Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
|
|
|
- Peter Ross
- 5 years ago
- Views:
Transcription
1 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
2 Survival in Melanoma by Stage Proportion Surviving Stage I (n = 9175) Stage II (n = 5739) Stage III (n =1 528) Stage IV (n = 1158) Yrs Balch CM, et al. J Clin Oncol. 2001;19:
3 THE CASE FOR CANCER IMMUNOTHERAPY No new truly curative anticancer cytotoxic drug developed in the last 20 years (until recently) The immune response is designed to identify and disable escape routes that cancers employ. Too many escape routes? Melanoma is among the most immunogenic of all solid cancers
4 TUMORS CREATE CHAOS Disordered Blood flow and vascular distribution Stroma and immune milieu Immune shaping Create selection pressure so that cancers can evade immune destruction Malignant evolution Tumors go to great lengths to evade or subvert the immune response


 2")
5 Tumors Evade Immune Detection and Destruction 1 The immune response to tumor cells can be evaded by a number of mechanisms: Reduced antigen presentation 1 Resistance to T-cell mediated killing 1 T-cell inhibition and anergy (eg, by upregulation of coinhibitory molecules, including PD-L1) 2 Treg-mediated immunosuppression 1 TUMOR
, also termed immune checkpoints, suppresses T-cell activation 1,3 APCs can express the signaling partners of these costimulatory and coinhibitory molecules")
6 Cosignaling Molecules Contribute to Immune Regulation 1 Cosignaling regulates T-cell activation 2 Signaling via costimulatory molecules (eg, CD28, GITR) promotes T-cell activation 3 Signaling via coinhibitory molecules (eg, PD-1, LAG-3), also termed immune checkpoints, suppresses T-cell activation 1,3 APCs can express the signaling partners of these costimulatory and coinhibitory molecules and direct T-cell function accordingly 2 Costimulatory molecules Coinhibitory molecules






7 Physiological Roles of Immune Checkpoint CTLA-4 pathway 1,2 Pathways (cont) Inhibits the activation of naïve and memory T cells at the lymph nodes, suppressing broad immune responses throughout the body CD80 CD28 DC MHC CD80 TCR CTLA-4 Naïve T cell - PD-1 pathway 1,2 Acts at sites of inflammation and tumor immunosuppression, inhibiting tumor-specific immune responses Tumor Cell PD-L1 PD-1 T cell -
8 Metastatic Melanoma: Treatment Advances Immunotherapy Target host Targeted Therapy Target tumor
9
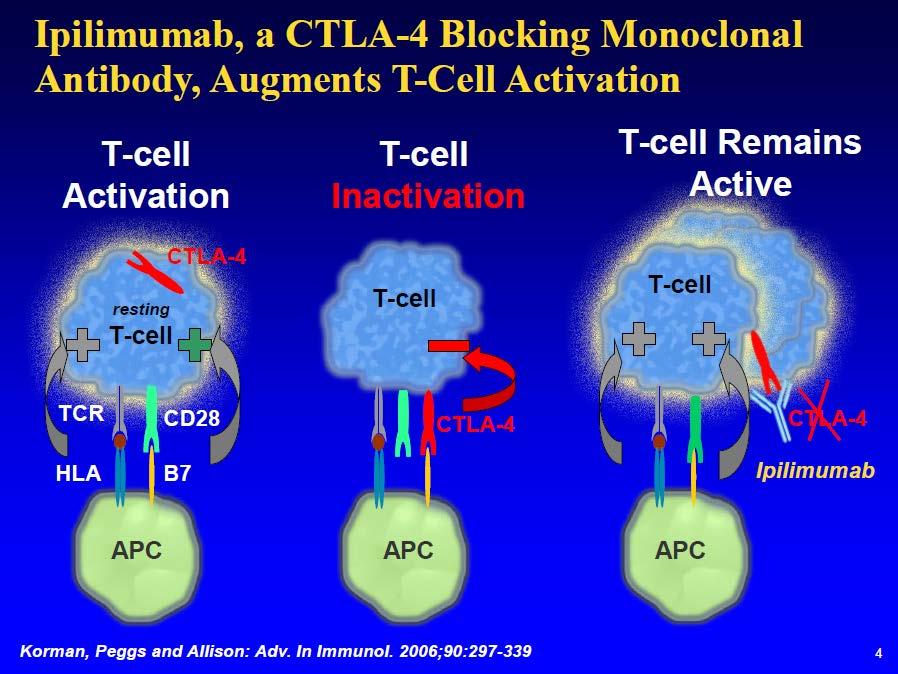
10 Ipilimumab CTLA-4 (cytotoxic T-lymphocyte associated antigen 4) a negative regulator of T cells Ipilimumab: IgG1 monoclonal Ab Block CTLA-4 Augments T cell activation and proliferation. Allowing the immune system to maintain responsiveness against an antigen Overcoming various mechanisms of immune evasion
11 NEJM 2011 June 30;364(26): NEJM 2010 August 19;363(8):
12 NEJM 2011 June 30;364(26): NEJM 2010 August 19;363(8):



13 Study 024: Phase III Placebo-Controlled Trial of Firstline DTIC ± IPI SCREENING INDUCTION MAINTENANCE Previously untreated, unresectable Stage III or IV melanoma (N = 502) R Ipilimumab 10 mg/kg q3w x4 Dacarbazine 850 mg/m 2 q3w x8 Placebo q3w x4 Dacarbazine 850 mg/m 2 q3w x8 Ipilimumab 10 mg/kg q12w Placebo q12w Week 1 Week 12 Week 24 Baseline tumor assessment First scheduled Tumor assessment Robert C et al. N Engl J Med 2011

14 Robert C et al. N Engl J Med 2011; Copyright 2011 Massachusetts Medical Society. Study 024: Overall Survival IPI + DTIC Placebo + DTIC IPI + DTIC vs Placebo + DTIC HR Median OS p-value vs 9.1 months <0.001


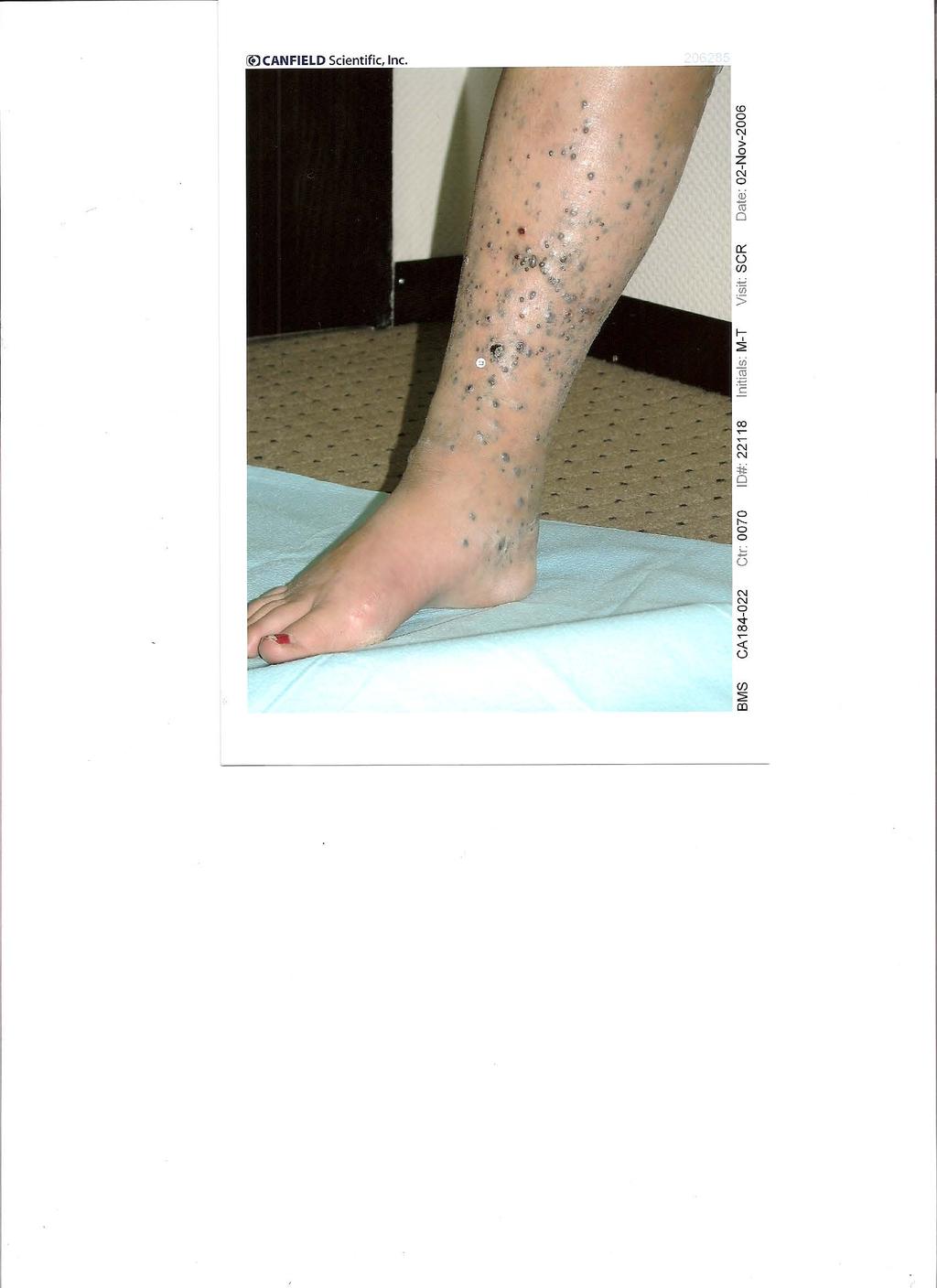
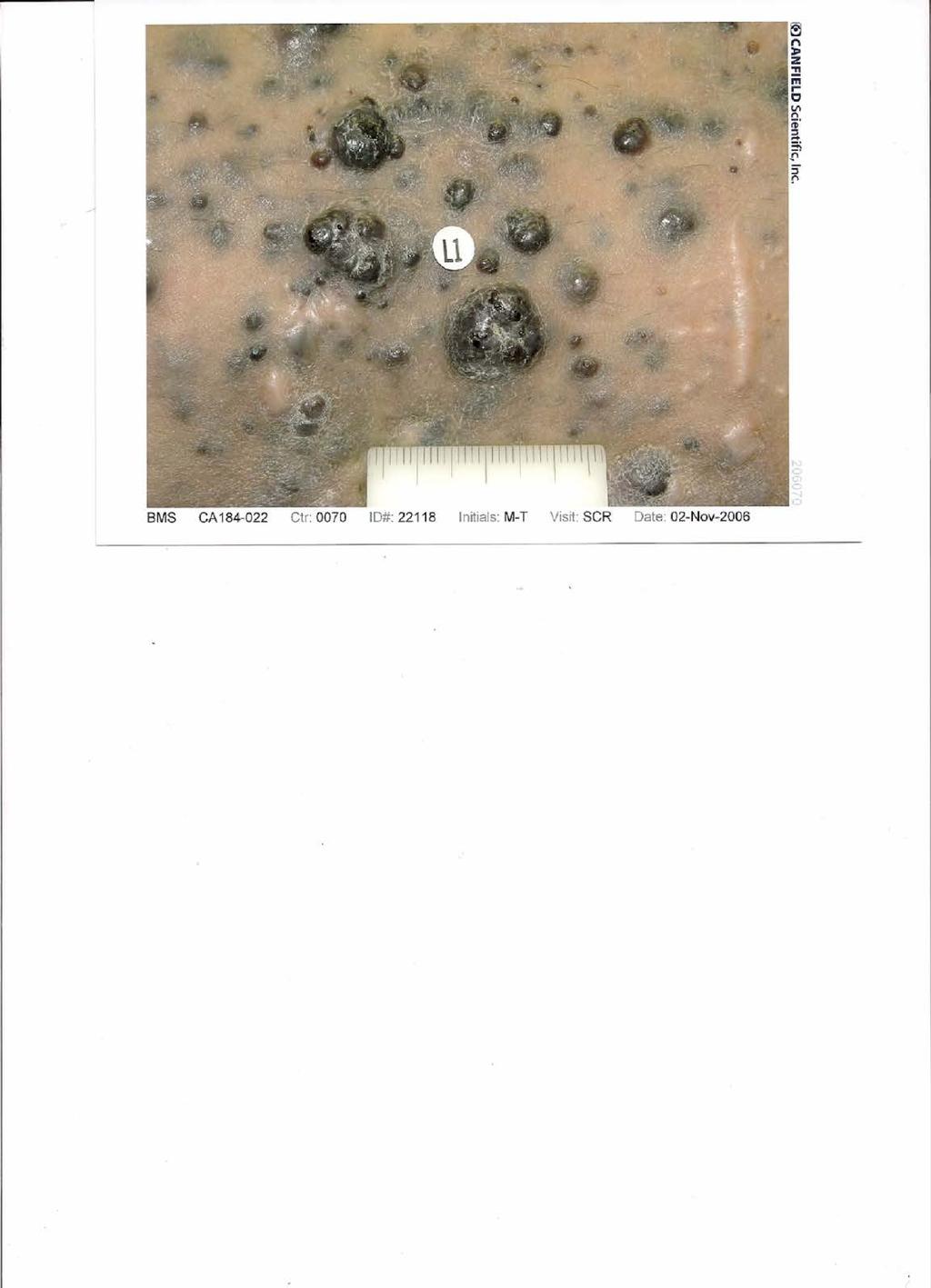
15 Metastatic Melanoma Response to Ipilimumab Before Ipilimumab After Ipilimumab
16 Ipilimumab in Melanoma: Phase I/II Trials Durable responses (CR, PR, SD) Durable late responses (~ 10%) Learning curve toxicity management Immune-related toxicity correlates with clinical benefit Immunosuppressive treatment does not interfere with anti-tumor response
17
18

19

20

21
22 IPILIMUMAB South African EAP
23 Baseline Characteristics of Treated Patients Total 108pts Age Median 59 Range Gender Male 73 (68%) Female 35 (32%) ECOG performance status 0 36 (33%) 1 63 (58%) 2 7 (6%) Unknown 2 (3%)
24 Overall Survival Median OS 1 year survival 2 year survival 3 year survival N Median Lower Upper % LowerUpper % LowerUpper % LowerUpper All 108 8,98 7,47 10,79 36% 26% 45% 20% 12% 27% 20% 12% 27% Mucosal & uveal 15 5,18 3,74 NA 8% 2% 13% 0% 0% 0% 0% 0% 0% Cutaneous & unknown 93 9,54 7,61 12,33 40% 30% 50% 23% 15% 32% 23% 15% 32%

25 Overall Survival of Cutaneous Met Melanoma Impact on the tail of the curve!
26 Ipilimumab: Pooled Survival Analysis From Phase II/III Trials in Advanced Melanoma Median OS: 11.4 mos (95% CI: ) Proportion Alive Ipilimumab Censored Mos Pts at Risk, n Ipilimumab Hodi S, et al European Cancer Congress. Abstract LBA 24. Schadendorf D, et al. J Clin Oncol. 2015;[Epub ahead of print]. 3-yr OS rate: 22% (95% CI: 20-24)

27 Anti-PD1 The interaction between the immune checkpoint receptor PD-1 and its ligands represents a potentially important tumor-specific immunomodulatory mechanism. By utilizing the PD-1 pathway, a tumor cell can prevent the activation of T-cells and therefore may block a key step that triggers the immune system. Ribas, NEJM June 2, epub ahead of print



28 PD-1 Receptor Blockade With Pembrolizumab Pembrolizumab is an antineoplastic agent, monoclonal antibody 1 Pembrolizumab is a high affinity antibody against PD-1, which exerts dual ligand blockade of the PD-1 pathway, including PD-L1 and PD-L2, on antigen-presenting or tumor cells. By inhibiting the PD-1 receptor from binding to its ligands, KEYTRUDA reactivates tumorspecific cytotoxic T lymphocytes in the tumor microenvironment and reactivates antitumor immunity 1 Inhibition 2 KEYTRUDA Antigen TCR MHC PD-1 Inactivated cytotoxic T cell PD-L2 PD-L1 APC/Tumor cell PD-1 Activated cytotoxic T cell PD-L2 PD-L1 APC/Tumor cell APC = antigen-presenting cell; MHC = major histocompatibility complex; PD-1 = programmed death receptor 1; PD-L1 = programmed death ligand 1; PD-L2 = programmed death ligand 2; TCR = T-cell receptor. 1. [Insert local label.] 2. Pardoll DM. Nat Rev Cancer. 2012;12(4):
29 KEYNOTE-002: Pembrolizumab vs Chemotherapy in Ipi-Refractory Melanoma Stratified by ECOG PS (0 vs 1); LDH (normal vs 110% ULN); BRAF status (wild type vs V600 mutant) Pts with advanced melanoma who progressed on or after Ipi (and targeted therapy, if BRAF V600+) (N = 540) Pembrolizumab 2 mg/kg IV q3w (n = 180) Pembrolizumab 10 mg/kg IV q3w (n = 181) Investigators choice of chemotherapy* (n = 179) *Carboplatin + paclitaxel, paclitaxel alone, carboplatin alone, dacarbazine, or temozolomide. Pts with PD confirmed by independent central review could cross over to pembrolizumab treatment after the first 3-mo assessment. Primary endpoint: PFS, OS Secondary endpoints: ORR, DoR Ribas A, et al. Lancet Oncol. 2015;16:
30 KEYNOTE-002: Efficacy and Safety PFS (%) An international, randomized phase II study in pts with advanced melanoma with PD within 24 wks after 2 Ipi doses ORR, % Pembro 2 mg/kg q3w 21 Pembro 10 mg/kg q3w 25 Chemotherapy 4 Grade 3/4 toxicity incidence higher with chemotherapy (26%) vs pembrolizumab (11% at 2 mg/kg and 14% at 10 mg/kg) Most frequent adverse events of any grade ( 10%) Pembrolizumab: fatigue, pruritus, and rash Chemotherapy associated primarily with grade 1/2 fatigue, nausea, vomiting, anemia, reduced appetite, alopecia Mos Ribas A, et al. Lancet Oncol. 2015;16:
31 KEYNOTE-006: Study Design Stratified by ECOG PS (0 vs 1), line of therapy (1st vs 2nd), and PD-L1 status (positive* vs negative) Unresectable stage III/IV melanoma, 1 prior therapy, known BRAF status, ECOG PS 0-1, no active brain metastases (N = 834) Primary endpoints: PFS, OS Pembrolizumab 10 mg/kg IV Q2W for 2 yrs (n = 278) Pembrolizumab 10 mg/kg IV Q3W for 2 yrs (n = 277) Ipilimumab 3 mg/kg IV Q3W x 4 doses (n = 256) Secondary endpoints: ORR, response duration, safety Assessments: Response at Wk 12, every 6 wks until Wk 48, then every 12 wks Survival every 12 wks * 1% staining in tumor, adjacent immune cells by IHC (22C3 antibody). Excluding anti CTLA-4, anti PD-1, or anti PD-L1 agents. Prior anti-braf therapy not required if normal LDH levels, no clinically significant tumor-related symptoms or evidence of rapidly progressing disease. Schachter J, et al. ASCO Abstract 9504.
32 KEYNOTE-006: Overall Response Rate With Pembrolizumab Greater ORR with KEYTRUDA 10 mg/kg every 3 weeks vs ipilimumab 1,a,b Response Rate (%) % ORR (95% CI, 27, 39) 6% CR 34% ORR (95% CI, 28, 40) 5% CR 27% PR 29% PR 12% ORR (95% CI, 8, 16) 1% CR 10% PR 0 Pembrolizumab 10 mg/kg Every 3 Weeks (N=277) Pembrolizumab 10 mg/kg Every 2 Weeks (N=279) Ipilimumab (N=278) Analysis cutoff date: 3 September Independent radiology plus oncologist review using RECIST 1.1. CR = complete response; ORR = overall response rate; PR = partial response. 1. [Insert local label.]
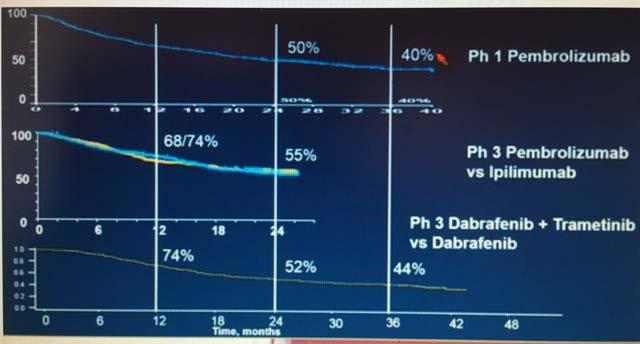
33 KEYNOTE-006: Estimated OS With pembrolizumab 1,2 Overall Survival, % No. at risk Kaplan-Meier Curve for OS (ITT Population) a % 74% HR Treatment Arm (95% CI) 50 P value c 58% 40 Pembro 10 mg/kg every weeks (0.52, 0.90) Pembro 10 mg/kg every weeks (0.47, 0.83) Ipilimumab Time (months) % reduction in the risk of death with KEYTRUDA 10 mg/kg every 3 weeks vs ipilimumab 37% reduction in the risk of death with KEYTRUDA 10 mg/kg every 2 weeks vs ipilimumab The recommended dose of KEYTRUDA is 2 mg/kg every 3 weeks 1 Analysis cutoff date: 3 March [Insert local label.] 2. Robert C et al, for the KEYNOTE-006 investigators. N Engl J Med. 2015;372(26):
34 KEYNOTE-006: Immune-Mediated AEs* Pembrolizumab Thyroid abnormalities (hyperthyroidism, hypothyroidism, thyroiditis), pneumonitis, nephritis more common Type 1 diabetes and uveitis only observed in pembrolizumab-treated pts Hepatitis, myositis similar to rates with ipilimumab Ipilimumab Colitis, hypophysitis more common Discontinuations ~ 5% in all arms ~ 10% of pts experienced grade 3/4 immune-mediated AEs No significant increase in incidence of immune-related AEs over time *Not adjusted for exposure. Schachter J, et al. ASCO Abstract 9504.
35 KEYNOTE-006 Conclusions Pembrolizumab associated with superior OS vs ipilimumab in pts with unresectable, stage III/IV melanoma with 1 previous line of therapy Median OS for pembrolizumab not reached at median follow-up of 23 mos At 24 mos, ~ 30% of pembrolizumab-treated pts still alive and free of disease progression Pembrolizumab responses as durable as those with ipilimumab and continue to accrue, including CRs Long term safety profile for pembrolizumab remains favorable Investigators suggest that results confirm pembrolizumab as a standard of care for advanced melanoma Schachter J, et al. ASCO Abstract 9504.
36 Phase III CheckMate 066: First-line Nivolumab vs Chemotherapy Stratified by PD-L1 status, M-stage Unresectable, treatmentnaive stage III or IV melanoma; BRAF wild type; ECOG PS 0-1; 18 yrs of age or older (N = 418) Primary endpoint: OS Nivolumab 3 mg/kg IV q2w + Placebo IV q3w (n = 210; 206 treated) Placebo IV q2w + Dacarbazine 1000 mg/m 2 IV q3w (n = 208; 205 treated) Secondary endpoints: PFS, ORR, PD-L1 correlates Treat until progression* or unacceptable toxicity * Pts may be treated beyond initial RECIST v1.1 defined progression if considered by the investigator to be experiencing clinical benefit and tolerating study drug. Robert C, et al. N Engl J Med. 2015;372:
37 OS: First-line Nivolumab vs Chemotherapy Objective response rate: 40.0% with nivolumab vs 13.9% with chemo (P <.001) Significantly better OS with nivolumab vs dacarbazine 100 HR 0.42 (99.79% CI: ; P <.001) Pts Surviving (%) Nivolumab Dacarbazine Median OS, Mos (95% CI) NR 10.8 ( ) 1-yr OS: 73% 1-yr OS: 42% Mos Robert C, et al. N Engl J Med. 2015;372:
38 CheckMate 067: Improved PFS with Nivo + Ipi or Nivo Alone vs Ipi Alone Proportion Alive and Progression Free Nivo + Ipi Nivo Ipi Median PFS, mos (95% CI) Nivo + Ipi (n = 314) 11.5 ( ) HR (99.5% CI) vs Ipi 0.42 ( )* HR (95% CI) vs Nivo 0.74 ( ) Nivo (n = 316) 6.9 ( ) 0.57 ( )* Ipi (n = 315) 2.9 ( ) Mos *Stratified log-rank P < vs Ipi. Exploratory endpoint. Wolchok JD, et al. ASCO Abstract LBA1. Reprinted with permission. _
39 Combination Immunotherapy ipilimumab + nivolumab melanoma 60% response versus single agent responses 44% (nivo), 19% (ipi) 12% CR 80% two year survival
40 Combination Immunotherapies Combination Therapy Mechanisms of Action Phase Indication Nivolumab + ipilimumab Anti-PD1 + anti-ctla-4 I/II Gastric, TNBC, PA, SCLC, Bladder, Ovarian II/III II Melanoma, RCC SCLC, GBM, NSCLC Nivolumab + BMS Anti-PD1 + anti-lag3 I Solid tumors Nivolumab + Viagenpumatucel-L Anti-PD1 + vaccine I NSCLC Nivolumab + urelumab Anti-PD1 + anti-4-1ββ I/II Solid Tumors, B-Cell NHL Atezolizumab + MOXR0916 Anti-PDL1 + anti-ox40 I Solid Tumors Atezolizumab + varlilumab Anti-PDL1 + anti-cd27 II RCC Atezolizumab + GDC-0919 Anti-PDL1 + IDO inhibitor I Solid Tumors Epacadostat + atezolizumab, durvalumab, or pembrolizumab IDO inhibitor + anti-pdl1 or anti-pd1 I/II Solid Tumors Pembrolizumab + T-Vec Anti-PD1 + vaccine III Melanoma Durvalumab + tremelimumab Anti-PDL1 + anti-ctla-4 I/II Melanoma I/II/III II SCCHN Mesothelioma, UBC, TNBC, PA III NSCLC, Bladder
41 Combination of PD-1, PDL-1 and CTLA-4 Blockade higher clinical response rates than single agent melanoma, NSCLC, head and neck lower tolerability and higher discontinuation rates management of toxicity in broad patient populations in community settings dosing and sequence cost
42
43 Effective Surveillance, Recognition, and Intervention Minimizes the Potential Impact of AEs 1,2 Management of AEs Proactive monitoring Early recognition and reporting Appropriate management Vigilant follow-up 1. Teply BA et al. Oncology (Williston Park). 2014;28 Suppl 3: Kannan R et al. Clin J Onc Nurs. 2015;18(3): , 326.
44 iraes Are Associated With Immuno-oncology Therapies a a The AEs described here represent some but not all iraes that may occur with immune checkpoint inhibitor therapies. 1. Teply BA et al. Oncology (Williston Park). 2014;28 Suppl 3: Hodi FS et al. N Engl J Med. 2010;363(8): Topalian SL et al. N Engl J Med. 2012;366(26): Mellati M et al. Diabetes Care. 2015;38(9):e137 e Forde PM et al. Anticancer Res. 2012;32(10):

:711 723. 3. Topalian SL et al. N Engl J Med. 2012;366(26):2443 2454. 4. Mellati M et al. Diabetes Care. 2015;38(9):e137 e138. 5. Forde PM et al. Anticancer Res.")
45 iraes Are Associated With Immuno-oncology Therapies a Hepatic Autoimmune hepatitis 1,3 ALT/AST increases 1,2 Endocrine Hypophysitis 1 3 Thyroiditis 1,3 Type 1 diabetes 4 Respiratory Renal Pneumonitis 1,3 Nephritis 1 Renal failure 5 Skin Gastrointestin al Colitis/diarrhea 1, 2 Macropapular rash 1 Pruritus 1,2 Neuromuscula r Peripheral sensory neuropathy 1 a The AEs described here represent some but not all iraes that may occur with immune checkpoint inhibitor therapies. 1. Teply BA et al. Oncology (Williston Park). 2014;28 Suppl 3: Hodi FS et al. N Engl J Med. 2010;363(8): Topalian SL et al. N Engl J Med. 2012;366(26): Mellati M et al. Diabetes Care. 2015;38(9):e137 e Forde PM et al. Anticancer Res. 2012;32(10):
46 Risk Evaluation and Management Strategy (REMS) GASTROINTESTINAL Any changes in normal bowel habits or changes from baseline (eg, last week, last visit) - Diarrhea - Abdominal pain - Blood or mucus in stool with or without fever - Peritoneal signs consistent with bowel perforation - Ileus SKIN Pruritus Rash (Maculopapular Rash) Viteligo NEUROLOGIC Monitor for symptoms of motor and sensory neuropathy - Unilateral or bilateral weakness - Sensory alterations - Paresthesia LIVER Elevations in liver function tests - AST >2.5 times upper limit of normal (ULN) - ALT >2.5 times ULN - Total bilirubin >1.5 times ULN ENDOCRINE Fatigue Headache Mental status changes Abdominal pain Unusual bowel habits Hypotension Abnormal thyroid function tests and/or serum chemistries
47 Kinetics of appearance of immune-related adverse event Weber J S et al. JCO 2012;30: by American Society of Clinical Oncology
48 Adverse Events CTLA-4: Rash, diarrhea, hepatitis, endocrine 24% grade 3/4 (1) PD-1/PD-L1: Rash, fatigue, arthralgias, pnuemonitis 6-12% grade 3/4 (2-4) Chemotherapy: Alopecia, nausea, myelosuppression ~50% grade 3/4 (5) (1) Hodi et al. NEJM 2010 (2) Hamid et al. NEJM 2013 (3) Topalian et al. NEJM 2012 (4) Weber et al. Lancet Oncol 2015 (5) Kelly et al. JCO 2001
49
50 Immunotherapy Summary Immunotherapy continues to grow in importance in the care of patients with melanoma Response patterns to immunotherapy agents vary but can be durable Vigilance for adverse events by the patient, their family, and their healthcare team important Growing evidence indicates that chemotherapy treatment and the use of corticosteroids for immune-related toxicities do not reduce the efficacy of immunotherapies Patients education about expectations with immunotherapy is also important
51 Treatment of Advanced Malignant Melanoma Standard of care BRAF V600E Positive BRAF V600E Negative Vemurafenib (+ - Cobimet) Dabrafenib + Trametinib Ipilimumab Pembrolizumab / Nivolumab T-VEC Clinical trials Pembrolizumab/Nivolumab Ipilimumab Ipilimumab + Nivolumab T-VEC Clinical trials
52 Future Directions Combination strategies including immunotherapy are currently being evaluated Targeted agents + immunotherapy Multiple immunotherapeutic agents Patients selection using clinical and biological biomakers Identification of additional tumor subtypes that can be effectively treated with immunotherapy

53 In your case, Dave, there are choices, surgery, outpatient immunotherapy, anti BRAF, anti MEK, anti PDI or whatever is in the box that our lovely Carol is holding.

54 THANK YOU
55
56 Ipilimumab Major benefit is in durable tumor regressions Impact on the tail of the curve!
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
Pembrolizumab: First in Class for Treatment of Metastatic Melanoma
 Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Section Editors: Christopher J. Campen and Beth Eaby-Sandy Pembrolizumab: First in Class for Treatment of Metastatic Melanoma CARRIE BARNHART, PharmD From Billings Clinic Cancer Center, Billings, Montana
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD
 Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Cancer Immunotherapy in the Modern Era. David R. Spigel, MD Sarah Cannon Research Institute Nashville, Tennessee
 Cancer Immunotherapy in the Modern Era David R. Spigel, MD Sarah Cannon Research Institute Nashville, Tennessee Key Events in the History of Cancer Immunotherapy 1890 First cancer vaccine developed (Coley)
Cancer Immunotherapy in the Modern Era David R. Spigel, MD Sarah Cannon Research Institute Nashville, Tennessee Key Events in the History of Cancer Immunotherapy 1890 First cancer vaccine developed (Coley)
NEW ZEALAND DATA SHEET
 NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY
 MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes
 Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Discover the PD-1 pathway and its role in cancer 105/15 -ONCO- 07/15
 Discover the PD-1 pathway and its role in cancer 105/15 -ONCO- 07/15 Immunology in cancer The role of immunology in cancer Evolving knowledge of the immune system has provided a better understanding of
Discover the PD-1 pathway and its role in cancer 105/15 -ONCO- 07/15 Immunology in cancer The role of immunology in cancer Evolving knowledge of the immune system has provided a better understanding of
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Emily Borders, Pharm.D., M.S., BCOP Oncology Clinical Pharmacist Stephenson Cancer Center Faculty Disclosure Learning Objectives
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Emily Borders, Pharm.D., M.S., BCOP Oncology Clinical Pharmacist Stephenson Cancer Center Faculty Disclosure Learning Objectives
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016
 Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Monthly Oncology Tumor Boards: A Multidisciplinary Approach to Individualized Patient Care Lung Cancer: Advanced Disease March 8, 2016 Jae Kim, MD City of Hope Comprehensive Cancer Center Karen Reckamp,
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
ESMO 2016 * Investor Meeting October 9, *European Society of Medical Oncology, October 7-11, 2016 ESMO 2016 NOT FOR PRODUCT PROMOTIONAL USE
 ESMO 2016 * Investor Meeting October 9, 2016 *European Society of Medical Oncology, October 7-11, 2016 1 Forward-Looking Information During this meeting, we will make statements about the Company s future
ESMO 2016 * Investor Meeting October 9, 2016 *European Society of Medical Oncology, October 7-11, 2016 1 Forward-Looking Information During this meeting, we will make statements about the Company s future
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Update on Melanoma Treatment. Tara C Mitchell, MD
 Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells
Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells