UKALL14. A randomized trial for adults with newly diagnosed acute lymphoblastic leukaemia
|
|
|
- Madlyn Carpenter
- 5 years ago
- Views:
Transcription



1 UKALL14 A randomized trial for adults with newly diagnosed acute lymphoblastic leukaemia UKALL14 Training Manual v1.0 27Nov2017 1
2 This training manual is primarily intended to be used as a training tool for site staff working on the UKALL14 trial. New staff are encouraged to read the manual in addition to the protocol and other essential documents for their role. Existing staff can also use the manual to update themselves following amendments, or as an aide-memoire. Please do not use this manual as a substitute for the current approved protocol and drug supply guidelines. If you have any questions, please contact the UKALL14 study team at UCL CTC. 2
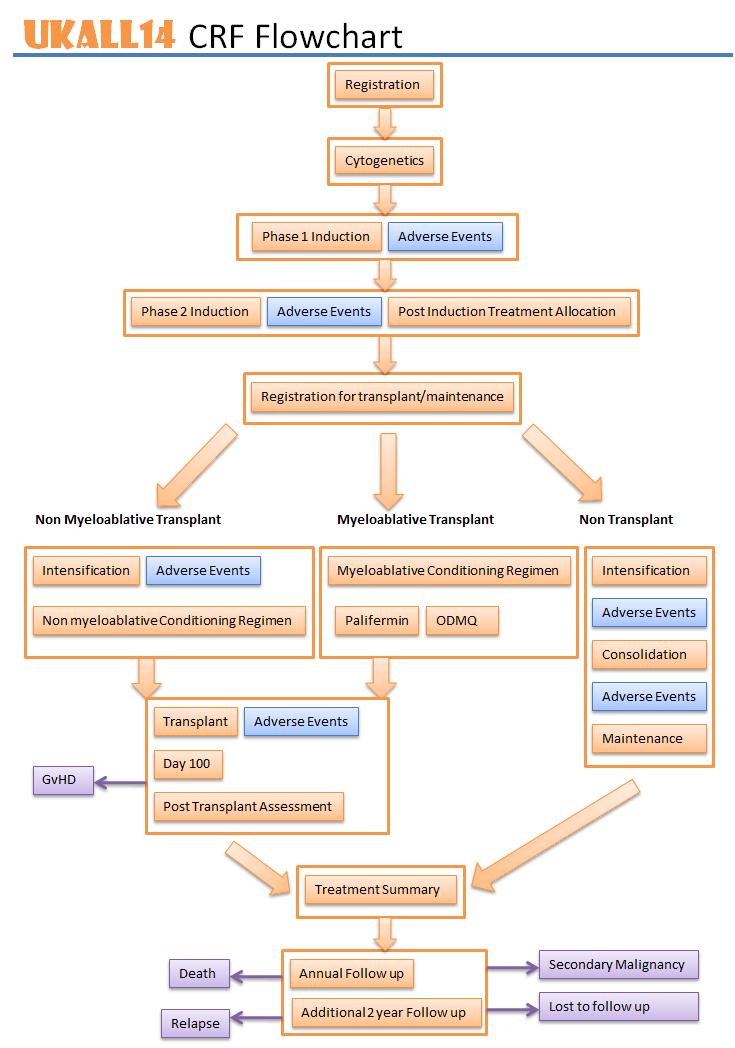
3 General Information 4 Randomised Patients Study Entry 20 Trial Treatment 27 Phase 1 Induction 30 Phase 2 Induction 34 Transplant 41 Myeloablative 44 Non-myeloablative 48 Intensification 53 Consolidation 57 Maintenance 63 Follow-up 67 Relapses 68 Second malignancies 69 Deaths 70 Data Management & CRF Guidance 71 Safety Reporting 74 Information for Pharmacies 82 Registration-only sub-study 88 3
4 4
5 General enquiries: Tel: Fax: Address: UKALL14 Trial Haematology Trials Group CR-UK & UCL Cancer Trials Centre 90 Tottenham Court Road London W1T 4TJ Refer to ISF section 2 or PSF section 1 for details of current team 5


6 The UCL CTC website can be used by site staff to access current versions of Investigator Site File & Pharmacy File documents mentioned within this manual: Go to website Click on All trials tab > UKALL14 Scroll down to View trial documents Click on the Download icon for the relevant document Protocols are password-protected contact UCL CTC for the password. 6
7 Lab name Address Samples to be sent UCL Cancer Institute MRD lab, London (See protocol appendix 8 for more information about this lab) Leukaemia Research Cytogenetics Group, Newcastle (See protocol appendix 7 for more information about this lab) Adult ALL MRD Laboratory UCL Cancer Institute Paul O Gorman Building 72 Huntley Street London WC1E 6DD Leukaemia Research Cytogenetics Group Northern Institute for Cancer Research Level 5, Sir James Spence Institute Royal Victoria Infirmary Queen Victoria Road Newcastle upon Tyne NE1 4LP BM samples at: o Baseline o End of phase 1 o End of phase 2 o 3 monthly post RIC transplant o Relapse Buccal swabs Pre-and postasparaginase samples Local cytogenetics report at: o Baseline 7
8 See protocol section and appendix 8 MRD samples, pre-and post asparaginase samples should be sent by courier or 1 st class post (at site s own cost) Samples taken on a Friday should be kept in the fridge over the weekend and sent first thing on Monday morning Kits are provided for taking and sending buccal swabs. Please contact UCL CTC if you need more kits. When posting sample(s), include a sample request form to identify the sample type(s) and timepoint(s) Plasma samples should be stored at -80 C wherever possible. Failing that, they should be stored at -20 C. Collection will be arranged at the end of the trial. Please ensure you keep a log of the samples you have stored. Ensure all samples & paperwork are anonymised prior to sending to labs Patients have only consented to share initials/dob/trial number/nhs no. Names must not be included 8
9 Please refer to Protocol Appendix 8. Charges apply to both randomised and registration only sub-study patients. The MRD laboratory is required to charge for MRD analysis MRD samples must be sent for both randomised patients and registration only patients to ensure standardised testing and to achieve best patient management The standard cost is 3,200 per patient A reduced fee of 200 will be charged if no marker can be identified on the baseline sample A list of charges is available on request Invoices will be sent directly to site please pay promptly Queries can be sent to the MRD lab allmrdlab@ucl.ac.uk and UKALL14 team at UCL CTC ctc.ukall14@ucl.ac.uk 9
10 Whenever a patient is referred to another hospital for part of their treatment or follow up, their care must be formally transferred: Complete and send the Centre Transfer form to UCL CTC (this is so we know where to direct our queries) Copies of the patient s CRFs up until the point of transfer must be provided to the new site The original site remains responsible for submitting and resolving queries on data for all visits up to the date of transfer The new centre will assume responsibility for submitting and resolving queries on data for all visits after the date of transfer If a patient s care is then transferred back, another Centre Transfer form must be completed and sent to UCL CTC. 10
11 Please refer to Protocol section 13.1 Sites must notify UCL CTC of deviations from the protocol or GCP immediately Sites should contact UCL CTC if they are in any doubt as to whether a certain situation constitutes an incident UCL CTC may detect an incident at site and request completion of an Incident Report form UCL CTC provide an incident report form, but a Trust incident report form may also be acceptable (if available) Please respond promptly to any queries UCL CTC will assess whether the case constitutes a serious breach if deemed to be a serious breach, UCL CTC will report to the REC and MHRA within the required 7 day timeline (refer to Protocol section 13.2) 11

12 Please refer to UKALL14 Monitoring Plan (held in ISF Section 1) There is no routine on-site monitoring for UKALL14 For cause monitoring may be undertaken in the event of non-compliance or poor CRF returns On site monitoring may also be carried out if requested by the site Central monitoring requests are ed to sites annually on the anniversary of the site activation date. This includes collection of: ISF/PSF checklists Site delegation logs Screening logs Drug accountability logs PI s CV and evidence of GCP training Please ensure we are kept up to date with site staff changes so that requests are directed to the correct people. An updated delegation log should be sent whenever there is a staff change. Up-to-date CVs & GCP training records must be held centrally at site. 12
13 Following completion of recruitment to the Rituximab randomisation in July 2017 and from implementation of protocol v11.0 onwards, a registration only sub-study has been introduced for patients with precursor B-cell ALL. Please note that there are different requirements for these patients, including: - Different Patient Information/Informed Consent document - Treatment of treating clinician s choice - Different case report forms - No AE/SAE/pregnancy reporting required Please refer to pages for procedures for randomised patients Please refer to pages for details of the registration only sub-study. 13
14 UKALL14 TRIAL SCHEMA Phase 1 Induction (4 weeks): precursor B-cell & T-cell patients (Philadelphia ve patients only) to receive Pegylated-Asparaginase plus standard phase 1 induction therapy Pre B-cell ALL T-cell ALL B1: Standard Phase 1 Therapy Alone B2: Standard Phase 1 Therapy + CD20 (Rituximab) Phase 2 Induction (4 weeks): precursor B-cell & T-cell patients to receive standard phase 2 induction therapy Standard Phase 1 Therapy Pre B-cell ALL T-cell ALL Standard Phase 2 Therapy T1: Standard Phase 2 Therapy PATIENTS IN COMPLETE REMISSION (CR) Risk Assessment performed on all patients at this time point T2: Standard Phase 2 Therapy + Nelarabine SIBLING DONOR High Risk NO SIBLING DONOR Standard Risk Aged 41 years and over * Intensification with HD- Methotrexate + pegylated asparaginase (Philadelphia ve patients only to receive pegylated asparaginase) To receive allo SCT (sibling), nonmyeloablative conditioning with fludarabine-melphalan and alemtuzumab SCT (sibling) Aged 40 years and under * To receive allo SCT (sibling), myeloablative conditioning with Etopside-TBI or Cyclophosphamide-TBI Aged 41 years and over * Intensification with HD-Methotrexate + pegylated asparaginase (Philadelphia ve patients only to receive pegylated asparaginase) To receive allo SCT (MUD), nonmyeloablative conditioning with fludarabine-melphalan and alemtuzumab Aged 40 years and under * To receive allo SCT (MUD), myeloablative conditioning with Etopside-TBI or Cyclophosphamide- TBI Continue methotrexate intensification, consolidation and maintenance * Age at study entry 14
15 Please refer to Protocol section 2.11 Aim 1B: To determine if the addition of rituximab to standard induction chemotherapy results in improved event free survival (EFS) in patients with precursor B-cell ALL Aim 1T: To determine if the addition of nelarabine improves outcome for patients with T-cell ALL Aim 1B & 1T are addressed by the B and T randomisations at study entry: B cell patients standard induction +/- rituximab (B-cell randomisation closed as of July 2017) T-cell patients - standard induction +/- nelarabine Aim 2: To determine the tolerability of pegylated asparaginase in induction treatment of all patients; to compare anti-asparaginase antibody levels between patients in the 2 randomisation groups from aim 1B Aim 2 is addressed by capturing data for all Philadelphia negative patients registered to the trial 15
16 Aim 3: To determine whether risk-adapted introduction of unrelated donor SCT results in greater EFS for patients at highest risk of relapse Aim 3 will be investigated in patients with high risk disease who do not have a sibling donor Aim 4: To compare 2 schedules of administration (standard vs collapsed) of keratinocyte growth factor (palifermin) for efficacy in preventing the severe mucosal toxicity of etoposide/tbi HSCT conditioning regimen. Aim 4 was addressed by the P randomisation in patients aged 40 and under having a sibling or unrelated donor myeloablative transplant (Palifermin randomisation closed as of April 2016) 16
17 The following IMPs are supplied for the trial free of charge: Rituximab (Mabthera ) - licensed - supplied by Roche (randomisation now closed) Nelarabine (Atriance ) - licensed - supplied by Novartis AG Palifermin (Kepivance ) - licensed until April 2016 previously supplied by Swedish Orphan Biovitrum (randomisation now closed) The following IMP is supplied for the trial at site s own cost: Pegylated Asparaginase (Oncaspar ) - licensed - supplied by Baxalta, now part of Shire Please liaise with pharmacy as early as possible when patients are consented to ensure there is sufficient stock of drugs. IMP supplied for the UKALL14 trial must only be used to treat randomised UKALL14 patients. 17
18 Please refer to Protocol section for full details Backbone chemotherapy, transplant conditioning and supportive care drugs specified in the protocol are standard treatment for this disease and are classified as NIMPs NIMPs for the trial must be sourced from hospital stock. Pharmacies are responsible for ensuring adequate supplies are maintained Dose banding is not allowed for IMPs, but local policy on dose banding may be followed for NIMPs Generic brands of NIMPs can be used as per local policy Every effort should be made to give NIMPs as per the protocol. See Protocol appendix 3 for details of dose modifications in case of toxicity. If further advice is required, please contact the TMG via ctc.ukall14@ucl.ac.uk Please see Drug Supply Guidelines for further information 18
19 Please refer to Protocol section for full details Local policies may be followed for: Tumour lysis prophylaxis Anti HSV and VZV prophylaxis PCP prophylaxis Antifungal prophylaxis (avoid azoles during treatment with vincristine) GCSF support See protocol section for guidance on thromboprophylaxis and management of methotrexate encephalopathy. Expert advice on haemostasis for individual patients can be obtained from: Professor Beverly Hunt Dr Charlotte Bradbury Copy in to any correspondence 19

20 20
21 Please refer to Protocol section 4.0. Informed consent must be obtained from the patient by a delegated person prior to any trial-specific intervention There are 2 patient information sheets & 2 consent forms to give to patients: Main PIS & consent Optional Additional Genetic Testing Buccal Swab PIS & consent Consent can be obtained for buccal swab at any time. We ask that as many patients as possible give samples to further our understanding of leukaemia. Document details of the consent process in the patient s notes: when the PIS was given discussion(s) about the trial with the patient when consent was taken who took consent 21
22 Please refer to Protocol section hours should be allowed for patients to consider participation in the trial If not possible, patients may consent on the same day provided the member of staff taking consent is satisfied that the patient understands the trial and its implications, and follows up with the patient to confirm ongoing willingness to participate Remember to complete the patient number on the top of the consent form following trial registration. The original consent form plus one copy must be stored at site (one in the ISF & one in the patient s medical notes). The patient must also be given a copy document in the notes that this has been done. Do not send consent forms to UCL CTC. 22
23 Patients cannot enter the trial until the results below confirming eligibility are known: Results required before registration Percentage of bone marrow blasts to confirm diagnosis of ALL (if not yet available, copy of diagnostic report) Patient s disease lineage Results not required in order to register Biochemistry Liver function tests Full blood counts (taken prior to starting steroid pre-phase treatment) Hepatitis B & C serology Negative pregnancy test (women of childbearing potential) Please refer to Protocol section 5.1 for a full list of screening investigations. 23
24 Please refer to Protocol section 5.2 Inclusion criteria a) Patients aged 25 and 65 old with acute lymphoblastic leukaemia (ALL) or aged 19 and 65 old with Philadelphia chromosome positive ALL b) Newly diagnosed, previously untreated ALL (a steroid pre-phase of 5-7 days is required and can start before registration) Exclusion criteria a) Mature B-cell leukaemia i.e. Burkitt s lymphoma t(8;14)(q24;q32) and variant c- myc translocations e.g. t(2;8)(p12;q24), t(8;22)(q24;q11) b) Known HIV infection c) Written informed consent c) Hepatitis B infection (positive HBsAg and/or HBcAb). Positive HBsAb only may be acceptable d) Hepatitis C infection (antibodies against hepatitis C or a PCR evaluation positive for hepatitis C DNA) e) Pregnant or lactating women f) Blast transformation of CML 24
25 Please refer to Protocol section Complete Registration & Randomisation Request form in full (including contact details on front page) and fax/ to UCL CTC If sending by , patient identifiable information (day/month of birth, NHS no) must be redacted before sending and then provided to UCL CTC by telephone Please contact UCL CTC if you require any guidance completing the registration form Send Registration & Randomisation Request form as early as possible, allowing minimum 2 hours for registrations to be processed (4pm cut off time for processing) UCL CTC will fax/ confirmation of the patient s randomisation, with trial number, back to the site Provide patient with a copy of their signed consent form and give them a contact card containing out-of-hours medical care details 25
26 Please refer to Protocol sections 5.1, 8.1.2, and appendix 8. Samples taken prior to consent can be used, but cannot be sent until patient has given their consent. Test Sample required Send to MRD baseline testing Constitutional DNA (optional) Cytogenetics 3-5ml bone marrow in EDTA Or 30-50ml blood in EDTA Buccal swab Report from local cytogenetics tests UCL Cancer Institute MRD lab UCL Cancer Institute MRD lab Leukaemia Research Cytogenetics Group, Newcastle Ensure all samples & paperwork are anonymised prior to sending to labs Patients have only consented to share initials/dob/trial number/nhs no. Names must not be included 26

27 27
 or T2 (standard induction + Nelarabine) Trial number format: B-cell randomised patients: 14-1-xxx T-cell randomised patients:")
28 Patients will undergo randomisation at study entry to determine their induction therapy: Pre-B cell patients randomised to: B1 (standard induction) or B2 (standard induction + Rituximab) now closed T-cell patients randomised to: T1 (standard induction) or T2 (standard induction + Nelarabine) Trial number format: B-cell randomised patients: 14-1-xxx T-cell randomised patients: 14-2-xxx 28
29 Please refer to Protocol section A steroid pre-phase is required prior to starting induction Dexamethasone 6mg/m 2 per day for 5-7 days May be started prior to trial registration 29
30 Please refer to Protocol section Pegylated asparaginase must not be given to Philadelphia positive patients at any point Day 4 pegylated asparaginase dose must be omitted in patients aged 41 years Liver function tests should be performed regularly whilst receiving pegylated asparaginase Blood counts must recover to the following levels before continuing to the next treatment phase: Neutrophils >0.75 x 10 9 /L Platelets >75 x 10 9 /L 30
31 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day 19 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 Day 28 Please see Protocol section UKALL14 Phase 1 induction Drug Dose Route Daunorubicin 30 mg/m 2 IV X X X X Vincristine 1.4mg/m 2 Max 2mg IV Dexamethasone 10mg/m 2 PO Max 20mg Pegylated 1000IU/m 2 IV Asparaginase** Methotrexate 12.5mg IT X X X X X X X X X X X X X X X X X* X X Imatinib (Philadelphia positive patients) 400mg 600mg*** PO X X X X X X X X X X X X X X X X X X X X X X X X X X X X * Omit day 4 dose in patients aged 41 ** Pegylated asparaginase must not be given to patients with Philadelphia positive disease *** Start imatimib at 400mg/day, escalate to 600mg/day within 2 weeks, if tolerated. Imatinib should be given continuously until transplant, if possible Rituximab was given to B-cell patients randomised to standard treatment + rituximab during Phase 1 Induction. Treatment deviations must be documented in patient notes, giving the reason why and associated clinical review/justification, and reported on relevant CRFs 31

32 Please see Protocol sections & Test Sample required When Send to Asparaginase activity & antiasparaginase antibodies* Asparaginase coagulation activity End of phase 1 MRD 5ml peripheral blood in serum tube 4.5ml peripheral blood in citrate tube for 5 minutes and store serum in 5 eppendorfs 3-5ml bone marrow aspirate in EDTA Patients aged 40: D3/4 & D18 Patients aged 41: D18 Patients aged 40: D3/4 & D18 Patients aged 41: D18 Count recovery at end of phase 1, or D35, whichever is sooner ** UCL Cancer Institute MRD lab Store locally at -80 C collection to be arranged at end of trial UCL Cancer Institute MRD lab * Not required for Philadelphia positive patients ** Repeat on D42 if hypocellular and no evidence of residual disease on Dd35 32
33 See protocol section for details of investigations to be carried out during treatment. CRF When to send How to send Induction Treatment Phase 1 form Induction Phase 1 AE form SAE reports Within 1 month of completing treatment phase Within 1 month of completing treatment phase Within 24 hours of becoming aware of SAE Post Post Fax/ See page 66 for details on reporting withdrawals from treatment See page 76 for details on reporting SAEs See page 70 for details on reporting deaths 33

34 Please refer to Protocol section Nelarabine should be given as soon as possible after count recovery following phase 2 induction, and no earlier than day 29 Nelarabine must not be given to patients who have unresolved grade 2 CNS toxicity at the end of phase 2. Monitor patients for signs of neurotoxicity & discontinue if grade 2 neurotoxicity toxicity Blood counts must recover to the following levels before continuing to the next treatment phase: Neutrophils >0.75 x 10 9 /L Platelets >75 x 10 9 /L

35 Day 1 Day 2 Day 3 Day 4 Day 5 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day 19 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 Day 28 Please see Protocol section UKALL14 Phase 2 induction Drug Dose Route Cyclophosphamide 1000 IV mg/m 2 X X Cytarabine 75mg/ IV X m 2 X X X X X X X X X X X X X X X Mercaptopurine 60mg/ PO X X X X X X X X X X X X X X X X X X X X X X X X X X X X m 2 Methotrexate 12.5mg IT Imatinib (Philadelphia positive patients) 400mg - 600mg PO X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X Nelarabine (arm T2) to start after count recovery no earlier than day 29. UKALL14 Phase 2 induction Nelarabine (arm T2 only) Drug Dose Route Nelarabine 1.5g/m 2 IV X X X Treatment deviations must be documented in patient notes, giving the reason why and associated clinical review/justification, and reported on relevant CRFs 35

36 Test Sample required When Send to End of phase 2 MRD 3-5ml bone marrow aspirate in EDTA Count recovery at end of phase 2, and before Nelarabine if on arm T2 UCL Cancer Institute MRD lab Result of end of phase 2 MRD will be sent to site within 10 days of receipt Please note that the MRD result is used for risk stratification so it is important that this sample is sent in a timely fashion 36

37 See protocol section for details of investigations to be carried out during treatment. CRF When to send How to send Induction Treatment Phase 2 form Induction Phase 2 AE form SAE reports Within 1 month of completing treatment phase Within 1 month of completing treatment phase Within 24 hours of becoming aware of SAE Post Post Fax/ See page 66 for details on reporting withdrawals from treatment See page 76 for details on reporting SAEs See page 70 for details on reporting deaths 37
38 Complete morphological remission should be confirmed locally on bone marrow examination upon count recovery (defined as 5% ALL blasts) If patient is not in CR at the end of phase 2 treatment: Patient should stop protocol treatment Further treatment will be at the local clinician s discretion The patient should enter follow up for the trial CRF required: CRF When to send How to send Treatment Summary form ASAP after stopping trial treatment Post 38

39 If patient is in CR at end of phase 2 treatment: Risk assessment is performed This determines whether the patient will continue with chemotherapy or have an allogeneic transplant 39
40 CRF When to send How to send Post Induction Treatment Allocation (PITA) form Post Induction Registration for Maintenance or Post Induction Registration for Transplant form Centre Transfer Form ASAP following completion of Induction Phase 2 treatment (but after completion of any ongoing donor search) ASAP following completion of Induction Phase 2 treatment (but after completion of any ongoing donor search) ASAP following completion of successful donor search Along with Post Induction Registration for Transplant form, if patient is to have transplant at another hospital Fax/ Fax/ Fax/ Fax/ 40
41 Inclusion criteria for transplant Eligibility for Transplant a) Completion of Phase 1 and Phase 2 treatment within the trial b) The following subgroups of patients will proceed to transplant: (i) Any patient with an HLA compatible sibling donor (ii) High risk* patients with an 8/8 molecularly matched donor at HLA-A, B, C and DR (iii) Patients with high risk* disease in whom no 8/8 match is available can proceed to transplant with a 7/8 matched unrelated donor OR umbilical cord unit(s) in the following circumstances: High risk cytogenetics Positive minimal residual disease (MRD) after phase 2 induction * See page 41 for definition of high risk disease 41
42 Eligibility for Transplant High risk disease a) Age 41 years b) Presenting WBC 30x10 9 /l (precursor-b disease) or 100x10 9 /l (T-lineage disease) c) High risk cytogenetics: one or more of the following abnormalities: (i) t(4;11)(q21;q23)/mll-af4 (ii) Low hypodiploidy/near triploidy (30-39 chromosomes/60-78 chromosomes) (iii) Complex karyotype (five or more chromosomal abnormalities) (iv) Philadelphia chromosome t(9;22)(q34;q11)/bcr-abl1 (detected by cytogenetic or molecular methods) d) High risk minimal residual disease (MRD) following phase 2 of induction (N.B. where there is no MRD marker, or if there is no phase 2 MRD sample, the patient will be assumed to have standard risk MRD) 42
43 Eligibility for Transplant If a patient aged 40 with a sibling donor and standard risk disease elects not to proceed to transplant, they will be permitted to proceed to continue with chemotherapy and will remain on trial. The decision should be clearly documented in the patient notes and on the post-induction treatment allocation form. Patients aged 41 at study entry should be considered for non-myeloablative transplant, regardless of whether they have a sibling donor If, for any reason, the protocol defined transplant conditioning is not considered suitable for a patient, their treatment plan should be discussed and agreed with the transplant coordinator in advance (Prof David Marks; david.marks@uhbristol.nhs.uk, please copy correspondence to ctc.ukall14@ucl.ac.uk) Patients who have agreed non-protocol transplants will remain on study, including collection of transplant data, unless they explicitly withdraw consent. 43
44 Please refer to Protocol section The protocol allows for either TBI-etoposide (preferred) or TBIcyclophosphamide conditioning, with IV methotrexate post transplant Local practice for scheduling conditioning regimens may be followed, but dosing must not change from that stipulated in the protocol. Immunosuppression should be given as per local policy Cyclosporin is recommended. 44
45 Day -7 Day -6 Day -5 Day -4 Day -3 Day -2 Day -1 Day 0 Day -7 Day -6 Day -5 Day -4 Day -3 Day -2 Day -1 Day 0 TBI-Etoposide conditioning (preferred) Drug Dose Route Fractionated TBI Total dose 1320cGy in 8 X X X X fractions Etoposide 60mg/kg IV X Haematopoietic stem cell infusion X TBI-Cyclophosphamide conditioning (alternative) Drug Dose Route Fractionated TBI Total dose 1320cGy in 8 X X X X fractions Cyclophosphamide 60mg/kg IV X X Haematopoietic stem cell infusion X Immunosuppression as per local policy suggest initially using Ciclosporin 3mg/kg/day IV starting on day -1 IV methotrexate 15mg/m 2 day +1 and 10mg/m 2 days +3, +6 &

46 CRF When to send How to send Myeloablative conditioning regimen form Within 30 days following completion of conditioning Post/fax/ Transplant form Within 30 days of transplant day 0 Post/fax/ Day 100 form Within 30 days after day 100 assessment Post/fax/ Post-transplant assessment form Treatment summary form GVHD form Graft failure form Within 30 days of each 3-monthly assessment (months 6-24 post transplant) Within 30 days after month 24 post transplant assessment As soon as possible after confirmation of GVHD As soon as possible after confirmation of graft failure Post/fax/ Post/fax/ Fax/ Fax/ SAE report Within 24 hours of becoming aware of SAE Fax/ 46

47 The protocol does not require samples to be sent to the central lab following myeloablative transplant. However, please note that if the patient relapses within the first 2 years post transplant, the following sample will be required: Test Sample required Send to MRD testing at relapse 3-5ml bone marrow in EDTA or 30-50ml peripheral blood in EDTA (if WBC >30x10 9 /l) UCL Cancer Institute MRD lab 47

48 Day -7 Day -6 Day -5 Day -4 Day -3 Day -2 Day -1 Day 0 3 monthly post transplant Please refer to Protocol section Fludarabine melphalan alemtuzumab conditioning Drug Dose Route Fludarabine 30mg/m 2 IV X X X X X Melphalan 140mg/m 2 IV X For recipients of unrelated donor allografts: Alemtuzumab 30mg IV X X For recipients of sibling allografts: Alemtuzumab 30mg IV X Haematopoietic stem cell infusion IV X Methotrexate 12.5mg IT X Immunosuppression as per local policy suggest initially using Ciclosporin 3mg/kg/day IV starting on day -1 48

49 Please refer to Protocol section Months post transplant Intrathecal methotrexate X X X X X X X X BM Aspirate for MRD X X X X X X X X Peripheral blood chimerism X X X X X X X X Follow up visit/data collection X X X X X X X X 49

50 CRF When to send How to send Non-myeloablative conditioning regimen form Within 30 days following completion of conditioning Post/fax/ Transplant form Within 30 days of transplant day 0 Post/fax/ Day 100 form Within 30 days after day 100 assessment Post/fax/ Post-transplant assessment form Treatment summary form GVHD form Graft failure form Within 30 days of each 3-monthly assessment (months 6-24 post-transplant) Within 30 days after month 24 post transplant assessment As soon as possible after confirmation of GVHD As soon as possible after confirmation of graft failure Post/fax/ Post/fax/ Fax/ Fax/ SAE report Within 24 hours of becoming aware of SAE Fax/ 50
51 Test Sample required Send to Mini-satellite regions* (pre-transplant) Post-transplant chimerism* (every 3 months until 24 months post transplant) Post-transplant MRD (every 3 months until 24 months post transplant or relapse) Peripheral blood or buccal swab from patient and donor as per local policy Peripheral blood from patient quantity as per local policy 3-5ml bone marrow in EDTA Local chimerism lab. Send anonymised results to UCL CTC Local chimerism lab. Send anonymised results to UCL CTC UCL Cancer Institute MRD lab Cell banking at relapse 3-5ml bone marrow in EDTA or 30-50ml peripheral blood in EDTA (if WBC >30x10 9 /l) UCL Cancer Institute MRD lab * Quantitative, lineage specific (myeloid & T-cell) chimerism should be performed by microsatellite PCR wherever possible. 51
52 Please refer to Protocol section DLI to be given for: Mixed chimerism Continued or progressive minimal residual disease Up to 5 DLI infusions, with escalating doses, can be given at 3 month intervals until normalisation of chimerism or MRD (see protocol for details). Do not give DLI if the patient has graft versus host disease DLI should not be given earlier than 6 months post transplant unless agreed in writing by the Transplant Coordinator, Prof David Marks When arranging unrelated donor transplants, sites are encouraged to store aliquots of donor lymphocytes in case DLI is required. 52

53 Please refer to Protocol section The following patients will proceed on to intensification once counts have recovered after phase 2 induction: Patients with no sibling donor and standard risk disease Patients aged 40 with a sibling donor but no high risk features who have elected not to proceed to transplant will be permitted to proceed to intensification and remain on trial Patients who are proceeding to transplant but experiencing >3 week delay arranging their transplant/identifying a donor intensification is given as holding therapy. Omit pegylated asparaginase in patients with Philadelphia positive disease Creatinine clearance must be >100mls/min before starting methotrexate. If creatinine clearance is <80mls/min, methotrexate must be reduced accordingly. 53

54 Route Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day 19 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 Day 28 Please refer to Protocol section UKALL14 Intensification Drug Dose Methotrexate 3 g/m 2 IV X X Pegylated 1000IU/ IV asparaginase* m 2 X X Imatinib (Philadelphia 400- PO positive patients) 600mg X X X X X X X X X X X X X X X X X X X X X X X X X X X X * Pegylated asparaginase must not be given to patients with Philadelphia positive disease Treatment deviations must be documented in patient notes, giving the reason why and associated clinical review/justification, and reported on relevant CRFs 54

55 Test Sample required When Send to Asparaginase activity & antiasparaginase antibodies* Asparaginase coagulation activity 5ml peripheral blood in serum tube 4.5ml peripheral blood in citrate tube for 5 minutes and store serum in 5 eppendorfs Prior to pegasparaginase dosing on D2 & D16 Prior to pegasparaginase dosing on D2 UCL Cancer Institute MRD lab Store locally at -80 C collection to be arranged at end of trial * Not required for Philadelphia positive patients 55

56 Please refer to Protocol section CRF When to send How to send Intensification form Intensification AE form SAE reports Within 1 month of completing treatment phase Within 1 month of completing treatment phase Within 24 hours of becoming aware of SAE Post/fax/ Post/fax/ Fax/ 56

57 Please refer to Protocol section Patients who have CNS involvement should have cranial irradiation before starting consolidation and be given maintenance mercaptopurine therapy during this time First cycle of consolidation to begin after counts recovered following intensification LFTs should be performed regularly whilst receiving pegylated asparaginase IT methotrexate can be moved +/-3 days to allow administration as per local & national guidance, for this phase Cytarabine treatment block schedule may be moved to take place during the week, as long as full dose is given for this phase Cycle 3 Days 1-42: D1-28: Treatment should be interrupted if patient experiences serious infection Counts must have recovered sufficiently before starting D29. A pause can be taken after day 28 to allow counts to recover if necessary 57
58 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day 19 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 Day 28 UKALL14 Consolidation 1 Drug Dose Route Cytarabine Etoposide Pegylated asparaginase* 75mg/ m 2 100mg/ m 2 IV IV Methotrexate 12.5mg IT Imatinib (philadelphia positive patiens) X X X X X X X X X X 1000IU/ IV X m mg PO X X X X X X X X X X X X X X X X X X X X X X X X X X X X X * Pegylated asparaginase must not be given to patients with Philadelphia positive disease UKALL14 Consolidation 2 Drug Dose Route Cytarabine 75mg/m 2 IV X X X X X Etoposide 100mg/m 2 IV X X X X X Methotrexate 12.5mg IT Imatinib (philadelphia positive patiens) mg PO X X X X X X X X Treatment deviations must be documented in patient notes, giving the reason and associated clinical review/justification, and reported on relevant CRFs 58

59 Day 29 Day 30 Day 31 Day 32 Day 33 Day 34 Day 35 Day 36 Day 37 Day 38 Day 39 Day 40 Day 41 Day 42 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14 Day 15 Day 16 Day 17 Day 18 Day 19 Day 20 Day 21 Day 22 Day 23 Day 24 Day 25 Day 26 Day 27 Day 28 UKALL14 Consolidation 3 Drug Dose Route Daunorubicin 25 mg/m 2 IV X X X X Vincristine 1.4mg/m 2 Max 2mg IV Dexamethasone 10mg/m 2 PO Max 20mg Pegylated 1000IU/m 2 IV Asparaginase* Methotrexate 12.5mg IT Imatinib (philadelphia positive patiens) mg PO * Pegylated asparaginase must not be given to patients with Philadelphia positive disease X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X X UKALL14 Consolidation 3 (continued) Drug Dose Route Cyclophosphamide 1000mg/m 2 IV X Cytarabine 75mg/m 2 IV X X X X X X X X Mercaptopurine 60mg/m 2 PO Imatinib (philadelphia positive patiens) mg PO X X X X X X X X X X X X X X X X X X X X X X X X X X X X Treatment deviations must be documented in patient notes, giving the reason and associated clinical review/justification, and reported on relevant CRFs 59
 400-600mg PO X X X X X X X X Treatment deviations must be documented in patient notes, giving the reason and associated clinical")
60 Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 UKALL14 Consolidation 4 Drug Dose Route Cytarabine 75mg/m 2 IV X X X X X Etoposide 100mg/m 2 IV X X X X X Methotrexate 12.5mg IT Imatinib (philadelphia positive patiens) mg PO X X X X X X X X Treatment deviations must be documented in patient notes, giving the reason and associated clinical review/justification, and reported on relevant CRFs 60

61 See protocol section for details of investigations to be carried out during treatment. CRF When to send How to send Consolidation Treatment form Consolidation AE form SAE reports Within 1 month of completing consolidation treatment Within 1 month of completing treatment phase Within 24 hours of becoming aware of SAE Post/fax/ Post/fax/ Fax/ See page 66 for details on reporting withdrawals from treatment See page 76 for details on reporting SAEs See page 70 for details on reporting deaths 61

62 The protocol does not require samples to be sent to the central lab during consolidation. However, please note that if the patient relapses during consolidation, the following sample will be required: Test Sample required Send to Cell banking at relapse 3-5ml bone marrow in EDTA or 30-50ml blood in EDTA (if WBC >30x10 9 /l) UCL Cancer Institute MRD lab 62
63 Please refer to Protocol section years of maintenance treatment starts when count recovery is reached following Consolidation cycle 4 No IMPs are given during maintenance treatment During maintenance, doses of mercaptopurine and methotrexate should be adjusted (+/- 25%) to maintain counts as follows: Neutrophils x 10 9 /L Platelets x 10 9 /L Drug Dose Route Frequency Vincristine 1.4mg/m 2 (max 2mg) IV Every 3 months Prednisolone 60mg/m 2 PO 5 days every 3 months Mercaptopurine 75mg/m 2 PO Daily Methotrexate 20mg/m 2 PO or IV Once per week (not on same day as co-trimoxazole) Intrathecal therapy during maintenance (to be given once neutrophils reach 0.75x10 9 /l and platelets reach 75x10 9 /l) Methotrexate 12.5mg IT Every 3 months 63
64 CRF When to send How to send Maintenance Treatment forms Treatment Summary form Within 30 days of completing each 3- month block of maintenance Within 30 days of completing/stopping maintenance treatment Post/fax/ Post/fax/ 64

65 The protocol does not require samples to be sent to the central lab during maintenance. However, please note that if the patient relapses during consolidation, the following sample will be required: Test Sample required Send to Cell banking at relapse 3-5ml bone marrow in EDTA or 30-50ml peripheral blood in EDTA (if WBC >30x10 9 /l) UCL Cancer Institute MRD lab 65
66 Send Treatment Summary form within 30 days of last trial treatment (trial treatment includes 24m post transplant follow-up even if patient is not receiving active treatment) A patient may stop trial treatment for any reason but will remain on trial and be followed up annually until death unless: Patient specifically withdraws consent (in which case, please complete and send the Lost to follow-up form as soon as possible) Patient was proven to have been ineligible. Relapsed? Send Relapse form as soon as possible following date of relapse Send MRD sample (bone marrow, or peripheral blood if WBC >30x109L) from time of relapse Relapse must be confirmed by morphological assessment and not molecular assessment Second cancer? Send Second Cancer form as soon as possible following diagnosis of second cancer Died? Send Death form within 7 calendar days of becoming aware of the death Provide overall cause of death on death form and refer to the death certificate where possible If the cause of death meets the criteria for an SAE (see protocol section ), complete and send an SAE report alongside the death form. 66
67 Follow-up begins from the anniversary of completing maintenance or end of 24 month post transplant follow-up or stopping trial treatment An annual follow-up form must be submitted every year (until the end of the study or death) for all surviving patients on the anniversary of their last trial treatment date (±30 days) There are 3 annual follow-up forms depending on the patient s status/progress: Send Not in CR after Phase 2 form if patient did not reach CR at any time during induction Send Relapse/Secondary Malignancy form if patient has relapsed or been diagnosed with a second cancer Send Annual Follow-up form if patient is in first CR and not diagnosed with a second cancer. Send Late Effects form within ±30 days of the 2 year follow-up appointment. Send Lost to Follow Up form as soon as possible for any patient who has been lost to follow up or who has withdrawn consent completely. 67

68 If a patient relapses at any point during the trial, the following CRF and sample must be sent: Please note that this only relates to clinical/morphological relapse, not molecular relapse whereby the patient becomes MRD positive only. CRF When to send How to send Relapse form ASAP following confirmation of relapse Fax/ Test Sample required Send to Cell banking at relapse 3-5ml bone marrow in EDTA or 30-50ml peripheral blood in EDTA (if WBC >30x10 9 /l) UCL Cancer Institute MRD lab 68
69 If a patient is diagnosed with a second primary malignancy at any point during the trial, the following CRF must be sent: CRF When to send How to send Second Cancer form ASAP following confirmation of diagnosis Fax/ 69
70 If a patient dies at any time during the trial, the following CRF must be sent: CRF When to send How to send Death form Within 7 calendar days of becoming aware of death Fax/ 70
71 71
72 72
73 See CRF Completion Guidelines. Ensure the current versions of the CRFs are used, as CRFs completed on outdated versions cannot be accepted Please return CRFs within the stated timeframes. Overdue CRF reports are sent out by UCL CTC to help sites keep track of what is outstanding UCL CTC will send each site batches of data clarification forms (DCFs) every 3 months If you have started on the previously sent DCF but not yet finished/sent it to UCL CTC, please phone UCL CTC to discuss. Sites who persistently fail to return data within the required timelines may be subjected to a for cause monitoring visit by UCL CTC 73

74 74
75 Please refer to Protocol section The maximum severity grade must be recorded for all adverse events that occur between informed consent and 30 days post consolidation (for nontransplant patients) or 30 days post transplant (for transplant patients) There is an AE form for each treatment phase to be used for this purpose Event terms and grades should be assigned using CTCAE v4.0 All grades of AEs must be reported in patient notes and AE forms, including Grade 1 & 2 events Pre-existing conditions do not qualify as AEs unless they worsen. Baseline AEs should be listed on the registration form Any AEs meeting the criteria for serious should be recorded on the AE form as well as an SAE report being submitted. 75
76 Please refer to Protocol section and CRF completion guidelines The following events are exempt from SAE reporting, but must be documented on the relevant CRF: Disease progression (use Relapse form) Disease related deaths (use Death form) Graft versus Host Disease (use GVHD form) Graft Failure (use Graft Failure form) Second primary malignancy (use second malignancy form) Report SAEs using the following form: CRF When to send How to send SAE report form Within 24 days of becoming aware of event Fax/ Please remember to include a contact name, phone number and address in case of any queries 76
77 SAE Reporting Timeframes Randomisation Timeframe (When IMP given) Timeframe (When no IMP given) Phase 1 induction B1 B2 T1, T2 From informed consent until 30 days post last Pegylated Asparaginase administration From informed consent until 30 post last Rituximab administration From informed consent until 30 days post last Pegylated Asparaginase administration 48 days from the date of randomisation for patients who do not receive Pegylated Asparaginase 54 days from the date of randomisation for patients who do not receive Rituximab. 48 days from the date of randomisation for patients who do not receive Pegylated Asparaginase Phase 2 induction B1, B2 T2 after Nelarabine administration Not required unless within phase 1 induction SAE reporting window or late effect of IMP From first dose of Nelarabine until 30 days post last Nelarabine administration Not required unless within phase 1 induction SAE reporting window From count recovery at the end of Phase 2 Induction until 35 days after count recovery at the end of Phase 2 Induction for patients not who do not receive Nelarabine Intensification B1, B2, T1, T2 From first administration of Pegylated Asparaginase until 30 days post last Pegylated Asparaginase administration Not required unless within phase 2 SAE reporting window 1 B1, B2, T1, T2 From first administration of Pegylated Asparaginase until 30 days post last Pegylated Asparaginase administration Not required Table extracted from protocol section
78 Intensifica Consolidation Phase 1 induction RIC Phase 2 induction transplant From first administration of Pegylated Not required unless within phase 2 SAE B1, B2, T1, T2 Asparaginase SAE until Reporting 30 days Timeframes post last reporting window Pegylated Asparaginase administration Randomisation Timeframe (When IMP given) Timeframe (When no IMP given) B1 1 B1, B2, T1, T2 B2 2 B1, B2, T1, T2 T1, T2 3 B1, B2, T1, T2 B1, B2 4 B1, B2, T1, T2 T2 after Nelarabine administration B1, B2, T1, T2 From informed consent until 30 days post From first administration of Pegylated last Pegylated Asparaginase Asparaginase until 30 days post last Pegylated Asparaginase administration administration From informed consent until 30 post last Not required Rituximab unless administration within consolidation 1 SAE reporting window or late effect of From informed consent IMP until 30 days post last Pegylated Asparaginase From first administration of Pegylated Asparaginase until 30 days post last Pegylated Not required Asparaginase unless within administration phase 1 induction SAE reporting window or late effect of IMP Not required unless within consolidation 3 SAE reporting window or late effect of IMP From first dose of Nelarabine until 30 days post last Nelarabine administration From start of conditioning chemotherapy until 30 days post-transplant 48 days from the date of randomisation for patients who do not receive Pegylated Not required Asparaginase 54 days from the date of randomisation for patients Not who required do not receive Rituximab. 48 days from the date of randomisation for patients who Not do required not receive Pegylated Asparaginase Not required unless within phase 1 induction SAE reporting window Not required From count recovery at the end of Phase 2 Induction until 35 days after count recovery at the end of Phase 2 Induction for patients not who do not receive From start of conditioning chemotherapy until 30 days Nelarabine post-transplant Intensification MAC transplant B1, B2, T1, T2 B1, B2, T1, T2 From first administration of Pegylated From Asparaginase start of conditioning until 30 days until post 30 last days Pegylated Asparaginase post-transplant administration Not required unless within phase 2 SAE From start of conditioning until 30 days reporting window post-transplant Maintenance on From first administration of Pegylated 1 B1, B2, T1, T2 Not Asparaginase required unless until 30 late days effect post of last IMP Not required Pegylated Asparaginase administration 2 B1, B2, T1, T2 Not required unless within consolidation 1 SAE reporting window or late effect of Not required Table extracted from protocol section
79 Venous thromboembolism (VTE) events are regarded as Adverse Events of Special Interest for this study Report as follows: Onset of VTE Report form to use How/when to send During SAE reporting window Outside SAE reporting window SAE report Thromboembolic Event Urgent Event Form See protocol section 12.3 for further information. By fax/ within 24 hours of becoming aware By fax/ within 7 days of becoming aware 79
80 Please refer to Protocol section 12.6 Pregnancies occurring in randomised female patients or in partners of randomised male patients at any point between start of trial treatment until 12 months after completing trial treatment must be reported using the following form: CRF When to send How to send Pregnancy report form Within 24 days of becoming aware of pregnancy Fax/ SAEs occurring in randomised patients during pregnancy must be reported on an SAE report form according to SAE reporting procedures 80
81 The pregnant patient/partner should be approached to request her consent for pregnancy monitoring using: Status of mother Trial patient Partner of trial patient Documents to use Pregnancy monitoring information sheet & consent form (patients) Pregnancy monitoring information sheet & consent form (partners) If the mother consents to pregnancy monitoring: The pregnancy must be followed-up until birth/termination. A follow-up Pregnancy Report must be submitted to UCL CTC within 24 hours of becoming aware of the outcome If the mother declines to consent: Please let UCL CTC know. No further data will be collected about the pregnancy. Completed consent forms must be filed in the ISF and patient notes. 81
82 82
83 Investigational Medicinal Products (IMPs) The following IMPs are supplied for the trial free of charge: Rituximab (Mabthera ) - licensed - supplied by Roche (randomisation now closed; no further orders to be placed) Nelarabine (Atriance ) - licensed - supplied by Novartis AG Palifermin (Kepivance ) licensed until April 2016 supplied by Swedish Orphan Biovitrum December 2010-April 2016 (randomisation now closed; no further orders to be placed) The following IMP is supplied for the trial at site s own cost: Pegylated Asparaginase (Oncaspar ) - licensed - supplied by Baxalta, now part of Shire IMP supplied for the UKALL14 trial must only be used to treat randomised UKALL14 patients. 83
 specified on the form and ensure UCL CTC is copied in ctc.ukall14@ucl.")
84 Please refer to the Drug Supply Guidelines for full details Site pharmacies are responsible for maintaining an adequate supply of IMP for each patient randomised Nelarabine and Pegylated Asparaginase must be ordered using the trial specific drug order forms, and sent to the address(es) specified on the form and ensure UCL CTC is copied in 84
85 Please refer to the Pharmacy Procedure for Reporting Temperature Excursions IMPs should be segregated and stored as per the SPCs All temperature readings outside the storage conditions specified in the SPC must be reported as excursions. If multiple temperature monitoring systems are used, report deviations which occur on ANY system. Actions to be taken upon identifying an excursion: Quarantine all affected trial stock IMMEDIATELY Complete the trial specific Notification of Temperature Excursion form to or fax to +44 (0) UCL CTC will check whether drug is safe to use and advise. N.B. Treating a patient with drug affected by a temperature excursion before the case has been reviewed and confirmation received that the IMP is safe to use may constitute a serious breach. 85
86 Accountability records must be kept up-to-date for all IMPs: Records of ordering and receipt Balance logs Dispensing logs Records of returns to pharmacy Destruction records Trial specific logs are provided; pharmacies can use own logs if they collect equivalent information Copies of accountability logs must be sent to UCL CTC upon request as part of central monitoring, plus any ad-hoc requests Traceability must be maintained for NIMPs and drugs used to treat registration only sub-study patients. Receipt of these drugs should be recorded centrally, so in the event of a batch recall pharmacy can identify which patients were given affected drug 86
87 Ensure a copy of the local Drug Destruction Procedure has been filed in relevant section of PSF Expired trial drugs must be quarantined UKALL14 team to request approval Upon approval of destruction, the IMP can be destroyed at site according to local pharmacy policy Record destruction on the Destruction Log and in Stock Balance accountability logs: Send a copy to UCL CTC File in the relevant section of the site pharmacy file 87

88 88
89 Registration only sub-study - overview From implementation of protocol v11.0 onwards, newly-diagnosed B-cell patients can now enter a UKALL14 registration only sub-study. Main aim is to collect basic data and samples to address laboratory aims Standard ALL treatment as per local clinician s choice No IMPs or NIMPs New CRFs to collect limited data No safety reporting 89
90 Registration only sub-study - aims Please refer to Protocol Appendix 1, section 2 Data and samples collected on registration only sub-study patients will be used to address the following laboratory aims: To characterise the genomic landscape of adult ALL To investigate the clonal origins of relapsed ALL To define a T-cell signature which predicts response to allo-hct To develop global risk models in adult ALL that integrate demographic, genetic and response information 90
91 Registration only sub-study - informed consent Please refer to Protocol Appendix 1, Section 3 Informed consent must be obtained from the patient by a delegated person prior to any trial-specific intervention There are 2 patient information sheets/consent forms to give to patients: Registration only sub-study PIS/consent Optional Additional Genetic Testing Buccal Swab PIS/consent Consent can be obtained for buccal swab at any time. We ask that as many patients as possible give samples to further our understanding of leukaemia. Document details of the consent process in the patient s notes: when the PIS was given discussion(s) about the trial with the patient when consent was taken who took consent 91
92 Registration only sub-study Please refer to Protocol Appendix 1, Section 3 24 hours should be allowed for patients to consider participation in the trial If this is not possible, patients may consent on the same day provided the member of staff taking consent is satisfied that the patient understands the trial and its implications and follows up with the patient to confirm ongoing willingness to participate and documents this in patient notes Remember to complete the patient number on the top of the consent form following trial registration The original consent form plus one copy must be stored at site (one in the ISF & one in the patient s medical notes). The patient must also be given a copy document in the notes that this has been done. Do not send consent forms to UCL CTC. - informed consent 92
93 Patients cannot enter the sub-study until the results below confirming eligibility are known: Results required before registration Percentage of bone marrow blasts to confirm diagnosis of ALL (if not yet available, copy of diagnostic report) Patient s disease lineage Medical history (specifically history of hepatitis B & C and HIV) Negative pregnancy test (women of childbearing potential) Please refer to Protocol Appendix 1 for a full list of screening investigations and eligibility criteria. 93
 Newly diagnosed, previously untreated ALL (a steroid pre-phase is permitted but not required) Exclusion criteria a) Mature B-cell leukaemia (eg.")
94 Registration only sub-study - eligibility Please refer to Protocol Appendix 1, section 5 Inclusion criteria a) Patients aged 25 and 65 old with B- cell ALL or aged 19 and 65 old with Philadelphia chromosome positive ALL b) Newly diagnosed, previously untreated ALL (a steroid pre-phase is permitted but not required) Exclusion criteria a) Mature B-cell leukaemia (eg. Burkitt s lymphoma) b) Known HIV infection c) Written informed consent c) Known history of hepatitis B infection* d) Known history of hepatitis C infection* e) Pregnant or lactating women f) Blast transformation of CML *As per national MHRA guidance, hepatitis testing must be done prior to administering rituximab 94
 and fax/email to UCL CTC If sending by email, patient identifiable information (NHS no, DOB)")
95 Registration only sub-study - registration Please refer to Protocol Appendix 1 Section 6 Pre-registration evaluations should be carried out as per local policy. Complete Registration only sub-study Registration form in full (including contact details on front page) and fax/ to UCL CTC If sending by , patient identifiable information (NHS no, DOB) must be redacted before sending and then provided to CTC by telephone Please allow a minimum of 2 hours for registrations to be processed (cut off time for same day processing is 4pm) CTC will fax/ confirmation of the patient s registration, with trial number, back to the site Provide patient with a copy of their signed consent form. 95
96 Please refer to Protocol Appendix 1 Section 8.3 Samples taken prior to consent can be used, but cannot be sent until patient has given their consent. Test Sample required Send to MRD baseline testing Constitutional DNA (optional) Cytogenetics 3-5ml bone marrow in EDTA or 30-50ml blood in EDTA Buccal swab Report from local cytogenetics tests UCL Cancer Institute MRD lab UCL Cancer Institute MRD lab Leukaemia Research Cytogenetics Group, Newcastle 96

97 Please refer to Protocol Appendix 1 Section 7 Treatment for registration only patients is decided by the local clinician May follow the UKALL14 backbone regimen but it is not mandated Any drugs used to treat registration only patients will not be regarded as IMPs Drugs must be sourced from hospital stock and will not be reimbursed Follow local practice with regards to recovery/continuation at each phase Accountability logs are not required - follow standard local practice regarding drug traceability. 97
98 Test Sample required When Send to End of phase 1 MRD End of phase 2 MRD Posttransplant MRD Cell banking at relapse 3-5ml bone marrow aspirate in EDTA 3-5ml bone marrow aspirate in EDTA 3-5ml bone marrow aspirate in EDTA 3-5ml bone marrow aspirate in EDTA or 30-50ml peripheral blood in EDTA (if WBC >30x10 9 /l) Count recovery at end of phase 1 Count recovery at end of phase 2 Every 3 months post non-myeloablative transplant When relapse suspected/ confirmed UCL Cancer Institute MRD lab Report can be sent on special request UCL Cancer Institute MRD lab Report will be sent within 10 days of receipt UCL Cancer Institute MRD lab Report will be sent within 10 days of receipt UCL Cancer Institute MRD lab 98

99 NEW CRFs Registration only Sub-study Entry form study entry, before starting induction treatment Registration only Induction Treatment form after induction phase 1 and phase 2 Registration only Post Induction Chemotherapy form after each phase of treatment/every 3 months during maintenance Registration only Annual Follow Up form from anniversary of completion of treatment/transplant And if transplant is given: Registration only Transplant Day 100 form Registration only GvHD form EXISTING CRFs Relapse form (send ASAP) Death form (send ASAP) Lost to Follow Up form (send ASAP) Centre Transfer form (send ASAP) CRFs should be sent within 30 days of timepoint unless stated otherwise 99
UKALL14 DRUG SUPPLY GUIDELINES
 CONTACT DETAILS UKALL14 DRUG SUPPLY GUIDELINES For further information on trial drugs, trial protocol, dosing, supply drug and distribution queries please contact: UKALL14 Trial Team Phone: 0207 679 9860
CONTACT DETAILS UKALL14 DRUG SUPPLY GUIDELINES For further information on trial drugs, trial protocol, dosing, supply drug and distribution queries please contact: UKALL14 Trial Team Phone: 0207 679 9860
UKALL14. A randomized trial for adults with newly diagnosed acute lymphoblastic leukaemia. Protocol version & date: Version
 UKALL14 A randomized trial for adults with newly diagnosed acute lymphoblastic leukaemia Trial Sponsor: University College London Trial Sponsor no: UCL/08/0167 Trial funder: Cancer Research UK Funder reference:
UKALL14 A randomized trial for adults with newly diagnosed acute lymphoblastic leukaemia Trial Sponsor: University College London Trial Sponsor no: UCL/08/0167 Trial funder: Cancer Research UK Funder reference:
Introduction: Trial contacts: Trial Management Group (TMG):
:") Introduction: Cancer Research UK is supporting central coordination through the Cancer Research UK & UCL Cancer Trials Centre (UCL CTC) the coordinating centre for the trial. Problems relating to this
Introduction: Cancer Research UK is supporting central coordination through the Cancer Research UK & UCL Cancer Trials Centre (UCL CTC) the coordinating centre for the trial. Problems relating to this
UKALL14. Non-Myeloablative Conditioning Regimen (1/1) Date started (dd/mm/yyyy) (Day 7) Weight (kg) BSA (m 2 )
 Date started (dd/mm/yyyy) (Day 7) Weight (kg) BSA (m 2 )") Non-Myeloablative Conditioning Regimen (1/1) started (dd/mm/yyyy) (Day 7) BSA (m 2 ) Weight (kg) Please enter the daily dose given in the table below: Day Fludarabine (mg) Melphalan (mg) Alemtuzumab (mg)
Non-Myeloablative Conditioning Regimen (1/1) started (dd/mm/yyyy) (Day 7) BSA (m 2 ) Weight (kg) Please enter the daily dose given in the table below: Day Fludarabine (mg) Melphalan (mg) Alemtuzumab (mg)
Acute Lymphoblastic Leukaemia Guidelines
 Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
Acute Lymphoblastic Leukaemia Guidelines Approved by Pathway Board for Haematological Malignancies Coordinating author: Adele Fielding, Royal Free London NHS Trust Date of issue: 12.03.2015 Version number:
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010
 Ryan Mattison, MD University of Wisconsin March 2, 2010") Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
Acute Lymphoblastic Leukemia (ALL) Ryan Mattison, MD University of Wisconsin March 2, 2010 ALL Epidemiology 20% of new acute leukemia cases in adults 5200 new cases in 2007 Most are de novo Therapy-related
ALL CONSOLIDATION- Cycle 3 (25-60 years)
") ALL CONSOLIDATION- (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It
ALL CONSOLIDATION- (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It
ALL Phase 2 Induction (25-60 years)
") ALL Phase 2 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
ALL Phase 2 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
Rob Wynn RMCH & University of Manchester, UK. HCT in Children
 Rob Wynn RMCH & University of Manchester, UK HCT in Children Summary Indications for HCT in children Donor selection for Paediatric HCT Using cords Achieving engraftment in HCT Conditioning Immune action
Rob Wynn RMCH & University of Manchester, UK HCT in Children Summary Indications for HCT in children Donor selection for Paediatric HCT Using cords Achieving engraftment in HCT Conditioning Immune action
ALL Phase 1 Induction (25-60 years)
") ALL Phase 1 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
ALL Phase 1 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
London Cancer ALL guidelines
 London Cancer ALL guidelines Page 1 of 7 CONTENTS OVERVIEW - main points in ALL management... 3 AGE-SPECIFIC THERAPEUTIC APPROACHES... 4 SPECIFIC THERAPEUTIC PROBLEMS... 5 SUPPORTIVE CARE... 6 PATIENTS
London Cancer ALL guidelines Page 1 of 7 CONTENTS OVERVIEW - main points in ALL management... 3 AGE-SPECIFIC THERAPEUTIC APPROACHES... 4 SPECIFIC THERAPEUTIC PROBLEMS... 5 SUPPORTIVE CARE... 6 PATIENTS
ALL-RELAPSE GROUP Päivi Lähteenmäki on behalf of the group
 ALL-RELAPSE GROUP 18.11.2014 Päivi Lähteenmäki on behalf of the group Meeting in Bergen and 2 telephone meetings (Sept, Oct) IntReALL-group in Lissabon (September, Thomas F) IntReALL SR : Denmark has registered
ALL-RELAPSE GROUP 18.11.2014 Päivi Lähteenmäki on behalf of the group Meeting in Bergen and 2 telephone meetings (Sept, Oct) IntReALL-group in Lissabon (September, Thomas F) IntReALL SR : Denmark has registered
Clinical Guidelines for Lymphoid Diseases Acute Lymphoblastic Leukaemia (ALL)
") Clinical Guidelines for Lymphoid Diseases Acute Lymphoblastic Leukaemia (ALL) Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-107 8 Dr Helen Barker
Clinical Guidelines for Lymphoid Diseases Acute Lymphoblastic Leukaemia (ALL) Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-107 8 Dr Helen Barker
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
ALL MAINTENANCE (25-60 years)
") ALL MAINTENANCE (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It may
ALL MAINTENANCE (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It may
SUPPLEMENTARY FILE GRAALL and GRAALL PROTOCOLS
 SUPPLEMENTARY FILE GRAALL- 2003 and GRAALL- 2005 PROTOCOLS INTRODUCTION 1 FIGURE 1. GRAALL- 2003 AND GRAALL- 2005 OVERALL SURVIVAL 2 GRAALL- 2003 PROTOCOL 3 1. GENERAL STUDY DESIGN 3 2. INCLUSION AND NON-
SUPPLEMENTARY FILE GRAALL- 2003 and GRAALL- 2005 PROTOCOLS INTRODUCTION 1 FIGURE 1. GRAALL- 2003 AND GRAALL- 2005 OVERALL SURVIVAL 2 GRAALL- 2003 PROTOCOL 3 1. GENERAL STUDY DESIGN 3 2. INCLUSION AND NON-
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand
 Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Appendix 6: Indications for adult allogeneic bone marrow transplant in New Zealand This list provides indications for the majority of adult BMTs that are performed in New Zealand. A small number of BMTs
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Biondi A, Schrappe M, De Lorenzo P, et al.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Biondi A, Schrappe M, De Lorenzo P, et al.
INITIATION SLIDES VERSION
 PARADIGM- 2 (BR36) OlaPArib and RADIotherapy or olaparib and radiotherapy plus temozolomide in newly-diagnosed Glioblastoma stratified by MGMT status: 2 parallel phase I studies INITIATION SLIDES VERSION
PARADIGM- 2 (BR36) OlaPArib and RADIotherapy or olaparib and radiotherapy plus temozolomide in newly-diagnosed Glioblastoma stratified by MGMT status: 2 parallel phase I studies INITIATION SLIDES VERSION
Acute Lymphoblastic and Myeloid Leukemia
 Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Vaccination to protect against shingles
 Vaccination to protect against shingles - An update for registered healthcare practitioners The programme from September 2018 and contraindications and precautions Revised July 2018 NES and HPS accept
Vaccination to protect against shingles - An update for registered healthcare practitioners The programme from September 2018 and contraindications and precautions Revised July 2018 NES and HPS accept
RITAZAREM. CRF Completion Guidelines
 RITAZAREM CRF Completion Trial Title: Protocol Number: An international, open label, randomised controlled trial comparing rituximab with azathioprine as maintenance therapy in relapsing ANCA-associated
RITAZAREM CRF Completion Trial Title: Protocol Number: An international, open label, randomised controlled trial comparing rituximab with azathioprine as maintenance therapy in relapsing ANCA-associated
MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA. BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS
 MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS Introduction The management of ALL, the most common childhood malignancy (1/3 rd of all malignancy), has
MANAGEMENT OF ACUTE LYMPHOBLASTIC LEUKEMIA BY Dr SUBHASHINI 1 st yr PG DEPARTMENT OF PEDIATRICS Introduction The management of ALL, the most common childhood malignancy (1/3 rd of all malignancy), has
One Day BMT Course by Thai Society of Hematology. Management of Graft Failure and Relapsed Diseases
 One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
One Day BMT Course by Thai Society of Hematology Management of Graft Failure and Relapsed Diseases Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital
Summary. Table 1 Blinatumomab administration, as per European marketing authorisation
 Cost-effectiveness of blinatumomab (Blincyto ) for the treatment of relapsed or refractory B precursor Philadelphia chromosome negative acute lymphoblastic leukaemia in adults. The NCPE assessment of blinatumomab
Cost-effectiveness of blinatumomab (Blincyto ) for the treatment of relapsed or refractory B precursor Philadelphia chromosome negative acute lymphoblastic leukaemia in adults. The NCPE assessment of blinatumomab
HSCT - Minimum Essential Data - A FOLLOW UP REPORT - ANNUAL
 CIC: HSCT - Minimum Essential Data - A FOLLOW UP REPORT - ANNUAL Disease PRIMARY DISEASE DIAGNOSIS Centre Identification EBMT Code (CIC): Hospital: Contact person: Unit: Email: Patient Data Date of this
CIC: HSCT - Minimum Essential Data - A FOLLOW UP REPORT - ANNUAL Disease PRIMARY DISEASE DIAGNOSIS Centre Identification EBMT Code (CIC): Hospital: Contact person: Unit: Email: Patient Data Date of this
Standard Regimens for Haematology
 Regimens for Haematology ChlVPP Chlorambucil 6mg/m 2 PO D1 to 14 Vinblastine 6mg/m 2 (max 10mg) IV on D1 & 8 Procarbazine 100mg/m 2 PO on D1 to 14 Prednisolone 40mg PO D1 to 14 ABVD Doxorubicin 25mg/m
Regimens for Haematology ChlVPP Chlorambucil 6mg/m 2 PO D1 to 14 Vinblastine 6mg/m 2 (max 10mg) IV on D1 & 8 Procarbazine 100mg/m 2 PO on D1 to 14 Prednisolone 40mg PO D1 to 14 ABVD Doxorubicin 25mg/m
ACUTE LYMPHOBLASTIC LEUKEMIA
 ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Adult ALL: NILG experience
 Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
Adult ALL: NILG experience R Bassan USC Ematologia, Ospedali Riuniti, Bergamo SIE Interregionale, Padova 12 5 2011 Now and then Northern Italy Leukemia Group 2000-10 Prospective clinical trials 09/00 10/07
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.
: Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.
R-IDARAM. Dexamethasone is administered as an IV infusion in 100mL sodium chloride 0.9% over 30 minutes.
 R-IDARAM Indication Secondary CNS lymphoma ICD-10 codes Codes with a prefix C85 Regimen details Day Drug Dose Route 1 Rituximab 375mg/m 2 IV infusion 1 Methotrexate 12.5mg Intrathecal 1 Cytarabine 70mg
R-IDARAM Indication Secondary CNS lymphoma ICD-10 codes Codes with a prefix C85 Regimen details Day Drug Dose Route 1 Rituximab 375mg/m 2 IV infusion 1 Methotrexate 12.5mg Intrathecal 1 Cytarabine 70mg
Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria
 Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria Incidence Diagnosis Prognostic factors Treatment Induction therapy - HSCT Indications for HSCT
Elisabeth Koller 3rd Medical Dept., Center for Hematology and Oncology, Hanusch Hospital, Vienna, Austria Incidence Diagnosis Prognostic factors Treatment Induction therapy - HSCT Indications for HSCT
Form 2011 R4.0: Acute Lymphoblastic Leukemia (ALL) Pre-HCT Data
 Pre-HCT Data") Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Acute myeloid leukemia: prognosis and treatment. Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg
 Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
Burkitt s Lymphoma or DLBCL with adverse features PATIENTS WITH GOOD PERFORMANCE STATUS
 Regimen R-CODOX M Indication Burkitt s Lymphoma or DLBCL with adverse features Therapeutic Intent Radical/Curative PATIENTS WITH GOOD PERFORMANCE STATUS Day Medication Dose Route Administration Details
Regimen R-CODOX M Indication Burkitt s Lymphoma or DLBCL with adverse features Therapeutic Intent Radical/Curative PATIENTS WITH GOOD PERFORMANCE STATUS Day Medication Dose Route Administration Details
Treatment of Thrombocytopenia After Allogeneic Hematopoietic Stem Cell Transplantation with Eltrombopag
 Treatment of Thrombocytopenia After Allogeneic Hematopoietic Stem Cell Transplantation with Eltrombopag Kırık Melya Pelin 1, Gündeş Ilknur 1, Sarıfakıoğulları Serpil 2, Haydaroğlu Handan 2, Pehlivan Mustafa
Treatment of Thrombocytopenia After Allogeneic Hematopoietic Stem Cell Transplantation with Eltrombopag Kırık Melya Pelin 1, Gündeş Ilknur 1, Sarıfakıoğulları Serpil 2, Haydaroğlu Handan 2, Pehlivan Mustafa
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH
 High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH Contents: Page No. 1. Overview 2 2. Admission 3 3. Admission Checklist 5 4. Inpatient management during chemotherapy 6 5. Inpatient
High Intensity Chemotherapy Guidelines for Haematology Patients at ASPH Contents: Page No. 1. Overview 2 2. Admission 3 3. Admission Checklist 5 4. Inpatient management during chemotherapy 6 5. Inpatient
AML 17 Protocol Amendments: Version 7.2 June 2012 to version 8.0 October 2012
 AML 17 Protocol Amendments: Version 7.2 June 2012 to version 8.0 October 2012 Section Original Change Page 1 The trial is open to all patients aged less than 60 years, whether adults or children, and also
AML 17 Protocol Amendments: Version 7.2 June 2012 to version 8.0 October 2012 Section Original Change Page 1 The trial is open to all patients aged less than 60 years, whether adults or children, and also
KYMRIAH (tisagenlecleucel)
") KYMRIAH (tisagenlecleucel) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
KYMRIAH (tisagenlecleucel) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
EBMT2008_22_44:EBMT :29 Pagina 454 CHAPTER 30. HSCT for Hodgkin s lymphoma in adults. A. Sureda
 EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 454 * CHAPTER 30 HSCT for Hodgkin s lymphoma in adults A. Sureda EBMT2008_22_44:EBMT2008 6-11-2008 9:29 Pagina 455 CHAPTER 30 HL in adults 1. Introduction
Scottish Medicines Consortium
 Scottish Medicines Consortium rituximab 10mg/ml concentrate for infusion (MabThera ) Roche (No.330/06) 10 November 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Scottish Medicines Consortium rituximab 10mg/ml concentrate for infusion (MabThera ) Roche (No.330/06) 10 November 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above
Gazyva (obinutuzumab)
") STRENGTH DOSAGE FORM ROUTE GPID 1000mg/40mL Vial Intravenous 35532 MANUFACTURER Genentech, Inc. INDICATION(S) Gazyva (obinutuzumab) is a CD20- directed cytolytic antibody and is indicated, in combination
STRENGTH DOSAGE FORM ROUTE GPID 1000mg/40mL Vial Intravenous 35532 MANUFACTURER Genentech, Inc. INDICATION(S) Gazyva (obinutuzumab) is a CD20- directed cytolytic antibody and is indicated, in combination
Medical Research Council Acute Lymphoblastic Leukaemia Trial XII (UKALL XII) Version 4.1 February 2006
 Version 4.1 February 2006") Medical Research Council Acute Lymphoblastic Leukaemia Trial XII (UKALL XII) Version 4.1 February 2006 Medical Research Council Working Party on Leukaemia in Adults Joint Trial with Eastern Cooperative
Medical Research Council Acute Lymphoblastic Leukaemia Trial XII (UKALL XII) Version 4.1 February 2006 Medical Research Council Working Party on Leukaemia in Adults Joint Trial with Eastern Cooperative
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
FAST FACTS Eligibility Reviewed and Verified By MD/DO/RN/LPN/CRA Date MD/DO/RN/LPN/CRA Date Consent Version Dated
 Page 1 of 8 COG-AALL1131: A Phase III Randomized Trial for Newly Diagnosed High Risk B-Lymphoblastic Leukemia (B-ALL) Including a Stratum Evaluating Dasatinib (IND#73789, NSC#732517) in Patients with Ph-like
Page 1 of 8 COG-AALL1131: A Phase III Randomized Trial for Newly Diagnosed High Risk B-Lymphoblastic Leukemia (B-ALL) Including a Stratum Evaluating Dasatinib (IND#73789, NSC#732517) in Patients with Ph-like
What s a Transplant? What s not?
 What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
4.05 Protocol name: Alemtuzumab (MabCampath ), intravenous
, intravenous") 4.05 Protocol name: (MabCampath ), intravenous Indication Treatment of CLL refractory to fludarabine (either primary i.e. 17p deletion, or secondary i.e. following previous fludarabine treatment), without
4.05 Protocol name: (MabCampath ), intravenous Indication Treatment of CLL refractory to fludarabine (either primary i.e. 17p deletion, or secondary i.e. following previous fludarabine treatment), without
Timing and complications of allogeneic stem cell transplant in Ph + ALL
 Timing and complications of allogeneic stem cell transplant in Ph + ALL Dr Ashlea Campbell Haematology Advanced Trainee Concord Repatriation and General Hospital Royal Prince Alfred Hospital 24 th Feb
Timing and complications of allogeneic stem cell transplant in Ph + ALL Dr Ashlea Campbell Haematology Advanced Trainee Concord Repatriation and General Hospital Royal Prince Alfred Hospital 24 th Feb
Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia
 Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia Policy Number: 8.01.32 Last Review: 7/2018 Origination: 7/2002 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Hematopoietic Cell Transplantation for Acute Lymphoblastic Leukemia Policy Number: 8.01.32 Last Review: 7/2018 Origination: 7/2002 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue
Guideline on the use of minimal residual disease as a clinical endpoint in multiple myeloma studies
 1 2 3 26 July 2018 EMA/CHMP/459559/2018 Committee for Medicinal Products for Human Use (CHMP) 4 5 6 Guideline on the use of minimal residual disease as a clinical endpoint in multiple Draft Draft agreed
1 2 3 26 July 2018 EMA/CHMP/459559/2018 Committee for Medicinal Products for Human Use (CHMP) 4 5 6 Guideline on the use of minimal residual disease as a clinical endpoint in multiple Draft Draft agreed
TRANSPARENCY COMMITTE OPINION. 19 December 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTE OPINION 19 December 2007 ATRIANCE 5 mg/ml, Solution for Infusion Pack of 6 vials (571 348-9) Applicant: GlaxoSmithKline nelarabine
The legally binding text is the original French version TRANSPARENCY COMMITTE OPINION 19 December 2007 ATRIANCE 5 mg/ml, Solution for Infusion Pack of 6 vials (571 348-9) Applicant: GlaxoSmithKline nelarabine
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
: Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
NCCP Chemotherapy Regimen. LEAM Autologous Transplant Conditioning Protocol
 INDICATIONS FOR USE: LEAM Autologous Transplant Conditioning Protocol Regimen *Reimbursement INDICATION ICD10 Code Status Autologous conditioning in non-hodgkins Lymphoma (NHL) C85 00468a Hospital Autologous
INDICATIONS FOR USE: LEAM Autologous Transplant Conditioning Protocol Regimen *Reimbursement INDICATION ICD10 Code Status Autologous conditioning in non-hodgkins Lymphoma (NHL) C85 00468a Hospital Autologous
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma
 UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Supported by a grant from Supported by a grant from UPDATE Autologous Stem Cell Transplantation for Lymphoma and Myeloma Jonathan W.
NCCP Chemotherapy Regimen
 INDICATIONS FOR USE: Azacitidine i INDICATION ICD10 Regimen Code *Reimbursement Status Intermediate-1 and low risk myelodysplastic syndromes (MDS) according to the International Prognostic Scoring System
INDICATIONS FOR USE: Azacitidine i INDICATION ICD10 Regimen Code *Reimbursement Status Intermediate-1 and low risk myelodysplastic syndromes (MDS) according to the International Prognostic Scoring System
MATRIX (Methotrexate, Cytarabine, Thiotepa and Rituximab)
") MATRIX (Methotrexate, Cytarabine, Thiotepa and Rituximab) Indication First line treatment of primary CNS lymphoma. ICD-10 codes Codes with a prefix C85 Regimen details Day Drug Dose Route 1 and 6 Rituximab
MATRIX (Methotrexate, Cytarabine, Thiotepa and Rituximab) Indication First line treatment of primary CNS lymphoma. ICD-10 codes Codes with a prefix C85 Regimen details Day Drug Dose Route 1 and 6 Rituximab
National Institute for Health and Care Excellence. Single Technology Appraisal (STA)
") Single Technology Appraisal (STA) Tisagenlecleucel-T for previously treated B-cell acute lymphoblastic Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please
Single Technology Appraisal (STA) Tisagenlecleucel-T for previously treated B-cell acute lymphoblastic Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Please
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Fludarabine + Cyclophosphamide + Rituximab (FCR) - FLAIR Study
 - FLAIR Study") Fludarabine + Cyclophosphamide + Rituximab (FCR) - FLAIR Study Front-Line therapy in CLL: Assessment of Ibrutinib-containing Regimes. ***See protocol for further details*** Available for Routine Use in
Fludarabine + Cyclophosphamide + Rituximab (FCR) - FLAIR Study Front-Line therapy in CLL: Assessment of Ibrutinib-containing Regimes. ***See protocol for further details*** Available for Routine Use in
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Acute Myeloid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_acute_myeloid_leukemia
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Acute Myeloid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_acute_myeloid_leukemia
BEAM. Lymphoma group OxBMT SCHEDULE SUMMARY. Date:
 xbt SCHEDULE SUARY Date: Day DRUG -7-6 -5-4 -3-2 -1 0 +1 Admission Carmustine (BCNU) Etoposide Cytarabine (Ara-C) elphalan Stem cell infusion Pentamidine* To prevent a specific pneumonia called PCP Cyclizine
xbt SCHEDULE SUARY Date: Day DRUG -7-6 -5-4 -3-2 -1 0 +1 Admission Carmustine (BCNU) Etoposide Cytarabine (Ara-C) elphalan Stem cell infusion Pentamidine* To prevent a specific pneumonia called PCP Cyclizine
Summary of Changes BMT CTN 1101 Version 7.0 to 8.0 Dated: January 18, Original text: Changed to: Rationale
 BMT CTN 1101 RIC ducb vs. Haplo Page 1 of 10 Date: January 20, 2017 Summary of Changes BMT CTN 1101 Version 7.0 to 8.0 Dated: January 18, 2017 A Multi-Center, Phase III, Randomized Trial of Reduced Intensity(RIC)
BMT CTN 1101 RIC ducb vs. Haplo Page 1 of 10 Date: January 20, 2017 Summary of Changes BMT CTN 1101 Version 7.0 to 8.0 Dated: January 18, 2017 A Multi-Center, Phase III, Randomized Trial of Reduced Intensity(RIC)
TRANSPARENCY COMMITTEE OPINION. 14 February 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 February 2007 GLIVEC 100 mg, capsule B/120 capsules (CIP: 358 493-5) GLIVEC 100 mg, capsule B/180 capsules (CIP:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 February 2007 GLIVEC 100 mg, capsule B/120 capsules (CIP: 358 493-5) GLIVEC 100 mg, capsule B/180 capsules (CIP:
National Cancer Intelligence Network Trends in incidence and outcome for haematological cancers in England:
 National Cancer Intelligence Network Trends in incidence and outcome for haematological cancers in England: 2001-2010 Trends in incidence and outcome for haematological cancers in England: 2001-2010 About
National Cancer Intelligence Network Trends in incidence and outcome for haematological cancers in England: 2001-2010 Trends in incidence and outcome for haematological cancers in England: 2001-2010 About
Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day
 28 day") Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day Indication First line treatment of multiple myeloma in patients who are eligible for stem cell transplantation. (NICE TA311) ICD-10 codes Codes with
Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day Indication First line treatment of multiple myeloma in patients who are eligible for stem cell transplantation. (NICE TA311) ICD-10 codes Codes with
National Institute for Health and Care Excellence. Single Technology Appraisal (STA)
") Single Technology Appraisal (STA) Gemtuzumab ozogamacin for untreated de novo acute myeloid leukaemia Response to consultee and commentator comments re-scope Please note: Comments received in the course
Single Technology Appraisal (STA) Gemtuzumab ozogamacin for untreated de novo acute myeloid leukaemia Response to consultee and commentator comments re-scope Please note: Comments received in the course
BR for previously untreated or relapsed CLL
 1 Protocol synopsis Title Rationale Study Objectives Multicentre phase II trial of bendamustine in combination with rituximab for patients with previously untreated or relapsed chronic lymphocytic leukemia
1 Protocol synopsis Title Rationale Study Objectives Multicentre phase II trial of bendamustine in combination with rituximab for patients with previously untreated or relapsed chronic lymphocytic leukemia
MUD HSCT as first line Treatment in Idiopathic SAA. Dr Sujith Samarasinghe Great Ormond Street Hospital for Children, London, UK
 MUD HSCT as first line Treatment in Idiopathic SAA Dr Sujith Samarasinghe Great Ormond Street Hospital for Children, London, UK No Financial Disclosures Guidelines for management of aplastic anaemia British
MUD HSCT as first line Treatment in Idiopathic SAA Dr Sujith Samarasinghe Great Ormond Street Hospital for Children, London, UK No Financial Disclosures Guidelines for management of aplastic anaemia British
AIH, Marseille 30/09/06
 ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
ALLOGENEIC STEM CELL TRANSPLANTATION FOR MYELOID MALIGNANCIES Transplant and Cellular Therapy Unit Institut Paoli Calmettes Inserm U599 Université de la Méditerranée ée Marseille, France AIH, Marseille
3.1 Clinical safety of chimeric or humanized anti-cd25 (ch/anti-cd25)
") 3 Results 3.1 Clinical safety of chimeric or humanized anti-cd25 (ch/anti-cd25) Five infusions of monoclonal IL-2 receptor antibody (anti-cd25) were planned according to protocol between day 0 and day
3 Results 3.1 Clinical safety of chimeric or humanized anti-cd25 (ch/anti-cd25) Five infusions of monoclonal IL-2 receptor antibody (anti-cd25) were planned according to protocol between day 0 and day
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
* Dose may vary dependent on tolerability and co-morbidities
 BC Cancer Protocol Summary for Treatment of Previously Untreated Multiple Myeloma and Not Eligible for Stem Cell Transplant Using Lenalidomide with Low-dose Dexamethasone Protocol Code Tumour Group Contact
BC Cancer Protocol Summary for Treatment of Previously Untreated Multiple Myeloma and Not Eligible for Stem Cell Transplant Using Lenalidomide with Low-dose Dexamethasone Protocol Code Tumour Group Contact
R-ICE Regimen- Rituximab, Etoposide, Ifosfamide (with MESNA), Carboplatin (+ Depocyte if CNS involvement)
, Carboplatin (+ Depocyte if CNS involvement)") R-ICE Regimen- Rituximab, Etoposide, Ifosfamide (with MESNA), Carboplatin (+ Depocyte if CNS involvement) Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case
R-ICE Regimen- Rituximab, Etoposide, Ifosfamide (with MESNA), Carboplatin (+ Depocyte if CNS involvement) Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case
Pharmacy Manual. Cambridge University Hospitals NHS Foundation Trust & University of Cambridge
 Page 1 of 11 Pharmacy Manual Trial Title: PRedicting Outcomes For Crohn s disease using a molecular biomarker (PROFILE) trial EudraCT Number: N/A (non-ctimp study) ISRCTN: 11808228 REC Reference: 17/EE/0382
Page 1 of 11 Pharmacy Manual Trial Title: PRedicting Outcomes For Crohn s disease using a molecular biomarker (PROFILE) trial EudraCT Number: N/A (non-ctimp study) ISRCTN: 11808228 REC Reference: 17/EE/0382
FAST FACTS Eligibility Reviewed and Verified By MD/DO/RN/LPN/CRA Date MD/DO/RN/LPN/CRA Date Consent Version Dated
 Page 1 of 6 COG-AALL1621, A Phase 2 Study of Inotuzumab Ozogamicin (NSC# 772518, IND#133494) in Children and Young Adults with Relapsed or Refractory CD22+ B-Acute Lymphoblastic Leukemia (B-ALL) FAST FACTS
Page 1 of 6 COG-AALL1621, A Phase 2 Study of Inotuzumab Ozogamicin (NSC# 772518, IND#133494) in Children and Young Adults with Relapsed or Refractory CD22+ B-Acute Lymphoblastic Leukemia (B-ALL) FAST FACTS
X M/ (R) Dose adjusted (DA)-EPOCH-R
 Dose adjusted (DA)-EPOCH-R") X M/ (R) adjusted (DA)-EPOCH-R Indication High-risk CD20+ diffuse large B cell lymphoma especially C-MYC and BCL-2 activated (i.e. double hit lymphoma) and mediastinal sclerosing (thymic) large B cell
X M/ (R) adjusted (DA)-EPOCH-R Indication High-risk CD20+ diffuse large B cell lymphoma especially C-MYC and BCL-2 activated (i.e. double hit lymphoma) and mediastinal sclerosing (thymic) large B cell
SUBCUTANEOUS Bortezomib + Thalidomide +Dexamethasone Available for Routine Use in
 SUBCUTANEOUS Bortezomib + Thalidomide +Dexamethasone Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby
SUBCUTANEOUS Bortezomib + Thalidomide +Dexamethasone Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby
PDF of Trial CTRI Website URL -
 Clinical Trial Details (PDF Generation Date :- Wed, 19 Dec 2018 02:45:15 GMT) CTRI Number Last Modified On 25/12/2017 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Clinical Trial Details (PDF Generation Date :- Wed, 19 Dec 2018 02:45:15 GMT) CTRI Number Last Modified On 25/12/2017 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
North West London Cancer Network
 GUIDELINES FOR THE MANAGEMENT OF ADULT ACUTE LEUKAEMIA INITIAL MANAGEMENT CONSIDERATIONS N.B.: If AML is suspected definitively diagnosed, please ensure that the patient is transferred immediately f treatment
GUIDELINES FOR THE MANAGEMENT OF ADULT ACUTE LEUKAEMIA INITIAL MANAGEMENT CONSIDERATIONS N.B.: If AML is suspected definitively diagnosed, please ensure that the patient is transferred immediately f treatment
DF/PCC CHART REVIEW FORM
 DF/PCC CHART REVIEW FORM Date of audit June 19-21, 2002 Protocol number 00-001 Patient s initials Patient s DOB Patient s 00-001 case ID number Patient s institutional MR number Patient s DFCI number Disease
DF/PCC CHART REVIEW FORM Date of audit June 19-21, 2002 Protocol number 00-001 Patient s initials Patient s DOB Patient s 00-001 case ID number Patient s institutional MR number Patient s DFCI number Disease
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Essential Out-of Hours Cancer Chemotherapy
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Essential Out-of Hours Cancer Chemotherapy Version No.: 4.0 Effective From: 27 December 2017 Expiry Date: 27 December 2020 Date Ratified: 19 July
The Newcastle upon Tyne Hospitals NHS Foundation Trust Essential Out-of Hours Cancer Chemotherapy Version No.: 4.0 Effective From: 27 December 2017 Expiry Date: 27 December 2020 Date Ratified: 19 July
OPERATIONS AND PATIENT SERVICES USER GUIDE. Procedures for transplant centres and international establishments
 OPERATIONS AND PATIENT SERVICES USER GUIDE Procedures for transplant centres and international establishments 1. INTRODUCTION 9 1.1. Introduction 9 1.2. User Guide 9 1.3. Services Provided by Anthony Nolan
OPERATIONS AND PATIENT SERVICES USER GUIDE Procedures for transplant centres and international establishments 1. INTRODUCTION 9 1.1. Introduction 9 1.2. User Guide 9 1.3. Services Provided by Anthony Nolan
Bone Marrow Transplantation and the Potential Role of Iomab-B
 Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
Bone Marrow Transplantation and the Potential Role of Iomab-B Hillard M. Lazarus, MD, FACP Professor of Medicine, Director of Novel Cell Therapy Case Western Reserve University 1 Hematopoietic Cell Transplantation
CIBMTR Center Number: CIBMTR Recipient ID: Today s Date: Date of HSCT for which this form is being completed:
 Chronic Myelogenous Leukemia (CML) Post-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic,
Chronic Myelogenous Leukemia (CML) Post-HSCT Data Sequence Number: Date Received: Registry Use Only Today s Date: Date of HSCT for which this form is being completed: HSCT type: autologous allogeneic,
NCCP Chemotherapy Protocol. CHOEP Therapy 21 days. Treatment of T-cell Non-Hodgkins Lymphoma C a
 CHOEP Therapy 21 days INDICATIONS FOR USE: INDICATION ICD10 Protocol Code Treatment of T-cell Non-Hodgkins Lymphoma C85 00396a ELIGIBILTY: Indication as above Age < 60 years Adequate haematological, renal
CHOEP Therapy 21 days INDICATIONS FOR USE: INDICATION ICD10 Protocol Code Treatment of T-cell Non-Hodgkins Lymphoma C85 00396a ELIGIBILTY: Indication as above Age < 60 years Adequate haematological, renal
This is a controlled document and therefore must not be changed
 AZACITIDINE NICE TA218 Treatment of adults not eligible for haematopoietic stem cell transplantation who have: Intermediate-2 and high-risk MDS according to the International Prognostic Scoring System
AZACITIDINE NICE TA218 Treatment of adults not eligible for haematopoietic stem cell transplantation who have: Intermediate-2 and high-risk MDS according to the International Prognostic Scoring System
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 July 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 ANTILYMPHOCYTE GLOBULINS FRESENIUS 20 mg/ml, solution to dilute for infusion 10 glass bottle(s) of 5
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 ANTILYMPHOCYTE GLOBULINS FRESENIUS 20 mg/ml, solution to dilute for infusion 10 glass bottle(s) of 5
Specimen Collection Requirements. Test Name Specimen Type Storage Time Storage Conditions
 1 Specimen Collection Requirements PURPOSE/PRINCIPLE: To outline proper specimen collection for molecular HLA testing, including tube type, minimum specimen amount, proper tube and requisition labeling,
1 Specimen Collection Requirements PURPOSE/PRINCIPLE: To outline proper specimen collection for molecular HLA testing, including tube type, minimum specimen amount, proper tube and requisition labeling,
This is a controlled document and therefore must not be changed or photocopied L.80 - R-CHOP-21 / CHOP-21
 R- / INDICATION Lymphoma Histiocytosis Omit rituximab if CD20-negative. TREATMENT INTENT Disease modification or curative depending on clinical circumstances PRE-ASSESSMENT 1. Ensure histology is confirmed
R- / INDICATION Lymphoma Histiocytosis Omit rituximab if CD20-negative. TREATMENT INTENT Disease modification or curative depending on clinical circumstances PRE-ASSESSMENT 1. Ensure histology is confirmed
An Introduction to Bone Marrow Transplant
 Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
Introduction to Blood Cancers An Introduction to Bone Marrow Transplant Rushang Patel, MD, PhD, FACP Florida Hospital Medical Group S My RBC Plt Gran Polycythemia Vera Essential Thrombocythemia AML, CML,
Research & Development. J H Pacynko and J Illingworth. Research, pharmacy and R&D staff
 Department Title of SOP Research & Development Safety reporting SOP SOP reference no: R&D GCP SOP 07 Authors: Current version number and date: J H Pacynko and J Illingworth Version 9, 31.01.18 Next review
Department Title of SOP Research & Development Safety reporting SOP SOP reference no: R&D GCP SOP 07 Authors: Current version number and date: J H Pacynko and J Illingworth Version 9, 31.01.18 Next review
ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS
 ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS Didier Blaise, MD Transplant and Cellular Therapy Unit (U2T) Department of Hematology Centre de Recherche en Cancérologie, Inserm U891
ALLOGENEIC STEM CELL TRANSPLANTATION FOR ACUTE MYELOBLASTIC LEUKEMIAS Didier Blaise, MD Transplant and Cellular Therapy Unit (U2T) Department of Hematology Centre de Recherche en Cancérologie, Inserm U891
DA-EPOCH-R (Etoposide/Inpatient)
") DA- (Etoposide/Inp) INDICATION High grade lymphoma. Omit rituximab if CD20 negative. PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record
DA- (Etoposide/Inp) INDICATION High grade lymphoma. Omit rituximab if CD20 negative. PRE-ASSESSMENT 1. Ensure histology is confirmed prior to administration of chemotherapy and document in notes. 2. Record
CAALL-F01 OVERVIEW, OUTLINES COMITE LEUCEMIES 19 NOVEMBRE 2015
 CAALL-F01 OVERVIEW, OUTLINES COMITE LEUCEMIES 19 NOVEMBRE 2015 Current outcomes in childhood and adolescent ALL: FRALLE 2000 protocol: 2176 pts; 1-20 years FRALLE Group Event-Free Overall Survival Survival
CAALL-F01 OVERVIEW, OUTLINES COMITE LEUCEMIES 19 NOVEMBRE 2015 Current outcomes in childhood and adolescent ALL: FRALLE 2000 protocol: 2176 pts; 1-20 years FRALLE Group Event-Free Overall Survival Survival
ELIGIBILITY: Newly diagnosed acute promyelocytic leukemia (APL) with high risk (WBC more than 10 x 10 9 /L)
 with high risk (WBC more than 10 x 10 9 /L)") BC Cancer Protocol Summary for First-Line Induction and Consolidation Therapy of Acute Promyelocytic Leukemia Using Arsenic Trioxide, Tretinoin (All-Trans Retinoic Acid) and DAUNOrubicin Protocol Code
BC Cancer Protocol Summary for First-Line Induction and Consolidation Therapy of Acute Promyelocytic Leukemia Using Arsenic Trioxide, Tretinoin (All-Trans Retinoic Acid) and DAUNOrubicin Protocol Code
FLAG-Ida + Gemtuzumab Ozogamicin Regimen (Also known as FLAG-Ida + GO3x2) (AML19 Trial Course 1)
 (AML19 Trial Course 1)") FLAG-Ida + Gemtuzumab Ozogamicin Regimen (Also known as FLAG-Ida + GO3x2) (AML19 Trial Course 1) AML19 Adults with Acute Myeloid Leukaemia or High-Risk Myelodysplastic Syndrome ***Refer to trial protocol
FLAG-Ida + Gemtuzumab Ozogamicin Regimen (Also known as FLAG-Ida + GO3x2) (AML19 Trial Course 1) AML19 Adults with Acute Myeloid Leukaemia or High-Risk Myelodysplastic Syndrome ***Refer to trial protocol
Summary. Olga Zając, Katarzyna Derwich, Katarzyna Stefankiewicz, Jacek Wachowiak. Rep Pract Oncol Radiother, 2007; 12(5):
:") Rep Pract Oncol Radiother, 2007; 12(5): 283-288 Preliminary Communication Received: 2007.03.27 Accepted: 2007.07.24 Published: 2007.10.18 Authors Contribution: A Study Design B Data Collection C Statistical
Rep Pract Oncol Radiother, 2007; 12(5): 283-288 Preliminary Communication Received: 2007.03.27 Accepted: 2007.07.24 Published: 2007.10.18 Authors Contribution: A Study Design B Data Collection C Statistical