News You Can Use: Recent Studies that Changed My Practice
|
|
|
- Everett Foster
- 6 years ago
- Views:
Transcription

1 News You Can Use: Recent Studies that Changed My Practice Melissa McNeil, MD, MPH Chief, Section of Women s Health Division of General Internal Medicine University of Pittsburgh Sarah Tilstra, MD, MSc University of Pittsburgh

2 Objectives To identify practice changing studies that have the potential to change our management of women immediately To review the merits of these studies and to evaluate their significance To articulate how we might incorporate the results of these studies in the management of our women patients
3 Case 1 Elinor is a 55 year old woman you are seeing in the office for a well woman visit. She asks you if she should be taking either calcium supplements or increasing calcium in her diet. What do you tell her?

4 The News Calcium intake and risk of fracture: systematic review. Bolland et al. BMJ September 29; 351 Calcium intake and bone mineral density: a systematic review and meta-analysis. Tai et al. BMJ 2015 September 29; 351

5 Background: Recommended Intake A calcium intake of mg/day has been recommended for older individuals to both treat and prevent osteoporosis Average intake in the diet of older people in Western countries around mg/dl day Therefore in order to achieve the recommended calcium intake either an increase in dietary consumption or calcium supplements are required

6 Background: Adverse Effects Recently concerns about the safety of increasing calcium intake have been raised: Increase in cardiovascular events Kidney stones Constipation Admission to the hospital for GE side effects The minor benefit in fracture risk attributed to calcium supplementation coupled with an increasing awareness of these risks have called into question the risk/benefit profile of calcium supplements
 and if so, whether effects are similar to those of calcium")
7 Objectives of the Two Studies Bolland et al: To examine the evidence underpinning recommendations to increase calcium intake through dietary sources or calcium supplements to prevent fractures Tai et al: To determine whether increasing calcium intake from dietary sources affects bone mineral density (BMD) and if so, whether effects are similar to those of calcium supplements

8 Study 1: Relationship of Calcium Intake and Fracture Calcium intake and risk of fracture: systematic review. Bolland et al. BMJ September 29; 351
9 Methods: Calcium and Fracture Risk Authors undertook a systematic review of RCTs and observational studies of calcium intake and fracture risk to examine the evidence underpinning recommendations to increase calcium intake as a means of preventing fractures Included trials: RCTs or cohort studies of dietary calcium, milk or dairy intake, or calcium supplements (with or without D) Fracture is the endpoint Participants >age 45
10 Results: Dietary Sources of Calcium RCTs: Only 2 studies with limited data No conclusions could be drawn Cohort Studies: 50 publications, 44 studies 14/22 studies reported no relation between calcium intake and total fracture risk 17/21 studies reported no relation between calcium intake and hip fracture 7/8 studies reported no relation between calcium intake and vertebral fracture Thus 43 of the 58 (74%) reported no association between dietary calcium intake and fracture outcome
11 Results: Calcium Supplements Randomized Controlled Trials 26 RCTs (n=69, 107) of calcium supplements that reported fracture outcomes 14 calcium monotherapy 8 CaD 4 were multi-arm or factorial Study details 20 trials used a calcium dose of > 1000 mg/day 21 were in individuals living in the community 15 had a duration of three or more years In 16 studies the mean age of participants was > 70 years In 10/19 studies that reported baseline intake the level was <800

12 Fig 1 Random effects models of effect of calcium supplements on risk of total fracture. Mark J Bolland et al. BMJ 2015;351:bmj.h by British Medical Journal Publishing Group

13 Fig 2 Random effects models of effect of calcium supplements on risk of hip fracture. Mark J Bolland et al. BMJ 2015;351:bmj.h by British Medical Journal Publishing Group

14 Fig 3 Random effects models of effect of calcium supplements on risk of vertebral fracture. Mark J Bolland et al. BMJ 2015;351:bmj.h by British Medical Journal Publishing Group
15 Summary: Impact of Increasing Dietary Calcium on Fracture Risk There is insufficient evidence to assess the effect of increasing dietary calcium on fracture risk 42 cohort studies assessed the relationship between dietary calcium and fracture risk Greater than 75% of analyses found no benefit Most studies did not report reduced risk of fracture in individuals with the recommended 1200 mg/d of calcium intake Thus observational trials do not support a hypothesis of dietary calcium deficiency
16 Summary: Impact of Increasing Calcium Supplementation on Fracture Risk In 26 RCTs, calcium supplementation reduced the risk of total fx by 11% and vertebral fx by 14% The results, however, were not consistent In particular, the largest trials with the lowest risk of bias showed no reduction Only one trial in frail elderly women in residential care with low dietary calcium intake/ low vitamin D showed significant reductions in fracture risk

17 Study 2: Impact of Dietary Calcium Supplementation on BMD Calcium intake and bone mineral density: a systematic review and meta-analysis. Tai et al. BMJ 2015 September 29; 351
 to determine : If increasing intake from the diet has effects on BMD And if")
18 Methods: Calcium and BMD Authors undertook a systematic review and metaanalysis of randomized controlled trials with BMD as an endpoint to determine if the recommendations to increase calcium intake to prevent osteoporosis are supported Included trials of dietary calcium or calcium supplementation in older adults (>50) to determine : If increasing intake from the diet has effects on BMD And if it is similar to the effects of calcium supplement
19 Eligible Trials of Calcium Supplementation Trial Characteristics Dietary Ca Source (n=15) Ca Supplements (n=51) Agent Studied: Number (%) Number (%) Ca Monotherapy 11 (73) 36 (71) Ca with vitamin D 4 (27) 13 (25) Multi arm with both 0 2 (4) Calcium dose > 1000mg/d 6 (40) 34 (67) Calcium dose < 500 mg/d 2 (13) 7 (14) Duration < 2 years 15(100) 37 (73) Duration > 3 years 0 13 (25) Community living 15 (100) 45 (88) Mostly women 13 (87) 48 (94) Mean age > 70 years 2 (13) 18 (35) Baseline Ca < 800mg/d 9/13 (69) 26/39 (67)
20 Analysis of RCTs of Dietary Calcium Time Point Studies Number BMD Change P Value Lumbar ( ) ( ) Femoral ( ) ( ) <0.001 Total Hip ( ) ( ) <0.001 Total Body ( ) ( ) <0.001
21 Analysis of RCTs of Supplemental Calcium Time Point Studies Number BMD Change P Value Lumbar ( ) < ( ),0.001 Femoral ( ) < ( ) <0.001 Total Hip ( ) ( ) <0.001 Total Body ( ) < ( ) <0.001
22 Summary of Results on BMD Increasing calcium intake from the diet slightly increased BMD by % over two years except at the forearm Calcium supplements increased BMD by % at all sites and at all time points In the RCTs of both dietary calcium and calcium supplements, the increase was present by one year but there were no further increases over time There was no difference in increase in BMD if: Vitamin D was added Calcium supplementation > or < 1000 mg/d Calcium supplemention < or > 500 mg/d Baseline dietary supplementation < or > 800 mg/d
23 Impact These results suggest that widespread untargeted use of either dietary calcium or calcium supplements in older individuals is unlikely to result in meaningful reduction in the incidence of fractures or improvement in bone mineral density

24 Case 2 She says, OK, no real benefit to increasing my calcium. But what about vitamin D? What do you tell her?


25 The News Hansen KE et al. Treatment of vitamin D insufficiency in postmenopausal women; A randomized clinical trial. JAMA Internal Medicine 2015; 176(10):
, bone mineral density (BMD), and muscle fitness in postmenopausal women with Vitamin D")
26 Objective The goal of this study was to evaluate the effects of high dose and low dose cholecalciferol on 1 year changes in Total Fractional Calcium Absorption(TFCA), bone mineral density (BMD), and muscle fitness in postmenopausal women with Vitamin D insufficiency (VDI)
D level less than 30 ng/ml Approximately 75% of postmenopausal US women have levels below that")
27 Background Low vitamin D levels reduce the TFCA leading to secondary hyperparathyroidism and decreased BMD VDI is currently defined as a serum 25(OH)D level less than 30 ng/ml Approximately 75% of postmenopausal US women have levels below that target
28 Methods This was a double-blind placebo-controlled RCT of postmenopausal women < 75 years with 25(OH)D levels of ng/ml Women were randomized to either: High dose cholecalciferol (loading dose of 50,000 IU/d for 15 days and then 50,000 every 15 days) 800 IU capsule of cholecalciferol every day Outcomes were assessed at one year and included laboratory testing, functional assessment, and clinical outcomes

29 Results Calcium absorption increased 1% (10 g/dl) in the high dose arm but decreased 2% in the low dose arm No difference between the high dose and low dose supplementation groups in BMD scores at any site, muscle mass, functional assessments such as the timed Up and Go or five sit-to stand test scores There were also no differences in falls, physical activity, or other functional status
30 Summary Neither low dose or high dose vitamin D supplementation had any impact on clinical outcomes in women less than 75 years of age
31 Impact This study does not support current recommendations to maintain serum 25(OH)D levels above 30 ng/ml. The IOM recommendations of 25(OH)D levels 20 ng/ml appear to be appropriate and the widespread testing for and supplementation of 25(OH)D levels below 30 ng/ml should be reconsidered.

32 Case 3 Marianne is a 60 year old woman who comes to you for advice. She received a letter from her radiologist telling her that she has increased breast density and that she should talk to her primary care physician to determine if any more testing is needed. What will you tell her?


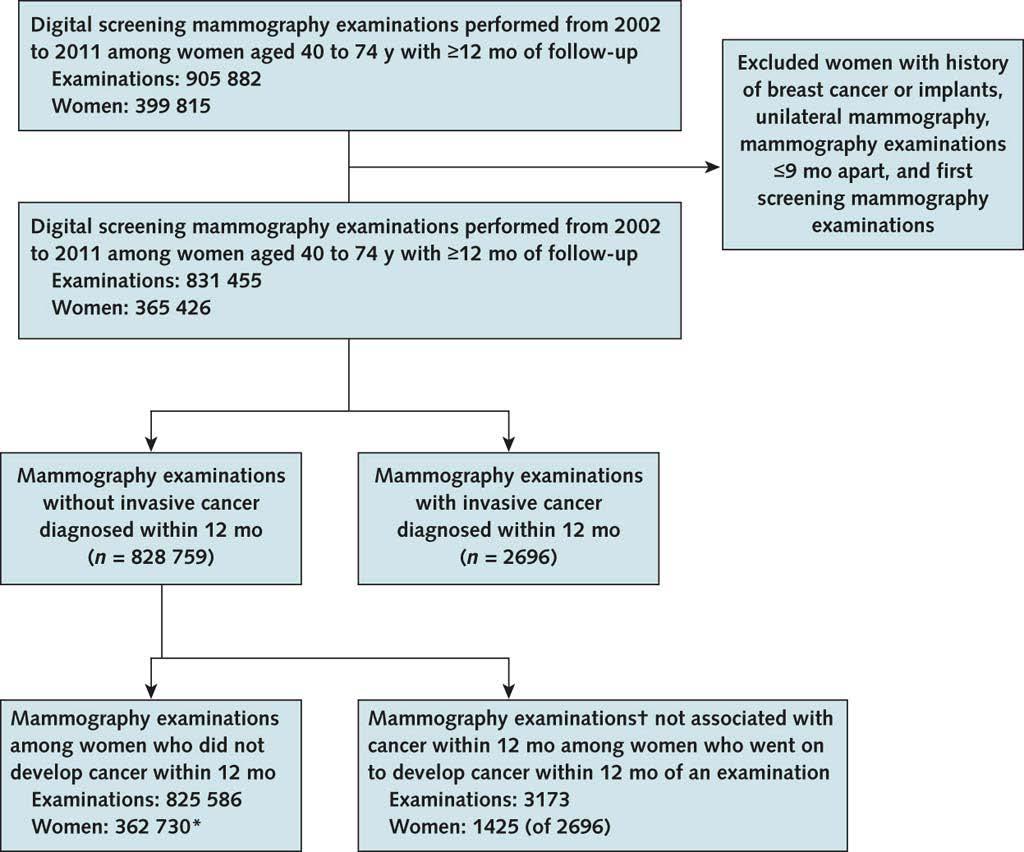
33 The News Kerlikowske K et al. Identifying women with dense breasts at high risk for interval cancer. 2015: Annals of Internal Medicine. 163(10)

34 Background Breast cancer advocates in many states have lobbied for patient notification about increased breast density because It is a marker of increased risk The sensitivity of mammograms is decreased false negative rate varies up to 10 fold across the categories of breast density 40% of women aged 40 to 74 years have dense breasts (defined as heterogeneously or extremely dense)


35 Background Different professional organizations have differing recommendations: ACOG: recommends against supplemental screening USPSTF and the ACS: state that there is insufficient information to recommend for or against supplemental screening American College of Radiology: suggests that supplemental ultrasound evaluation could be considered. Despite the lack of data and absence of consensus, 24 states have now required that patients with increased breast density be notified of their increased risk and suggest that they discuss additional screening with their providers.

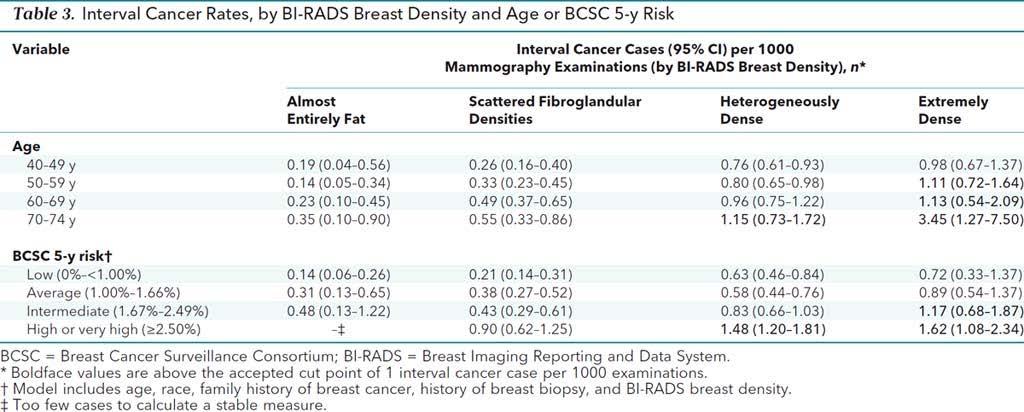
36 Objective The goal of this study was to determine which patients with increased breast density are associated with high interval cancer rates and thus would benefit from supplemental screening
37 Methods Data from the Breast Cancer Surveillance Consortium (BCSC) mammography registries were analyzed Women aged aged 40 to 74 years Who underwent digital screening mammography Between 2002 and 2011 An interval cancer rate greater than 1 case per 1000 mammograms was considered to be unacceptable performance Interval cancer rates were analyzed with different predictive scenarios including: breast density alone, breast density modified by age, and breast density modified by 5 year calculated BCSC breast cancer risk
38 Methods
39 Results
40 Results
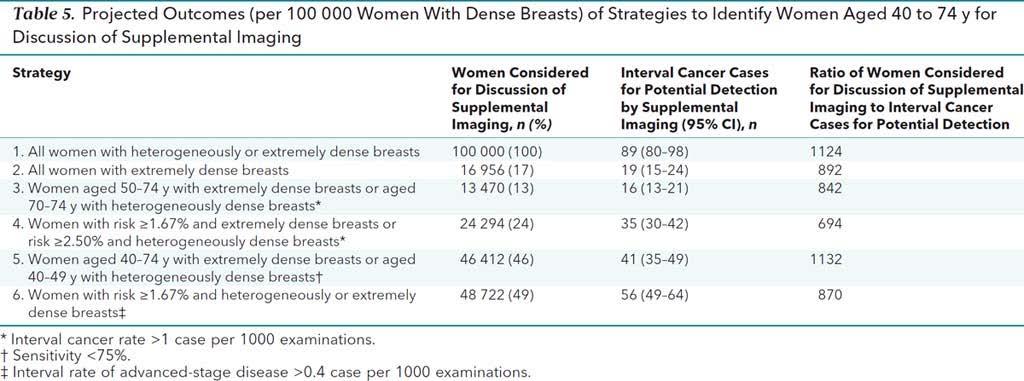
41 Summary About half of women with heterogeneously dense breasts or extremely dense breasts were at low to average 5 year breast cancer risks (0% to 1.66%). Interval cancer rates greater than 1 case per 1000 mammography examinations were observed in women: With extremely dense breasts and a 5 year cancer rate of >1.67% With heterogeneously dense breasts and a 5 year cancer rate of >2.5% These two groups represented only 24% of women with dense breasts suggesting that the majority of women with dense breasts are not at risk for increased interval cancer detection
42 Impact Increased breast density alone should not prompt additional supplemental imaging. The most important prognostic factor identified to date to help determine which patients with increased breast density are at risk for interval cancers is the 5 year BCSC breast cancer risk. Physicians should calculate individual breast cancer risks for all patients and use this information in counseling patients about decision making about alternative breast cancer screening strategies.
43 Case 4 Karen presents to you for a well woman visit. She is 42 years old. She asks you if she should begin breast cancer screening. She has no family history of breast cancer and no prior history of breast biopsies. She is an average risk patient for breast cancer. What do you tell her?

44 The News Oeffinger KC et al. Breast cancer screening for women at average risk 2015 guideline update from the American Cancer Society. JAMA. 2015; 314(15):
 commissioned a systematic review of the breast cancer screening literature taking into account the quality of the")
45 Background Currently the guidelines for breast cancer screening vary among professional organizations causing women and providers much uncertainty about what to recommend In response to new evidence from long-term followup data of screening trials, the American Cancer Society (ACS) commissioned a systematic review of the breast cancer screening literature taking into account the quality of the evidence about the balance of benefits and harms

46 Methods The ACS assembled an interdisciplinary group of experts and tasked them with developing guidelines for average risk women Guidelines were developed and graded: A strong recommendation is meant to convey that benefits > harms Qualified recommendations suggest that there is clear evidence of benefit but less certainty about either the balance of benefits and harms or about patients values and preferences (which, when considered, could lead to different decisions by different patients). Critical outcomes were considered to be prevention of breast cancer deaths, quality of life years gained by screening, life expectancy, false positives, overdiagnosis, and overtreatment Breast cancer characteristics at diagnosis and short and long term emotional effects such as anxiety and depression were considered important but not critical outcomes. A total of 10 RCTs, 22 cohort studies, and 13 case control studies were considered
47 Recommendation 1: Screening Mammography Should Begin at Age 45 (Strong) This recommendation was based on analyzing breast cancer incidence and mortality in 5 year intervals for women between 40 and 50; previous screening trials had clustered outcomes in 10 year age increment The five year risk of breast cancer among women 40 to 44 (0.6%) is less than that in women aged 45 to 49 (0.9%) and women aged 50 to 54 (1.1%) The risk of breast cancer mortality reduction is similarly different with a reduction of 18% in women 40 to 44 and 32% in women 45 to 49 They further qualify this recommendation by stating that all women should have the opportunity to begin screening at age 40 if they so desire

48 Results: Breast Cancer Burden by Age at Diagnosis
49 Recommendation 2: Women aged 45 to 54 should be screened annually (Qualified) Screening interval is important to reduce the diagnosis of interval cancers that appear clinically between screening examinations Data reviewed suggested that in women greater than age 50 few interval cancers were detected; in contrast, in women in their 40s the rate of interval cancers was 40% of the control group incidence rate in the first 12 months after a normal screening examination. It is unclear if this difference is age related or influenced by menopausal state and several studies have suggested that menopausal state is the more important factor.
50 Recommendation 3: After age 55 Biannual Mammography is Recommended (Qualified) The benefits of annual screening are reduced after the menopausal transition; most women will be post menopausal by age 55 More frequent screening over a lifetime carries an increased risk of false positives Balancing risks and benefits 55 is the recommended age at which to transition to biannual screening
51 Recommendation 4: Women should continue screening mammography as long as they have a life expectancy of 10 years (Qualified) Breast cancer incidence continues to increase until age 80, and 26% of breast cancer deaths are attributed to a diagnosis after age 74 For women who are healthy and have a life expectancy greater than 10 years, decisions should be individualized
52 Recommendation 5: The ACS does not recommend clinical breast examinations (CBE) for breast cancer screening (Qualified). The ACS based this recommendation on the fact that there were no studies demonstrating a benefit of CBE in addition to mammography They also cited moderate quality evidence that CBE increases false positive examinations
53 Limitations and Cautions Most of the screening trials began before 2000 and Used only film mammography and Had different breast cancer treatment regimens Thus the long term follow up information may not represent the impact of screening and breast cancer treatment today The ACS also included observational cohorts in its data analysis which the USPSTF does not include because of the inherent risk of bias in cohort studies Patient preferences may vary from individual to individual and the ACS recognizes that different patients may have a different weighing of risks and benefits.
54 Impact The new guidelines are helpful in offering an evidenced based review of newer literature and framing the benefits of screening in the context of harms. It must be remembered that these guidelines refer to women of average breast cancer risk and offer a rational approach to screening in this population of women.

55 Case 5 Karen is still not convinced. She asks you if there is any data to support that less is more and that the reduction in frequency of screening will be safe? What do you tell her?

56 The News Harding C et al. Breast cancer screening, incidence, and mortality across US counties. JAMA Internal Medicine. 2015; 175(9):

57 Background The goal of breast cancer screening is to reduce breast cancer mortality presumably by detecting breast cancers earlier in their course of disease If this is the case, there should be both an increase in the detection of smaller cancers and because of this a decrease in the detection of larger, poor prognosis cancers Since mammography rates vary widely across the United States, associations can be drawn between screening and breast cancer size, incidence, and mortality.

58 Objective Local data on rates of mammography screening and breast cancer diagnosis are available for approximately one-fourth of the US population. These data were used to examine the associations between rates of modern screening mammography and the incidence of breast cancer, mortality from breast cancer, and tumor size
59 Methods US counties reporting breast cancer screening and mortality to the Surveillance, Epidemiology and End Results (SEER) Cancer Registries were analyzed Initial screening took place from January 1 to December 21, 2000 Women over 40 were included in the analysis and no upper age limit was imposed Over 95% of the cancer diagnoses (n=53,207) had 10 years of follow up at the time of final analysis Screening rates varied from 39.1% to 77.8%; breast cancer incidence and breast cancer mortality by county were correlated to the baseline mammography use
 Despite an increase in breast cancer diagnosis with increased screening rates, there was no decrease in breast cancer mortality (RR 1.")
60 Results An increase of 10% in the rate of screening was associated with an increase in breast cancer diagnosis (RR 1.16: 95% CI ) Despite an increase in breast cancer diagnosis with increased screening rates, there was no decrease in breast cancer mortality (RR 1.01: 95% CI )
61 Results Screening was associated with an increase in tumors <2 cm in size but not in larger breast cancers

62 Limitations These results are correlations and thus are subject to inherent biases. It is possible that different regions have different breast cancer incidences and that areas with higher breast cancer rates have higher screening rates. It is also possible that women with higher risks of breast cancer request more screening.
63 Summary The most straightforward explanation for this finding of more small tumors but no mortality difference is over-diagnosis of clinically irrelevant tumors which would increase incidence but not impact mortality.
64 Impact Increased breast cancer screening is not necessarily associated with better outcomes. Data such as these are informative in considering current recommendations for the frequency of mammography and the importance of individualized recommendations based on breast cancer risk assessment.

65 Case 6 Janet is a 65 year old woman who presents for her annual wellness exam. She has been post-menopausal on HT for 12 years. Previous attempts to wean her off have failed. She received a letter in the mail from her insurance company telling her that her hormones would no longer be covered as they are very dangerous, and asks you about stopping them. She has no PMH except for wellcontrolled HTN

66 The News The North American Menopause Society statement on continuing use of systemic hormone therapy after age 65. Menopause 2015 Jul; 22:693
 for women who are affected by vasomotor symptoms past age 65 strictly")
67 Background Oral and transdermal estrogens were placed on the Beers list of potentially inappropriate medications (PIMs) in 2003 Physicians have been reluctant to continue hormone therapy (HT) for women who are affected by vasomotor symptoms past age 65 strictly because of age
68 Background Many quality accrediting and reporting programs are using the list of PIMs as an outcome measure for physicians and health plans THUS physicians are withholding these medications insurance companies are not paying for them and patient access is further compromised Two studies in 2015 confirm that the duration of vasomotor symptoms has previously been underestimated and is now thought to last well into the 6 th and 7 th decade for some women

69 Objective To update the 2012 North American Menopause Society position statement, specifically regarding the use of hormone therapy in healthy women with moderate to severe vasomotor symptoms

70 Methods Expert consensus statement from the North American Menopause Society; no further details provided
71 Recommendations It is acceptable for a healthy woman to continue HT with the lowest effective dose after the age of 60 if she is being treated for persistent moderate to severe vasomotor symptoms or osteoporosis and has no other adequate treatment options The benefits of vasomotor symptom management must outweigh the risks of HT for the patient, and that this decision must be made jointly between the patient and her physician
72 Recommendations Women should be counseled about the risks of HT including increased VTE, stroke, breast cancer risk The risks of continuing HT should be evaluated annually as women age and risk factors change HT should not be stopped on the basis of age alone

73 Cautions The risks of HT over age 60 remain real and there is limited data in women on HT above age 70 to guide further recommendations While HT was placed on the Beers list 13 years ago in the midst of the WHI controversy, it remains there even after review in 2012 Despite the wiliness of physicians to prescribe HT to patients, more and more health plans are limiting financial coverage of these medications to patients, especially > age 65
74 Impact The continuation of use of HT in women over 60 for vasomotor symptoms or severe osteoporosis seems acceptable but remains an ongoing conversation between patient and physician and should prompt an annual reassessment of the risks and benefits.
75 Take Home Messages Widespread untargeted use of either dietary calcium or calcium supplements in older individuals is unlikely to result in meaningful reduction in the incidence of fractures Widespread testing for and supplementation of 25(OH)D levels below 30 ng/ml should be reconsidered Increased breast density alone should not prompt additional supplemental imaging; the most important prognostic factor identified to date to help determine which patients with increased breast density are at risk for interval cancers is the 5 year BCSC breast cancer risk

76 Take Home Messages The new ACS guidelines are helpful in offering an evidenced based review of newer literature and framing the benefits of screening in the context of harms Increased breast cancer screening is not necessarily associated with better outcomes and emphasize the importance of individualized recommendations based on breast cancer risk assessment The continuation of use of HT in women over 60 for vasomotor symptoms or severe osteoporosis seems acceptable but remains an ongoing conversation between patient and physician and should prompt an annual reassessment of the risks and benefits

77
10.2 Summary of the Votes and Considerations for Policy
 CEPAC Voting and Policy Implications Summary Supplemental Screening for Women with Dense Breast Tissue December 13, 2013 The last CEPAC meeting addressed the comparative clinical effectiveness and value
CEPAC Voting and Policy Implications Summary Supplemental Screening for Women with Dense Breast Tissue December 13, 2013 The last CEPAC meeting addressed the comparative clinical effectiveness and value
SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016
 Guidelines for Breast Cancer Screening: An Update SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016 Robert A. Smith, PhD Cancer Control Department American Cancer Society Atlanta, GA I have
Guidelines for Breast Cancer Screening: An Update SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016 Robert A. Smith, PhD Cancer Control Department American Cancer Society Atlanta, GA I have
5/24/16. Current Issues in Breast Cancer Screening. Breast cancer screening guidelines. Outline
 Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016
 Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016 FACT Breast Cancer Screening Saves Lives Since 1990, screening
Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016 FACT Breast Cancer Screening Saves Lives Since 1990, screening
OVERVIEW WOMEN S HEALTH: YEAR IN REVIEW
 OVERVIEW WOMEN S HEALTH: YEAR IN REVIEW Judith Walsh, MD, MPH Professor of Medicine UCSF Update in Women s Health for SGIM Drs. Mary Beattie and Pam Charney Review of literature from March, 2008 through
OVERVIEW WOMEN S HEALTH: YEAR IN REVIEW Judith Walsh, MD, MPH Professor of Medicine UCSF Update in Women s Health for SGIM Drs. Mary Beattie and Pam Charney Review of literature from March, 2008 through
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
3/21/11 Tabar et al Lancet 2003;361:
 1 2 3 Tabar et al Lancet 2003;361:1405-1410 4 Tabar et al Lancet 2003;361:1405-1410 Tabar Rad Clin NA 2000;38:625-652, via R. Edward Hendrick, PhD, U. Colorado 5 6 7 8 Screening 40-49 50-59 60-69 Interval
1 2 3 Tabar et al Lancet 2003;361:1405-1410 4 Tabar et al Lancet 2003;361:1405-1410 Tabar Rad Clin NA 2000;38:625-652, via R. Edward Hendrick, PhD, U. Colorado 5 6 7 8 Screening 40-49 50-59 60-69 Interval
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Osteoporosis Update DR. SYLVIE OUELLETTE RHEUMATOLOGIST
 Osteoporosis Update DR. SYLVIE OUELLETTE RHEUMATOLOGIST Disclosures! Speaker programs! AbbVie, Amgen! Research! Amgen, Novartis! Education/ conference support! Amgen, Roche! Advisory Boards! AbbVie, Amgen,
Osteoporosis Update DR. SYLVIE OUELLETTE RHEUMATOLOGIST Disclosures! Speaker programs! AbbVie, Amgen! Research! Amgen, Novartis! Education/ conference support! Amgen, Roche! Advisory Boards! AbbVie, Amgen,
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
The U.S. Preventive Services Task Force (USPSTF) CLINICAL GUIDELINE
 CLINICAL GUIDELINE") Annals of Internal Medicine CLINICAL GUIDELINE Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement Albert L. Siu, MD, MSPH, on behalf of the U.S. Preventive Services
Annals of Internal Medicine CLINICAL GUIDELINE Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement Albert L. Siu, MD, MSPH, on behalf of the U.S. Preventive Services
Current Strategies in the Detection of Breast Cancer. Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF
 Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow
 Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2017 2/2018 2/2017 Description of Procedure or Service Vitamin D,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2017 2/2018 2/2017 Description of Procedure or Service Vitamin D,
Breast Cancer Screening
 Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Calcium and Cancer Prevention and Treatment
 Calcium and Cancer Prevention and Treatment By: Corrine VanDeMaele and Lindsay Wexler Calcium - Ca - Ca++ Most abundant mineral in human body Functions: Supports structure of bone and teeth Muscle contraction
Calcium and Cancer Prevention and Treatment By: Corrine VanDeMaele and Lindsay Wexler Calcium - Ca - Ca++ Most abundant mineral in human body Functions: Supports structure of bone and teeth Muscle contraction
Update on vitamin D. J Chris Gallagher Professor of Medicine and Endocrinology Creighton University Omaha,Nebraska USA
 Update on vitamin D J Chris Gallagher Professor of Medicine and Endocrinology Creighton University Omaha,Nebraska 68131 USA Cali, Colombia 2016 definitions DRIs are the recommended dietary reference intakes
Update on vitamin D J Chris Gallagher Professor of Medicine and Endocrinology Creighton University Omaha,Nebraska 68131 USA Cali, Colombia 2016 definitions DRIs are the recommended dietary reference intakes
Controversies in Breast Cancer Screening
 Controversies in Breast Cancer Screening Arash Naeim, MD PhD Associate Professor of Medicine Divisions of Hematology-Oncology and Geriatric Medicine David Geffen School of Medicine University of California,
Controversies in Breast Cancer Screening Arash Naeim, MD PhD Associate Professor of Medicine Divisions of Hematology-Oncology and Geriatric Medicine David Geffen School of Medicine University of California,
Tissue Breast Density
 Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Tissue Breast Density Reporting breast density within the letter to the patient is now mandated by VA law. Therefore, this website has been established by Peninsula Radiological Associates (PRA), the radiologists
Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals
 Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals Literature Review (January 2009) Hormone Therapy for Women Women's Health
Hormones and Healthy Bones Joint Project of National Osteoporosis Foundation and Association of Reproductive Health Professionals Literature Review (January 2009) Hormone Therapy for Women Women's Health
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2018 2/2019 2/2018 Description of Procedure or Service Vitamin D,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testing_serum_vitamin_d_levels 9/2015 2/2018 2/2019 2/2018 Description of Procedure or Service Vitamin D,
Screening Mammograms: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Screening Mammography Policy and Politics. Kevin L. Piggott, MD, MPH August 29, 2015
 Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Breast Cancer Screening September 21, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
FIRST DO NO HARM: AN EBM ODYSSEY. Cathleen Colón-Emeric, MD, MHS Geriatrics, Department of Medicine Durham VA GRECC
 FIRST DO NO HARM: AN EBM ODYSSEY Cathleen Colón-Emeric, MD, MHS Geriatrics, Department of Medicine Durham VA GRECC colon001@mc.duke.edu 919 660-7517 Learning Objectives 1. Describe the types of studies
FIRST DO NO HARM: AN EBM ODYSSEY Cathleen Colón-Emeric, MD, MHS Geriatrics, Department of Medicine Durham VA GRECC colon001@mc.duke.edu 919 660-7517 Learning Objectives 1. Describe the types of studies
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Breast Cancer Screening for Women at Average Risk
 1/51 Special Communication October 20, 2015 Breast Cancer Screening for Women at Average Risk 2015 Guideline Update From the American Cancer Society 1 2 3 Kevin C. Oeffinger, MD ; Elizabeth T. H. Fontham,
1/51 Special Communication October 20, 2015 Breast Cancer Screening for Women at Average Risk 2015 Guideline Update From the American Cancer Society 1 2 3 Kevin C. Oeffinger, MD ; Elizabeth T. H. Fontham,
Vitamin D for the Prevention of Osteoporotic Fractures
 TITLE: Vitamin D for the Prevention of Osteoporotic Fractures AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Vitamin D for the Prevention of Osteoporotic Fractures AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
Coordinator of Post Professional Programs Texas Woman's University 1
 OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
OSTEOPOROSIS Update 2007-2008 April 26, 2008 How much of our BMD is under our control (vs. genetics)? 1 2 Genetic effects on bone loss: longitudinal twin study (Makovey, 2007) Peak BMD is under genetic
ADVANCES IN WOMEN S HEALTH: A CRITICAL REVIEW OF THE YEAR S MOST IMPORTANT PAPERS
 ADVANCES IN WOMEN S HEALTH: A CRITICAL REVIEW OF THE YEAR S MOST IMPORTANT PAPERS Judith Walsh, MD, MPH Professor of Medicine Division of General Internal Medicine UCSF Women s Health Center of Excellence
ADVANCES IN WOMEN S HEALTH: A CRITICAL REVIEW OF THE YEAR S MOST IMPORTANT PAPERS Judith Walsh, MD, MPH Professor of Medicine Division of General Internal Medicine UCSF Women s Health Center of Excellence
BONE HEALTH BASICS. Promoting Healthy Bones: Sorting Out the Science. Learning Objectives. Guest Speaker
 Copyright 11 by the Preventive Cardiovascular Nurses Association Promoting Healthy Bones: Sorting Out the Science Guest Speaker Robert P. Heaney, MD, FACP, FASN Professor and Professor of Medicine Creighton
Copyright 11 by the Preventive Cardiovascular Nurses Association Promoting Healthy Bones: Sorting Out the Science Guest Speaker Robert P. Heaney, MD, FACP, FASN Professor and Professor of Medicine Creighton
Shared Decision Making in Breast and Prostate Cancer Screening. An Update and a Patient-Centered Approach. Sharon K. Hull, MD, MPH July, 2017
 Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer
 Ontario Health Technology Assessment Series 2007; Vol. 7, No. 1 Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer An Evidence-Based Analysis January 2007 Medical Advisory
Ontario Health Technology Assessment Series 2007; Vol. 7, No. 1 Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer An Evidence-Based Analysis January 2007 Medical Advisory
RALOXIFENE Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA Is the request for the prevention (risk reduction) of breast cancer?
 of breast cancer?") Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Calcium intake and risk of fracture: systematic review
 open access Calcium intake and risk of fracture: systematic review Mark J Bolland, 1 William Leung, 2 Vicky Tai, 1 Sonja Bastin, 3 Greg D Gamble, 1 Andrew Grey, 1 Ian R Reid 1 1 Department of Medicine,
open access Calcium intake and risk of fracture: systematic review Mark J Bolland, 1 William Leung, 2 Vicky Tai, 1 Sonja Bastin, 3 Greg D Gamble, 1 Andrew Grey, 1 Ian R Reid 1 1 Department of Medicine,
BREAST CANCER SCREENING IS A CHOICE
 BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
Osteodensitometry in primary and secondary osteoporosis
 Osteodensitometry in primary and secondary osteoporosis Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG) Research question The main goal of the present research was the assessment
Osteodensitometry in primary and secondary osteoporosis Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen (IQWiG) Research question The main goal of the present research was the assessment
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium and Vitamin D Supplementation is an Ineffective Strategy for the Prevention of Fractures in Older People
 Calcium and Vitamin D Supplementation is an Ineffective Strategy for the Prevention of Fractures in Older People For the Motion: Professor Roger Francis, Institute for Ageing and Health, Newcastle University,
Calcium and Vitamin D Supplementation is an Ineffective Strategy for the Prevention of Fractures in Older People For the Motion: Professor Roger Francis, Institute for Ageing and Health, Newcastle University,
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
GENERAL COMMENTS. The Task Force Process Should be Fully Open, Balanced and Transparent
 December 9, 2013 Submitted Electronically United States Preventive Services Task Force c/o Dr. Robert Cosby Agency for Healthcare Research and Quality 540 Gaither Road Rockville, MD 20850 RE: USPSTF Draft
December 9, 2013 Submitted Electronically United States Preventive Services Task Force c/o Dr. Robert Cosby Agency for Healthcare Research and Quality 540 Gaither Road Rockville, MD 20850 RE: USPSTF Draft
Advances in Breast Cancer Diagnosis and Treatment. Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015
 Advances in Breast Cancer Diagnosis and Treatment Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015 Advances in Breast Cancer Diagnosis and Treatment Recommendations
Advances in Breast Cancer Diagnosis and Treatment Heidi Memmel, MD FACS Surgical Director of Caldwell Breast Center September 26, 2015 Advances in Breast Cancer Diagnosis and Treatment Recommendations
Update in Outpatient Medicine ACP Scientific Session November 12, 2016
 Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Screening for Breast Cancer
 Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER
 GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER") NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
General principles of screening: A radiological perspective
 General principles of screening: A radiological perspective Fergus Coakley MD, Professor and Chair, Diagnostic Radiology, Oregon Health and Science University General principles of screening: A radiological
General principles of screening: A radiological perspective Fergus Coakley MD, Professor and Chair, Diagnostic Radiology, Oregon Health and Science University General principles of screening: A radiological
Q: Why is breast cancer a big deal?
 I hate breast cancer. As a radiologist who specializes in breast imaging, my career is devoted to the detection and diagnosis of breast cancer. I am passionate about women s health and my goal is to find
I hate breast cancer. As a radiologist who specializes in breast imaging, my career is devoted to the detection and diagnosis of breast cancer. I am passionate about women s health and my goal is to find
Objectives. Polypharmacy Seminar. Causes of Polypharmacy. Polypharmacy 8/05/12. National Prescribing Curriculum Module
 Polypharmacy Seminar Objectives On completion of this module you should be able to: state the major guiding principles in rational prescribing recognise, and substantiate, over-prescribing or inappropriate
Polypharmacy Seminar Objectives On completion of this module you should be able to: state the major guiding principles in rational prescribing recognise, and substantiate, over-prescribing or inappropriate
What every woman should know about. Screening Mammograms
 What every woman should know about Screening Mammograms What is breast screening? Regular examination of a woman s breasts to find breast cancer early. It includes mammography (breast X-ray) and a physical
What every woman should know about Screening Mammograms What is breast screening? Regular examination of a woman s breasts to find breast cancer early. It includes mammography (breast X-ray) and a physical
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Breast Cancer Screening and Diagnosis
 Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Name of Policy: Boniva (Ibandronate Sodium) Infusion
 Infusion") Name of Policy: Boniva (Ibandronate Sodium) Infusion Policy #: 266 Latest Review Date: April 2010 Category: Pharmacology Policy Grade: Active Policy but no longer scheduled for regular literature reviews
Name of Policy: Boniva (Ibandronate Sodium) Infusion Policy #: 266 Latest Review Date: April 2010 Category: Pharmacology Policy Grade: Active Policy but no longer scheduled for regular literature reviews
Let s look a minute at the evidence supporting current cancer screening recommendations.
 I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
Foundational funding sources allow BCCHP to screen and diagnose women outside of the CDC guidelines under specific circumstances in Washington State.
 Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
Breast Cancer Risk Factors 8/3/2014
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
DINE AND LEARN ENDOCRINOLOGY PEARLS. Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC
 DINE AND LEARN ENDOCRINOLOGY PEARLS Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC OUTLINE HRT and CVD HRT and Breast Cancer Osteoporosis When to treat How long to treat for Bisphosphonates BMD
DINE AND LEARN ENDOCRINOLOGY PEARLS Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC OUTLINE HRT and CVD HRT and Breast Cancer Osteoporosis When to treat How long to treat for Bisphosphonates BMD
Vitamin D: Conflict of Interest Statement Corporate. Outline 7/5/2016
 Vitamin D: What s New and Not? Clifford J Rosen MD Maine Medical Center Research Institute rosenc@mmc.org Conflict of Interest Statement Corporate NO STOCKS or EQUITY Editor UpToDate, New England Journal
Vitamin D: What s New and Not? Clifford J Rosen MD Maine Medical Center Research Institute rosenc@mmc.org Conflict of Interest Statement Corporate NO STOCKS or EQUITY Editor UpToDate, New England Journal
Nutraceuticals and Cardiovascular Disease: Are we fishing?
 Nutraceuticals and Cardiovascular Disease: Are we fishing? ACC Rockies 2013 March 20,2013 Sheri L. Koshman BScPharm, PharmD, ACPR Assistant Professor, Division of Cardiology, University of Alberta sheri.koshman@ualberta.ca
Nutraceuticals and Cardiovascular Disease: Are we fishing? ACC Rockies 2013 March 20,2013 Sheri L. Koshman BScPharm, PharmD, ACPR Assistant Professor, Division of Cardiology, University of Alberta sheri.koshman@ualberta.ca
V t i amin i n D a nd n d Calc l iu i m u : Rol o e l in i n Pr P eve v nt n io i n and n d Tr T eatment n of o Fr F actur u es and n d Fa F ll l s
 Vitamin D and Calcium: Role in Prevention and Treatment of Fractures and Falls Osteoporosis 21: New Insights In Research, Diagnosis, and Clinical Care Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic
Vitamin D and Calcium: Role in Prevention and Treatment of Fractures and Falls Osteoporosis 21: New Insights In Research, Diagnosis, and Clinical Care Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Ultrasound: Improving Breast Cancer Detection
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/advances-in-womens-health/ultrasound-improving-breast-cancerdetection/3514/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/advances-in-womens-health/ultrasound-improving-breast-cancerdetection/3514/
MEDICAL POLICY EFFECTIVE DATE: 08/21/14 REVISED DATE: 04/16/15, 06/16/16, 07/20/17 SUBJECT: SCREENING FOR VITAMIN D DEFICIENCY
 MEDICAL POLICY SUBJECT: SCREENING FOR VITAMIN D DEFICIENCY A nonprofit independent licensee of the BlueCross BlueShield Association PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not
MEDICAL POLICY SUBJECT: SCREENING FOR VITAMIN D DEFICIENCY A nonprofit independent licensee of the BlueCross BlueShield Association PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not
The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis
 The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis Mark J Bolland, Andrew Grey, Greg D Gamble, Ian R Reid Summary Background Vitamin D insufficiency
The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential meta-analysis Mark J Bolland, Andrew Grey, Greg D Gamble, Ian R Reid Summary Background Vitamin D insufficiency
Melissa Hartman, DO Women s Health Orlando VA Medical Center
 Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
A response by Servier to the Statement of Reasons provided by NICE
 A response by Servier to the Statement of Reasons provided by NICE Servier gratefully acknowledges the Statement of Reasons document from NICE, and is pleased to provide information to assist NICE in its
A response by Servier to the Statement of Reasons provided by NICE Servier gratefully acknowledges the Statement of Reasons document from NICE, and is pleased to provide information to assist NICE in its
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Vitamin D and Calcium Therapy: how much is enough
 Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco DISCLOSURE Nothing to disclose 1 RECOMMENDATIONS
Rethinking Breast Cancer Screening
 Rethinking Breast Cancer Screening NAMS Meeting, October, 2014 Russell Harris, MD, MPH University of North Carolina, Chapel Hill Conflicts of Interest Financial: none Intellectual: I have been researching
Rethinking Breast Cancer Screening NAMS Meeting, October, 2014 Russell Harris, MD, MPH University of North Carolina, Chapel Hill Conflicts of Interest Financial: none Intellectual: I have been researching
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
The Endocrine Society Guidelines
 Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
Vitamin D and Calcium Therapy: how much is enough DISCLOSURE Daniel D Bikle, MD, PhD Professor of Medicine VA Medical Center and University of California San Francisco Nothing to disclose RECOMMENDATIONS
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET NO DISCLOSURES 3/7/2015. Laura Esserman MD MBA
 Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET But soon.... Laura Esserman MD MBA 2 Breast Cancer Gene Expression Profiling Prognostic Tests 1. OncotypeDX Recurrence Score
Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET But soon.... Laura Esserman MD MBA 2 Breast Cancer Gene Expression Profiling Prognostic Tests 1. OncotypeDX Recurrence Score
Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care
 Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care Jason Cord, M.D. SCPMG Regional Chief of Breast Imaging PIC for Breast Imaging,
Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care Jason Cord, M.D. SCPMG Regional Chief of Breast Imaging PIC for Breast Imaging,
denosumab (Prolia ) Policy # Original Effective Date: 07/21/2011 Current Effective Date: 04/19/2017
 Policy # Original Effective Date: 07/21/2011 Current Effective Date: 04/19/2017") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Based on review of available data, the Company may consider the use of denosumab (Prolia) for the
 for the") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Henda s Law. Supplemental screening for women with dense breast tissue and increased risk
 . Henda s Law Supplemental screening for women with dense breast tissue and increased risk The 2011 Texas Legislature passed House Bill 2102 which is effective 1st September 2011. The law is informally
. Henda s Law Supplemental screening for women with dense breast tissue and increased risk The 2011 Texas Legislature passed House Bill 2102 which is effective 1st September 2011. The law is informally
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Menopausal hormone therapy currently has no evidence-based role for
 IN PERSPECTIVE HT and CVD Prevention: From Myth to Reality Nanette K. Wenger, M.D. What the studies show, in a nutshell The impact on coronary prevention Alternative solutions Professor of Medicine (Cardiology),
IN PERSPECTIVE HT and CVD Prevention: From Myth to Reality Nanette K. Wenger, M.D. What the studies show, in a nutshell The impact on coronary prevention Alternative solutions Professor of Medicine (Cardiology),
RED FATE CARDS. Photocopy the following Fate Cards on red paper or cardstock. Cut out each card and print the word Fate Card on the back of each card.
 RED FATE CARDS Photocopy the following Fate Cards on red paper or cardstock. Cut out each card and print the word Fate Card on the back of each card. You are female. You are a thin, small-framed elderly
RED FATE CARDS Photocopy the following Fate Cards on red paper or cardstock. Cut out each card and print the word Fate Card on the back of each card. You are female. You are a thin, small-framed elderly
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Cancer Screening 2009: New Tests, New Choices
 Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Prevention of osteoporosis: cost-effectiveness of different pharmaceutical treatments Ankjaer-Jensen A, Johnell O
 Prevention of osteoporosis: cost-effectiveness of different pharmaceutical treatments Ankjaer-Jensen A, Johnell O Record Status This is a critical abstract of an economic evaluation that meets the criteria
Prevention of osteoporosis: cost-effectiveness of different pharmaceutical treatments Ankjaer-Jensen A, Johnell O Record Status This is a critical abstract of an economic evaluation that meets the criteria
HRT & Menopause Where Do We Stand Now?
 HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over
 Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC
 PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria: