David Lewin MD Medical University of South Carolina
|
|
|
- Gyles Dawson
- 6 years ago
- Views:
Transcription




1 Top 10 Advances in GI Pathology David Lewin MD Medical University of South Carolina
2 No Disclosures
3 Overview Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3) Surgical pathology (2)
4 Most Significant GI Advances arenot Presented at Pathology Meetings or Digestive Disease Week Combined meeting of AGA, AASLD, ASGE, SSAT 15,000+ attendees 4331 Posters 340 (searching for pathology ) ASCO 30,000 + attendees 21,000 abstracts 970 GI USCAP 1960 Posters 137 GI Posters 94 Liver and Pancreas Posters Journals Impact Factor NEJM: Gastroenterology: Hepatology: Gut: J. Hepatology: 7.4 Am J Hepatology: Am J Pathology: AJSP: 4.106

5
6 #10 to # 8 Imaging abstracts Toward a Optical Biopsy Threats to pathology
7
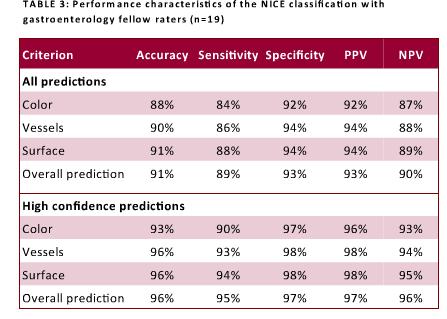
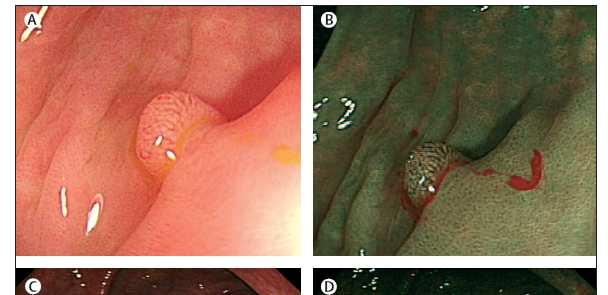
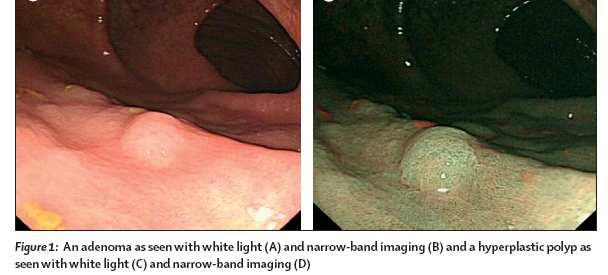
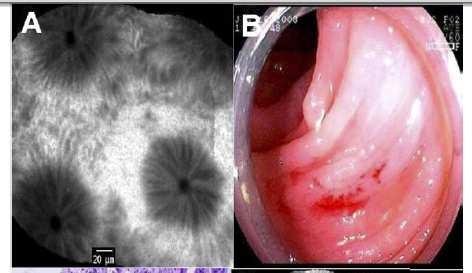
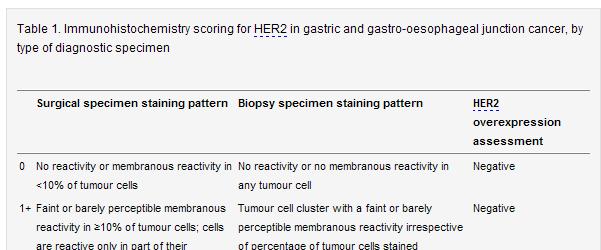
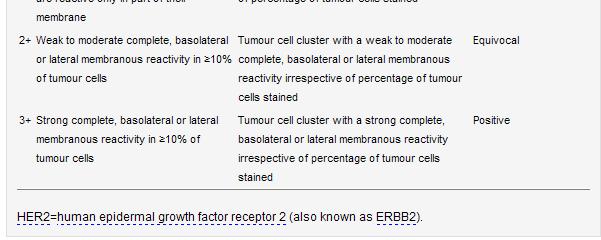
8 Narrow Band Imaging Short wavelength, narrow-bandwidth blue light Provided at a push of the button on scope Enhances mucosal detail and vascular structures Allows assessment of microvascular density Increased angiogenesis appears darker



9 Barrett Esophagus
10
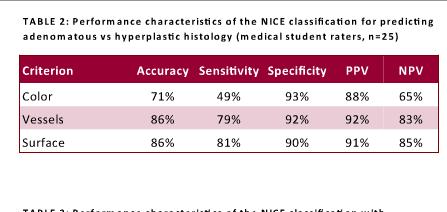
11 Results

12
13
14 Results
15

16
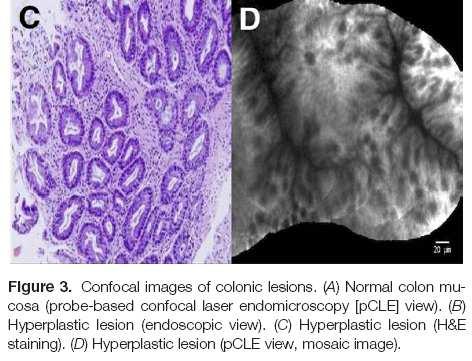
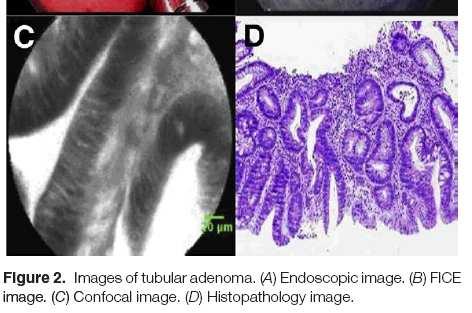
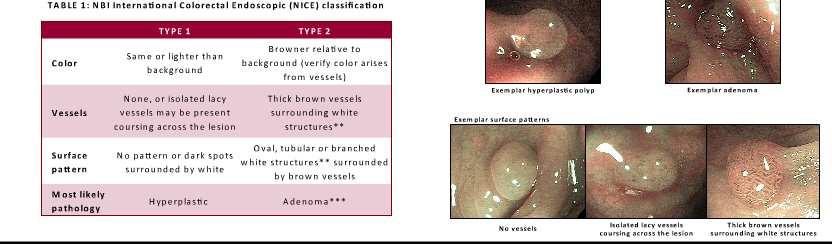
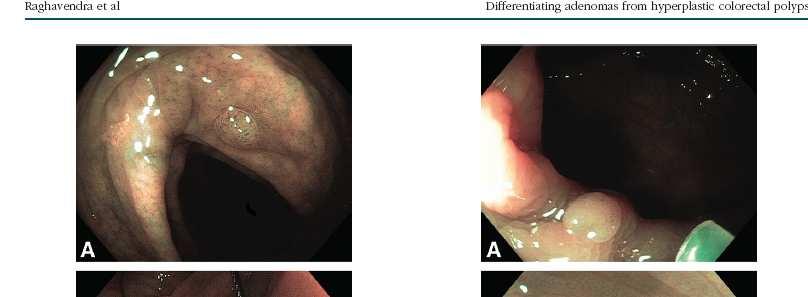
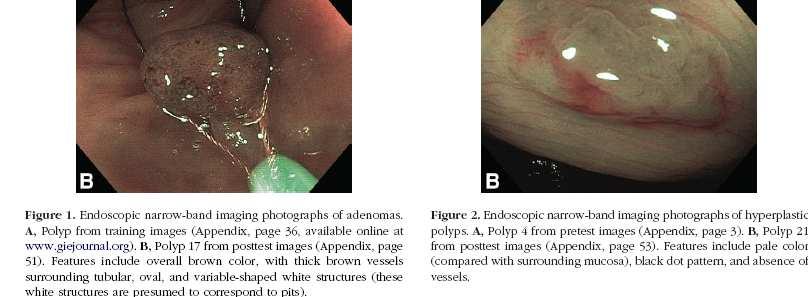
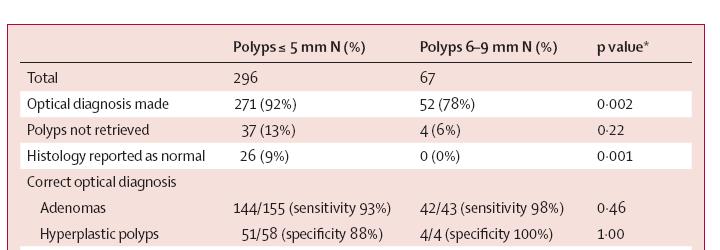
17 Hyperplastic Polyp Adenoma
18 Results GS = Gold standard Simplified = compared to histology Modified = Neoplastic = adenoma + all polyps greater than 1 cm
19 # 7 and 6 Molecular KRAS and HER2/neu Opportunities for pathology
20
21 Phase 3 trial: Cetuximab combined with Irinotecanin first-line therapy for metastatic colorectal cancer (CRYSTAL) FOLFIRI (irinotecan, fluorouracil, leucovorin) Cetuximab (Erbitux): Immunoglobulin G1 monoclonal antibody against epidermal growth factor receptor (EGFR) Subgroup analysis for KRAS mutational status 540 patients (of 1200 from initial study) 64% wild-type KRAS KRAS mutations in codons12 and 13 via PCR
22 Bottom Line For tumor response: Significant benefit in KRAS wild type tumors (p=0.3) No significant benefit for progression free survival (p=0.7) or over-all survival (p=0.44)
23


24
25 Trastuzumab: monoclonal antibody against human epidermal growth factor receptor 2 (HER2 or ERBB2) 594 pts randomized to standard chemo (capecitabine or fluorouracil + cisplatin) vs standard chemo + iv trastuzumab HER2 + by 3+ immunohistochemistry or FISH + 22% (810 of 3665 cancers)
26
27
28 # 5 to 3 Endoscopic Therapy Endoscopic resections Specimens we will receive Radiofrequency Ablation Treatment and alteration of specimens may receive NOTES (natural orifice translumenalendoscopic surgery) Future?

29 ESMD V EMR
30 Methods/ Results 145 colorectal tumors treated by ESMD 228 treated by EMR ESMD Longer procedure time (108 vs29 min) Higher en bloc resection rate (84% v 33%) Larger resection specimens (37 vs28 mm) 2 recurrences (2%) vs33 (14%) with EMR Perforation rate (6%) vs1.3% with EMR 31-34% Adenomas, 66-69% Carcinomas (sm1) sm1 = no invasion deeper than 1,000 um from muscularis mucosa

31 ESMD
32 EMD
33
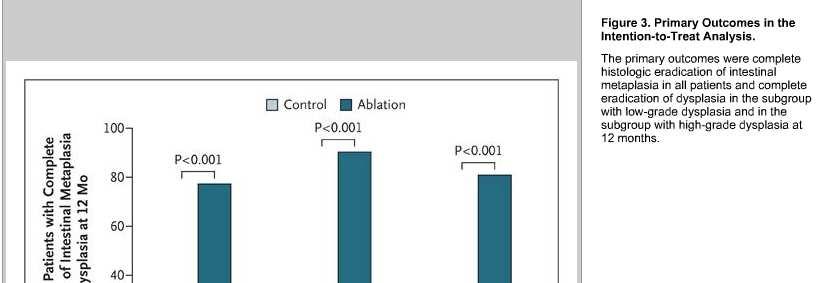
34 Methods Use of HALO (BARRX Medical) 191 eligible for review by central pathology 22 did not meet entry criteria 6 upgraded to cancer, 14 downgraded (indefor no dys), 2 negfor IM 169 met pathology criteria (LGD or HGD) 127 randomized (64 LGD, 63 HGD) 2:1 RF vssham
35
36
37 Implications A treatment modality for low grade and high grade dysplasia in BE Subsquamous intestinal metaplasia 5.1% after RF Still need screening endoscopy post RF with biopsy of the previous BE segment
38 NOTES (Natural Orifice Translumenal Endoscopic Surgery) First described in a survival porcine model in 2000 at DDW. 429 human NOTES case have been published to date 316 transvaginal, 113 transgastric Most with laparoscopic assistance DDW abstracts presented
39 Abstract Topics DDW 2011 Navigation (9 studies) Visualization of peritoneal cavity and mediastinum Closure (5 studies) Endoscopic closure of access to the peritoneal cavity Complications (2 studies) Tolerance (2 studies) Development of therapeutic interventions Cholecystectomy, appendectomy, adhesiolysis, tubal ligation, oophorectomy, gastroenterostomy Ultimate indication has not been found


40
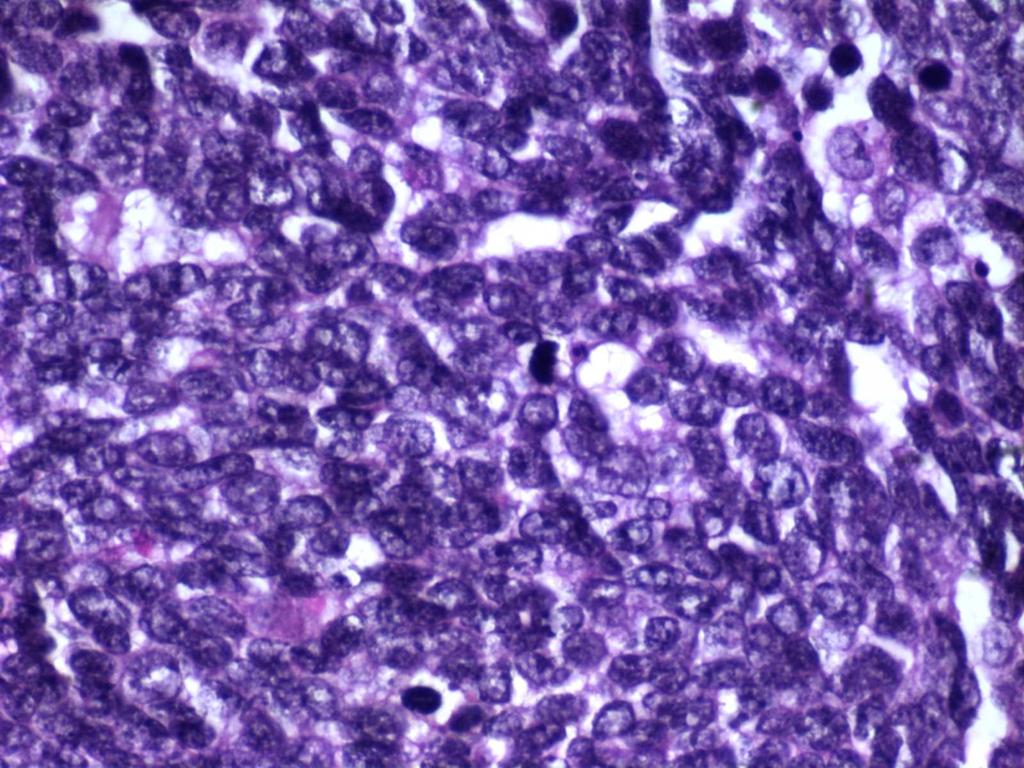
41 Top 2 Changes in pathology nomenclature and grading Neuroendocrine tumors of the gastrointestinal tract
42 New WHO 4 th edition Classification of Tumours of the Digestive System BosmanFT, et al. WHO Classification of Tumoursof the Digestive System. Lyon, France: IARC Press; WHO 1980 WHO 2000 WHO 2010 I. Carcinoid 1. Well-differentiatedendocrine tumor (WDET) 2. Well-differentiated endocrine carcinoma (WDEC) 3. Poorly differentiated endocrine carcinoma/ small cell carcinoma (PDEC) II. Mucocarcinoid III. Mixed forms carcinoidadenocarcinoma 4. Mixed exocrine-endocrine carcinoma (MEEC) 1. NET G1 (carcinoid) 2. NET G2* 3. NEC G3 a) large cell or small cell type 4. Mixed adenoneuroendocrine carcinoma (MANEC) IV. Pseudotumorlesions 5. Tumor-like lesions (TLL) 5. Hyperplastic and preneoplastic lesions NET = neuroendocrine tumor-well differentiated; NEC = neuroendocrine carcinoma-poorly differentiated;g = grade; * If Ki67 index exceeds 20%, this NET may be labeled G3
43 Neuroendocrine Tumors Histology: Well or Poorly Differentiated Mitotic Count (per 10 HPF) G1 = 2 G2 = 2-20 G3 = > 20 Immunohistochemistry: Expression of neuroendocrine markers (chromogranin or synaptophysin) Proliferative activity via Ki-67 G1 = < 2% G2 = 2 20% G3 = > 20% Stage
44
45
46
47 Modified TNM
48
49
50 Summary Top Articles/ presentations in the following areas Imaging (3) Molecular (2) Therapeutics (3) Surgical pathology (2)
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
NPQR Quality Payment Program (QPP) Measures 21_18247_LS.
 Measures 21_18247_LS.") NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Enterprise Interest Nothing to declare Update of mixed tumours of the GI tract, the pancreas and the liver Introduction to the concept of mixed tumours and clinical implication Jean-Yves SCOAZEC Surgical
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
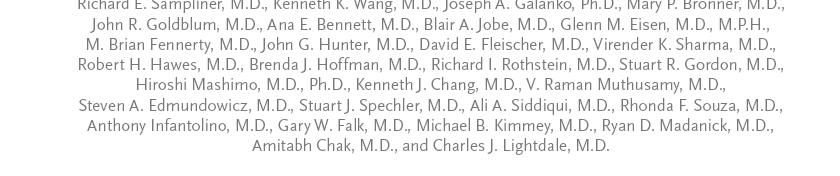
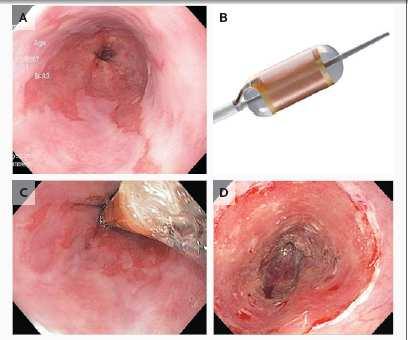
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Description of Procedure or Service. Policy. Benefits Application
 Corporate Medical Policy KRAS, NRAS, BRAF Mutation Analysis and Related File Name: Origination: Last CAP Review: Next CAP Review: Last Review: kras_nras_braf_mutation_analysis_and_related_treatment_in_metastatic_colorectal_cancer
Corporate Medical Policy KRAS, NRAS, BRAF Mutation Analysis and Related File Name: Origination: Last CAP Review: Next CAP Review: Last Review: kras_nras_braf_mutation_analysis_and_related_treatment_in_metastatic_colorectal_cancer
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Stage 4 gastric adenocarcinoma icd 10
 > Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
> Stage 4 gastric adenocarcinoma icd 10 stage iii; Carcinoma of colon, stage iv; Colon cancer metastatic to unspecified site; Hereditary nonpolyposis colon cancer; Malignant tumor of colon; Metastasis.
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Commissioning policies agreed by PCTs in Yorkshire and the Humber at Board meeting of YH SCG on December
 Commissioning policies agreed by PCTs in Yorkshire and the Humber at Board meeting of YH SCG on December 17 2010. 32/10 Imatinib for gastrointestinal stromal tumours (unresectable/metastatic) (update on
Commissioning policies agreed by PCTs in Yorkshire and the Humber at Board meeting of YH SCG on December 17 2010. 32/10 Imatinib for gastrointestinal stromal tumours (unresectable/metastatic) (update on
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
CASE REPORT. Introduction. Case Report. Kimitoshi Kubo 1, Noriko Kimura 2, Katsuhiro Mabe 1, Yusuke Nishimura 1 and Mototsugu Kato 1
 doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Pharmacy Management Drug Policy
 11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
11/13, 10/12, 11/11, 1, 6/10, Page 1 of 5 DESCRIPTION: Cetuximab is a recombinant humanized monoclonal antibody that binds specifically to the extracellular domain of the human epidermal growth factor
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading?
 Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
Editorial: Advanced endoscopic therapeutics in Barrett s neoplasia; where are we now and where are we heading? Dr. Gaius Longcroft-Wheaton MB,BS, MD, MRCP(UK), MRCP(Gastro) Consultant gastroenterologist
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
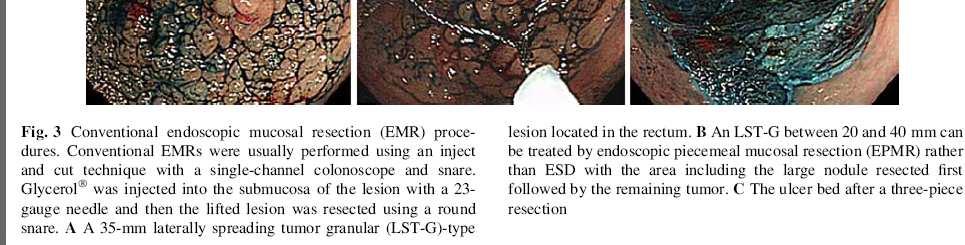
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Information Technology Solutions
 2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
of the clinical trial data for this outcome. Therefore, perc considered that the cost-effectiveness of cetuximab plus FOLFIRI would be at the higher end of the EGP s range of best estimates. Therefore,
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Name of Policy: Panitumumab, Vectibix
 Name of Policy: Panitumumab, Vectibix Policy #: 369 Latest Review Date: June 2014 Category: Pharmacology Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Panitumumab, Vectibix Policy #: 369 Latest Review Date: June 2014 Category: Pharmacology Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Clinical Policy: Cetuximab (Erbitux) Reference Number: PA.CP.PHAR.317
 Reference Number: PA.CP.PHAR.317") Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
Clinical Policy: (Erbitux) Reference Number: PA.CP.PHAR.317 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that patients
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
Objectives. Briefly summarize the current state of colorectal cancer
 Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
Disclaimer I do not have any financial conflicts to disclose. I will not be promoting any service or product. This presentation is not meant to offer medical advice and is not intended to establish a standard
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
How to stage early BE cancer - EUS or endoscopic removal?
 How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong
 Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
Application of Chromoendoscopy, NBI and AFI in Esophagus why, who, and how? Philip Chiu Associate Professor Department of Surgery, Prince of Wales Hospital The Chinese University of Hong Kong Cancer of
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Composite neuroendocrine carcinoma and squamous cell carcinoma with regional lymph node metastasis: a case report
 Fujihara et al. Journal of Medical Case Reports (2018) 12:227 https://doi.org/10.1186/s13256-018-1775-z CASE REPORT Composite neuroendocrine carcinoma and squamous cell carcinoma with regional lymph node
Fujihara et al. Journal of Medical Case Reports (2018) 12:227 https://doi.org/10.1186/s13256-018-1775-z CASE REPORT Composite neuroendocrine carcinoma and squamous cell carcinoma with regional lymph node
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Name of Policy: Natural Orifice Transluminal Endoscopic Surgery (NOTES)
") Name of Policy: Natural Orifice Transluminal Endoscopic Surgery (NOTES) Policy #: 326 Latest Review Date: March 2018 Category: Surgery Policy Grade: B Background/Definitions: As a general rule, benefits
Name of Policy: Natural Orifice Transluminal Endoscopic Surgery (NOTES) Policy #: 326 Latest Review Date: March 2018 Category: Surgery Policy Grade: B Background/Definitions: As a general rule, benefits
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Appendix 4: WHO Classification of Tumours of the pancreas 17
 S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
S3.01 The WHO histological tumour type must be recorded. CS3.01a The histological type of the tumour should be recorded based on the current WHO classification 17 (refer to Appendices 4-7). Appendix 4:
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
Colon, Rectum, and Appendix
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix. Presentation Outline. Overview Tumor Characteristics
 Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
Colon, Rectum, and Appendix 2011 Reporting Requirements and CSv02.03.02 NCCN/ASCO Treatment Guidelines by Stage FCDS 2011 Educational Webcast Series September 15, 2011 Steven Peace, CTR Presentation Outline
OVERALL CLINICAL BENEFIT
 cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
cetuximab plus FOLFIRI to convert unresectable liver metastatses to resectable, perc confirmed that neither the FIRE-3 study nor the CRYSTAL study were designed to assess resectability and, in the absence
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per