Neutropenic Fever. CID 2011; 52 (4):e56-e93
|
|
|
- Austin Fox
- 5 years ago
- Views:
Transcription
1 Neutropenic Fever CID 2011; 52 (4):e56-e93
2 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected ANC < 500 cells/mm 3 within the next 48 hours
3 65M with AML develops acute fever to C 7 days after completing induction chemotherapy. His peripheral blood WBC count is 1 (x10 3 /mm 3 ) and differential with 50% neutrophils. What is his ANC? A 5 B 50 C 500 D 5000 E Ummm I m bad at math.
4 Calculating ANC 2.3 x 1000 = 2300 x 0.81 = 1863

5 Chemotherapy Induced Neutropenia Severe neutropenia ANC < 100
6
7 Classification Initial neutropenic fever Typically coincides with neutrophil nadir Standard protocol concern for bacterial infection Persistent neutropenic fever Fever despite 4-7 days of empiric antibiotic therapy Complex management concern for fungal infection Recrudescent neutropenic fever Fever that recurs following initial response Wide differential
8 Etiology / Microbiology Infectious (~20%) Bacterial translocation Intestinal Oropharyngeal Community-acquired Respiratory viruses Healthcare-associated MDR organisms, C.diff CLABSI, CAUTI Opportunistic Herpes virus reactivation Fungal Non-infectious Underlying malignancy Blood products Tumor lysis Hematoma Thrombosis Phlebitis Atelectasis Viscus obstruction Drug fever Myeloid reconstitution
9 Clinical Evaluation Symptoms and signs of inflammation may be minimal or absent in the severely neutropenic patient Cellulitis with minimal to no erythema Pulmonary infection without discernable infiltrate on radiograph Meningitis without pleocytosis in the CSF Urinary tract infection without pyuria Peritonitis - abdominal pain without fever or guarding Sickles, Arch Intern Med 1975; 135;715-9
10 The Work Up Physical Exam: Periodontium Palate Lung Abdomen Perineum Skin Tissue around the nails BM biopsy site Blood cultures x2 CXR Targeted workup UA & urine cx C.diff Exit site cultures Catheter tip cultures CT chest CT abdomen/pelvis NP swab (resp virus)

11 Ecthyma Gangrenosum Bacteria: Pseudomonas GNR Staphylococcus aureus Fungus: Aspergillus Fusarium
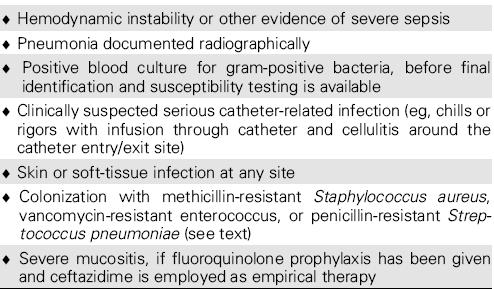
12 Initial Neutropenic Fever Empiric antibiotics: Pseudomonas and Streptococcus coverage INPT: Cefepime OR Zosyn OR Imipenem +/- Aminoglycoside (severe sepsis, significant risk for resistance) +/- Vancomycin OUTPT: Augmentin + Cipro Bacterial etiology: Gram-negative organisms Pseudomonas aeruginosa, E. coli, Klebsiella Gram-positive organisms Coag neg Staph, Viridans Streptococcus, MRSA Corynebacterium jeikeium

13 65M with AML admitted for induction chemo. PICC line placed on admission. Develops neutropenia on HD#12 and fever to C on HD#15. Patient notes some chills but no other complaints. No recent antibiotic use. Exam unremarkable other than P108. CXR negative. Blood cultures performed. Next best step in management? A B C D E Observe off antibiotics Start levofloxacin Start cefepime Start vanco + cefepime Start vanco + cefepime + gent

14 Empiric Vancomycin Randomized trials comparing regimens with and without vancomycin for empiric therapy of initial neutropenic fever - no mortality benefit, no reduction in duration of fever.
15 Empiric Vancomycin
16 65M with AML admitted for induction chemo. PICC line placed on admission. HD#12 neutropenia. HD#15 Tm C. Exam: P108, lethargic/confused. CXR negative. Patient started on vanco + cefepime + gent. HD#17 still febrile C x 2d, but mental status back to baseline. D15 and D16 BCxs remain negative. Next best step in management? A B C D E Stop vanco Change cefepime to imipenem Switch to linezolid, imipenem, tobra Add micafungin Continue current regimen
17 Antimicrobial Modification Vancomycin can cause nephrotoxicity especially with trough levels > 15. Synergistic nephrotoxicity with vancomycin in combination with aminoglycosides.
18 65M AML admit for induction chemo. PICC line placed. HD#12 neutropenia. HD#15 Tm C. Exam: P108, lethargic/confused. CXR negative. Patient started on vanco + cefepime + gent. HD#17 still febrile C x 2d, but MS back to baseline. D15 BCxs positive for pan-sensitive E.coli (2 of 2 sets + at same time). D16 BCxs negative. Next best step in management? A B C D E Continue current regimen Switch current regimen to ceftriaxone D/C vanco, continue cefepime and gent D/C vanco and gent, continue cefepime Pull PICC line, continue cefepime only
19 Antimicrobial Modification De-escalation of empiric antimicrobial therapy = avoid anti-pseudomonals Piperacillin/Tazobactam Cefepime Imipenem
20 Management Algorithm Neutropenic Fever Do I need vanco? Vanco + Anti-Pseudomonal Anti-Pseudomonal UNIDENTIFIED organism/infection IDENTIFIED organism/infection D/C vanco D/C AG Remains febrile De-escalate abxs Patient stable No abx changes Patient unstable Needs further E&M Patient stable No abx changes
21 Early Management Summary D/C vanco after 48 hours if no evidence of GP infection. No need to perform more BC after first hours if patient clinically stable and no new symptoms. Can simplify regimen if organism isolated. No need to double cover Pseudomonas if sensitive to monotherapy. Median time to defervescence ~5 days. Treatment duration typically until ANC > 500. If clinical worsening: Aggressive diagnostics Modify antibiotics to cover for resistant organisms Start anti-candida therapy
22 65M AML admit induction chemo. PICC line placed. HD#12 neutropenia. HD#15 Tm C. Exam: OK. CXR neg. Patient started on cefepime. HD#17 still febrile C x 2d. D15 & D16 BCxs negative. HD#20 still febrile but clinically unchanged. Next best step in management? A B C D E Stop all antibiotics due to drug fever Switch to linezolid, imipenem, tobra Add on micafungin Obtain CT chest/abd/pelvis Call ID

23 Antifungal Therapy Most common fungal infections = Candida and Aspergillus Candida: - can occur early in the course of neutropenic fever - primary manifestation = bloodstream infection Aspergillus: - severe neutropenia lasting at least days - primary manifestation = sinus and/or lung infection


24 Fungus 101 YEAST: Candida, Cryptococcus MOLD: Aspergillus, Mucor


25 Invasive Mold Aspergillus Zygomyces Mucor Rhizopus Absidia Fusarium Halo sign Air crescent sign Halo sign, air crescent sign, cavitating nodule Invasive mold Abnormal CT chest BAL with biopsy or IR guided biopsy

26 65M AML s/p induction chemo. Developed neutropenic fever HD#12 treated with cefepime and defervesced. Doing well but still neutropenic. HD#24 spikes new fever and CT chest performed. BAL with negative GS, fungal and AFB stains. Cultures pending.

27 65M AML admit induction chemo. PICC line placed. HD#7 neutropenia. HD#10 Tm C. Exam: OK. CXR neg. Defervesces on cefepime. HD#25 Tm 39 0 C, chest pain. Blood cxs obtained. CT chest with halo sign. What is the next best step in management? A B C D E Start vanco Wait for culture results Add on micafungin Add on voriconazole Add on lipid amphotericin
28 Anti-Fungal Therapy Empiric: Normal CT chest and/or sinus Non-specific infiltrate on CT chest No other evidence of invasive fungus USE: Echinocandin or Amphotericin Presumed or Definite Invasive Aspergillus: Classic CT chest findings (no previous Voriconazole) Positive culture or biopsy with typical hyphae Positive Galactomannan USE: Voriconazole


29 65M AML s/p induction chemo. Develops neutropenic fever HD#12 with RLQ abdominal pain and diarrhea. Stool C.diff PCR negative. Blood cxs results pending, CT AP with findings below: Colonic wall thickening from cecum to transverse colon
30 AML neutropenic fever HD#12. Patient with RLQ abdominal pain and diarrhea. Stool Cdiff PCR negative. CT Abd/Pelvis with colonic wall thickening. What is the next best step in management? A B C D E Vanco (IV), cefepime, tobramycin Vanco (PO) and cefepime Cefepime and fluconazole Zosyn Vanco (IV & PO), Zosyn, Micafungin
31 Neutropenic Colitis Typhlitis ANC < 500, usually AML Abdominal pain Diarrhea initially, ileus later CT or US with bowel wall thickening Rule-out C.diff Need anaerobic coverage: Zosyn, Imipenem, Cefepime + Metronidazole
32 Summary Neutropenic fever definition and classification High risk versus Low risk Initial, Persistent, Recrudescent Microbiology Bacterial translocation, CAI, HAI, opportunistic Clinical evaluation Neutropenia = lack of inflammation Management Initial NF need Pseudomonas and Strep coverage Vanco NOT routinely indicated De-escalate empiric therapy after hours Persistent/Recrudescent NF think fungal infection Duration until ANC > 500
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Use of Antifungal Drugs in the Year 2006"
 Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
Use of Antifungal Drugs in the Year 2006" Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Interactive Cases. Victor Tseng, MD
 Interactive Cases Victor Tseng, MD WHO HAS A NEUTROPENIC FEVER? 61 M ANC 800 + T 38.9 being treated for stage IIIA CRC 22 F ANC 120 + T 37.0 getting consolidation for ALL 53 F ANC 580 (710 yesterday)
Interactive Cases Victor Tseng, MD WHO HAS A NEUTROPENIC FEVER? 61 M ANC 800 + T 38.9 being treated for stage IIIA CRC 22 F ANC 120 + T 37.0 getting consolidation for ALL 53 F ANC 580 (710 yesterday)
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Use of Antifungals in the Year 2008
 Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Use of Antifungals in the Year 2008 Jose G. Montoya, MD Associate Professor of Medicine Associate Chief for Clinical Affairs Division of Infectious Diseases Stanford University School of Medicine Diagnosis
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
UPDATE ON FEBRILE NEUTROPENIA
 UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
UPDATE ON FEBRILE NEUTROPENIA Clinical approach and management Dr.Shafiq A. Alimad Head of medical department at university of science and technology hospital YICID 15-December-2014 INTRODUCTION Cancer
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Common Fungi. Catherine Diamond MD MPH
 Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Common Fungi Catherine Diamond MD MPH Birth Month and Day & Last Four Digits of Your Cell Phone # BEFORE: http://tinyurl.com/kvfy3ts AFTER: http://tinyurl.com/lc4dzwr Clinically Common Fungi Yeast Mold
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Note: Page numbers of article titles are in boldface type. A AAP. See American Academy of Pediatrics (AAP) Acyclovir dosing in infants, 185 187 American Academy of Pediatrics (AAP) COFN of, 199 204 Amphotericin
Antimicrobial Management of Febrile Neutropenic Sepsis
 Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Antimicrobial Management of Febrile Neutropenic Sepsis Written by: Dr J Joseph, Consultant Haematologist Dr K Gajee, Consultant Microbiologist Amended by: Larissa Claybourn, Antimicrobial Pharmacist Date:
Fungal Infections: Reporting. Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center
 Fungal Infections: Management and Reporting Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center February 25, 2010 Objectives Review common fungal infections in HCT patients Review current available
Fungal Infections: Management and Reporting Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center February 25, 2010 Objectives Review common fungal infections in HCT patients Review current available
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008
 Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Shannon Carty, PGY-2 ICCR IRB Project Proposal April 9, 2008 Study Title: Observational Study to Determine the Effect of an Emergency Department Adult Oncology Stat Antibiotic Protocol on Clinical Outcomes
Neutropenic Sepsis Guideline
 Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Neutropenic Sepsis Guideline Neutropenic Sepsis Guideline - definitions Suspected or proven infection in a neutropenic patient is a MEDICAL EMERGENCY and is an indication for immediate assessment and prompt
Fever Without a Source Age: 0-28 Day Pathway - Emergency Department Evidence Based Outcome Center
 Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
Age: 0-28 Day Pathway - Emergency Department EXCLUSION CRITERIA Toxic appearing No fever Born < 37 weeks gestational age INCLUSION CRITERIA Non-toxic with temperature > 38 C (100.4 F) < 36 C (96.5 F) measured
ID Emergencies. BGSMC Internal Medicine Edwin Yu
 ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BGSMC Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
Fever. National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital
 Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Fever National Pediatric Nighttime Curriculum Written by Debbie Sakai, M.D. Institution: Lucile Packard Children s Hospital Case 1 4-month-old well-appearing girl admitted for croup and respiratory distress.
Ready to answer the questions?
 파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
파워포인트문서의제목 Reference 1. IDSA GUIDELINES. Clinical Practice Guidelines for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Disease Society of America.
Is pre-emptive therapy a realistic approach?
 Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Is pre-emptive therapy a realistic approach? J Peter Donnelly PhD, FRCPath Department of Haematology Radboud University Nijmegen Medical Centre Nijmegen, The Netherlands Is pre-emptive therapy a realistic
Pneumonia in the Immunocompromised Host
 SIOP PODC Supportive Care Education Presentation Date: 26 th October 2015 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p1bk39ernlb Pneumonia in
SIOP PODC Supportive Care Education Presentation Date: 26 th October 2015 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p1bk39ernlb Pneumonia in
Febrile neutropenia. Febrile neutropenia. Febrile neutropenia. Febrile neutropenia 1/30/2019. Infection in patients with cancer
 Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Manit Sae-teaw B.Pharm, BCP, BCOP Glad dip in pharmacotherapy Faculty of pharmaceutical sciences Ubon Ratchathani University Fever Oral temperature measurement of 38.3 C (101.0 F) single 38.0 C (100.4
Advanced Pediatric Emergency Medicine Assembly
 (+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
(+)Joan Shook, MD, FACEP Professor of Pediatrics, Baylor College of Medicine; Chief Safety Officer and Chief Clinical Information Officer, Texas Children's Hospital Advanced Pediatric Emergency Medicine
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines
 Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
Cystic Fibrosis: Pulmonary Exacerbations Management Guidelines Inclusion Criteria: Age 1 year with cystic fibrosis admitted for a pulmonary exacerbation. Exclusion Criteria: ICU Admission Newborn with
Objec&ves. Clinical Presenta&on
 Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
Michelle A. Barron, MD Associate Professor of Medicine Division of Infectious Diseases University of Colorado Denver Objec&ves Determine who is at risk for invasive candidiasis. Understand whether prophylaxis
Case Studies in Fungal Infections and Antifungal Therapy
 Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Case Studies in Fungal Infections and Antifungal Therapy Wayne L. Gold MD, FRCPC Annual Meeting of the Canadian Society of Internal Medicine November 4, 2017 Disclosures No financial disclosures or industry
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association
 Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
IDSA GUIDELINES Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America Alison G. Freifeld, 1 Eric
Things your mother never told you about antibiotics, UTI s, and Pneumonia. Rob Kaplan, MD July 12 and 14, 2017
 Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases. Y.L. Kwong Department of Medicine University of Hong Kong
 Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Prophylaxis versus Diagnostics-driven approaches to treatment of Invasive fungal diseases Y.L. Kwong Department of Medicine University of Hong Kong Pathogenic yeast Candida Cryptococcus Trichosporon Pathogenic
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Infections in Non-HIV Immunocompromised Hosts
 Infections in Non-HIV Immunocompromised Hosts Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
Infections in Non-HIV Immunocompromised Hosts Fredrick M. Abrahamian, D.O., FACEP Associate Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA
8/11/2015. Febrile neutropenia Bone marrow transplant Immunosuppressant medications
 Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Dean Van Loo Pharm.D. Febrile neutropenia Bone marrow transplant Immunosuppressant medications Steroids Biologics Antineoplastic Most data from cancer chemotherapy Bone marrow suppression Fever is the
Top 5 papers in clinical mycology
 Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
Top 5 papers in clinical mycology Dirk Vogelaers Department of General Internal Medicine University Hospital Ghent Joint symposium BVIKM/BSIMC and SBMHA/BVMDM Influenza-associated aspergillosis in critically
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
 MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSP There are no translations available. MANAGEMENT OF FEVER IN PEDIATRIC PATIENTS FOLLOWING HEMATOPOIETIC STEM CELL TRANSPLANTATION
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
ID Emergencies. BUMC-P Internal Medicine Edwin Yu
 ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
ID Emergencies BUMC-P Internal Medicine Edwin Yu Learning Objectives Bacterial meningitis IDSA guidelines: Clin Infect Dis 2004; 39:1267-84 HSV encephalitis IDSA guidelines: Clin Infect Dis 2008; 47:303-27
PROGRESSI NELLA TERAPIA ANTIFUNGINA. A tribute to Piero Martino
 PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
PROGRESSI NELLA TERAPIA ANTIFUNGINA A tribute to Piero Martino 1946-2007 ITALIAN ICONS IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI IERI, OGGI, E DOMANI 1961 CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES
Bad Bugs in the Blood!
 Bad Bugs in the Blood! How to Work Up and Treat Bloodstream Infections Sharanjeet Thind M.D. Director of Inpatient Infectious Diseases, VA Medical Center Assistant Professor of Medicine, OUHSC, College
Bad Bugs in the Blood! How to Work Up and Treat Bloodstream Infections Sharanjeet Thind M.D. Director of Inpatient Infectious Diseases, VA Medical Center Assistant Professor of Medicine, OUHSC, College
Mortality Rate was unsightly!!! 4/24/2013. Sepsis Quality Improvement Project
 Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Libby, MT Sepsis Quality Improvement Project Barb Dumont RN, Director of Quality and Risk Management Mike Julius RN, ED Manager Cathy Wolfe RN, Chief Nursing Officer. Mortality Rate was unsightly!!! percent
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Invasive Pulmonary Aspergillosis in
 Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
Infection & Sepsis Symposium Porto, April 1-3, 2009 Invasive Pulmonary Aspergillosis in Non-Immunocompromised Patients Stijn BLOT, PhD General Internal Medicine & Infectious Diseases Ghent University Hospital,
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS
 MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
MANAGEMENT OF HOSPITAL-ACQUIRED FUNGAL INFECTIONS Paul D. Holtom, MD Associate Professor of Medicine and Orthopaedics USC Keck School of Medicine Numbers of Cases of Sepsis in the United States, According
Top Curbside Consult Questions in Inpatient ID
 Top Curbside Consult Questions in Inpatient ID Management of the Hospitalized Patient October 2014 Jennifer Babik, MD, PhD Assistant Clinical Professor Division of Infectious Diseases, UCSF Disclosures
Top Curbside Consult Questions in Inpatient ID Management of the Hospitalized Patient October 2014 Jennifer Babik, MD, PhD Assistant Clinical Professor Division of Infectious Diseases, UCSF Disclosures
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Febrile Neutropenia. These podcasts are designed to give medical students an overview of key topics in pediatrics. The
Ailyn T. Isais-Agdeppa, MD*, Lulu Bravo, MD*
 A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
A FIVE-YEAR RETROSPECTIVE STUDY ON THE COMMON MICROBIAL ISOLATES AND SENSITIVITY PATTERN ON BLOOD CULTURE OF PEDIATRIC CANCER PATIENTS ADMITTED AT THE PHILIPPINE GENERAL HOSPITAL FOR FEBRILE NEUTROPENIA
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital
 Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS
 ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS COMMERCIAL RELATIONS DISCLOSURE 2500 9000 15000 Astellas Gilead Sciences Pfizer Inc Expert advice Speaker s bureau Speaker s bureau OUTLINE OF THE PRESENTATION
ADEQUATE ANTIFUNGAL USE FOR BLOODSTREAM INFECTIONS COMMERCIAL RELATIONS DISCLOSURE 2500 9000 15000 Astellas Gilead Sciences Pfizer Inc Expert advice Speaker s bureau Speaker s bureau OUTLINE OF THE PRESENTATION
Neutropenic Fever 1 InpatientPediatric Treatment
 Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
Neutropenic Fever InpatientPediatric Treatment (Hematologic Cancers and Stem Cell Patients) te: This algorithm should not be used for patients receiving CAR cell therapy. Page of 8 Patient presents with
HAEMATOLOGY ANTIFUNGAL POLICY
 HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
HAEMATOLOGY ANTIFUNGAL POLICY PROPHYLAXIS Primary Prophylaxis Patient Group Patients receiving intensive remissioninduction chemotherapy for Acute Leukaemia (excluding patients receiving vinca alkaloids)
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital
 Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital Introduction Nosocomial bacteriuria or candiduria develops in up to 25%
Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital Introduction Nosocomial bacteriuria or candiduria develops in up to 25%
The EM Educator Series
 The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
The EM Educator Series The EM Educator Series: Why is my patient with gallbladder pathology so sick? Author: Alex Koyfman, MD (@EMHighAK) // Edited by: Brit Long, MD (@long_brit) and Manpreet Singh, MD
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host
 Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
Diagnostic Procedures for Pulmonary Infiltrates in the Compromised Host Michael Douvas, MD Heme/Onc Gerald Donowitz, MD - ID Eric Davis, MD - Pulmonary Disclosure Drs. Davis, Donowitz, and Douvas do not
PAGL Inclusion Approved at January 2017 PGC
 Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
Guideline for the prophylaxis and treatment of fungal infections in Haematology patients 1. Introduction PAGL Inclusion Approved at January 2017 PGC Haematology, CHUGGS June 2016 This guideline sets out
Guideline for the Management of Fever and Neutropenia in Children with Cancer and/or Undergoing Hematopoietic Stem-Cell Transplantation
 Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
Guideline for the Management of Fever Neutropenia in Children with Cancer /or Undergoing Hematopoietic Stem-Cell Transplantation COG Supportive Care Endorsed Guidelines Click here to see all the COG Supportive
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
The McMaster at night Pediatric Curriculum Community Acquired Pneumonia Based on CPS Practice Point Pneumonia in healthy Canadian children and youth and the British Thoracic Society Guidelines on CAP Objectives
ECMM Excellence Centers Quality Audit
 ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
ECMM Excellence Centers Quality Audit Person in charge: Department: Head of Department: Laboratory is accredited according to ISO 15189 (Medical Laboratories Requirements for quality and competence) Inspected
Infections in acute leukemia in Indian Children
 Journal of College of Medical Sciences-Nepal, 2013, Vol-9, No-1, 40-47 Infections in acute leukemia in Indian Children Original Article B Roy, 1 A Biswas, 2 A Chaterjee, 3 A Pan 4, K Basu 5 1 Associate
Journal of College of Medical Sciences-Nepal, 2013, Vol-9, No-1, 40-47 Infections in acute leukemia in Indian Children Original Article B Roy, 1 A Biswas, 2 A Chaterjee, 3 A Pan 4, K Basu 5 1 Associate
Disclosures. Background. Definitions. Why Worry about these Infants? Goals. Bacterial infection in the neonate and young infant: a review
 Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
Disclosures Bacterial infection in the neonate and young infant: a review Russell J. McCulloh, MD Med-Peds Infectious Diseases August 8, 2017 I have no financial interests to disclose Funding: Eva and
SUPPLEMENT ARTICLE DEFINITIONS
 SUPPLEMENT ARTICLE The Infectious Diseases Society of America 2002 Guidelines for the Use of Antimicrobial Agents in Patients with Cancer and Neutropenia: Salient Features and Comments Kenneth V. I. Rolston
SUPPLEMENT ARTICLE The Infectious Diseases Society of America 2002 Guidelines for the Use of Antimicrobial Agents in Patients with Cancer and Neutropenia: Salient Features and Comments Kenneth V. I. Rolston
When is failure failure?
 When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
When is failure failure? Bart-Jan Kullberg, M.D. Radboud University Nijmegen The Netherlands The ICU patient with candidemia!! Female, 39 years old!! Multiple abdominal surgeries for Crohn's disease!!
Ceftizoxime in the treatment of infections in patients with cancer
 Journal of Antimicrobial Chemotherapy (98), Suppl. C, 67-73 Ceftizoxime in the treatment of infections in patients with cancer V. Fainstein, R. Bolivar,. Elting, M. Valdivieso and G. P. Bodey Department
Journal of Antimicrobial Chemotherapy (98), Suppl. C, 67-73 Ceftizoxime in the treatment of infections in patients with cancer V. Fainstein, R. Bolivar,. Elting, M. Valdivieso and G. P. Bodey Department
INTRA-ABDOMINAL INFECTIONS
 INTRA-ABDOMINAL INFECTIONS Learning Objectives: 1. Describe patient risk factors, signs and symptoms that may indicate an intra-abdominal infection 2. Identify tests and significant laboratory values used
INTRA-ABDOMINAL INFECTIONS Learning Objectives: 1. Describe patient risk factors, signs and symptoms that may indicate an intra-abdominal infection 2. Identify tests and significant laboratory values used
Pneumonia. Definition of pneumonia Infection of the lung parenchyma Usually bacterial
 Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Pneumonia Definition of pneumonia Infection of the lung parenchyma Usually bacterial Epidemiology of pneumonia Commonest infectious cause of death in the UK and USA Incidence - 5-11 per 1000 per year Worse
Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections. Presenter. Disclosures
 Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections Presenter James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University
Evidence-Based Approaches to the Safe and Effective Management of Invasive Fungal Infections Presenter James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University
The Febrile Infant. SJRH ED Rounds Dec By: Robin Clouston
 1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
1 The Febrile Infant SJRH ED Rounds Dec 11 2018 By: Robin Clouston 2 Objectives Discuss the risk of serious bacterial infection (SBI) in the neonate or young infant (
Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing
 Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing October 11, 2017 Paul Lewis, PharmD, BCPS (AQ-ID) Johnson City Medical Center Johnson City, TN 1 Outline Introduction to stewardship
Think Globally: Strategies to Improve the Culture of Antibiotic Prescribing October 11, 2017 Paul Lewis, PharmD, BCPS (AQ-ID) Johnson City Medical Center Johnson City, TN 1 Outline Introduction to stewardship
FEBRILE NEUTROPENIA CURRENT GUIDELINES FOR CHILDREN Alia Zaidi, MD. St. Jude International Outreach Program
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 Recording Link at www.cure4kids.org: https://www.cure4kids.org/ums/home/conference_rooms/enter.php?room=p25oti35nt7
Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy.
, including Antibiotic Lock Therapy.") Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy. Written by: Dr K Gajee, Consultant Microbiologist Date: June 2017 Approved by: Drugs & Therapeutics Committee
Management of Catheter Related Bloodstream Infection (CRBSI), including Antibiotic Lock Therapy. Written by: Dr K Gajee, Consultant Microbiologist Date: June 2017 Approved by: Drugs & Therapeutics Committee
Antifungal Update 2/22/12. Which is the most appropriate initial empirical therapy in a candidemic patient?
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco 3/3 blood cultures are positive for an unidentified
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco 3/3 blood cultures are positive for an unidentified
An Update in the Management of Candidiasis
 An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
An Update in the Management of Candidiasis Daniel B. Chastain, Pharm.D., AAHIVP Infectious Diseases Pharmacy Specialist Phoebe Putney Memorial Hospital Adjunct Clinical Assistant Professor UGA College
Fungal infection in the immunocompromised patient. Dr Kirsty Dodgson
 Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Fungal infection in the immunocompromised patient Dr Kirsty Dodgson Aims Discuss different types of fungi Overview of types of clinical infections Clinical Manifestations Fungus Includes Moulds Aspergillus
Antifungal Update. Candida: In Vitro Antifungal Susceptibility Testing
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Fungal Infection Post-Infusion Data
 Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Fungal Infection Post-Infusion Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: Event date: / / Visit: 100 day 6 months 1 year 2 years >2 years. Specify: CIBMTR Form 2146 revision
Fungal infections in ICU. Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia
 Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
Fungal infections in ICU Tang Swee Fong Department of Paediatrics Universiti Kebangsaan Malaysia Epidemiology of invasive fungal infections - US +300% Martin GS, et al. N Engl J Med 2003;348:1546-1554
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
TOWARDS PRE-EMPTIVE? TRADITIONAL DIAGNOSIS. GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% β-d-glucan Neg Predict Value 100% PCR
 TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
TOWARDS PRE-EMPTIVE? GALACTOMANNAN Sensitivity 61% Specificity 93% Neg Predict Value >95% TRADITIONAL DIAGNOSIS β-d-glucan Neg Predict Value 100% PCR diagnostics FUNGAL BURDEN FIRST TEST POSITIVE FOR ASPERGILLOSIS
Severe and Tertiary Peritonitis
 Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
+ Objectives. n Define who is at risk for SBI. n Clarify risk stratification. n Provide treatment guidelines. n Bust some myths
 Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Objectives n Define wo is at risk for SBI n Clarify risk stratification n Provide treatment guidelines Neonatal Fever Benjamin B. Constance, MD, FAWM n Bust some myts Based on Case wat do you want to know?
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA
 Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA 43 Case 3: probability split! Gram variable, grows on BA, MAC, barely on CHOC Oxidase positive Vitek: probability split, Acinetobacter
Case 3: what grew? BA Gram stain morphology Mucoid colonies on BA 43 Case 3: probability split! Gram variable, grows on BA, MAC, barely on CHOC Oxidase positive Vitek: probability split, Acinetobacter
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Acute Cholangitis. Kelsey Knotts PharmD Candidate Class of 2016
 Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Acute Cholangitis Kelsey Knotts PharmD Candidate Class of 2016 Learning Objectives 1. Describe the mechanism of the development of acute cholangitis 2. Identify common causative organisms in acute cholangitis
Guidelines in the Management of Febrile Neutropenia for Clinical Practice
 REFERENCES 1. Tangka FK, Trogdon JG, Richardson LC, Howard D, Sabatino SA, Finkelstein EA. Cancer treatment cost in the United States: has the burden shifted over time? Cancer. 2010;116(14):3477-3484.
REFERENCES 1. Tangka FK, Trogdon JG, Richardson LC, Howard D, Sabatino SA, Finkelstein EA. Cancer treatment cost in the United States: has the burden shifted over time? Cancer. 2010;116(14):3477-3484.
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS. Part I: EMPIRICAL THERAPY
 TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
TREATMENT STRATEGIES FOR INVASIVE FUNGAL INFECTIONS Part I: EMPIRICAL THERAPY CAUSES OF DEATH IN PATIENTS WITH MALIGNANCIES NIJMEGEN, THE NETHERLANDS n = 328 BACTERIAL INFECTION FUNGAL INFECTION 7% 36%
ISF criteria (International sepsis forum consensus conference of infection in the ICU) Secondary peritonitis
 Secondary peritonitis") Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Appendix with supplementary material. This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Supplementary Tables Table S1. Definitions
Antifungal Update 2/24/11. Which is the most appropriate initial empirical therapy in a candidemic patient?
 Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Antifungal Update B. Joseph Guglielmo, Pharm.D. Professor and Chair Department of Clinical Pharmacy School of Pharmacy University of California San Francisco The patient spikes a new fever and 3/3 blood
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014
 Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
Good Morning! Welcome Applicants! FRIDAY, N OVEMBER, 7 TH 2014 Prep Question You are camping with a group of boys at a rural campground in the southeastern Unites States when one of the campers is bitten
9/7/2018. Faculty. Overcoming Challenges in the Management of Invasive Fungal Infections. Learning Objectives. Faculty Disclosure
 Faculty Overcoming Challenges in the Management of Invasive Fungal James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University Departments of Pharmacy and Infectious
Faculty Overcoming Challenges in the Management of Invasive Fungal James S. Lewis II, PharmD, FIDSA ID Clinical Pharmacy Coordinator Oregon Health and Science University Departments of Pharmacy and Infectious
Fungal Infections in Neutropenic Hematological Disorders
 Fungal Infections in Neutropenic Hematological Disorders 23 Dr Farah Jijina 24 Fungal Infections in Neutropenic Hematological Disorders 25 Dr Farah Jijina 26 Fungal Infections in Neutropenic Hematological
Fungal Infections in Neutropenic Hematological Disorders 23 Dr Farah Jijina 24 Fungal Infections in Neutropenic Hematological Disorders 25 Dr Farah Jijina 26 Fungal Infections in Neutropenic Hematological
Fever in neonates (age 0 to 28 days)
") Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Fever in neonates (age 0 to 28 days) INCLUSION CRITERIA Infant 28 days of life Temperature 38 C (100.4 F) by any route/parental report EXCLUSION CRITERIA Infants with RSV Febrile Infant 28 days old Ill
Infectious Disease in the Critically Ill Patient
 Infectious Disease in the Critically Ill Patient Heather L. Evans, MD MS FACS Director of Surgical Infectious Disease Harborview Medical Center Asst. Professor UW Department of Surgery New Antibiotics:
Infectious Disease in the Critically Ill Patient Heather L. Evans, MD MS FACS Director of Surgical Infectious Disease Harborview Medical Center Asst. Professor UW Department of Surgery New Antibiotics: