DIAGNOSIS OF LUNG CANCER. Dr. Sayeed ahmed, Assistant prof, MD,DAA.
|
|
|
- Clare Mosley
- 6 years ago
- Views:
Transcription
1 DIAGNOSIS OF LUNG CANCER Dr. Sayeed ahmed, Assistant prof, MD,DAA.
2 Diagnosis of lung cancer can be done by 1) Clinical presentation 2) Investigations a) non invasive b) invasive
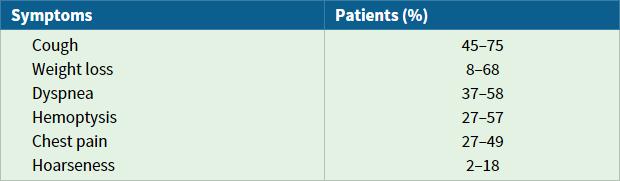
3 Clinical Presentation
4 Metastatic Manifestations Intrathoracic metastases - Superior Vena Cava Syndrome - Malignant Pleural Effusion - Recurrent Laryngeal Nerve Palsy - Phrenic Nerve Palsy - Pancoast s Syndrome - Horner s Syndrome - Involvement of heart and pericardium - Involvement of esophagus
5 Extrathoracic manifestations - Brain metastases - Skeletal metstases - Adrenal metastases - Lymph node metastases - Hepatic metastases

6 Extended Clinical Evaluation
7 NON INVASIVE INVESTIGATIONS
8 Sputum Cytology The sensitivity and specificity of sputum cytology are 66% and 99%, respectively Its accuracy depends on the expertise of the health care team in obtaining the sample (three samples are required), the preservation technique, and the size and location of the lesion. Central lesions are more likely to yield positive cytologic results than are peripheral lesions. Sputum cytology should be obtained in all patients with central lesions who are at risk for more invasive biopsy techniques. In addition, patients with hemoptysis with or without a mass on chest radiographs should have sputum cytology obtained.
9 Chest Radiography The majority of lung cancers are detected initially by plain chest radiograph. In certain situations, the plain film may be sufficient to detect spread to the mediastinum. For example, the presence of bulky lymphadenopathy in the superior or contralateral mediastinal areas may be considered adequate evidence of metastatic disease to preclude further imaging evaluation of the chest. The chest radiograph is simply too insensitive a measure of mediastinal lymph node involvement with lung cancer, and thus, further noninvasive or invasive assessment is usually necessary.
10 Computed Tomography of the Chest CT of the chest is the most widely available and commonly used noninvasive modality for evaluation of the mediastinum in lung cancer CT is helpful in defining the size, location, and characteristics of the primary mass (e.g., smooth-bordered, spiculated, calcified), the presence or absence of lymphadenopathy and, if performed through the adrenal glands, the presence of abnormalities in the liver and adrenal glands. The bony structures of the thoracic cavity can also be evaluated by chest CT.
11 Numerous studies of CT have been performed comparing clinical staging by CT with the gold standards of mediastinoscopy or surgery. The results demonstrated that regardless of the lymph node size used as a threshold for defining malignant adenopathy, CT findings in isolation could not be considered as conclusive evidence that lymph nodes were malignant. The most widely accepted criterion for an abnormal lymph node is a short-axis lymph node diameter of 1 cm or greater on CT.
12 Other criteria used are : 1. A long axis diameter of 1c m, 2. A short axis diameter of 1.5 cm, 3. A short axis diameter of 1 cm plus evidence of central necrosis or disruption of the capsule, and 4. A short axis diameter of 2 cm regardless of nodal morphology.
13 The American College of Chest Physicians (ACCP) compiled the studies assessing the performance characteristics of CT scan for staging the mediastinum in a meta-analytic format.thirty-five studies were identified, comprising 5111 evaluable patients. The pooled sensitivity of CT scanning for staging the mediastinum was 51% (95% CI, 47% 54%) and the pooled specificity was 86% (95% CI, 84% 88%).
14 The corresponding positive and negative likelihood ratios were 3.4 and 0.6, respectively, confirming that CT scanning has a limited ability either to rule in or to exclude mediastinal metastasis. However, because CT usually guides the selection of nodes for biopsy by mediastinoscopy or needle aspiration, it remains an important diagnostic tool in lung cancer. Accurate noninvasive node staging is essential because the choice of individual nodes for sampling by minimally invasive techniques, including transbronchial, transthoracic, or transesophageal needle aspiration, will be directed by the findings of the CT scan.
15 The limitation of CT-based mediastinal lymph node evaluation is evident in the fact that 5% to 15% of patients with clinical T1N0 lesions will be found to have positive lymph node involvement by surgical lymph node sampling. the most important message in evaluating the accuracy of CT scanning is that approximately 40% of all nodes deemed malignant by CT criteria are actually benign, depending on the patient population.specificity can be affected by clinical factors such as the presence of obstructive pneumonitis.
16 CT can also be helpful in the evaluation of pleural effusion in patients withlung cancer. The CT scan can indicate the presence or absence of fluid, the contour of the pleural space, and whether or not nodules or masses are present on the pleural surface. Given the limitations of the imperfect sensitivity and specificity of CT, it is usually inappropriate to rely solely on the CT scan to determine mediastinal lymph node status. Nonetheless, CT continues to play an important and necessary role in the evaluation of patients with lung cancer and is recommended as part of the evaluation of patients who present with newly diagnosed or suspected lung cancer.
17 Positron Emission Tomography PET is a metabolic imaging technique based on the function of a tissue rather than on its anatomy. Lung cancer cells demonstrate increased cellular uptake of glucose and a higher rate of glycolysis when compared with normal cells. The radiolabeled glucose analogue [ 18 F]fluoro-2- deoxy-d-glucose (FDG) undergoes the same cellular uptake as glucose but, after phosphorylation, is not further metabolized and becomes trapped in cells.
18 Accumulation of the isotope can then be identified using a PET detector. Specific criteria for an abnormal PET scan are either a standard uptake value of greater than 2.5 or uptake in the lesion that is greater than the background activity of the mediastinum. It has proved useful in differentiating neoplastic from normal tissues.
19 In 2865 evaluable patients, the pooled estimates of sensitivity and specificity for identifying mediastinal metastasis were 74% (95% CI, 69% 79%) and 85% (95% CI, 82% 88%), respectively. Corresponding positive and negative likelihood ratios for mediastinal staging with PET scanning were 4.9 and 0.3, respectively. These findings demonstrate that PET scanning is more accurate than CT scanning for staging of the mediastinum in patients with lung cancer, though PET is far from perfect.
20 Whereas a negative mediastinal PET may obviate the need for mediastinoscopy prior to thoracotomy in certain situations, a positive mediastinal PET should not negate further evaluation or the possibility of resection. In the latter case, lymph node sampling should still be pursued because the possibility of a false-positive PET scan cannot be ignored.
21 It should be remembered that PET is primarily a metabolic examination and has limited anatomic resolution. It is possible for PET to identify lymph node stations but not individual lymph nodes. CT scanning provides much more anatomic detail but lacks the functional information provided by PET.
22 Disadvantages the technique is not infallible because certain non-neoplastic processes, including granulomatous and other inflammatory diseases as well as infections, may also demonstrate positive PET imaging. Furthermore, size limitations are also an issue, with the lower limit of resolution of the study being approximately 7 to 8 mm depending on the intensity of uptake of the isotope in the abnormal cells. One should not rely on a negative PET finding for lesions less than 1 cm on CT scan.
23 Newer technology includes CT/PET fusion, a single machine that incorporates CT and PET during the same scan. This allows the clinician to obtain anatomic (CT) and functional (PET) images simultaneously. Early work suggests improvement in the number of patients correctly staged with this modality over CT or PET alone. The future of PET in lung cancer may also include its use to evaluate response to treatment.
24 Magnetic Resonance Imaging There are very few circumstances in which magnetic resonance imaging (MRI) is a useful tool in staging lung cancer. However, MRI can be useful in evaluating superior sulcus tumors, especially for possible invasion of the brachial plexus, and for evaluating vertebral invasion.
25 Adrenal and Hepatic Imaging For adrenal masses, CT, MRI, percutaneous biopsy, and even adrenalectomy can be used to help delineate benign from malignant disease. Well-defined, low-attenuation (fatty) lesions with a smooth rim on unenhanced CT are more likely to be benign adenomas,but the CT appearance of many lesions is insufficiently distinctive.
26 Follow-up scanning with repeat CT, serial ultrasonography, MRI (especially with chemical shift and dynamic gadolinium-enhanced techniques), or 6-β-iodo- 131 I-methylnorcholesterol scanning can sometimes help with the critical distinction between metastatic disease and adenoma. Percutaneous adrenal biopsy is a relatively safe and effective means of achieving a definitive diagnosis in doubtful cases and is especially important when the histology of the adrenal mass will dictate subsequent management.
27 Most liver lesions are benign cysts and hemangiomas, but contrast CT (or ultrasound) is often required to establish a likely diagnosis. Percutaneous biopsy can be performed when diagnostic certainty is required.
28 INVASIVE TECHNIQUES
29 Mediastinoscopy Mediastinoscopy remains the gold standard for invasively staging the mediastinum in patients with known or suspected lung cancer. Mediastinoscopy is most often used to sample nodes of the paratracheal (station 4), and anterior subcarinal (station 7) region. The subcarinal area is more difficult to sample and thus has a lower yield.
30 An extended cervical mediastinoscopy can be carried out to reach aortopulmonary and paraaortic lymph nodes (stations 5 and 6) by using the same cervical incision as mediastinoscopy but dissecting into a different fascial plane. Alternatively, an anterior mediastinotomy (the so-called Chamberlain procedure) may be needed to sample lymph nodes in these aortopulmonary and para-aortic locations (stations 5 and 6).
31 Overall, mediastinoscopy has a reported sensitivity of 78%, with a specificity of 100%. Mediastinoscopy may also be able to differentiate between stage IIIA and IIIB mediastinal involvement. As with any surgical procedure, mediastinoscopy has risks and limitations. It requires general anesthesia, with a morbidity of 2% and a mortality of 0.08%
32 Transthoracic Needle Aspiration Transthoracic needle aspiration (TTNA), usually under CT or fluoroscopic guidance, is an expedient and relatively safe way to diagnose the primary tumor mass and establish a diagnosis of lung cancer. As a general rule, if a lesion is less than 3 cm in size and lateral to the midclavicular line, bronchoscopy would not be the diagnostic procedure of choice. TTNA should be considered under such circumstances if tissue diagnosis is necessary. The sensitivity and specificity of TTNA are 90% and 97%, respectively
33 TTNA may be essential only in certain situations: 1. patients who are poor surgical candidates but who require tissue diagnosis prior to treatment, 2. patients in whom a noncancerous lesion is strongly suspected, 3. patients who request that a diagnosis of cancer be confirmed prior to considering surgery, and 4. patients with high likelihood of metastatic disease.
34 One drawback of TTNA is the risk of pneumothorax. Several investigations have reported a 22% to 45% risk of pneumothorax for CT-guided TTNA. Although pneumothorax may lead to hemodynamic compromise without therapeutic tube thoracostomy, in most cases of pneumothorax secondary to TTNA, treatment is not required. The primary factors shown to increase the risk or incidence of pneumothorax are the presence of emphysema, a smaller lesion size, and a greater depth of needle penetration from the pleural surface to the edge of the lesion.
35 Fiberoptic Bronchoscopy Patients with known or suspected lung cancer may have symptoms due to endobronchial involvement that require airway inspection with bronchoscopy: shortness of breath, unilateral wheezing, hemoptysis, and cough. Endobronchial lesions can be visualized easily and biopsied through a flexible bronchoscope. The yield with three or more biopsies should approach 100% for centrally located lesions.
36 Data from 4507 patients revealed that central endobronchial biopsies provide the highest sensitivity (74%), followed by brushings brushing (61%) and washings (47%). The combination provides a diagnosis in 88% of cases.
37 When lung cancer presents with submucosal infiltration or extrinsic compression from peribronchial disease, endobronchial forceps biopsy has a lower yield (55%) than transbronchial needle aspiration (TBNA) (71%). In these situations, normal mucosal markings are often obscured and the surface is replaced with bronchial collateral vessels and firmer surface tissue, which may have to be penetrated to reach malignant cells. In addition, peribronchial tumor may be inaccessible to biopsy forceps. TBNA can be more effective if the lesion is close enough to the tracheobronchial tree to be encountered with a 1.3- to 1.5-cm-long needle.
38 Transbronchial needle aspiration (TBNA) The use of TBNA in staging lung cancer has been reported to be both sensitive and specific in diagnosing spread of cancer to lymph nodes. The overall sensitivity of TBNA for NSCLC is 78%, and the specificity is 99%.
39 The standard method of performing TBNA starts with a CT scan of the chest to guide needle aspirations toward the most involved group of lymph nodes. Lesions localized by a CT scan can be accessed with bronchoscopy by measuring the number of CT slices above or below the carina (or other airway landmarks) and placing the needle the required distance above or below the landmark corresponding to that number of CT slices.
40 It has been shown that a plateau in yield for malignancy is achieved after seven passes with the needle through a lymph node. The importance of having a qualified and experienced cytopathologist on site cannot be overemphasized. Thorough interpretation by such individuals who are available for rapid on-site evaluation has been shown to enhance yield from TBNA.
41 All samples should contain a preponderance of lymphocytes to define true nodal sampling. Specimens without lymphocytes should be deemed unsatisfactory, and the presence of respiratory epithelium should raise concerns about contamination. TBNA allows for minimally invasive sampling of the mediastinum and hilar lymph nodes and potentially avoids more invasive procedures such as mediastinoscopy, mediastinotomy, and open thoracotomy.
42 Endoscopic Ultrasound Endoscopic ultrasound (EUS) is another modality that has significantly impacted lung cancer staging, primarily due to its superior ability to sample the posterior mediastinum through the esophageal wall. Currently, EUS with fine-needle aspiration is performed using real-time ultrasound. In pooled analysis of more than 1000 patients with lung cancer and mediastinal adenopathy, EUS has a sensitivity and specificity of 84% and 99.5%, respectively
43 In patients with lung cancer who have no adenopathy seen on CT scan, EUS has been shown to sample nodes as small as 3 mm in diameter. This is useful given the high incidence of metastasis found in normal-sized lymph nodes in lung cancer.
44 Lymphatic pathways favor spread to aortopulmonary window nodes from left upper lobe tumors and to subcarinal nodes from left and right lower lobe lesions. EUS has been studied in patients with known lung cancer without enlarged mediastinal lymph nodes on CT, and it has detected mediastinal involvement (stage III or IV disease) in up to 42% of cases.
45 In addition, EUS has the advantage of being able to stage lung cancer from locations outside the mediastinum. The left lobe of the liver, a substantial part of the right lobe of the liver, and the left (but not the right) adrenal gland can be identified and sampled in 97% of patients. In addition, left pleural effusions can be visualized and sampled during an EUS procedure. EUS is increasingly being combined with endobronchial ultrasound (EBUS) for minimally invasive staging of lung cancer
46 Endobronchial Ultrasound Perhaps the greatest addition in the armamentarium for staging lung cancer is endobronchial ultrasound with fine-needle aspiration (EBUS-TBNA). EBUS-TBNA is indicated for the assessment of mediastinal and hilar lymph nodes and diagnosis of lung and mediastinal tumors.
47 It can be used to sample the highest mediastinal (station 1), the upper paratracheal (station 2R, 2L), the lower paratracheal (station 4R, 4L), the subcarinal (station 7), as well as the hilar (station 10), and the interlobar (station 11) lymph nodes. The para-aortic (station 6), aortopulmonary window or subaortic (station 5), paraesophageal (station 8), and pulmonary ligament (station 9) lymph node stations are usually not accessible by this technique.
48 Pooled analysis of nearly 1000 patients shows that EBUS-TBNA has a sensitivity and specificity of 90% and 100%, respectively. The combination of EUS and EBUS has shown better yield than either technique alone and may provide near-complete access to the mediastinum for staging, even in the radiologically normal mediastinum.
49 2015 WHO Classification of Lung Tumors
50 Histologic Type and Subtypes : Epithelial tumors 1. Adenocarcinoma a) Lepidic adenocarcinomae b) Acinar adenocarcinoma c) Papillary adenocarcinoma d) Micropapillary adenocarcinomae e) Solid adenocarcinoma f) Invasive mucinous adenocarcinomae Mixed invasive mucinous and nonmucinous adenocarcinoma
51 a) Colloid adenocarcinoma b) Fetal adenocarcinoma c) Enteric adenocarcinoma d) Minimally invasive adenocarcinoma Nonmucinous Mucinous a) Preinvasive lesions Atypical adenomatous hyperplasia Adenocarcinoma in situ Nonmucinous Mucinous
52 2. Squamous cell carcinoma Keratinizing squamous cell carcinoma Nonkeratinizing squamous cell carcinoma Basaloid squamous cell carcinoma Preinvasive lesion a) Squamous cell carcinoma in situ 3. Neuroendocrine tumors Small cell carcinoma Combined small cell carcinoma Large cell neuroendocrine carcinoma Combined large cell neuroendocrine carcinoma
53 4. Carcinoid tumors Typical carcinoid tumor Atypical carcinoid tumor 5. Preinvasive lesion Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia 6. Large cell carcinoma 7. Adenosquamous carcinoma 8. Sarcomatoid carcinomas Pleomorphic carcinoma Spindle cell carcinoma Giant cell carcinoma Carcinosarcoma Pulmonary blastoma
54 9. Other and Unclassified carcinomas Lymphoepithelioma-like carcinoma NUT carcinomae 10. Salivary gland-type tumors Mucoepidermoid carcinoma Adenoid cystic carcinoma Epithelial-myoepithelial carcinoma Pleomorphic adenoma
55 11. Papillomas Squamous cell papilloma Exophytic Inverted Glandular papilloma Mixed squamous and glandular papilloma 12. Adenomas Sclerosing pneumocytoma Alveolar adenoma Papillary adenoma Mucinous cystadenoma Mucous gland adenoma
56 Mesenchymal tumors: Pulmonary hamartoma Chondroma PEComatous tumors Lymphangioleiomyomatosis PEComa, benign Clear cell tumor PEComa, malignant Congenital peribronchial myofibroblastic tumor Diffuse pulmonary lymphangiomatosis
57 Inflammatory myofibroblastic tumor Epithelioid hemangioendothelioma Pleuropulmonary blastoma Synovial sarcoma Pulmonary artery intimal sarcoma Pulmonary myxoid sarcoma with EWSR1 CREB1 translocation Myoepithelial tumors Myoepithelioma Myoepithelial carcinoma
58 Lymphohistiocytic tumors: Extranodal marginal zone lymphomas of mucosaassociated Lymphoid tissue (MALT lymphoma) Diffuse large cell lymphoma Lymphomatoid granulomatosis Intravascular large B cell lymphoma Pulmonary Langerhans cell histiocytosis Erdheim Chester disease
59 Tumors of ectopic origin Germ cell tumors Teratoma, mature Teratoma, immature Intrapulmonary thymoma Melanoma Meningioma, NOS Metastatic tumors
60 THANK YOU
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis)
") Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
Minimally invasive adenocarcinoma. 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS)
") Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions. Alper Toker, MD
 Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions Alper Toker, MD Istanbul University, Istanbul Medical School Department of Thoracic Surgery The mediastinum is a complex anatomic
Mediastinoscopy, Mediastinotomy And Thoracoscopy For Mediastinal Lesions Alper Toker, MD Istanbul University, Istanbul Medical School Department of Thoracic Surgery The mediastinum is a complex anatomic
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
MEDIASTINAL LYMPH NODE METASTASIS IN PATIENTS WITH CLINICAL STAGE I PERIPHERAL NON-SMALL-CELL LUNG CANCER
 MEDIASTINAL LYMPH NODE METASTASIS IN PATIENTS WITH CLINICAL STAGE I PERIPHERAL NON-SMALL-CELL LUNG CANCER Tsuneyo Takizawa, MD a Masanori Terashima, MD a Teruaki Koike, MD a Hideki Akamatsu, MD a Yuzo
MEDIASTINAL LYMPH NODE METASTASIS IN PATIENTS WITH CLINICAL STAGE I PERIPHERAL NON-SMALL-CELL LUNG CANCER Tsuneyo Takizawa, MD a Masanori Terashima, MD a Teruaki Koike, MD a Hideki Akamatsu, MD a Yuzo
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
May 2017 Imaging Case of the Month. Prasad M. Panse, MD and Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, Arizona USA
 May 2017 Imaging Case of the Month Prasad M. Panse, MD and Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, Arizona USA Clinical History: A 32-year-old man presented for routine
May 2017 Imaging Case of the Month Prasad M. Panse, MD and Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, Arizona USA Clinical History: A 32-year-old man presented for routine
Basic Data. Sex:Male 31 years old Occupation: 搬家工人
 Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Bronchoscopy and endobronchial ultrasound for diagnosis and staging of lung cancer
 FRANCISCO AÉCIO ALMEIDA, MD, MS, FCCP Associate Staff Member, Director, Interventional Pulmonary Medicine Fellowship Program, Respiratory Institute, Cleveland Clinic, Cleveland, OH Bronchoscopy and endobronchial
FRANCISCO AÉCIO ALMEIDA, MD, MS, FCCP Associate Staff Member, Director, Interventional Pulmonary Medicine Fellowship Program, Respiratory Institute, Cleveland Clinic, Cleveland, OH Bronchoscopy and endobronchial
Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules
 Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Standardized transbronchial needle aspiration procedure for intrathoracic lymph node staging of non-small cell lung cancer
 Original Article on Transbronchial Needle Aspiration (TBNA) Standardized transbronchial needle aspiration procedure for intrathoracic lymph node staging of non-small cell lung cancer Xu-Ru Jin 1 *, Min
Original Article on Transbronchial Needle Aspiration (TBNA) Standardized transbronchial needle aspiration procedure for intrathoracic lymph node staging of non-small cell lung cancer Xu-Ru Jin 1 *, Min
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endobronchial ultrasound-guided transbronchial needle aspiration for mediastinal
EBUS-TBNA in PET-positive lymphadenopathies in treated cancer patients
 ORIGINAL ARTICLE LUNG IMAGING EBUS-TBNA in PET-positive lymphadenopathies in treated cancer patients Juliana Guarize 1, Monica Casiraghi 1, Stefano Donghi 1, Chiara Casadio 2, Cristina Diotti 1, Niccolò
ORIGINAL ARTICLE LUNG IMAGING EBUS-TBNA in PET-positive lymphadenopathies in treated cancer patients Juliana Guarize 1, Monica Casiraghi 1, Stefano Donghi 1, Chiara Casadio 2, Cristina Diotti 1, Niccolò
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
The cases treated with lung cancer in the hospital center xhaferr kongoli in the period time of
 The cases treated with lung cancer in the hospital center xhaferr kongoli in the period time of 13-15 Introduction: Lung cancer is one of the most common and serious types of cancer. Cancer that begins
The cases treated with lung cancer in the hospital center xhaferr kongoli in the period time of 13-15 Introduction: Lung cancer is one of the most common and serious types of cancer. Cancer that begins
Corporate Medical Policy Electromagnetic Navigation Bronchoscopy
 Corporate Medical Policy Electromagnetic Navigation Bronchoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: electromagnetic_navigation_bronchoscopy 1/2010 3/2017 3/2018 9/2017
Corporate Medical Policy Electromagnetic Navigation Bronchoscopy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: electromagnetic_navigation_bronchoscopy 1/2010 3/2017 3/2018 9/2017
Mediastinal Mysteries: What can be solved with EBUS?
 Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Endoscopic and Endobronchial Ultrasound Staging for Lung Cancer. Michael B. Wallace, MD, MPH Professor of Medicine Mayo Clinic, Jacksonville
 Endoscopic and Endobronchial Ultrasound Staging for Lung Cancer Michael B. Wallace, MD, MPH Professor of Medicine Mayo Clinic, Jacksonville Background: Lung Cancer 170,000 cases/yr in U.S. (# 1 cancer)
Endoscopic and Endobronchial Ultrasound Staging for Lung Cancer Michael B. Wallace, MD, MPH Professor of Medicine Mayo Clinic, Jacksonville Background: Lung Cancer 170,000 cases/yr in U.S. (# 1 cancer)
Sectional Anatomy Quiz II
 Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Patients with pathologically diagnosed involved mediastinal
 MINI-SYMPOSIUM ON EMERGING TECHNIQUES FOR LUNG CANCER STAGING European Trends in Preoperative and Intraoperative Nodal Staging: ESTS Guidelines P. De Leyn, MF, PhD,* D. Lardinois, MD, P. Van Schil, MD,
MINI-SYMPOSIUM ON EMERGING TECHNIQUES FOR LUNG CANCER STAGING European Trends in Preoperative and Intraoperative Nodal Staging: ESTS Guidelines P. De Leyn, MF, PhD,* D. Lardinois, MD, P. Van Schil, MD,
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP ESMO-Christie Lung Cancer Course Manchester 2017 Overview What is Endobronchial Ultrasound? Why & When Do We
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP ESMO-Christie Lung Cancer Course Manchester 2017 Overview What is Endobronchial Ultrasound? Why & When Do We
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
Uncommon Lung Tumors:
 4th World Congress of Thoracic Imaging Uncommon Lung Tumors: Exhibit Category: Thoracic Neoplasms 1 Tae Jung Kim, 1 Boda Nam, 2 Joungho Han, 1 Kyung Soo Lee Department of 1 Radiology and 2 Pathology Samsung
4th World Congress of Thoracic Imaging Uncommon Lung Tumors: Exhibit Category: Thoracic Neoplasms 1 Tae Jung Kim, 1 Boda Nam, 2 Joungho Han, 1 Kyung Soo Lee Department of 1 Radiology and 2 Pathology Samsung
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Lung Cancer: Diagnosis, Staging and Treatment
 PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Recommendations 1 For mediastinal nodal staging in patients with suspected or proven non-small-cell lung cancer
 Guideline 545 Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline, in cooperation with the
Guideline 545 Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline, in cooperation with the
A Case of Pediatric Plasma Cell Granuloma
 August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Cancer in the United States, 2004
 Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Lung Cancer Risks. Cancer in the United States, Cancer Death Rates, US The Scheme: From Nicotine Addiction to Lung Cancer
 Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Utilizing EBUS (Endobronchial Ultrasound) for Diagnosis of Lung Cancer and other Pulmonary Diseases
 for Diagnosis of Lung Cancer and other Pulmonary Diseases") Utilizing EBUS (Endobronchial Ultrasound) for Diagnosis of Lung Cancer and other Pulmonary Diseases Akintayo Sokunbi, M.D MidMichigan Hospital Midland, Michigan Objectives Discuss EBUS guided biopsy principles
Utilizing EBUS (Endobronchial Ultrasound) for Diagnosis of Lung Cancer and other Pulmonary Diseases Akintayo Sokunbi, M.D MidMichigan Hospital Midland, Michigan Objectives Discuss EBUS guided biopsy principles
GUIDELINE RECOMMENDATIONS
 European Journal of Cardio-Thoracic Surgery 48 (2015) 1 15 doi:10.1093/ejcts/ezv194 Cite this article as: Vilmann P, Frost Clementsen P, Colella S, Siemsen M, De Leyn P, Dumonceau J-M et al. Combined endobronchial
European Journal of Cardio-Thoracic Surgery 48 (2015) 1 15 doi:10.1093/ejcts/ezv194 Cite this article as: Vilmann P, Frost Clementsen P, Colella S, Siemsen M, De Leyn P, Dumonceau J-M et al. Combined endobronchial
Role of EBUS in mediastinal staging of lung cancer. -Dr. Nandakishore Baikunje
 Role of EBUS in mediastinal staging of lung cancer -Dr. Nandakishore Baikunje Overview of the seminar Introduction Endosonography to stage the mediastinum Technical aspects of EBUS-TBNA for mediastinal
Role of EBUS in mediastinal staging of lung cancer -Dr. Nandakishore Baikunje Overview of the seminar Introduction Endosonography to stage the mediastinum Technical aspects of EBUS-TBNA for mediastinal
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Pathology of Mediastinal Tumors
 SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms
SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms