Unmet Medical Needs and Latest Multiple Myeloma Treatment
|
|
|
- Asher Robinson
- 5 years ago
- Views:
Transcription

 National University Health System (NUHS)")
 National University of Singapore")
1 Unmet Medical Needs and Latest Multiple Myeloma Treatment Professor Chng Wee Joo Director National University Cancer Institute of Singapore (NCIS) National University Health System (NUHS) Deputy Director Cancer Science Institute, Singapore (CSI) National University of Singapore (NUS) 15 Apr 2017
2
3 Treatment Goals Young Patients (<65 years) Best OS outcome with possibility of cure MRD negative and maintained Is this needed for all patients? Old Patients (>70 years) Maximize OS with good quality of life [Caveat: Cost to achieve these aims]
4 Treatment of Transplant Eligible NDMM
5 Phases of Treatment Induction Stem cell Transplant Consolidation Maintenance


6 Phases of Treatment Induction Stem cell Transplant Consolidation Maintenance Objective Rapid and Deep Response Able to harvest Minimal toxicity

7 Significant improvement in post-induction CR/nCR and VGPR rates with bortezomib-based induction regimens
8 EVOLUTION Trial: RVdC, RVd, and CyBorD in NDMM Induction 8, 3-week cycles Maintenance 4, 6-week cycles N = yrs old Untreated NDMM Karnofsky performance status 50% Rand Modified after interim analysis RVdC (n = 48) LEN: 15 mg PO; D 1-14 BORT: 1.3 mg/m 2 IV; D 1, 4, 8, 11 DEX: 40 mg PO; D 1, 8, 15 Cy: 500 mg/m 2 PO a ; D 1, 8 RVd (n = 42) LEN: 25 mg PO; D 1-14 BORT: 1.3 mg/m 2 IV; D 1, 4, 8, 11 DEX: 40 mg PO; D 1, 8, 15 CyBorD (n = 33) BORT: 1.3 mg/m 2 IV; D 1, 4, 8, 11 DEX: 40 mg PO; D 1, 8, 15 Cy: 500 mg/m 2 PO a ; D 1, 8 CyBorD-mod (n = 17) BORT: 1.3 mg/m 2 IV; D 1, 4, 8, 11 DEX: 40 mg PO; D 1, 8, 15 Cy: 500 mg/m 2 PO a ; D 1, 8, 15 Primary objective: Rate of CR + VGPR Secondary objectives: Safety, ORR, DOR, TTR, TTP, PFS, OS Thromboprophylaxis with aspirin, warfarin, or LMWH was required BORT 1.3 mg/m 2 IV; D 1, 8, 15, 22 Pts could undergo stem cell mobilization and transplant after 2 and 4 induction cycles, respectively a Given as a single dose, rounded to the nearest 50 mg. BORT, bortezomib; CR, complete response; Cy, cyclophosphamide; CyBorD, cyclophosphamide, bortezomib, dexamethasone; CyBorD-mod, cyclophosphamide, bortezomib, dexamethasone with modified cyclophosphamide dosing ; DEX, dexamethasone; DOR, duration of response; IV, intravenous; LEN, lenalidomide; LMWH, low molecular weight heparin; NDMM, newly diagnosed multiple myeloma; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; PO, by mouth; pt, patient; Rand, randomized; RVd, lenalidomide, bortezomib, and dexamethasone; RVdC, lenalidomide, bortezomib, dexamethasone, and cyclophosphamide; TTP, time to progression; TTR, time to response; VGPR, very good partial response. Kumar S et al. Blood. 2012;119:
9 EVOLUTION Trial: Response Patient experience on study RVdC (n = 48) RVd (n = 42) CyBorD (n = 33) CyBorD-mod (n = 17) Median follow-up, mos Median cycles, n (range) 5 (1-12) 6 (1-12) 6 (3-12) 6 (3-12) Best response across all cycles, n (%) ORR ( PR) 35 (88) 35 (85) 24 (75) 17 (100) CR 10 (25) 10 (24) 7 (22) 8 (47) scr 6 (15) 7 (17) 3 (9) 5 (29) VGPR 23 (58) 21 (51) 13 (41) 9 (53) Progression 1 (3) 1 (2) 1 (3) 0 Best response across all cycles among patients 65 yrs, n/n (%) CR 6/28 (21) 6/28 (21) 2/21 (10) 7/12 (58) VGPR 15/28 (54) 17/28 (61) 5/21 (24) 8/12 (67) ORR ( PR) 24/28 (86) 26/28 (93) 14/21 (67) 12/12 (100) CR, complete response; CyBorD, cyclophosphamide, bortezomib, dexamethasone; CyBorD-mod, cyclophosphamide, bortezomib, dexamethasone with modified cyclophosphamide dosing; ORR, overall response rate; PR, partial response; RVd, lenalidomide, bortezomib, and dexamethasone; RVdC, lenalidomide, bortezomib, dexamethasone, and cyclophosphamide; scr, stringent complete response; VGPR, very good partial response. Kumar S et al. Blood. 2012;119:
10 EVOLUTION Trial: Adverse Events Grade 3 Hematologic, n (%) RVdC (n = 48) RVd (n = 42) CyBorD (n = 33) CyBorD-mod (n = 17) Neutropenia 21 (44) 4 (10) 10 (30) 4 (24) Febrile neutropenia 4 (8) 1 (2) 2 (6) 0 Thrombocytopenia 7 (15) 5 (12) 4 (12) 0 Leukopenia 6 (13) 0 3 (9) 1 (6) Anemia 4 (8) 3 (7) 0 2 (12) Lymphopenia 4 (8) 1 (2) 4 (12) 0 Nonhematologic, n (%) Pneumonia 2 (4) 2 (5) 0 1 (6) Neuropathy 6 (13) 7 (17) 3 (9) 3 (18) Fatigue 8 (17) 3 (7) 1 (3) 0 Diarrhea 3 (6) 1 (2) 1 (3) 1 (6) Nausea 0 1 (2) 0 0 Thromboembolism 1 (2) CyBorD, cyclophosphamide, bortezomib, dexamethasone; CyBorD-mod, cyclophosphamide, bortezomib, dexamethasone with modified cyclophosphamide dosing; RVd, lenalidomide, bortezomib, and dexamethasone; RVdC, lenalidomide, bortezomib, dexamethasone, and cyclophosphamide. Kumar S et al. Blood. 2012;119:
11 IFM : Phase 3 Trial of CyBorD vs VTD Study Design Transplant-eligible patients with NDMM aged < 66 years Multicenter, prospective, randomized phase 3 trial of induction Tx prior to ASCT 170 patients randomized to four 21-day cycles of CyBorD BORT 1.3 mg/m²/d SC days 1, 4, 8 and 11 DEX 40 mg/d PO days 1-4 and 9-12 Cy 500 mg/m²/d PO days 1, 8, patients randomized to four 21-day cycles of VTD BORT 1.3 mg/m²/d SC days 1, 4, 8 and 11 DEX 40 mg/d PO days 1-4 and 9-12 THAL 100 mg/d PO days 1-21 ASCT, autologous stem cell transplant; BORT, bortezomib; Cy, cyclophosphamide; CyBorD, cyclophosphamide, bortezomib, dexamethasone; DEX, dexamethasone; NDMM, newly diagnosed multiple myeloma; PO, by mouth; SC, subcutaneous; THAL, thalidomide; Tx, therapy; VTD, bortezomib, thalidomide, dexamethasone. Moreau P et al. Blood. 2015;126:393.
12 IFM : Phase 3 Trial of CyBorD vs VTD Results and Authors Conclusions Outcome a CyBorD (n = 169) VTD (n = 169) P value CR, % VGPR, % PR, % CD34+ stem cell harvest, 10 6 /kg b Grade 3/4 adverse events, % Neutropenia Thrombocytopenia Anemia Peripheral neuropathy Patients achieved higher rates of VGPR and PR, greater harvest of stem cells, and less hematologic toxicity with VTD vs CyBorD Supports preferential use of VTD prior to ASCT a Intent-to-treat population. b CyBorD, n = 154; VTD, n = 157. ASCT, autologous stem cell transplant; CR, complete response; CyBorD, cyclophosphamide, bortezomib, dexamethasone; PR, partial response; SC, subcutaneous; VGPR, very good partial response; VTD, bortezomib, thalidomide, dexamethasone. Moreau P et al. Blood. 2015;126:393.
13 Phases of Treatment Induction Stem cell Transplant Consolidation Maintenance Objective Increase CR rates
14 Is ASCT still needed in Era of Novel Agents

15 Significant improvement in post-induction and posttransplant CR/nCR and VGPR rates with bortezomibbased induction regimens

16 16

17 17

18 IFM 2009: Phase 3 Trial of RVd ± ASCT Study Design 1-3 ASCT, autologous stem cell transplant; BORT, bortezomib; CR, complete response; CYC, cyclophosphamide; DEX, dexamethasone; G-CSF, granulocyte colony-stimulating factor; GEP, gene expression profiling; HR, hazard ratio; IFM, Intergroupe Francophone du Myelome; ISS, International Staging System; LEN, lenalidomide; MEL, melphalan; MRD, minimal residual disease; NDMM, newly diagnosed multiple myeloma; ORR, overall response rate; PFS, progression-free survival; PO, oral administration; pt, patient; RVd, lenalidomide, bortezomib, and low-dose dexamethasone; SC, stem cell; TTP, time to progression; VGPR, very good partial response. 1. Attal M et al. Blood. 2015;126: Avet-Loiseau H et al. Blood. 2015;126:
19 IFM 2009: Phase 3 Trial of RVd ± ASCT Patient Disposition RVd + ASCT (n = 350) RVd, no ASCT (n = 350) 3-yr PFS, % HR 1.5 (95% CI, ) Stratified log-rank P < yr OS, % Stratified log-rank P =.25 CR, % P < 0.01 SPM, n (%) 23 (6.6) 18 (5.1) PFS benefit of ASCT was consistent across subgroups including age ( or > 60 yrs), sex, Ig isotype (IgG or others), ISS stage (I or II or III), cytogenetics (standard or high risk), and response after 3 cycles of RVd (CR or not) ASCT, autologous stem cell transplant; CR, complete response; HR, hazard ratio; IFM, Intergroupe Francophone du Myelome; Ig, immunoglobulin; ISS, International Staging System; OS, overall survival; PFS, progression-free survival; RVd, lenalidomide, bortezomib, and low-dose dexamethasone; SPM, second primary malignancy. 1. Attal M et al. Blood. 2015;126:391.
20 Phases of Treatment Induction Stem cell Transplant Consolidation Maintenance Objective Increase MRD negative rates

21

22

23 How to deepen response - Consolidation 2 nd Mel 200 ASCT 2-4 cycles of consolidation treatment Ladetto M et al. JCO 2010; 28:
24 RANDOMIZATION INDUCTION VEL-THAL-DEX INDUCTION THAL-DEX PBSC COLLECTION CTX TRANSPLANTATION MEL 200 MEL 200 CONSOLIDATION VEL-THAL-DEX CONSOLIDATION THAL-DEX MAINTENANCE DEX Cavo et al. Blood 2012; 120: 9-19

25 25
26 Phases of Treatment Induction Stem cell Transplant Consolidation Maintenance Objective Maintain deepest response Increase OS Tolerable with good QoL

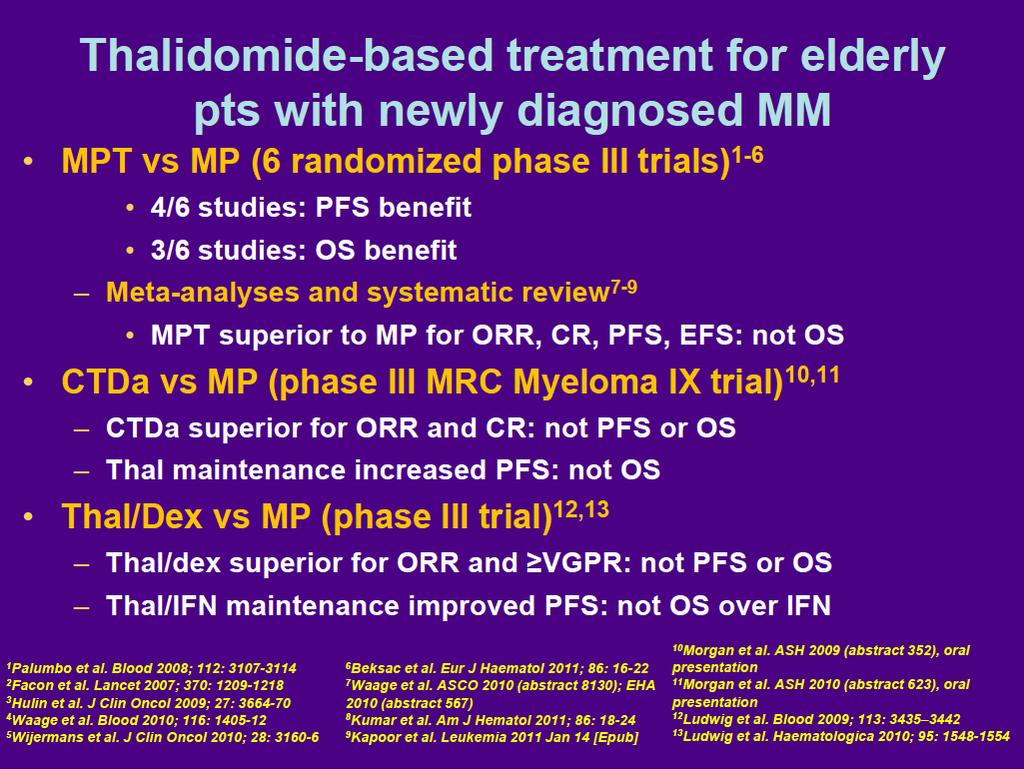
27 1. Attal M, et al. Blood. 2006;108: ; 2. Spencer A, et al. J Clin Oncol. 2009;27: ; 3. Barlogie B, et al. N Engl J Med. 2006;354: ; 4. Barlogie B, et al. Blood. 2008;112: ; 5. Barlogie B, et al, J Clin Oncol. 2010;28: ; 6. Lokhorst HM, et al. Blood. 2010;115: ; 7. Morgan GJ, et al. Blood. 2010;116. Abstract 623; 8. Stewart AK, et al. Blood. 2010;116. Abstract 39. Phase 3 Studies of Thalidomide Maintenance Thal Induction Treatment ASCT Maintenance Thal PFS/OS Increase Survival post-relapse Thal/PAM vs PAM vs None 1 2X + + / + Similar Thal/Pred vs Pred 2 1X + + / + Similar Thal vs No Thal X + + / + post-thal Thal vs IFN 6 + 1X/2X + + / post-thal Thal vs None 7 + 1X + + / post-thal Thal/Pred vs None 8 + 1X + + / post-thal PAM = pamidronate; PD = progressive disease.; Pred = prednisone; Thal = thalidomide.


28 LEN Maintenance After ASCT in MM: OS Analysis Studies Included in the Meta-Analysis a Starting dose of 10 mg/day on days 1-28/28 was increased to 15 mg/day if tolerated and continued until PD. b Patients received 10 mg/day on days 1-21/28 until PD. ASCT, autologous stem cell transplant; DEX, dexamethasone; LEN, lenalidomide; MM, multiple myeloma; MNTC, maintenance; MPR, melphalan, prednisone, and lenalidomide; NDMM, newly diagnosed multiple myeloma; OS, overall survival;; PD, progressive disease; Tx, treatment. Attal M, et al. Lenalidomide Maintenance After High-Dose Melphalan and Autologous Stem Cell Transplant in Multiple Myeloma: A Meta-Analysis of Overall Survival. ASCO 2016, abstract 8001.
.")
29 LEN Maintenance After ASCT in MM: OS Analysis OS 26% reduction in risk of death, with an estimated 2.5-year increase in median survival a a Median for LEN treatment arm was extrapolated to be 116 months based on median of the CTL arm and HR (median, 86 months; HR = 0.74). ASCT, autologous stem cell transplant; CTL, control; HR, hazard ratio; LEN, lenalidomide; MM, multiple myeloma; NE, not estimable; OS, overall survival; pt, patient. Attal M, et al. Lenalidomide Maintenance After High-Dose Melphalan and Autologous Stem Cell Transplant in Multiple Myeloma: A Meta-Analysis of Overall Survival. ASCO 2016, abstract 8001.

30 LEN Maintenance After ASCT in MM: OS Analysis Subgroup Analysis a Number of patients. b Cytogenetic data were only available for the IFM and GIMEMA studies. c CrCl post-asct data were only available for the CALGB and IFM studies. ASCT, autologous stem cell transplant; CR, complete response; CrCl, creatinine clearance; CTL, control; HR, hazard ratio; ISS, International Staging System; LEN, lenalidomide; MM, multiple myeloma; OS, overall survival; PD, progressive disease; PR, partial response; SD, stable disease; VGPR, very good partial response. Attal M, et al. Lenalidomide Maintenance After High-Dose Melphalan and Autologous Stem Cell Transplant in Multiple Myeloma: A Meta-Analysis of Overall Survival. ASCO 2016, abstract 8001.
31 Secondary Primary Malignancies Study name HR p-value IFM CALGB MM RV-MM-PI Summary estimate Outcome: Odds of developing secondary primary malignancy; LM vs placebo/no maintenance (>1 implies increased risk of secondary primary malignancy with LM) Minimal heterogeneity for estimate of secondary primary malignancy: Cochran Q = 1.67 (p = 0.644), I 2 = 0% Singh PP et al. Proc ASH 2013;Abstract 407.
32 Issues Related to Maintenance Universal improvement in PFS Rarely improve OS Quality of life becomes important Toxicity related to long-term use of therapeutic agent

33

34
35
36 Summary for Approach to Transplant Eligible patients Triplet induction Velcade based [VRD/KRD for HR patients] Transplant still needed [Double transplant for HR patients] Consider further consolidation for patient with suboptimal response Maintenance may prolong OS
37 Treatment of NDMM in transplant Ineligible Patients
38
39
 LEN + LoDEX: 18 Cycles (72 weeks) LENALIDOMIDE 25 mg")
40 RANDOMIZATION 1:1:1 (N = 1623) PD or Unacceptable Toxicity PD, OS, and Subsequent anti-mm Tx FIRST (MM-020): Final Survival Analysis Study Design 1,2 Screening Arm A Rd Continuous (n = 535) Active Tx + PFS Follow-Up Phase LEN + LoDEX: Continuously LENALIDOMIDE 25 mg days 1-21/28 LoDEX 40 mg days 1, 8, 15, 22/28 LT Follow-Up Arm B Rd18 (n = 541) LEN + LoDEX: 18 Cycles (72 weeks) LENALIDOMIDE 25 mg days 1-21/28 LoDEX 40 mg days 1, 8, 15, 22/28 Arm C MPT (n = 547) MEL + PRED + THAL 12 Cycles (72 weeks) MELPHALAN 0.25 mg/kg days 1-4/42 PREDNISONE 2 mg/kg days 1-4/42 THALIDOMIDE 200 mg days 1-42/42 Pts aged > 75 yrs: LoDEX 20 mg days 1, 8, 15, 22/28; THAL 100 mg days 1-42/42; MEL 0.2 mg/kg days 1-4 Stratification: Age ( 75 vs > 75 yrs), country, and ISS stage (I/II vs III) Thromboprophylaxis was mandatory Data cutoff: January 21, 2016 FIRST, Frontline Investigation of Revlimid and Dexamethasone versus Standard Thalidomide; ISS, International Staging System; LoDex, low-dose dexamethasone; LT, long-term; MM, multiple myeloma; OS, overall survival; PD, progressive disease; PFS, progression-free survival; pts, patients; Tx, treatment. 1. Facon T, et al. Final Analysis of Overall Survival From the FIRST Trial. ASH 2016, abstract Benboubker L, et al. N Engl J Med. 2014;371:
41 Survival Probability FIRST (MM-020): Final Survival Analysis Progression-Free Survival Updated PFS was prolonged with Rd continuous a 1.0 Results remain consistent nearly 3 years after the original PFS analysis year PFS Median PFS, mos 4-year PFS, % Rd continuous Rd MPT % HR (95% CI) Rd continuous vs MPT: 0.69 ( ), P < % 14.3% Progression-Free Survival (Months) a PFS is based on investigator assessment of IMWG criteria; Data cutoff: January 21, FIRST, Frontline Investigation of Revlimid and Dexamethasone versus Standard Thalidomide; HR, hazard ratio; IMWG, International Myeloma Working Group; MPT, melphalan, prednisone, thalidomide; PFS, progression-free survival; Rd continuous, lenalidomide plus low-dose dexamethasone until disease progression; Rd18, lenalidomide plus low-dose dexamethasone for 18 cycles. Facon T, et al. Final Analysis of Overall Survival From the FIRST Trial. ASH 2016, abstract 241.
42 Survival Probability FIRST (MM-020): Final Survival Analysis Overall Survival The pre-specified final OS analysis for the primary comparison showed that Rd continuous significantly extended OS vs MPT year OS 59.0% 58.0% Median OS, mos 4-yr OS, % Rd continuous Rd MPT % HR (95% CI) Rd continuous vs MPT: 0.78 ( ), P = Overall Survival (Months) FIRST, Frontline Investigation of Revlimid and Dexamethasone versus Standard Thalidomide; HR, hazard ratio; MPT, melphalan, prednisone, thalidomide; OS, overall survival; Rd continuous, lenalidomide plus low-dose dexamethasone until disease progression; Rd18, lenalidomide plus low-dose dexamethasone for 18 cycles. Facon T, et al. Final Analysis of Overall Survival From the FIRST Trial. ASH 2016, abstract 241.

43

44

45
46
47


48
49

50 VISTA: Bortezomib as Initial Standard Therapy in MM San Miguel et al. N Engl J Med 2008;359: ; Updated by Mateos et al JCO 2010

51 SWOG S0777: RVd vs Rd With Rd Maintenance Phase 3 Study Design 1,2 BORT, bortezomib; D, day; DEX, dexamethasone; HSV, herpes simplex virus; ISS, International Staging System; LEN, lenalidomide; NDMM, newly diagnosed multiple myeloma; ORR, overall response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PO, oral administration; pt, patient; Rd, lenalidomide and low-dose dexamethasone; RVd, bortezomib, lenalidomide, and low-dose dexamethasone; SCT, stem cell transplant. 1. Durie B et al. Blood. 2015;126:
52 SWOG S0777: RVd vs Rd With Rd Maintenance Survival Analyses RVd (n = 242) Rd (n = 232) Median PFS (95% CI), mos 43 (39-51) 31 (26-40) HR (96% Wald CI) ( ) 1-sided stratified log-rank P value.0066 a Median OS (95% CI), mos NR 63 (55-69) HR sided log-rank P value.0114 a This analysis reached the prespecified significance level of.02. HR, hazard ratio; Rd, lenalidomide and low-dose dexamethasone; NR, not reached; OS, overall survival; PFS, progression-free survival; Rd, lenalidomide and low-dose dexamethasone; RVd, bortezomib, lenalidomide, and low-dose dexamethasone. Durie B et al. Blood. 2015;126:25.
53 Summary of Approach to Transplant Ineligible Patients MP is no longer good enough MPR is not a good regimen MPT, Rd, VMP are all active VRd better than Rd Continuous treatment prolongs PFS
54 Management of Relapse Disease
55 Relapse situations Two clear scenarios Slow, asymptomatic relapse No symptoms Slowly progressing disease Low tumor burden Cytogenetic low risk Good performance status Fast, symptomatic relapse Symptoms Radiply progressing disease High tumor burden Organ involvement Cytogenetic high risk Poor performance status Observation Prompt treatment initiation needed The challenge: Identify appropriate time to initiate treatment for situations in between
56 How Does the Timing of Relapse Influence Treatment Decisions? Early relapse: within < 1 year May indicate resistant disease Change from initial treatment Incorporate novel agent, if not previously used Late relapse: after > 2 years Consider rechallenge with initial therapy If previous therapy was effective If previous therapy was given for a short, defined duration Consider addition of another agent
57 Can treatment be individualized at relapse?
58 Multiple factors drive treatment choice in relapsed/refractory MM Comorbidity e.g. renal impairment* Tolerance to prior therapies Side effects Treatment availability Prior therapies received Influential factors Pre-existing toxicities e.g. PN Time interval since last therapy Age Previous SCT Performance status Subtype e.g. t(4;14) *Occurs in up to 50% MM patients; Can repeat induction therapy where relapse occurs >6 mo. after treatment PN, peripheral neuropathy; SCT, stem cell transplant Moreau P, et al. Ann Oncol 2013;24:vi133 vi137; Lonial S. Hematology Am Soc Hematol Educ Program 2010;2010:
59 Options Thalidomide based Revlimid based (include retreatment) Velcade based (include retreatment) Triplet better than doublet Combiation Chemotherapy (DT-PACE, DCEP) Especially if extramedullary disease Transplant (including AlloSCT)
60 Emerging Therapies 1.New Generation Proteasome Inhibitor a) Carfilzomib (Onyx) Aspire, Endeavour b) Ixazomib (Millenium) - Tourmaline 2.New Generation Imids a) Pomalidomide (Celgene) MM003 3.Histone Deacetylase Inhibitor a) Panobinostat (Novartis) - Panorama 4.Monoclonal Antibodies a) Daratumumab (Anti-CD38) Sirius, Pollux, Castor b) Elotuzumab (Anti-CS1) - Eloquent 5.CDK4/6 Inhibitor 6.Venetoclax (BCL2) 7.Selinexor 8.Immunotherapies
61 Trials in Relapse MM (1-3 prior lines) Panorama Endeavour Castor Aspire Eloquant-2 Tourmaline-1 Pollux VD PVD VD KD VD DVD RD KRD RD Elo-RD RD IRD RD DRD ORR(%) CR (%) scr (%) NR NR 2 2 NR NR 4 14 NR NR NR NR 7 18 MRD NR NR NR NR NR NR NR NR NR NR NR NR 2 10 PFS/mths NR NR HR

 Response and progression (IMWG 2011 criteria 1 ) assessed by an independent")
62 Randomization TOURMALINE-MM1: Phase 3 study of weekly oral ixazomib plus lenalidomide-dexamethasone Global, double-blind, randomized, placebo-controlled study design N=722 1:1 Ixazomib + Lenalidomide + Dexamethasone Ixazomib: 4 mg on days 1, 8, and 15 Lenalidomide: 25 mg* on days 1-21 Dexamethasone: 40 mg on days 1, 8, 15, 22 Repeat every 28 days until progression, or unacceptable toxicity Stratification: Prior therapy: 1 vs 2 or 3 ISS: I or II vs III PI exposure: yes vs no Placebo + Lenalidomide + Dexamethasone Placebo: on days 1, 8, and 15 Lenalidomide: 25 mg* on days 1-21 Dexamethasone: 40 mg on days 1, 8, 15, 22 Primary endpoint: PFS Key secondary endpoints: OS OS in patients with del(17p) Response and progression (IMWG 2011 criteria 1 ) assessed by an independent review committee (IRC) blinded to both treatment and investigator assessment *10 mg for patients with creatinine clearance 60 or 50 ml/min, depending on local label/practice 1. Rajkumar S, et al. Blood 2011;117:
63 Outcomes by cytogenetic risk group IRd ORR, % VGPR, % CR, % Median PFS, months Placebo -Rd IRd Placebo -Rd Median OS was not reached in either arm IRd Placebo -Rd IRd Placebo -Rd All patients 78.3* * * * Standard-risk patients All high-risk patients * 79* 60 45* 21 12* Patients with * del(17p) Patients with t(4;14) alone *p<0.05 for comparison between regimens. Alone or in combination with t(4;14 or t(14;16). Data not included on patients with t(14:16) alone due to small numbers (n=7). HR In the IRd arm, median PFS in high-risk patients was similar to that in the overall patient population and in patients with standard-risk cytogenetics
64 Different Ixazomib Trials C16010 (Tourmaline 1) 5 patients C16013 Asia Phase 1 11 patients C16019 Phase 3 maintenance in posttransplant patients 10 patients C16021 Phase 3 maintenance in nontransplant eligible 8 patients (Ongoing

65 65
66
67
68 Click to add Title Click to add contents Second level Third level
69 Considerations in Making Choices Efficacy Toxicities Access / Cost Route of administration / Schedule / Logistics
70 Unmet Needs Treatment of HR disease Incl extramedullary disease, PCL Cost of Drugs and Drug Access Predictive Marker Choice of Drugs and combinations

71 Thank you for your attention
Update on Multiple Myeloma Treatment
 Update on Multiple Myeloma Treatment Professor Chng Wee Joo Director National University Cancer Institute of Singapore (NCIS) National University Health System (NUHS) Deputy Director Cancer Science Institute,
Update on Multiple Myeloma Treatment Professor Chng Wee Joo Director National University Cancer Institute of Singapore (NCIS) National University Health System (NUHS) Deputy Director Cancer Science Institute,
COMy Congress The case for IMids. Xavier Leleu. Hôpital la Milétrie, PRC, CHU, Poitiers, France
 Xavier Leleu Hôpital la Milétrie, PRC, CHU, Poitiers, France The case for IMids COMy Congress 21 Disclosures Grants/research support: Amgen, Bristol-Myers Squibb, Celgene, Janssen, Millennium/Takeda, Novartis,
Xavier Leleu Hôpital la Milétrie, PRC, CHU, Poitiers, France The case for IMids COMy Congress 21 Disclosures Grants/research support: Amgen, Bristol-Myers Squibb, Celgene, Janssen, Millennium/Takeda, Novartis,
Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma. Michele Cavo, MD University of Bologna Bologna, Italy
 Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma Michele Cavo, MD University of Bologna Bologna, Italy Treatment Paradigm for Autotransplant-Eligible Patients With Multiple Myeloma
Initial Therapy For Transplant-Eligible Patients With Multiple Myeloma Michele Cavo, MD University of Bologna Bologna, Italy Treatment Paradigm for Autotransplant-Eligible Patients With Multiple Myeloma
To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors
 To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors James Berenson, MD Institute for Myeloma and Bone Cancer Research West Hollywood, CA Financial Disclosures Takeda, Celgene
To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors James Berenson, MD Institute for Myeloma and Bone Cancer Research West Hollywood, CA Financial Disclosures Takeda, Celgene
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
Disclosures for Palumbo Antonio, MD
 Disclosures for Palumbo Antonio, MD Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board o relevant conflicts of interest to declare o relevant
Disclosures for Palumbo Antonio, MD Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board o relevant conflicts of interest to declare o relevant
Myeloma update ASH 2014
 Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
MULTIPLE MYELOMA. TREATMENT in 2017 MC. VEKEMANS
 MULTIPLE MYELOMA TREATMENT in 2017 MC. VEKEMANS NATURAL HISTORY of MM WHO SHOULD BE TREATED? DEFINITION MGUS Smouldering Multiple Myeloma Symptomatic Multiple Myeloma Monoclonal component (blood and/or
MULTIPLE MYELOMA TREATMENT in 2017 MC. VEKEMANS NATURAL HISTORY of MM WHO SHOULD BE TREATED? DEFINITION MGUS Smouldering Multiple Myeloma Symptomatic Multiple Myeloma Monoclonal component (blood and/or
IMiDs (Immunomodulatory drugs) and Multiple Myeloma
 and Multiple Myeloma") www.comtecmed.com/comy comy@comtecmed.com IMiDs (Immunomodulatory drugs) and Multiple Myeloma Xavier Leleu Service des Maladies du Sang Hôpital Huriez, CHRU, Lille, France www.comtecmed.com/comy comy@comtecmed.com
www.comtecmed.com/comy comy@comtecmed.com IMiDs (Immunomodulatory drugs) and Multiple Myeloma Xavier Leleu Service des Maladies du Sang Hôpital Huriez, CHRU, Lille, France www.comtecmed.com/comy comy@comtecmed.com
Multiple myeloma, 25 (45) years of progress. The IFM experience in patients treated with frontline ASCT. Philippe Moreau, Nantes
 years of progress. The IFM experience in patients treated with frontline ASCT. Philippe Moreau, Nantes") Multiple myeloma, 25 (45) years of progress The IFM experience in patients treated with frontline ASCT Philippe Moreau, Nantes Shibata T. Prolonged survival in a case of multiple myeloma treated with high
Multiple myeloma, 25 (45) years of progress The IFM experience in patients treated with frontline ASCT Philippe Moreau, Nantes Shibata T. Prolonged survival in a case of multiple myeloma treated with high
Is autologous stem cell transplant the best consolidation after initial therapy?
 Is autologous stem cell transplant the best consolidation after initial therapy? William Bensinger, MD Professor of Medicine, Division of Oncology University of Washington School of Medicine Director,
Is autologous stem cell transplant the best consolidation after initial therapy? William Bensinger, MD Professor of Medicine, Division of Oncology University of Washington School of Medicine Director,
How I Treat Transplant Eligible Myeloma Patients
 How I Treat Transplant Eligible Myeloma Patients Michele Cavo Seràgnoli Institute of Hematology, Bologna University School of Medicine, Italy Podcetrtek, Slovene, April 14 th, 2012 NEW TREATMENT PARADIGM
How I Treat Transplant Eligible Myeloma Patients Michele Cavo Seràgnoli Institute of Hematology, Bologna University School of Medicine, Italy Podcetrtek, Slovene, April 14 th, 2012 NEW TREATMENT PARADIGM
Role of consolidation therapy in Multiple Myeloma. Pieter Sonneveld. Erasmus MC Cancer Institute Rotterdam The Netherlands
 Role of consolidation therapy in Multiple Myeloma Pieter Sonneveld Erasmus MC Cancer Institute Rotterdam The Netherlands Disclosures Research support : Amgen, Celgene, Janssen, Karyopharm Advisory Boards/Honoraria:
Role of consolidation therapy in Multiple Myeloma Pieter Sonneveld Erasmus MC Cancer Institute Rotterdam The Netherlands Disclosures Research support : Amgen, Celgene, Janssen, Karyopharm Advisory Boards/Honoraria:
CREDIT DESIGNATION STATEMENT
 CME Information LEARNING OBJECTIVES Integrate emerging research information on the use of proteasome inhibitors and immunomodulatory agents to individualize induction treatment recommendations and maintenance
CME Information LEARNING OBJECTIVES Integrate emerging research information on the use of proteasome inhibitors and immunomodulatory agents to individualize induction treatment recommendations and maintenance
Consolidation and maintenance therapy for transplant eligible myeloma patients
 Consolidation and maintenance therapy for transplant eligible myeloma patients Teeraya Puavilai, M.D. Division of Hematology, Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University
Consolidation and maintenance therapy for transplant eligible myeloma patients Teeraya Puavilai, M.D. Division of Hematology, Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University
Living Well with Myeloma Teleconference Series Thursday, March 24 th :00 PM Pacific/5:00 PM Mountain 6:00 PM Central/7:00 PM Eastern
 Living Well with Myeloma Teleconference Series Thursday, March 24 th 216 4: PM Pacific/5: PM Mountain 6: PM Central/7: PM Eastern Speakers Dr. Brian Durie, IMF Chairman Cedars Sinai Samuel Oschin Cancer
Living Well with Myeloma Teleconference Series Thursday, March 24 th 216 4: PM Pacific/5: PM Mountain 6: PM Central/7: PM Eastern Speakers Dr. Brian Durie, IMF Chairman Cedars Sinai Samuel Oschin Cancer
Progress in Multiple Myeloma
 Progress in Multiple Myeloma Sundar Jagannath, MD Professor, New York Medical College Adjunct Professor, New York University St. Vincent s Comprehensive Cancer Center, NY Faculty Disclosure Advisory Board:
Progress in Multiple Myeloma Sundar Jagannath, MD Professor, New York Medical College Adjunct Professor, New York University St. Vincent s Comprehensive Cancer Center, NY Faculty Disclosure Advisory Board:
Induction Therapy in Transplant Eligible MM 2 December Tontanai Numbenjapon, M.D.
 Induction Therapy in Transplant Eligible MM 2 December 2017 Tontanai Numbenjapon, M.D. What we need from induction therapy in NDMM Depth of response: MRD-negative, scr, CR Longest response Acceptable toxicity
Induction Therapy in Transplant Eligible MM 2 December 2017 Tontanai Numbenjapon, M.D. What we need from induction therapy in NDMM Depth of response: MRD-negative, scr, CR Longest response Acceptable toxicity
Novel Combination Therapies for Untreated Multiple Myeloma
 Novel Combination Therapies for Untreated Multiple Myeloma Andrzej J. Jakubowiak, MD, PhD Director, Myeloma Program New York, NY, October 27, 201 Disclosures 2 Employee Consultant Major Stockholder Speakers
Novel Combination Therapies for Untreated Multiple Myeloma Andrzej J. Jakubowiak, MD, PhD Director, Myeloma Program New York, NY, October 27, 201 Disclosures 2 Employee Consultant Major Stockholder Speakers
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
Highlights from EHA Mieloma Multiplo
 Highlights from EHA Mieloma Multiplo Michele Cavo Istituto di Ematologia L. e A. Seràgnoli Alma Mater Studiorum Università degli studi di Bologna Firenze, 22-23 Settembre 27 Myeloma XI TE pathway 7 R :
Highlights from EHA Mieloma Multiplo Michele Cavo Istituto di Ematologia L. e A. Seràgnoli Alma Mater Studiorum Università degli studi di Bologna Firenze, 22-23 Settembre 27 Myeloma XI TE pathway 7 R :
Managing Newly Diagnosed Multiple Myeloma
 Managing Newly Diagnosed Multiple Myeloma 26 Jan 2018 Alfred Garfall, MD Assistant Professor of Medicine Diagnosis of Multiple Myeloma Traditional criteria: Monoclonal plasma cells + attributable CRAB
Managing Newly Diagnosed Multiple Myeloma 26 Jan 2018 Alfred Garfall, MD Assistant Professor of Medicine Diagnosis of Multiple Myeloma Traditional criteria: Monoclonal plasma cells + attributable CRAB
Treatment Strategies for Transplant-ineligible NDMM Patients
 1 Treatment Strategies for Transplant-ineligible NDMM Patients Thierry Facon, MD Professor of Hematology Service des Maladies du Sang University of Lille Lille, France Multiple Myeloma affects primarily
1 Treatment Strategies for Transplant-ineligible NDMM Patients Thierry Facon, MD Professor of Hematology Service des Maladies du Sang University of Lille Lille, France Multiple Myeloma affects primarily
Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma
 Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma Ravi Vij, MD MBA Professor of Medicine Washington University School of Medicine Section of Stem Cell Transplant
Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma Ravi Vij, MD MBA Professor of Medicine Washington University School of Medicine Section of Stem Cell Transplant
Relapsed Myeloma Sequencing Treatments
 Relapsed Myeloma Sequencing Treatments Noopur Raje, MD Director, Center for Multiple Myeloma MGH Cancer Center Professor of Medicine Harvard Medical School Disclosures Consultant /Advisory Board: Celgene,
Relapsed Myeloma Sequencing Treatments Noopur Raje, MD Director, Center for Multiple Myeloma MGH Cancer Center Professor of Medicine Harvard Medical School Disclosures Consultant /Advisory Board: Celgene,
Consolidation and Maintenance therapy
 University of Salamanca Consolidation and Maintenance therapy María-Victoria Mateos, MD, PhD University Hospital of Salamanca, Spain Disclosure form MVM has served as member of advisory boards or received
University of Salamanca Consolidation and Maintenance therapy María-Victoria Mateos, MD, PhD University Hospital of Salamanca, Spain Disclosure form MVM has served as member of advisory boards or received
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham
 Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
TREATMENT FOR NON-TRANSPLANT ELIGIBLE MULTIPLE MYELOMA
 TREATMENT FOR NON-TRANSPLANT ELIGIBLE MULTIPLE MYELOMA Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang Mai University OUTLINE Overview of treatment
TREATMENT FOR NON-TRANSPLANT ELIGIBLE MULTIPLE MYELOMA Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang Mai University OUTLINE Overview of treatment
Approach to the Treatment of Newly Diagnosed Multiple Myeloma. S. Vincent Rajkumar Professor of Medicine Mayo Clinic
 Approach to the Treatment of Newly Diagnosed Multiple Myeloma S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of
Approach to the Treatment of Newly Diagnosed Multiple Myeloma S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of
Antibodies are a standard part of first relapse management in multiple myeloma (MM): Yes
: Yes") Antibodies are a standard part of first relapse management in multiple myeloma (MM): Yes Ajay Nooka, MD MPH FACP Assistant Professor, Division of Bone Marrow Transplant Winship Cancer Institute, Emory
Antibodies are a standard part of first relapse management in multiple myeloma (MM): Yes Ajay Nooka, MD MPH FACP Assistant Professor, Division of Bone Marrow Transplant Winship Cancer Institute, Emory
Terapia del mieloma. La terapia di prima linea nel paziente giovane. Elena Zamagni
 Terapia del mieloma La terapia di prima linea nel paziente giovane Elena Zamagni Istituto di Ematologia ed Oncologia Medica Seràgnoli Università degli Studi di Bologna Newly diagnosed MM Candidate for
Terapia del mieloma La terapia di prima linea nel paziente giovane Elena Zamagni Istituto di Ematologia ed Oncologia Medica Seràgnoli Università degli Studi di Bologna Newly diagnosed MM Candidate for
Multiple Myeloma: Induction, Consolidation and Maintenance Therapy
 Multiple Myeloma: Induction, Consolidation and Maintenance Therapy James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Establish the Goals of
Multiple Myeloma: Induction, Consolidation and Maintenance Therapy James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Establish the Goals of
Multiple Myeloma: Approach to the Elderly
 Multiple Myeloma: Approach to the Elderly Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON PMH Myeloma Day May 12, 2017 Peter Anglin MD Disclosures Speakers Bureau Advisory Boards
Multiple Myeloma: Approach to the Elderly Peter Anglin MD, FRCPC, MBA Stronach Regional Cancer Centre Newmarket, ON PMH Myeloma Day May 12, 2017 Peter Anglin MD Disclosures Speakers Bureau Advisory Boards
Upfront Therapy for Myeloma Tailoring Therapy across the Disease Spectrum
 Upfront Therapy for Myeloma Tailoring Therapy across the Disease Spectrum S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic
Upfront Therapy for Myeloma Tailoring Therapy across the Disease Spectrum S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic
Treatment of elderly multiple myeloma patients
 SAMO Interdisciplinary Workshop on Myeloma March 30 th -31 st 2012, Seehotel Hermitage, Lucerne Treatment of elderly multiple myeloma patients Federica Cavallo, MD, PhD Federica Cavallo, MD, PhD Division
SAMO Interdisciplinary Workshop on Myeloma March 30 th -31 st 2012, Seehotel Hermitage, Lucerne Treatment of elderly multiple myeloma patients Federica Cavallo, MD, PhD Federica Cavallo, MD, PhD Division
Daratumumab: Mechanism of Action
 Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (D) vs Bortezomib and Dexamethasone () in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio
Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (D) vs Bortezomib and Dexamethasone () in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio
Best of ASH 2017 DR. BRIAN DURIE. Brian GM Durie, MD Thursday, January 11, 2018
 Best of ASH 2017 DR. BRIAN DURIE Brian GM Durie, MD Thursday, January 11, 2018 1 ASH Overview 2017 Total myeloma abstracts: 981 Important/Interesting: oral ~40 posters ~60 100 2 Which abstracts impact
Best of ASH 2017 DR. BRIAN DURIE Brian GM Durie, MD Thursday, January 11, 2018 1 ASH Overview 2017 Total myeloma abstracts: 981 Important/Interesting: oral ~40 posters ~60 100 2 Which abstracts impact
TREATING RELAPSED / REFRACTORY MYELOMA AT THE LEADING EDGE
 TREATING RELAPSED / REFRACTORY MYELOMA AT THE LEADING EDGE PRESENTED BY: Pooja Chaukiyal MD Hematologist/Oncologist New York Oncology Hematology Albany, NY April 16, 2016 Background The prognosis for patients
TREATING RELAPSED / REFRACTORY MYELOMA AT THE LEADING EDGE PRESENTED BY: Pooja Chaukiyal MD Hematologist/Oncologist New York Oncology Hematology Albany, NY April 16, 2016 Background The prognosis for patients
COMy Congress A New Era of Advances in Myeloma. S. Vincent Rajkumar Professor of Medicine Mayo Clinic
 A New Era of Advances in Myeloma S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive
A New Era of Advances in Myeloma S. Vincent Rajkumar Professor of Medicine Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive
Post Transplant Maintenance- for everyone? Disclosures
 Post Transplant Maintenance- for everyone? NO Because of limited survival data, not all patients require maintenance April 2012 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Joseph Mikhael,
Post Transplant Maintenance- for everyone? NO Because of limited survival data, not all patients require maintenance April 2012 Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Joseph Mikhael,
Current management of multiple myeloma. Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School
 Current management of multiple myeloma Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School JorgeJ_Castillo@dfci.harvard.edu Multiple myeloma MM is a plasma cell neoplasm characterized
Current management of multiple myeloma Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School JorgeJ_Castillo@dfci.harvard.edu Multiple myeloma MM is a plasma cell neoplasm characterized
Multiple Myeloma: ASH 2008
 Multiple Myeloma: ASH 2008 Steven Coutre, M.D. Associate Professor of Medicine Division of Hematology Stanford University School of Medicine About These Slides These slides accompany CCO s comprehensive
Multiple Myeloma: ASH 2008 Steven Coutre, M.D. Associate Professor of Medicine Division of Hematology Stanford University School of Medicine About These Slides These slides accompany CCO s comprehensive
Multiple Myeloma Brian Berryman, M.D. March 8 th, 2014
 Multiple Myeloma 2014 Brian Berryman, M.D. March 8 th, 2014 Kyle, R. A. et al. Blood 2008;111:2962-2972 Updates in Multiple Myeloma CCO Independent Conference Coverage of the 2013 Annual Meeting of
Multiple Myeloma 2014 Brian Berryman, M.D. March 8 th, 2014 Kyle, R. A. et al. Blood 2008;111:2962-2972 Updates in Multiple Myeloma CCO Independent Conference Coverage of the 2013 Annual Meeting of
Management of Multiple
 Management of Multiple Myeloma in the Elderly Xavier Leleu Service des Maladies du Sang Hôpital Huriez, CHRU, Lille, France INSERM U837, équipe 3 IRCL, CHRU, Lille, France IMPRT Institut de Médecine Prédictive
Management of Multiple Myeloma in the Elderly Xavier Leleu Service des Maladies du Sang Hôpital Huriez, CHRU, Lille, France INSERM U837, équipe 3 IRCL, CHRU, Lille, France IMPRT Institut de Médecine Prédictive
Continuous Therapy as a Standard of Care CON. JL Harousseau Institut de Cancérologie de l Ouest Nantes Saint Herblain France
 Continuous Therapy as a Standard of Care CON JL Harousseau Institut de Cancérologie de l Ouest Nantes Saint Herblain France 1 In France and in the IFM all debates 2 In France and in the IFM all debates
Continuous Therapy as a Standard of Care CON JL Harousseau Institut de Cancérologie de l Ouest Nantes Saint Herblain France 1 In France and in the IFM all debates 2 In France and in the IFM all debates
Timing of Transplant for Multiple Myeloma
 Timing of Transplant for Multiple Myeloma Wenming CHEN Beijing Chaoyang Hospital Capital Medical University Multiple myeloma resrarch center of Beijing Initial Approach to Treatment of Myeloma Nontransplantation
Timing of Transplant for Multiple Myeloma Wenming CHEN Beijing Chaoyang Hospital Capital Medical University Multiple myeloma resrarch center of Beijing Initial Approach to Treatment of Myeloma Nontransplantation
Role of Maintenance and Consolidation Therapy in Multiple Myeloma: A Patient-centered Approach
 Role of Maintenance and Consolidation Therapy in Multiple Myeloma: A Patient-centered Approach Jacob Laubach, MD Assistant Professor in Medicine Harvard Medical School Clinical Director of the Jerome Lipper
Role of Maintenance and Consolidation Therapy in Multiple Myeloma: A Patient-centered Approach Jacob Laubach, MD Assistant Professor in Medicine Harvard Medical School Clinical Director of the Jerome Lipper
Michel Delforge Belgium. New treatment options for multiple myeloma
 Michel Delforge Belgium New treatment options for multiple myeloma Progress in the treatment of MM over the past 40 years 1962 Prednisone + melphalan 1990s Supportive care 1999 First report on thalidomide
Michel Delforge Belgium New treatment options for multiple myeloma Progress in the treatment of MM over the past 40 years 1962 Prednisone + melphalan 1990s Supportive care 1999 First report on thalidomide
Clinical Case Study Discussion: Maintenance in MM
 www.comtecmed.com/comy comy@comtecmed.com Evangelos Terpos, MD, PhD National & Kapodistrian University of Athens, School of Medicine, Athens, Greece Clinical Case Study Discussion: Maintenance in MM Disclosure
www.comtecmed.com/comy comy@comtecmed.com Evangelos Terpos, MD, PhD National & Kapodistrian University of Athens, School of Medicine, Athens, Greece Clinical Case Study Discussion: Maintenance in MM Disclosure
Novel treatment strategies for multiple myeloma: a focus on oral proteasome inhibitors
 Novel treatment strategies for multiple myeloma: a focus on oral proteasome inhibitors Antonio Palumbo M.D. Takeda Pharmaceuticals International AG Introduction Multiple genetically-distinct subclones
Novel treatment strategies for multiple myeloma: a focus on oral proteasome inhibitors Antonio Palumbo M.D. Takeda Pharmaceuticals International AG Introduction Multiple genetically-distinct subclones
Induction Therapy: Have a Plan. Sagar Lonial, MD Professor, Winship Cancer Institute Director of Translational Research, B-cell Malignancy Program
 Induction Therapy: Have a Plan Sagar Lonial, MD Professor, Winship Cancer Institute Director of Translational Research, B-cell Malignancy Program Topics When to treat? Smoldering vs Symptomatic Risk stratification
Induction Therapy: Have a Plan Sagar Lonial, MD Professor, Winship Cancer Institute Director of Translational Research, B-cell Malignancy Program Topics When to treat? Smoldering vs Symptomatic Risk stratification
Christine Chen Princess Margaret Cancer Centre September 2013
 Christine Chen Princess Margaret Cancer Centre September 2013 Disclosures Research Support Celgene, Janssen, GSK Employee N/A Consultant N/A Major Stockholder Speakers Bureau/ Scientific Advisory Board
Christine Chen Princess Margaret Cancer Centre September 2013 Disclosures Research Support Celgene, Janssen, GSK Employee N/A Consultant N/A Major Stockholder Speakers Bureau/ Scientific Advisory Board
Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions
 Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions Friday, December 8, 2017 Atlanta, Georgia Friday Satellite Symposium preceding the 59th ASH Annual Meeting &
Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions Friday, December 8, 2017 Atlanta, Georgia Friday Satellite Symposium preceding the 59th ASH Annual Meeting &
Updates in Multiple Myeloma: 12 months in 10 minutes
 Updates in Multiple Myeloma: 12 months in 10 minutes Aaron Rosenberg MD, MS Assistant Prof. Medicine UC Davis Comprehensive Cancer Center Division of Hematology and Oncology Outline Standard of care for
Updates in Multiple Myeloma: 12 months in 10 minutes Aaron Rosenberg MD, MS Assistant Prof. Medicine UC Davis Comprehensive Cancer Center Division of Hematology and Oncology Outline Standard of care for
Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions
 Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions Friday, December 8, 2017 Atlanta, Georgia Friday Satellite Symposium preceding the 59th ASH Annual Meeting &
Getting Clear Answers to Complex Treatment Challenges in Multiple Myeloma: Case Discussions Friday, December 8, 2017 Atlanta, Georgia Friday Satellite Symposium preceding the 59th ASH Annual Meeting &
Management of Multiple Myeloma: The Changing Paradigm
 Management of Multiple Myeloma: The Changing Paradigm High-Dose Chemotherapy and Stem Cell Transplantation Todd Zimmerman, MD University of Chicago Medical Center Case Presentation R.M. is a 64 year old
Management of Multiple Myeloma: The Changing Paradigm High-Dose Chemotherapy and Stem Cell Transplantation Todd Zimmerman, MD University of Chicago Medical Center Case Presentation R.M. is a 64 year old
Highlights in multiple myeloma
 3 CONGRESS HIGHLIGHTS Highlights in multiple myeloma P. Vlummens, MD SUMMARY Multiple myeloma (MM) remains a devastating disease, even in the era of novel agents. As such, the search for new treatment
3 CONGRESS HIGHLIGHTS Highlights in multiple myeloma P. Vlummens, MD SUMMARY Multiple myeloma (MM) remains a devastating disease, even in the era of novel agents. As such, the search for new treatment
Treatment Advances in Multiple Myeloma: Expert Perspectives on Translating Clinical Data to Practice
 Treatment Advances in Multiple Myeloma: Expert Perspectives on Translating Clinical Data to Practice Friday, December 2, 2016 San Diego, California This program is supported by educational grants from
Treatment Advances in Multiple Myeloma: Expert Perspectives on Translating Clinical Data to Practice Friday, December 2, 2016 San Diego, California This program is supported by educational grants from
Current Management of Multiple Myeloma. December 2012 Kevin Song MD FRCPC Leukemia/BMT Program of B.C.
 Current Management of Multiple Myeloma December 2012 Kevin Song MD FRCPC Leukemia/BMT Program of B.C. Disclosures Honoraria Speaker Celgene, Janssen, Novartis Celgene, Janssen Research Support Celgene
Current Management of Multiple Myeloma December 2012 Kevin Song MD FRCPC Leukemia/BMT Program of B.C. Disclosures Honoraria Speaker Celgene, Janssen, Novartis Celgene, Janssen Research Support Celgene
UK MRA Myeloma XII Relapsed Intensive Study CI: Prof Gordon Cook
 UK Myeloma Research Alliance Myeloma XII study (ACCoRD): Augmented Conditioning & Consolidation in Relapsed Disease UK MRA Myeloma XII Relapsed Intensive Study CI: Prof Gordon Cook Sponsor ID: Pending
UK Myeloma Research Alliance Myeloma XII study (ACCoRD): Augmented Conditioning & Consolidation in Relapsed Disease UK MRA Myeloma XII Relapsed Intensive Study CI: Prof Gordon Cook Sponsor ID: Pending
Multiple Myeloma: Diagnosis and Primary Treatment
 Multiple Myeloma: Diagnosis and Primary Treatment George Somlo, MD City of Hope Comprehensive Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Educational Objectives Discuss considerations
Multiple Myeloma: Diagnosis and Primary Treatment George Somlo, MD City of Hope Comprehensive Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Educational Objectives Discuss considerations
To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York
 To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York Sundar Jagannath Director, Multiple Myeloma Program Tisch Cancer Institute Mount Sinai Medical Center Maintenance
To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York Sundar Jagannath Director, Multiple Myeloma Program Tisch Cancer Institute Mount Sinai Medical Center Maintenance
Choosing upfront and salvage therapy for myeloma in the ASEAN context
 Choosing upfront and salvage therapy for myeloma in the ASEAN context Daryl Tan Consultant Department of Haematology Singapore General Hospital Adjunct Assistant Professor Duke-NUS Graduate Medical School
Choosing upfront and salvage therapy for myeloma in the ASEAN context Daryl Tan Consultant Department of Haematology Singapore General Hospital Adjunct Assistant Professor Duke-NUS Graduate Medical School
Meu paciente realizou um TACTH na 1a linha, e agora? Tandem, Manutenção, Consolidação? Marcelo C Pasquini, MD, MS Medical College of Wisconsin
 Meu paciente realizou um TACTH na 1a linha, e agora? Tandem, Manutenção, Consolidação? Marcelo C Pasquini, MD, MS Medical College of Wisconsin Post Auto HCT Options for MM Maintenance Lenalidomide vs.
Meu paciente realizou um TACTH na 1a linha, e agora? Tandem, Manutenção, Consolidação? Marcelo C Pasquini, MD, MS Medical College of Wisconsin Post Auto HCT Options for MM Maintenance Lenalidomide vs.
Upcoming Therapies for Myeloma in Alberta. Dr Christopher Venner Cross Cancer Institute
 Upcoming Therapies for Myeloma in Alberta Dr Christopher Venner Cross Cancer Institute Outline Diagnosis Hope for earlier diagnosis Prognosis Update in staging system for modern era highlights clear improvements
Upcoming Therapies for Myeloma in Alberta Dr Christopher Venner Cross Cancer Institute Outline Diagnosis Hope for earlier diagnosis Prognosis Update in staging system for modern era highlights clear improvements
Multiple Myeloma in 2016 Progress and Challenges DONNA E. REECE, M.D. PRINCESS MARGARET CANCER CENTRE 01 APRIL 2016
 Multiple Myeloma in 2016 Progress and Challenges DONNA E. REECE, M.D. PRINCESS MARGARET CANCER CENTRE 01 APRIL 2016 Key Features of Myeloma Biology Myeloma is not one disease 1 At least 7 subtypes based
Multiple Myeloma in 2016 Progress and Challenges DONNA E. REECE, M.D. PRINCESS MARGARET CANCER CENTRE 01 APRIL 2016 Key Features of Myeloma Biology Myeloma is not one disease 1 At least 7 subtypes based
The TOURMALINE-MM1 study: results and expert insights
 The TOURMALINE-MM1 study: results and expert insights Professor Faith Davies UAMS Myeloma Institute, Arkansas, USA This educational meeting was organised and fully funded by Takeda UK Ltd. Takeda medicines
The TOURMALINE-MM1 study: results and expert insights Professor Faith Davies UAMS Myeloma Institute, Arkansas, USA This educational meeting was organised and fully funded by Takeda UK Ltd. Takeda medicines
VI. Autologous stem cell transplantation and maintenance therapy
 Hematological Oncology Hematol Oncol 2013; 31 (Suppl. 1): 42 46 Published online in Wiley Online Library (wileyonlinelibrary.com).2066 Supplement Article VI. Autologous stem cell transplantation and maintenance
Hematological Oncology Hematol Oncol 2013; 31 (Suppl. 1): 42 46 Published online in Wiley Online Library (wileyonlinelibrary.com).2066 Supplement Article VI. Autologous stem cell transplantation and maintenance
MAINTENANCE AND CONTINUOUS THERAPY OF MYELOMA. Myeloma Day 11/18/2017 Aric Hall, MD Assistant Professor UW School of Medicine & Public Health
 MAINTENANCE AND CONTINUOUS THERAPY OF MYELOMA Myeloma Day 11/18/2017 Aric Hall, MD Assistant Professor UW School of Medicine & Public Health Disclosures I have no significant conflicts of interest to disclose.
MAINTENANCE AND CONTINUOUS THERAPY OF MYELOMA Myeloma Day 11/18/2017 Aric Hall, MD Assistant Professor UW School of Medicine & Public Health Disclosures I have no significant conflicts of interest to disclose.
Is Transplant a Necessity or a Choice: Focus on the necessity for CR and MRD
 Is Transplant a Necessity or a Choice: Focus on the necessity for CR and MRD Ajai Chari, MD Associate Professor of Medicine Director of Clinical Research Multiple Myeloma Program Mount Sinai Medical Center
Is Transplant a Necessity or a Choice: Focus on the necessity for CR and MRD Ajai Chari, MD Associate Professor of Medicine Director of Clinical Research Multiple Myeloma Program Mount Sinai Medical Center
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Making Sense of Myeloma Treatment Advances
 Making Sense of Myeloma Treatment Advances Webinar 1, May 17, 217 Updates From the 16th International Myeloma Workshop and the American Association for Cancer Research 217 Annual Meeting Speakers Moderator:
Making Sense of Myeloma Treatment Advances Webinar 1, May 17, 217 Updates From the 16th International Myeloma Workshop and the American Association for Cancer Research 217 Annual Meeting Speakers Moderator:
Il trattamento del Mieloma su stratificazione di rischio: è oggi possibile?
 Il trattamento del Mieloma su stratificazione di rischio: è oggi possibile? Francesca Gay, MD Divisione Ematologia 1 AO Città della Salute e della Scienza, Torino, Italy Focus sul MM 2014 Cagliari, 30-31
Il trattamento del Mieloma su stratificazione di rischio: è oggi possibile? Francesca Gay, MD Divisione Ematologia 1 AO Città della Salute e della Scienza, Torino, Italy Focus sul MM 2014 Cagliari, 30-31
Daratumumab: Mechanism of Action
 An Open-label, Randomised, Phase 3 Study of Daratumumab, Lenalidomide, and Dexamethasone (D) Versus Lenalidomide and Dexamethasone () in Relapsed or Refractory Multiple Myeloma (RRMM): POLLUX* Meletios
An Open-label, Randomised, Phase 3 Study of Daratumumab, Lenalidomide, and Dexamethasone (D) Versus Lenalidomide and Dexamethasone () in Relapsed or Refractory Multiple Myeloma (RRMM): POLLUX* Meletios
Methods: Studies included in the analysis
 Efficacy and safety of long-term ixazomib maintenance therapy in patients with newly diagnosed multiple myeloma not undergoing transplant: An integrated analysis of four phase 1/2 studies Meletios A. Dimopoulos,
Efficacy and safety of long-term ixazomib maintenance therapy in patients with newly diagnosed multiple myeloma not undergoing transplant: An integrated analysis of four phase 1/2 studies Meletios A. Dimopoulos,
ClinicalTrials.gov Identifier: NCT
 Efficacy of Daratumumab, Lenalidomide, and Dexamethasone Versus Lenalidomide and Dexamethasone Alone for Relapsed or Refractory Multiple Myeloma Among Patients With to 3 Prior Lines of Therapy Based on
Efficacy of Daratumumab, Lenalidomide, and Dexamethasone Versus Lenalidomide and Dexamethasone Alone for Relapsed or Refractory Multiple Myeloma Among Patients With to 3 Prior Lines of Therapy Based on
Autologous Stem Cell Transplantation in Multiple Myeloma Optimal Frontline Therapy and Maintenance Therapy
 Autologous Stem Cell Transplantation in Multiple Myeloma Optimal Frontline Therapy and Maintenance Therapy Donna E. Reece, M.D. Princess Margaret Hospital Toronto, ON CANADA 10 December 2011 ASCT in Myeloma..
Autologous Stem Cell Transplantation in Multiple Myeloma Optimal Frontline Therapy and Maintenance Therapy Donna E. Reece, M.D. Princess Margaret Hospital Toronto, ON CANADA 10 December 2011 ASCT in Myeloma..
New Treatment Paradigms in Transplant-Eligible Myeloma Patients
 New Treatment Paradigms in Transplant-Eligible Myeloma Patients Michele Cavo Seràgnoli Institute of Hematology, Bologna University School of Medicine, Italy Turkey, March 1 st 2013 NEW TREATMENT PARADıGM
New Treatment Paradigms in Transplant-Eligible Myeloma Patients Michele Cavo Seràgnoli Institute of Hematology, Bologna University School of Medicine, Italy Turkey, March 1 st 2013 NEW TREATMENT PARADıGM
Risk stratification in the older patient; what are our priorities?
 Risk stratification in the older patient; what are our priorities? Sonja Zweegman MD PhD Amsterdam The Netherlands Negative impact of age on survival Meta-analysis of European trials (MP vs MPT, VMP vs
Risk stratification in the older patient; what are our priorities? Sonja Zweegman MD PhD Amsterdam The Netherlands Negative impact of age on survival Meta-analysis of European trials (MP vs MPT, VMP vs
Treatment of elderly patients with multiple myeloma
 Treatment of elderly patients with multiple myeloma Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY Improved survival in multiple myeloma and the impact
Treatment of elderly patients with multiple myeloma Mario Boccadoro DIVISIONE UNIVERSITARIA DI EMATOLOGIA AZIENDA OSPEDALIERA SAN GIOVANNI TORINO, ITALY Improved survival in multiple myeloma and the impact
Experience with bortezomib (Velcade) in multiple myeloma. Peter Černelč Clinical center Ljubljana Department of Haematology
 in multiple myeloma. Peter Černelč Clinical center Ljubljana Department of Haematology") Experience with bortezomib (Velcade) in multiple myeloma Peter Černelč Clinical center Ljubljana Department of Haematology Our experience with bortezomib (Velcade) in multiple myeloma 1. Our first experience
Experience with bortezomib (Velcade) in multiple myeloma Peter Černelč Clinical center Ljubljana Department of Haematology Our experience with bortezomib (Velcade) in multiple myeloma 1. Our first experience
Multiple Myeloma What is New? Can we talk cure? Rafat Abonour, M.D.
 Multiple Myeloma What is New? Can we talk cure? Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm Nearly 24, new cases diagnosed in the US per year and 11, worldwide
Multiple Myeloma What is New? Can we talk cure? Rafat Abonour, M.D. Multiple Myeloma Facts Second most prevalent hematologic neoplasm Nearly 24, new cases diagnosed in the US per year and 11, worldwide
MULTIDISCIPLINARY MULTIPLE MYELOMA CARE
 MULTIDISCIPLINARY MULTIPLE MYELOMA CARE Regional Lecture Series Leveraging a Multidisciplinary Approach to Multiple Myeloma Care Leveraging a Multidisciplinary Approach to Multiple Myeloma Care Abhinav
MULTIDISCIPLINARY MULTIPLE MYELOMA CARE Regional Lecture Series Leveraging a Multidisciplinary Approach to Multiple Myeloma Care Leveraging a Multidisciplinary Approach to Multiple Myeloma Care Abhinav
Proteasome inhibitor (PI) and immunomodulatory drug (IMiD) refractory multiple myeloma is associated with inferior patient outcomes
 and immunomodulatory drug (IMiD) refractory multiple myeloma is associated with inferior patient outcomes") Alliance A061202. A phase I/II study of pomalidomide, dexamethasone and ixazomib versus pomalidomide and dexamethasone for patients with multiple myeloma refractory to lenalidomide and proteasome inhibitor
Alliance A061202. A phase I/II study of pomalidomide, dexamethasone and ixazomib versus pomalidomide and dexamethasone for patients with multiple myeloma refractory to lenalidomide and proteasome inhibitor
Therapie des Multiplen Myeloms Alles im Fluss? Peter Neumeister, MD Division Hematology Medical University Graz
 Therapie des Multiplen Myeloms Alles im Fluss? Peter Neumeister, MD Division Hematology Medical University Graz 15.6.218 Newly Diagnosed Multiple Myeloma Transplant Eligible NDMM TE VCD is preferable to
Therapie des Multiplen Myeloms Alles im Fluss? Peter Neumeister, MD Division Hematology Medical University Graz 15.6.218 Newly Diagnosed Multiple Myeloma Transplant Eligible NDMM TE VCD is preferable to
Managing Myeloma Virtual Grand Rounds Newly Diagnosed, Transplant Eligible Patient. Case Study
 Managing Myeloma Virtual Grand Rounds Newly Diagnosed, Transplant Eligible Patient Case Study 2 2011 Newly Diagnosed Patient The patient is a 61-year-old Caucasian female History of high blood pressure
Managing Myeloma Virtual Grand Rounds Newly Diagnosed, Transplant Eligible Patient Case Study 2 2011 Newly Diagnosed Patient The patient is a 61-year-old Caucasian female History of high blood pressure
Novel Therapies for the Treatment of Newly Diagnosed Multiple Myeloma
 Novel Therapies for the Treatment of Newly Diagnosed Shaji K. Kumar, MD Professor of Medicine Mayo Clinic College of Medicine Consultant, Division of Hematology Medical Director, Cancer Clinical Research
Novel Therapies for the Treatment of Newly Diagnosed Shaji K. Kumar, MD Professor of Medicine Mayo Clinic College of Medicine Consultant, Division of Hematology Medical Director, Cancer Clinical Research
Stato dell arte: dalle opzioni terapeutiche alla strategia terapeutica nel 2017
 Stato dell arte: dalle opzioni terapeutiche alla strategia terapeutica nel 2017 Elena Zamagni Istituto di Ematologia Seragnoli Università di Bologna Eligibility for ASCT Yes Induction: 3-drug regimens
Stato dell arte: dalle opzioni terapeutiche alla strategia terapeutica nel 2017 Elena Zamagni Istituto di Ematologia Seragnoli Università di Bologna Eligibility for ASCT Yes Induction: 3-drug regimens
DARA Monotherapy Studies
 Usmani, SZ. Blood. 26. http://dx.doi.org/.82/blood-26-3-752. Lokhorst HM, et al. N Engl J Med. 25;373(3):27-29. Lonial S, et al. Lancet. 25. I DARA Monotherapy Studies Baseline Characteristics Median (range)
Usmani, SZ. Blood. 26. http://dx.doi.org/.82/blood-26-3-752. Lokhorst HM, et al. N Engl J Med. 25;373(3):27-29. Lonial S, et al. Lancet. 25. I DARA Monotherapy Studies Baseline Characteristics Median (range)
Disclosures. Consultancy, Research Funding and Speakers Bureau: Celgene Corporation, Millennium, Onyx, Cephalon
 Pomalidomide With or Without Low-dose Dexamethasone in Patients With Relapsed/Refractory Multiple Myeloma: Outcomes in Patients Refractory to Lenalidomide and Bortezomib Ravi Vij 1, Paul G. Richardson
Pomalidomide With or Without Low-dose Dexamethasone in Patients With Relapsed/Refractory Multiple Myeloma: Outcomes in Patients Refractory to Lenalidomide and Bortezomib Ravi Vij 1, Paul G. Richardson
H. Lee Moffitt Cancer Center and Research Institute, University of California, San Francisco & Tisch Cancer Institute, Mount Sinai School of Medicine
 Pomalidomide, Cyclophosphamide, and Dexamethasone Is Superior to Pomalidomide and Dexamethasone in Relapsed and Refractory Myeloma: Results of a Multicenter Randomized Phase II Study Rachid Baz, Thomas
Pomalidomide, Cyclophosphamide, and Dexamethasone Is Superior to Pomalidomide and Dexamethasone in Relapsed and Refractory Myeloma: Results of a Multicenter Randomized Phase II Study Rachid Baz, Thomas
Multiple Myeloma. Dr. Janet MacEachern BA, MD, FRCP(C) Grand River Regional Cancer Center Kitchener, Ontario
 Grand River Regional Cancer Center Kitchener, Ontario") Multiple Myeloma Dr. Janet MacEachern BA, MD, FRCP(C) Grand River Regional Cancer Center Kitchener, Ontario Disclosures Relationships with financial sponsors: Grants/Research Support: n/a Speakers Bureau/Honoraria:
Multiple Myeloma Dr. Janet MacEachern BA, MD, FRCP(C) Grand River Regional Cancer Center Kitchener, Ontario Disclosures Relationships with financial sponsors: Grants/Research Support: n/a Speakers Bureau/Honoraria:
Managing Major Adverse Events in Relapsed/Refractory Multiple Myeloma
 Welcome to Managing Myeloma. I am Dr. Ajay Nooka. In today's presentation, I will discuss managing major adverse events in relapsed/refractory multiple myeloma. In this video, I will provide you with information
Welcome to Managing Myeloma. I am Dr. Ajay Nooka. In today's presentation, I will discuss managing major adverse events in relapsed/refractory multiple myeloma. In this video, I will provide you with information
ClinicalTrials.gov Identifier: NCT
 Efficacy of Daratumumab, Bortezomib, and Dexamethasone Versus Bortezomib and Dexamethasone in Relapsed or Refractory Multiple Myeloma Based on Prior Lines of Therapy: Updated Analysis of CASTOR Maria-Victoria
Efficacy of Daratumumab, Bortezomib, and Dexamethasone Versus Bortezomib and Dexamethasone in Relapsed or Refractory Multiple Myeloma Based on Prior Lines of Therapy: Updated Analysis of CASTOR Maria-Victoria
Advances in the Management of Myeloma Parameswaran Hari, MD
 Advances in the Management of Myeloma Parameswaran Hari, MD Medical College of Wisconsin Milwaukee, WI What is the standard? Induction/Transplant/Maintenance UPDATED OS DATA from CALGB 100104 & IFM 2005-02
Advances in the Management of Myeloma Parameswaran Hari, MD Medical College of Wisconsin Milwaukee, WI What is the standard? Induction/Transplant/Maintenance UPDATED OS DATA from CALGB 100104 & IFM 2005-02
Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto)
 and Dr. Matt Cheung (Staff Hematologist, University of Toronto)") MULTIPLE MYELOMA Updated March 2017 by Doreen Ezeife, PGY-5 resident, University of Calgary Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist,
MULTIPLE MYELOMA Updated March 2017 by Doreen Ezeife, PGY-5 resident, University of Calgary Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist,
Multiple myeloma. November 24, 2017 at Vientiane, Laos
 Multiple myeloma November 24, 2017 at Vientiane, Laos Teeraya Puavilai, M.D. Division of Hematology, Department of Medicine Faculty of Medicine Ramathibodi, Mahidol University, Thailand Multiple myeloma
Multiple myeloma November 24, 2017 at Vientiane, Laos Teeraya Puavilai, M.D. Division of Hematology, Department of Medicine Faculty of Medicine Ramathibodi, Mahidol University, Thailand Multiple myeloma
Daratumumab: Mechanism of Action
 Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (DVd) vs Bortezomib and Dexamethasone (Vd) in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio
Phase 3 Randomized Controlled Study of Daratumumab, Bortezomib and Dexamethasone (DVd) vs Bortezomib and Dexamethasone (Vd) in Patients with Relapsed or Refractory Multiple Myeloma (RRMM): CASTOR* Antonio