Systemic Therapy of Melanoma Current Approved Options
|
|
|
- Elfreda Skinner
- 5 years ago
- Views:
Transcription
1 Systemic Therapy of Melanoma Current Approved Options Stage IIb-III (high risk) Melanoma Only High-dose IFNα is approved by US FDA Stage IV (inoperable) survival <2% at 5+ years Only one cytotoxic agent is approved by FDA Dacarbazine (Temozolomide) with % response in modern trials, rarely durable Only one biologic approved in modern times High-dose IL-2, with 15% response and 5% durable responses
2 Opportunities from Chemotherapy and Biological Agents Tumor bulk reduction in and of itself may facilitate biological therapy Chemotherapy may reduce Treg and other elements of immunosuppressive environment Chemotherapy may serve as means to release tumor antigen Each of these needs to be assessed rigorously to establish proof of principle
3 Chemotherapy of Melanoma: Little impact to date Tumor cell resistance to cytotoxic drugs (Dacarbazine, TMZ): I. Alkyl guanine alkyl transferase expression (AGAT) Resistance Patrin, an oral AGAT inhibitor doubles toxicity of DTIC/TMZ Tawbi et al., Proc ASCO 2006 II. III. Mismatch Repair Required for Responsiveness to Alkylators Sobol, et al Proc ASCO 2006 Base Excision Repair -- β pol and other mechanisms now understood PARPi of strong interest: Plummer et al., Proc ASCO 2006 #8013 Tumor cell resistance to apoptosis BCL2 Survivin UBC9 XIAP Tumor induced immunosuppression STAT3 PDL1 FASL
4 1.0 Overall Survival by Protocol Survival Probability E1675 E1686 E1687 E2681 E2683 E2685 E3690 E Survival Time (Months) Manola, et al., J. Clinical.Oncology 1999
5 Empiric Combinations without Intermediate Surrogate Markers have Failed to Improve Outcome in Large Phase III Trials Dacarbazine and IFN Dacarbazine and Tamoxifen CBD and Tamoxifen CVD and IL-2 IFN
6 Recent Phase III Trials of Chemotherapy Combinations DTIC +/- IFN +/- Tam DTIC vs Dartmouth Falkson et al: JCO ; 1998 Chapman et al: JCO 1999

7 E3695: Survival Data
8 CTEP-sponsored studies of combination targeted therapy NCI solicited studies in renal cell, glioma, and melanoma have not incorporated chemotherapy (yet) Melanoma targets of interest: VEGF, Raf, Ras, mtor Tipifarnib + Sorafenib Bevacizumab + Sorafenib CCI Sorafenib CCI Bevacizumab In all studies, tumor and surrogate tissue samples to be collected for biologic studies & banked.
9 Phase I trial of Lomeguatrib (Patrin) combined with dacarbazine for treatment of patients with melanoma The DNA repair enzyme O6-Alkylguanine Alkyl transferase (AGT) reverses O6-methylguanine (O6-MeG) base lesion induced by DTIC Depletion of AGT using O6-MeG analogs enhances DTIC cytotoxicity in preclinical and phase I trials of O6-Benzylguanine Lomeguatrib (Patrin) is orally bioavailable potent O6-MeG analog well-tolerated as a single agent First phase I experience for PN combined with DTIC reported in patients who failed prior CTx Tawbi et al., # :



10 Mechanism of Action of Patrin DTIC G - Me cell death AGT cell survival Patrin cell death
11 Results Adverse events observed in 50% of pts: grade 1-2 nausea and vomiting, grade 1-2 fatigue Hematologic toxicity prominent: gr3-4 neutropenia in 14 pts (47%) gr3-4 thrombocytopenia in 4 pts (13%) even at doses of DTIC 50% of usual clinical doses Prolonged neutropenia represented all doselimiting toxicities (DLT) observed so far The MTD not yet reached: hematologic toxicities requiring dose modification of DTIC frequent (42% of all cycles administered).
12 Conclusions Oral Patrin alters toxicity and tolerability of DTIC induces prolonged hematologic toxicity at dosages that are <50% of routine dosages tolerated w/o Patrin Results consistent with phase I studies of O 6 -MeG analogs but with major advantage of oral route Patrin allows for schedules of administration that provide maximal and prolonged depletion of AGT. In this study Patrin was tolerated at 40 mg bid for 10 days MTD of Patrin combined with DTIC to be refined and efficacy in first line therapy defined in ongoing study
13 To Die or not to Die: DNA Repair Pathways Liu, L. et al. Clin Cancer Res 2006;12:
14 Mechanism of Resistance II: MMR Functional MMR is required for cytotoxicity of DTIC MMR deficiency associated with resistance Decreased expression of MLH1, MSH2 and MSH6 related to decreased response Epigenetic silencing by promoter gene hypermethylation leads to loss of MMR
15 Mechanism of Resistance II: MMR Pilot study of tumor tissues from DTIC/TMZ treated patients with response or nonresponse: Tumor tissues from 17 patients with metastatic melanoma treated with alkylator-based therapy at the UPCI Melanoma Program examined Analysis of clinical response vs MLH1: responder vs non-responder IHC performed for MLH1 7/9 sensitive tumors exhibit high MLH1 expression compared with 1/7 resistant tumors (p=0.015) Sobol, Tawbi, Kirkwood Proc ASCO 2006
16 Mechanism of Resistance: MMR MLH1 expression MLH-1 Expression 1 = Non-Responders 2 = Responders Series1 Series1 Series2 Series2 Series3 Series3 Series4 Series4 Series5 Series5 Series6 Series6 Series7 Series7 Series8 Series8 Series9 Series9 Series10 Series10 Series11 Series11 Series12 Series12 Series13 Series13 Series14 Series14 Series15 Series15 Series16 Series16 Series17 Series
17 Abrogating Resistance II: Reactivate MMR Reversal of promoter hypermethylation of MMR genes increases alkylating agent sensitivity 5-aza-2 -deoxycytidine re-activates MMR pathway TMZ + Patrin + 5-aza-2 -deoxycytidine shows enhanced cytotoxicity in drug-resistant ovarian cancer cell lines Dual DNA repair modulation of interest 5-azacytidine is a demethylator already in clinical use for acute leukemia and MDS

18 To Die or not to Die: DNA Repair Pathways Liu, L. et al. Clin Cancer Res 2006;12:
19 Mechanism of Resistance III: BER N 7 -MeG is recognized by DNA glycosylases that initiate BER. DNA intermediate (5 -drp) induces DNA replication block and triggers cellular toxicity. 5 -drp is substrate removed by DNA polymerase β (pol-β) Alkylating agents induce increased cytotoxicity in pol-β deficient cells
20 Mechanism of Resistance III: BER Pol-β expression Series1 Series1 Series2 Series2 Series3 Series3 Series4 Series4 Series5 Series5 Series6 Series6 Series7 Series7 Series8 Series8 Series9 Series9 Series10 Series10 Series11 Series11 Series12 Series12 Series13 Series13 Series14 Series14 Series15 Series15 Series16 Series16 Series17 Series
21 Abrogating Resistance III: Targeting BER Pol-β expression can be inhibited with sirna, but no small molecule inhibitor is yet available Methoxyamine an alternate route to inhibit BER Poly (ADP)-Ribose Polymerase (PARP) is an enzyme recruited early at site: negatively charged riboses push DNA strands apart allowing BER proteins to access DNA PARP inhibitors are already in phase I trials (UK)
22 Phase II study of poly (ADP-ribose) polymerase inhibitor (PARPi) AGO14699 in combination with TMZ 40 patients with measurable cutaneous MM AGO mg and TMZ 200 mg/m2 5x daily q 4 weeks Two stage study powered to detect 25% improvement in response to TMZ with patients at 3 responses Toxicity: Grade IV-- Platelets 12% and ANC 15%; Gr V: 1 Response: PR in 4 and prolonged SD in 4 of 20 eval; 20 TE Plummer et al., 2006 # :457
23 Chemotherapy/Drug Resistance Conclusions Alkylating agent efficacy is decreased due to tumor resistance based upon DNA repair Small molecule inhibitors are available or in development for each known pathway Future is likely to be multi-targeted approach: combining inhibitors and protecting stem cells Individualized therapy is possible based on assessment of DNA repair potential
24 Common themes of successful interventions Immunomodulation Induction of autoimmunity anti-pigmentary and other phenomena
25 Proportion Alive and Relapse-Free 25 Updated Durable Relapse-Free Survival Is Highly Significant for E E1684 IFN vs Observation: p 2 =0.02, p 1 =0.01, HR= Time (Years) Time Interval Group Observation 89/140 12/51 3/39 0/35 1/32 1/29 0/15 0/3 Interferon 73/146 14/68 3/53 1/50 2/48 2/44 0/31 0/10 (# events/# at risk) Proportion Alive and Relapse-Free E1690 IFN vs Observation: p 2 =0.09, HR= Time (Years) Time Interval Group Observation 105/212 16/94 5/72 2/44 0/13 Interferon 98/215 15/108 5/85 2/53 0/20 (# events/# at risk) E1694 Proportion Alive and Relapse-Free IFN vs GMK: p 2 =0.006, HR= Time (Years) Proportion Alive and Relapse-Free E2696 GMK + Concurrent IFN vs GMK Alone: p 2 =0.18, HR=1.56 GMK + Sequential IFN vs GMK Alone: p =0.14, HR= Time (Years) Time Interval Group Interferon 118/436 28/257 8/123 3/47 0/3 GMK 153/439 40/240 6/113 3/40 0/0 (# events/# at risk) Time Interval Group Concurrent 10/36 5/25 2/14 0/4 Sequential 8/36 4/26 3/17 1/7 GMK Alone 16/35 3/17 1/11 0/3 (# events/# at risk)
26 E A randomized study of four weeks of high-dose interferon alpha-2b in stage T3-T4 or N1 (microscopic) melanoma Hypothesis: Induction IV IFN is necessary and sufficient to achieve durable adjuvant benefit in intermediate-risk melanoma patients STRATIFICATION Pathologic Lymph Node Status Known Unkown Lymph Node Staging Procedure Sentinel Lymph Node Procedure Elective Lymph Node Dissection No Lymphadenectomy Breslow Depth mm mm > 4 mm Ulceration of Primary Lesion Yes No Disease Stage Lymph Node Positive Lymph Node Negative R A N D O M I Z E Arm A: Observation Arm B: 4 week high-dose IFN alfa-2b (Intron A) 20 MU/m 2 /d qd IV for 5 consecutive days out of 7 (M-F) every week times 4 weeks
27 Neoadjuvant Therapy of Stage III UPCI Study Biomarker discovery predict treatment efficacy correlate with long-term disease impact Define molecular mechanisms of IFN action Which of multiple known direct pro-apoptotic, indirect immunomodulatory, anti-angiogenic effects are critical? Measure clinical response early at 4 weeks to determine correlation with RFS and OS Moschos, Kirkwood Proc ASCO 2005; J. Clin Onc July 1, 2006
28 UPCI Schema Stage IIIB, IIIC melanoma (Tx, N2b, or or N3, M0) IFN-α2b induction therapy (20 MU/m 2 /d /d IV IV 5d/wk, 4 wks) IFN maintenance therapy (10 MU/m 2 /d /d tiw, wks) Enrollment Excisional biopsy (sample 1) Radical regional lymphadenectomy (sample 2)
29 UPCI Results 20 patients (age: median 59, range 40-78, 13 males) 11 with recurrent disease 15 completed 4 weeks of HDI At 4 weeks of treatment: Clinical responses 1 complete, 10 partial Pathologic responses 3 complete, 2 microscopic residual disease
30 HDI increases the number of immunologically relevant cells infiltrating regional lymph node metastatic tumor post-treatment CD pre-treatment CD3+ responders CD3+ nonresponders p=0.09 post-treatment CD pre-treatment CD4+ responders CD4+ nonresponders p=0.14 post-treatment CD11c CD11c+ responders CD11c+ nonresponders p=0.09 post-treatment CD56 CD56+ responders CD56+ nonresponde p= pre-treatment pre-treatment post-treatment CD83 CD83+ responders CD83+ nonresponders p=0.06 post-treatment CD86 CD86+ responders CD86+ nonresponders p= pre-treatment pre-treatment


31 CD3 pt et et CD11c et et pt before after


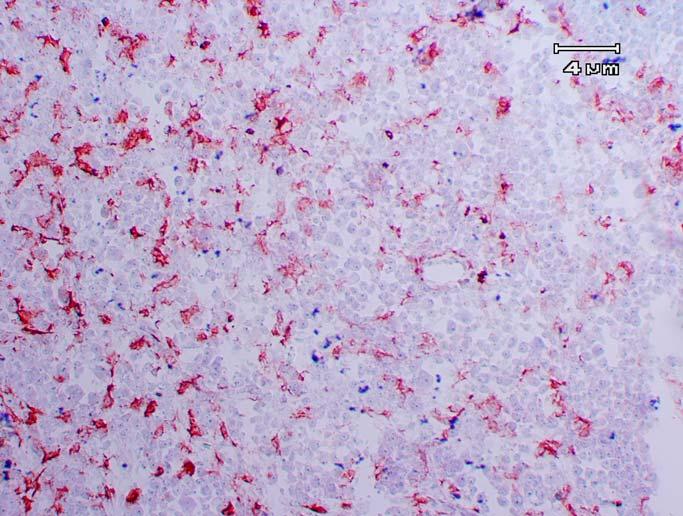
32 HDI Down-Regulates pstat3 Tyr705 And STAT3 Expression in Tumor Cells Pretreatment Post treatment IHC H&E Blue = pstat3tyr705 Red = STAT3
33 HDI Down-Regulates pstat3 Tyr705 and STAT3 in Regional Lymph Node Melanoma pstat3 STAT3 (post-pre)/pre % P =.002 P =.028 Mean n = pre post pre post -60 pstat3 STAT3

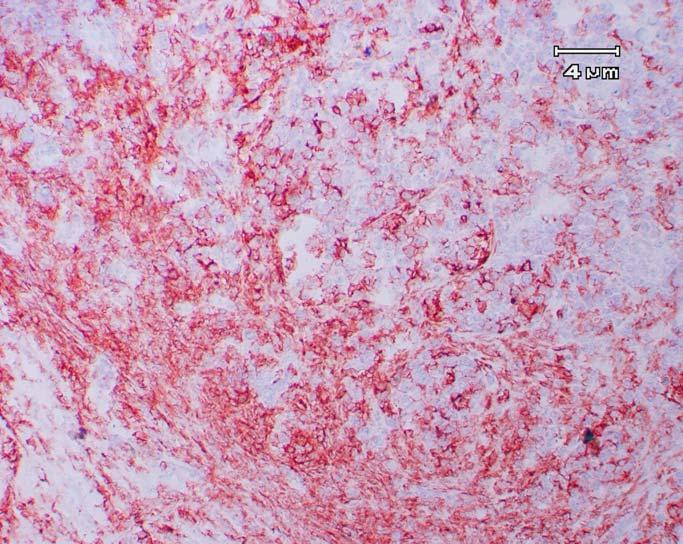
34 HDI Up-Regulates pstat1 Tyr701 as it Down-Regulates pstat3 Tyr705 and therefore Alters STAT1/STAT3 Balance Snap-Frozen Regional Lymph Node Tumor Pretreatment Post treatment Blue = pstat1 tyr701 Red = pstat3 tyr705 Frozen section IHC
35 HDI Up-regulates pstat1 Tyr701 and Down-regulates pstat3 Tyr705 in Melanoma mean n = 11 P = pre post pre post pre post pstat1 pstat3 pstat1/pstat3 pstat1 pre pstat1 post (Post-pre)/pre% pstat3 pre pstat1/pstat3 pre P =.049 pstat3 post pstat1/pstat3 post P = pstat1 tyr701 pstat3 tyr705 pstat1/pstat3 ratio
36 Conclusions of Neoadjuvant High-Dose IFN-α2b Trial UPCI Improved clinical response at day 29 55% of patients with objective response Radiographic and pathologic criteria Relapse-free and overall survival data too early for final assessment Molecular and immunologic impact including: pstat3/stat3, IFNAR2 pstat1, pstat1/3 ratio, and TAP2 CD3 T cell and CD11c dendritic cell populations in tumor
37 Current Approaches to Improve Results with Adjuvant Therapy Hellenic Oncology Group Trial comparing Induction alone vs 1 year of modified HDI Autoantibody response predicts RFS and OS (Gogas 2006) IMI trial of HDI Induction q. 2 mos x 4 (80 doses, n=300, Endpoint=RFS, OS) DeCOG trial of HDI Induction q. 4 mos x 1 year (60 doses, n=800, Endpoint=OS) Accrual is now ~15/month with 14 sites Intermediate endpoint MX protein induction


38 Progressive Paraneoplastic Vitiligo Immune recognition and response to melanosomal markers of melanoma may be harnessed therapeutically Nordlund, Kirkwood J Am Acad Derm 198:102, 1983
39 Overall survival plot by antibodies 1,0 OS Probability,5 0, Months
40 Current Trials to Build upon IFN IFN combined with other agents for stage IV Peptide and DC-based Vaccines (04-125) Antibodies to GD3 UPCI /LUD Anti-CTLA4 CP (UPCI ) Neoadjuvant approach is reasonable for exploration of all new agents of promise Define influence GM-CSF, anti-ctla4, and other immunomodulators in tumor
41 Mechanism of Anti-CTLA4 is likely relevant to several biologicals Autoimmune reactions seen at a greater frequency with anti-ctla4 antibody than with any other biological agent Autoimmune responses with High-dose IL-2 (Atkins, NEJM 1987) and High-dose IFNα (Gogas NEJM 2006) are correlated with durable antitumor benefit
42 Progress in the Combined Modality Therapy of Melanoma Multiple scientifically valid approaches to therapy & trials that are currently in study Analysis of relevant endpoints --both Clinical (PFSR and OS) and Laboratory; Neoadjuvant designs are powerful Power sufficient to detect relevant differences Patience in awaiting mature results to avoid underestimation of the magnitude & durability of the results
The Challenge of Bringing Forward New Agents for Systemic Therapy of Melanoma
 The Challenge of Bringing Forward New Agents for Systemic Therapy of Melanoma John M. Kirkwood, MD Director, Melanoma and Skin Cancer Program University of Pittsburgh Cancer Institute Professor & Vice
The Challenge of Bringing Forward New Agents for Systemic Therapy of Melanoma John M. Kirkwood, MD Director, Melanoma and Skin Cancer Program University of Pittsburgh Cancer Institute Professor & Vice
Neoadjuvant approaches to the establishment of adjuvant therapeutic efficacy with IFN, anti-ctla4 and
 Neoadjuvant approaches to the establishment of adjuvant therapeutic efficacy with IFN, anti-ctla4 and combinations Ahmad A. Tarhini, MD, PhD Assistant Professor of Medicine, Clinical i l and Translational
Neoadjuvant approaches to the establishment of adjuvant therapeutic efficacy with IFN, anti-ctla4 and combinations Ahmad A. Tarhini, MD, PhD Assistant Professor of Medicine, Clinical i l and Translational
Adjuvant Therapy of High Risk Melanoma
 Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008
 ADJUVANT THERAPY Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008 Updated analysis and discussion of current
ADJUVANT THERAPY Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008 Updated analysis and discussion of current
Cytokines: Interferons, Interleukins and Beyond. Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center
 Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011
 Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
HDAC Inhibitors and PARP inhibitors. Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine
 HDAC Inhibitors and PARP inhibitors Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine Histone Acetylation HAT Ac Ac Ac Ac HDAC Ac Ac Ac Ac mrna DACs
HDAC Inhibitors and PARP inhibitors Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine Histone Acetylation HAT Ac Ac Ac Ac HDAC Ac Ac Ac Ac mrna DACs
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Systemic Management of Melanoma
 Systemic Management of Melanoma From explorations of advanced disease to adjuvant high-risk and precursor arenas in search of better understanding and therapeutic success John M. Kirkwood, MD Director,
Systemic Management of Melanoma From explorations of advanced disease to adjuvant high-risk and precursor arenas in search of better understanding and therapeutic success John M. Kirkwood, MD Director,
Cancer Registry Report. Cancer Focus: Melanoma
 Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 1 October 2016 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Immunology in the CNS
STATE OF THE ART 4: Combination Immune Therapy-Chemotherapy. Elizabeth M. Jaffee (JHU) James Yang (NCI) Jared Gollob (Duke) John Kirkwood (UPMI)
 James Yang (NCI) Jared Gollob (Duke) John Kirkwood (UPMI)") STATE OF THE ART 4: Combination Immune Therapy-Chemotherapy Elizabeth M. Jaffee (JHU) James Yang (NCI) Jared Gollob (Duke) John Kirkwood (UPMI) Topics for Consideration What are the rules for integrating
STATE OF THE ART 4: Combination Immune Therapy-Chemotherapy Elizabeth M. Jaffee (JHU) James Yang (NCI) Jared Gollob (Duke) John Kirkwood (UPMI) Topics for Consideration What are the rules for integrating
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
CDC Recommendations for Skin Cancer Prevention. Systemic Therapy for Melanoma. Melanoma Incidence by Age and Gender: U.S.
 Systemic Therapy for Melanoma Adil Daud M.D. UCSF 0.016 0.016 1:74 1:74 Lifetime Risk Risk Lifetime 0.014 0.014 0.012 0.012 1:100 1:100 0.010 0.010 1:150 1:150 0.008 0.008 0.006 0.006 1:250 1:250 0.004
Systemic Therapy for Melanoma Adil Daud M.D. UCSF 0.016 0.016 1:74 1:74 Lifetime Risk Risk Lifetime 0.014 0.014 0.012 0.012 1:100 1:100 0.010 0.010 1:150 1:150 0.008 0.008 0.006 0.006 1:250 1:250 0.004
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
The 2010 Gastrointestinal Cancers Symposium Oral Abstract Session: Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract
 The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
Design considerations for Phase II trials incorporating biomarkers
 Design considerations for Phase II trials incorporating biomarkers Sumithra J. Mandrekar Professor of Biostatistics, Mayo Clinic Pre-Meeting Workshop Enhancing the Design and Conduct of Phase II Studies
Design considerations for Phase II trials incorporating biomarkers Sumithra J. Mandrekar Professor of Biostatistics, Mayo Clinic Pre-Meeting Workshop Enhancing the Design and Conduct of Phase II Studies
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
presentation session & clinical Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania
 Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
Melanoma: highlights from the oral presentation session & clinical science symposium at ASCO 2009 Keith T. Flaherty, M.D. Abramson Cancer Center of the University of Pennsylvania Abstracts to be discussed
PARP inhibitors for breast cancer
 PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
References: Published Clinical Trials in Metastatic Melanoma
 References: Published Clinical Trials in Metastatic Melanoma Melanoma historical data summary While results from open-label, or uncontrolled, or small # center studies can vary enormously, results from
References: Published Clinical Trials in Metastatic Melanoma Melanoma historical data summary While results from open-label, or uncontrolled, or small # center studies can vary enormously, results from
Human leukocyte antigen (HLA) system
 system") Is HLA a determinant of prognosis or therapeutic response to cytokines, IFN and anti-ctla4 blocking antibodies in melanoma? Helen Gogas, M.D. Ass. Professor in Medical Oncology 1st Department of Medicine,
Is HLA a determinant of prognosis or therapeutic response to cytokines, IFN and anti-ctla4 blocking antibodies in melanoma? Helen Gogas, M.D. Ass. Professor in Medical Oncology 1st Department of Medicine,
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
One Moment Please. Skin Cancer. Today s Webcast Friday, 09/09/11, Noon. David Carr, MD
 One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008
 Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008 REPORTS ON IMPORTANT ONGOING CLINICAL TRIALS CTLA-4 directed
Clinical Perspectives Highlights from the Perspectives in Melanoma XII Conference Scheveningen/The Hague, the Netherlands, October 2-4, 2008 REPORTS ON IMPORTANT ONGOING CLINICAL TRIALS CTLA-4 directed
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Vaccine Therapy for Cancer
 Vaccine Therapy for Cancer Lawrence N Shulman, MD Chief Medical Officer Senior Vice President for Medical Affairs Chief, Division of General Oncology Dana-Farber Cancer Institute Disclosures for Lawrence
Vaccine Therapy for Cancer Lawrence N Shulman, MD Chief Medical Officer Senior Vice President for Medical Affairs Chief, Division of General Oncology Dana-Farber Cancer Institute Disclosures for Lawrence
Glioblastoma and CNS tumors
 Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Glioblastoma and CNS tumors PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Amsterdam, 27 May 2017 Patrick Roth Department of Neurology and Brain Tumor Center University Hospital Zurich Challenges in immunooncology
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Protocol Abstract and Schema
 Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
Protocol Abstract and Schema This is a phase I/II study to determine: 1) the maximum tolerated dose (MTD) or recommended phase II dose of ABT-888 in combination with radiation therapy, and 2) the efficacy
GOG-172: Survival Outcomes
 CHEMOTHERAPY GOG-172: Survival Outcomes Progression-Free Survival Overall Survival Proportion Progression-Free 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Rx Group IV IP PF Failed Total 50 160 210 63 142
CHEMOTHERAPY GOG-172: Survival Outcomes Progression-Free Survival Overall Survival Proportion Progression-Free 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Rx Group IV IP PF Failed Total 50 160 210 63 142
Clinical: Ipilimumab (MDX-010) Update and Next Steps
 Update and Next Steps") Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
gp100 (209-2M) peptide and High Dose Interleukin-2 in HLA-A2+ Advanced Melanoma Patients Cytokine Working Group Experience
 peptide and High Dose Interleukin-2 in HLA-A2+ Advanced Melanoma Patients Cytokine Working Group Experience") gp100 (209-2M) peptide and High Dose Interleukin-2 in HLA-A2+ Advanced Melanoma Patients Cytokine Working Group Experience Metastatic Melanoma- Progress in Past 30 years Approved Therapies (USA) Date DTIC
gp100 (209-2M) peptide and High Dose Interleukin-2 in HLA-A2+ Advanced Melanoma Patients Cytokine Working Group Experience Metastatic Melanoma- Progress in Past 30 years Approved Therapies (USA) Date DTIC
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study
 temozolomide and radiation to treat glioblastoma: A retrospective study") Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Concomitant (without adjuvant) temozolomide and radiation to treat glioblastoma: A retrospective study T Sridhar 1, A Gore 1, I Boiangiu 1, D Machin 2, R P Symonds 3 1. Department of Oncology, Leicester
Advances in Melanoma
 Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
GOG212: Taxane Maintenance
 GOG212: Taxane Maintenance Epithelial Ovarian or Primary Peritoneal Cancer Optimal or Suboptimal Cytoreduction Clinical C with normal CA125, no symptoms, normal CT Primary Carboplatin and Paclitaxel (or
GOG212: Taxane Maintenance Epithelial Ovarian or Primary Peritoneal Cancer Optimal or Suboptimal Cytoreduction Clinical C with normal CA125, no symptoms, normal CT Primary Carboplatin and Paclitaxel (or
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Melanoma. Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania
 Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Update on Breast Cancer
 Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics. Timothy Cloughesy, MD University of California, Los Angeles
 Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
New Biological and Immunological Therapies for Cancer
 New Biological and Immunological Therapies for Cancer Sant P. Chawla, M.D., FRACP The Sarcoma Oncology Center, Santa Monica CA 90403 7 th International Conference on Drug Discovery &Therapy 1 Promising
New Biological and Immunological Therapies for Cancer Sant P. Chawla, M.D., FRACP The Sarcoma Oncology Center, Santa Monica CA 90403 7 th International Conference on Drug Discovery &Therapy 1 Promising
Enlarge Slides. One Moment Please. Skin Cancer. Thomas Olencki, DO David Carr, MD. Today s Webcast Friday, 09/09/11, Noon
 New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
Off-Label Treatments. Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease. Outline
 Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Off-Label Treatments Clinical Trials for Recurrent GBM UCSF Radiation Oncology Course: Management of Recurrent Disease Jennifer Clarke, MD, MPH Assistant Professor Division of Neuro-Oncology Depts of Neurological
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Improving Immunotherapy for Melanoma
 Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
Virtual Journal Club. Ovarian Cancer. Reference Slides. Platinum-Sensitive Recurrent Ovarian Cancer: Making the Most of Emerging Targeted Therapies
 Virtual Journal Club Ovarian Cancer Reference Slides Platinum-Sensitive Recurrent Ovarian Cancer: Making the Most of Emerging Targeted Therapies Mansoor R. Mirza, MD Copenhagen University Hospital Rigshospitalet
Virtual Journal Club Ovarian Cancer Reference Slides Platinum-Sensitive Recurrent Ovarian Cancer: Making the Most of Emerging Targeted Therapies Mansoor R. Mirza, MD Copenhagen University Hospital Rigshospitalet
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Carcinosarcoma Trial rial in s a in rare malign rare mali ancy
 Carcinosarcoma Trials in a rare malignancy BACKGROUND Rare and highly aggressive epithelial malignancies Biphasic tumors with epithelial and mesenchymal components Uterine carcinomas (UCS) uncommon with
Carcinosarcoma Trials in a rare malignancy BACKGROUND Rare and highly aggressive epithelial malignancies Biphasic tumors with epithelial and mesenchymal components Uterine carcinomas (UCS) uncommon with
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition
 Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition Lisa A Carey, MD Disclosures for Lisa A Carey, MD No real or apparent conflicts of interest to disclose Basal-Like
Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition Lisa A Carey, MD Disclosures for Lisa A Carey, MD No real or apparent conflicts of interest to disclose Basal-Like
University of California Los Angeles, Los Angeles, CA; 2. Department of Dermatology, University of Kiel, Kiel, Germany;
 Final Efficacy Results of A3671009, a Phase III Study of Tremelimumab vs Chemotherapy (Dacarbazine or Temozolomide) in First-line Patients With Unresectable Melanoma Antoni Ribas, 1 Axel Hauschild, 2 Richard
Final Efficacy Results of A3671009, a Phase III Study of Tremelimumab vs Chemotherapy (Dacarbazine or Temozolomide) in First-line Patients With Unresectable Melanoma Antoni Ribas, 1 Axel Hauschild, 2 Richard
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Update on PARP inhibitors
 Professor of Medicine Harvard Medical School Boston MA Update on PARP inhibitors Ursula Matulonis, M.D. Chief, Division of Gynecologic Oncology Brock-Wilson Family Chair Dana-Farber Cancer Institute History
Professor of Medicine Harvard Medical School Boston MA Update on PARP inhibitors Ursula Matulonis, M.D. Chief, Division of Gynecologic Oncology Brock-Wilson Family Chair Dana-Farber Cancer Institute History
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer
 Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Venetoclax in MCL. Prof. Le Gouill Nantes Medical University, France
 Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
The Good, the Bad and the Ugly: Clinical trials which assess vaccine characteristics. ISBT Meeting, San Francisco, CA November 4-8, 2004
 The Good, the Bad and the Ugly: Clinical trials which assess vaccine characteristics ISBT Meeting, San Francisco, CA November 4-8, 2004 Ideal cancer vaccine trial 1. An informative immune assay 2. Ability
The Good, the Bad and the Ugly: Clinical trials which assess vaccine characteristics ISBT Meeting, San Francisco, CA November 4-8, 2004 Ideal cancer vaccine trial 1. An informative immune assay 2. Ability
Personalized medicine - cancer immunotherapy
 Personalized medicine - cancer immunotherapy Özcan Met, PhD Senior Staff Scientist, Cell Therapy Director Center for Cancer Immune Therapy Department of Hematology Department of Oncology University Hospital
Personalized medicine - cancer immunotherapy Özcan Met, PhD Senior Staff Scientist, Cell Therapy Director Center for Cancer Immune Therapy Department of Hematology Department of Oncology University Hospital
Joseph J. Muscato, M.D., FACP Missouri Cancer Associates, Columbia Medical Director Virginia and Norm Stewart Cancer Center Boone Hospital
 Joseph J. Muscato, M.D., FACP Missouri Cancer Associates, Columbia Medical Director Virginia and Norm Stewart Cancer Center Boone Hospital One of the things we oncologists face is criticism for small
Joseph J. Muscato, M.D., FACP Missouri Cancer Associates, Columbia Medical Director Virginia and Norm Stewart Cancer Center Boone Hospital One of the things we oncologists face is criticism for small
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Adjuvant interferon therapy for malignant melanoma: the debate
 窑 Review 窑 Chinese Journal of Cancer Adjuvant interferon therapy for malignant melanoma: the debate Qiang Zhou 1,2, Xiao Shi Zhang 1,2 1 State Key Laboratory of Oncology in South China, Guangzhou, Guangdong
窑 Review 窑 Chinese Journal of Cancer Adjuvant interferon therapy for malignant melanoma: the debate Qiang Zhou 1,2, Xiao Shi Zhang 1,2 1 State Key Laboratory of Oncology in South China, Guangzhou, Guangdong
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
September 2017 A LOOK AT PARP INHIBITORS FOR OVARIAN CANCER. Drugs Under Review. ICER Evidence Ratings. Other Benefits. Value-Based Price Benchmarks
 September 2017 Drugs Under Review ICER s report reviewed the clinical effectiveness and value of olaparib (Lynparza, AstraZeneca), rucaparib (Rubraca, Clovis Oncology), and niraparib (Zejula, Tesaro),as
September 2017 Drugs Under Review ICER s report reviewed the clinical effectiveness and value of olaparib (Lynparza, AstraZeneca), rucaparib (Rubraca, Clovis Oncology), and niraparib (Zejula, Tesaro),as
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
What's New in Oncodermatopathology: Immunotherapy Reactions
 What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
Precision Genetic Testing in Cancer Treatment and Prognosis
 Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
Precision Genetic Testing in Cancer Treatment and Prognosis Deborah Cragun, PhD, MS, CGC Genetic Counseling Graduate Program Director University of South Florida Case #1 Diana is a 47 year old cancer patient
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Adjuvant treatment in melanoma. María González Cao Servicio Oncología Médica Institut Universitari Dexeus-Quiron. Barcelona Formigal, 24th June 2016
 Adjuvant treatment in melanoma María González Cao Servicio Oncología Médica Institut Universitari Dexeus-Quiron. Barcelona Formigal, 24th June 2016 Charles M. Balch et al. JCO 2009;27:6199-6206 Survival
Adjuvant treatment in melanoma María González Cao Servicio Oncología Médica Institut Universitari Dexeus-Quiron. Barcelona Formigal, 24th June 2016 Charles M. Balch et al. JCO 2009;27:6199-6206 Survival
Proteasome inhibitor (PI) and immunomodulatory drug (IMiD) refractory multiple myeloma is associated with inferior patient outcomes
 and immunomodulatory drug (IMiD) refractory multiple myeloma is associated with inferior patient outcomes") Alliance A061202. A phase I/II study of pomalidomide, dexamethasone and ixazomib versus pomalidomide and dexamethasone for patients with multiple myeloma refractory to lenalidomide and proteasome inhibitor
Alliance A061202. A phase I/II study of pomalidomide, dexamethasone and ixazomib versus pomalidomide and dexamethasone for patients with multiple myeloma refractory to lenalidomide and proteasome inhibitor
Name of Policy: Yervoy (Ipilimumab)
") Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Yervoy (Ipilimumab) Policy #: 335 Latest Review Date: October 2013 Category: Pharmacology Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Innovazioni Terapeutiche In Oncologia Dott. Massimo Ghiani A USL N 8 Ospedale A. Businco Oncologia Medica III. Tarceva TM
 Innovazioni Terapeutiche In Oncologia Dott. Massimo Ghiani A USL N 8 Ospedale A. Businco Oncologia Medica III Tarceva TM Tarceva TM (erlotinib HCl) High-affinity, reversible inhibitor of HER1/EGFR Tyrosine
Innovazioni Terapeutiche In Oncologia Dott. Massimo Ghiani A USL N 8 Ospedale A. Businco Oncologia Medica III Tarceva TM Tarceva TM (erlotinib HCl) High-affinity, reversible inhibitor of HER1/EGFR Tyrosine
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant