Gross examination of pancreaticobiliary cancer specimens. Dr Vlad Maksymov MD, PhD, FRCPC OPA meeting September
|
|
|
- Jade Dean
- 5 years ago
- Views:
Transcription


1 Gross examination of pancreaticobiliary cancer specimens Dr Vlad Maksymov MD, PhD, FRCPC OPA meeting September
2 Learning Objectives Review issues related to the surgical anatomy and gross examination of the pancreaticoduodenectomy pancreaticobiliary cancer / specimen. Review and discuss existing terminology for margins and the need for standardized assessment of these specimens (as well as, discuss the role of standardized terminology amongst pathologists, radiologists, surgeons and oncologists in the optimal care of patients with pancreaticobiliary cancer). Discuss how gross examination of pancreaticoduodenectomy/pancreaticobiliary cancer specimen affects synoptic reporting. At the end of the session, the participants will be able to answer questions for self assessment.
3 Pancreaticoduodenectomy Pylorus preserving PD Standard/classic PD (Whipple procedure) Extended PD (includes dissection of retroperitoneal and aorta-caval lymph nodes (used in Asia) (A Nakao, et al, 2004) Total PD Pancreaticoduodenectomy (PD) specimen present a challenge for surgical pathologists because of the relative rarity of these specimens, combined with anatomic complexity (V V Adsay, et al, 2014)
4 PD specimen contains: Pancreatic head Most of duodenum (sometimes portion of jejunum) Distal segment of the common bile duct (CBD) If standard (classic) PD it also contains the pylorus and a segment of the stomach antrum (this become less common/nv Adsay, et al, 2014) If pylorus preserving PD - (no pylorus and antrum) Gallbladder and cystic duct
5 Whipple surgery involves following steps: The pancreatic neck is transected from the body of the pancreas The pancreatic head is dissected from the retroperitoneal soft tissues, including Superior Mesenteric/Portal Vein (SMV) and Superior Mesenteric Artery (SMA) SMV usually came out freely/relatively easily unless there is direct invasion of SMV or fibrous adhesions In the posterior-inferior aspect of the uncinate process the pancreatic tissues is dissected from the retroperitoneal soft tissues just right lateral along SMA. Common Hepatic Duct (often still called CBD) is transected at/above the union between the Cystic and Common Hepatic Duct and anastomosed to the jejunum.
6 Whipple surgery: For a pylorus preserving PD the duodenum is transected 1-2 cm distal to the pylorus For standard/classic PD the antrum is transected For both types of PD, the proximal jejunum is transected approximately 5 to 10 cm distal to ligament of Treitz. Extended PD includes dissection of retroperitoneal and aorta-caval lymph nodes (used in Asia) (A Nakao, et al, 2004)
7

8 M Katz, et al, 2010



9 Khalifa MA, Maksymov V, Rowsell C. Virchow's Arch. 2009
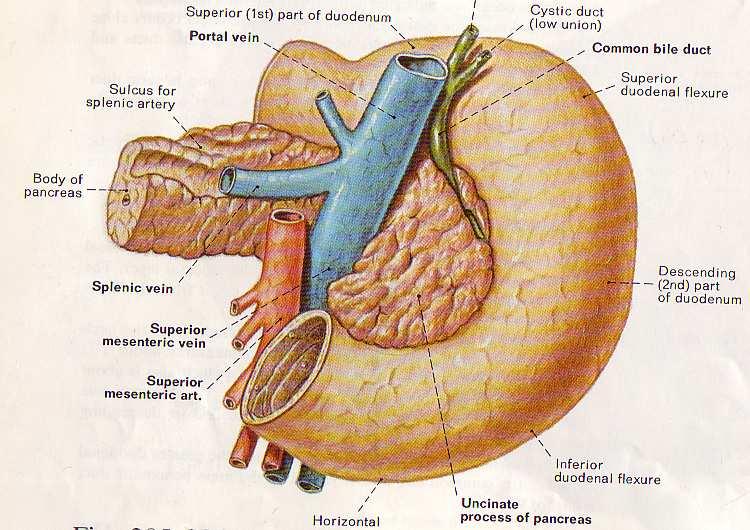
10 anatomy (in situ) on the posterior aspect of the pancreas; probes are inserted into major vessels. splenic vein superior mesenteric / portal vein Khalifa MA, Maksymov V, Rowsell C. Virchow's Arch. 2009


11 Khalifa MA, Maksymov V, Rowsell C. Virchow's Arch. 2009
12 This view shows the specimen with the vessels removed. The vascular groove can be seen. Khalifa MA, Maksymov V, Rowsell C. Virchow's Arch. 2009
13 Typically surgical margins of the PD specimen Luminal (proximal gastric and distal duodenal/jejunal) Pancreatic (also known as distal pancreatic (DP), it results from transecting the pancreatic neck Bile duct (BD) Anterior margin Retroperitoneal (RP RM) (also known as radial) or uncinate margin American Joint Committee on Cancer(2009) cancer staging manual recommends using the term SMA margin instead retroperitoneal or uncinate margin
14 Anatomic mapping of the retroperitoneal margin (RPM) M Khallifa, V Maksymov, C Rowsell, Virchows Archiv, 2009) RPM margin is actually a combination of surfaces/margins facing to the different anatomical structures (combination of the dissection and resection margins) Uncinate (SMA) margin (resection). Posterior surface of uncinate process (dissection margin). SMV/Vascular groove (dissection margin). Goal: to develop approach allowing to identify involvement of the SMV or SMA and give feedback to the surgeons and radiologists
15 Resection versus Dissection margin (Khalifa M A, Maksymov V, Rowsell C H, 2009) Resection margin- results from the surgeon s resection (using a sharp knife or blade). Dissection margin results from the separation of the pancreas using the hand and/or scissors or similar tools). Mobilization Margin (Jamieson, N Nigel, et al, 2010)

16 Khalifa MA, Maksymov V, Rowsell C, Virchow's Arch, 2009

17 Maksymov V, Hogan M, Khalifa MA, 2012
18 Margin versus free surfaces (N V Adsay, et al, 2014 and personal communication) Manually dissected (by surgeon) compartments are regarded as margin, and those that come off readily and are serosa covered are regarded as free surfaces Prefer to refer to only the posterior-inferior aspect of the uncinate process as margin to posterior-right aspect of the pancreatic head as free surface free surfaces are similar to dissection margin as per (Khalifa M A, Maksymov V, Rowsell C H, 2009)
19 Posterior free surfaces (N V Adsay, et al, 2014 and personal communication) Not true margin in the sense that 1) There is nothing the surgeon can do about them (they cannot go any further, or they cannot change their approach in order to take more next time etc; because this tissue more or less peels off readily. 2) These surfaces are akin to radial surfaces in any other organ including the serosal surface. this tissue clearly has a different covering than the true/real uncinate margin.
20 Anterior free surfaces (N V Adsay, et al, 2014) Anterior pancreaticoduodenal junctional region: the anterior free surface typically contains abundant adipose tissue and is convex in appearance. Anterior versus posterior free surfaces (N V Adsay, personal communication): it become clear most people had some sort of protocol for posterior free surfaces but nothing for anterior free surfaces.self-contradictory, considering that these 2 surfaces biologically are very similar and ought to be sampled and treated with the same principles.
21 Uncinate margin (SMA margin) The posterior-inferior aspect of the uncinate process Cut surface/stapled surface produced by surgeons using different tools dissecting uncinate process from SMA Bumpy appearance (contrary to vascular bed) Very vascular areas (can see staples, sutures) Some consider as mesopancreas (adipose tissue rich in peripheral nerves and vessels) Facing to SMA/right lateral to SMA Surgeons use different tools to do skeletonization of SMA Exposed pancreatic tissue indicator of not complete skeletonization
.")
22 M. A. Khalifa, V. Maksymov, C. H. Rowsell, and S. Hanna. HPB (Oxford). 2007; 9(2):
.")
23 M. A. Khalifa, V. Maksymov, C. H. Rowsell, and S. Hanna. HPB (Oxford). 2007; 9(2):
.")
24 M. A. Khalifa, V. Maksymov, C. H. Rowsell, and S. Hanna. HPB (Oxford). 2007; 9(2):
25 Frozen sections issues (M. A. Khalifa, V. Maksymov, C. H. Rowsell, and S. Hanna. HPB (Oxford). 2007; 9(2): ) Surgical technique for a PD resection involves clearance of all tissue along the portal vein/smv and along the right of SMA FS on SMA margin typically unhelpful as artery provides the absolute boundary FS on neck and bile duct resection margin may be appropriate
26 Superior Mesenteric Vein/Vascular groove margin/surface Concavity where the SMV/PV comes in contact with retroperitoneal surface of the pancreas In the majority of cases, pathologist recognize it as a concave depression with a smooth, glistening surface immediately to the left (posterior view) of the uncinate process
27
28 N.V Adsay et al. Am J Surg Pathol Apr;38(4):
29 Margin SMAM/uncinate (retroperitoneal) margin Maksymov V, Hogan M, Khalifa MA 2012 CAP RCPUK Verbeke Leeds Protocol/ Verbeke et al SMVM Medial* Posterior PNM BDM Anterior /-*** Other** Anatomical based mapping / authors approach Medial circumferential resection margin, the part of the surface of the pancreatic head that faces the superior mesenteric vessels * * following description is available in CAP Cancer protocols. Pancreas (exocrine), 2012: deep retroperitoneal posterior surface of the pancreas recommend inking the posterior surface of the pancreas and submission of sections through the tumor at its closest approach to this surface *** In author s opinion anterior margin present in pylorus preserving pancreaticoduodenectomy and absent in standard Whipple procedure
30 MARGIN INVOLVEMENT ( Maksymov V, Hogan M, Khalifa MA 2012) Margin Based on CAP approach Based on our approach (0 mm rule) (0 mm rule) (1 mm rule) SMA (uncinate) 9** (36.0%) 9** (36.0%) 14 (56.0%) SMV (groove) - 9 (36.0%) 18 (72.0%) Posterior surface of UP - 1 (4.0%) 5 (20.0%) Pancreatic neck 1 (4.0%) 1 (4.0%) 1 (4.0%) BDM 1 (4.0%) 1 (4.0%) 1 (4.0%) Total R1 9 (36.0%)* 14 (56.0%)* 20 (80.0%)* * Due to multifocality of resection margin involvement within the same specimen in some patients, the total number of involved margin exceeds the total number of R1 cases. ** In one more case, the SMAM was involved by metastatic carcinoma in a lymph node and this case was not included since it was considered as locoregional metastasis
31 The above findings illustrate that different approaches to the assessment and reporting retroperitoneal margin can changes the results and adversely affect the final statistics used in pancreatic cancer studies and clinical trials. Highlight needs for standardized assessment of the PD specimen
32 Gross examination is poorly reliable in the: assessment of the maximal dimension of the tumor selection of the sections to assess margin status Identification of lymph nodes Solution: extensive sampling or submission in total
33

34
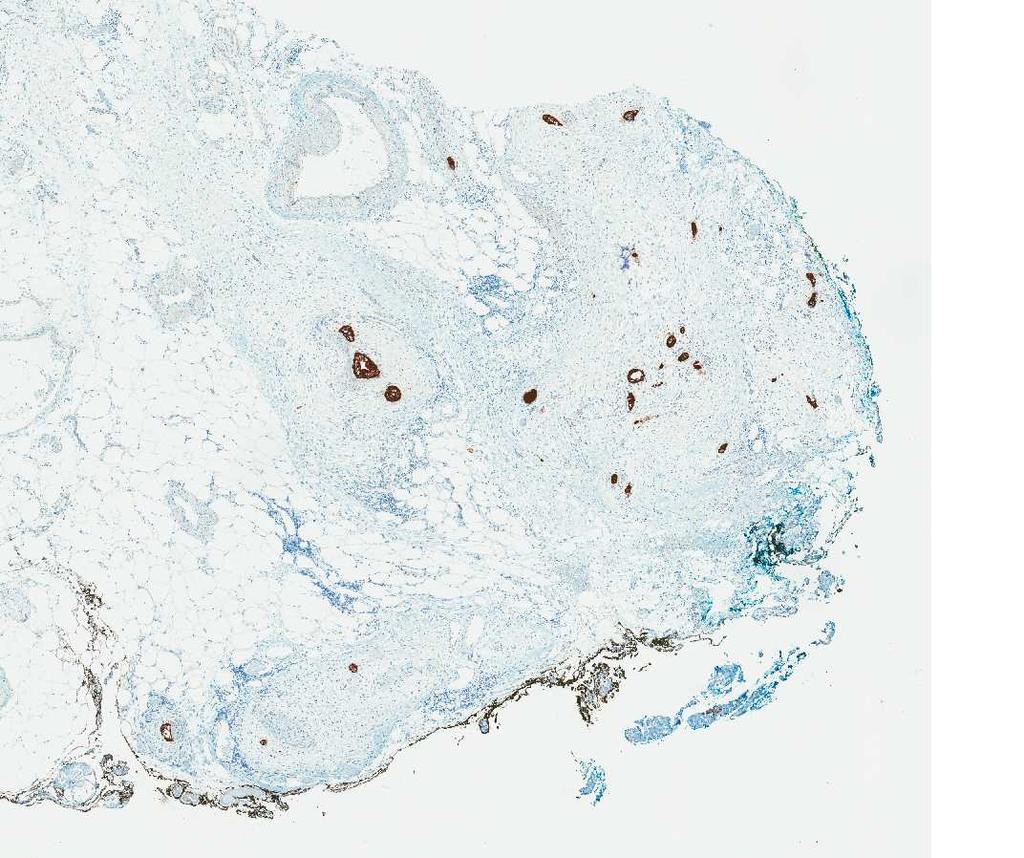
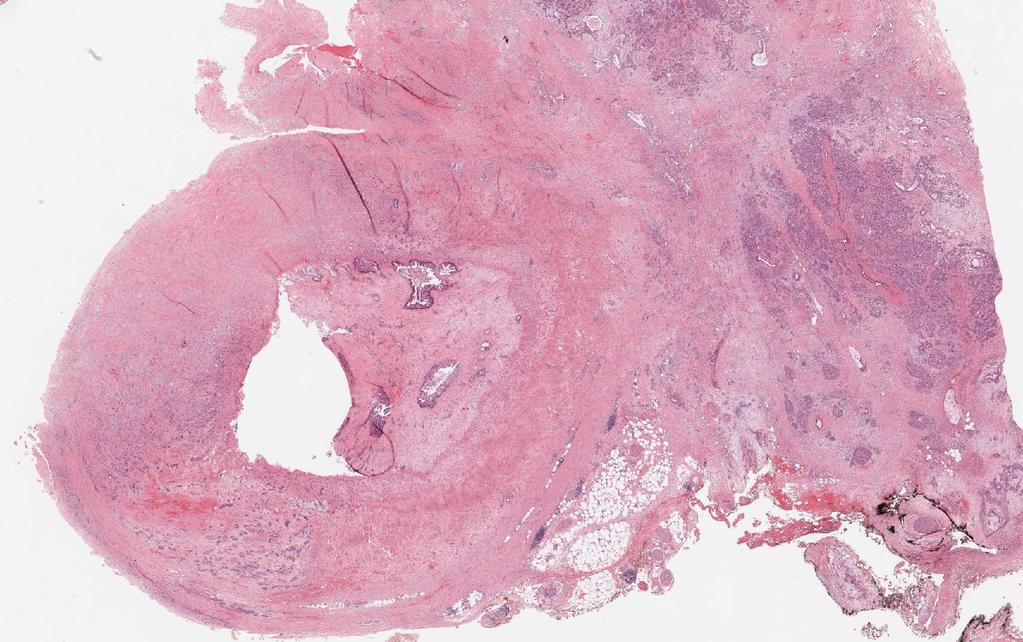
35 In this same study, invasion of the peripancreatic adipose tissue by single malignant glands are present (circle). NB: Invasion can t be identified on gross examination or with CT imaging.
36
37 Integrating pathology and radiology disciplines: an emerging opportunity? James Sorace et al. BMC Medicine 2012,10:100 Pathology and radiology form the core of cancer diagnosis, yet the workflow's of both specialties remain ad hoc and occur in separate silos, with no direct linkage between reporting system. isolation of radiology and pathology workflows can be detrimental to the quality and outcomes of patient care The opportunity has emerged to develop an integrated reporting system that supports both specialties




38




39
40
41 V Maksymov et al, American Journal of Clinical Pathology, Volume 138, Issue suppl_2, 1 November 2012, Pages A038, Published: 23 October 2015 Results indicate that even if radiologically confirmed tumor contact with SMV/PV confluence is less than 50% or even 25% adenocarcinoma will most likely be identified at the SMVM or within 1 mm (if margin submitted in total for microscopic examination) Patient Pathologic status Pre-operative radiology (circumference involvement) + Microscopic evidence of adenocarcinoma present at the margin - Adenocarcinoma is microscopically identified more than 1 mm from margin 1 + Contact (obliterated) 2 + Contact (50-75%) 3 + Contact (50%) 4 + Contact (25-50%) 5 + Contact (25%) 6 + Contact (25%) 7 + Contact (25%) 8 + Separate, 2 mm from tumor 9 1 mm Contact (50%) 10 1 mm Contact (50%) 11 1 mm Contact (25-50%) 12 1 mm Contact (25-50%) 13 1 mm Contact (25%) 14 1 mm Separate, 2 mm from tumor 15 1 mm Separate, 3 mm from tumor 16 1 mm Separate, 13 mm from tumor 17 - Separate, 8 mm from tumor 18 - Separate, 8 mm from tumor 19 - Separate 16 mm from tumor 20 - Separate 20 mm from tumor
42 V Maksymov et al, American Journal of Clinical Pathology, Volume 138, Issue suppl_2, 1 November 2012, Pages A038, Published: 23 October Presented at the Annual Meeting of the American Society of Clinical Pathology, 2012, Boston, USA. Complete correlation between preoperative imaging and microscopy (with the exception of one patient) Tumors were identified at or within 1 mm from SMVM even in patients where the radiologist identified less than 25% circumferential tumor contact with SMV/PV confluence Results indicate that even if radiologically confirmed tumor contact with SMV/PV confluence is less than 50% or even 25% adenocarcinoma will most likely be identified at the SMVM or within 1 mm (if margin submitted in total for microscopic examination);
 Distal margin (distal duodenal) SMA margin SMV / vascular groove margin/surface Posterior margin/surface Anterior margin/surface (NB: controversial, for discussion) Bile duct")
43 V Maksymov, M Khalifa, D Divaris and D Driman (2013) advocate for changes to the CAP checklist such that the following margins are evaluated in all PD specimens (changes in red): Proximal margin (gastric or duodenal) Distal margin (distal duodenal) SMA margin SMV / vascular groove margin/surface Posterior margin/surface Anterior margin/surface (NB: controversial, for discussion) Bile duct margin Pancreatic resection margin anterior surface pancreatic neck SMA posterior surface SMV groove Illustration modified from: Verbeke CS and Menon KV. HPB 2009;11:
44 Suggested unified reporting of the margins Margin(s) involved by invasive carcinoma Proximal resection margin (gastric or duodenal) Distal resection margin (distal duodenal) SMA/Uncinate process (retroperitoneal) resection margin (nonperitonealized surface of the uncinate process) SMV/Vascular groove dissection margin/surface Bile duct resection margin Pancreatic resection margin Other (specify): Invasive carcinoma involves other posterior retroperitoneal surface of pancreas
 Bile duct margin Pancreatic resection margin Other (specify): + Invasive carcinoma involves posterior retroperitoneal surface of pancreas Uncinate (retroperitoneal/superior mesenteric")
45 Margin(s) involved by invasive carcinoma Proximal margin (gastric or duodenal) Distal margin (distal duodenal) Uncinate process (retroperitoneal) margin (non-peritonealized surface of the uncinate process) Bile duct margin Pancreatic resection margin Other (specify): + Invasive carcinoma involves posterior retroperitoneal surface of pancreas Uncinate (retroperitoneal/superior mesenteric artery) margin Pancreatic neck/parenchymal resection margin DELETE ADDED
46 Positive margin definition: UK, Japan, Australia: -1 mm or less (1 mm rule) College of American Pathologist (2013 edition) rule) - malignant cells at the margin (0 mm Controversial data for many reasons. Importance: radiation oncologist - radiation or no?
47 Why it is important? Reporting of SMV/groove/margin/surface involvement: Tumor present microscopically at the SMV surface margin (SMA margin negative) radiation?
48 Why it is important? Pathologic reporting of SMV/groove/margin/surface involvement: important for quality assurance, including feedback to the radiologist and surgeons who makes preoperative and intraoperative decisions as to the separation of the vessel from pancreatic head, especially in borderline resectable cases
49 Main methods/protocols 1. Axial slicing method (no duct dissection) (Leeds Pathology Protocol (LEEPP), Menon KV, Gomez D, Smith AM, Anthoney A, Verbeke CS. HPB (Oxford), 2009; Verbeke CS, Gladhaug IP. B J Surg 2012) 2. Duct dissection method. 3. Combination (combine approach to grossing).
50 Combined approach. Shaved all margin (5-10 mm in thickness) and serially sectioned perpendicular to margins and submitted in total, oriented. Advantages: definite margin status and increase number of identified lymph nodes. Ampulla of Vater removed in block and sectioned longitudinally along long axis of CBD, submitted in total. Advantages: important to distinguish between pancreatic, ampullary and distal bile duct cancer. Remaining specimen serial slicing in axial plane (or other planes if necessary)
51 Pathologic staging (exocrine pancreas) (Based on AJCC/UICC TNM, 7th edition Protocol web posting date: August 2016 Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor ptis: Carcinoma in situ pt1: Tumor limited to the pancreas, 2 cm or less in greatest dimension pt2: Tumor limited to the pancreas, more than 2 cm in greatest dimension pt3: Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery pt4: Tumor involves the celiac axis or the superior mesenteric artery
52 Pathologic staging (exocrine pancreas) ( June 2017, includes ptmn requirements from the 8 th edition, AJCC Staging manual pt1: Tumor 2 cm in greatest dimension pt1a: Tumor 0.5 cm in greatest dimension pt1b: Tumor >0.5 cm and <1 cm in greatest dimension pt1c: Tumor 1 2 cm in greatest dimension pt2: Tumor >2 cm and 4 cm in greatest dimension pt3: Tumor >4 cm in greatest dimension pt4: Tumor involves the celiac axis, superior mesenteric artery, and/or common hepatic artery
53 Tumor size The T categories T1-T3 are defined by tumor size as it provides better prognostic stratification than classification based on extension into peripancreatic tissue (8 th Edition AJCC). (Lim JE, Chien MW, Earle CC. Ann Surg. 2003;237(1): Matsumoto G, Muta M, Tsuruta K, Horiguchi S, Karasawa K, Okamoto A. Pancreatology. 2007;7(2-3): Moon HJ, An JY, Heo JS, Choi SH, Joh JW, Kim YI. Pancreas. 2006;32(1): Saka B, Balci S, Basturk O, et al. Ann Surg Oncol. 2016;23(6): Allen PJ, Kuk D, Castillo CF, et al. Ann Surg. 2017;265(1): ) Tumor size is determined by measurement of the gross lesion and should be corroborated on microscopic assessment. (8th Edition AJCC).
54 V Maksymov, D Driman. World Pancreas Forum, Switzerland, 2017*** Pancreatic ductal adenocarcinoma was diagnosed in 30 cases. Extension of tumor into peripancreatic fat identified in all cases (pt3, based on 7 th edition of AJCC). According to the new 8 th Edition of AJCC size based criteria, these cases would have been reported as follows: pt3 (n=4) and pt2 (n=26). The average size of tumor was 3.2 cm. In our series, a finding of invasion of peripancreatic fat by single glands without desmoplasia was common and as result the true maximum dimension was most likely bigger than size measured on macroscopic examination or radiological assessment. *** The winner of travel grant
55 Conclusion The following discussion illustrate that different approaches to the assessment and reporting can completely change statistics and affect final understanding in all scientific trials etc. Standardized assessment of PD specimens now must include assessment of SMV dissection margin/surface (not only Uncinate process (SMA) resection margin). It is important for interdisciplinary collaboration) and quality assurance: 1) feedback for the radiology team 2) for the surgeon who is planning/making decision before and during the surgery to proceed with the separation of the SMV/PV from RP surface or not or perform wedge resection/en block resection of SMV/PV
56 Which anatomical structure (s) are facing to the Uncinate process (retroperitoneal) margin in the human body? A) Superior Mesenteric Artery and Superior Mesenteric Vein B) Vena cava Inferior C) Superior Mesenteric Artery D) Superior Mesenteric Vein
57 Which term is best in the description of the Superior Mesenteric Vein Margin? A) Resection margin B) Surface /Dissection margin C) Retroperitoneal margin
58 Which term is suggested by AJCC (Cancer Staging Manual, Seventh Edition) to be used instead of Uncinate process margin? A) Posterior pancreatic margin B) Superior Mesenteric Artery margin C) Retroperitoneal margin
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
 DOI:10.1111/j.1477-2574.2012.00561.x HPB ORIGINAL ARTICLE An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
DOI:10.1111/j.1477-2574.2012.00561.x HPB ORIGINAL ARTICLE An anatomical-based mapping analysis of the pancreaticoduodenectomy retroperitoneal margin highlights the urgent need for standardized assessment
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 285 Cases
 Original Article doi: 0.6/tjpath.08.06 Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 8 Cases Özgür EKİNCİ Department
Original Article doi: 0.6/tjpath.08.06 Evaluation of All Surgical Margins in Pancreatic Resection Specimens by Proper Grossing Techniques: Surgical Pathology Experience of 8 Cases Özgür EKİNCİ Department
Pancreaticoduodenectomy the anatomy and the surgical approaches
 Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Pancreaticoduodenectomy the anatomy and the surgical approaches Paul BS LAI Division of Hepato biliary and Pancreatic Surgery Department of Surgery The Chinese Univesity of Hong Kong Whipple s operation
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Topics: Staging and treatment for pancreatic cancer. Staging systems for pancreatic cancer: Differences between the Japanese and UICC systems
 M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
M. J Hep Kobari Bil Pancr and S. Surg Matsuno: (1998) Staging 5:121 127 system for pancreatic cancer 121 Topics: Staging and treatment for pancreatic cancer Staging systems for pancreatic cancer: Differences
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer
 Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
Masters of Surgery Page 1 of 5 Cattell-Braasch maneuver combined with superior mesenteric artery first approach for resection of borderline resectable pancreatic cancer Tingsong Yang 1, Fairweather Mark
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Protocol for the Examination of Specimens From Patients With Carcinoma of the Pancreas Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Pylorus Preserving Pancreaticoduodenectomy
 REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
REVIEW Pylorus Preserving Pancreaticoduodenectomy Jacqueline M. Garonzik-Wang, M. B. Majella Doyle Pancreaticoduodenectomy (PD) has become the standard of care for resectable pancreatic cancer and premalignant
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer
 Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer 1 Vinit Baliyan, MD; 1 Hamed Kordbacheh, MD; 2 Eric P Tamm, MD; 3 Theodore S Hong, MD; 4 Carlos Fernandez-Del
Interactive Exhibit On Imaging Updates For Staging And Response Assessment In Pancreatic Cancer 1 Vinit Baliyan, MD; 1 Hamed Kordbacheh, MD; 2 Eric P Tamm, MD; 3 Theodore S Hong, MD; 4 Carlos Fernandez-Del
An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein
 J Gastrointest Surg (2007) 11:425 431 DOI 10.1007/s11605-007-0131-1 An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein Rory L. Smoot & John D. Christein &
J Gastrointest Surg (2007) 11:425 431 DOI 10.1007/s11605-007-0131-1 An Innovative Option for Venous Reconstruction After Pancreaticoduodenectomy: the Left Renal Vein Rory L. Smoot & John D. Christein &
Pathways of Regional Spread in Pancreatic Cancer
 Pathways of Regional Spread in Pancreatic Cancer 12 Chusilp Charnsangavej, M.D. Regional spread of pancreatic ductal adenocarcinoma is common at the time of diagnosis, and it is often associated with poor
Pathways of Regional Spread in Pancreatic Cancer 12 Chusilp Charnsangavej, M.D. Regional spread of pancreatic ductal adenocarcinoma is common at the time of diagnosis, and it is often associated with poor
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Jacob Elebro 1,2* and Karin Jirström 1
 Elebro and Jirström Diagnostic Pathology 2014, 9:80 RESEARCH Open Access Use of a standardized diagnostic approach improves the prognostic information of histopathologic factors in pancreatic and periampullary
Elebro and Jirström Diagnostic Pathology 2014, 9:80 RESEARCH Open Access Use of a standardized diagnostic approach improves the prognostic information of histopathologic factors in pancreatic and periampullary
Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts
 Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts Version: DistalExtrahepaticBileDucts 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm
Protocol for the Examination of Specimens from Patients With Carcinoma of the Distal Extrahepatic Bile Ducts Version: DistalExtrahepaticBileDucts 4.0.0.1 Protocol Posting Date: June 2017 Includes ptnm
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
I patients with nonendocrine pancreas carcinoma
 LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS
 BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*)
") Hiroshima Journal of Medical Sciences Vol. 33, No. 2, 179,...183, June, 1984 HJM 33-24 179 Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*) Tsuneo TAN AKA, Motomu KODAMA, Rokuro
Hiroshima Journal of Medical Sciences Vol. 33, No. 2, 179,...183, June, 1984 HJM 33-24 179 Surgical Treatment for Periampullary Carcinoma A Study of 129 Patients*) Tsuneo TAN AKA, Motomu KODAMA, Rokuro
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Laparoscopy-assisted D2 radical distal subtotal gastrectomy
 Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases
 Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Original Article Radical nerve dissection for the carcinoma of head of pancreas: report of 30 cases Qing Lin, Langping Tan, Yu Zhou, Quanbo Zhou, Rufu Chen Department of Biliary and Pancreatic Surgery,
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy?
 Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
Ann Surg Oncol (2013) 20:3626 3633 DOI 10.1245/s10434-013-3080-9 ORIGINAL ARTICLE PANCREATIC TUMORS Is it Time to Stop Checking Frozen Section Neck Margins During Pancreaticoduodenectomy? Neha L. Lad,
ORIGINAL ARTICLE. Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma
 ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
ORIGINAL ARTICLE Helical Computed Tomography in the Diagnosis of Portal Vein Invasion by Pancreatic Head Carcinoma Usefulness for Selecting Surgical Procedures and Predicting the Outcome Hiroyoshi Furukawa,
1 Right & left Hepatic ducts Gastric Impression of spleen
 Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Pancreatic Model 1 Right & left Hepatic ducts 14 Gastric Impression of spleen 2 Common hepatic duct 15 Renal Impression of spleen 3 Cystic Duct 16 Colic Impression of spleen 4 Common Bile Duct 17 Splenic
Classification of nodal stations in gastric cancer
 Review Article Classification of nodal stations in gastric cancer Fausto Rosa 1, Guido Costamagna 2, Giovanni Battista Doglietto 1, Sergio Alfieri 1 1 Department of Digestive Surgery, 2 Department of Digestive
Review Article Classification of nodal stations in gastric cancer Fausto Rosa 1, Guido Costamagna 2, Giovanni Battista Doglietto 1, Sergio Alfieri 1 1 Department of Digestive Surgery, 2 Department of Digestive
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Anatomy of the liver and pancreas
 Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Protocol for the Examination of Specimens From Patients With Carcinoma of the Exocrine Pancreas
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Exocrine Pancreas Protocol applies to all epithelial tumors of the exocrine pancreas. Endocrine tumors and tumors of the ampulla
Protocol for the Examination of Specimens From Patients With Carcinoma of the Exocrine Pancreas Protocol applies to all epithelial tumors of the exocrine pancreas. Endocrine tumors and tumors of the ampulla
Surgical anatomy of the biliary tract
 HPB, 2008; 10: 7276 REVIEW ARTICLE Surgical anatomy of the biliary tract DENIS CASTAING Centre hépato-biliaire, Hôpital Paul Brousse, Assistance Publique- Hôpitaux de Paris, Université Paris XI, Paris,
HPB, 2008; 10: 7276 REVIEW ARTICLE Surgical anatomy of the biliary tract DENIS CASTAING Centre hépato-biliaire, Hôpital Paul Brousse, Assistance Publique- Hôpitaux de Paris, Université Paris XI, Paris,
Prevention Of Pancreaticojejunal Fistula After Whipple Procedure
 ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
ISPUB.COM The Internet Journal of Surgery Volume 4 Number 2 Prevention Of Pancreaticojejunal Fistula After Whipple Procedure N Barbetakis, K Setsiz Citation N Barbetakis, K Setsiz. Prevention Of Pancreaticojejunal
Lecture 02 Anatomy of the LIVER
 Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater Protocol applies to all intra-ampullary, peri-ampullary, and mixed intra- and peri-ampullary carcinomas. Well-differentiated
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ampulla of Vater Protocol applies to all intra-ampullary, peri-ampullary, and mixed intra- and peri-ampullary carcinomas. Well-differentiated
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
-Ensherah Mokheemer. -Shatha Al-Jaberi محمد المحتسب- 1 P a g e
 9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Outcomes of pancreaticoduodenectomy in patients with metastatic cancer
 Korean J Hepatobiliary Pancreat Surg 2014;18:147-151 http://dx.doi.org/.14701/kjhbps.2014.18.4.147 Original Article Outcomes of pancreaticoduodenectomy in patients with metastatic cancer Joo Hwa Kwak,
Korean J Hepatobiliary Pancreat Surg 2014;18:147-151 http://dx.doi.org/.14701/kjhbps.2014.18.4.147 Original Article Outcomes of pancreaticoduodenectomy in patients with metastatic cancer Joo Hwa Kwak,
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Standard 4.6: The Importance of CAP Protocols and Understanding Synoptic Reporting
 Standard 4.6: The Importance of CAP Protocols and Understanding Synoptic Reporting Jerry Hussong, MD, FCAP Cedars Sinai Medical Center, Los Angeles CA M. Asa Carter, CTR Manager, Accreditation and Standards
Standard 4.6: The Importance of CAP Protocols and Understanding Synoptic Reporting Jerry Hussong, MD, FCAP Cedars Sinai Medical Center, Los Angeles CA M. Asa Carter, CTR Manager, Accreditation and Standards
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Pancreaticoduodenectomy performed in a patient with situs ambiguous accompanied with isolated levocardia, malrotation, and normal spleen
 CASE REORT pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2014.87.6.340 Annals of Surgical Treatment and Research ancreaticoduodenectomy performed in a patient with situs ambiguous accompanied
CASE REORT pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2014.87.6.340 Annals of Surgical Treatment and Research ancreaticoduodenectomy performed in a patient with situs ambiguous accompanied
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Protocol for the Examination of Specimens from Patients with Carcinoma of the Ampulla of Vater
 Protocol for the Examination of Specimens from Patients with Carcinoma of the Ampulla of Vater Protocol applies to all intra-ampullary, peri-ampullary, and mixed intra- and peri-ampullary carcinomas. Welldifferentiated
Protocol for the Examination of Specimens from Patients with Carcinoma of the Ampulla of Vater Protocol applies to all intra-ampullary, peri-ampullary, and mixed intra- and peri-ampullary carcinomas. Welldifferentiated
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors
 AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
AJCP / REPORTING RECOMMENDATIONS FOR PANCREATIC SPECIMENS CONTAINING MALIGNANT TUMORS Recommendations for the Reporting of Pancreatic Specimens Containing Malignant Tumors Jorge AlboresSaavedra, David
Uveal Melanoma. Protocol applies to malignant melanoma of the uvea.
 Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.