Surgical Issues in Neoadjuvant Chemotherapy
|
|
|
- Regina Grant
- 5 years ago
- Views:
Transcription
1 14 th Bossche Mamma Congress Ruwenbergstraat AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women s Cancer Center Associate Division Chief for Breast Surgery Brigham and Women s Hospital Associate Professor of Surgery Harvard Medical School
2 Accepted Facts Neoadjuvant Therapy No survival advantage or disadvantage In breast pathologic response rate correlates with both DFS and OS Allows down-staging of disease large tumors and BCT in select patients reduces need for axillary node dissection Requires a multi-disciplinary approach.
3 Neoadjuvant Therapy and Survival ~1500pts, AC ~2300 pts, AC/T Rastogi P et al. J Clin Oncol 2008;26:

4 OS by response to neoadjuvant tx TNBC vs non-tnbc Adapted from Liedtke C et al. JCO 2008
5 Neoadjuvant Therapy and BCT Trial %BCT Chemo first % BCT Surgery first Royal Marsden Institut Curie NSABP B EORTC Tumor shrinkage 79% pts (36% ccr and 43% cpr)
6 Neoadjuvant Chemotherapy and BCT Fisher B et al. J Clin Oncol 1997;15:
7 LRR after Neoadjuvant therapy LRR not different in patients downstaged to BCT No differences in LRR after NAC by surgery type Mieog J et al. Br J Surg 2007;94: Mamounas E et al. J Clin Oncol 2012;30:
8 Where are we now? King T and Morrow M. Nat Rev Clin Oncol 2015;12:
9 CALGB Randomized phase II trial, addition of carboplatin and/or bevacizumab to paclitaxel in TNBC In breast pcr: 60% with addition of carbo 219 (54%) BCS candidates 59% with addition of bev increased to 68% 185 (46%) not BCS candidates 78 (42%) converted to BCS eligible 31% chose mastectomy 53 (68%) chose BCS 48 (91%) completed BCS Sikov W et al. J Clin Oncol 2015;33:13-21 Golshan M et al. Ann Surg 2015;262:
10 Where do we go from here? pcr BCS
11 Surgical Challenges Neoadjuvant Therapy Need accurate imaging tools for quantifying response Need a standard method for monitoring response Consider differences in response by subtype


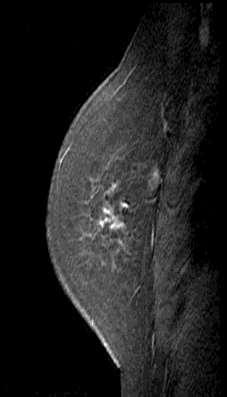
12 How Do We Know What to Resect? THIS? OR THIS?
13 Residual Imaging Tumor Size Compared to Path Tumor Size Imaging Modality Sensitivity Specificity Accuracy Clinical breast exam 49-50% 49-50% 54% Mammography 79-81% 79-81% 32% Ultrasound 89-90% 30-33% 60% MRI* 86-92% 60-86% 90% * Varies by tumor subtype and definition of pcr Adapted from Dialani et al. Ann Surg Oncol March 2015
14 MRI as a predictor of pcr TBCRC 017 Multicenter, retrospective study, pooled data 8 NCI centers 746pts, Overall, pcr rates 24% (defined as no invasive ca or DCIS) TN: 37% Her2 positive: 38% (78% received trastuzamab) De Los Santos JF et al, Cancer, 2013
15 MRI as a predictor of pcr TBCRC 017 Multicenter, retrospective study, pooled data 8 NCI centers 746pts, Overall, pcr rates 24% (defined as no invasive ca or DCIS) TN: 37% Her2 positive: 38% (78% received trastuzamab) De Los Santos JF et al, Cancer, 2013
16 Breast Imaging in Neoadjuvant Patients A Practical Approach CLINICAL T1,T2 N0 Mammogram /US pre- and post-treatment MRI pre- and posttreatment ONLY if downstaging to BCT Clip placed in breast tumor No routine axillary US CLINICAL T3,T4 N0 Mammogram/US pre- and post-treatment MRI pre- and posttreatment ONLY if downstaging to BCT Clip placed in breast tumor Routine axillary US No metastatic work-up Metastatic workup pretreatment
17 Approach to Lumpectomy After Neoadjuvant Chemotherapy Remove any suspicious clinical or radiologic findings Generous sample of normal breast tissue It is NOT necessary to remove the entire volume of tissue initially occupied by tumor
18 Challenges with Neoadjuvant Therapy Pattern of Response negative margins?
19 Guidelines for Re-excision after Neoadjuvant Chemotherapy In the setting of BCT and neoadjuvant chemotherapy, if viable tumor is present throughout the specimen even if it does not extend to the margin, a further re-excision should be considered. American College of Radiology, the American College of Surgeons, the College of American Pathology, and the Society of Surgical Oncology
20 Margins After Neoadjuvant Therapy Consensus Statement Does Not Apply! When margins are negative surgeons need to use the description of the response/residual disease both qualitatively and quantitatively to determine need for re-excision negative margins?
21 Neoadjuvant Chemotherapy Surgical Management of the Breast Evaluating the extent of residual disease remains a problem Resection and detailed pathology review are often the only way to determine suitability for BCT Persistent finding of scattered, viable tumor in resection specimens should prompt consideration of re-excision vs mastectomy
22 Axillary Management Neoadjuvant Chemotherapy NAC downstages axilla ~ 40% of patients (tumor subtype specific) Potential to consider SLNB after NAC avoid ALND Should management dependent on pretreatment clinical nodal stage? Clinically node negative Clinically node positive
23 Axillary Node Downstaging Neoadjuvant Chemotherapy NSABP B18 Surgery first (n = 743) Chemo first (n = 735) Overall node + 57% 41% 1-3 nodes + 30% 24% 4-9 nodes + 17% 12% > 10 nodes + 10% 4% p < Can we do SLN biopsy after NAC and avoid ALND? Fisher B, J Clin Oncol 1997;15:2483
24 SNB Before Neoadjuvant Therapy Arguments in Favor Information on the status of SLN can be obtained without the confounding effects of neoadjuvant therapy This may provide an advantage regarding: Further surgical management of the axilla Selection of optimal local-regional XRT Limited information on axillary recurrence rates with SLN after NAC
25 SNB Before Neoadjuvant Therapy Disadvantages Requires two surgical procedures Does not take advantage of the potential downstaging effects of neoadjuvant therapy on lymph nodes Commits all patients with pre-treatment positive nodes to ALND Uncertain prognostic value of negative nodes after NAC if the SLN was the only positive node and was removed
26 Sentinel Lymph Node Biopsy Neoadjuvant Therapy Clinically node negative; before or after? After treatment + + Identification rate? + False neg rate?
27 SLN Biopsy Before or After NAC clinically node negative SLN Identification rate False-negative rate BEFORE McMasters et al (2000) 86% and 90% 5.8 and11.8% ALMANAC trial (2006) 96.1% 6.7% NSABP B32 (2007) 97.2% 9.8% Kim et al* (2006) 96% (41-100%) 7.3% (0-29%) AFTER NSABP B27 (2005) 85% 10.7% Hunt et al (2009) 97.4% 5.9% Xing et al**(2006) 90% (72-100%) 12% (0-33%) Kelly et al***(2009) 89.6% (95%CI ) 8.4 (95%CI ) single agent vs dual agent *Metanalysis 69 trials, 8059 pts; ** metaanalysis 21 trials, 1273 pts; ***metaanalysis 24 trials, 1799 pts
28 SLN Biopsy After Neoadjuvant Chemotherapy MDACC , T1-3, cn0, n = 3746pts SLN found SLN false negative SLN before chemo n = % 4.2% (23/542) SLN after chemo n = % (p = 0.02) 5.9% (5/84) (p = 0.48) No difference in LRR (median f/u 47 mos) Hunt KK, Ann Surg 2009;250:558
29 Neoadjuvant Chemotherapy Decreases Axillary Dissection MDACC , T1-3, cn0, n = 3746pts % Node Positive SN first Chemo first P T T <.0001 T No difference in LRR (median f/u 47 mos) Hunt KK, Ann Surg 2009;250:558
30 Predictors of LRR after NAC pre- vs post-treatment nodal status NSABP B-18 (AC)/B-27 (AC-T) MVA: Predictors of LRR combined dataset at 10yrs Variable HR p Age 50 yrs vs < 50yrs 0.78 ( ) 0.03 Clin. Tumor Size > 5 cm vs 5cm 1.51 ( ) <0.001 Clin. Node (+) vs. Clin. Node (-) 1.61 ( ) <0.001 ypnode(-)/no breast pcr vs. ypnode(-)/breast pcr ypnode(+) vs. ypnode(-)/breast pcr 1.55 ( ) 2.71 ( ) < Mamounas E et al JCO 2012


31 LRF by Path Nodal Status and pcr B-18/B-27 : cn0 Lumpectomy pts >= 50yrs < 50yrs Low rates of regional recurrence all patients irrespective of path nodal and pcr status Mamounas E et al JCO 2012


32 LRF by Path Nodal Status and pcr B-18/B-27 : cn0 Mastectomy pts No PMRT Allowed T< 5cm T > 5cm Low rates regional recurrence all groups; increased CW recurrence node + after tx Mamounas E et al JCO 2012
33 Sentinel Lymph Node Biopsy Neoadjuvant Therapy A Practical Approach Clinically node negative SLN biopsy after NAC Intraoperative Frozen Section of SLN calnd for failed mapping calnd for any positive LN including micrometastatic disease Radiation tx decisions made on final node status and pcr status
34 Sentinel Lymph Node Biopsy Neoadjuvant Therapy Clinically node positive pt that converts to cn0? After treatment Identification rate? False neg rate?
 49 ER+/HER 2-7 (80) 9 12 (52) 23 ER+/HER2+ 33 (66) 50 20 (27) 74 ER-/HER2+ 17 (27) 63 16 (18) 89 ER-/HER2-17 (72) 24 17 (36) 47 *No residual invasive or in situ")
35 MSKCC Neoadjuvant Therapy N = 245 cn0 and N1 Surgical Database Clinical Stage I-III breast cancer, enrollment 11/2013-7/ /440 pts had completed surgical therapy % pcr breast and axilla* N =133 cn1 % pcr axilla ALL (133) 49 ER+/HER 2-7 (80) 9 12 (52) 23 ER+/HER2+ 33 (66) (27) 74 ER-/HER2+ 17 (27) (18) 89 ER-/HER2-17 (72) (36) 47 *No residual invasive or in situ disease in breast and axilla; includes patients that were initially cn0
36 ACOSOG Z1071 Eligible T0-T4, N1-2, M0 Biopsy Proven Nodal disease n = 663 cn1 SN ID rate 95% 649 SN ALND 2 SN identified n = 525, 79% Failed to meet primary endpoint FNR 10% FNR 12.6% (9.9, 16.1) Boughey JC, JAMA 2013
37 ACOSOG Z1071 cn1 patients How do we translate these findings in clinical practice??? FNR by Number of SN # SN Removed % of Cases 12% 24% 47% False Negative Rate 32% 21.1% 9.1% p=.007 Boughey JC, JAMA 2013
38 SLN Biopsy After Neoadjuvant Therapy cn1 convert cn0 ACOSOG Z1071 SENTINA SN FNAC N (cN+)* 153 Mapping Dual recommended (79%) Technetium required Pre-op biopsy? Yes Not required (biopsy =25%) Nodal pcr 41% 52% ypn0 (?) 35% IR 92.7% 80.1% 87.6% FNR (Overall) 12.6% 14.2% 8.4% 1 SLN 31.5% 24.3% 18.2% 2 SLN 21.1% 18.5% 4.9% 3SLN 9.1% 7.3% Technetium required, IHC *1737 patients enrolled in 4 arm multicenter trial. 592 ARM C were cn+ to cn0 Yes
39 SLN After Neoadjuvant Chemotherapy # of SN ACOSOG Z1071 N=649 cn+ convert to cn0 False Negative Rate (%) SENTINA N=592 SN-FNAC N=153 GANEA 2 N= Consistent unacceptable FNR unless 3 SN removed Residual disease resistant to treatment? No data on LRR in this setting Do know importance of path node status in predicting LRF in patients that start out cn+ implications for RT
40 Pre- vs post-treatment nodal status impact on LRR cn+ ypn+ LLR >25% cn+ ypn- no breast pcr cn- ypn- no breast pcr cn+ ypn- breast pcr cn- ypn- breast pcr Updated Analysis NSABP B-18 (AC)/B-27 (AC-T) Mamounas E et al JCO 2012
41 SLN biopsy after NAC cn1 convert to cn0 suggestions to minimize the FNR Dual agent mapping Normal exam after chemotherapy Remove 3 SN Include IHC detected disease as node positive Leave a clip at time of biopsy and localize for SLN
42 SLN Biopsy After Neoadjuvant Therapy cn1 convert cn0 ACOSOG Z1071 SENTINA SN FNAC N (cN+)* 153 Mapping Dual recommended (79%) Technetium required Pre-op biopsy? Yes Not required (biopsy =25%) Nodal pcr 41% 52% ypn0 (?) 35% IR 92.7% 80.1% 87.6% FNR (Overall) 12.6% 14.2% 8.4% 1 SLN 31.5% 24.3% 18.2% 2 SLN 21.1% 18.5% 4.9% 3SLN 9.1% 7.3% Technetium required, IHC *1737 patients enrolled in 4 arm multicenter trial. 592 ARM C were cn+ to cn0 Yes
 in the definition of residual nodal dz after neoadj tx reduces the")
43 Inclusion of micromets (<0.2mm) in the definition of residual nodal dz after neoadj tx reduces the pcr rate and improves the accuracy of SLN 2014 SABC

44 Placement of a clip + identification of the clip during SLN and removal at least 2 SLN reduces FNR
45 Targeted Axillary Dissection Calculated the ability of the clipped node +/- SLN to reflect the status of the nodal basin in all-comers undergoing NAC Clipped node n=191 pts; 120 path node +, pcr 37% FNR 4.2% (95%CI ) SLN n=118; 74 path node+, pcr 37% FNR 10.1% (95%CI ) SLN + clipped node n=118, 74 path node+, pcr 37% FNR 1.4% (95%CI ) Not a study restricted to cn1 pts that converted to cn0 after therapy Median number SLN removed 2.7 (<3 SLN) so the FNR of the SLN procedure alone not optimized in this analysis.
46 Sentinel Lymph Node Biopsy Neoadjuvant Therapy A Practical Approach Clinically node positive converts to node neg SLN biopsy after NAC w/ dual mapping agents Remove at least 3 SLN, Intraoperative Frozen Section of all SLN calnd for failed mapping fewer than 3 SLN any positive LN including micrometastatic disease/itcs (unless on trial)
47 69 th Annual Society of Surgical Oncology Cancer Symposium Boston, MA March 3 rd, 2016 How Often Does Neoadjuvant Chemotherapy Avoid Axillary Dissection in Patients with Histologically Confirmed Nodal Metastases: Results of a Prospective Study Anita Mamtani, MD, Andrea V. Barrio, MD, Tari A. King, MD, George Plitas, MD, Kimberly J. Van Zee, MD, Melissa Pilewskie, MD, Mahmoud B. El-Tamer, MD, Mary L. Gemignani, MD, Alexandra S. Heerdt, MD, Lisa M. Sclafani, MD, Virgilio Sacchini, MD, Hiram S. Cody III, MD, Sujata Patil, PhD, and Monica Morrow, MD Breast Service, Department of Surgery Memorial Sloan Kettering Cancer Center New York, NY
48 Objectives Determine the frequency with which ALND is avoided after NAC in biopsy-proven N+ patients Identify patient populations likely to benefit from this approach
49 Patient Population Clinical stage II III breast cancer Receiving NAC 11/ /2015 n = 534 Biopsy-proven N+ n = 195
50 Results Stage II-III, biopsy-proven N+ n = 195 ct4 or cn2/n3 n = 40 (21%) Downstaging to SLNB possible n = 155 (79%) ALND n = 40
51 Results Stage II-III, biopsy-proven N+ n = 195 Pre-neoadjuvant ct4 or cn2/n3 n = 40 Downstaging to SLNB possible n = 155 Post-neoadjuvant ALND n = 40 cn+: Not eligible for SLNB n = 23 (15%) cn0: Eligible for SLNB n = 132 (85%) SLNB deferred intraoperatively n = 4 SLNB n = 128
52 SLNB: Technical Details n = 128 Technical Factors n (%) SLN identified 125 (98%) # SLN removed 0 (failed mapping) 1 or (2%) 15 (12%) 110 (86%) Median # SLN removed 4.0
53 SLNB: Outcomes n = 128 SLNB attempted n = SLN retrieved underwent n = 110 SLNB ALND avoided in 62 of 128 (48%) of patients who ypn+ n = 48 ypn0 n = 62 ALND n = 48 No ALND n = 62
54 Nodal pcr by Receptor Status Receptor Status n % All 96 / % ER+/HER2-15 / 73 21% ER-/HER2-26 / 55 47% ER+/HER2+ 26 / 37 70% ER-/HER2+ 29 / 30 97% p <
55 Summary Of 195 biopsy-proven N+ patients, 132 (68%) were eligible for SLNB after NAC 3 SLN retrieved in 86% of cases Study # SLN retrieved, median 3 SLN, % SENTINA (Arm C, n = 592) 2 34% Z1071 (N1 arm, n = 651) 3 57% SN FNAC (n = 153) 2.7* Not reported * Mean reported
56 Conclusions This study supports the feasibility of identifying 3 SLN after NAC in the majority of patients presenting with nodal metastases Avoidance of ALND is an additional indication for NAC in patients with operable breast cancer Long-term follow-up will determine rates of regional failure in this cohort
57 Post NAC Trials of Axillary Management cn1 to cn0 ALLIANCE A11202 Schema Clinical T1-3 N1 M0 BC Neoadjuvant Chemotherapy BCT or Mastectomy Sentinel Lymph Node Surgery SLN Negative Randomization SLN Positive NSABP B-51/RTOG 1304 (NRG 9353) Schema Clinical T1-3 N1 M0 BC Axillary nodal involvement (FNA or core needle biopsy) Neoadjuvant chemo (+ Anti-HER-2 therapy for HER-2 neu pts) Definitive surgery with histologic documentation of negative axillary nodes (by axillary dissection or by SLNB axillary dissection Stratification Type of surgery (mastectomy vs lumpectomy) ER status (+ vs -), HER-2 status (+ vs -) pcr in breast (yes vs no) ALND Breast/chest wall and nodal XRT (no Axillary RT) No further axillary surgery. Breast/chest wall and nodal XRT (incl. Axilla) No Regional Nodal XRT with breast XRT if BCS & No chest wall XRT if mastectomy Randomization Regional Nodal XRT with breast XRT if BCS and chest wall XRT if mastectomy
58 Post NAC Trials of Axillary Management cn1 to cn0 ALLIANCE A11202 Schema Clinical T1-3 N1 M0 BC Neoadjuvant Chemotherapy BCT or Mastectomy Sentinel Lymph Node Surgery SLN Negative SLN Positive NSABP B-51/RTOG 1304 (NRG 9353) Schema Clinical T1-3 N1 M0 BC Axillary nodal involvement (FNA or core needle biopsy) Neoadjuvant chemo (+ Anti-HER-2 therapy for HER-2 neu pts) Definitive surgery with histologic documentation of negative axillary nodes (by axillary dissection or by SLNB axillary dissection Randomization Can axillary RT replace ALND? Randomization Can response to NAC be used to select patients who do not need PMRT or extended nodal field RT?
59 Thank You
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!?
 CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Breast Cancer: Management of the Axilla in Greg McKinnon MD FRCSC SON Vancouver Oct 2016
 Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer
 Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer
 Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Can We Omit Surgery with Suggestion of pcr by Biopsy in Breast? Fudan University Shanghai Cancer Center Ke-Da Yu, M.D.
 Can We Omit Surgery with Suggestion of pcr by Biopsy in Breast? Fudan University Shanghai Cancer Center Ke-Da Yu, M.D. I have no relevant financial relationship with commercial interests to disclose. More
Can We Omit Surgery with Suggestion of pcr by Biopsy in Breast? Fudan University Shanghai Cancer Center Ke-Da Yu, M.D. I have no relevant financial relationship with commercial interests to disclose. More
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Welcome to. American College of Surgeons. Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar
 Breast Surgical Trial Webinar") American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director Welcome to American College of Surgeons Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar Moderator:
American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director Welcome to American College of Surgeons Clinical Research Program (ACS-CRP) Breast Surgical Trial Webinar Moderator:
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease?
 Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
Spotlights on the surgery role at San Antonio
 Spotlights on the surgery role at San Antonio Riccardo Masetti, MD Professor of Surgery Director, Multidisciplinary Breast Center Catholic University Rome, Italy Roma, 21 maggio 2017 Prof. Masetti has
Spotlights on the surgery role at San Antonio Riccardo Masetti, MD Professor of Surgery Director, Multidisciplinary Breast Center Catholic University Rome, Italy Roma, 21 maggio 2017 Prof. Masetti has
Ultrasound or FNA for Predicting Node Positive in Breast Cancer
 Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Surgical Management of the Axilla
 Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions
 1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
ORIGINAL ARTICLE BREAST ONCOLOGY. Ann Surg Oncol DOI /s
 Ann Surg Oncol DOI 10.1245/s10434-016-5246-8 ORIGINAL ARTICLE BREAST ONCOLOGY How Often Does Neoadjuvant Chemotherapy Avoid Axillary Dissection in Patients With Histologically Confirmed Nodal Metastases?
Ann Surg Oncol DOI 10.1245/s10434-016-5246-8 ORIGINAL ARTICLE BREAST ONCOLOGY How Often Does Neoadjuvant Chemotherapy Avoid Axillary Dissection in Patients With Histologically Confirmed Nodal Metastases?
ARROCase - April 2017
 ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change
 Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
Page 1. AD vs. no AD. Survival. Randomized Trials. All trials reported higher survival in the AD group. Years. Node-NegativeNegative
 Sentinel Node Biopsy: The Past, The Present, and The Future Thomas B. Julian, M.D., F.A.C.S. Associate Professor of Human Oncology Drexel University College of Medicine Director of Breast Surgical Oncology
Sentinel Node Biopsy: The Past, The Present, and The Future Thomas B. Julian, M.D., F.A.C.S. Associate Professor of Human Oncology Drexel University College of Medicine Director of Breast Surgical Oncology
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
Sentinel Lymph Node Biopsy Should be Performed BEFORE Neoadjuvant Chemotherapy
 The London Cancer Alliance West and South Sentinel Lymph Node Biopsy Should be Performed BEFORE Neoadjuvant Chemotherapy Dimitri J Hadjiminas, MD, MPhil, FRCS (Consultant Breast & Endocrine Surgeon Imperial
The London Cancer Alliance West and South Sentinel Lymph Node Biopsy Should be Performed BEFORE Neoadjuvant Chemotherapy Dimitri J Hadjiminas, MD, MPhil, FRCS (Consultant Breast & Endocrine Surgeon Imperial
03/14/2019. Postmastectomy radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D.
 radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy
 Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Update on the Surgical Management of Breast Cancer: What Happens After Imaging?
 Update on the Surgical Management of Breast Cancer: What Happens After Imaging? Henry Kuerer, MD, PhD, FACS Department of Breast Surgical Oncology MD Anderson Cancer Center Outline Limiting and eliminating
Update on the Surgical Management of Breast Cancer: What Happens After Imaging? Henry Kuerer, MD, PhD, FACS Department of Breast Surgical Oncology MD Anderson Cancer Center Outline Limiting and eliminating
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Evaluation of the Axilla Post Z-0011 Trial New Paradigm
 Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Updates on management of the axilla in breast cancer the surgical point of view
 Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Evolution of Regional Nodal Management of Breast Cancer
 Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights
 2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer
 The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Case Conference: Post-Mastectomy Radiotherapy
 Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Relevance. Axillary Node Recurrence. Purpose. Case Presentation: Is axillary staging required? Two trends have emerged:
 Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective
 Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
SABCS ANCO REVIEW. SABCS 2014 Surgery Review. ! Diagnostic workup! Lumpectomy " Local staging, technique, margins
 Frederick M. Dirbas Associate Professor of Surgery, Stanford Univ School of Medicine Physician Leader, Breast Cancer Clinical Care Prgm, Stanford Cancer Institute SABCS 2014 - ANCO REVIEW SABCS 2014 Surgery
Frederick M. Dirbas Associate Professor of Surgery, Stanford Univ School of Medicine Physician Leader, Breast Cancer Clinical Care Prgm, Stanford Cancer Institute SABCS 2014 - ANCO REVIEW SABCS 2014 Surgery
Donna Plecha, MD 1, Shiyu Bai, BS 2, Helen Patterson 3, Cheryl Thompson, PhD 4, and Robert Shenk, MD 5
 Ann Surg Oncol DOI 10.1245/s10434-015-4527-y ORIGINAL ARTICLE BREAST ONCOLOGY Improving the Accuracy of Axillary Lymph Node Surgery in Breast Cancer with Ultrasound-Guided Wire Localization of Biopsy Proven
Ann Surg Oncol DOI 10.1245/s10434-015-4527-y ORIGINAL ARTICLE BREAST ONCOLOGY Improving the Accuracy of Axillary Lymph Node Surgery in Breast Cancer with Ultrasound-Guided Wire Localization of Biopsy Proven
EDITORIAL. Ann Surg Oncol (2011) 18: DOI /s
 18: DOI /s") Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Maria João Cardoso, MD, PhD
 Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Financial Disclosure. Learning Objectives. None. To understand the clinical applicability of the NCDB Breast Cancer PUF
 Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
DOES NEOADJUVANT Rx REALLY DOWN STAGE BR CA? DR KHANYILE DEPARTMENT OF MEDICAL ONCOLOGY, University of Pretoria
 DOES NEOADJUVANT Rx REALLY DOWN STAGE BR CA? DR KHANYILE DEPARTMENT OF MEDICAL ONCOLOGY, University of Pretoria BREAST CA STAGING TNM STAGING: - T x N - x - 0-0 - is - 1-1(1mic/1a/1b/1c) - 2(a/b) - 2-3(a/b/c)
DOES NEOADJUVANT Rx REALLY DOWN STAGE BR CA? DR KHANYILE DEPARTMENT OF MEDICAL ONCOLOGY, University of Pretoria BREAST CA STAGING TNM STAGING: - T x N - x - 0-0 - is - 1-1(1mic/1a/1b/1c) - 2(a/b) - 2-3(a/b/c)
Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing Breast Conserving Surgery
 Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
NEOADJUVANT THERAPY FOR BREAST CANCER: LOCAL EXPERT OPINION AND RECENT EVIDENCE
 NEOADJUVANT THERAPY FOR BREAST CANCER: LOCAL EXPERT OPINION AND RECENT EVIDENCE Dr. Joanne Chiu Medical Oncology Queen Mary Hospital The University of Hong Kong HONG KONG SURVEY FOR NEOADJUVANT THERAPY
NEOADJUVANT THERAPY FOR BREAST CANCER: LOCAL EXPERT OPINION AND RECENT EVIDENCE Dr. Joanne Chiu Medical Oncology Queen Mary Hospital The University of Hong Kong HONG KONG SURVEY FOR NEOADJUVANT THERAPY
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Evolution of Breast Surgery
 Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
ALND. Dr. MJ Vrancken
 ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
Introduction. Approximately 20% of invasive breast cancers
 Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Practice of Axilla Surgery
 Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
What are Adequate Margins of Resection for Breast-Conserving Therapy?
 What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
At many centers in the United States and worldwide,
 ORIGINAL ARTICLES A Declining Rate of Completion Axillary Dissection in Sentinel Lymph Node-positive Breast Cancer Patients Is Associated With the Use of a Multivariate Nomogram Julia Park, MS, Jane V.
ORIGINAL ARTICLES A Declining Rate of Completion Axillary Dissection in Sentinel Lymph Node-positive Breast Cancer Patients Is Associated With the Use of a Multivariate Nomogram Julia Park, MS, Jane V.
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
What the surgeon wants from the radiologist before breast cancer surgery. Erica Patocskai Isabelle Trop
 What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
THE SURGEON S ROLE: THE AXILLA. Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital
 THE SURGEON S ROLE: THE AXILLA Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital What are the concerns with treatment to the axilla Not necessary for
THE SURGEON S ROLE: THE AXILLA Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital What are the concerns with treatment to the axilla Not necessary for
Savitri Krishnamurthy, MD 1
 EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
Lessons Learnt from Neoadjuvant Hormone Therapy. 10 Lessons Learnt from Neoadjuvant Endocrine Therapy. Lesson 1
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy. Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
2017 Topics. Biology of Breast Cancer. Omission of RT in older women with low-risk features
 2017 Topics Biology of Breast Cancer Early-stage HER2+ breast cancer-can we avoid RT? Prediction tools for locoregional recurrence Omission of RT in older women with low-risk features Local-Regional Recurrence
2017 Topics Biology of Breast Cancer Early-stage HER2+ breast cancer-can we avoid RT? Prediction tools for locoregional recurrence Omission of RT in older women with low-risk features Local-Regional Recurrence
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
Neoadjuvant chemotherapy (NACT) in young women with breast cancer. Hanne Melgaard Nielsen, MD Ph.D Department of Oncology, Aarhus University Hospital
 in young women with breast cancer. Hanne Melgaard Nielsen, MD Ph.D Department of Oncology, Aarhus University Hospital") Neoadjuvant chemotherapy (NACT) in young women with breast cancer Hanne Melgaard Nielsen, MD Ph.D Department of Oncology, Aarhus University Hospital Young women according to EUSOMA guidelines Is under
Neoadjuvant chemotherapy (NACT) in young women with breast cancer Hanne Melgaard Nielsen, MD Ph.D Department of Oncology, Aarhus University Hospital Young women according to EUSOMA guidelines Is under