (adj) P value 0.85* Sparano JCO; 2010; Thomas. JCO 2007;26:5210; Valero Clin Br Ca 2012;12:240
47 Combination taxane chemotherapy options Line of Rx ORR (%) TTP (mo) OS (mo) X vs. XD (511) 1 st 3 rd Capecitabine (X) 30% Cape/docetaxel (XD) 42%* 6.1* 14.5 * T vs. GT (529) 1 st Paclitaxel (T) 26.9% Gemcitabine/Paclitaxel (GT) 43.1%* 6.1* 18.6* O Shaughnessy J JCO 2002;20:2812 Albain K JCO 2008;26:3950
48 Cochrane Analysis: Single Agent vs Combinatation Chemotherapy for MBC Metastatic breast cancer has inherent drug resistance Combination chemotherapy should reduce the different sensitive subpopulations of cancer cells leading to an improved disease response Cochrane analysis (2009) 43 randomized trials of single agent vs. combination chemotherapy (9742 pts) Combination therapy improved OS: HR=0.88, p< Combination therapy improved OS with taxanes (HR = 0.83) but not with anthracyclines (HR = 0.94) Cross-over design was absent in the majority of studies Conclusion insufficient data to state the net clinical benefit of combination therapy c/w sequential therapy April 15, 2009
49 Choosing Wisely- An ABIM Initiative ASCO Top 10 List (released October 2013) Number 7: Don t use combination chemotherapy (multiple drugs) instead of chemotherapy with one drug when treating an individual for metastatic breast cancer unless the patient needs a rapid response to relieve tumorrelated symptoms.
50 Schedule is as Important as Dose ORR TTP (mo) OS (mo) CALGB 9840 Wkly paclitaxel 42% 9 24 Q3w paclitaxel 29% 5 12 Nab-paclitaxel Q3w 300mg/m2 46% Wkly 100mg/m2 63% Wkly 150mg/m2 74% Docetaxel Wkly docetaxel 20.3% Q3w docetaxel 35.6% Siedman JCO 2008;26:1642; Rivera E Cancer 112:1455, 2008; Gradishar WJ JCO 2009;27:3611
51 Meta-Analysis Weekly Paclitaxel comparable to docetaxelbased regimens for MBC in terms of OS (HR 0.87), PFS (HR 0.76), TTP (HR 1.13), ORR (1.01) Paclitaxel has fewer grade 3 or 4 adverse events including anemia (RR 0.64), thrombocytopenia (RR 0.62), mucositis (RR0.08), diarrhea (RR0.19), and fatigue (RR 0.43) WX et al. Curr Med Res Opin 2013; 29:
52 First-Line Chemotherapy CALGB 40502/NCCTG N063H Randomized Phase III Trial of Weekly Paclitaxel compared to Weekly Nanoparticle Albumin Bound Nab-Paclitaxel or Ixabepilone +/- Bevacizumab - as First-Line Therapy for - Locally Recurrent or Metastatic Breast Cancer N = 799 Untreated Stage IV Strata: Adj taxanes ER/PR status 1 Control Exp 2 nab-paclitaxel 150 mg/m 2 weekly + bevacizumab 10 mg/kg q 2 wks 2 paclitaxel 90 mg/m 2 weekly + bevacizumab 10 mg/kg q 2 wks 1 ixabepilone 16 mg/m 2 weekly + bevacizumab 10 mg/kg q 2 wks 3 Restage q 2 cycles until disease progression Rugo H et al, ASCO 2012
53 Proportion Proportion Progression Alive Free CALGB Analyses Triple Triple Negative Disease paclitaxel Pac nab-paclitaxel Nab Ixa ixabepilone Months From Study Entry overall findings: - Weekly paclitaxel > ixabepilone - Weekly paclitaxel less toxic than either (in general) TNBC Subset: - No real difference from parent trial - 98% received bevacizumab Paclitaxel Nab-paclitaxel Ixabepilone Median PFS (mo) (P=.12) 7.6 (P<.001) TTF (mo) (P=.0005) 5.1 (P=.0014) OS (mo) (P=.92) 21 (P=.10)
54 Twelves et al. J Clin Oncol 2010; 28(suppl):958s (abstract CRA1004). Phase III EMBRACE Trial of Eribulin Versus Treatment of Physician s Choice for Heavily Pretreated MBC Eligibility criteria: Locally recurrent or metastatic breast cancer 2-5 prior chemotherapies: 2 for advanced disease Prior anthracycline and taxane Progression 6 months since last chemotherapy Neuropathy grade 2 R A N D O M I Z E 2 : 1) Eribulin mesylate 1.4 mg/m 2, days 1, 8 q 3 weeks Treatment of Physician s Choice (TPC) Any monotherapy approved for treatment of cancer or supportive care only Primary endpoint: OS Secondary endpoints: PFS, ORR, safety
55 Phase III EMBRACE Trial: Overall Survival OS: 13.1 vs 10.7 mos PFS: 3.7 vs 2.2 mos Cortes J Lancet 2011;377:914
56 Phase III EMBRACE Trial: Grade 3/4 Adverse Events Eribulin (n = 503) TPC (n = 247) Neutropenia 45% 21% Leukopenia 14% 6% Anemia 2% 4% Febrile Neutropenia 4% 1% Asthenia/Fatigue 9% 10% a Peripheral Neuropathy 8% 2% a Nausea 1% a 2% a Dyspnea 4% a 3% Hand-Foot Syndrome < 1% a 4% a a Grade 3 only The incidence of fatal adverse events related to treatment was 1% in both arms. Twelves et al. J Clin Oncol 2010; 28(suppl):958s (abstract CRA1004).

 Prior")



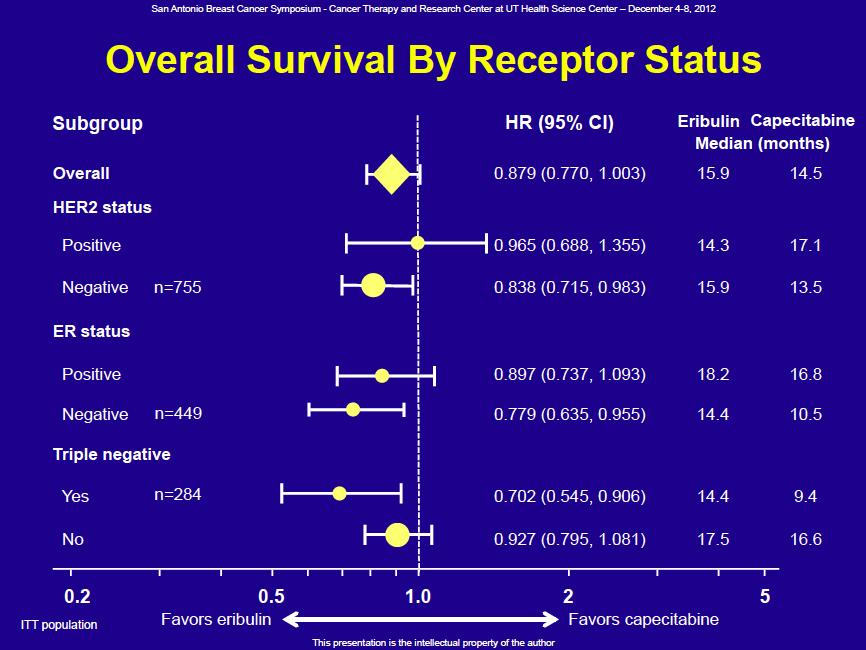
57 Chemotherapy for TNBC A Phase III, Randomized Trial Comparing Eribulin to Capecitabine In Patients With Metastatic Breast Cancer Previously Treated With Anthracyclines And Taxanes Patients (N=1102) Locally advanced or MBC 3 prior chemotherapy regimens ( 2 for advanced disease) Prior anthracycline and taxane in (neo)adjuvant setting or for locally advanced or MBC Kaufmann P et al, SABCS 2012 Eribulin mesylate 1.4 mg/m 2 2- to 5-min IV Day 1 & 8 q21 days Randomization 1:1 Capecitabine 1250 mg/m 2 BID orally Days 1-14, q21 days Co-primary endpoint OS and PFS Secondary endpoints Quality of life ORR Duration of response 1-, 2- and 3-year survival Tumor-related symptom assessments Safety parameters Population PK (eribulin arm only)
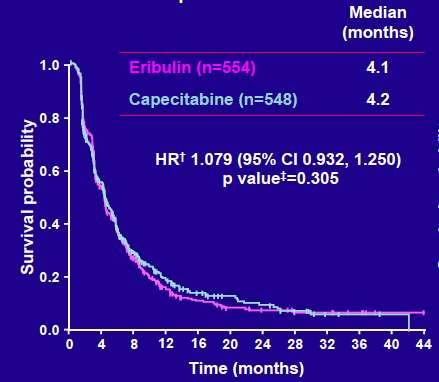
58 Progression-Free Survival
59
60 Conclusions Eribulin equivalent to capecitabine after anthracycline/taxane therapy Eribulin appears superior for TN disease Different toxicity profiles - Eribulin (IV): neutropenia, alopecia, neuropathy - Capecitabine (Oral): HFS, diarrhea
61 Optimal Duration of First Line Chemotherapy for MBC Progression Free Survival 11 trials 2,269 pts 36 % Gennari A et al. JCO 2011;29:
62 Overall Survival (1st Line Chemo) 11 trials 2,269 pts Gennari A et al. JCO 2011;29:

63 (A) Treatment scheme. Phase III, Multicenter Randomized Trial of Maintenance Chemotherapy vs Observation in Patients with MBC After Achieving Disease Control with 6 Cycles PG Paclitaxel: 175mg/m2 q 21d Gemcitabine: 1250mg/m2 d1,8 -Used modern day taxane regimen that is well-tolerated and shown to have increased PFS and OS as first line therapy without clinically meaningful increase in toxicity -Hormonal therapy was not allowed in either group (~75% of pts ER +) -Median age 47.5 years -Primary endpoint: PFS in patients with disease control after 6 cycles Park Y H et al. JCO 2013;31: Park et al. JCO 2013;31: by American Society of Clinical Oncology
64 Kaplan Meier Curves for PFS and OS with Maintenance PG -Mean of 6 additional cycles in maintenance group (range: 3 20 cycles) -28% of patients assigned to maintenance did not to receive chemo -3.7 mos improvement in PFS associated with 8.8 mos improvement in OS -PFS in TN patients HR 0.52 (CI ) -Benefit driven by impact in younger, premenopausal, ER negative women with extensive, yet responsive disease Park et al. JCO 2013;31: 1732
65 Future Therapies Clinical trials.gov: 400 studies currently recruiting and open for MBC TN specifically: 41 studies Many targeting specific pathways related to molecular profiling PARP inhibitors GPNMB (CDX-011) PIK3CA HSP 90 Angiogenesis Aurora Kinase MET FGFR mtor ADC (folate) EGFR HER3 ɣ-secretase estradiol JAK2 LIV-1 AKT Src
66 Conclusions Optimal therapy for MBC: Combine Clinical Picture, Patient Preferences, and Molecular Subtyping to formulate the best treatment plan Molecular Profiling is evolving, but not yet validated for clinical decisions Sequential therapies are less toxic and likely as good as combination therapy for the majority of patients New therapies are on the horizon, but will require tissue biopsies, target validation, and screening many for the accrual of one
67 Leading Causes of Death Pneumonia 2. Tuberculosis Heart disease 2. Cancer 8. Cancer 7. Influenza/pneumonia
68 Learning from the Past Pneumonia Breast Cancer Antibiotics Vaccination Targeted Therapies Immune modulation Improved sanitation and refrigeration Prevention and Early Diagnosis



69 Thank you for your attention

70 First, isolated, ipsilateral, resectable recurrence IBTR or CW recurrence Axillary or IM LN Fully excised CALOR Trial > 1 drug, 3-6 cycles
71 CALOR: Disease-Free Survival N=162 ER + subset ER neg subset 5-yr OS 88% vs 76%, HR 0.41, P=.02 Aebi S et al, SABCS 2012
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015
 Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned
 The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA
 Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Hormone-Independent Metastatic Breast Cancer. Beth Overmoyer MD, FACP Assistant Professor of Medicine HMS Dana Farber Cancer Institute SOBO 2012
 Hormone-Independent Metastatic Breast Cancer Beth Overmoyer MD, FACP Assistant Professor of Medicine HMS Dana Farber Cancer Institute SOBO 2012 Metastatic Breast Cancer MBC is a heterogeneous disease without
Hormone-Independent Metastatic Breast Cancer Beth Overmoyer MD, FACP Assistant Professor of Medicine HMS Dana Farber Cancer Institute SOBO 2012 Metastatic Breast Cancer MBC is a heterogeneous disease without
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
4, :00 PM 9:00 PM
 Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Management of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot
 Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Breast Cancer: Chemotherapy and Novel Agents
 North Carolina Oncology Association & South Carolina Oncology Society Joint Membership Meeting ~ February 26 27, 2010 The Ballantyne Resort ~ Charlotte, NC Breast Cancer: Chemotherapy and Novel Agents
North Carolina Oncology Association & South Carolina Oncology Society Joint Membership Meeting ~ February 26 27, 2010 The Ballantyne Resort ~ Charlotte, NC Breast Cancer: Chemotherapy and Novel Agents
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2014 San Antonio Breast Cancer Symposium Review
 2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
When is Chemotherapy indicated in Advanced Luminal Breast Cancer?
 When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico
 Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of ncology (VHI), Medica Scientia
Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of ncology (VHI), Medica Scientia
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Common disease 175,000 new cases/year 44,000 deaths/year Less than 10% with newly diagnosed at presentation have stage IV disease Chronic disease,
 Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
Overview and future horizons of PARP inhibitors in BRCAassociated. Judith Balmaña
 Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
Systemic therapy of triple negative advanced breast cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development
 Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Emerging Therapies for Triple Negative Breast Cancer
 Emerging Therapies for Triple Negative Breast Cancer Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Emerging Therapies for Triple Negative Breast Cancer Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Update on Breast Cancer
 Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Eribulin for locally advanced or metastatic breast cancer third line; monotherapy
 Eribulin for locally advanced or metastatic breast cancer third line; monotherapy April 2009 This technology summary is based on information available at the time of research and a limited literature search.
Eribulin for locally advanced or metastatic breast cancer third line; monotherapy April 2009 This technology summary is based on information available at the time of research and a limited literature search.
Mechanisms of Resistance to. Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center
 Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
National Horizon Scanning Centre. Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy
 in combination with non-taxanes for metastatic breast cancer - first line therapy") Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy December 2007 This technology summary is based on information available at the time of research and
Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy December 2007 This technology summary is based on information available at the time of research and
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER
 SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica?
 2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Triple negative breast cancer Biology and targeted therapy
 Triple negative breast cancer Biology and targeted therapy MR SCI MED DR I BOŽOVIĆ -SPASOJEVIĆ INSTITUT ZA ONKOLOGIJU I RADIOLOGIJU SRBIJE I VA N A B O Z O V I C @ O U T L O O K. C O M Current challanges
Triple negative breast cancer Biology and targeted therapy MR SCI MED DR I BOŽOVIĆ -SPASOJEVIĆ INSTITUT ZA ONKOLOGIJU I RADIOLOGIJU SRBIJE I VA N A B O Z O V I C @ O U T L O O K. C O M Current challanges
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Endocrine treatment might NOT be the preferred option in Hrpos MBC. Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015
 Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
Overview of nab-paclitaxel in Breast Cancer
 Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Chemotherapy for Isolated Locoregional Recurrence
 Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Triple-Negative Breast Cancer
 June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
Science-Based Innovation-Focused ADC Company. Corporate Overview June 2018
 Science-Based Innovation-Focused ADC Company Corporate Overview June 2018 Forward-Looking Statements This presentation, in addition to historical information, contains certain forwardlooking statements
Science-Based Innovation-Focused ADC Company Corporate Overview June 2018 Forward-Looking Statements This presentation, in addition to historical information, contains certain forwardlooking statements
Systemic Therapy for Locally Advanced Breast Cancer
 Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA
 For projector and public [noacic] Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA 1 st Appraisal Committee meeting
For projector and public [noacic] Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA 1 st Appraisal Committee meeting
Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS. Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology
 Senior Consultant, Medical Oncology") Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology Overview of TNBC Still best way to define in clinical practice!? Survival (%) Treatment
Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology Overview of TNBC Still best way to define in clinical practice!? Survival (%) Treatment
Heather Wakelee, M.D.
 Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Sponsored by Educational Grant Support from Adjuvant (Post-Operative) Lung Cancer Chemotherapy Heather Wakelee, M.D.
Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Sponsored by Educational Grant Support from Adjuvant (Post-Operative) Lung Cancer Chemotherapy Heather Wakelee, M.D.
Pathways Underlying Aggressive Breast Cancers
 Origin of Breast Cancer Subtypes Pathways Underlying Aggressive Breast Cancers HER2 and ER can be expressed in any subtype. Triple Negative -- a mixture of subtypes Joyce O Shaughnessy, MD Baylor Sammons
Origin of Breast Cancer Subtypes Pathways Underlying Aggressive Breast Cancers HER2 and ER can be expressed in any subtype. Triple Negative -- a mixture of subtypes Joyce O Shaughnessy, MD Baylor Sammons
Role of Primary Resection for Patients with Oligometastatic Disease
 GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Systemic chemotherapy for metastatic breast cancer
 Oncology and Translational Medicine October 2015, Vol. 1, No. 5, P226 232 DOI 10.1007/s10330-014-0048-6 REVIEW ARTICLE Systemic chemotherapy for metastatic breast cancer Yannan Zhao, Biyun Wang ( ) Department
Oncology and Translational Medicine October 2015, Vol. 1, No. 5, P226 232 DOI 10.1007/s10330-014-0048-6 REVIEW ARTICLE Systemic chemotherapy for metastatic breast cancer Yannan Zhao, Biyun Wang ( ) Department
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
New Drug Development in HER2+ Breast Cancer
 New Drug Development in HER2+ Breast Cancer Philippe Aftimos, M.D. Senior Research Physician Clinical Pharmacology Unit Institut Jules Bordet Background Amplification of HER2 occurs in approximately 20%
New Drug Development in HER2+ Breast Cancer Philippe Aftimos, M.D. Senior Research Physician Clinical Pharmacology Unit Institut Jules Bordet Background Amplification of HER2 occurs in approximately 20%