Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto
|
|
|
- Merilyn Terry
- 5 years ago
- Views:
Transcription




1 Wharton Head and Neck Centre The Toronto General Hospital Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto Controversies in The Management of Head and Neck and Thyroid Cancer Royal College of Physicians London, December 5-6, 2013
2 Evolution of Organ Preservation Strategies 1960 s Laryngectomy/Pharyngectomy 1970 s Laryngectomy alone Planned radiation with surgery for salvage 1980 s Irradiation +/- Chemotherapy (5FU, Mitomycin C) 1990 s VA Trial, (Neoadjuvant Chemo/Rad or Laryngectomy) 2000 s Adoption of Organ Preservation Approaches s 100% TL Functional Larynx? 40% TL Quality of Life? I have seen the future and it doesn t work. Robert Fulford
3 Cancer of the Larynx- We have seen the future and yes some works. Lets explore in our Tumour Board.
4 Purpose of the Case Presentation Review the Management of early and late Complex laryngeal cases with a focus on Principles of Management How to minimise complications Management of recurrence and review Reconstructive Options when salvage Surgery needed in the chemoradiated patient.

5 Case #1 55 year old truck driver presents with an 8 month history of hoarseness 40 pack year smoker No comorbidity Biopsy- Microinvasive SCC
6 Questions Would you do any further investigations? What would be your primary treatment approach? If TOL what are your limitations for this approach? How do you inform patients regarding treatment options? If primary radiotherapy what volume and technique?

7 Case # 2.Does gender influence how you manage?? 36 year old female presents with longstanding history of hoarseness 10 pack year history of smoking No Comorbidity Examination Altered mobility
8 Treatment options for bulky T2? If non-surgical approach which approach? Altered Fractionation alone ChemoRT Induction followed by RT or Surgery What would you estimate the probability of local control? Do women have a better outcome-harwood et al PMH?
9 Case # 3 81 yo male with 6 mo h/o hoarseness, progressively worsening PMH: htn, gerd, asthma, prostate ca (primary RT) PSH: herniorrhaphy, appendectomy SH: worked in GM plant, quit tobacco 50yrs prior PE: ulceration left TVC extending into ventricle, normal mobility T2


10 Does age influence how you would treat him T2

11 Case # 4-Advanced Glottic Cancer 72 year old male presents with progressive hoarseness, odynophagia Diabetic Mild Emphysema CAD with stent 1yr ago 50pk year smoker Exam-fixed cord


12
13 Questions What other investigations would you consider? What are the Current Organ Preservation Options? What Approach would you chose? Surgical Issues Primary Surgery Primary TEP (Y/N) Does he need a flap to bolster repair?

14 Case #5 T2NOMO 38 yo male, healthy mechanic, with 3 yr h/o intermittent hoarseness, with progressive changes over last 6 months PMH: htn, hypercholesterolemia PSH: knee surgery Meds: ramipril, HCTZ, losec SH: 20pk yrs, moderate ETOH Tx-RTOG bid protocol 66 Gy in 6/52 using in 35 fractions.

15 Tx-RTOG bid protocol 66 Gy in 6/52
16 One Year later following treatment with RTOG bid protocol 66 Gy in 6/52 Now c/olaryngeal Perichondritis- Management

17 1.Antibotics 2.Steroids. 3. Role of hyperbaric O2 4.How do you exclude residual cancer? 5.When do you resort to surgery? 6.Do you use a flap to bolster the repair,if so describe.
18 Don t close your pharynx too tightly. Liberal use of patch flaps. Savary fistula tube if repair is circumferential If dysphagia occurs how do you treat Expectant-PPIs Serial dilatations. Any Role for myotomy Botulinum toxin-how often to inject When do you stent? If so what type
19 Case #6 T2N0M0 Cancer of R.Hypopharynx 62 yr old female with 3month history of sore throat, some slight dysphagia diagnosed with ulcerative lesion R piriform sinus.cord mobile.no cervical adenopathy. Metastatic Survey clear. Biopsy- Sq.cell cancer-mod. Differentiated Patient co-morbidities - hypertension.type II Diabetes. Management options-


20 T2NOMO-What to do? Management options
21 What are the Options to treat? Management options- Radiation alone,concurrent chemo/rads. Primary surgery-partial pharyngectomy with flap repair.
22 Treatment Early (T1, T2) carcinoma - Piriform sinus - Posterior pharyngeal wall Laser excision/robotic excision ± neck dissection Partial pharyngectomy + neck (II, III, IV) - Trans hyoid or - Lateral pharyngectomy approach Radiation or Chemoradiation Overall 3 yrs. 70%





23 T4a Management Options?



24 Surgery

25

26 Salvage Surgery You choose a non surgical approach patient returns 6 months after chemort with recurrent disease
27 Should we consider salvage for failure of organ preservation approaches? Goodwin, J: Laryngoscope, 2000
28 Primary Surgery or Concurrent Chemo/radiation What Investigations? What Operation? Extent of Neck Dissection? Primary TEP? Flap reconstruction; What and How?

29 What is Wrong with Chemotherapy Based Organ Preservation Strategies? As well as synergistic tumor effects, we are seeing increasing early and late toxicity. Rates of treatment related deaths are higher particularly patients with pre-treatment co-morbidity. (diabetes, vascular disease, immunosuppressive therapy) Pharyngeal dysfunction and stenosis is a major problem- up to 30% of patients remain G-tube dependant 6-9 months after therapy. ARE WE PRESERVING A NON-FUNCTIONAL STRUCTURE?
30 Quality of Life Outcomes in Organ Preservation RFP Recently Circulated by NCI reflects NCI s recognition of the critical importance. of the impact of cancer and its treatment on individuals living years beyond a cancer diagnosis Cognitive deficits Memory loss Other malignancies


31 Salvage Surgery Following Irradiation ± Chemotherapy Problems - Extent of recurrence - neck only - neck & primary - Hostile wound - High fistula rate - Need for flap repair
32 Grau C. Salvage laryngectomy & pharyngocutaneous fistulae after primary radiotherapy for head and neck cancer: a national survey from DAHANCA. Head & Neck. 25(9):711-6, 2003 Fistula Rate 9% to 57% Parikh, Gullane 1998

33 Reconstructive Options Following Salvage Laryngopharyngectomy 2010 Pectoralis Major Pedicled Flap Radial Forearm Flap Free Jejunal Graft Anterolateral Thigh Flap Gastro-omental Flap Gastric Transposition How do we decide?

34 When should we use a Pedicled Pectoralis Major Flap? minimum of 1.5cm residual pharyngeal mucosa In Repair of partial Pharyngeal defects


35 Radial Forearm Flap Savary Fistula tube vital

 Most commonly used flap in our centre")
36 When should we use a Anterolateral Thigh Flap? Stricture rate No stent 33% Stent < 10% (p=0.571) Most commonly used flap in our centre for repair of total circumferential defects.



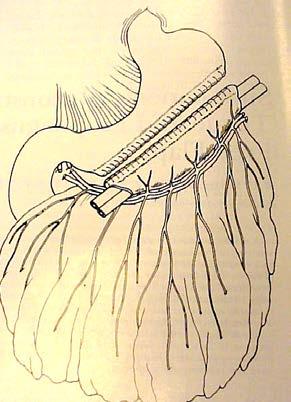

37 Gastro-Omental Flap In salvage pharyngectomy following organ preservation therapy in good performance patients.



38 Summary Advantages Free Gastro-Omental Transfer One Stage, Low Morbidity Unlimited tube diameter, Swallowing Speech Harvest with Omentum Disadvantages abdominal harvest, mucoid secretions *Patel R, Makitie A, Goldstein D, Gullane P, Brown D, Irish J, Gilbert R: Morbidity and Functional Outcomes Following Gastro-Omental Free Flap Reconstruction of Circumferential Pharyngeal Defects. Head and Neck Journal, ; May 2009
39 Options in Pharyngeal Reconstruction 2013 Flap - Speech Morbidity Gastric Pullup Forearm + Stent Free Gastro- Omental Free Jejunum Anterolateral Thigh +Stent IMAP Flap It s role to be evaluated
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma
 Original Article Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma Guo-Hua Hu, Shi-Xun Zhong, Qing Xiao, 1 Yi Qian,
Original Article Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma Guo-Hua Hu, Shi-Xun Zhong, Qing Xiao, 1 Yi Qian,
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Management of complications after laryngopharyngectomy
 Management of complications after laryngopharyngectomy Dr Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), DLO, DOHNS, FRCS (ORL-HNS), FAMS Consultant ENT / Head and Neck Surgeon Tan Tock Seng Hospital
Management of complications after laryngopharyngectomy Dr Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), DLO, DOHNS, FRCS (ORL-HNS), FAMS Consultant ENT / Head and Neck Surgeon Tan Tock Seng Hospital
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Salvage Laryngectomy. after R T Failure Indications, Complications and Results. Aug
 Salvage Laryngectomy after R T Failure Indications, Complications and Results Aug.3.2013 Acknowledgments I am grateful to the following individuals who have allowed me to use their slides during this presentation:
Salvage Laryngectomy after R T Failure Indications, Complications and Results Aug.3.2013 Acknowledgments I am grateful to the following individuals who have allowed me to use their slides during this presentation:
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Chapter 117: Reconstruction of the Hypopharynx and Cervical Esophagus. Richard E. Hayden
 Chapter 117: Reconstruction of the Hypopharynx and Cervical Esophagus Richard E. Hayden In 1877 Czerny performed the first recorded pharyngoesophageal reconstruction, using local cervical skin flaps for
Chapter 117: Reconstruction of the Hypopharynx and Cervical Esophagus Richard E. Hayden In 1877 Czerny performed the first recorded pharyngoesophageal reconstruction, using local cervical skin flaps for
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Swallowing after a Total Laryngectomy
 Swallowing after a Total Laryngectomy Diane Longnecker, M.S.,CCC-SLP, BCS-S Baylor Institute for Rehabilitation at Baylor University Medical Center Dallas, TX Disclosure Statement No relevant financial
Swallowing after a Total Laryngectomy Diane Longnecker, M.S.,CCC-SLP, BCS-S Baylor Institute for Rehabilitation at Baylor University Medical Center Dallas, TX Disclosure Statement No relevant financial
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Salvage Circular Laryngopharyngectomy and Radial Forearm Free Flap for Recurrent Hypopharyngeal Cancer
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Salvage Circular Laryngopharyngectomy and Radial Forearm Free Flap for Recurrent Hypopharyngeal Cancer Nicolas
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Salvage Circular Laryngopharyngectomy and Radial Forearm Free Flap for Recurrent Hypopharyngeal Cancer Nicolas
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Title. CitationInternational Journal of Clinical Oncology, 20(6): 1. Issue Date Doc URL. Rights. Type. File Information
: 1. Issue Date Doc URL. Rights. Type. File Information") Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
PRINCIPLES OF RADIATION ONCOLOGY
 PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
ORIGINAL ARTICLE. The Thoracoacromial/Cephalic Vascular System for Microvascular Anastomoses in the Vessel-Depleted Neck
 ORIGINAL ARTICLE The Thoracoacromial/Cephalic Vascular System for Microvascular Anastomoses in the Vessel-Depleted Neck Jeffrey R. Harris, MD; E. Lueg, MD; E. Genden, MD; M. L. Urken, MD Objective: To
ORIGINAL ARTICLE The Thoracoacromial/Cephalic Vascular System for Microvascular Anastomoses in the Vessel-Depleted Neck Jeffrey R. Harris, MD; E. Lueg, MD; E. Genden, MD; M. L. Urken, MD Objective: To
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES HEAD AND NECK HYPOPHARYNX Head & Neck Site Group Hypopharynx 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND EARLY DETECTION 3 4. DIAGNOSIS
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Information and support
 13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer
 Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer Angela Campanelli, MS, CCC SLP Board Certified Specialist in Swallowing and Swallowing Disorders
Swallow Study and the Laryngectomy Patient Long Term Dysphagia after Treatment for Head and Neck Cancer Angela Campanelli, MS, CCC SLP Board Certified Specialist in Swallowing and Swallowing Disorders
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA
 LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA * E.D. KITCHER, J. YARNEY 1, R.K. GYASI 2 AND C. CHEYUO Departments of Surgery and 2 Pathology, University of Ghana Medical School, P O Box
LARYNGEAL CANCER AT THE KORLE BU TEACHING HOSPITAL ACCRA GHANA * E.D. KITCHER, J. YARNEY 1, R.K. GYASI 2 AND C. CHEYUO Departments of Surgery and 2 Pathology, University of Ghana Medical School, P O Box
Learning Objectives. Head and Neck Cancer: Post-Treatment Changes. Neck Dissection Classification * Radical neck dissection. Radical Neck Dissection
 Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Clinical Case Presentation. Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006
 Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Piero Nicolai SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART. Department of Otorhinolaryngology University of Brescia
 Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Accepted 5 September 2008 Published online in 3 March 2009 Wiley InterScience ( DOI: /hed.21016
 ORIGINAL ARTICLE MORBIDITY AND FUNCTIONAL OUTCOMES FOLLOWING GASTRO-OMENTAL FREE FLAP RECONSTRUCTION OF CIRCUMFERENTIAL PHARYNGEAL DEFECTS Rajan S. Patel, MBChB, MD, FRCS (ORL-HNS), Antti A. Makitie, MD,
ORIGINAL ARTICLE MORBIDITY AND FUNCTIONAL OUTCOMES FOLLOWING GASTRO-OMENTAL FREE FLAP RECONSTRUCTION OF CIRCUMFERENTIAL PHARYNGEAL DEFECTS Rajan S. Patel, MBChB, MD, FRCS (ORL-HNS), Antti A. Makitie, MD,
The Role of Docetaxel in the Treatment of Head and Neck Cancer
 GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
Division of Reconstructive Surgery, Head and Neck Institute, Amrita Institute of Medical Siences, Kochi , Kerala, India
 Free full text on www.ijps.org Reconstruction of the laryngopharynx Daxesh Patel, Moni Abraham Kuriakose, Subramania Iyer Division of Reconstructive Surgery, Head and Neck Institute, Amrita Institute of
Free full text on www.ijps.org Reconstruction of the laryngopharynx Daxesh Patel, Moni Abraham Kuriakose, Subramania Iyer Division of Reconstructive Surgery, Head and Neck Institute, Amrita Institute of
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Research Article Predictors of Salivary Fistulas in Patients Undergoing Salvage Total Laryngectomy
 International Scholarly Research Notices, Article ID 373825, 6 pages http://dx.doi.org/10.1155/2014/373825 Research Article Predictors of Salivary Fistulas in Patients Undergoing Salvage Total Laryngectomy
International Scholarly Research Notices, Article ID 373825, 6 pages http://dx.doi.org/10.1155/2014/373825 Research Article Predictors of Salivary Fistulas in Patients Undergoing Salvage Total Laryngectomy
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY
 CLINICAL REVIEW David W. Eisele, MD, Section Editor CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY Robert P. Takes, MD, PhD, 1 Primož Strojan, MD, PhD,
CLINICAL REVIEW David W. Eisele, MD, Section Editor CURRENT TRENDS IN INITIAL MANAGEMENT OF HYPOPHARYNGEAL CANCER: THE DECLINING USE OF OPEN SURGERY Robert P. Takes, MD, PhD, 1 Primož Strojan, MD, PhD,
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
The influence of closure technique in total laryngectomy on the development of a pseudo-diverticulum and dysphagia
 Eur Arch Otorhinolaryngol (2017) 274:1967 1973 DOI 10.1007/s00405-016-4424-4 HEAD AND NECK The influence of closure technique in total laryngectomy on the development of a pseudo-diverticulum and dysphagia
Eur Arch Otorhinolaryngol (2017) 274:1967 1973 DOI 10.1007/s00405-016-4424-4 HEAD AND NECK The influence of closure technique in total laryngectomy on the development of a pseudo-diverticulum and dysphagia
Case Presentation. Faysal Ghazzay Ahmed
 Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Faysal Ghazzay Ahmed Case Presentation He is 49 years old male living in Al-Qaem Town (Al-Anbar Gov.), Muslim, and was previously serving in the army, but now he is idle. He was admitted to Al-Jumhoory
Pharyngoesophageal Strictures in Head and Neck Cancer
 Pharyngoesophageal Strictures in Head and Neck Cancer Barbara P. Messing, M.A., CCC-SLP, BRS-S, S, John Saunders, M.D., Patrick K. Ha, M.D., Marshall Levine, M.D., Ray Blanco, M.D., Eva Zinreich, M.D.,
Pharyngoesophageal Strictures in Head and Neck Cancer Barbara P. Messing, M.A., CCC-SLP, BRS-S, S, John Saunders, M.D., Patrick K. Ha, M.D., Marshall Levine, M.D., Ray Blanco, M.D., Eva Zinreich, M.D.,
Long Term Toxicities of Head & Neck Cancer Therapies. Faith Mutale Abramson Cancer Center University of Pennsylvania
 Long Term Toxicities of Head & Neck Cancer Therapies Faith Mutale Abramson Cancer Center University of Pennsylvania Head & Neck Cancer 2-3% of all cancers 1-2% of all cancer deaths Incidence includes:
Long Term Toxicities of Head & Neck Cancer Therapies Faith Mutale Abramson Cancer Center University of Pennsylvania Head & Neck Cancer 2-3% of all cancers 1-2% of all cancer deaths Incidence includes:
Pharyngoesophageal reconstruction after resection of hypopharyngeal carcinoma: a new algorithm after analysis of 142 cases
 Denewer et al. World Journal of Surgical Oncology 2014, 12:182 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Pharyngoesophageal reconstruction after resection of hypopharyngeal carcinoma: a new
Denewer et al. World Journal of Surgical Oncology 2014, 12:182 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Pharyngoesophageal reconstruction after resection of hypopharyngeal carcinoma: a new
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Learning objectives Describe anatomically and clinically the di ifference between laryngeal cancer and hypopharyngeal cancer Be able to describe clini
 Laryngeal cancer Hanwei PENG, MD, PhD Thyroid Surgery Research Center, SU UMC Head and Neck Department, Cancer Hospital, SUMC Learning objectives Describe anatomically and clinically the di ifference between
Laryngeal cancer Hanwei PENG, MD, PhD Thyroid Surgery Research Center, SU UMC Head and Neck Department, Cancer Hospital, SUMC Learning objectives Describe anatomically and clinically the di ifference between
FRCS Otolarynoglogy VIVA Course Dundee Guidelines. Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool
 FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION
 THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
Chondroradionecrosis of the Larynx: Diagnostic and Therapeutic Measures for Saving the Organ from Radiotherapy Sequelae
 Clinical and Experimental Otorhinolaryngology Vol. 2, No. 3: 115-119, September 2009 DOI 10.3342/ceo.2009.2.3.115 Original Article Chondroradionecrosis of the Larynx: Diagnostic and Therapeutic Measures
Clinical and Experimental Otorhinolaryngology Vol. 2, No. 3: 115-119, September 2009 DOI 10.3342/ceo.2009.2.3.115 Original Article Chondroradionecrosis of the Larynx: Diagnostic and Therapeutic Measures
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer
 Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
Neck Imaging Reporting and Data System: An Atlas of NI-RADS Categories for Head and Neck Cancer Bethany Cavazuti Patricia Hudgins Tanya Rath Char Branstetter Kristen Baugnon Amanda Corey Ashley Aiken Disclosures
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Case Number: RT (M) Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor
 Potential Audiences: Intent Doctor, Oncology Special Nurse, Resident Doctor") Squamous Cell Carcinoma with Isolated Upper Mediastinum Nodal Metastasis with Unknown Primary: the Role and Treatment Consideration of RT with Chemotherapy Case Number: RT2009-82(M) Potential Audiences:
Squamous Cell Carcinoma with Isolated Upper Mediastinum Nodal Metastasis with Unknown Primary: the Role and Treatment Consideration of RT with Chemotherapy Case Number: RT2009-82(M) Potential Audiences:
Introduction/Learning Objectives. Incontinence: Natural History. Course Outline 10/14/2016. Urinary Incontinence: Conservative Measures
 Management of Urinary Complications after Prostatectomy Course Faculty: Introduction/Learning Objectives Jaspreet S. Sandhu, MD Associate Attending Urologist Department of Surgery/Urology Memorial Sloan
Management of Urinary Complications after Prostatectomy Course Faculty: Introduction/Learning Objectives Jaspreet S. Sandhu, MD Associate Attending Urologist Department of Surgery/Urology Memorial Sloan
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Surgical treatment of hypopharyngeal cancer
 BEHBUT CEVANŞİR KULAK BURUN BOĞAZ HASTALIKLARI VE BAŞ BOYUN CERRAHİSİ DERNEĞİ Tr-ENT 2018;28(3):105-111 Original Article 105 Surgical treatment of hypopharyngeal cancer Selçuk Güneş 1, Bora Başaran 2,
BEHBUT CEVANŞİR KULAK BURUN BOĞAZ HASTALIKLARI VE BAŞ BOYUN CERRAHİSİ DERNEĞİ Tr-ENT 2018;28(3):105-111 Original Article 105 Surgical treatment of hypopharyngeal cancer Selçuk Güneş 1, Bora Başaran 2,
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Hoarseness. Evidence-based Key points for Approach
 Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Free posterior tibial flap reconstruction for hypopharyngeal squamous cell carcinoma
 Chen et al. World Journal of Surgical Oncology 2014, 12:163 WORLD JOURNAL OF SURGICAL ONCOLOGY CASE REPORT Open Access Free posterior tibial flap reconstruction for hypopharyngeal squamous cell carcinoma
Chen et al. World Journal of Surgical Oncology 2014, 12:163 WORLD JOURNAL OF SURGICAL ONCOLOGY CASE REPORT Open Access Free posterior tibial flap reconstruction for hypopharyngeal squamous cell carcinoma
Benefits of Genomic Medicine: What to Tell the Patient
 Benefits of Genomic Medicine: What to Tell the Patient Christine H. Chung, M.D. Associate Professor of Oncology Director, HNC Therapeutics Program Johns Hopkins University No Conflict of Interest to Disclose
Benefits of Genomic Medicine: What to Tell the Patient Christine H. Chung, M.D. Associate Professor of Oncology Director, HNC Therapeutics Program Johns Hopkins University No Conflict of Interest to Disclose
DELAYED TREATMENT OF PHARYNGOESOPHAGEAL TRAUMA
 Delayed Treatment of Pharyngoesophageal Trauma Chapter 41 DELAYED TREATMENT OF PHARYNGOESOPHAGEAL TRAUMA NICI EDDY BOTHWELL, MD* INTRODUCTION PHARYNGOESOPHAGEAL STRICTURES TRACHEOESOPHAGEAL FISTULAS PHARYNGOESOPHAGEAL
Delayed Treatment of Pharyngoesophageal Trauma Chapter 41 DELAYED TREATMENT OF PHARYNGOESOPHAGEAL TRAUMA NICI EDDY BOTHWELL, MD* INTRODUCTION PHARYNGOESOPHAGEAL STRICTURES TRACHEOESOPHAGEAL FISTULAS PHARYNGOESOPHAGEAL
Tongue cancer. Patient information
 What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
What is cancer? The human body is made up of billions of cells. In healthy people, cells grow, divide and die. New cells constantly replace old ones in an orderly way. This process ensures each part of
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Disclosure. Access 10/4/2013. The emerging role of TransOralRobotic Surgery (TORS) Organ preservation in the management of head and neck cancer
 Organ preservation in the management of head and neck cancer") Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Introduction. Etiology. Incidence 2/18/17
 Introduction Urethral stricture refers to narrowing of the urethral lumen from scar tissue. Usually used for anterior urethral disease Posterior Urethral strictures usually is a stenotic process after
Introduction Urethral stricture refers to narrowing of the urethral lumen from scar tissue. Usually used for anterior urethral disease Posterior Urethral strictures usually is a stenotic process after
Surgery. Head and Neck Cancers III: Treatment and Survival. Lip. Surgery might be the only treatment
 Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1