Management of 17p Deleted CLL Patients in the Era of Targeted Therapy
|
|
|
- Garey Lucas
- 5 years ago
- Views:
Transcription

1 Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11, 2016
2 Conflict of Interest Disclosure I hereby declare the following potential conflicts of interest concerning my presentation: Consultancy: Janssen, Pharmacyclics, Celgene, Roche/Genentech, Gilead, Infinity, Abbvie, Sun Biopharma Research Funding: Acetylon Discussion of off-label drug use: venetoclax, idelalisib for upfront therapy
3 Overall Survival by FISH Patients surviving (%) Del 17p: 32 m Del 11q: 79 m 17p- 11q- 12q trisomy Normal 13q deletion as sole abnormality Months NEJM 2000;343:1910
4 CLL8: Survival after FCR by FISH 17p deletion +12q 13q-single 11q- Not 17p-/11q-/+12q/13q- 17p- Lancet 2010: 376: 1164
5 CLL8: Impact of TP53 Mutation on OS TP53: wild type mutated Therapy: FCR FC
6 CLL8 Multivariable Analysis: Predictive Factors Cox regression including: FC, FCR, TP53, NOTCH1, SF3B1, and treatment interaction PFS: HR p-value FCR <.001 TP53 mut <.001 SF3B1 mut NOTCH1 mut Interaction OS: HR p-value FCR TP53 mut <.001 NOTCH1 mut Interaction
7 MVA Analysis: Impact of MRD and Clinical Response in CLL8 & COX regression PFS MRD status Univariate comparison 10 HR Lower 95 % CI Upper p value Positive vs. negative < Clinical response PR vs. CR = Deletion 17p Yes vs. no < IgHV analysis Unmutated vs. mutated < 0.001
8 Incidence of Genetic Lesions CLL8: CLL3X:* CLL2H: # 1st Line High-Risk F-refractory (FC vs. FCR) (Allo-SCT) (Alemtuzumab) n=635 n=80 n=97 TP53 mut NOTCH1 mut SF3B1 mut IGHV UM p q *Dreger et al. abstract 966, Tue 8:45, # Schnaiter et al. abstract 710, Mo 4:45
9 Ibrutinib (PCI-32765): BTK Inhibitor O Forms a specific and irreversible bond with cysteine-481 in Btk NH 2 Potent Btk inhibition N N N N IC 50 = 0.5 nm Orally available N O Once daily dosing results in 24-hr sustained target inhibition
10 Phase II in CLL/SLL PCYC-1102-CA 116 patients treated with ibrutinib monotherapy Endpoints: ORR, PFS, OS, Safety, PK/PD Enrolled May 2010 July 2011 Treatment Naïve (TN) 65 yrs 420 mg/d or 840 mg/d ibrutinib (n=31) Median follow-up 20.3 months Relapsed/Refractory (R/R) 420 mg/d or 840 mg/d ibrutinib (n=61) Median follow-up 22.1 months High-risk* Relapsed/Refractory (HR) 420 mg/d ibrutinib (n=24) Median follow-up 14.7 months *High risk defined as progression of disease < 24 months after initiation of a chemoimmunotherapy regimen or failure to respond
11 100% 80% 60% 40% 1102 Best Response (Investigator-Assessed) 90% 84% 89% 7% 11% 23% 1% 3% 80% 74% 55% CR npr PR PR+L SD PD 20% 0% Median DOR in months (range)3 Month 30 (95% CI) 6% 10% 0% 3% 4% 2% 4% 5% 2% TN (n = 31) R/R (n = 101) Total (N = 132) NR (0 to 35.0+) NR (0 to 35.2+) NR (0 to 35.2+) 100.0% (NE) 79.1% (64.2 to 88.4) 85.3 (74.4 to 91.8) 5/6 patients who received prior idelalisib responded to ibrutinib (4PR, 1 PR+L) 2/5 responders continue treatment with one additional patient moving on to SCT O Brien et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7014).
12 1102 PFS by Cytogenetics (FISH) in 1.0 Relapsed/Refractory CLL Progression-Free Survival (Proportion) month PFS Del17p Del11q No del17p/ 11q 45.9% 74.2% 87.0% (95% CI) ( ) ( ) ( ) Median PFS 28.1 mos NR NR del17p del11q No del17p or del11q + Censored Months From Initiation of Study Treatment O Brien et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7014).
13 Overall Survival by Cytogenetics (FISH) in Relapsed/Refractory Population 1.0 Overall Survival (Proportion) del17p del11q No del17p or del11q + Censored Del17p Del11q No del17p/11q 30-month OS 65.9% 84.9% 93.9% (95% CI) ( ) ( ) ( ) Median OS NR NR NR Months From Initiation of Study Treatment O Brien et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 7014).
14 MDACC: EFS on Ibrutinib Del 17p only No complex karyo Thompson et al. Cancer

 Stratification according to: Disease refractory to purine analog chemoimmunotherapy (no response or relapsed within 12 months)")
15 Byrd et al. N Engl J Med Jul 17;371(3): RESONATE Phase 3 Study Design Patients with previously treated CLL/SLL R A N D O M I Z E 1:1 Oral ibrutinib 420 mg once daily until PD or unacceptable toxicity n=195 IV ofatumumab initial dose 300 mg followed by 2000 mg 11 doses over 24 weeks n=196 Crossover to ibrutinib 420 mg once daily after IRC-confirmed PD (n=57) Stratification according to: Disease refractory to purine analog chemoimmunotherapy (no response or relapsed within 12 months) Presence or absence of 17p13.1 (17p del) At time of interim analysis, median time on study was 9.4 months

16 PCYC 1112 RESONATE: PFS by Del17p Brown et al. ASH 2014.
17 PCYC 1112 RESONATE: PFS by Del17p Brown et al. ASH 2014.

18 RESONATE: Characteristics of Patients With Progressive Disease
19 Outcomes of Del(17p) CLL Patients Treated with Ibrutinib (n=243) Del17p by FISH* S T U D Y PCYC-1102 Central laboratory PCYC-1112 Local assessment PCYC-1117 Central laboratory Once-daily ibrutinib 420 mg (n=232) or 840 mg (n=11) until PD or unacceptable toxicity R/R (n=241) TN (n=2) Endpoints ORR*, PFS, and OS Sustained hematologic improvement over baseline Grade 3 adverse events (AEs) of clinical interest PCYC-1102/1103 Complex karyotype outcomes *% of del17p reflected the assay specific definition of positive and negative. ORR includes CR, CRi, PR, npr, and PR-L. Complex karyotype: 3 unrelated chromosomal abnormalities by stimulated cytogenetics as assessed by a reference laboratory. J. Jones et al. EHA Annual Meeting Abstract S429.
 Median duration of response (DOR) not reached at 30 months For patients who achieved CR/CRi (n=23), an estimated 81% maintained response at 30")
20 Overall Response Rate Median time on study, mo (range) 42 (0.9-61) 31 (0.3-37) 28 (0.5-31) 28 (0.3-61) Median duration of response (DOR) not reached at 30 months For patients who achieved CR/CRi (n=23), an estimated 81% maintained response at 30 months J. Jones et al. EHA Annual Meeting Abstract S429.
21 PFS for Patients with Del17p CLL on Ibrutinib Estimated 12- mo PFS, % (95% CI) Estimated 24- mo PFS, % (95% CI) Estimated 30- mo PFS, % (95% CI) 80% (74, 84) 63% (57, 69) 55% (48, 62) Median time on study = 28 months (range: ) J. Jones et al. EHA Annual Meeting Abstract S429.
: 239 days Non-RT (n=53): 582 days PD, progressive disease; RT, Richter s transformation. J. Jones et al. EHA Annual Meeting 2016.")
22 Cumulative Incidence of Richter s Transformation and Other Progression Cumulative incidences similar for RT and other PD in the first year All but 2 RT events occurred in the first 2 years Median time to PD for patients who have progressed RT (n=28): 239 days Non-RT (n=53): 582 days PD, progressive disease; RT, Richter s transformation. J. Jones et al. EHA Annual Meeting Abstract S429.


23 PFS and OS by Lactate Dehydrogenase Levels, Prior Therapies, and Bulky Disease J. Jones et al. EHA Annual Meeting Abstract S429.
24 PFS of Del17p Patients +/- Complex Karyotype in the PCYC-1102/1103 Study Median PFS, mo Del17p + CK (n=22) 25 Del17p no CK (n=10) 52 Median OS, mo Del17p + CK (n=22) 32 Del17p no CK (n=10) NR 69% of del17p patients had CK vs. 31% of del17p patients without CK Median age (range): 65 y (49-79) vs 60 y (44-82) Median prior therapies (range): 4 (1-9) vs 2.5 (0-12) Median platelets (range): 72»10 9 /L (20-151) vs 110»10 9 /L (17-310) Rai stage III-IV: 64% vs 40% CK, complex karyotype; NR, not reached. J. Jones et al. EHA Annual Meeting Abstract S429.
25 OSU, Survival: Progressive CLL v. Richter s Median = 17 months Median = 3.5 months
26 Characteristics of Patients with Identified Mutations at CLL Relapse Patient Age No. Prior Therapies Cytogenetics Study Treatment Duration on Ibrutinib Best Response Identified Mutation del(17p13.1), mg qd 621 days PR C481S BTK del(17p13.1), complex karyotype 420 mg qd 673 days PR R665W PLCγ del(11q22.3) complex karyotype BR x 6 cycles, 420 mg qd Ofatumumab x 24 weeks, 420 mg qd 388 days CR C481S BTK 674 days CR C481S BTK del(17p13.1), complex karyotype 840 mg qd 868 days PR C481S BTK del(17p13.1), complex karyotype Ofatumumab x 24 weeks, 420 mg qd 505 days PR * No mutations identified in kinases with homology at C481 L845F, R665W, S707Y PLCγ2, C481S BTK Woyach et al, NEJM 2014
27 Frontline Ibrutinib in del(17p) 100 Overall Survival Overall Survival (%) Relapsed/Refractory Previously Untreated P = Months Previously Untreated Relapsed Refractory N Median Follow-up 15 months 26 months Rai Stage III/IV 63% 75% Bulky adenopathy IGHV unmutated 23% 50% 63% 75% PFS 82%, OS 80% at 24 mos Farooqui MZ, et al. Lancet Oncol. 2015;16(2):
28 Venetoclax (ABT-199) Response in Response Overall response Relapsed/Refractory CLL/SLL All (n = 116) del(17p) (n = 31) F- Refractory (n = 70) IGHV Unmutated (n = 46) 79% 71% 79% 76% CR 20% 16% 16% 17% PR 59% 55% 63% 59% Bulky nodes (>5 cm) N CR/CRi % (95% CI) ORR % (95% CI) Yes 67 6 (2, 15) 78 (66, 87) No (24, 53) 83 (70, 93) Roberts AW, et al. N Engl J Med Online ahead of print.
29 Venetoclax (ABT-199) in Relapsed/Refractory CLL/SLL Roberts AW, et al. N Engl J Med Online ahead of print.


30 Detailed Risk Stratification of Patients for Tumor Lysis 2014 EHA Annual Meeting, Poster
31 Venetoclax in High-Risk R/R CLL with del17p: Baseline Characteristics Characteristic, n (%) N=107 a (%) Age, years Median, range 67, Sex Male 70 (65) Prior therapies Median, range 2, 1 10 Prior bendamustine / refractory 54 (50) / 38 (70) Prior fludarabine / refractory 78 (73) / 34 (44) Bulky nodes One or more nodes 5 cm 57 (53) Absolute lymphocyte count 25 x 10 9 /L 54 (51) Low 19 (18) TLS risk category Medium 43 (40) High 45 (42) Rai stage III or IV 51(48) IGHV Unmutated 30 (81) Stilgenbauer et al., ASH 2015 (abstract LBA-6, oral presentation)
32 Venetoclax in R/R CLL with 17p del iwcll Response (74%) MRD-negativity Median time-to-first response: 0.8 months ( ) Median time to CR/Cri (16%): 8.2 months ( ) Of 45 patients tested, 18 achieved MRD-negativity in peripheral blood Stilgenbauer S et al, Blood 2015; 126(23): LBA-6.
33 Del 17p CLL: Durability of Venetoclax Activity Duration of Response (N=85) PFS and OS (N=107) 12-month estimates: All responders: 84.7% CR/CRi/nPR: 100% 12-month estimates (95% CI): PFS: 72.0% (61.8, 79.8) OS: 86.7% (78.6, 91.9) MRD-negative: 94.4% Stilgenbauer et al, ASH 2015
34 Venetoclax after Failure of Ibrutinib Characteristic Ibrutinib Arm n=41 Idelalisib Arm n=13 Median age, years (range) 67 (48 80) 69 (56 75) Male, n (%) 31 (76) 9 (69) Prior therapies Median (range) 5 (1 12) a 3 (1 9) b Prior ibrutinib, n (%) 41 (100) 3 (23) Median months (range) on ibrutinib 16 (1 56) 5 (2 10) Prior idelalisib, n (%) 3 (7) 13 (100) Median months (range) on idelalisib 10 (2 31) 10 (1 27) Intolerant to prior ibrutinib/idelalisib 11 (27) 6 (38) As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.
35 Disease Burden and Biologic Disease Burden at Study Entry, n (%) ALC Characteristics Ibrutinib Arm n=41 Idelalisib Arm n=13 25 x 10 9 /L 16 (39) 5 (39) Bulky disease 1 or more nodes >5 cm 14 (34) 7 (54) 1 or more nodes >10 cm 8 (20) 5 (39) Prognostic Factors, n/n (%) IGHV unmutated 24/28 (86) 6/8 (75) del(17)(p13.1) 19/39 (46) 0/13 (0) del(11)(q22.3) 12/41 (29) 3/13 (23) TP53 mutation 14/39 (36) 0/12 (0) As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.
 23/31 (74) 5/9 (56) Median time to 50% reduction in nodal masses, days (range) 50 (44 162) 50 (49 52) As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.")
36 Best Percent Change from Baseline in Nodal Mass by CT Scan Ibrutinib Arm n=41 Idelalisib Arm n=13 Assessed, post baseline CT or MRI scans, n (%) 31 (76) 9 (69) Achieved 50% reduction in nodal masses, n/n (%) 23/31 (74) 5/9 (56) Median time to 50% reduction in nodal masses, days (range) 50 (44 162) 50 (49 52) As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.



37 Best Objective Responses To Date Ibrutinib Arm (Up to Week 36) Idelalisib Arm 61% ORR a 3 CR 1 npr 19 PR b 50% ORR a 5 PR a Patients who have not reached assessment were not included in best objective response rate calculation b 2 subsequently progressed after achieving a PR at Week 24: 1 Richter s Transformation at Week 30 and 1 CLL progression at Week 32 As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.
 Partial response 20 (53) 11 (48) Stable disease 13 (34) 3 (13) Disease progression 1 (3) 2 (9) D/C prior to assessment 4 (10) 4 (17) As of August 25, 2015 Jones JA et al.")
38 Venetoclax after Failure of Ibrutinib: Response at Weeks 8 & 24 Median 19 wks on venetoclax in the ibrutinib arm N=41 Week 8 Week 24 Assessed, n Not yet assessed 3 18 Overall Response, n (%) Complete response 0 3 (13) Partial response 20 (53) 11 (48) Stable disease 13 (34) 3 (13) Disease progression 1 (3) 2 (9) D/C prior to assessment 4 (10) 4 (17) As of August 25, 2015 Jones JA et al. Blood 2015; 126(23): 715.
39 Survival after Failure of Venetoclax 70 patients enrolled in Australia ( ) M : Venetoclax Monotherapy (Phase I) M : Venetoclax + Rituximab (Phase I) M : Venetoclax Monotherapy (Phase II, del(17p) CLL) 28 patients discontinued venetoclax: 16 (57%) Richter Transformation 7 (25%) CLL progression 5 (18%) other reasons Median 7.5 mos on venetoclax and 12 months (0 34) follow-up after discontinuation Median 4 prior regimens, 59% del 17p
40 Survival After Discontinuation of Venetoclax CLL (n=7), 1y OS 69% RS (n=16), 1y OS 48% Median OS 1 year CLL vs RS, p=0.88 Others (n=5) Months




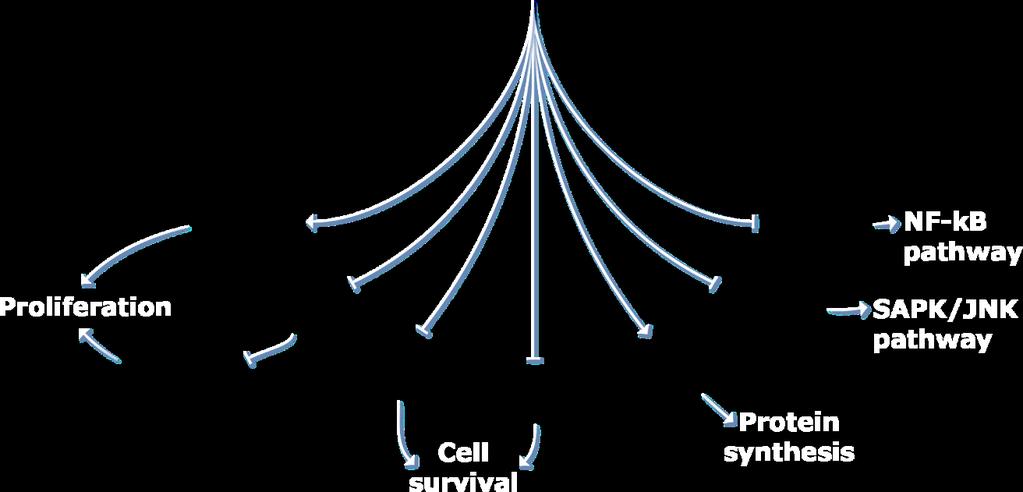




41 PI3K Signaling Pathway as a Target in B Cells
42 GILEAD 116: PFS, Including Extension Study* Idelalisib + R vs Placebo + R All Patients Progression-free Survival (% ) Idelalisib + R (N=110) Placebo + R (N=110) N at risk Time (months) IDELA + R PBO + R Median PFS (95% CI) HR (95% CI) p-value IDELA + R 19.4 mo (16.6, ) PBO + R 7.3 mo (5.5, 8.5) 0.25 (0.16, 0.39) < *Placebo + R includes those patients who received open-label idelalisib after unblinding without prior progression (n=42). Blood 2014; 124: 330
 Del17p/TP53mut (n=46) 0 2 4 6 8 10 12 14 16 18 20 22 24 26 Time (months) N at risk Mutated 19 18 18 18 17 12 9 5 3 2 1 0")
43 PFS Subgroup Analysis* Idelalisib + R (N=110) IGHV: Unmutated vs Mutated Del17p/TP53mut: Present vs Not Present Progression-free Survival (% ) Mutated (n=19) Unmutated (n=91) No del17p/tp53mut (n=64) Del17p/TP53mut (n=46) Time (months) N at risk Mutated Unmut Time (months) No del Del Median PFS (95% CI) p-value Median PFS (95% CI) p-value Mut NR (10.7, ) Unmut 19.4 mo (16.6, ) 0.75 No del 20.3 mo (19.4, ) Del 16.6 mo (13.9, ) 0.94 *Including extension study Blood 2014; 124: 330
44 GILEAD 115: BR-Idela vs BR IRC-Assessed PFS Study 115: Primary Endpoint Probability of PFS (%) Probability of PFS IDELA + BR BR + Placebo IDELA + BR BR + Placebo Median PFS (mo) HR (95% CI) 0.33 (0.24, 0.45) p-value < Median follow-up time = 12 mont No. at risk (events) Time (months) IDELA + BR 207 (0) 154 (25) 74 (51) 27 (61) 6 (63) 1 (64) BR + Placebo 209 (0) 145 (46) 36 (111) 11 (126) 1 (131) 0 (132) HR, hazard ratio; IRC, independent review committee. Zelenetz et al., ASH 2015 Abstract LBA-5
45 Results: Overall Survival Study 115: Secondary Endpoint 100 Probability of Survival (%) Probability of PFS IDELA + BR BR + Placebo No. of deaths (%) 34 (16.4) 51 (24.4) Median OS (mo) NR NR HR (95% CI) 0.55 (0.36, 0.86) p-values = (stratified) and (unstratified) IDELA + BR BR + Placebo No. at risk (events) Time (months) IDELA + BR 207 (0) 181 (14) 104 (27) 52 (30) 13 (33) 1 (34) BR + Placebo 209 (0) 180 (20) 93 (35) 33 (47) 8 (51) 0 (51) Zelenetz et al., ASH 2015 Abstract LBA-5
46 (New) Safety Information (March 2016) + Idela Control *Idela +/- BR Untreated CLL *Idela +/- R Prev treated NHL *Idela +/- BR Prev treated NHL N= % death N= % death Idela +/- R 2-3 prior therapies CLL Idela +/- Ofa 2-3 prior therapies CLL N= % death N= % death Idela +/- BR 2-3 prior therapies CLL
47 Infection Risk Already Known Median Prior Therapies DFCI Initial Therapy Initial Therapy Overall Relapsed Phase I (2-3) 5 Gr 3-4 ANC 29% 28% / 22% 43% Febrile neutropenia Grade 3-4 Infection Opportunistic Infns 3% / 5% 11.1% 13% 17% / 17% 31.6% 5.6% PsA bacteremia 2 PJP 1 fungal 1 CMV 1 brain abscess Most PJP / CMV on combo studies with BR No PJP or CMV on 116 or 119 studies; a few on PJP 2 fungal 1 CMV
48 Idelalisib + Rituximab in 65 Years Median time on therapy 22.4 months 97% ORR, 19% CR PFS 83% at 36 months 9 patients with del(17p)/tp53 mutation 100% ORR, 33% CR O Brien S, et al. Blood. 2015; 126(25):
49 Idelalisib + R in Untreated CLL Over 65: All Cause AEs 25% Adverse Event n (%) with any Grade n (%) with Grade 3 Diarrhea** 35 (64) 15 (42) Pyrexia 27 (42) 2 (3) Nausea 24 (38) 1 (2) Rash 37 (58) 8 (13) Chills 23 (36) 0 (0) Cough 21 (33) 1 (2) Fatigue 20 (31) 0 (0) Pneumonia 18 (28) 12 (19) **10 patients reported as Gr 3 colitis, including 6 lacking any AE report of Gr 3 diarrhea Med time to Gr 3 diarrhea/colitis = 9 mos Lab Abnormality* n (%) with Increase to Grade 3 Transaminase elevations 15 (23) Neutropenia 18 (28) Anemia 2 (3) Thrombocytopenia 1 (2) O Brien S, et al. Blood. 2015; 126(25):
50 Grade 3 4 Immune Tox More Common in Median Prior Therapies Less Pretreated Patients Phase I 3 Overall Relapsed 2 Initial Therapy 1 Upfront idela + ofa 5 1 (2-3) 0 0 Diarrhoea/Colitis 5.6% 14% 42% 13% Transaminitis 2% 14% 23% 52% Pneumonitis 5.6% 3% (6% pneumonitis/ fibrosis) 13% Rash 0 5% 13% 13% 1. O Brien SM et al. Poster 1994 presented at ASH 2014; 2. Coutré SE et al. Oral presentation at EHA 2015: S433.OI: / ; 3. Brown JR et al. Blood 2014;123:
51 Summary: Idelalisib Highly active in R/R (and untreated) CLL Extends PFS and OS in high risk relapsed patients No difference based on IGHV or 17p status Several categories of toxicity: Autoimmune: transaminitis, diarrhea /colitis, and pneumonitis Neutropenia and sepsis (primary cause of infectious deaths on recently halted upfront trials): not as common without BR, monitor closely and use growth factor Opportunistic infections previously described: PJP, CMV Prophylaxis mandatory for PJP, VZV, neutropenia CMV monitoring when febrile Idelalisib should not be used in the upfront setting (unless absolutely necessary) Limited data on response after ibrutinib
52 PFS by Ibrutinib vs Idelalisib (first KI)
53 PFS for Alternate KI by Discontinuation Reason RT excluded from analysis
54 Where Are We with 17p Deleted CLL? Three very active classes of drugs Start with ibrutinib, follow with venetoclax or PI3K Duration of ibrutinib response is still shorter than without del 17p : as little as 28 mos Efficacy of sequencing single agents is unknown To achieve durable responses, combinations are certainly needed, but no data yet

55 Allogeneic SCT for CLL in the Era of Novel Agents 2014 by American Society of Hematology Peter Dreger et al. Blood 2014;124:
56 Outcomes RIC SCT in CLL GCLLSG MDACC Seattle DFCI CLL3X N Conditioning FC-based +/- FCR mostly 2 GyTBI + F FB ATG PFS 42% yrs 4 yrs yrs yrs OS 65% 51% 41% 62% NRM 23% 17% 32% 18% Relapse 40% 39% 36% 40% Key Poor Prognostic Factors -CD4 < 100 -Low serum IgG Uncontrolled disease at SCT -Alem TCD -LNs >= 5 cm -Alem w/in 12 mos Uncontrolled disease -SCT pre DFCI % at 5 yrs 83% 9.5% 26%
57 DFCI CLL SCT: PFS pre and post 2004 Probability RIC, >=2004 _ RIC, < MAC, >= MAC, <2004 RIC Years from Transplantation Leukemia epub


58 TP53, SF3B1, and NOTCH1 Mutations and Outcome of Allotransplantation Dreger et al. Blood 2013: 121 (16);
59 Who Should Have SCT in the Era of BCR Inhibitors? del 17p patients, potentially in first remission (if post ibrutinib) but definitely in any later remission (especially if you are running out of known active agents or cannot access them) Progressors on ibrutinib?? Progressors on idelalisib vs venetoclax: Less clear, may have prolonged remission with ibrutinib
60 Issues with Considering SCT after Novel Agents Remissions are not deep, often insufficient to be optimal for SCT Time to recurrence after stopping the drug can be short Waiting for relapse may be too late due to fulminant relapse With current single agents, venetoclax is by far best for prepping a patient for transplant How to avoid resistance and/or better prepare for SCT? Combination therapy : potential for deeper remissions (ideally MRD negative) that may allow breaks, which will reduce selective pressure for resistance, or allow for SCT for consolidation
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients
 MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Management of CLL in the Targeted Therapy Era
 Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Chronic Lymphocytic Leukemia. Paolo Ghia
 Chronic Lymphocytic Leukemia Paolo Ghia Complex Karyotype: a novel predictive marker? Thompson PA et al. Cancer 2015 Complex karyotype superseded del(17p) Anderson MA et al. Blood 2017 Ibrutinib and Idela
Chronic Lymphocytic Leukemia Paolo Ghia Complex Karyotype: a novel predictive marker? Thompson PA et al. Cancer 2015 Complex karyotype superseded del(17p) Anderson MA et al. Blood 2017 Ibrutinib and Idela
Advances in CLL 2016
 Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD
: Refresher Course for Hematologists Ekarat Rattarittamrong, MD") Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
FCR and BR: When to use, how to use?
 FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division
 Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Chronic lymphocytic Leukemia
 Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
Management of Chronic Lymphatic Leukemia Beyond conventional therapy
 3 rd Young Hematologists Orientation Program SGPGI Lucknow August 18 th -19 th 218 Management of Chronic Lymphatic Leukemia Beyond conventional therapy Prof. Hari Menon. MD DM Department of Hemato-Oncology
3 rd Young Hematologists Orientation Program SGPGI Lucknow August 18 th -19 th 218 Management of Chronic Lymphatic Leukemia Beyond conventional therapy Prof. Hari Menon. MD DM Department of Hemato-Oncology
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT
 We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
CLL: future therapies. Dr. Nathalie Johnson
 CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
DFCR. Dept. of Medical Oncology, Dana-Farber Cancer Institute 2. Dept. of Medical Oncology, Beth Israel Deaconess Medical Center Boston, USA
 A Phase IB/II Study of Duvelisib in Combination with FCR (DFCR) For Frontline Therapy for Younger CLL Patients DFCR Matthew S. Davids, MD, MMSc 1, David C. Fisher, MD 1, Svitlana Tyekucheva, PhD 1, Haesook
A Phase IB/II Study of Duvelisib in Combination with FCR (DFCR) For Frontline Therapy for Younger CLL Patients DFCR Matthew S. Davids, MD, MMSc 1, David C. Fisher, MD 1, Svitlana Tyekucheva, PhD 1, Haesook
LEUCEMIA LINFATICA CRONICA: TERAPIA DEL PAZIENTE IN RECIDIVA
 CORSO TEORICO-PRATICO PER LA GESTIONE OTTIMALE DEI PAZIENTI AFFETTI DA LINFOMA MANTELLARE, LINFOMA FOLLICOLARE E LEUCEMIA LINFATICA CRONICA Torino, 21-23 Maggio 2018 LEUCEMIA LINFATICA CRONICA: TERAPIA
CORSO TEORICO-PRATICO PER LA GESTIONE OTTIMALE DEI PAZIENTI AFFETTI DA LINFOMA MANTELLARE, LINFOMA FOLLICOLARE E LEUCEMIA LINFATICA CRONICA Torino, 21-23 Maggio 2018 LEUCEMIA LINFATICA CRONICA: TERAPIA
1. What to test. 2. When to test
 Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Impact of CLL biological features on
Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Biomarkers: the triad of questions 1. What to test 2. When to test 3. Who to test Impact of CLL biological features on
L approccio terapeu-co. Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro
 L approccio terapeu-co Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro DISCLOSURE Nome: Maria Rosaria Cognome: Villa Impiego nell industria farmaceu7ca negli ul7mi 5 anni: NO Interssi
L approccio terapeu-co Maria Rosaria Villa U.O.C. Ematologia P.O. Ascalesi ASLNA1Centro DISCLOSURE Nome: Maria Rosaria Cognome: Villa Impiego nell industria farmaceu7ca negli ul7mi 5 anni: NO Interssi
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia
, a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia") Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
15 th Annual Miami Cancer Meeting
 15 th Annual Miami Cancer Meeting CLL and CML Mohamed A. Kharfan-Dabaja, MD, MBA, FACP Director, Blood and Marrow Transplantation and Cellular Therapies Mayo Clinic Jacksonville, FL 15 th Annual Miami
15 th Annual Miami Cancer Meeting CLL and CML Mohamed A. Kharfan-Dabaja, MD, MBA, FACP Director, Blood and Marrow Transplantation and Cellular Therapies Mayo Clinic Jacksonville, FL 15 th Annual Miami
Chronic Lymphocytic Leukemia: State of the Art
 14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
CLL - venetoclax. Peter Hillmen St James s University Hospital Leeds 10 th May 2016
 CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy
 New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
New Evidence reports on presentations given at ASH 2009 Improving Response to Treatment in CLL with the Addition of Rituximab and Alemtuzumab to Chemoimmunotherapy From ASH 2009: Chronic Lymphocytic Leukemia
CLL treatment algorithm and state of the art
 CLL treatment algorithm and state of the art Davide Rossi, M.D., Ph.D. Hematology IOSI - Oncology Institute of Southern Switzerland IOR - Institute of Oncology Research Bellinzona - Switzerland CLL subgroups
CLL treatment algorithm and state of the art Davide Rossi, M.D., Ph.D. Hematology IOSI - Oncology Institute of Southern Switzerland IOR - Institute of Oncology Research Bellinzona - Switzerland CLL subgroups
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Chronic lymphocytic leukemia. E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015
 Chronic lymphocytic leukemia E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015 Disclosures Travelling to ASH: Roche Consulting services: Janssen Questions in CLL: answers
Chronic lymphocytic leukemia E. Van Den Neste Cliniques UCL Saint-Luc, Brussels Post-ASH meeting January 2015 Disclosures Travelling to ASH: Roche Consulting services: Janssen Questions in CLL: answers
Chronic lymphocytic leukemia
 Chronic lymphocytic leukemia Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2017 Disclosures Speaker
Chronic lymphocytic leukemia Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2017 Disclosures Speaker
Emerging Treatments and Evolving Pathways for the Management of Chronic Lymphocytic Leukemia
 Emerging Treatments and Evolving Pathways for the Management of Chronic Lymphocytic Leukemia This educational activity is supported by an educational grant from AbbVie Faculty Jennifer R Brown, MD PhD
Emerging Treatments and Evolving Pathways for the Management of Chronic Lymphocytic Leukemia This educational activity is supported by an educational grant from AbbVie Faculty Jennifer R Brown, MD PhD
Post-ASH 2015 Chronic Lymphocytic Leukaemia. Anna Schuh Consultant Haematologist Oxford
 Post-ASH 2015 Chronic Lymphocytic Leukaemia Anna Schuh Consultant Haematologist Oxford NEWS IN FRONT-LINE Consort Diagram CLL10 Study: FCR VS BR in Front-line 688 CLL patients screened centrally for: immunophenotype
Post-ASH 2015 Chronic Lymphocytic Leukaemia Anna Schuh Consultant Haematologist Oxford NEWS IN FRONT-LINE Consort Diagram CLL10 Study: FCR VS BR in Front-line 688 CLL patients screened centrally for: immunophenotype
Outcomes of patients with CLL after discontinuing idelalisib
 Outcomes of patients with CLL after discontinuing idelalisib Jacqueline C. Barrientos, Manmeen Kaur, Alexis Mark, Jaewon Chung, Nancy Driscoll, Alison Bender, Kanti R. Rai ASH Annual Meeting Abstracts
Outcomes of patients with CLL after discontinuing idelalisib Jacqueline C. Barrientos, Manmeen Kaur, Alexis Mark, Jaewon Chung, Nancy Driscoll, Alison Bender, Kanti R. Rai ASH Annual Meeting Abstracts
Advances in the treatment of Chronic Lymphocytic Leukemia
 Advances in the treatment of Chronic Lymphocytic Leukemia Lab of B Cell Neoplasia - Division of Experimental Oncology Strategic Research Program on CLL Department of Onco-Hematology Università Vita-Salute
Advances in the treatment of Chronic Lymphocytic Leukemia Lab of B Cell Neoplasia - Division of Experimental Oncology Strategic Research Program on CLL Department of Onco-Hematology Università Vita-Salute
CLL: Future Therapies. Dr. Anca Prica
 CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances
 Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances 2017 Master Class Course John C. Byrd, MD D Warren Brown Chair of Leukemia Research Distinguished University
Chronic Lymphocytic Leukemia: Prognostic Factors, Supportive Care Issues and Therapeutic Advances 2017 Master Class Course John C. Byrd, MD D Warren Brown Chair of Leukemia Research Distinguished University
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
Chronic lymphocytic leukemia
 Chronic lymphocytic leukemia How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2018 Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA DISCLOSURES I am on
Chronic lymphocytic leukemia How the Experts Treat Hematologic Malignancies Las Vegas, NV 3/2018 Tanya Siddiqi, MD Assistant Professor City of Hope National Medical Center Duarte, CA DISCLOSURES I am on
Clinical Overview: MRD in CLL. Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel
 Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
LEUCEMIA LINFATICA CRONICA
 LEUCEMIA LINFATICA CRONICA Gianluca Gaidano SCDU Ematologia Dipartimento di Medicina Traslazionale Università del Piemonte Orientale Novara Outline CLL biology and pathogenesis Prognostication and prediction
LEUCEMIA LINFATICA CRONICA Gianluca Gaidano SCDU Ematologia Dipartimento di Medicina Traslazionale Università del Piemonte Orientale Novara Outline CLL biology and pathogenesis Prognostication and prediction
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Chronic Lymphocytic Leukemia Update. Learning Objectives
 Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Chronic Lymphocytic Leukemia: State of the Art
 14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
BTK Inhibitors and BCL2 Antagonists
 BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
CHRONIC LYMPHOCYTIC LEUKEMIA
 CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: January, 2017 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted
CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: January, 2017 The recommendations contained in this guideline are a consensus of the Alberta Provincial Hematology Tumour Team synthesis of currently accepted
Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto)
 and Dr. Matt Cheung (Staff Hematologist, University of Toronto)") CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
allosct and CLL in the BCRi era time for a study
 allosct and CLL in the BCRi era time for a study Patient characteristics in BCRi studies and allosct candidates DIFFER Facts on BCRi no Cure Risk factors for shorter BCRi efficacy in MV analysis? PA-refractory
allosct and CLL in the BCRi era time for a study Patient characteristics in BCRi studies and allosct candidates DIFFER Facts on BCRi no Cure Risk factors for shorter BCRi efficacy in MV analysis? PA-refractory
Update: Chronic Lymphocytic Leukemia
 ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
What s on the Horizon for Chronic Lymphocytic Leukemia?
 What s on the Horizon for Chronic Lymphocytic Leukemia? Matthew S. Davids, MD, MMSc Associate Director Center for Chronic Lymphocytic Leukemia Assistant Professor of Medicine Harvard Medical School Dana
What s on the Horizon for Chronic Lymphocytic Leukemia? Matthew S. Davids, MD, MMSc Associate Director Center for Chronic Lymphocytic Leukemia Assistant Professor of Medicine Harvard Medical School Dana
ASH up-date: Changing the Standard of Care for Patients with. (or: Who to treat with What When?)
") ASH up-date: Changing the Standard of Care for Patients with B-cell Chronic Lymphocytic Leukaemia (or: Who to treat with What When?) Dr Anna Schuh, MD, PhD, MRCP, FRCPath Consultant and Senior Lecturer
ASH up-date: Changing the Standard of Care for Patients with B-cell Chronic Lymphocytic Leukaemia (or: Who to treat with What When?) Dr Anna Schuh, MD, PhD, MRCP, FRCPath Consultant and Senior Lecturer
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Update on Management of CLL. Presenter Disclosure Information. Chronic Lymphocytic Leukemia. Audience Response Question?
 Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Department of Medicine, Division of Hematology-Oncology, Weill Cornell Medical College, New York, NY 3
 The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
Leukemia. Roland B. Walter, MD PhD MS. Fred Hutchinson Cancer Research Center University of Washington
 Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Idelalisib given front-line for the treatment of CLL results in frequent and severe immune-mediated toxicities
 Idelalisib given front-line for the treatment of CLL results in frequent and severe immune-mediated toxicities Benjamin L. Lampson, Tiago R. Matos, Siddha N. Kasar, Haesook Kim, Elizabeth A. Morgan, Laura
Idelalisib given front-line for the treatment of CLL results in frequent and severe immune-mediated toxicities Benjamin L. Lampson, Tiago R. Matos, Siddha N. Kasar, Haesook Kim, Elizabeth A. Morgan, Laura
Quando e se è possibile e u/le o0enere una remissione completa
 Quando e se è possibile e u/le o0enere una remissione completa 1) Clinical heterogeneity Disease characteris:cs Pa:ent characteris:cs 2) Modern chemoimmunotherpy approaches 3) New mechanism- based treatment
Quando e se è possibile e u/le o0enere una remissione completa 1) Clinical heterogeneity Disease characteris:cs Pa:ent characteris:cs 2) Modern chemoimmunotherpy approaches 3) New mechanism- based treatment
Management of Patients With Relapsed Chronic Lymphocytic Leukemia
 Management of Patients With Relapsed Chronic Lymphocytic Leukemia Polina Shindiapina, MD, PhD, and Farrukh T. Awan, MD Abstract The management of chronic lymphocytic leukemia (CLL) has improved significantly
Management of Patients With Relapsed Chronic Lymphocytic Leukemia Polina Shindiapina, MD, PhD, and Farrukh T. Awan, MD Abstract The management of chronic lymphocytic leukemia (CLL) has improved significantly
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
CLL Ireland Information Day Presentation
 CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
CLL Ireland Information Day Presentation 5 May 2018 Professor Patrick Thornton Consultant Haematologist, Senior Lecturer RCSI, and Clinical Director Hermitage Medical Clinic Laboratory Chronic Lymphocytic
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL. Michael Hallek University of Cologne
 Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL Michael Hallek University of Cologne 100 90 80 70 60 Substantial progress in CLL therapy in one decade 50 40 complete remissions
Risikoprofil-gesteuerte, individualisierte Therapiestrategien bei der CLL Michael Hallek University of Cologne 100 90 80 70 60 Substantial progress in CLL therapy in one decade 50 40 complete remissions
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Apply recent clinical research findings with the newly FDA-approved combination of obinutuzumab and chlorambucil to the management and care of patients with previously
CME Information LEARNING OBJECTIVES Apply recent clinical research findings with the newly FDA-approved combination of obinutuzumab and chlorambucil to the management and care of patients with previously
CHRONIC LYMPHOCYTIC LEUKEMIA
 CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
CHRONIC LYMPHOCYTIC LEUKEMIA Effective Date: June, 2018 Copyright (2018) Alberta Health Services This material is protected by Canadian and other international copyright laws. All rights reserved. This
The International Peer-Reviewed Journal for The the International Practicing Oncologist/Hematologist. Other Advances in Leukemia/MDS ALL AML MDS
 The Oncologist The International Peer-Reviewed Journal for The the International Practicing Oncologist/Hematologist Peer-Reviewed Journal for the Practicing Oncologist/Hematologist 20 th Anniversary Overview
The Oncologist The International Peer-Reviewed Journal for The the International Practicing Oncologist/Hematologist Peer-Reviewed Journal for the Practicing Oncologist/Hematologist 20 th Anniversary Overview
UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD
 UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD DISCLOSURE Speaker s bureau: Pharmacyclics, Janssen, Seattle Genetics, Astra Zeneca Consultant: Juno therapeutics, Astra Zeneca, BeiGene, Pharmacyclics
UPDATES IN CHRONIC LYMPHOCYTIC LEUKEMIA TANYA SIDDIQI, MD DISCLOSURE Speaker s bureau: Pharmacyclics, Janssen, Seattle Genetics, Astra Zeneca Consultant: Juno therapeutics, Astra Zeneca, BeiGene, Pharmacyclics
CLL Biology and Initial Management. Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology
 CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
CLL Biology and Initial Management Gordon D. Ginder, MD Director, Massey Cancer Center Lipman Chair in Oncology CLL- Epidemiology Most common adult leukemia 25-30% in western world Incidence in US 4.5
Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria
 Chronic lymphocytic Leukemia Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria georg.hopfinger@wgkk.at CLL Diagnosis and Staging Risk Profile Assessment
Chronic lymphocytic Leukemia Georg Hopfinger 3. Med.Abt and LBI for Leukemiaresearch and Haematology Hanusch Krankenhaus,Vienna, Austria georg.hopfinger@wgkk.at CLL Diagnosis and Staging Risk Profile Assessment
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Defining the New Treatment Paradigm for Patients With Chronic Lymphocytic Leukemia
 Defining the New Treatment Paradigm for Patients With Chronic Lymphocytic Leukemia Mollie Moran, CNP The James Cancer Hospital at The Ohio State University Jeffrey Jones, MD/MPH Ohio State University Comprehensive
Defining the New Treatment Paradigm for Patients With Chronic Lymphocytic Leukemia Mollie Moran, CNP The James Cancer Hospital at The Ohio State University Jeffrey Jones, MD/MPH Ohio State University Comprehensive
2015 Oncology Annual Meeting in Chicago. prime Downloadable Slides in Chronic Lymphocytic Leukemia and Indolent Non-Hodgkin Lymphoma.
 2015 Oncology Annual Meeting in Chicago prime Downloadable Slides in Chronic Lymphocytic Leukemia and Indolent Non-Hodgkin Lymphoma May 29-June 2 Ibrutinib Combined With Bendamustine and Rituximab in Previously
2015 Oncology Annual Meeting in Chicago prime Downloadable Slides in Chronic Lymphocytic Leukemia and Indolent Non-Hodgkin Lymphoma May 29-June 2 Ibrutinib Combined With Bendamustine and Rituximab in Previously
Sequencing of chronic lymphocytic leukemia therapies
 CHRONIC LYMPHOCYTIC LEUKEMIA Sequencing of chronic lymphocytic leukemia therapies Jacqueline C. Barrientos CLL Research and Treatment Program, Department of Internal Medicine, Hofstra Northwell School
CHRONIC LYMPHOCYTIC LEUKEMIA Sequencing of chronic lymphocytic leukemia therapies Jacqueline C. Barrientos CLL Research and Treatment Program, Department of Internal Medicine, Hofstra Northwell School
Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation
 Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation Dr. med. Petra Langerbeins Universitätsklinik Köln Deutsche CLL Studiengruppe (DCLLSG) OFFENLEGUNG
Aktuelle Therapiestandards und neue Entwicklungen bei der CLL Primärtherapie und Risikostratifikation Dr. med. Petra Langerbeins Universitätsklinik Köln Deutsche CLL Studiengruppe (DCLLSG) OFFENLEGUNG
GVHD & GVL in the lymphoma setting: The case of CLL
 GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
GVHD & GVL in the lymphoma setting: The case of CLL Peter Dreger Dept. Internal Medicine V University of Heidelberg EBMT: SCT for CLL 2000-2010 Update January 2012 allo auto 400 350 300 250 200 150 100
Media Inquiries: Satu Glawe Phone: Bernadette King Phone:
 Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
State of the Art Treatment for Relapsed Mantle Cell Lymphoma
 Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
NASDAQ: TGTX Jefferies Healthcare Conference June 2015
 NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Is there a place for allogeneic stem cell transplantation in chronic lymphocytic leukaemia in the era of the new molecules?
 185 Is there a place for allogeneic stem cell transplantation in chronic lymphocytic leukaemia in the era of the new molecules? D. Selleslag, MD SUMMARY Allogeneic stem cell transplantation can cure about
185 Is there a place for allogeneic stem cell transplantation in chronic lymphocytic leukaemia in the era of the new molecules? D. Selleslag, MD SUMMARY Allogeneic stem cell transplantation can cure about
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth
 Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth") VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, Chronic Lymphocytic Leukemia. Paolo Ghia
 CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013 Chronic Lymphocytic Leukemia Paolo Ghia CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013
CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013 Chronic Lymphocytic Leukemia Paolo Ghia CLL: MRD as a Surrogate Endpoint for Clinical Trials White Oak February 27, 2013
Presented at the 60th Annual ASH Meeting and Exposition December 1 4, 2018 San Diego, CA
 Phase I/II Study of Umbralisib (TGR-1202) in Combination with Ublituximab (TG-1101) and Pembrolizumab in Patients with Relapsed/ CLL and Richter s Transformation Anthony R. Mato, MD MSCE 1, Jakub Svoboda,
Phase I/II Study of Umbralisib (TGR-1202) in Combination with Ublituximab (TG-1101) and Pembrolizumab in Patients with Relapsed/ CLL and Richter s Transformation Anthony R. Mato, MD MSCE 1, Jakub Svoboda,
Richter s Syndrome: Risk, Predictors and Treatment
 Richter s Syndrome: Risk, Predictors and Treatment 10/23/2015 John N. Allan MD Assistant Professor of Medicine Division of Hematology and Medical Oncology CLL Research Center Weill Cornell Medicine Agenda
Richter s Syndrome: Risk, Predictors and Treatment 10/23/2015 John N. Allan MD Assistant Professor of Medicine Division of Hematology and Medical Oncology CLL Research Center Weill Cornell Medicine Agenda
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
NASDAQ: TGTX. 33 rd Annual JP Morgan Healthcare Conference
 NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX. J.P. Morgan Healthcare Conference January 2017
 NASDAQ: TGTX J.P. Morgan Healthcare Conference January 2017 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX J.P. Morgan Healthcare Conference January 2017 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Results from the Phase 3 DUO. of Duvelisib vs Ofatumumab in Relapsed/Refractory CLL/SLL
 Results from the Phase 3 DUO TM Study of Duvelisib vs Ofatumumab in Relapsed/Refractory CLL/SLL Ian Flinn 1, Peter Hillmen 2, Marco Montillo 3, Zsolt Nagy 4, Árpád Illés 5, Gabriel Etienne 6, Julio Delgado
Results from the Phase 3 DUO TM Study of Duvelisib vs Ofatumumab in Relapsed/Refractory CLL/SLL Ian Flinn 1, Peter Hillmen 2, Marco Montillo 3, Zsolt Nagy 4, Árpád Illés 5, Gabriel Etienne 6, Julio Delgado
Debate Examining Controversies in the Front-line Management of CLL: Chemo-immunotherapy vs. Continuous TKI Therapy
 Debate Examining Controversies in the Front-line Management of CLL: Chemo-immunotherapy vs. Continuous TKI Therapy Steven Coutre, MD Stanford Cancer Institute William G. Wierda, MD, PhD The University
Debate Examining Controversies in the Front-line Management of CLL: Chemo-immunotherapy vs. Continuous TKI Therapy Steven Coutre, MD Stanford Cancer Institute William G. Wierda, MD, PhD The University
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib
Role of Targeted Therapies in the Management of Chronic Lymphocytic Leukemia: From Clinical Data to Individualized Care Ryan Jacobs, MD
 Role of Targeted Therapies in the Management of Chronic Lymphocytic Leukemia: From Clinical Data to Individualized Care Ryan Jacobs, MD Department of Hematology Levine Cancer Institute Carolinas Health
Role of Targeted Therapies in the Management of Chronic Lymphocytic Leukemia: From Clinical Data to Individualized Care Ryan Jacobs, MD Department of Hematology Levine Cancer Institute Carolinas Health
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia
 Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies
 December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
, ublituximab, and ibrutinib in patients with advanced CLL and NHL") Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
BACKGROUND AND RATIONALE
 SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
SYNOPSIS Observational study on the use of B cell receptor kinase inhibitors and BCL2 antagonists prior to allogeneic hematopoietic stem cell transplantation for B cell malignancies: A joint project of
ACALABRUTINIB IN MCL
 ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
pan-canadian Oncology Drug Review Final Clinical Guidance Report Idelalisib (Zydelig) for Chronic Lymphocytic Leukemia August 18, 2015
 for Chronic Lymphocytic Leukemia August 18, 2015") pan-canadian Oncology Drug Review Final Clinical Guidance Report Idelalisib (Zydelig) for Chronic Lymphocytic Leukemia August 18, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is
pan-canadian Oncology Drug Review Final Clinical Guidance Report Idelalisib (Zydelig) for Chronic Lymphocytic Leukemia August 18, 2015 DISCLAIMER Not a Substitute for Professional Advice This report is