ESMO Preceptorship Breast Cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia
|
|
|
- Lizbeth Lamb
- 5 years ago
- Views:
Transcription



1 ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia
2 Outline Rational for immune-based therapy in BC How to enhance immunogenicity? Evidences from clinical data How to monitor and to predict response?
3 TILs in EBC Reference N Trial Endpoint Subtype analyzed Result Denkert (JCO, 2010) 840 GBG G-3 pcr All pcr:41% in TIL+ BC Validated in G-5 Loi (JCO, 2013) 2009 BIG 2-98 DFS Preplanned analysis of molecular subtypes Prognostic impact in TNBC (n=256): HR:0.31 ( ) Loi (AnnOnc, 2014) 935 FinHer DFS Preplanned analysis of molecular subtypes Prognostic impact in TNBC (n=134): HR:0.31 ( ) Adams (JCO, 2014) 506 ECOG 2197 ECOG 1199 DFS TNBC HR:0.84 ( ) Dieci (AnnOnc, 2014) 278 MFS OS TNBC HR:0.86 ( ) HR:0.86 ( ) Denkert (JCO 2015) 580 Gepar- Sixto trial pcr TNBC and HER2 pcr rate was 59.9% in LPBC and 33.8% for non- LPBC (P <.001)
4 Mutational load of breast cancer Budczies J eta l. The Journal of Pathology: Clinical Research, 2015, Volume 1, Issue 4, pages ,

5 Classical pathology and mutational load of breast cancer integration of two worlds Budczies J eta l. The Journal of Pathology: Clinical Research, 2015, Volume 1, Issue 4, pages ,

6 Phase I open-label dose-escalation vaccine trial of dher2 protein with AS15 adjuvant in HER2-overexpressing patients with high-risk breast cancer G. Curigliano et al. 2016
7 Endpoints Primary: Safety Secondary: Humoral immunogenicity Cell-mediated immunogenicity Impact of escalating doses of HER2 G. Curigliano et al. 2016
8 Study design Cohorts N Dose (Route: IM) Timing Cohort µg dher2/as15 D 0, 14, 28, 42 (70 & 98) Cohort µg dher2/as15 D 0, 14, 28, 42 (70 & 98) Cohort µg dher2/as15 D 0, 14, 28, 42 (70 & 98) Cohort µg W 0, 4, 14, 34, 38
9 Study design: Treatment 2 weeks 4 weeks screening week analysis PBMC Ab X X X X X X X X X X X X X X X X MUGA
10 GMT (EU/ml) Immunogenicity dher2-as anti-ecd Ab titers Cohort 1 (20mcg dher2) Cohort 2 (100mcg dher2) Cohort 3 (500mcg dher2) 1000 Cohort 3 (500 µg) 100 Cohort 2 (100 µg) Cohort 1 (20 µg) G. Curigliano et al. 2016
11 Responders anti ECD and anti ICD % anti-ecd antibody responders % anti-icd antibody responders % of responder patients % of responder patients Cohort 1 Cohort 2 Cohort 3 Cohort 4 0 Cohort 1 Cohort 2 Cohort 3 Cohort 4 G. Curigliano et al. 2016
12 d-her2 induces antibodies that specifically bind the native HER2 receptor The ECD binding ratio seems to increase with the dose of HER2 protein when assessed after the administration of four dher2 + AS15 doses. SKBR3 BT Day 0 Day 56 Day 0 Day 56 % A B C 0 Cohort 1 Cohort 2 Cohort 3 Cohort 4 G. Curigliano et al. 2016
13 How to enhance immunogenicity? DRUG Doxorubicin Cyclophosphamide EFFECT ON IMMUNE SYSTEM Induces immunogenic cell death Increases proliferation of CD8 T cells Stimulates antigen presentation by DCs Stimulates MCP1 and M6PR Induces immunogenic cell death Suppressed Treg inhibitory functions and restoration of the proliferative capacity of effector T cells and NK cell cytotoxicity. Taxanes Enhance T cell and NK cell function Increase recruitment of TIL Increase efficacy of immuno-stimulatory agents Gemcitabine Reduce the number of myeloid suppressor cells Increase the antitumor activity of CD8(+) T cells and activated NK cells Oxaliplatin Induces immunogenic cell death Increases MHC I complex Inhibits PDL2 13
doi:10.")
14 β-catenin signalling prevents anti-tumour immunity Spranger S et al, Nature 523, (09 July 2015)doi: /nature14404
15 Evidence from clinical trials Pembrolizumab (Merck) Humanized IgG4 anti- PD-1 antibody MPDL3280 (Genentech) engineered human IgG1 anti-pd-l1 antibody
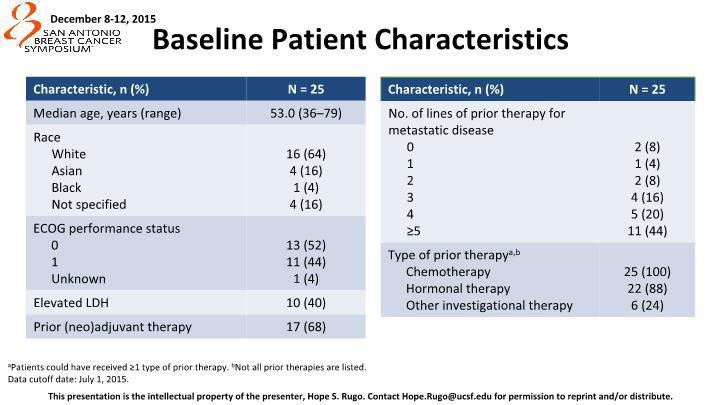
16 Pembrolizumab in TNBC Recurrent or metastatic ER-/PR-/HER2- breast cancer ECOG PS 0-1 PD-L1+ tumour No systemic steroid therapy Pembro 10 mg/kg Q2W CR PR/SD Discontinuation permitted Treat for 24 mo or until PD or toxicity No autoimmune disease (active or history of) No active brain metastases Confirmed PD Discontinue PD-L1 positivity: 58% of all patients screened had PD-L1-positive tumors Treatment: 10 mg/kg IV Q2W Response assessment: Performed every 8 weeks per RECIST v1.1 a PD-L1 expression was assessed in archival tumor samples using a prototype IHC assay and the 22C3 antibody. Only patients with PD-L1 staining in the stroma or in 1% of tumor cells were eligible for enrollment. b If clinically stable, patients are permitted to remain on pembrolizumab until progressive disease is confirmed on a second scan performed 4 weeks later. If progressive disease is confirmed, pembrolizumab is discontinued. An exception may be granted for patients with clinical stability or improvement after consultation with the sponsor.

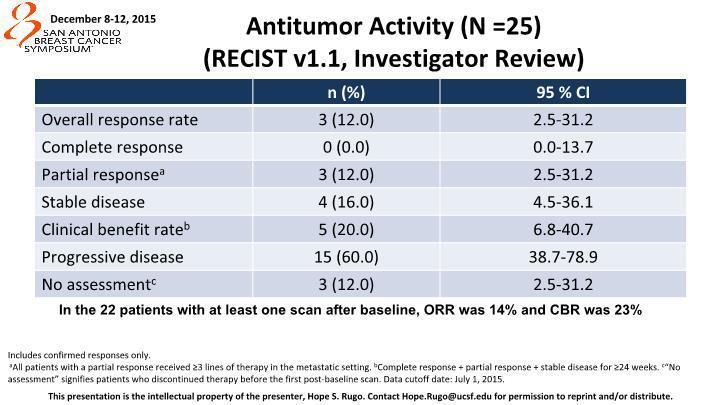
17 Pembrolizumab in TNBC n =32 Confirmed complete response (nodal disease) Confirmed partial response Stable disease Progressive disease Objective response rate: 18.5% Stable disease: 25.9% Nanda, SABCS 2015
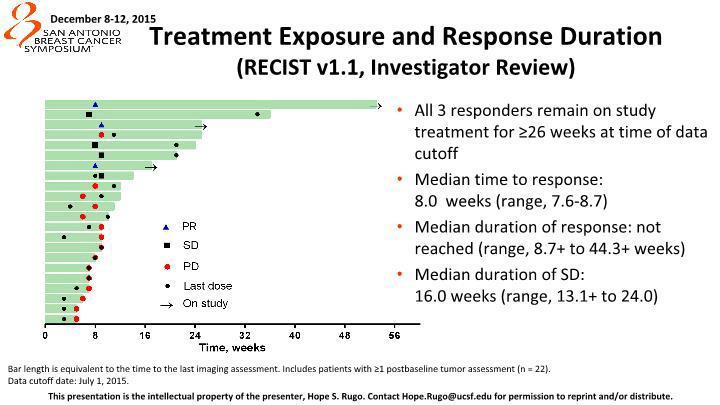
18 Pembrolizumab in TNBC Responder Nonresponder PD after CR, PR, or SD Last dose Treatment ongoing Best overall response CR PR SD PD Median follow-up duration: 9.9 months (range, ) Median time to response: 18 weeks (range, 7-32) Median duration of response a : not reached (range, 15 to 40+ weeks) PFS 1.9 ms; 6 ms PFS- 23% Time, weeks a Kaplan-Meier estimate. Analysis cut-off date: November 10, Nanda, SABCS 2014

19 Atezolizumab in ER+ BC
20 Atezolizumab in ER+ BC
21 Atezolizumab in ER+ BC
22 Atezolizumab in ER+ BC
23 Atezolizumab in ER+ BC
24 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc Best Overall Response 1L (n = 9) Confirmed ORR (95% CI) a 66.7% (29.9, 92.5) ORR (95% CI) b 88.9% (51.7, 99.7) 2L (n = 8) 25% (3.2, 65.1) 75.0% (34.9, 96.8) 3L+ (n = 7) 28.6% (3.7, 71.0) 42.9% (9.9, 81.6) All Patients N = % (22.1, 63.4) 70.8% (48.9, 87.4) CR 11.1% % PR 77.8% 75.0% 42.9% 66.7% Response rates were higher for patients who received atezolizumab/nabpaclitaxel treatment as 1L therapy compared to 2L+ SD 11.1% 25.0% 28.6% 20.8% PD % 8.3% a Confirmed ORR defined as at least 2 consecutive assessments of complete or partial response. b Including investigator-assessed unconfirmed responses. Efficacy-evaluable patients were dosed by June 1, 2015, and were evaluable for response by RECIST v1.1. Minimum efficacy follow up was 3 months. Adams S, et al. SABCS [abstract ].
 continued on treatment at time of data cut off Adams S, et al. SABCS.")
25 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc Including investigator-assessed unconfirmed responses. 11 of 17 responses (65%) continued on treatment at time of data cut off Adams S, et al. SABCS [abstract ].
26 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc IC0 (n = 7) IC1/2/3 (n = 9) Unknown (n = 8) ORR (95% CI) 57.1% (18.4, 90.1) 77.8% (40.0, 97.2) 75% (34.9, 96.8) CR % PR 57.1% 77.8% 62.5% SD 42.9% 22.2% 0 PD % Including investigator-assessed unconfirmed responses. Responses were observed in both IC0 and IC1/2/3 patients Adams S, et al. SABCS [abstract ].

27 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc Proliferating activated CD8+ T cells transiently peaked at the end of the first cycle of atezolizumab treatment Adams S, et al. SABCS [abstract ].
28 Phase III Study of Atezolizumab and Nab- Paclitaxel in mtnbc Randomized, double-blind, placebo-controlled Phase 3 trial of nab-paclitaxel ± atezolizumab as 1 st line therapy in mtnbc (NCT ) Study design Histologically documented locally advanced or metastatic TNBC No prior therapy for advanced disease ECOG PS 0-1 Measurable disease per RECIST v1.1 Patients with significant CV or CNS disease (except asymptomatic brain metastases), autoimmune disease or prior checkpoint inhibitor therapy are excluded Target accrual: ~350 pts Stratification factors: Presence of liver metastases Prior taxane therapy Nab-paclitaxel 100 mg/m 2 QW 3/4 + Atezolizumab 840 mg Q2W PD-L1 expression status (centrally evaluated by IHC using the SP142 assay) R 1:1 Nab-paclitaxel 100 mg/m 2 QW 3/4 + Placebo Q2W Co-primary endpoints: PFS in all patients PFS according to PD-L1 expression Secondary endpoints: OS ORR Response duration Safety/tolerability PK HR QoL Emens et al. SABCS 2015 (abstract OT )
 engineered human IgG1 anti-pd-l1 antibody MEDI4736 (AZ) Human IgG1 anti-pd-l1 antibody Tremelimumab (AZ) Human IgG2 Anti-CTLA-4")
29 Immunotherapy in TNBC Nivolumab (BMS) Human IgG4 anti-pd-1 antibody Pembrolizumab (Merck) Humanized IgG4 anti- PD-1 antibody MPDL3280 (Genentech) engineered human IgG1 anti-pd-l1 antibody MEDI4736 (AZ) Human IgG1 anti-pd-l1 antibody Tremelimumab (AZ) Human IgG2 Anti-CTLA-4 antibody
30 Immunotherapy in TNBC Phase Setting Subtype PD-L1 expression as inclusion criteria Combination/comparator Nivolumab II Metastatic TN No Monotherapy after induction with RT and CT Primary EP Pembrolizumab II Metastatic IBC HER2- No monotherapy Disease control rate Ib/II Metastatic TN No + eribulin DLT/ORR II Metastatic TN Cohort B (positive) Cohort C (strong) Ib/II Metastatic/ LABC HER2+ Presence of PD-L1 expression monotherapy PFS ORR/Safety + trastuzumab Safety/ORR II Metastatic HR+ No + Tamoxifen + Vorinostat Safety/ORR Atezolizumab III Metastatic TN No + nabpaclitaxel vs nabpaclitaxel Durvalumab II Metastatic HER2- No + tremelimumab (AZ) ORR PFS
31 Immunotherapy in TNBC: neoadjuvant setting Neoadjuvant setting NCT PD-1 blockade plus chemotherapy as Neoadjuvant treatment for TNBC Not yet opened Pembrolizumab Nab-paclitaxel Anthracycline Cyclophosphamide Carboplatin Merck Sharp & Dohme Corp. NCT /2 Anti PD-L1 therapy plus Nab-Paclitaxel and dosedense AC as Neoadjuvant treatment for Stage I-III Triple Negative Breast Cancer Recruiting MEDI4736 Nab-Paclitaxel Doxorubicin Cyclophosphamide Yale University
32 Immunotherapy in TNBC: neoadjuvant setting N=272 Primary endpoint: EFS Secondary endpoint: pcr (ypt0-yptis ypn0) surgery R +/-ATEZOLIZUMAB 1200 mg Nab-Paclitaxel 125 mg/m 2 + CBDCA AUC2
33 Immunotherapy in TNBC: neoadjuvant setting N=174 Primary endpoint: pcr (ypt0 ypn0) Nab-Paclitaxel EC surgery R MEDI 4736/Durvalumab Placebo Window of opportunity 2weeks Nab-P 125 mg/m 2 Epirubicin 90 mg/m 2 + Cyclophosphamide 600 mg/m 2 MEDI 4736/Durvalumab 2g total q4w
34 Adaptive Phase II Randomized Non-comparative Trial of Nivolumab After Induction Treatment in Triple-negative Breast Cancer (TNBC) Patients: TONIC-trial (The Netherlands Cancer Institute) Treatment Arm Assigned intervention Active Comparator: Radiation therapy Radiotherapy on metastatic lesion Active Comparator: Low dose doxorubicin 15 mg flat dose, once weekly for 2 weeks Active Comparator: Cyclophosphamide metronomic schedule, 50 mg daily orally for 2 weeks Active Comparator: Cisplatin 40 mg/m2, weekly for 2 weeks Active Comparator: No induction treatment Nivolumab 3 mg/kg, every 2 weeks after induction treatment Radiation: Radiation therapy 20 Gy to metastatic lesion Nivolumab 3 mg/kg, every 2 weeks after induction treatment Low dose doxorubicn Nivolumab 3 mg/kg, every 2 weeks after induction treatment Metronomics CTX Nivolumab 3 mg/kg, every 2 weeks after induction treatment Weekly cisplatin Nivolumab 3 mg/kg, every 2 weeks after induction treatment
 No active brain metastases Pembro")


35 Targeting stroma and inflammation Recurrent or metastatic LBC or IBC ECOG PS 0-1 No systemic steroid therapy No autoimmune disease (active or history of) No active brain metastases Pembro 200 mg Q3W + CTX 50 mg/die Complete Response Partial Response or Stable Disease Confirmed Progressive Disease b Discontinuation Permitted Treat for 24 months or until progression or intolerable toxicity Discontinue PD-L1 positivity: Stratification factor Treatment: metronomic CT plus pembrolizumab Response assessment: Performed every 8 weeks per RECIST v1.1 PI G. Curigliano et al.

36 Predicting immune-response Herbst RS et al Nature 515, , 2014
37 Predicting response Immune cells function in an interacting hierarchy that coordinates the activities of various cell types according to genetic and environmental contexts. Development of a graphical approaches to construct an extensible immune reference map from mass cytometry data of cells from different organs. The maps recapitulated canonical cellular phenotypes and revealed reproducible, tissue-specific deviations.

38 Democratizing systems immunology with modular transcriptional repertoire analyses Chaussabel D et al. Nature Reviews Immunology 14, (2014)
39 Conclusions Is there a rational for immune-based therapy in BC? YES Evidences from clinical data? LIMITED Can you enhance immunogenicity? MAY BE Can we monitor and to predict response? NO, BUT
40 Challenges Predicting responsive patients by modular transcriptional repertoire analysis Tissue and blood biomarkers for combination immunotherapies Role of microbioma and modulation of microbioma Managing combination-associated toxicity
41 Thank you
ESMO Preceptoship in Immuno-Oncology. Clinical Development: Breast Cancer
 ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Systemic therapy of triple negative advanced breast cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development
 Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
Breast Cancer Immunotherapy. Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy
 Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Immunotherapy for Breast Cancer Clinical Development
 Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Management of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
Immunotherapy in breast cancer. Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy
 Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immunotherapy for Breast Cancer
 Immunotherapy for Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia, Milano, IT Lymphocytic infiltration assessed by HES and
Immunotherapy for Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia, Milano, IT Lymphocytic infiltration assessed by HES and
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy
 Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Emerging Strategies in Triple-Negative Breast Cancer
 Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Treatment of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Checkpoint Inhibitors in Triple-Negative Breast Cancer (TNBC): Where to Go From Here
: Where to Go From Here") Review Article Checkpoint Inhibitors in Triple-Negative Breast Cancer (TNBC): Where to Go From Here Maryann J. Kwa, MD; and Sylvia Adams, MD, MS Advances in cancer immunotherapy and a growing body of research
Review Article Checkpoint Inhibitors in Triple-Negative Breast Cancer (TNBC): Where to Go From Here Maryann J. Kwa, MD; and Sylvia Adams, MD, MS Advances in cancer immunotherapy and a growing body of research
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Now Available: Final Rule for FDAAA 801 and NIH Policy on Clinical Trial Reporting
 A service of the U.S. National Institutes of Health Now Available: Final Rule for FDAAA 801 and NIH Policy on Clinical Trial Reporting Trial record 1 of 1 for: Keynote 355 Previous Study Return to List
A service of the U.S. National Institutes of Health Now Available: Final Rule for FDAAA 801 and NIH Policy on Clinical Trial Reporting Trial record 1 of 1 for: Keynote 355 Previous Study Return to List
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Overview of nab-paclitaxel in Breast Cancer
 Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD
 Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance
 Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
The Expert Thoughts. Alessandra Fabi Oncologia Medica 1
 The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
The Expert Thoughts Alessandra Fabi Oncologia Medica 1 My Thoughts Neoadjuvant: from the lessons of the history Adjuvant: Escalation and De-escalation Advanced and HER2+ : field for immunomodulation Brain
Breast Cancer New Horizons in the Era of Immunotherapy
 Breast Cancer New Horizons in the Era of Immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation Research (MedSIR)
Breast Cancer New Horizons in the Era of Immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation Research (MedSIR)
San Francisco, CA United States January 27, 2018
 San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Immunotherapy for Breast Cancer HOPE S. RUGO, MD Professor of Medicine Division of Hematology and Oncology Director,
San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Immunotherapy for Breast Cancer HOPE S. RUGO, MD Professor of Medicine Division of Hematology and Oncology Director,
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
Perspectivas de desarrollo de la inmunoterapia en cáncer de mama hereditario. Luis de la Cruz Merino Oncología Médica HUVMacarena (Sevilla)
") Perspectivas de desarrollo de la inmunoterapia en cáncer de mama hereditario Luis de la Cruz Merino Oncología Médica HUVMacarena (Sevilla) Outline Immunology and breast cancer Clinical trials with modern
Perspectivas de desarrollo de la inmunoterapia en cáncer de mama hereditario Luis de la Cruz Merino Oncología Médica HUVMacarena (Sevilla) Outline Immunology and breast cancer Clinical trials with modern
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Point of View on Early Triple Negative
 Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group
 Hal Hirte Canadian Cancer Clinical Trials Group") Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Lo Studio Geparsepto. Alessandra Fabi Oncologia Medica 1
 Lo Studio Geparsepto Alessandra Fabi Oncologia Medica 1 nab-paclitaxel Versus Solvent-Based Paclitaxel in Neoadjuvant Chemotherapy for Early Breast Cancer (GeparSepto GBG 69): A Randomised, Phase III Trial
Lo Studio Geparsepto Alessandra Fabi Oncologia Medica 1 nab-paclitaxel Versus Solvent-Based Paclitaxel in Neoadjuvant Chemotherapy for Early Breast Cancer (GeparSepto GBG 69): A Randomised, Phase III Trial
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari
 Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
Highlights in breast cancer
 CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
2014 San Antonio Breast Cancer Symposium Review
 2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Amreen Husain, 10 Eric P. Winer, 11 Sylvia Adams, 12 Peter Schmid 13
 IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy. Javier Cortes, Ramon y
 Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation
Optimizing anti-her-2 therapies for ABC Potential role of immunotherapy Javier Cortes, Ramon y Cajal University Hospital, Madrid, Spain Vall d Hebron Institute of Oncology (VHIO), Medica Scientia Innovation
ULTIMATE GBG 95 UC-0140/1606 BIG UnLock The IMmune cells ATtraction in ER+ breast cancer
 ULTIMATE GBG 95 UC-0140/1606 BIG 16-01 UnLock The IMmune cells ATtraction in ER+ breast cancer A PHASE II TRIAL TESTING DURVALUMAB COMBINED WITH ENDOCRINE THERAPY IN PATIENTS WITH ER+/HER2- BREAST CANCER
ULTIMATE GBG 95 UC-0140/1606 BIG 16-01 UnLock The IMmune cells ATtraction in ER+ breast cancer A PHASE II TRIAL TESTING DURVALUMAB COMBINED WITH ENDOCRINE THERAPY IN PATIENTS WITH ER+/HER2- BREAST CANCER
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Presenter Disclosure Information
 Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Disclosure Information. Mary L. Disis
 Disclosure Information Mary L. Disis I have the following financial relationships to disclose: Consultant for: VentiRx, Celgene, Emergent, EMD Serono Speaker s Bureau for: N/A Grant/Research support from:
Disclosure Information Mary L. Disis I have the following financial relationships to disclose: Consultant for: VentiRx, Celgene, Emergent, EMD Serono Speaker s Bureau for: N/A Grant/Research support from:
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Ca Cardias e Stomaco: le diversita e le terapie
 XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
XXII Riunione Nazionale I.T.M.O. Ca Cardias e Stomaco: le diversita e le terapie Maria Di Bartolomeo s.s. Oncologia Medica Gastroenterologica Fondazione IRCCS Istituto Nazionale Tumori Milano OUTLINE History
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib