RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer
|
|
|
- Dwight Phillips
- 5 years ago
- Views:
Transcription
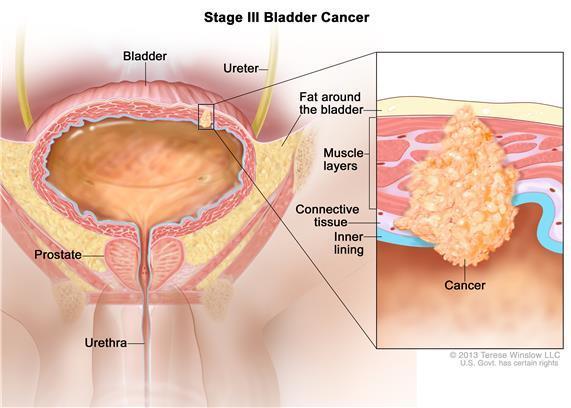
1 RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer IX CIS and EURASIA ONCOLOGY and RADOLOGY CONGRESS, ONCOUROLOGY SESSION 16 June 2016 Richard E Greenberg, MD, FACS Chief Urologic Oncology, Fox Chase Cancer Center Professor of Urology, Lewis Katz School of Medicine at Temple University, Philadelphia, Pennsylvania, USA

2 Fox Chase Cancer Center Philadelphia, PA., USA
:575.")
3 Epidemiology 75,000 new cases and 16,000 deaths in 2014 Number increased > 50% in the US ( ) 3-4 times more common in men Whites twice as often as AA Highest incidence in the Northeast US and least in Hawaii and Utah Median age at diagnosis: 69 in men and 71 in women Int J Cancer. 2001;91(4):575.
4 Risk factors 50% of all cases caused by smoking for both men and women (HR 3.89 and 4.65) 20% of all cases has occupational exposure: aromatic amines, benzidine and their derivatives (metal workers, painters, rubber industry, leather workers, electrical workers, miners, cement workers, transport operators) 5 fold increase was observed in subjects who worked for > 10 years as hairdressers or barbers in LA Chronic cystitis (squamous cell) Schistosoma haematobium, Foley FAMILIAL: HEREDITARY NONPOLYPOSIS COLORECTAL CANCER (LYNCH II) Iatrogenic: Radiation (controversial) Cyclophosphamide (4.5-fold increased risk of bladder cancer ) Phenacetin (increased risk of TCC renal pelvis) Pioglitazone (Actos)
5 Clinical Presentation & Diagnosis Hematuria (intermittent, gross, painless, and present throughout micturition) 12% incidence of bladder cancer ( Urol. 2000;163(2):524). Pain advanced disease Voiding symptoms (irritative or obstructive) DIAGNOSIS: UA Urine cytology (false-positive results are rare) Cystoscopy => the gold standard (often multifocal the entire urothelium needs to be evaluated if a tumor is found) Imaging ( CT urogram) For patients with confirmed muscle-invasive bladder cancer, CT CAP is the optimal form of staging, including CT urogram for complete radiologic evaluation of the upper urinary tracts
6 Pathology Urothelial TCC (low-grade and high-grade) 90% BLADDER (94%) RENAL PELVIS (5%) URETER (1%) Multicentric and bilateral (up to 10%) Up to 50% of upper tract Ca will develop bladder Ca Squamous (5%) Adenocarcinoma (1-2% ) Small cell Sarcomas

7 Bladder Cancer o non-muscle-invasive or superficial (NMIBC) 70% - 75% of patients (i.e., stage Ta, Tis, or T1) In the absence of muscularis propria in the specimen, data suggests that 20-40% of patients will have either residual tumor and/or unrecognized muscle invasive disease => repeated biopsy is mandatory! (Guidelines) o muscle-invasive (MIBC) o metastatic

8 NMIBC
9 Treatment options for NMIBC Standard treatment options: o TUR with fulguration recurrence after initial resection around 80% o TUR with fulguration followed by intravesical chemotherapy epirubicin, mitomycin C, thiotepa, pirarubicin reduced the odds of recurrence by 39% o TUR with fulguration followed by intravesical chemotherapy followed by BCG an induction phase of six weekly treatments followed by three weekly treatment every 3 months CR rates of about 70%, Decreasing the need for salvage cystectomy No survival advantage Risk factors for recurrence and progression are: o High-grade o CIS o Tumor > 3 cm o Multiple tumors o History of prior bladder cancer

10 MIBC
11 Treatment for MIBC (stage II - III) 1. Neoadjuvant chemo, followed by radical cystectomy 2. Radical cystectomy (? +/- adjuvant chemo or RT) 3. EBRT plus concomitant chemo 4. EBRT alone
12 Neoadjuvant Chemotherapy BA trial (Medical Research Council and the EORTC) J Clin Oncol 29 (16): , patients with T2 T4a disease randomized to - definitive treatment (surgery or RT) - 3 cycles of neoadjuvant cisplatin, vinblastine, and methotrexate RESULTS: - Median follow-up of 8.0 years OS was significantly greater (HR 0.84, P =.037). - The survival benefit 6% absolute increase SWOG study NEJM 349 (9): , patients with stage T2 to stage T4a a) 3 cycles of neoadjuvant MVAC b) cystectomy RESULTS: - 5-year OS was 57% vs 43% (two-sided P value =.06). - No deaths were associated with neoadjuvant chemotherapy and preoperative chemotherapy did not prevent cystectomy - 38% had a pathologic CR - 85% of those achieving a pathologic CR were alive at 5 years
13 Neoadjuvant chemo Meta-analysis (Lancet 361 (9373): , 2003) 2,688 pts, 10 randomized trials of neoadjuvant chemo cisplatin-based chemotherapy was associated with a significant 13% relative reduction in the risk of death and resulted in an improvement in 5-year survival from 45% to 50% (P =.016) Meta-analysis (A. J Urol 171 (2 Pt 1): 561-9, 2004) 2605 pts, 11 randomized controlled trials eight trials that used multiagent, cisplatin-based chemotherapy, neoadjuvant chemotherapy was associated with a 6.5% absolute benefit in 5-year OS (50% vs. 56.5%; P =.006)




14 Neoadjuvant Chemotherapy is Standard of Care for MIBC Magnitude of benefit similar to adjuvant 5FU therapy for CRC, which is widely accepted International Standard of Care (Level 1) Bajorin et al, JCO, Eur Urol 48, 202 (Aug, 2005).
15 yet underutilized National database query only 11.6% of stage III patients received perioperative chemotherapy Survey of 14 academic centers only 35% received perioperative chemotherapy Of these, 30% neoadjuvant, 60% adjuvant Of the neoadjuvant patients, only 65% received cisplatin Commonly cited reason is time (delay to surgery) and perceived toxicity David et al. J Urol, 2007 Feifer. GU ASCO 2011
16 von der Maase et al. J Clin Oncol, 2000 What is standard neoadjuvant chemotherapy? Cisplatin based Prospective neoadjuvant studies used conventional MVAC or CMV regimens Data in the metastatic setting showed similar outcomes with GC vs. conventional MVAC, but less neutropenic fever/sepsis with GC. In practice GC is more commonly used, despite lack of prospective neoadjuvant data NCCN guidelines currently list GC, CMV or accelerated/dose dense MVAC as options Conventional MVAC is no longer recommended


17
18 Phase II Clinical Trial of Neoadjuvant AMVAC in MIBC Hypothesis: AMVAC will yield similar pt0 rate to standard MVAC with shorter time to surgery and less toxicity Primary Objective To asses the rate of complete response (pt0) at surgery Secondary Objectives Toxicity, Overall Survival, Correlative Studies Inclusion Clinical stage: T2-T4a, cn0-n1 Candidate for surgery PS 0 or 1 EF normal CrCl > 50 ml/min (measured or calculated) Exclusion Any 100% non urothelial histology Any component of small cell carcinoma Previous systemic chemotherapy Neuropathy > Gr 1








19 Pathologic Response T3, T4, N+ 35% T0 38% T2 13% T1 8% Tis Ta 8%
20 Summary Collective experience in the neoadjuvant and metastatic setting shows AMVAC to be safe Q2 week administration is efficient, minimizing delays to surgery Optimal number of cycles is not defined, but 3 and 4 have both been explored with pt0 results similar to historical controls. Neoadjuvant AMVAC is now our standard of care at FCCC, becoming more common at other centers
21 Radical cystectomy Radical cystectomy with pelvic lymph node dissection oincludes removal of the bladder, perivesical tissues, prostate, and seminal vesicles in men and removal of the uterus, tubes, ovaries, anterior vaginal wall, and urethra in women operioperative mortality rate of 2% to 3% oearly complications (any complication within 3 months of surgery)=> 28% ofive-year OS = 50% to 60%
22 Results of radical cystectomy Stage Recurrence-Free Overall Survival 5 y. 10y. 5 y. 10y. T2 N N T3a N N T3b N N T4a N N Stein et al JCO 2001;19:666
23 Results of radical cystectomy Stage Recurrence-Free /Overall Survival 5 years Organ-confined (<pt2pno) 73% 62% non-organ-confined (>pt2pno) 56% 49% Positiv lymph nodes (pt1-4, pn+) 33% 24% Madersbacher et al JCO 2003;21:690
24 Adjuvant chemotherapy Eight randomized trials have compared chemo with observation after definitive therapy, only 4 completed accrual Only 2 showed benefit from adjuvant chemo (each trial enrolled fewer than 100 patients) Not standard of care Could be considered for node positive disease, lymphovascular invasion, positive margins in pts who are candidates for cisplatin-based chemotherapy
25 EBRT alone frail, elderly patients or those medically unfit best results are seen in patients with solitary lesions and without carcinoma in situ or hydronephrosis local recurrence after RT alone is up to 70% (inferior results compared to cystectomy) 5 year OS from 20 40% not considered an acceptable alternative to radical cystectomy in otherwise healthy patients
26 Tri-modal Bladder-sparing protocol TURBT (maximally resect the tumor) Synchronous Therapy: RT + chemotherapy (cisplatin, paclitacel, fluorouracil, mitomycin C) Cystoscopy after 40 Gy no tumor + tumor Consolidation: RT + CT (completed to a dose of about 65 Gy) cystectomy
27 Results of bladder-sparing therapy and cystectomy Bladder-sparing n Pat. 5y. OS 5y. Survival therapy % with Bladder % Houssett NA Sauer Shipley Shipley Rodel Cystectomy Dalbagni NA Stein NA
28 Bladder-sparing protocol T2: 5y / 10y OS: 74% / 66% T3-T4a: 5y / 10y OS: 53% / 52% Shiply et al. Urology 2002;60:62
29 Combined-modality treatment and organ preservation in invasive bladder cancer Rödel et al. JCO 2002;20: pts with T1 high-risk, T1-4, N0-1 - between 1982 and Transurethral resection a) RT (n=126) b) RCT (n=289) 2. RT median 54 Gy, CT cisplatin week 1 and 5 (25 mg/m2/d on 5 consecutive days) in 145 pts; carboplatin (65 mg/m2/d on 5 consecutive days) in 95 pts (Cr Cl < 60) or cisplatin (20 mg/m2/d on consecutive days) and 5-fluorouracil (5- FU) (600 mg/m2/d; 120-hour continuous infusion) was applied to 49 patients.) 3. Restaging-TUR after 6 weeks RESULTS: Complete remission 72% Local control after CR 64% (10 y.) Distant metastasis 35% (10 y.) Disease-specific survival 42% (10 y.) Preservation of bladder >80%
30 Disease-specific survival for patients after salvage cystectomy 50% 45% 21% 18% Rödel et al. JCO 2002;20:3061
31 Randomized trials that directly compare the bladder-preserving chemoradiation therapy approach with radical cystectomy have not been performed; the relative effectiveness of these two treatments is unknown
32 TUR alone Additional surgical bladder preservation techniques Radical endoscopic resection Higher rates of recurrence than radical surgery or multimodal treatments Focal lesions. No hydro, negative resection bed biopsy, no UT TUR plus systemic chemotherapy Cisplatin based neoadjuvant ot adjuvant protocol Reserved fpr patients refusing standard therapy Partial cystectomy(2-3% of MIBC ) Limited disease inpatients medically unfit for radical surgery Solitary tumor amenable to complete resection No CIS
33 Metastatic disease the median survival is about 15 months 5 year survival rate is about 15 % A poor performance status (Karnofsky < 80), the presence of visceral (ie, pulmonary, liver, bone) metastases correlate with shortened survival The presence of these unfavorable features was associated with a median survival of 4 months
34 Front line therapy A cisplatin-based combination chemotherapy regimen is the preferred initial therapy Cisplatin-based combination chemotherapy results in superior survival when compared with single-agent cisplatin Cisplatin-based regimens: MVAC Methotrexate, vinblastine, doxorubicin, and cisplatin GC Gemcitabine plus cisplatin PCG Paclitaxel, gemcitabine, and cisplatin
35 MVAC MVAC is a standard first-line option 269 patients with advanced urothelial carcinoma randomly assigned to treatment with either MVAC or single-agent cisplatin. Results: 1. improvement in the ORR: 39 vs. 12% 2. increase in PFS: 10 vs. 4 months 3. improvement in OS: 13 vs. 11 months J Clin Oncol. 1992;10(7):1066.
36 GC A phase III trial 405 patients were randomly assigned to either GC or MVAC RESULTS: Similar ORR (49 vs. 36%). Similar time to progression (7 months in each arm). Similar OS (14 vs. 15 months). Similar quality of life, though patients experienced less weight loss, a better performance status, and less fatigue. Less serious (grade 3/4) toxicity, including neutropenia (71 vs. 82%), neutropenic sepsis (2 vs. 14%), and mucositis (1 vs. 22%) Alternate dosing schedules with the GC regimen have used a threeweek instead of four-week schedule J Clin Oncol. 2000;18(17):3068.
. - A trend towards an improvement in PFS (8.3 vs. 7.")
37 PCG European Organization for the Research and Treatment of Cancer Study (EORTC 30987) o 626 patients with advanced urothelial carcinoma and randomly assigned them to treatment with GC or PGC for a maximum of six cycles. o A median follow-up of 4.6 years o RESULTS: - An increase in the ORR (56 vs 44%, p = 0.003). - A trend towards an improvement in PFS (8.3 vs. 7.6 months) - A trend towards longer OS (15.8 vs months, P = 0.075) - Increased incidence of serious (grade 3/4) toxicity, including neutropenia (65 vs. 51%), fatigue (15 vs. 11%), and infections (18 vs 14 %) - These results suggest that PGC is a treatment option for patients with metastatic urothelial carcinoma J Clin Oncol. 2012;30(10):1107.
38 Carboplatin + Gemcitabine EORTC patients with impaired renal function (GFR <60 but >30 ml/min) and/or a poor performance status ( ECOG 2) were randomly assigned to Carbo/Gem or methotrexate, carboplatin, plus vinblastine (MCAVI). RESULTS: ORR (41 vs. 30%) that did not reach statistical significance. No difference in median OS (9 vs. 8 months) No difference in median PFS (6 vs. 4 months) Less serious (grade 3/4) toxicity overall (9 vs. 21%), including neutropenia (52 vs. 63% percent) and febrile neutropenia (5 vs. 15%). Option for patients with impaired renal function or a poor performance status (ECOG 2)
39 Cisplatin contraindications ECOG 2 or greater or Karnofsky 60 to 70 or less Cr clearance < 60 ml/min A hearing loss (measured at audiometry) of 25 db at two contiguous frequencies Grade 2 or greater neuropathy NYHA class III or greater CHF
40 Non platinum regimens Paclitaxel plus gemcitabine appears to be more active than docetaxel plus gemcitabine: Paclitaxel plus gemcitabine ORR 54 70% and median OS of months Toxicity with this combination is primarily hematologic, although severe pulmonary toxicity was reported J Clin Oncol. 2005;23(6):1185. Docetaxel plus gemcitabine: ORR % and median OS of months Cancer. 2003;98(9):1863; Br J Cancer. 2005;92(4):645.
41 Second line chemotherapy response rates < 20% no one regimen is considered to be the standard second-line therapy Ifosfamide, oxaliplatin, pacitaxel, docetaxel, gemcitabine
42 Treatment of muc Advanced UC is a uniformly fatal disease after failure of platinum chemotherapy Median survival is short Durable responses are not routinely observed in this patient population Grade 3-4 toxicities are high with 2L chemotherapy Difficult to treat patient population Vinflunine is the only approved agent in the EU, but has no survival benefit compared with BSC in the intent-to-treat population Vinflunine was tested in a pure 2L population ORR of 8.6% (vs 0% for BSC) 1 No single-agent therapy has been observed to improve median OS mos Vinflunine + BSC: 6.9 mo BSC: 4.6 mo BSC, best supportive care; VFL, vinflunine; 2L, second-line. Reference: 1. Bellmunt et al. J Clin Oncol
43 Immune Checkpoint Inhibition in Urothelial Cancer
 T cell Tumor cell T cell Atezolizumab (anti-pdl1) Signaling through")



44 Atezolizumab (MPDL3280A): A Humanized Anti-PDL1 Antibody Atezolizumab (anti-pdl1) T cell Tumor cell T cell Atezolizumab (anti-pdl1) Signaling through programmed deathligand 1 (PD-L1), which is expressed in many cancers including muc, can inhibit antitumor immune responses Atezolizumab can enhance T-cell priming and reinvigorate suppressed immune cells by inhibiting binding of PD-L1 to PD-1 and B7.1 By leaving the PD-L2/PD-1 interaction intact, atezolizumab has the potential to preserve peripheral immune homeostasis 1,2 Dendritic cell References: 1. Akbari et al. Mucosal Immunol Matsumoto et al. Biochem Biophys Res Commun

 Co-primary Endpoints ORR (confirmed) per RECIST v.1.")
45 IMvigor 210: Phase II Study Locally advanced or metastatic cancer of the bladder, renal pelvis, ureter or urethra Predominant transitional cell histology Progression during or following platinum No restriction on number of prior lines of therapy Creatinine clearance 30 ml/min ECOG PS 0-1 Tumor tissue evaluable for PD-L1 testing a Atezolizumab 1200 mg IV q3 weeks until loss of clinical benefit Response assessment q9 weeks (q12 weeks after 54 weeks) Co-primary Endpoints ORR (confirmed) per RECIST v.1.1 (central independent review) Investigator-assessed ORR per modified RECIST Primary endpoints met if null hypothesis (ORR of 10%) rejected at significance level (α) of 5% Key Secondary Endpoints PFS, DOR, OS, Safety a PD-L1 prospectively assessed by central laboratory. Patients and investigators blinded to PD-L1 IHC status. Trial Identifier: NCT
 Death (n = 3) Other (n = 2) Physician decision (n = 2) Non-compliance (n = 1) Excluded (n = 170 a ) Brain metastasis (n = 26) ECOG PS2 (n = 22) Inadequate hematologic/end organ")
46 Screened (n = 486) Enrolled (n = 316) Received treatment (N = 311) Still on therapy (n = 88) Discontinued treatment (n = 223) Progression of disease (n = 196) Adverse event (n = 11) Withdrawal by subject (n = 8) Death (n = 3) Other (n = 2) Physician decision (n = 2) Non-compliance (n = 1) Excluded (n = 170 a ) Brain metastasis (n = 26) ECOG PS2 (n = 22) Inadequate hematologic/end organ function (n = 18) Life expectancy < 12 wk (n = 15) Informed consent form not signed (n = 14) No measurable disease (n = 13) Inadequate tissue (n = 7) Other (e.g. autoimmune disease, prior therapy, abnormal laboratory results; n = 53) Treated patients b : Europe 26.4% United States/Canada 73.4% Safety/efficacy evaluable (N = 311) a Includes re-screened patients. b Excludes 1 patient with unknown site.





47 PD-L1 Immune Cell Expression and Prevalence IHC Status of Treated Patients in IMvigor 210 Study (N = 311) 5% 1 but < 5% < 1% IC2/3 IC1 IC0 IC2/3 32% n = 100 IC0 33% n = 103 IC1 35% n = 108 IMvigor 210 enrolled an all-comer population VENTANA PD-L1 (SP142) CDx Assay was used to prospectively measure tumor-infiltrating immune cell (IC) PD-L1 expression based on 3 IHC scoring levels Images at 10x magnification.
48 Baseline Characteristics Characteristic N = 311 Age, median (range) 66 y (32-91 y) Male 78% Bladder primary tumor 75% Creatinine Clearance < 60 ml/min 35% ECOG PS 1 62% Hemoglobin 10 g/dl 22% Metastatic sites at baseline Visceral a 78% Liver 31% Prior systemic regimen setting Metastatic 78% 2 regimens for metastatic disease 20% 3 regimens for metastatic disease 20% No significant differences in baseline demographics between PD-L1 subgroups a Visceral metastasis defined as liver, lung, bone, any non-lymph node or soft tissue metastasis. Data cutoff May 5, 2015.
49 RECIST v1.1 Criteria by Independent Review a PD-L1 subgroup n CR (%) ORR (%) 95% CI P value b IC2/ % 27% 19, 37 <.0001 IC1/2/ % 18% 13, All 311 4% 15% 11, IC % 10% 5, 18 N/A c IC % 9% 4, 16 N/A c IMvigor 210 met its co-primary endpoints in all subgroups tested ORR by independent review (RECIST v1.1) and investigator (mrecist) were concordant Early response data are likely to mature in subsequent analyses a Objective response evaluable population: all treated patients had measurable disease at baseline per investigator-assessed RECIST v1.1. = c No formal hypothesis testing conducted. Data cutoff May 5, Follow up 24 weeks. b P-value for H o : ORR 10% versus H a : ORR 10%, where 10% ORR is historical control, α
 patients with tumor assessments had SLD reduction SLD, sum of longest diameters. a > 100% increase. b Per confirmed RECIST v1.1 (independent review).")
50 Mean SLD Reduction from Baseline, % 51/85 (60%) a Efficacy: Changes in Target Lesions by PD-L1 Subgroup PD-L1 status IC2/3 ORR b 27% aaa 38/88 (43%) 0 IC1 10% aa 27/85 (32%) 0 IC0 9% -100 PD SD PR CR Unknown 111/258 (43%) patients with tumor assessments had SLD reduction SLD, sum of longest diameters. a > 100% increase. b Per confirmed RECIST v1.1 (independent review). Data cutoff May 5, Follow up 24 weeks. Patients without post-baseline tumor assessments not included. Several patients with CR had < 100% reduction due to lymph node target lesions. All lymph nodes returned to normal size per RECIST v1.1.
51 Efficacy: Subgroup Analyses ORR, % (95% CI) a Subgroup IC2/3 All Prior systemic regimens, metastatic setting b 1 26% (12, 43) 12% (7, 19) 2 39% (17, 64) 18% (9, 30) 3 20% (6, 44) 13% (6, 24) Metastatic sites at baseline Visceral 17% (9, 28) 10% (6, 14) Liver 15% (4, 34) 6% (2, 13) Lymph node only 38% (19, 59) 33% (20, 49) ECOG PS 1 19% (10, 31) 10% (6, 15) Hemoglobin < 10 g/dl 21% (7, 42) 9% (3,18) Median DOR not yet reached in any of the subgroup populations a Per RECIST v1.1 (independent review). b In patients with 0 prior regimens, ORR (95% CI) was 26% (11, 46) in IC2/3 patients (n = 27) and 20% (11, 31) in all-comer patients (n = 70). Data cutoff May 5, Follow up 24 weeks.
 100 80 60 40 20 0 IC2/3 IC0/1 + Censored 0 1 2 3 4 a Per RECIST v1.1 (independent review). Data cutoff May 5, 2015. Follow up 24 weeks. 5 6 7 8 9 10 11 Time, months No.")
52 Progression-Free Survival Survival Progression-Free Survival IC2/3 n = 100 IC0/1 n = 211 All N = 311 Median PFS, a mo (95% CI) 2.1 (2.1, 4.1) 2.1 (2.0, 2.1) 2.1 (2.1, 2.1) IC2/3 IC0/1 + Censored a Per RECIST v1.1 (independent review). Data cutoff May 5, Follow up 24 weeks Time, months No. at Risk IC2/3: IC0/1:
 100 Median follow up: 7 mo (range, 0-11 mo) 80 60 40 20 0 IC2/3 IC0/1 + Censored 0 1 2 3 4 5 6 7 8 9 10 11 Time, months No.")
53 Overall Survival Preliminary Analyses of Overall Survival Survival IC2/3 n = 100 IC0/1 n = 211 All N = 311 Median OS, mo (95% CI) NR (7.6, NE) 6.7 (5.7, 8.0) 7.9 (6.7, NE) 100 Median follow up: 7 mo (range, 0-11 mo) IC2/3 IC0/1 + Censored Time, months No. at Risk IC2/3: IC0/1: NR, not reached; NE, not estimable. Data cutoff May 5, Follow up 24 weeks.
54 Conclusions IMvigor 210 met its co-primary endpoints in IC2/3, IC1/2/3 and all-comer subgroups, demonstrating significant improvement over a historical 10% ORR Durable responses were seen in a heavily pretreated population with muc that progressed on platinum-based chemotherapy Median duration of response was not reached in any IC or prognostic subgroup (e.g. liver metastases at baseline) Higher PD-L1 IC status was associated with higher ORR Overall survival data are immature at this time Atezolizumab was well tolerated with a low rate of treatmentrelated Grade 3-4 toxicities and no treatment-related renal toxicity No treatment-related deaths were observed Atezolizumab has the potential to change the standard of care in metastatic urothelial carcinoma

55 PD-1 Pathway and Immune Surveillance Programmed cell death receptor 1 (PD-1) is a negative co-stimulatory receptor expressed primarily on activated T cells 1,2 Binding of PD-1 to its ligands PD-L1 and PD-L2 inhibits effector T-cell function 1,2,3 Expression of PD-L1 on tumor cells and macrophages can suppress immune surveillance and permit neoplastic growth 1,2,3 1. Keir ME et al. Annu Rev Immunol. 2008;26: Pardoll DM. Nat Rev Cancer. 2012;12: Hirano F et al. Cancer Res. 2005;65:
56 Pembrolizumab Phase I: PFS and OS
57 PD-1/L1 Blocking Antibodies in Clinical Development in Urothelial Cancer Company Agent Target Bristol-Myers Squibb Nivolumab PD-1 Merck Pembrolizumab (MK-3475) PD-1 Genentech/Roche Atezolizumab (MPDL3280A) PD-L1 Medimmune/AZ Durvalumab (MEDI4736) PD-L1 Merck Serono/Pfizer Avelumab (MSB C) PD-L1
58 2 nd line and beyond 1 st line Ongoing Trials with Checkpoint Inhibitors Bladder Cancer Non-muscleinvasive bladder cancer Muscle-invasive bladder cancer Metastatic bladder cancer Low grade High grade Neoadjuvant Adjuvant Cisplatin-eligible Cisplatin-ineligible In development Pembrolizumab/ BCG In development Trimodality Atezolizumab (Ph III) Maintenance Pembrolizumab (Ph II) Atezolizumab (Ph II) BCG-refractory In development Pembrolizumab (Ph II) Avelumab (Ph III) Pembrolizumab (Ph II) Cisplatin-refractory Pembrolizumab (Ph III) Atezolizumab (Ph III) Nivolumab (Ph II) Adapted from: Fakhrejahani F et al. Curr Opin Urol 2015;25:
59 Take home messages Absence of muscularis propria in the biopsy specimen => repeated biopsy is needed! Neoadjuvant chemo, followed by radical cystectomy is standard of care NCCN: GC, CMV or accelerated/dose dense MVAC as options Optimal number of cycles is not defined, but 3 and 4 have both been explored with pt0 results similar to historical controls Adjuvant chemo => considered for node positive disease, lymphovascular invasion, positive margins Front line regimens for metastatic disease: AMVAC, GC or PGC No standard second-line chemotherapy: Ifosfamide, oxaliplatin, pacitaxel, docetaxel, AND CLINICAL TRIALS Checkpoint inhibitors are now approved for second line Rx:ATEOILIZUMAB Research ongoing with adjuvant check point inhibitors

60 What takes me home
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena
 I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena XII Corso di aggiornamento AIRTUM per operatori dei Registri Tumori Reggio Emilia
I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena XII Corso di aggiornamento AIRTUM per operatori dei Registri Tumori Reggio Emilia
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO
 AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
PREVENTION & SCREENING
 A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Treatment of muscle invasive bladder cancer. ie: pt2. N. Mottet
 Treatment of muscle invasive bladder cancer ie: pt2 N. Mottet Disclosures Astellas BMS Pierre Fabre Sanofi MIBC: really undertreated 28 691 MIBC in the US (national database). Gray Eur Urol 2013 Patients
Treatment of muscle invasive bladder cancer ie: pt2 N. Mottet Disclosures Astellas BMS Pierre Fabre Sanofi MIBC: really undertreated 28 691 MIBC in the US (national database). Gray Eur Urol 2013 Patients
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Exploring New Strategies in Bladder Cancer
 Exploring New Strategies in Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, Genitourinary Translational Working Group Co-Director, Signal Transduction Program Smilow Cancer
Exploring New Strategies in Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, Genitourinary Translational Working Group Co-Director, Signal Transduction Program Smilow Cancer
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Cancer Drugs Fund. Managed Access Agreement. Atezolizumab for untreated metastatic urothelial cancer where cisplatin is unsuitable
 Cancer Drugs Fund Managed Access Agreement Atezolizumab for untreated metastatic urothelial cancer where cisplatin is unsuitable NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Cancer Drugs Fund Data
Cancer Drugs Fund Managed Access Agreement Atezolizumab for untreated metastatic urothelial cancer where cisplatin is unsuitable NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Cancer Drugs Fund Data
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Integrating Immunotherapy into Urologic Oncology: The New Urothelial Cancer Paradigm
 Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer
 Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma of the bladder
 Annals of Oncology : -5. 999. 999 Klimer Academic Publishers. Printed in the Netherlands. Original article Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma
Annals of Oncology : -5. 999. 999 Klimer Academic Publishers. Printed in the Netherlands. Original article Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Understanding Systemic Chemotherapy Options in Bladder Cancer. Part III: Chemoradiotherapy
 Understanding Systemic Chemotherapy Options in Bladder Cancer Tuesday, July 25, 2017 Part III: Chemoradiotherapy Presented by Dr. Jean Hoffman-Censits is a genitourinary medical oncologist at the Sidney
Understanding Systemic Chemotherapy Options in Bladder Cancer Tuesday, July 25, 2017 Part III: Chemoradiotherapy Presented by Dr. Jean Hoffman-Censits is a genitourinary medical oncologist at the Sidney
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA
 IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Media Release. Basel, 21 July 2017
 Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Bladder Cancer. Clinical Case Conference
 Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Sponsor / Company: Sanofi Drug substance(s): Docetaxel (Taxotere )
: Docetaxel (Taxotere )") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Oral Communications & Posters
 Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
J Clin Oncol 23: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 23 NUMBER 21 JULY 20 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine Plus Cisplatin, With Methotrexate, Vinblastine,
VOLUME 23 NUMBER 21 JULY 20 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Long-Term Survival Results of a Randomized Trial Comparing Gemcitabine Plus Cisplatin, With Methotrexate, Vinblastine,
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Issues in the Management of High Risk Superficial Bladder Cancer
 Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
symposium article introduction symposium article
 Annals of Oncology 17 (Supplement 5): v118 v122, 2006 doi:10.1093/annonc/mdj965 Long-term survival results of a randomized trial comparing gemcitabine/cisplatin and methotrexate/ vinblastine/doxorubicin/cisplatin
Annals of Oncology 17 (Supplement 5): v118 v122, 2006 doi:10.1093/annonc/mdj965 Long-term survival results of a randomized trial comparing gemcitabine/cisplatin and methotrexate/ vinblastine/doxorubicin/cisplatin
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
R&D Conference Call. CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu.
 R&D Conference Call CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu July 4, 2016 Forward-Looking Statements This presentation may include forward-looking
R&D Conference Call CHUGAI PHARMACEUTICAL CO., LTD. Department Manager of Oncology Lifecycle Management Dept. Megumi Uzu July 4, 2016 Forward-Looking Statements This presentation may include forward-looking
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Neoplasie uroteliali 2017 Highlights. Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy
 Neoplasie uroteliali 2017 Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy Disclosures Consulting or Advisory Role: Company: Roche, Bayer, Merck & Co. Inc., Astra
Neoplasie uroteliali 2017 Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy Disclosures Consulting or Advisory Role: Company: Roche, Bayer, Merck & Co. Inc., Astra
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D.
 Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
1.0 Dr D Mitchell Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) clinical management guidelines for muscle invasive and advanced transitional cell carcinoma of bladder Dr Darren Mitchell Consultant Clinical
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) clinical management guidelines for muscle invasive and advanced transitional cell carcinoma of bladder Dr Darren Mitchell Consultant Clinical
Urothelial Carcinoma Highlights
 Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer
 Media Release Basel, 8 January 2016 Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer Higher expression of PD-L1 (programmed death-ligand 1)
Media Release Basel, 8 January 2016 Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer Higher expression of PD-L1 (programmed death-ligand 1)
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Immunotherapy and urothelial carcinoma. Yohann Loriot
 Immunotherapy and urothelial carcinoma Yohann Loriot Immunothérapie en clinique : Cancers de vessie Où en sommes nous? Données phase I/II FDA «breakthrough designation» Prochaines étapes? Immunothérapie
Immunotherapy and urothelial carcinoma Yohann Loriot Immunothérapie en clinique : Cancers de vessie Où en sommes nous? Données phase I/II FDA «breakthrough designation» Prochaines étapes? Immunothérapie
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER
 THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
Invasive Bladder Transitional Cell Carcinoma OBJECTIVES
 Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Policy. Medical Policy Manual Approved Revised: Do Not Implement Until 3/2/19. Nivolumab (Intravenous)
") Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,