4/13/2010. Silverman, Buchanan Breast, 2003
|
|
|
- Jodie Wilkinson
- 6 years ago
- Views:
Transcription




1 Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk in invasive cancer ER negative Sorting risk in invasive cancer ER positive Lifestyle risk factors Tailoring What? Ductal carcinoma in situ Diagnosis for about 20% of all new cases Usually diagnosed by mammography t to be confused with invasive ductal carcinoma May be diagnosed by core biopsy or excisional biopsy Spans all ages and all risk factors May be multifocal or diffuse, but is usually within a single quadrant Variations--DCIS 1
2 DCIS: What is the Risk? Studies of DCIS risk have mostly looked at the risk of recurrence in the same breast When DCIS recurs, about half of the cases are DCIS, and half are invasive breast cancer When DCIS recurs, the vast majority recur in the same area of the breast where the first event took place We think that we just didn t get it all out! The risk of recurrence definitely is highest if the margins of the original biopsy have DCIS Careful pathologic review is VERY important Rule out areas of invasive cancer Check on resection margins Age Affects DCIS Recurrence in the Same Breast Silverman, Buchanan Breast, 2003 USC/VNPI DCIS Scoring Index Using the USC/VPNI Risk Index Score Size Margins Pathology Age 1point <15 mm 5/8 inch >10 mm 3/8 inch t high grade necrosis 2 points 3 points mm inch 1-9 mm.04-3/8 inch t high grade With necrosis >41mm 1.7 inch up <1mm microscopic High grade >61 years years <39 years Add up the points for each category Total is the risk rating Example: A 55 year old woman with a 12 mm DCIS, removed with margins widely clear of DCIS (more than 10 mm all around). Pathology shows moderately differentiated DCIS with comedonecrosis. Points: =6 2
3 Recur at 10 yrs Outcomes of DCIS Surgery Only by USC/VNPI Score USC/VNPI Score 4-6 USC/VNPI Score 7-9 4% 27% 63% % Invasive 0% 46% 40% Cancer Survival at 10 years 100% 97.7% 97.6% USC/VNPI Score Evidence-Based DCIS Treatment Total mastectomy: reduces risk by >95% Partial mastectomy: With good margins, risk as per USC/VPI Addition of breast radiation: reduces risk by 50% Addition of Tamoxifen: reduces risk by 25% All three surgery, radiation, Tam: reduces risk by about 75% DCIS Treatment Recommendations Mastectomy: Risk of subsequent recurrence certainly less than 5%, probably less than 2% Lumpectomy alone: May be OK for low risk women, elderly Requires careful long term surveillance Lumpectomy + radiation therapy: Younger women, higher risk women Lumpectomy + radiation therapy + hormone therapy: Highest risk women Postmenopausal women probably should consider Arimidex or Femara te: lymph nodes usually NOT sampled Invasive Breast Cancer Tailoring primary surgical treatment: Mastectomy an option for any patient Partial mastectomy an option for those with Tumors under 5 cm before or after chemo inflammatory breast cancer Acceptable cosmetic outcome Radiation therapy after surgery: High risk of local failure on chest wall after Mx Younger women with partial mastectomy radiation: lupus, scleroderma, refusal 3
4 Adjuvant Therapy Tailoring Risk of distant recurrence: prognostic factors Size and node status Progesterone receptor expression Proliferation rate, differentiation Her2 status OncotypeDx Mammaprint Adjuvant Therapy Tailoring What treatment will work for this tumor: predictive factors Estrogen and progesterone receptor status Her2 status Proliferation index; differentiation Oncotype?Mammaprint Adjuvant Therapy Tailoring Host factors: Age of patient Comorbid illnesses factored with risk of recurrence, so ask which disease is patient likely to die from? Comorbid illnesses predicting risk of side effects from treatment and/or long term toxicity from treatment 4
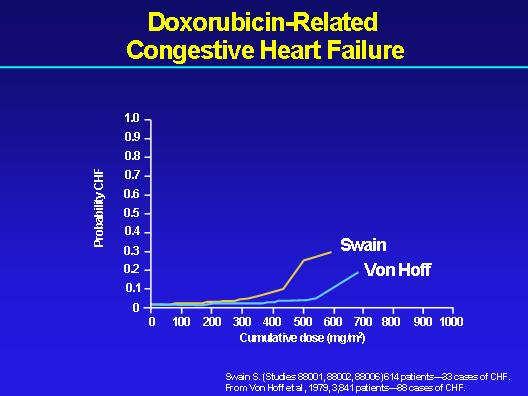
5 HER2 STATUS HER2 STATUS Positive Negative Positive Negative Comorbid? Triple Negative Breast Cancer Best available current adjuvant therapy is anthracycline based, usually also taxane based, chemotherapy Triple negative is more common in women under 50; therapy usually given to them Higher response to chemo vs ER +, but generally also worse relapse rate Older women less overall benefit, need to tailor for these women due to risks Breast Chemotherapy and Comorbidities Serial clinical trials suggest: Anthracycline containing chemo is superior to non- anthracycline therapy (maybe one exception) Addition of taxane (Taxol, Taxotere) is also superior to non-taxane treatment But: Taxanes cause neuropathy, sometimes irreversible Anthracyclines can cause CHF 5

6 6

7 Tailoring to ER Negative, Her2 Negative Breast CA High risk for CHF: Combination of taxane and cyclophosphamide Older: CMF (cyclophosphamide, methotrexate, fluorouracil) High risk for neuropathy: Anthracycline, fluorouracil, cyclophosphamide Neither: Anthracycline, cyclophosphamide, taxane ER Negative, Her2 Positive Her2 is a cell surface growth factor receptor that is highly overexpressed in 20-25% 25% of invasive breast cancer Most tumors also ER negative Rapidly growing; most chemo sensitive group Probably most sensitive to anthracycline rx Herceptin trastuzumab is a monoclonal antibody to the external receptor that has a high level of antitumor activity in vitro Trastuzumab may be added to adjuvant chemotherapy the standard is one year Trastuzumab Risks Short term is well tolerated only only occasional infusion reactions INCREASES the risk of CHF when given after anthracyclines Mechanism is unknown Often reversible longer longer term results not yet known Cuts the risk of relapse by 50%! 7
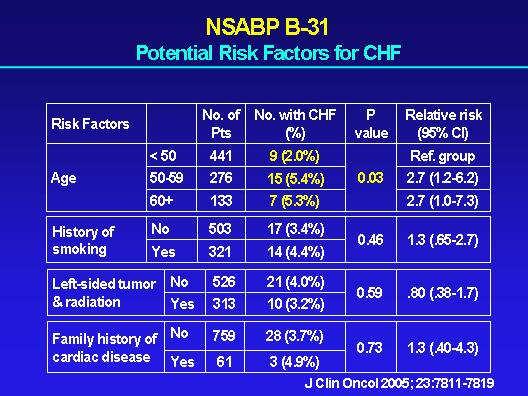
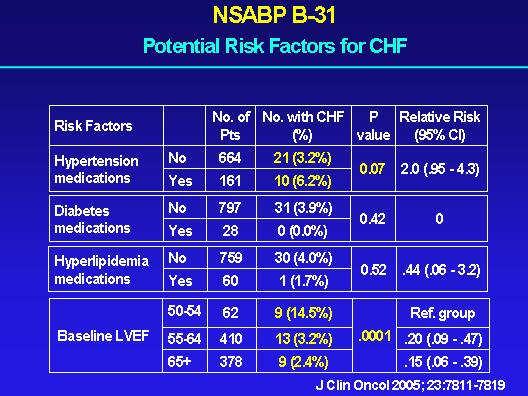
8 Tailoring Chemo/Trastuzumab Low Risk premenopausal women Anthracycline + taxane + Herceptin Overall relapse risk reduction about 80% Hypertension Substitute non-anthracycline regimen Taxane and Herceptin Older women n-anthracycline regimen + Herceptin Very meticulous monitoring of LVEF HER2 STATUS Positive Negative Comorbid? Comorbid? Relapse Risk in ER + Breast Ca High relapse risk? Positive lymph nodes Younger age High risk by Oncotype Dx Risk applies to node neg and node positive Low risk = no benefit from chemo??high risk by Mammaprint 8
9 Prognostic/Predictive Factors in Breast Cancer: Oncotype R 21-gene RT-PCR assay used for node-negative, negative, ER positive (lower risk) tumors predicts risk of metastases over 10 yrs Predicts responsiveness to chemotherapy for the high scoring tumors, no response for lowest scores HT Only High relapse risk? Chemo + HT Comorbid HT + mod chemo Tailoring Hormone Therapy Postmenopausal women Aromatase inhibitors are treatment of choice Superior in randomized trials Arimidex, Femara, Aromasin Effect greatest in oldest women Tamoxifen second choice Intolerance of aromatase inhibitors Risks: thrombotic events, ca uterus Some experts mix these two regimens Both treatments are for five years Tailoring Hormone Therapy Premenopausal women Lose menses due to chemotherapy Aromatase inhibitors for five years Tamoxifen for five years loss of menses Tamoxifen for five years Lupron or other GNRH agonist for five years Add either Tamoxifen or aromatase inhibitor 9
10 Adjuvant Therapy Outcomes Example: 64 yo woman with 3 cm ER+ tumor, but 10 nodes positive Risk of relapse in 10 yrs is 82%! Risk of relapse with chemo + hormones reduced by 45% to only 37% Example: 35 yo woman with 1.5 cm ER+ Her2 + cancer with 3 nodes Risk of relapse in 10yrs is 75% Risk reduction with chemo, hormones, and Herceptin is about 65%, resulting in 10% risk What About BRCA Positive Women? Risk of ca is quite high: up to 80% lifetime BRCA1: high rates triple negative cancer BRCA2: more varied types Most women are younger, so the treatment is more aggressive Bilateral mastectomy much more frequent when diagnosed with breast cancer Oophorectomy should be considered: may provide base for hormone therapy New Directions for BRCA patients: PARP inhibitors Chemo induces DNA break PARP and BRCA are both DNA repair proteins Cancer cells in BRCA patients have no BRCA function at all; their normal cells have half the BRCA, but that works OK If you inhibit PARP in a BRCA cancer cell, then you can t repair DNA damage; the normal cells survive Add a DNA damaging agent like cisplatin or carboplatin, and higher rates of cell death occur Risk Reducing Lifestyle Changes? Diet Everybody asks, nobody knows Two large randomized trials of lowering sat fat and/or increasing vegetables had opposite outcomes in women after breast cancer WHI results also negative for cohort with ca breast Alcohol: does increase risk of getting breast cancer Obesity: also increases risk Exercise: decreases risk of getting breast cancer 10
11 Improving Outcomes: Lifestyle Interventions after Breast Cancer LACE Study: Kaiser Permanente 1897 women after diagnosis, self-reported alcohol use (90% wine!) Compared to no alcohol, even amounts as low as ½ drink/day increased risk of Recurrence 34% Death due to breast cancer 51% Stronger effect seen in postmenopausal women 51% recurrence increase and and overweight/obese women 58% increase Yikes! Controversial, but we know that alcohol consumption increases risk of getting breast cancer Needs other large studies of women to look at this Improving Outcomes: Effects of Overweight/Obesity Danish Study: based on national health records of 18,967 women with breast ca For BMI greater than 25 Recurrence risk increased 42-46% 46% Mortality due to breast cancer increased 26-38% Worst risk groups: older postmenopausal women, BMI over 30 also associated with larger cancers, more + nodes Cannot sort out other variables, as this study from registries, but effect is important Analysis of E1199 study looking at African American outcomes showed that obesity was the ONLY risk factor that explained any outcome differences Awaiting results: Exercise Retrospective studies comparing BrCa survivors to their friends consistently show reduced risk due to exercise, up to 50% Observational studies Nurses, WHI, cardiac studies also show consistent reduction in BC risk at all ages Many studies showing feasibility of exercise programs after BC NO large randomized trials Summing Up Breast cancer is heterogeneous with respect to risk and sensitivity to therapy Patient choices particularly important for primary surgical/radiation therapy, especially for DCIS Comorbid conditions, particularly age and hypertension, alter treatment choices Predictive tests such as Oncotype also alter treatment choice for ER + tumors Lifestyle factors alter outcomes 11
Breast Cancer. Excess Estrogen Exposure. Alcohol use + Pytoestrogens? Abortion. Infertility treatment?
 Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer Breast Cancer Excess Estrogen Exposure Nulliparity or late pregnancy + Early menarche + Late menopause + Cystic ovarian disease + External estrogens exposure + Breast Cancer Excess Estrogen
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Evolving Practices in Breast Cancer Management
 Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Evolving Practices in Breast Cancer Management The Georgia Tumor Registrars Association 2016 Priscilla R. Strom, MD, FACS Objectives 1. understand newer indications for neoadjuvant treatment 2. understand
Systemic Treatment of Breast Cancer. Hormone Therapy and Chemotherapy, Curative and Palliative
 Systemic Treatment of Breast Cancer Hormone Therapy and Chemotherapy, Curative and Palliative Systemic Therapy Invasive breast cancers Two forms Curative Palliative Curative Systemic Therapy Adjuvant Therapy
Systemic Treatment of Breast Cancer Hormone Therapy and Chemotherapy, Curative and Palliative Systemic Therapy Invasive breast cancers Two forms Curative Palliative Curative Systemic Therapy Adjuvant Therapy
My Personalized Breast Cancer Worksheet
 My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer. Breast Cancer. Established breast cancer risk factors. Established breast cancer risk factors. Cancer incidence.
 Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Update from the 29th Annual San Antonio Breast Cancer Symposium
 Update from the 29th Annual San Antonio Breast Cancer Symposium The San Antonio Breast Cancer Symposium is one of the most important breast cancer conferences. Approximately 8,000 physicians, oncologists,
Update from the 29th Annual San Antonio Breast Cancer Symposium The San Antonio Breast Cancer Symposium is one of the most important breast cancer conferences. Approximately 8,000 physicians, oncologists,
Breast Cancer Breast Managed Clinical Network
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
Breast Cancer & Personalized Medicine
 Principles of Drug Development and Discovery Breast Cancer & Personalized Medicine Grace Leung, Efrat Shalom-Berensohn, Felipe Castro, Kate Burke-Wallace and Shiv Gaglani Breast Cancer... 2 nd most common
Principles of Drug Development and Discovery Breast Cancer & Personalized Medicine Grace Leung, Efrat Shalom-Berensohn, Felipe Castro, Kate Burke-Wallace and Shiv Gaglani Breast Cancer... 2 nd most common
Advances in Neoadjuvant and Adjuvant Therapy for Breast Cancer
 Advances in Neo and Adjuvant Therapy for Breast Cancer Nicole Kounalakis, MD, and Christina Finlayson, MD OVERVIEW Systemic therapy for breast cancer is evolving rapidly. The medical treatment of cancer
Advances in Neo and Adjuvant Therapy for Breast Cancer Nicole Kounalakis, MD, and Christina Finlayson, MD OVERVIEW Systemic therapy for breast cancer is evolving rapidly. The medical treatment of cancer
Breast cancer remains the most common malignancy and the second leading. cause of cancer mortality in women in the United States.
 Dr. Andrew Seidman s Commentary I. Breast Cancer Overview Breast cancer remains the most common malignancy and the second leading cause of cancer mortality in women in the United States. The following
Dr. Andrew Seidman s Commentary I. Breast Cancer Overview Breast cancer remains the most common malignancy and the second leading cause of cancer mortality in women in the United States. The following
Clinical Management Guideline for Breast Cancer
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Ideal neo-adjuvant Chemotherapy in breast ca. Dr Khanyile Department of Medical Oncology, University of Pretoria
 Ideal neo-adjuvant Chemotherapy in breast ca Dr Khanyile Department of Medical Oncology, University of Pretoria When is neo-adjuvant Chemo required? Locally advanced breast ca: - Breast conservative surgery
Ideal neo-adjuvant Chemotherapy in breast ca Dr Khanyile Department of Medical Oncology, University of Pretoria When is neo-adjuvant Chemo required? Locally advanced breast ca: - Breast conservative surgery
Highlights: 2008 San Antonio Breast Cancer Symposium
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/conference-coverage/highlights-2008-san-antonio-breast-cancersymposium/4099/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/conference-coverage/highlights-2008-san-antonio-breast-cancersymposium/4099/
BREAST CANCER BREAST CANCER
 BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Breast Cancer Treatment
 Breast Cancer Treatment Treatment 2 aspects 1. Treatment of the breast itself: Local Treatment 2. Treatment of the whole body = Systemic treatment Local Treatment Surgery +/- Radiation Usually: a. Breast
Breast Cancer Treatment Treatment 2 aspects 1. Treatment of the breast itself: Local Treatment 2. Treatment of the whole body = Systemic treatment Local Treatment Surgery +/- Radiation Usually: a. Breast
Intro to Cancer Therapeutics
 An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Presenter: Dr. Suman Rao May 13, 2016
 Presenter: Dr. Suman Rao May 13, 2016 1 2010 Breast Cancer Estimates 207,090 NEW CASES 4% Melanoma of Skin 2% Thyroid 31% Breast 13% Lung & Bronchus 2% Pancreas 11% Colon & Rectum 4% Ovary 6% Uterus 3%
Presenter: Dr. Suman Rao May 13, 2016 1 2010 Breast Cancer Estimates 207,090 NEW CASES 4% Melanoma of Skin 2% Thyroid 31% Breast 13% Lung & Bronchus 2% Pancreas 11% Colon & Rectum 4% Ovary 6% Uterus 3%
Treatment Options for Breast Cancer in Low- and Middle-Income Countries: Adjuvant and Metastatic Systemic Therapy
 Women s Empowerment Cancer Advocacy Network (WE CAN) Conference Bucharest, Romania October 2015 Treatment Options for Breast Cancer in Low- and Middle-Income Countries: Adjuvant and Metastatic Systemic
Women s Empowerment Cancer Advocacy Network (WE CAN) Conference Bucharest, Romania October 2015 Treatment Options for Breast Cancer in Low- and Middle-Income Countries: Adjuvant and Metastatic Systemic
Clinico- Pathological Features And Out Come Of Triple Negative Breast Cancer
 Clinico- Pathological Features And Out Come Of Triple Negative Breast Cancer Dr. HassanAli Al-Khirsani, MBChB, CABM, F.I.C.M.S AL-Sadder teaching hospital, oncology unit Dr. Nasser Ghaly Yousif, MBChB,G.P.
Clinico- Pathological Features And Out Come Of Triple Negative Breast Cancer Dr. HassanAli Al-Khirsani, MBChB, CABM, F.I.C.M.S AL-Sadder teaching hospital, oncology unit Dr. Nasser Ghaly Yousif, MBChB,G.P.
Breast Cancer? Breast cancer is the most common. What s New in. Janet s Case
 Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Focus on CME at The University of Calgary What s New in Breast Cancer? Theresa Trotter, MD, FRCPC Breast cancer is the most common malignancy affecting women in Canada, accounting for almost a third of
Breast Cancer Statistics
 1 in 8 Breast Cancer Statistics Incidence Mortality Prevalence 2 Breast Cancer Incidence Breast Cancer Mortality Breast Cancer Prevalence ~$100,000 Female Breast Anatomy Breasts consist mainly of fatty
1 in 8 Breast Cancer Statistics Incidence Mortality Prevalence 2 Breast Cancer Incidence Breast Cancer Mortality Breast Cancer Prevalence ~$100,000 Female Breast Anatomy Breasts consist mainly of fatty
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Section: Genetic Testing Last Reviewed Date: March Policy No: 42 Effective Date: June 1, 2014
 Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Breast cancer staging update. Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director
 Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Breast cancer staging update Ekaterini Tsiapali, MD, FACS MedStar Regional Breast Program Site Director 1 1 Review of the AJCC 8 th edition breast cancer staging Review of genomic assays as stage modifiers
Toxicities of Chemotherapy Regimens used in Early Breast Cancer
 Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
SFMC Breast Cancer Site Study: 2011
 SFMC Breast Cancer Site Study: 2011 Introduction Breast cancer is the most frequently diagnosed cancer among American women, except for skin cancers. It is the second leading cause of cancer death in women,
SFMC Breast Cancer Site Study: 2011 Introduction Breast cancer is the most frequently diagnosed cancer among American women, except for skin cancers. It is the second leading cause of cancer death in women,
Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology
 BREAST CANCER 24 Breast Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by William J. Gradishar, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern
BREAST CANCER 24 Breast Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by William J. Gradishar, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
ESMO Breast Cancer Preceptorship Singapore November Special Issues in Treatment of Young Women with Breast Cancer
 ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
Gene Expression Profiling for Managing Breast Cancer Treatment. Policy Specific Section: Medical Necessity and Investigational / Experimental
 Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
Medical Policy Gene Expression Profiling for Managing Breast Cancer Treatment Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date:
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
HEALTH CARE DISPARITIES. Bhuvana Ramaswamy MD MRCP The Ohio State University Comprehensive Cancer Center
 HEALTH CARE DISPARITIES Bhuvana Ramaswamy MD MRCP The Ohio State University Comprehensive Cancer Center Goals Understand the epidemiology of breast cancer Understand the broad management of breast cancer
HEALTH CARE DISPARITIES Bhuvana Ramaswamy MD MRCP The Ohio State University Comprehensive Cancer Center Goals Understand the epidemiology of breast cancer Understand the broad management of breast cancer
Molecular Characterization of Breast Cancer: The Clinical Significance
 Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Oncotype DX MM /01/2008. HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
 of Service: Office") Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
TRANSPARENCY COMMITTEE OPINION. 15 February 2006
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 February 2006 Taxotere 20 mg, concentrate and solvent for solution for infusion B/1 vial of Taxotere and 1 vial
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 February 2006 Taxotere 20 mg, concentrate and solvent for solution for infusion B/1 vial of Taxotere and 1 vial
Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS
 The Oncologist Understanding and Treating Triple-Negative Breast Cancer Across the Age Spectrum Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS The University of North Carolina Lineberger Cancer
The Oncologist Understanding and Treating Triple-Negative Breast Cancer Across the Age Spectrum Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS The University of North Carolina Lineberger Cancer
Gynecologic Care for Breast Cancer Survivors. Case
 Gynecologic Care for Breast Cancer Survivors Mindy Goldman, MD Clinical Professor Dept. of Ob/Gyn and Reproductive Sciences Director, Women s Cancer Care Program, UCSF Breast Care Center and Women s Health
Gynecologic Care for Breast Cancer Survivors Mindy Goldman, MD Clinical Professor Dept. of Ob/Gyn and Reproductive Sciences Director, Women s Cancer Care Program, UCSF Breast Care Center and Women s Health
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
BREAST CANCER. Dawn Hershman, MD MS. Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center.
 BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
PHARMACOGENETICS OF BREAST CANCER
 PHARMACOGENETICS OF BREAST CANCER MALGORZATA JAREMKO, PhD Mount Sinai School of Medicine, Department of Genetics and Genomic Sciences Outlines Breast cancer therapeutic situation Pharmacogenetics of antiestrogen
PHARMACOGENETICS OF BREAST CANCER MALGORZATA JAREMKO, PhD Mount Sinai School of Medicine, Department of Genetics and Genomic Sciences Outlines Breast cancer therapeutic situation Pharmacogenetics of antiestrogen
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST CANCER PATHOLOGY
 BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
BREAST CANCER PATHOLOGY FACT SHEET Version 4, Aug 2013 This fact sheet was produced by Breast Cancer Network Australia with input from The Royal College of Pathologists of Australasia I m a nurse and know
Patient Guide to Breast Cancer Surgery and Treatment
 Patient Guide to Breast Cancer Surgery and Treatment An educational guide prepared by Genomic Health This is your booklet. It is designed to help you through this challenging time. Use it as a guide during
Patient Guide to Breast Cancer Surgery and Treatment An educational guide prepared by Genomic Health This is your booklet. It is designed to help you through this challenging time. Use it as a guide during
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer.
 Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Retrospective analysis to determine the use of tissue genomic analysis to predict the risk of recurrence in early stage invasive breast cancer. Goal of the study: 1.To assess whether patients at Truman
Breast Cancer FAQ. How does Breast Cancer spread? Breast cancer spreads by invading into
 FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
FAQ Breast Cancer What is Breast Cancer? Breast Cancer is the second leading cause of cancer deaths in women today (second to lung cancer) and is the most common cancer among women excluding non-melanoma
Latest News in Breast Cancer Research
 Latest News in Breast Cancer Research Highlights from the 2011 San Antonio Breast Cancer Symposium www.cancercare.org This special edition of the CancerCare Connect booklet series highlights cutting-edge
Latest News in Breast Cancer Research Highlights from the 2011 San Antonio Breast Cancer Symposium www.cancercare.org This special edition of the CancerCare Connect booklet series highlights cutting-edge
Ca in situ e ormonoterapia. Discussant : LORENZA MARINO
 Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
Update from the 25th Annual San Antonio Breast Cancer Symposium December 11 14, 2002
 Update from the 25th Annual San Antonio Breast Cancer Symposium December 11 14, 2002 Nearly 5,000 physicians, oncologists, radiologists, epidemiologists, basic scientists, and breast cancer advocates from
Update from the 25th Annual San Antonio Breast Cancer Symposium December 11 14, 2002 Nearly 5,000 physicians, oncologists, radiologists, epidemiologists, basic scientists, and breast cancer advocates from
Understanding and Optimizing Treatment of Triple Negative Breast Cancer
 Understanding and Optimizing Treatment of Triple Negative Breast Cancer Edith Peterson Mitchell, MD, FACP Clinical Professor of Medicine and Medical Oncology Program Leader, Gastrointestinal Oncology Department
Understanding and Optimizing Treatment of Triple Negative Breast Cancer Edith Peterson Mitchell, MD, FACP Clinical Professor of Medicine and Medical Oncology Program Leader, Gastrointestinal Oncology Department
The TAILORx Trial: A review of the data and implications for practice
 The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Current Status and Future Development of Tools for Prognosis and Prediction - USA
 Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
SYSTEMIC THERAPY OPTIONS FOR BREAST CANCER IN 2014
 SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the
SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Educator Navigation Guide
 Decoding Breast Cancer Virtual Lab Educator Navigation Guide Decoding Cancer Nav Guide 2 Introduction In this virtual lab, students test tissue samples from different patients with breast cancer in order
Decoding Breast Cancer Virtual Lab Educator Navigation Guide Decoding Cancer Nav Guide 2 Introduction In this virtual lab, students test tissue samples from different patients with breast cancer in order
Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey
 MYERS et al. ORIGINAL ARTICLE Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey J.A. Myers MD FRCPC, G.
MYERS et al. ORIGINAL ARTICLE Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey J.A. Myers MD FRCPC, G.
Chapter 5: Epidemiology of MBC Challenges with Population-Based Statistics
 Chapter 5: Epidemiology of MBC Challenges with Population-Based Statistics Musa Mayer 1 1 AdvancedBC.org, Abstract To advocate most effectively for a population of patients, they must be accurately described
Chapter 5: Epidemiology of MBC Challenges with Population-Based Statistics Musa Mayer 1 1 AdvancedBC.org, Abstract To advocate most effectively for a population of patients, they must be accurately described
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC
 Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Philippine Society of Medical Oncology
 Philippine Society of Medical Oncology Unit 1418, 14/F, orth Tower, Cathedral Heights Bldg., St. Luke s Medical Center E. Rodriguez Sr. Avenue, Quezon City 1099, Philippines Telefax: (632) 721-9326/ 723-0101
Philippine Society of Medical Oncology Unit 1418, 14/F, orth Tower, Cathedral Heights Bldg., St. Luke s Medical Center E. Rodriguez Sr. Avenue, Quezon City 1099, Philippines Telefax: (632) 721-9326/ 723-0101
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Breast Cancer Treatment, Outcomes and Recent Advances. Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School
 Breast Cancer Treatment, Outcomes and Recent Advances Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School National Statistics 1 in 8 women in the U.S. (12-13%) will
Breast Cancer Treatment, Outcomes and Recent Advances Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School National Statistics 1 in 8 women in the U.S. (12-13%) will
American Society of Clinical Oncology June , New Orleans
 American Society of Clinical Oncology June 5-8 2004, New Orleans The 2004 annual meeting of the American Society of Clinical Oncology (ASCO) was held June 5 8 in New Orleans, Louisiana. This conference
American Society of Clinical Oncology June 5-8 2004, New Orleans The 2004 annual meeting of the American Society of Clinical Oncology (ASCO) was held June 5 8 in New Orleans, Louisiana. This conference
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Key Words. Adjuvant therapy Breast cancer Taxanes Anthracyclines
 The Oncologist Mayo Clinic Hematology/Oncology Reviews Adjuvant Therapy for Breast Cancer: Recommendations for Management Based on Consensus Review and Recent Clinical Trials BETTY A. MINCEY, a,b FRANCES
The Oncologist Mayo Clinic Hematology/Oncology Reviews Adjuvant Therapy for Breast Cancer: Recommendations for Management Based on Consensus Review and Recent Clinical Trials BETTY A. MINCEY, a,b FRANCES
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Breast Carcinoma at Coast Province General Hospital- Mombasa Kenya
 10 Breast Carcinoma at Coast Province General Hospital- Mombasa Kenya G.G.O. Calleb MBChB MMed FCS-ECSA Consultant Surgeon Coast Province General Hospital P O Box 91176 Mombasa-Kenya. Background: The aim
10 Breast Carcinoma at Coast Province General Hospital- Mombasa Kenya G.G.O. Calleb MBChB MMed FCS-ECSA Consultant Surgeon Coast Province General Hospital P O Box 91176 Mombasa-Kenya. Background: The aim
Ductal Carcinoma in Situ (DCIS)
") Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /