Systemic therapy for HER2+ Advanced Breast Cancer
|
|
|
- Annabel Underwood
- 5 years ago
- Views:
Transcription





1 Systemic therapy for HER2+ Advanced Breast Cancer F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program Coordinator EORTC Breast Group Chair
2 DISCLOSURES Consultant/Ad Board: Astellas/Medivation, AstraZeneca, Celgene, Daiichi-Sankyo, Eisai, GE Oncology, Genentech, GlaxoSmithKline, Macrogenics, Merck- Sharp, Merus BV, Novartis, Pfizer, Pierre-Fabre, Roche, Sanofi, Teva
3 MANAGEMENT OF HER-2 + MBC: ABC: primary or metastatic HER-2 status? Pivotal trials Combinations with CT and ET: when & which agents? Continue HER-2 blockade beyond progression (change of paradigm) Which anti-her-2 agent? Dual blockade? Best sequence of therapies? Overall good safety profile of anti-her-2 therapies but cardiac surveillance & management guidelines needed Important problem of brain metastases
4 HER-2 POSITIVE MBC Anti-HER-2 therapy should be offered early to all HER-2+ MetaBC patients, except in the presence of contra-indications for use of such therapy (LoE: 1 A). (91%)
5
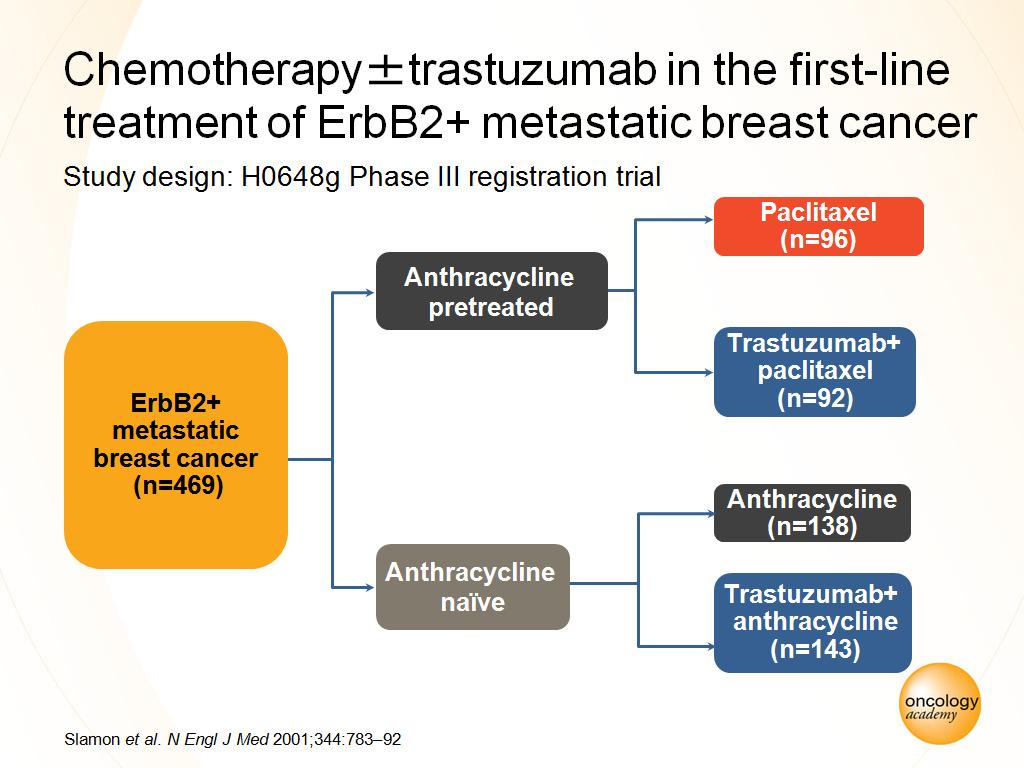
6 Longer OS: 25.1 vs ms (p=0.046) Longer TTP: 7.4 vs. 4.6 ms (p<0.001) Higher RR: 50 vs. 32% (p<0.001) Longer duration: 9.1 vs. 6.1 ms (p<0.001)
7

8 IMPORTANCE OF STARTING ANTI-HER-2 AGENT EARLY ON
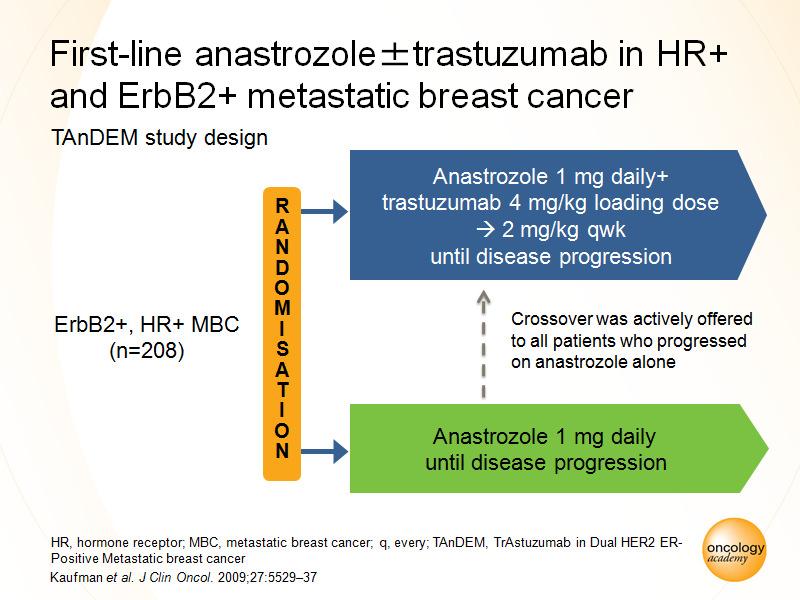
9 ER + / HER-2+ MBC For highly selected patients* with ER+/HER-2+ MBC, for whom ET is chosen over CT, ET should be given in combination with anti-her-2 therapy (either trastuzumab or lapatinib) since the combination provides PFS benefit (i.e. time without CT ) compared to ET alone. (LoE: 1 A) (72%) The addition of anti-her-2 therapy to ET in the 1 st line setting has not led to a survival benefit but long-term follow was not collected in the available trials. In addition, this strategy is currently being directly compared with CT + anti-her2 therapy. * Will be defined in the manuscript
10

11 IMPORTANCE OF STARTING ANTI-HER-2 AGENT EARLY ON
12 ER + / HER-2+ MBC For patients with ER+/HER-2+ MBC, for whom CT + anti-her2 therapy was chosen as 1 st line therapy and provided a benefit, it is reasonable to use ET + anti-her2 therapy as maintenance therapy, after stopping CT, although this strategy has not been studied. (LoE: 1 C) (80%)
13 HER-2 POSITIVE MBC MAIN MESSAGES: All patients with HER-2+ MBC who relapse after adjuvant anti-her-2 therapy should be considered for further anti-her-2 therapy, except in the presence of contraindications (LoE: 1 B) (97%) CHANGE IN PARADIGM IN ONCOLOGY!
14 Trastuzumab Beyond Trastuzumab: GBG-26 Study MBC HER2-positive Progression under trastuzumab-based first-line therapy (TFI < 6 weeks) with taxane (n = 114) or monotherapy or nontaxane (n = 42) R Capecitabine 2500 mg/m 2 bid d1-14 q21 days + continuation of trastuzumab 6 mg/kg q3 weeks (n = 78) Capecitabine 2500 mg/m 2 bid d1-14 q21 days (n = 78) R, randomization; TFI, treatment-free interval; MBD, metastatic breast cancer Von Minckwitz G, et al. J Clin Oncol. 2009;27(12):
15 Continuation of Trastuzumab Prolongs Time to Progression by Nearly 3 Months PFS Probability * Time from 1st progression, months * Trastuzumab + Capecitabine (n = 78) Capecitabine (n = 78) HR = 0.69 (two-sided P =.0338; one-sided P =.0169) Von Minckwitz G, et al. J Clin Oncol. 2009;27(12): *Median TTP in months TTP, time to progression; HR hazard ratio
16 HER-2 POSITIVE MBC In patients achieving a complete remission, the optimal duration of maintenance anti-her2 therapy is unknown and needs to be balanced against treatment toxicity, logistical burden and cost. Stopping anti-her2 therapy, after several years of sustained complete remission, may be considered in some patients, particularly if treatment re-challenge is available in case of progression. (LoE: Expert Opinion) (93%)
17 HER-2 POSITIVE MBC In the 1 st line setting, for HER-2+ MBC previously treated (in the adjuvant setting) or untreated with trastuzumab, combinations of CT + trastuzumab are superior to combinations of CT + lapatinib in terms of PFS and OS. (LoE: 1 A) (85%)
18 Gelmon, K. ASCO 2012 MA.31/ EGF COMPLETE TRIAL
19 MA.31/ EGF COMPLETE TRIAL Treatment Discontinuations OFF PROTOCOL TREATMENT (n = 382) LTAX/L=202 TTAX/T=180 Reason Number (%) Number (%) Death 5 (2.5) 10 (5.6) Intercurrent Illness 3 (1.5) 3 (1.7) Progressive Disease 143 (70.8) 121 (67.2) Toxicity 36 (17.8) 19 (10.6) Refused Treatment 2 (1.0) 4 (2.2) Symptomatic Progression 4 (2.0) 3 (1.7) Other 9 (4.5) 20 (11.1) Gelmon, K. ASCO 2012


20 NEW QUESTION: The optimal timing to use lapatinib? CEREBEL trial MA 31 Trial HR: 1.70 ( ) X ALTTO Trial ADAPTED FROM JAVIER CORTES
21 EGF104900: Phase III Study Evaluated Dual HER2 Blockade HER2 (FISH+/IHC3+) metastatic breast cancer Progression on Anthracycline Taxane Trastuzumab Progression on most recent trastuzumab regimen R A N D O M IZ E Lapatinib 1500 mg/d PO (n = 148) Crossover allowed to lapatinib + trastuzumab if progression after at least 4 weeks on therapy Primary endpoint: Progression-free survival Secondary endpoints: Overall survival Overall response rate Clinical benefit rate Lapatinib 1000 mg/d PO + trastuzumab 4 2 mg/kg IV weekly (n = 148) Staging occurred at 4, 8, 12, 16 weeks, and then every 8 weeks Steady state of single-agent lapatinib occurs at approximately 7 days Blackwell KL, J Clin Oncol 2010;28(7): Blackwell KL, et al. Cancer Res. 2009;69(24 Suppl): Abstract 61.
.74 (.57-.97) Log-rank P-value.")
22 EGF104900: Significant Overall Survival (OS) Benefit With Trastuzumab + Lapatinib Following Disease Progression % L N = 148 L+T N = 148 Died, N (%) 113 (78) 105 (72) Survival, % % 6 Month OS 56% 41% Median, months Hazard ratio (95% CI).74 ( ) Log-rank P-value Month OS Patients at risk: Time from Randomization, months L L+T Blackwell KL, et al. Cancer Res. 2009;69(Suppl 2): Abstract 61.

23 Trastuzumab and Pertuzumab Bind to Different Regions on HER2 and Have Synergistic Activity Trastuzumab HER2 receptor Pertuzumab Dimerisation domain of HER2 Subdomain IV of HER2 Trastuzumab suppresses HER2 activity Flags cells for destruction by the immune system Pertuzumab inhibits HER2 heterodimerization THE CONCEPT OF DUAL BLOCKADE Suppresses multiple HER signaling pathways Flags cells for destruction by the immune system
24 CLEOPATRA TRIAL: Phase III, Randomized, Double-Blind, Placebo- Controlled; Placebo + Trastuzumab + Docetaxel vs. Pertuzumab + Trastuzumab + Docetaxel in Patients with Previously Untreated HER-2+ MBC n=406 Placebo + trastuzumab PD Patients with HER2-positive MBC centrally confirmed (N = 808) 1:1 Docetaxel* 6 cycles recommended Pertuzumab + trastuzumab PD n=402 Docetaxel* 6 cycles recommended PRIMARY ENDPOINT: PFS Randomization was stratified by geographic region and prior treatment status (neo/adjuvant chemotherapy received or not) *<6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion Baselga, J. SABCS 2011
25 CLEOPATRA TRIAL: Median PFS and OS CAUTION!!!! Only 21% -26% pts had previously received (neo)adjuvant trastuzumab Progression-free Survival (%) HR=0.62 p< Ptz+T+D: 18.5 mo. Pla+T+D: 12.4 mo. =6.1 mo Time (months) Overall Survival (%) HR 0.68 p = Ptz+T+D: 56.5 mo. Pla+T+D: 40.8 mo. =15.7 mo Time (months) Baselga et al., NEJM 2012., Swain et al., NEJM, 2015.
26 Overall survival subgroup analyses An exploratory subgroup analysis was performed for patients who had received prior neoadjuvant and/or adjuvant trastuzumab therapy (88 patients). The observed hazard ratio of 0.68 (95% CI ) indicates overall survival benefit in the pertuzumab arm for this subpopulation.
27 Adverse events (all grades) with 25% incidence or 5% difference between arms n (%) Placebo + trastuzumab + docetaxel (n=396) Pertuzumab + trastuzumab + docetaxel (n=408) Diarrhea 191 (48.2) 278 (68.1) Alopecia 240 (60.6) 248 (60.8) Neutropenia 197 (49.7) 216 (52.9) Nausea 168 (42.4) 179 (43.9) Fatigue 148 (37.4) 155 (38.0) Rash 95(24.0) 149 (36.5) Decreased appetite 105 (26.5) 121(29.7) Mucosal inflammation 79 (19.9) 112 (27.5) Asthenia 121 (30.6) 110 (27.0) Vomiting 97 (24.5) 104 (25.5) Peripheral edema 122 (30.8) 101 (24.8) Pruritus 40 (10.1) 68 (16.7) Constipation 101 (25.5) 63 (15.4) Febrile neutropenia 30 (7.6) 56 (13.7) Dry skin 23 (5.8) 44 (10.8) Highlighted are adverse events with 5% higher incidence No increase in cardiac toxicity!

28 Phase II Study of Pertuzumab, Trastuzumab, and Weekly Paclitaxel 36 evaluable pts with 1 st or 2 nd line HER2+ MBC ORR = 47% No cardiac events Datko F et al, SABCS Abstract P

29 Safety of pertuzumab plus trastuzumab plus vinorelbine for 1 st line treatment of pts with HER2-+ LABC or MBC Edith A. Perez, José Manuel López-Vega, Lucia Del Mastro, Thierry Petit, Claudio Zamagni, Ulrich Freudensprung, Lydie Bastière-Truchot, Ru Walker, Michael Andersson. SABCS 2013, Poster
30 1 st Line Phase III MARIANNE Study Patients with HER2 positive progressive or recurrent locally advanced breast cancer or previously untreated metastatic breast cancer n=1092 Patients stratified by: World region Neo/Adjuvant therapy (Y/N) Trastuzumab + taxane DID NOT SHOW SUPERIORITY OF DUAL BLOCKADE! Visceral disease (Y/N) T-DM1 + pertuzumab Great Trastuzumab majority and/or of pts previously pretreated with Trastuzumab lapatinib based therapy in (Y/N) the (neo)adjuvant setting T-DM1 + placebo Primary endpoints: PFS as assessed by IRF; Safety Secondary endpoints: OS; PFS by investigator; PRO analyses; Biomarkers Superiority design with a Non-inferiority analysis between each of the experimental arms and the control arm Interim futility analysis: Option to drop experimental arm
31
32
33 T-DM1 treatment resulted in non-inferior but not superior PFS compared with trastuzumab plus a taxane in pts with locally advanced or metastatic HER2+ BC. The addition of pertuzumab to T-DM1 provided no efficacy benefit
34 PHEREXA study design NCT HER2-positive MBC (centrally confirmed) Prior taxane and H Progression during or after H-based therapy for MBC N = Arm A: H (8 mg/kg 6 mg/kg) + X (1,250 mg/m 2 ) n = 224 Arm B: H (8 mg/kg 6 mg/kg) + X (1,000 mg/m 2 ) + P (840 mg 420 mg) n = 228 First pt included: Jan 30, 2010 Last pt included: Aug 12, 2013 Clinical cut-off: May 29, 2015 Presented by Ander Urruticoechea
35 Primary analysis: PFS by independent review facility ITT population Proportion progression-free Arm A Arm B Time (months) a Stratified. CI, confidence interval; FU, follow-up. Arm A: H + X (n = 224) Arm B: H + X + P (n = 228) Events, n (%) 158 (71) 168 (74) mpfs (months) (months) 2.1 HR (95% CI) a 0.82 ( ) Log-rank p-value a 0.07 mfu (months) Presented by Ander Urruticoechea
36 Secondary analysis: OS ITT population a Stratified. Proportion surviving Arm A Arm B Arm A: H + X (n = 224) Arm B: H + X + P (n = 228) Events, n (%) 115 (51) 98 (43) mos (months) (months) 8.0 HR (95% CI) a 0.68 ( ) mfu (months) Time (months) Statistical significance cannot be claimed due to the hierarchical testing of OS after the primary IRF PFS endpoint Presented by Ander Urruticoechea
37 HER-2 POSITIVE MBC: 1 st line The standard 1 st line therapy for patients previously untreated with anti-her-2 therapy is the combination of CT + trastuzumab and pertuzumab, because it has proven to be superior to CT + trastuzumab in terms of OS in this population. (LoE: 1 A) (86%) For patients previously treated (in the (neo)adjuvant setting) with anti-her-2 therapy, the combination of CT + trastuzumab and pertuzumab is an important option for 1 st line therapy. (LoE: 1 A) (76%) Few (88) of these pts were treated in the Cleopatra trial and all with trastuzumab-free interval > 12 months.
38 HER-2 POSITIVE MBC There are currently no data supporting the use of dual blockade with trastuzumab + pertuzumab and CT beyond progression (i.e. continuing dual blockade beyond progression) and therefore this 3 drug regimen should not be given beyond progression outside clinical trials. (86%) There are no data on how to treat patients who have a relapse after receiving CT + trastuzumab + pertuzumab in the early setting.
39 HER-2 POSITIVE MBC In a HER-2+ MBC patient, previously untreated with the combination of CT + trastuzumab + pertuzumab, it is acceptable to use this treatment after 1 st line, although currently no data exists in this setting. (LoE: Expert Opinion) (76%)
40 HER-2 POSITIVE MBC After 1 st line trastuzumab-based therapy, T-DM1 provides superior efficacy relative to other HER-2-based therapies in the 2 nd line (vs. lapatinib + capecitabine) and beyond (vs. treatment of physician s choice). T-DM1 should be preferred in patients who have progressed through at least 1 line of trastuzumab-based therapy, because it provides an OS benefit. (LoE: 1 A) (88%) However, there are no data on the use of T-DM1 after dual blockade with trastuzumab + pertuzumab.


41 EMILIA Study Design HER2+ (central) LABC or MBC (N = 980) T-DM1 3.6 mg/kg q3w IV PD Prior taxane and trastuzumab Progression on metastatic tx or within 6 mos of adjuvant tx 1:1 Capecitabine 1000 mg/m 2 orally bid, days 1 14, q3w + Lapatinib 1250 mg/day orally qd PD Stratification factors: World region, number of prior chemo regimens for MBC or unresectable LABC, presence of visceral disease Primary end points: PFS by independent review, OS, and safety Key secondary end points: PFS by investigator, ORR, duration of response, time to symptom progression Blackwell K, et al. J Clin Oncol. 2012;30(15S): Abstract LBA1 & Vema S et al, ESMO 2012
42 EMILIA Study T-DM1 vs Cap+Lap ~5 MS BENEFIT IN OS Probably a new standard of care!
 PD 2 prior HER2-directed therapies for advanced BC Prior treatment with trastuzumab, lapatinib, and a taxane 1 Treatment of physician s choice (TPC) b (n=200) PD T-DM1 c")
43 TH3RESA Study Schema HER2-positive (central) advanced BC a (N=600) 2 T-DM1 3.6 mg/kg q3w IV (n=400) PD 2 prior HER2-directed therapies for advanced BC Prior treatment with trastuzumab, lapatinib, and a taxane 1 Treatment of physician s choice (TPC) b (n=200) PD T-DM1 c (optional crossover) Stratification factors: World region, number of prior regimens for advanced BC, d presence of visceral disease Co-primary endpoints: PFS by investigator and OS Key secondary endpoints: ORR by investigator and safety a Advanced BC includes MBC and unresectable locally advanced/recurrent BC. b TPC could have been single-agent chemotherapy, hormonal therapy, or HER2-directed therapy, or a combination of a HER2-directed therapy with a chemotherapy, hormonal therapy, or other HER2-directed therapy. c First patient in: Sep Study amended Sep 2012 (following EMILIA 2nd interim OS results) to allow patients in the TPC arm to receive T-DM1 after documented PD. d Excluding single-agent hormonal therapy. BC, breast cancer; IV, intravenous; ORR, objective response rate; PD, progressive disease; q3w, every 3 weeks


44 SUPERIOR PFS SABCS % of TPC arm pts received T-DM1 crossover therapy 3 ms OS BENEFIT
45 COMMON TOXICITIES OF T-DM1 Thrombocytopenia Grade 3 in approximately 10% of patients Nadir on day 8; Nadir is typically lowest in cycle 1 Not typically cumulative Usually manageable with dose reduction Severe hemorrhage is rare, but small number of cases have been reported Transaminase elevation Grade 3 in approximately 5% of patients Not typically cumulative Usually manageable with dose reduction Severe hepatic dysfunction very rare Diéras et al, SABCS 2012, Abstract P
46 UNCOMMON TOXICITIES OF T-DM1 Pneumonitis( 1% of pts) Typically grade 1/2 T-DM1 should be discontinued Nodular regenerative hyperplasia (<0.5%) Can lead to noncirrhotic portal hypertension Requires biopsy to diagnose T-DM1 should be discontinued Diéras et al, SABCS 2012, Abstract P
47 HER-2 POSITIVE MBC In patients achieving a complete remission, the optimal duration of maintenance anti-her2 therapy is unknown and needs to be balanced against treatment toxicity, logistical burden and cost. Stopping anti-her2 therapy, after several years of sustained complete remission, may be considered in some patients, particularly if treatment re-challenge is available in case of progression. (LoE: Expert Opinion) (93%)
48 HER-2 POSITIVE MBC: CHEMOTHERAPY COMPONENT Regarding the CT component of HER-2 positive MBC treatment: When pertuzumab is not given, 1 st line regimens for HER-2 MBC can include trastuzumab combined with a vinorelbine or a taxane. (LoE: 1 A) (88%) Differences in toxicity between these regimens should be considered and discussed with the patient in making a final decision. Other CT agents can be administered with trastuzumab but are not as well studied and are not preferred. In manuscript: Single agent vinorelbine in association with anti-her-2 therapy has shown superior or equal efficacy compared to taxanes and has a better tolerability.
49 Extrapolating from HER-2+ disease: Vinorelbine seems at least as good as taxane and significantly less toxic TRAVIOTA: Taxane + Trastuzumab vs. Vinorelbine + Trastuzumab Vinorelbine & Capecitabine: Consistent efficacy results & NO ALOPECIA First-line MBC No prior trastuzumab Measurable Disease N=81 RR Paclitaxel or Docetaxel + Trastuzumab Vinorelbine + Trastuzumab TTP Taxane Arm 58% 6.0 months Vinorelbine Arm 66% 8.5 months p=0.09 Burstein HJ, et al. Cancer. 2007;110:
50 HER-2 POSITIVE MBC: CHEMOTHERAPY COMPONENT For later lines of therapy, trastuzumab can be administered with several CT agents, including but not limited to, vinorelbine (if not given in 1 st line), taxanes (if not given in 1 st line), capecitabine, eribulin, liposomal anthracyclines, platinum, gemcitabine, or metronomic CM. (LoE: 2 A) 891%) The decision should be individualized and take into account different toxicity profiles, previous exposure, patient preferences, and country availability.
51 HER-2 POSITIVE MBC: CHEMOTHERAPY COMPONENT CT agents to combine with a dual blockade of trastuzumab + pertuzumab are docetaxel (LoE: 1 A) or paclitaxel (LoE: 1 B). Also possible are vinorelbine (LoE: 2 A) and nab-paclitaxel (LoE: 2 B). (86% Consensus)
52 New anti-her agents

53 Margetuximab-Fc-optimized anti-her2 Monoclonal Ab Derived from 4D5, parent antibody of trastuzumab Margetuximab and trastuzumab bind same epitope on HER2 with high affinity Fc domain modifications enhance NK cell and macrophage activation Enhanced binding to low affinity variants of activating Fcγ receptor, CD16A Diminished binding to inhibitory Fcγ receptor, CD32B Enhanced antibody dependent cell-mediated cytotoxicity in vitro Patients with high affinity Fc receptors had prolonged PFS with trastuzumab (Musolino et al., J Clin Oncol 26: (2008)) SOPHIA will test if enhanced ADCC leads to superior outcomes in HER+ MBC Nordstrom JL, et al. Breast Cancer Research 13:R123,
 R 1:1 Randomization (n = 530) Arm 2 trastuzumab + chemotherapy Sequential Primary Endpoints: Progression-Free Survival & Overall Survival: PFS")
54 SOPHIA Study to Establish Superiority to Trastuzumab Arm 1 margetuximab + chemotherapy HER2+ mbc, 1-2 lines in metastatic setting (prior trastuzumab, pertuzumab, T-DM1) PI Choice of Chemotherapy (capecitabine, eribulin, gemcitabine or vinorelbine) R 1:1 Randomization (n = 530) Arm 2 trastuzumab + chemotherapy Sequential Primary Endpoints: Progression-Free Survival & Overall Survival: PFS (N=257, HR=0.67, α=0.05, power=90%) OS (N=358, HR=0.75, α=0.05, power=80%) 54
55 Brain Metastases
56 Incidence of CNS Metastases in Trastuzumab-Treated Patients Case Series Patient Population # Overall % Bendell et al, 2003 Trastuzumab-treated Clayton et al, 2004 Trastuzumab-treated Lai et al, 2004 Trastuzumab-treated Lower et al, 2003 Trastuzumab-treated Non-trastuzumab-treated Pinder et al, 2007 Trastuzumab-treated first-line Non-trastuzumab-treated Shmueli et al, 2004 Trastuzumab-treated Stemmler et al, 2006 Trastuzumab-treated Yardley et al, 2007 HER2-positive MBC Yau et al, 2006 Trastuzumab-treated Leyland-Jones B. J Clin Oncol. 2009;27(31):
57 BRAIN METASTASES Patients with a single or a small number of potentially resectable brain metastasis should be treated with surgery or radiosurgery. Radiosurgery is also an option for some unresectable brain metastases. (LoE: 1 B) (92%) If surgery/radiosurgery is performed it may be followed by whole brain radiotherapy but this should be discussed in detail with the patient, balancing the longer duration of intracranial disease control and the risk of neurocognitive effects (LoE: 1 B) (72%) A multi-disciplinary discussion including neurosurgeons, radiation oncologists and medical oncologists is indispensable in determining the optimal treatment for each patient. The treatment plan can also be a combination of these three available therapeutic approaches
58 HER-2 POSITIVE MBC & BRAIN METASTASES Because patients with HER2+ve MBC and brain metastases can live for several years, consideration of long term toxicity is important and less toxic local therapy options (e.g. stereotactic RT) should be preferred to whole brain RT, when available and appropriate (e.g. in the setting of a limited number of brain metastases). (LoE: 1C) (89%)
59 HER-2 POSITIVE MBC & BRAIN METASTASES in patients with HER2 positive ABC who develop brain metastases with stable extracranial disease, systemic therapy should not be changed. (LoE: 1 C) (95%) For patients with HER2 positive cancers where brain metastases are the only site of recurrence, the addition of CT to local therapy is not known to alter the course of the disease. It is recommended to re-start the anti-her2 therapy (trastuzumab) if this had been stopped. (LoE: 1 C) (83%)
 HER2 negative (n = 48) P<.0001 40 20 0 0 10 20 30 40 Time from diagnosis of mcns disease (months) Kirsch DG, et al. J Clin Oncol.")
60 Trastuzumab Improves Survival in Patients With mcns Disease: U S Retrospective Analysis Survival (%) HER2 positive, trastuzumab (n = 36) HER2 positive, no trastuzumab (n = 11) HER2 negative (n = 48) P< Time from diagnosis of mcns disease (months) Kirsch DG, et al. J Clin Oncol. 2005;23(9):
61 LANDSCAPE STUDY: a FNCLCC phase II study with lapatinib and capecitabine in pts with brain metastases from HER-2+ MBC before whole brain RT 45 pts Primary endpoint: CNS volumetric response CNS-OR: 29/43 = 67.4% (95% CI: 52-81) CNS volumetric change N = 43 (%) 80% reduction 9 (20.9) 50-<80% reduction 20 (46.5) 20- <50% reduction 6 (14) > 0- <20% reduction 2 (4.7) Progression* 6 (14) * 2 patients had extra-cns disease progression NSS improvement: 14/24 = 58.3% (95% CI: ) IMP: pts previously untreated with WBRT; phase 2 study Bachelot et al, ASCO 2011
62 CEREBEL Study: A Phase III Randomized Open-Label Study of Lapatinib plus Capecitabine vs Trastuzumab + Capecitabine in HER2-Positive Metastatic Breast Cancer Inclusion Criteria: Stage IV HER2+ breast cancer Prior anthracycline and a taxane Prior treatment with CT, trastuzumab, HT, RT is permitted LVEF 50%, normal organ function Main Exclusion Criteria: History and/or current evidence of CNS metastases Prior therapy with lapatinib or ErbB2 inhibitor other than trastuzumab R A N D O M I Z E EARLY CLOSURE!! Capecitabine 2500 mg/m 2 bid d1-14 q21 days + Trastuzumab loading dose 8 mg/kg 6 mg/kg q3 weeks 475 pts enrolled 40% completed 12 months, had PD or died Lapatinib 1250 mg PO qd continuously + capecitabine 2000 mg/m 2 /d PO days 1-14 q3 weeks Primary endpoint: Incidence of CNS metastases at site of first relapse Secondary endpoints: Incidence of CNS progression at any time, time to first CNS progression, PFS, OS, ORR, CBR, duration of response, toxicity, pharmacogenetics, and biomarker analysis
63 Primary endpoint: CNS endpoints (modified ITT) Lapatinib + capecitabine (N=251) Trastuzumab + capecitabine (N=250) CNS as first site of relapse, n (%) 8 (3) 12 (5) Incidence of CNS progression at any time, n (%) Time to first CNS progression, median (range) 17 (7) 15 (6) OR (95% CI) 0.65 (0.26, 1.63) 1.14 (0.52, 2.51) p-value (2 17) 4.4 (2 27) - - LOW NUMBER OF BRAIN METS TRASTUZUMAB + CAPECITABINE BETTER
64 HER-2 POSITIVE MBC All patients with HER-2+ MBC who relapse after adjuvant anti- HER-2 therapy should be considered for further anti-her-2 therapy, except in the presence of contraindications (LoE: 1 B) (97%) The choice of the anti-her-2 agent will depend on countryspecific availability, the specific anti-her-2 therapy previously administered, and the relapse free interval. (88%) The optimal sequence of all available anti-her-2 therapies is currently unknown. (88%) The optimal duration of anti-her-2 therapy for MBC (i.e. when to stop these agents) is currently unknown. (97%)
65 MANAGEMENT OF HER-2 + MBC: MANY QUESTIONS SILL UNANSWERED Optimal duration of anti-her-2 therapy for ABC (indefinitely?) At progression should only the cytotoxic drug be changed of both the cytotoxic and the anti-her-2 agent Is treatment beyond PD also true for other anti-her-2 agents? Dual blockade for everyone or some? The role of the dual blockade without CT Triple blockade? Best sequence of anti-her-2 therapies Mechanisms of resistance & ways to overcome it; Predictive markers (role of PI3K mutations,...) NEW ANTI-HER-2 AGENTS in development




66
SYSTEMIC THERAPY FOR HER-2+ ABC
 SYSTEMIC THERAPY FOR HER-2+ ABC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & NR Committee Chair EORTC
SYSTEMIC THERAPY FOR HER-2+ ABC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & NR Committee Chair EORTC
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
New Drug Development in HER2+ Breast Cancer
 New Drug Development in HER2+ Breast Cancer Philippe Aftimos, M.D. Senior Research Physician Clinical Pharmacology Unit Institut Jules Bordet Background Amplification of HER2 occurs in approximately 20%
New Drug Development in HER2+ Breast Cancer Philippe Aftimos, M.D. Senior Research Physician Clinical Pharmacology Unit Institut Jules Bordet Background Amplification of HER2 occurs in approximately 20%
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Her 2 Positive Metastatic Breast Cancer
 Her 2 Positive Metastatic Breast Cancer Alison Jones November 2013 Mrs Hermione Positive (then and now!) Diagnosed 2007 T2 N1 Mo ER ve; Her2 ve Mastectomy ANC; FEC/T Herceptin (12months) August 2010metastatic
Her 2 Positive Metastatic Breast Cancer Alison Jones November 2013 Mrs Hermione Positive (then and now!) Diagnosed 2007 T2 N1 Mo ER ve; Her2 ve Mastectomy ANC; FEC/T Herceptin (12months) August 2010metastatic
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
A vision for HER2 future
 School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Advances in the Management of Metastatic Her 2 Positive Breast Cancer
 Advances in the Management of Metastatic Her 2 Positive Breast Cancer Sunil Verma MD, MSEd, FRCPC Medical Oncologist Research Lead, Division of Medical Oncology Chair, Breast Medical Oncology Sunnybrook
Advances in the Management of Metastatic Her 2 Positive Breast Cancer Sunil Verma MD, MSEd, FRCPC Medical Oncologist Research Lead, Division of Medical Oncology Chair, Breast Medical Oncology Sunnybrook
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Enfermedad con sobreexpresión de HER-2 neu
 Enfermedad con sobreexpresión de HER-2 neu Elsa Dalmau Parc Taulí Sabadell. Hospital Universitari. Enfermedad con sobreexpresión de HER-2 neu ÍNDICE Neoadyuvancia Adyuvancia Enfermedad avanzada Enfermedad
Enfermedad con sobreexpresión de HER-2 neu Elsa Dalmau Parc Taulí Sabadell. Hospital Universitari. Enfermedad con sobreexpresión de HER-2 neu ÍNDICE Neoadyuvancia Adyuvancia Enfermedad avanzada Enfermedad
Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy. Javier Cortes, Ramon y
 Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation
Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Emerging Agents in HER2-positive Disease. Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ
 Emerging Agents in HER2-positive Disease Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ Signal Transduction by the HER Family and Potential Mechanisms
Emerging Agents in HER2-positive Disease Mary Cianfrocca, DO Director, Breast Oncology Program Banner MD Anderson Cancer Center Gilbert, AZ Signal Transduction by the HER Family and Potential Mechanisms
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Management of HER2+ MBC SOBO 2012 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for Women s Cancer
Northwestern University Feinberg School of Medicine Management of HER2+ MBC SOBO 2012 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for Women s Cancer
Breast cancer update. Iryna Kuchuk, MD Oncology department Meir Medical Center
 Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
José Baselga, MD, PhD
 i n t e r v i e w José Baselga, MD, PhD Dr Baselga is Physician-in-Chief at Memorial Sloan-Kettering Cancer Center in New York, New York. Tracks 1-15 Track 1 Track 2 Track 3 Track 4 Track 5 Track 6 Track
i n t e r v i e w José Baselga, MD, PhD Dr Baselga is Physician-in-Chief at Memorial Sloan-Kettering Cancer Center in New York, New York. Tracks 1-15 Track 1 Track 2 Track 3 Track 4 Track 5 Track 6 Track
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer * Substances without published evidence based on at
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer * Substances without published evidence based on at
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot
 Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Post-ESMO 2012: Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich T.Rordorf, SAMO Luzern 1
 Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Policy No: dru281. Medication Policy Manual. Date of Origin: September 24, Topic: Perjeta, pertuzumab. Next Review Date: May 2015
 Medication Policy Manual Topic: Perjeta, pertuzumab Committee Approval Date: May 9, 2014 Policy No: dru281 Date of Origin: September 24, 2012 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPORTANT
Medication Policy Manual Topic: Perjeta, pertuzumab Committee Approval Date: May 9, 2014 Policy No: dru281 Date of Origin: September 24, 2012 Next Review Date: May 2015 Effective Date: June 1, 2014 IMPORTANT
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Il trattamento medico
 III Sessione: La malattia in fase avanzata Il trattamento medico Emilio Bria Oncologia, Dipartimento di Medicina, Università di Verona, Azienda Ospedaliera Universitaria Integrata Verona emilio.bria@univr.it
III Sessione: La malattia in fase avanzata Il trattamento medico Emilio Bria Oncologia, Dipartimento di Medicina, Università di Verona, Azienda Ospedaliera Universitaria Integrata Verona emilio.bria@univr.it
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
PIK3CA Mutations in HER2-Positive Breast Cancer
 2016.4.29. GBCC PIK3CA Mutations in HER2-Positive Breast Cancer Seock-Ah Im, MD, PhD. Department of Internal Medicine Seoul National University Hospital Contents Introduction TCGA data HER2 signaling pathway
2016.4.29. GBCC PIK3CA Mutations in HER2-Positive Breast Cancer Seock-Ah Im, MD, PhD. Department of Internal Medicine Seoul National University Hospital Contents Introduction TCGA data HER2 signaling pathway
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Novel Preoperative Therapies for HER2-Positive Breast Cancer
 Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Nuovo paradigma terapeutico nel trattamento del carcinoma mammario HER2+ metastatico: dagli studi alla pratica clinica Prima linea di trattamento
 Nuovo paradigma terapeutico nel trattamento del carcinoma mammario HER2+ metastatico: dagli studi alla pratica clinica Prima linea di trattamento Prof. Sabino De Placido Dip. di Endocrinologia ed Oncologia
Nuovo paradigma terapeutico nel trattamento del carcinoma mammario HER2+ metastatico: dagli studi alla pratica clinica Prima linea di trattamento Prof. Sabino De Placido Dip. di Endocrinologia ed Oncologia
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara
 Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
Cerebel trial Any impact on the clinical practice? Antonio Frassoldati Oncologia Clinica - Ferrara CNS metastases in HER2+ BC The proportion of patients with HER2+ advanced breast cancer who have CNS metastases
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
Current Management of Breast Cancer
 Current Management of Breast Cancer F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program Coordinator
Current Management of Breast Cancer F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program Coordinator
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
(Neo) Adjuvant systemic therapy for HER-2+ EBC
 Adjuvant systemic therapy for HER-2+ EBC") (Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
(Neo) Adjuvant systemic therapy for HER-2+ EBC F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESMO Board of Directors & NR Committee Chair ESO Breast Cancer Program
Lo studio BOLERO-1 Quali potranno essere le future ricadute nella pratica clinica? Antonella Ferro UO Oncologia Medica Trento
 Lo studio BOLERO-1 Quali potranno essere le future ricadute nella pratica clinica? Antonella Ferro UO Oncologia Medica Trento TRASTUZUMAB most important breakthrough in the management of BC Trastuzumab
Lo studio BOLERO-1 Quali potranno essere le future ricadute nella pratica clinica? Antonella Ferro UO Oncologia Medica Trento TRASTUZUMAB most important breakthrough in the management of BC Trastuzumab
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
Update HER2. Rupert Bartsch. Department of Medicine 1, Clinical Division of Oncology Comprehensive Cancer Center Vienna Medical University of Vienna
 Update HER2 Rupert Bartsch Department of Medicine 1, Clinical Division of Oncology Comprehensive Cancer Center Vienna Medical University of Vienna HER2: A Unique Story of Success Analysis of outcome in
Update HER2 Rupert Bartsch Department of Medicine 1, Clinical Division of Oncology Comprehensive Cancer Center Vienna Medical University of Vienna HER2: A Unique Story of Success Analysis of outcome in
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands
 What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
Innovations In The Management Of
 Innovations In The Management Of HER2+ Breast Cancer Dr. Sandeep Goyle Consultant Medical Oncologist Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute Mumbai, India Introduction - Self
Innovations In The Management Of HER2+ Breast Cancer Dr. Sandeep Goyle Consultant Medical Oncologist Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute Mumbai, India Introduction - Self
HER2 Biology and Treatment in Breast Cancer
 HER2 Biology and Treatment in Breast Cancer Sandra M. Swain, MD, FACP Director, Washington Cancer Institute Washington Hospital Center Professor of Medicine Georgetown University Washington DC Off-Label
HER2 Biology and Treatment in Breast Cancer Sandra M. Swain, MD, FACP Director, Washington Cancer Institute Washington Hospital Center Professor of Medicine Georgetown University Washington DC Off-Label
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre
 Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Dennis J Slamon, MD, PhD
 I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
Resistance to anti-her2 therapies. Service d Oncologie Médicale
 Resistance to anti-her2 therapies Pr David Khayat Service d Oncologie Médicale Groupe Hospitalier Pitié Salpêtrière -Paris Disclosure statment Trastuzumab in HER2+ MBC A major impact but resistance will
Resistance to anti-her2 therapies Pr David Khayat Service d Oncologie Médicale Groupe Hospitalier Pitié Salpêtrière -Paris Disclosure statment Trastuzumab in HER2+ MBC A major impact but resistance will
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
2014 San Antonio Breast Cancer Symposium Review
 2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Present and emerging treatment options in Her-2/neu overexpressing metastatic breast cancer
 Present and emerging treatment options in Her-2/neu overexpressing metastatic breast cancer Christoph C. Zielinski Clinical Division of Oncology, Department of Medicine I and Comprehensive Cancer Center,
Present and emerging treatment options in Her-2/neu overexpressing metastatic breast cancer Christoph C. Zielinski Clinical Division of Oncology, Department of Medicine I and Comprehensive Cancer Center,
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Metastasi viscerali: altre opzioni oltre la chemioterapia. Ormonoterapia e Agentianti-Her2. - Valentina Sini -
 Metastasi viscerali: altre opzioni oltre la chemioterapia. Ormonoterapia e Agentianti-Her2 - Valentina Sini - Metastatic Breast Cancer ER- Her2-20% ER- Her2+ ER+ Her2+ 5% 15% ER+ Her2- ER+ Her2+ ER- Her2+
Metastasi viscerali: altre opzioni oltre la chemioterapia. Ormonoterapia e Agentianti-Her2 - Valentina Sini - Metastatic Breast Cancer ER- Her2-20% ER- Her2+ ER+ Her2+ 5% 15% ER+ Her2- ER+ Her2+ ER- Her2+
Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA
 For projector and public [noacic] Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA 1 st Appraisal Committee meeting
For projector and public [noacic] Lead team presentation Eribulin for treating locally advanced or metastatic breast cancer after two or more prior chemotherapy regimens STA 1 st Appraisal Committee meeting
Page. Objectives: Hormone Therapy Resistance: Challenges and Opportunities. Research Support From Merck
 Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
DEBATE: NUEVOS TRATAMIENTOS EN CÁNCER DE MAMA POSICIONAMIENTO Y ALGORITMO TERAPÉUTICO CÁNCER DE MAMA HER 2 POSITIVO
 DEBATE: NUEVOS TRATAMIENTOS EN CÁNCER DE MAMA POSICIONAMIENTO Y ALGORITMO TERAPÉUTICO CÁNCER DE MAMA HER 2 POSITIVO DEBATE: NUEVOS TRATAMIENTOS EN CÁNCER DE MAMA POSICIONAMIENTO Y ALGORITMO TERAPÉUTICO
DEBATE: NUEVOS TRATAMIENTOS EN CÁNCER DE MAMA POSICIONAMIENTO Y ALGORITMO TERAPÉUTICO CÁNCER DE MAMA HER 2 POSITIVO DEBATE: NUEVOS TRATAMIENTOS EN CÁNCER DE MAMA POSICIONAMIENTO Y ALGORITMO TERAPÉUTICO
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
AGO e. V. in der DGGG e.v. sowie in der DKG e.v.
 AGO e. V. in der DGGG e.v. sowie in der DKG e.v. Guidelines Breast Version 2015.1 www.ago-online.de Disease-Free and Overall Survival in Metastatic Breast Cancer AGO e. V. in der DGGG e.v. sowie in der
AGO e. V. in der DGGG e.v. sowie in der DKG e.v. Guidelines Breast Version 2015.1 www.ago-online.de Disease-Free and Overall Survival in Metastatic Breast Cancer AGO e. V. in der DGGG e.v. sowie in der
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
FDA Briefing Document Oncologic Drugs Advisory Committee Meeting. September 12, sbla /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc.
 Applicant: Genentech, Inc.") /51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
/51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned
 The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico
 Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of ncology (VHI), Medica Scientia
Secuencia óptima de tratamiento de quimioterapia en el cáncer de mama metastásico Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of ncology (VHI), Medica Scientia
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;