Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
|
|
|
- Catherine Farmer
- 5 years ago
- Views:
Transcription
1 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
2 Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment, characteristically associated with increased numbers of white cells in the bone marrow and/or peripheral blood. The course of leukaemia may vary from a few days or weeks to many years, depending on the type.
3 Epidemiology and aetiology The incidence of leukaemia of all types in the population is approximately 10/ per annum, of which just under half are cases of acute leukaemia. Males are affected more frequently than females.
4 Acute leukaemia occurs at all ages. Acute lymphoblastic leukaemia shows a peak of incidence in children aged 1 5 years. All forms of acute myeloid leukaemia have their lowest incidence in young adult life and there is a striking rise over the age of 50. Chronic leukaemias occur mainly in middle and old age.
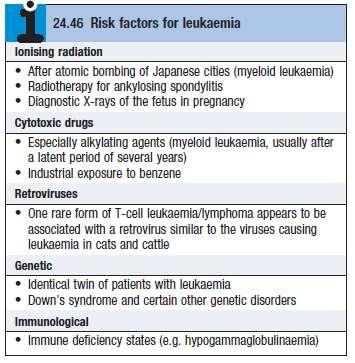
5 The cause of the leukaemia is unknown in the majority of patients. Several risk factors, however, have been identified.
6
7 Terminology and classification Leukaemias are traditionally classified into four main groups: acute lymphoblastic leukaemia (ALL) acute myeloid leukaemia (AML) chronic lymphocytic leukaemia (CLL) chronic myeloid leukaemia (CML).
8 In acute leukaemia, there is proliferation of primitive stem cells, leading to an accumulation of blasts, predominantly in the bone marrow, which causes bone marrow failure. In chronic leukaemia, the malignant clone is able to differentiate, resulting in an accumulation of more mature cells.
9 The diagnosis of leukaemia is usually suspected from an abnormal blood count, often a raised white count, and is confirmed by examination of the bone marrow. This includes the morphology of the abnormal cells, analysis of cell surface markers (immunophenotyping), clone-specific chromosome abnormalities and molecular changes.
10 The features in the bone marrow not only provide an accurate diagnosis but also give valuable prognostic information, allowing therapy to be tailored to the patient s disease.
11 Acute leukaemia There is a failure of cell maturation in acute leukaemia. Proliferation of cells which do not mature leads to an accumulation of primitive cells which take up more and more marrow space at the expense of the normal haematopoietic elements. Eventually, this proliferation spills into the blood.
12 Acute myeloid leukaemia (AML) is about four times more common than acute lymphoblastic leukaemia (ALL) in adults. The clinical features are usually those of bone marrow failure (anaemia, bleeding or infection).

13
14 Investigations Blood examination usually shows anaemia with a normal or raised MCV. The leucocyte count may vary from as low as 1 109/L to as high as /L or more. Severe thrombocytopenia is usual but not invariable. Frequently, blast cells are seen in the blood film but sometimes blast cells may be infrequent or absent.
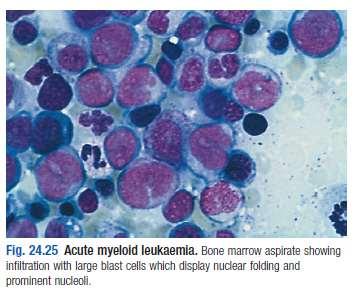
15 A bone marrow examination will confirm the diagnosis. The bone marrow is usually hypercellular, with replacement of normal elements by leukaemic blast cells in varying degrees (but more than 20% of the cells). Classification and prognosis are determined by immunophenotyping, chromosome and molecular analysis.
16

17 Management
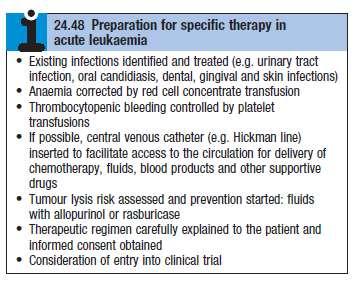
18 Specific therapy If a decision to embark on specific therapy has been taken, the patient should be prepared.
19
20 The aim of treatment is to destroy the leukaemic clone of cells without destroying the residual normal stem cell compartment from which repopulation of the haematopoietic tissues will occur.
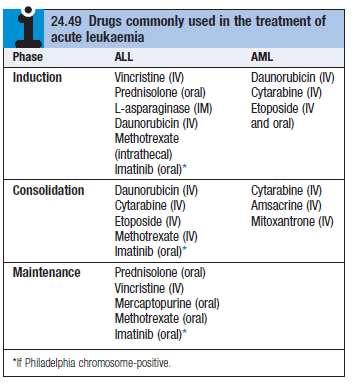
21 Remission induction. In this phase, the bulk of the tumour is destroyed by combination chemotherapy. The patient goes through a period of severe bone marrow hypoplasia, requiring intensive support and inpatient care from a specially trained multidisciplinary team.
22 Remission consolidation. If remission has been achieved, residual disease is attacked by therapy during the consolidation phase. This consists of a number of courses of chemotherapy, again resulting in periods of marrow hypoplasia.
23 Remission maintenance. If the patient is still in remission after the consolidation phase for ALL, a period of maintenance therapy is given, with the individual as an outpatient and treatment consisting of a repeating cycle of drug administration.
24 In patients with ALL, it is necessary to give prophylactic treatment to the central nervous system, as this is a sanctuary site where standard therapy does not penetrate.
25
26 Supportive therapy Aggressive and potentially curative therapy, which involves periods of severe bone marrow failure, would not be possible without appropriate supportive care.
27 Anaemia. Anaemia is treated with red cell concentrate transfusions. Bleeding. Thrombocytopenic bleeding requires platelet transfusions. Coagulation abnormalities occur and need accurate diagnosis and treatment.
28 Infection. Fever (> 38 C) lasting over 1 hour in a neutropenic patient indicates possible septicaemia. Parenteral broad-spectrum antibiotic therapy is essential. Empirical therapy is given according to local bacteriological resistance patterns: for example, with a combination of an aminoglycoside (e.g. gentamicin) and a broad-spectrum penicillin (e.g. piperacillin/tazobactam) or a single-agent beta-lactam (e.g. meropenem).
29 Gram-positive infection may require vancomycin therapy. If fever has not resolved after 3 5 days, empirical antifungal therapy is added.
30 Patients with ALL are susceptible to infection with Pneumocystis jirovecii, which causes a severe pneumonia. Prophylaxis with co-trimoxazole is given during chemotherapy.
31 Isolation facilities and barrier nursing practices are used to guard against infections.
32 Metabolic problems. Frequent monitoring of fluid balance and renal, hepatic and haemostatic function is necessary. Patients are often severely anorexic and diarrhoea is common as a consequence of the side-effects of therapy; they may find drinking difficult and hence require intravenous fluids and electrolytes.
33 Cellular breakdown during induction therapy (tumour lysis syndrome) releases intracellular ions and nucleic acid breakdown products, causing hyperkalaemia, hyperuricaemia, hyperphosphataemia and hypocalcaemia. This may cause renal failure. Allopurinol and intravenous hydration are given to try to prevent this.
34 Psychological problems. Psychological support is a key aspect of care. Patients should be kept informed, and their questions answered and fears allayed as far as possible.
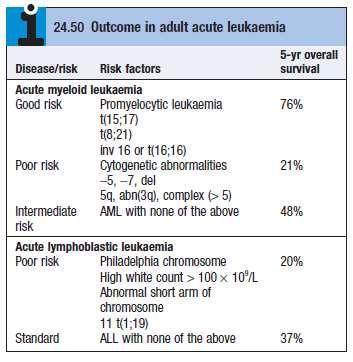
35 Haematopoietic stem cell transplantation In patients with high-risk acute leukaemia, allogeneic HSCT can improve 5-year survival from 20% to around 50%.
36 Prognosis Without treatment, the median survival of patients with acute leukaemia is about 5 weeks. This may be extended to a number of months with supportive treatment.
37
38 Patients who achieve remission with specific therapy have a better outlook. Around 80% of adult patients under 60 years of age with ALL or AML achieve remission. Advances in treatment have led to steady improvement in survival from leukaemia.
39 Chronic myeloid leukaemia Chronic myeloid leukaemia (CML) is a myeloproliferative stem cell disorder resulting in proliferation of all haematopoietic lineages but manifesting predominantly in the granulocytic series. Maturation of cells proceeds fairly normally. The disease occurs chiefly between the ages of 30 and 80 years, with a peak incidence at 55 years.
40 The defining characteristic of CML is the chromosome abnormality known as the Philadelphia (Ph) chromosome. The fragment from chromosome 9 that joins the BCR carries the abl oncogene, which forms a fusion gene with the remains of the BCR.
41 This BCR ABL fusion gene codes for a protein with tyrosine kinase activity, which plays a causative role in the disease as an oncogene influencing cellular proliferation, differentiation and survival.
42 Natural history The disease has three phases: A chronic phase, in which the disease is responsive to treatment and is easily controlled, which used to last 3 5 years. With the introduction of imatinib therapy, this phase has been prolonged to longer than 8 years in many patients.
43 An accelerated phase (not always seen), in which disease control becomes more difficult. Blast crisis, in which the disease transforms into an acute leukaemia, which is relatively refractory to treatment. This is the cause of death in the majority of patients.
44 Clinical features Symptoms at presentation may include lethargy, weight loss, abdominal discomfort and sweating, may be asymptomatic. Splenomegaly is present in 90%; in about 10%, the enlargement is massive. Hepatomegaly occurs in about 50%. Lymphadenopathy is unusual.
45 Investigations There is usually a normocytic, normochromic anaemia. The leucocyte count can vary from 10 to /L. In the blood film, the full range of granulocyte precursors is seen.
46 Blast transformation is characterised by a dramatic increase in the number of circulating blasts
47 Bone marrow should be obtained to confirm the diagnosis and phase of disease by morphology, chromosome analysis to demonstrate the presence of the Ph chromosome, and RNA analysis to demonstrate the presence of the BCR ABL gene product. Blood LDH levels are elevated and the uric acid level may be high due to increased cell breakdown.
48 Management Chronic phase Imatinib specifically inhibits BCR ABL tyrosine kinase activity and reduce the uncontrolled proliferation of white cells. It is recommended as first-line therapy in chronic-phase CML.
49 Accelerated phase and blast crisis For patients presenting in accelerated phase, imatinib is indicated if the patient has not already received it. Hydroxycarbamide can be an effective single agent. When blast transformation occurs, the type of blast cell should be determined.
50 Patients progressing to advanced-phase disease on imatinib may respond to a secondgeneration tyrosine kinase inhibitor and may be considered for allogeneic HSCT
51 Chronic lymphocytic leukaemia Chronic lymphocytic leukaemia (CLL) is the most common variety of leukaemia, accounting for 30% of cases. In this disease, B lymphocytes, which would normally respond to antigens by transformation and antibody formation, fail to do so.
52 Clinical features The onset is usually insidious and diagnosis may be incidental on a FBC. Presenting problems may be anaemia, infections, painless lymphadenopathy, and systemic symptoms such as night sweats or weight loss.
53 Investigations The diagnosis is based on the peripheral blood findings of a mature lymphocytosis (> 5 109/L) with characteristic morphology and cell surface markers.
54 Other useful investigations in CLL include a reticulocyte count and a direct Coombs test, as autoimmune haemolytic anaemia may occur. Serum immunoglobulin levels should be estimated. Bone marrow examination by aspirate and trephine is not essential for the diagnosis of CLL, but may be helpful in difficult cases, for prognosis and to monitor response to therapy.
55
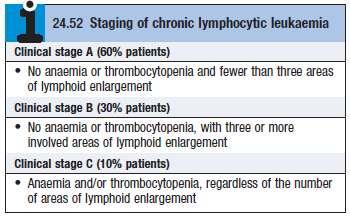
56 Management No specific treatment is required for most clinical stage A patients, unless progression occurs. Life expectancy is usually normal in older patients.
57 Treatment is only required if there is evidence of bone marrow failure, massive or progressive lymphadenopathy or splenomegaly, systemic symptoms, a rapidly increasing lymphocyte count or autoimmune haemolytic anaemia or thrombocytopenia. Initial therapy for those requiring treatment (stages B and C) may consist of oral chemotherapy with the alkylating agent chlorambucil.
58 Supportive care is increasingly required in progressive disease. Radiotherapy may be used for lymphadenopathy which is causing discomfort or local obstruction, and for symptomatic splenomegaly.
59 Thank you!
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
LEUKAEMIA and LYMPHOMA. Dr Mubarak Abdelrahman Assistant Professor Jazan University
 LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
LEUKAEMIA and LYMPHOMA Dr Mubarak Abdelrahman Assistant Professor Jazan University OBJECTIVES Identify etiology and epidemiology for leukemia and lymphoma. Discuss common types of leukemia. Distinguish
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
BIOS222 Pathology and Clinical Science 2
 BIOS222 Pathology and Clinical Science 2 Session 5 Lymphatic and Haematological Disorders 3 Bioscience Department www.endeavour.edu.au Session Learning Outcomes At the end of the session, you should be
BIOS222 Pathology and Clinical Science 2 Session 5 Lymphatic and Haematological Disorders 3 Bioscience Department www.endeavour.edu.au Session Learning Outcomes At the end of the session, you should be
Blood Cancers in the Community
 Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Tasigna. Tasigna (nilotinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1 of 6 Last Review Date: March 16, 2018 Tasigna Description Tasigna (nilotinib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1 of 6 Last Review Date: March 16, 2018 Tasigna Description Tasigna (nilotinib)
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Tasigna. Tasigna (nilotinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1of 5 Last Review Date: September 15, 2017 Tasigna Description Tasigna (nilotinib)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.77 Subject: Tasigna Page: 1of 5 Last Review Date: September 15, 2017 Tasigna Description Tasigna (nilotinib)
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Blood Cancer: Chronic Myelogenous Leukaemia
 Published on: 30 May 2017 Blood Cancer: Chronic Myelogenous Leukaemia What Is Cancer? The body is made up of cells that grow and die in a controlled way. Sometimes, cells keep dividing and growing without
Published on: 30 May 2017 Blood Cancer: Chronic Myelogenous Leukaemia What Is Cancer? The body is made up of cells that grow and die in a controlled way. Sometimes, cells keep dividing and growing without
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Version: 6 Date: 2 nd March 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES
 GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Acute Lymphoblastic Leukaemia
 Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
Acute Lymphoblastic Leukaemia Terri Boyer 17 th October 2006 Overview Disease information: Aetiology of ALL proposed theory, contributing factors Symptoms Complications Diagnostic approaches - morphology
SPECIAL AUTHORIZATION REQUEST FOR COVERAGE OF HIGH COST CANCER DRUGS
 SPECIAL AUTHORIZATION REQUEST FOR COVERAGE OF HIGH COST CANCER DRUGS (Filgrastim, Capecitabine, Imatinib, Dasatinib, Erolotinib, Sunitinib, Pazopanib, Fludarabine, Sorafenib, Crizotinib, Tretinoin, Nilotinib,
SPECIAL AUTHORIZATION REQUEST FOR COVERAGE OF HIGH COST CANCER DRUGS (Filgrastim, Capecitabine, Imatinib, Dasatinib, Erolotinib, Sunitinib, Pazopanib, Fludarabine, Sorafenib, Crizotinib, Tretinoin, Nilotinib,
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand
 Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
TRANSPARENCY COMMITTEE OPINION. 14 February 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 February 2007 GLIVEC 100 mg, capsule B/120 capsules (CIP: 358 493-5) GLIVEC 100 mg, capsule B/180 capsules (CIP:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 February 2007 GLIVEC 100 mg, capsule B/120 capsules (CIP: 358 493-5) GLIVEC 100 mg, capsule B/180 capsules (CIP:
Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study
 Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Original Research Article Bone marrow aspiration as the initial diagnostic tool in the diagnosis of leukemia - A case study Priyanka Poonam 1*, N.K. Bariar 2 1 Tutor, Department of Pathology, Patna Medical
Acute Myeloid Leukemia: A Patient s Perspective
 Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
2017 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients
 07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Flow Cytometry. Bone Marrow Aspirate and Biopsy. Leukemia and Myelodysplastic Syndromes
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Elise Frans, MN, RN, CWON Oncology CNS University of Washington Medical Center delterzo@uw.edu 1 History & Physical Labs:
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital
 By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
By Angela Gascoigne Haematology CNS Chesterfield Royal Hospital Myeloproliferative Neoplasms Essential Thrombocythaemia Polycythaemia Vera Myelofibrosis Essential Thrombocythaemia (ET) Chronic condition
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS Heme Malignancies/BMT CNS Seattle Cancer Care Alliance/UWMC Lymphoid 1 Myeloid 2 Presenting Signs and Symptoms Diagnostic Evaluation
MYELOPROLIFERATIVE DISEASE. Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG
, MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG") MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS
 Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 2 Dr Helen Barker MDT Lead
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 2 Dr Helen Barker MDT Lead
This is a controlled document and therefore must not be changed
 AZACITIDINE NICE TA218 Treatment of adults not eligible for haematopoietic stem cell transplantation who have: Intermediate-2 and high-risk MDS according to the International Prognostic Scoring System
AZACITIDINE NICE TA218 Treatment of adults not eligible for haematopoietic stem cell transplantation who have: Intermediate-2 and high-risk MDS according to the International Prognostic Scoring System
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin
 Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Guidelines on the Management of a Child with Sickle Cell Disease and low Haemoglobin Document Information Version: 2 Date: 28 th December 2013 Authors (incl. job title): Professor David Rees (Consultant
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162
 Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Charles Mxxx DCEM2 Toulouse Purpan Medical School 01/26/2012 ECN Item 162 Definition Pathophysiology Clinical signs and symptoms Biology and Diagnosis Different types of AL Prognosis and Treatment Malignant
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Bosulif. Bosulif (bosutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.22 Section: Prescription Drugs Effective Date: April 1,2018 Subject: Bosulif Page: 1 of 5 Last Review
BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib
 BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib Protocol Code Tumour Group Contact Physician ULKAMLAS Leukemia/BMT Dr. Donna Hogge ELIGIBILITY: Acute myeloid
BC Cancer Protocol Summary for Therapy of Acute Myeloid Leukemia Using azacitidine and SORAfenib Protocol Code Tumour Group Contact Physician ULKAMLAS Leukemia/BMT Dr. Donna Hogge ELIGIBILITY: Acute myeloid
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Stem cell transplantation. Dr Mohammed Karodia NHLS & UP
 Stem cell transplantation Dr Mohammed Karodia NHLS & UP The use of haemopoeitic stem cells from a donor harvested from peripheral blood or bone marrow, to repopulate recipient bone marrow. Allogeneic From
Stem cell transplantation Dr Mohammed Karodia NHLS & UP The use of haemopoeitic stem cells from a donor harvested from peripheral blood or bone marrow, to repopulate recipient bone marrow. Allogeneic From
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA
 BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
BLASTIC CRISIS AND MYELOFIBROSIS SIMULTANEOUS COMPLICATIONS IN A CASE OF CHRONIC MYELOCYTIC LEUKEMIA Abstract Pages with reference to book, From 151 To 153 Khalid Hassan ( Department of Pathology (Haematology)
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway. Chronic Myeloid Leukaemia
 Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Hull and East Yorkshire and North Lincolnshire NHS Trusts Haematology Multidisciplinary Team Guideline and Pathway Chronic Myeloid Leukaemia 1 BACKGROUND The Hull and North Lincolnshire Haematology Multidisciplinary
Early diagnosis saves lives #SpotLeukaemia
 Early diagnosis saves lives #SpotLeukaemia Leukaemia... is a blood cancer affects people of all ages Leukaemia symptoms are hard to spot, as they are similar to the symptoms of common, unrelated conditions.
Early diagnosis saves lives #SpotLeukaemia Leukaemia... is a blood cancer affects people of all ages Leukaemia symptoms are hard to spot, as they are similar to the symptoms of common, unrelated conditions.
R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01
 West of Scotland Cancer Network Chemotherapy Protocol R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01 Indication B cell Chronic Lymphocytic Leukaemia First line therapy in patients under 70 years of
West of Scotland Cancer Network Chemotherapy Protocol R-FC for Chronic Lymphocytic Leukaemia LKWOS-005/01 Indication B cell Chronic Lymphocytic Leukaemia First line therapy in patients under 70 years of
PROBLEMS OF THE HEMATOLOGICAL SYSTEM
 PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
PROBLEMS OF THE HEMATOLOGICAL SYSTEM UNIT 5 Review A & P of Hematological system Outline focused exam Differentiate and start to evaluate diagnostic exams used to assess problems of the hematological system
Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD
 Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
CHRONIC MYELOGENOUS LEUKEMIA. By Ting Huai Shi Pd. 6
 CHRONIC MYELOGENOUS LEUKEMIA By Ting Huai Shi Pd. 6 PHYSIOLOGY Chronic myelogenous leukemia (CML) is one of four forms of leukemia. It is caused by a spontaneous somatic mutations, and therefore, non-hereditary.
CHRONIC MYELOGENOUS LEUKEMIA By Ting Huai Shi Pd. 6 PHYSIOLOGY Chronic myelogenous leukemia (CML) is one of four forms of leukemia. It is caused by a spontaneous somatic mutations, and therefore, non-hereditary.
North West London Cancer Network
 GUIDELINES FOR THE MANAGEMENT OF ADULT ACUTE LEUKAEMIA INITIAL MANAGEMENT CONSIDERATIONS N.B.: If AML is suspected definitively diagnosed, please ensure that the patient is transferred immediately f treatment
GUIDELINES FOR THE MANAGEMENT OF ADULT ACUTE LEUKAEMIA INITIAL MANAGEMENT CONSIDERATIONS N.B.: If AML is suspected definitively diagnosed, please ensure that the patient is transferred immediately f treatment
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS
 Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1 Dr Helen Barker MDT Lead
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1 Dr Helen Barker MDT Lead
Flow Cytometry. Leukemia and Myelodysplastic Syndromes. Bone Marrow Aspirate and Biopsy
 Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
Diagnostic Evaluation of Blood Disorders Leukemia and Myelodysplastic Syndromes Lenise Taylor, MN, RN, AOCNS, BMTCN BMT/Immunotherapy CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org History
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
PATHOLOGY & PATHOPHYSIOLOGY
 PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF BLOOD DISORDERS OF BLOOD Disorders of Blood Infections Tumours Nutritional disorders Coagulation disorders Congenital disorders Septicaemia Leukemia Iron deficiency
PATHOLOGY & PATHOPHYSIOLOGY DISORDERS OF BLOOD DISORDERS OF BLOOD Disorders of Blood Infections Tumours Nutritional disorders Coagulation disorders Congenital disorders Septicaemia Leukemia Iron deficiency
Neoplastic proliferation arising from white blood cells. Introductory remarks. Classification
 Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
Neoplastic proliferation arising from white blood cells Lymphoproliferative and myeloproliferative diseases and syndromes Oliver Rácz, 2012-2017 1 Introductory remarks Leukemia and lymphoma are old descriptive
This was a multicenter study conducted at 11 sites in the United States and 11 sites in Europe.
 Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL)
") Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
Guidelines for the Management of Chronic Lymphocytic Leukaemia (CLL) Version History Version Date Summary of Change/Process 2.0 08.05.08 Endorsed by the Governance Committee 2.1 16.02.11 Circulated at
a resource for physicians Recommended Referral Timing for Stem Cell Transplant Evaluation
 a resource for physicians Recommended Referral Timing for Stem Cell Transplant Evaluation This resource has been developed to help guide you regarding the appropriate timing and conditions for a referral
a resource for physicians Recommended Referral Timing for Stem Cell Transplant Evaluation This resource has been developed to help guide you regarding the appropriate timing and conditions for a referral
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Acute Lymphoblastic Leukaemia Guidelines
 Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Reference: NHS England 1602
 Clinical Commissioning Policy Proposition: Clofarabine for refractory or relapsed acute myeloid leukaemia (AML) as a bridge to stem cell transplantation Reference: NHS England 1602 First published: TBC
Clinical Commissioning Policy Proposition: Clofarabine for refractory or relapsed acute myeloid leukaemia (AML) as a bridge to stem cell transplantation Reference: NHS England 1602 First published: TBC
WHAT ARE PAEDIATRIC CANCERS
 WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
WHAT ARE PAEDIATRIC CANCERS INTRODUCTION Childhood cancers are RARE 0.5% of all cancers in the West Overall risk that a child will develop cancer during first 15 years of life is 1 in 450 and 1 in 600
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation
 Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
Case Study Diagnostic challenge: Acute leukemia with biphenotypic blasts and BCR-ABL1 translocation Ling Wang 1 and Xiangdong Xu 1,2,* 1 Department of Pathology, University of California, San Diego; 2
FLOW CYTOMETRY PRINCIPLES AND PRACTICE. Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018
 FLOW CYTOMETRY PRINCIPLES AND PRACTICE Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018 Aims and Objectives Principles of flow cytometry Preparation Steps involved
FLOW CYTOMETRY PRINCIPLES AND PRACTICE Toby Eyre Consultant Haematologist Oxford University Hospitals NHS Foundation Trust June 2018 Aims and Objectives Principles of flow cytometry Preparation Steps involved
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Recommended Timing for Transplant Consultation
 REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Leukemia and Myelodysplastic Syndromes
 Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
Leukemia and Myelodysplastic Syndromes Lenise Taylor, RN, MN, AOCNS, BMTCN Oncology CNS Seattle Cancer Care Alliance/UWMC ltaylor@seattlecca.org Lymphoid 1 Myeloid 2 Diagnostic Evaluation of Blood Disorders
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital
 Ray Mun Koo Haematology Advanced Trainee Canberra Hospital") Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
Haematological Emergencies (Part 1) Ray Mun Koo Haematology Advanced Trainee Canberra Hospital Case Number 1 43 year old male presenting with fevers, abdominal distension and weight gain over 2 weeks.
2013 Pathology Student
 About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
About this guide If you re reading this introduction, it means you are probably either a) covering hematopathology in your pathology class right now, or b) studying for boards. Either way, you ve come
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
NCCP Chemotherapy Regimen
 INDICATIONS FOR USE: Azacitidine i INDICATION ICD10 Regimen Code *Reimbursement Status Intermediate-1 and low risk myelodysplastic syndromes (MDS) according to the International Prognostic Scoring System
INDICATIONS FOR USE: Azacitidine i INDICATION ICD10 Regimen Code *Reimbursement Status Intermediate-1 and low risk myelodysplastic syndromes (MDS) according to the International Prognostic Scoring System
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
DEPARTMENT OF CLINICAL HEMATOLOGY
 DEPARTMENT OF CLINICAL HEMATOLOGY What is blood? Blood is the vital fluid of the body, which performs diverse functions from delivering oxygen to each and every cell of the body to fighting against infections
DEPARTMENT OF CLINICAL HEMATOLOGY What is blood? Blood is the vital fluid of the body, which performs diverse functions from delivering oxygen to each and every cell of the body to fighting against infections
The BCR-ABL1 fusion. Epidemiology. At the center of advances in hematology and molecular medicine
 At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
At the center of advances in hematology and molecular medicine Philadelphia chromosome-positive chronic myeloid leukemia Robert E. Richard MD PhD rrichard@uw.edu robert.richard@va.gov Philadelphia chromosome
DERBY-BURTON CANCER NETWORK CONTROLLED DOC NO:
 OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Chronic Myelogenous Leukemia (Hematology) By DEISSEROTH READ ONLINE
 By DEISSEROTH READ ONLINE") Chronic Myelogenous Leukemia (Hematology) By DEISSEROTH READ ONLINE If searched for the ebook by DEISSEROTH Chronic Myelogenous Leukemia (Hematology) in pdf format, in that case you come on to correct
Chronic Myelogenous Leukemia (Hematology) By DEISSEROTH READ ONLINE If searched for the ebook by DEISSEROTH Chronic Myelogenous Leukemia (Hematology) in pdf format, in that case you come on to correct