Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
|
|
|
- Zoe Edwards
- 5 years ago
- Views:
Transcription

1 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
2 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1. When to do nothing 2. When to watch 3. When to test 4. When to refer 2

3 Ask Google about anemia 3

4 Anemia Symptoms 4
5 When does anemia lead to fatigue? 27% 45% Hematocrit 5
6 6
7 67M with erythrocytosis
8 67M with erythrocytosis WBC HGB HCT MCV PLT DEC He feels great Incidentally discovered on routine labs at physical Vitals: HR 65, BP 122/76, O 2 sat 98% PMH: Hypertension (controlled) 8
9 67M with erythrocytosis A. Recheck CBC in 3 months B. Send a serum erythropoietin C. Send him for a sleep study D. Send him for an echocardiogram E. Send iron studies (Ferritin, Fe, TIBC) 9

10 Erythrocytosis Evaluation 10
11 EPO 1.1 (normal 4-20) Highly suppressed Lab Results JAK2V617F POSITIVE A JAK2 mutation is pathognomonic for a myeloproliferative neoplasm ~99% of polycythemia vera ~50% of essential thrombocythemia 11
12 67M with JAK2+ Polycythemia Vera A. Follow until HCT > 60% B. ASA C. ASA + therapeutic phlebotomy to goal HCT<45% D. ASA + hydrea to goal HCT<45% E. ASA + bone marrow transplant evaluation 12
13 He comes back to see me in 2 months WBC HGB HCT MCV PLT DEC FEB Why is the MCV so high!? 13
14 Now on a stable dose of hydrea WBC HGB HCT MCV PLT DEC FEB APR Remember: Polycythemia Vera is a clonal stem cell disorder, thus affecting all lineages 14
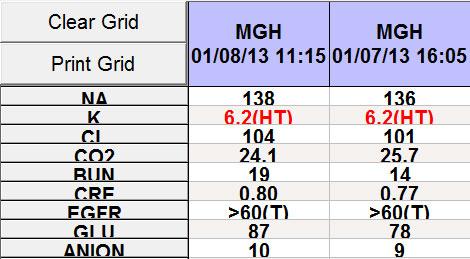
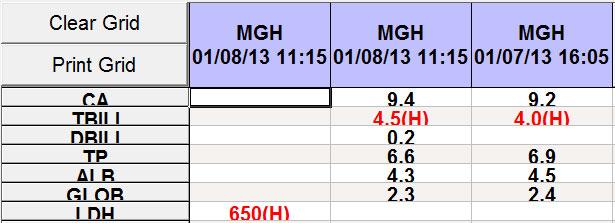
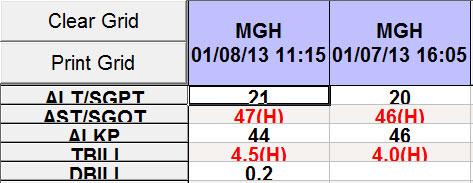
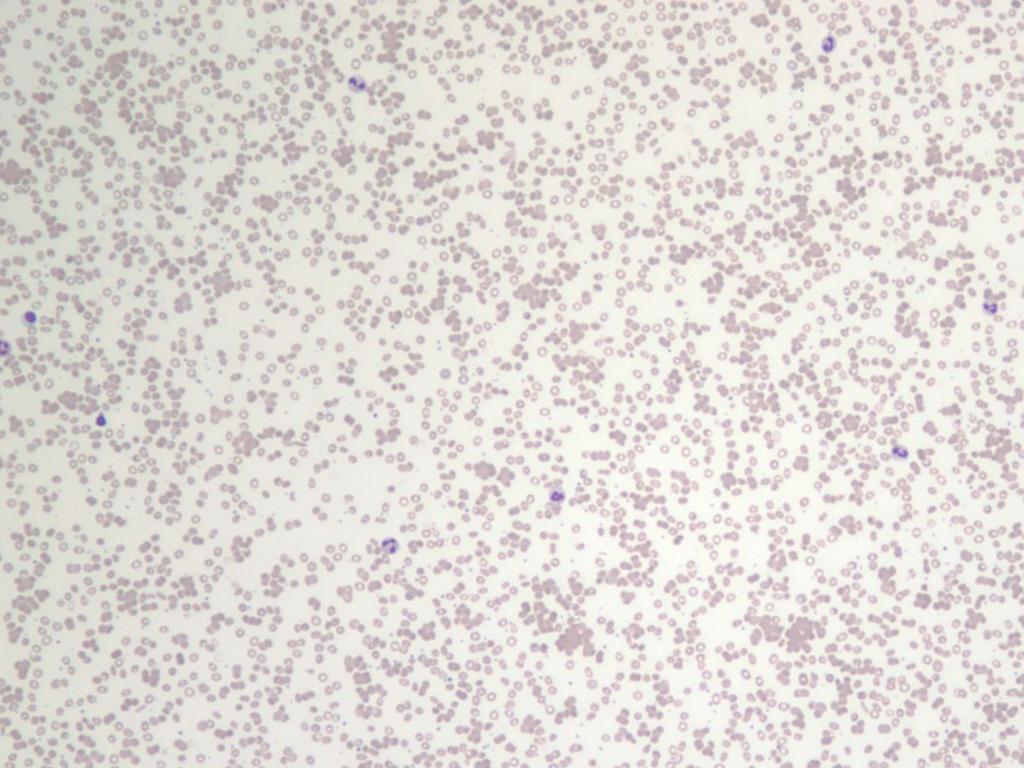
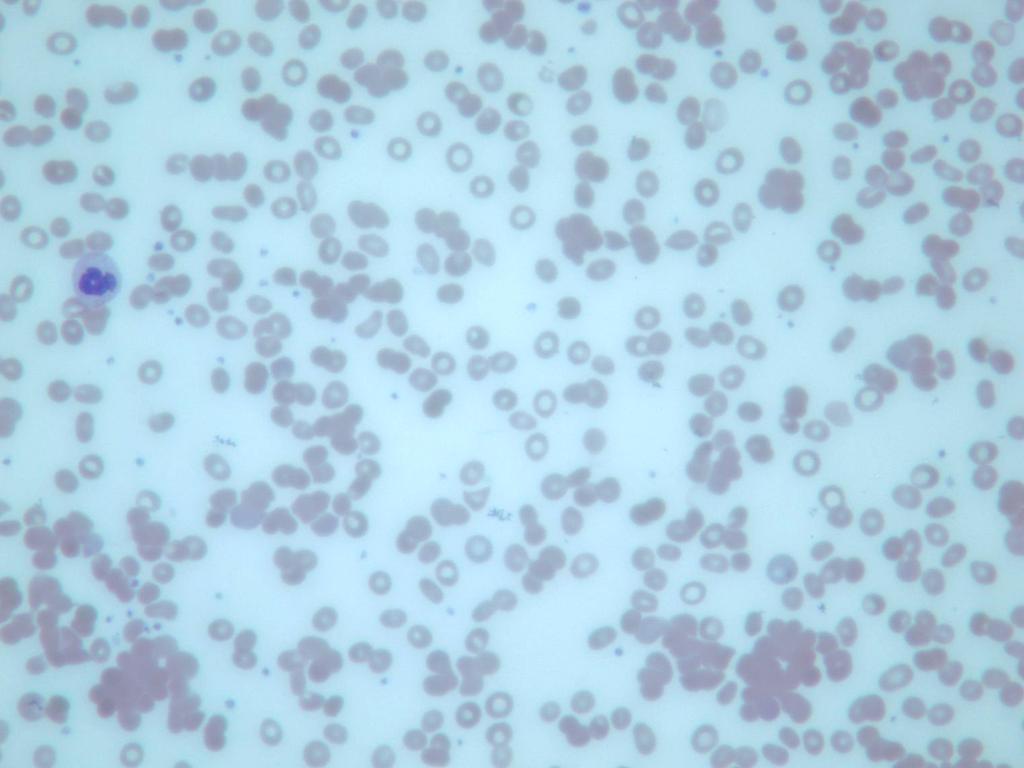
15 65F with anemia

16 65F with anemia 16
17 65F with anemia A. Looks like iron deficiency B. Looks like B12 deficiency C. Looks like chronic kidney disease D. Why is the RDW so wide? E. We need some more labs 17
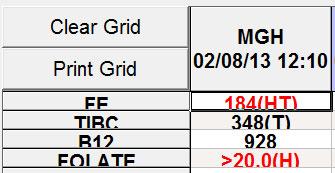
18 65F with anemia CREAT 1.1 BILI 0.1 LDH 282 (normal up to 200) FERRITIN 160 FE 35, TIBC 253 B12 normal FOLATE normal EPO 27 (normal range 3-19) Serum protein electrophoresis: normal 18
19 The trend in the MCV 08/ /
20 65F with anemia and increasing MCV A. Worsening liver disease B. Started a new medication (e.g. methotrexate) C. Drinking more (e.g. toxic effects of alcohol) D. Worsening renal disease despite normal creatinine E. MDS needs a bone marrow biopsy 20
21 Each of us has our own MCV baseline Normocytic is relative to the individual patient Even modest alcohol, especially in older patients, can lead to macrocytosis without anemia
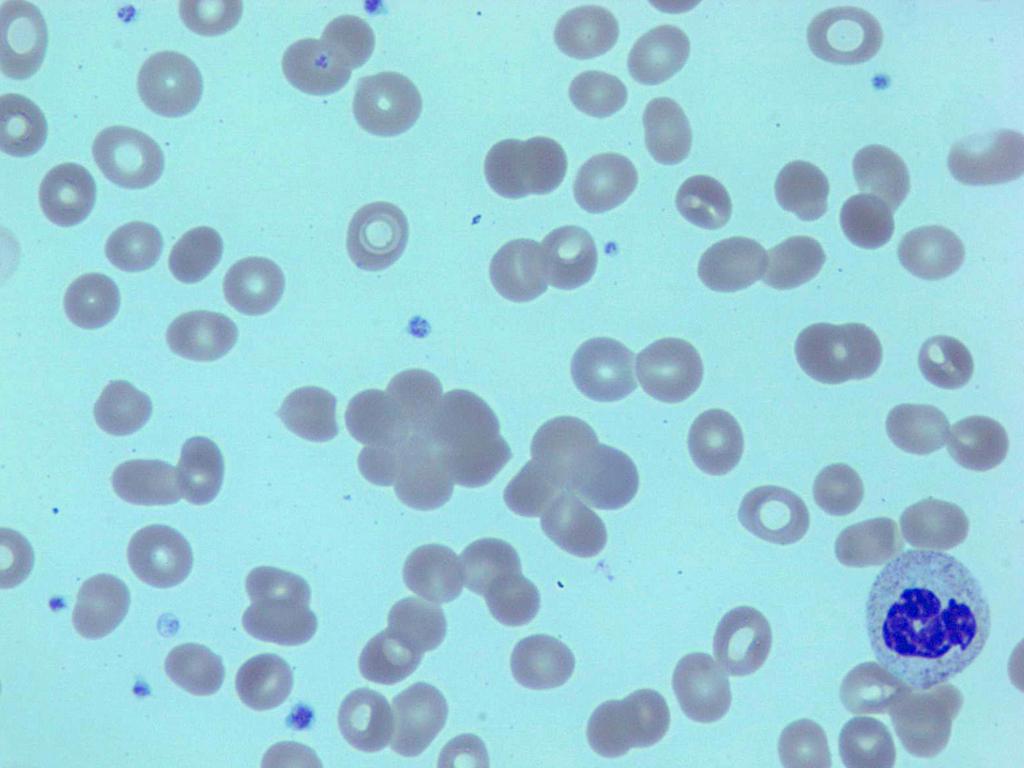
22 34M with a cold
23 34M with a cold Young child in daycare : I caught a cold Felt better, but never quite fully recovered Wife said that he looked a little yellow last week Now in the ED with my heart is racing WBC 7.4, HCT 17.2, MCV 87, PLT 184 BILIRUBIN TOTAL 1.5, DIRECT 0.4 LDH
24 34M with a cold A. Needs a bone marrow biopsy B. Needs a PT, PTT, and Fibrinogen C. Needs a haptoglobin checked D. Expect to see schistocytes on the smear E. Expect to see spherocytes on the smear 24
25 Autoimmune hemolytic anemia BM: would show erythroid hyperplasia PT, PTT, Fibrinogen: should be normal Haptoglobin: would expect it to be low Schistocytes: NO. Spherocytes: YES. 25
26 AIHA A. Start steroids. B. Start steroids and IVIG. C. Check mycoplasma IgG and IgM. D. Send a Coombs test (direct antiglobulin test). E. Check HIV. 26
27 AIHA DAT + : IgG Warm autoantibody IgG Usually idiopathic Can be associated with a lymphoproliferative disease Steroids DAT + : Complement Cold autoantibody IgM Often associated with a mycoplasma infection Self-limited, steroids generally are not helpful 27
28 Trends: LFTs, LDH, WBC, MCV, NRBC, RETIC 3/10 3/3 2/17 2/10 2/1 1/31 1/30 1/29 1/28 1/27 1/25 ALT AST ALKP TBILI DBILI <0.2 <0.2 < LDH WBC HGB HCT MCV PLT RDW NRBC% RETIC >23.0 >
29 A little aside on EPO
30 Erythropoietin Produced in specialized fibroblasts in the kidney Highly responsive to hypoxia Normal range is usually
31
32 HGB=15 HCT=45% EPO=10 32
33 HGB=9 HCT=27% EPO=100 33
34 HGB=6 HCT=18% EPO=
35 What suppresses EPO production? Pretty much everything. Age Renal disease Illness Inflammation Cancer Take care when interpreting an EPO result in a hospitalized patient 35
36 So when is the serum EPO useful? Helpful in the outpatient setting when one is wondering what the contribution of low EPO production is having on the HGB/HCT 81F with CREAT 0.9 and HGB 9.5, HCT 28%, MCV 89 EPO should be If the EPO comes back at 19, though it will be flagged in the normal range, the EPO is actually low given the degree of anemia 36
37 45M with thrombocytopenia
38 45M with thrombocytopenia 38
39 45M with thrombocytopenia A. Probably a transient viral process. B. Probably a medication side-effect. C. Probably ITP (immune thrombocytopenic purpura). D. Probably Aplastic Anemia. E. Probably MDS. F. Probably Acute Leukemia (AML or ALL). 39
40 Context: 45M with thrombocytopenia 45M Time course seems to be going on for a few weeks Concerns: All three lines are low ANC is down Red herrings? Exposures in India 40

41 45M with thrombocytopenia 2-weeks later 41
42 What do we need for work-up? A. HIV, HBC, HCV, CMV, EBV testing. B. Peripheral blood flow cytometry for PNH. C. Coombs test, LDH, Reticulocyte count. D. Bone marrow biopsy. E. Trial of steroids +/- IVIG. 42
43 A D are all correct Suspect aplastic anemia Aplastic anemia is caused by a toxic or autoimmune attack on the hematopoietic stem cell It leads to pancytopenia because of underproduction LDH is typically LOW RETIC is typically <0.5% Rule out destructive processes 43
44 74M with diarrhea and weight loss

45 74M with diarrhea and weight loss CREAT 0.9 BILI 0.6 LDH 260 RETIC 2.4% ALBUMIN 2.9 HIV+ on Rx, suppressed VL and normal CD4 BMI 16 45
46 Anemia is caused by A. Low level of HIV despite treatment B. Co-infection with Hepatitis C C. TTP: Thrombotic Thrombocytopenia Purpura D. Lymphoma infiltration of the bone marrow E. Severe malnutrition 46

47 David BMI 16. Albumin 2.9. Prealbumin 9. Patient 47
48 Marrow aplasia Bone marrow biopsy: <5% cellularity Gelatinous transformation of the bone marrow Seen in cases of AIDS Severe protein malnutrition Anorexia 48
49 56F with anemia and a rejected CBC 49


50 56F with anemia 50

51 56F with anemia
52 What is going on? A. Warm autoimmune hemolytic anemia. B. Paroxysmal Nocturnal Hemoglobinuria. C. Drug-induced hemolytic anemia. D. Cryoglobulinemia. E. Cold agglutinin disease. 52
53 56F with anemia
54
55
56

57 56F with anemia
58 56F with anemia


59 How do you treat cold-agglutinins? A. Steroids. B. IVIG. C. Cytoxan. D. Rituximab. E. Rituximab and Fludarabine. 59

60
61 An intriguing and practical paper on iron absorption 61
62 Recommended daily iron 62
:1981-1989.")
63 Hypothesis: supplemental iron downregulates the body s ability to absorb the next dose of iron Blood. Volume 126(17): October 22, 2015
64 Iron dose vs. Iron absorbed
65 Iron dose vs. Iron absorbed AM Dose PM Dose
66 Feosol Original Ferrous Sulfate 325 mg 20% elemental iron Elemental Fe 65 mg 66
67 Feosol Natural Release Carbonyl iron 100% elemental iron Elemental Fe 45 mg 67

68 Feosol Complete Iron polysaccharide + Heme iron polypeptide Elemental Fe 28 mg 68

69 Ferrous Gluconate Fe Gluconate 240 mg 12% elemental iron Elemental Fe 28 mg 69

70 Ferrous Fumarate Fe Fumarate 54 mg 33% elemental iron Elemental Fe 18 mg 70


71 MegaFood Blood Builder 71
72 So then what to tell our patients? Many of the side effects of iron can be avoided by trying a lower dose formulation Much of the benefit of iron supplementation can be derived from taking them every-other-day I like to start patients on a MON/WED/FRI schedule and see how they do iron of their choice. 72



73 73
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi
.ms4.25.Oct.15 Hemolytic Anemia. Abdallah Abbadi") Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Anemia (3).ms4.25.Oct.15 Hemolytic Anemia Abdallah Abbadi Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k, retics 12%, LDH
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Anemia (3).ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh
.ms Hemolytic Anemia. Abdallah Abbadi Feras Fararjeh") Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Anemia (3).ms4.26.2.18 Hemolytic Anemia Abdallah Abbadi Feras Fararjeh Case 3 24 yr old female presented with anemia syndrome and jaundice. She was found to have splenomegaly. Hb 8, wbc 12k, Plt 212k,
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Approach to the abnormal CBC
 Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
New phase 2 Clinical Trial Enrolling Now
 New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Updates for your practice August 2013 TLALELETSO. HIV & Anemia. Continued on Page 2
 dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
3 Ruba hussein Dr. ahmad Dr. ahmad
 3 Ruba hussein Dr. ahmad Dr. ahmad The arrangement of this sheet differs from that of the record. Anemia of peripheral removal in which we are losing hemoglobin and RBCs mass and the two major Causes are:
3 Ruba hussein Dr. ahmad Dr. ahmad The arrangement of this sheet differs from that of the record. Anemia of peripheral removal in which we are losing hemoglobin and RBCs mass and the two major Causes are:
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
The Irony of Anemia How to interpret the CBC
 Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
New phase 2 Clinical Trial Enrolling Now
 New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
New phase 2 Clinical Trial Enrolling Now Warm Autoimmune Hemolytic Anemia (waiha) and Cold Agglutinin Disease (CAD) Designed for patients Age 18 or older With a primary diagnosis of waiha who had a recurrence,
Does Morphology Matter in 2017
 Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009
 HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
HAEMOLYTIC ANAEMIA Dairion Gatot, Soegiarto Ganie, Savita Handayani. Divisi Hematologi & Onkologi Medik Departemen Ilmu Penyakit Dalam FK-USU/RS H.Adam Malik Medan 2009 WHEN BY THEN Hb 9 g% transfusion
HEMOLY L TIC AN A EMIA
 HEMOLYTIC ANEMIA In a healthy person, a red blood cell survives 90 to 120 days in the circulation, so about 1% of human red blood cells break down each day. The spleen (part of the reticulo-endothelial
HEMOLYTIC ANEMIA In a healthy person, a red blood cell survives 90 to 120 days in the circulation, so about 1% of human red blood cells break down each day. The spleen (part of the reticulo-endothelial
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
The function of the bone marrow. Living with Aplastic Anemia. A Case Study - I. Hypocellular bone marrow failure 5/14/2018
 The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
The function of the bone marrow Larry D. Cripe, MD Indiana University Simon Cancer Center Bone Marrow Stem Cells Mature into Blood Cells Mature Blood Cells and Health Type Function Term Red Cells Carry
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration
 Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Overview of Aplastic Anemia. Overview of Aplastic Anemia. Epidemiology of aplastic anemia. Normal hematopoiesis 10/6/2017
 Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Paroxysmal Nocturnal Hemoglobinuria
 Paroxysmal Nocturnal Hemoglobinuria Barry Skikne MD, FACP, FCP(SA) Professor of Hematology Division of Hematologic Malignancies and Cellular Therapeutics Cardinal Clinical Manifestations PNH Clonal disease
Paroxysmal Nocturnal Hemoglobinuria Barry Skikne MD, FACP, FCP(SA) Professor of Hematology Division of Hematologic Malignancies and Cellular Therapeutics Cardinal Clinical Manifestations PNH Clonal disease
Preferred Clinical Services for Leading Age Florida August 26-27, 2015
 DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
MDS: Who gets it and how is it diagnosed?
 MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
Examination Tests from Pathological Physiology. Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc.
 Examination Tests from Pathological Physiology Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc. Authors: Prof. MUDr. Pavel Maruna, CSc. Doc. MUDr. Martin
Examination Tests from Pathological Physiology Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc. Authors: Prof. MUDr. Pavel Maruna, CSc. Doc. MUDr. Martin
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Anemia In the Insurance Applicant What do the numbers mean?
 Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Updates in the Management of Anemia in Cancer. Taylor M. Ortiz, MD May 19, 2017
 Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL. Revised May 30, 2012
 CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Living with PNH 7/3/2013. Paroxysmal Nocturnal Hemoglobinuria (PNH): A Chronic, Systemic, and Life- Threatening Disease
: A Chronic, Systemic, and Life- Threatening Disease") Living with PNH Laurence A. Boxer, MD University of Michigan Case Study 15 year old awakened in the morning with chest pain and a sore throat. She experienced chest pain all day accompanied with coughing
Living with PNH Laurence A. Boxer, MD University of Michigan Case Study 15 year old awakened in the morning with chest pain and a sore throat. She experienced chest pain all day accompanied with coughing
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
CHERYL KOVALSKI, DO FACOI NO DISCLOSURES ACOI BOARD REVIEW 2018
 CHERYL KOVALSKI, DO FACOI NO DISCLOSURES ACOI BOARD REVIEW 2018 ANEMIA Hemoglobin
CHERYL KOVALSKI, DO FACOI NO DISCLOSURES ACOI BOARD REVIEW 2018 ANEMIA Hemoglobin
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Extra Notes 3. Warm. In the core (center) of the body, where the temperature is 37 C.
 of the body, where the temperature is 37 C.") Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
Extra Notes 3 *The numbers of the slides are according to the last year slides. Slide 33 Autoimmune hemolytic anemia : Abnormal circulating antibodies that target normal antigen on the RBC and cause lysis.
2. Non- hemolytic anemias 3. Normocytic Normochromic Normocytic Normochromic Blood loss. (MCV<80 fl) (MCV fl) (MCV>100 fl)
 (MCV fl) (MCV>100 fl)") Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Case # 1. RBC Loss. CASE #1 (Continued) Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss
 Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss") Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
 Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Hematology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified hematologist
Solving Medical Mysteries Deducing diagnoses from clues in the CBC. Donald S. Houston MD PhD FRCPC
 Solving Medical Mysteries Deducing diagnoses from clues in the CBC Donald S. Houston MD PhD FRCPC Presenter Disclosure Faculty / Speaker s name: Donald S. Houston Relationships with commercial interests:
Solving Medical Mysteries Deducing diagnoses from clues in the CBC Donald S. Houston MD PhD FRCPC Presenter Disclosure Faculty / Speaker s name: Donald S. Houston Relationships with commercial interests:
Lisa B. Weissmann, MD
 Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
APPROACHING TO PANCYTOPENIA
 APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
Hematologic changes in systemic diseases. Chittima Sirijerachai
 Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
Hematologic changes in systemic diseases Chittima Sirijerachai Systemic diseases Infection Renal diseases Liver diseases Connective tissue diseases Malignancy Anemia of chronic disease (ACD) Chronic infections:
(anemia) ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2
 ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2") ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
Deconstructing the CBC
 Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Lisa B. Weissmann, MD
 Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
GOOD MORNING! Thursday, July Heidi Murphy, MD Leslie Carter-King, MD
 GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
GOOD MORNING! Thursday, July 10 2014 Heidi Murphy, MD Leslie Carter-King, MD PREP QUESTION Almost all infants experience a transient increase in bilirubin concentrations known as physiologic jaundice during
Interpreting an Abnormal CBC
 Interpreting an Abnormal CBC Nicholas A. Forward MD, MSc, FRCPC Assistant Professor Division of Hematology Dalhousie University Nick.Forward@nshealth.ca Disclosures No conflicts of interest particularly
Interpreting an Abnormal CBC Nicholas A. Forward MD, MSc, FRCPC Assistant Professor Division of Hematology Dalhousie University Nick.Forward@nshealth.ca Disclosures No conflicts of interest particularly
SOLIRIS (eculizumab) Slide # 1. How do we treat PNH?
 Slide # 1. How do we treat PNH?") Treating PNH How do we treat PNH? Hemolytic anemia Iron, folic acid Transfusion Steroids Eculizumab Thrombosis Coumadin prophylaxis Acute treatment with lytic agents (clot busters) Anticoagulation therapy
Treating PNH How do we treat PNH? Hemolytic anemia Iron, folic acid Transfusion Steroids Eculizumab Thrombosis Coumadin prophylaxis Acute treatment with lytic agents (clot busters) Anticoagulation therapy
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Symptoms and Signs in Hematology (2)/ 2013
/ 2013") Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Dr Anzo William Adiga
 Anemia Dr Anzo William Adiga +256777363201 anzoism2008@gmail.com Definition of Anemia Deficiency in the oxygen-carrying capacity of the blood due to a diminished erythrocyte mass. May be due to: Erythrocyte
Anemia Dr Anzo William Adiga +256777363201 anzoism2008@gmail.com Definition of Anemia Deficiency in the oxygen-carrying capacity of the blood due to a diminished erythrocyte mass. May be due to: Erythrocyte
Clinical implications for decreased lymphocytes (lymphopenia) o Corticosteroid therapy, adrenocortical hyperfunction, stress, shock
 o Corticosteroid therapy, adrenocortical hyperfunction, stress, shock") Learning Objectives At the completion of this program, the participants will be able to: 1. Identify the components of the CBC and Differential and their clinical implications. 2. Identify normal pediatric
Learning Objectives At the completion of this program, the participants will be able to: 1. Identify the components of the CBC and Differential and their clinical implications. 2. Identify normal pediatric
Brrrr, It s Cold In Here
 Brrrr, It s Cold In Here Kate Grogan, MD Transfusion Medicine Fellow Physician, BloodworksNW 4/24/15 Patient 20 year old female Viral illness Presents one week later with severe hemolysis Hgb 5.6 Increased
Brrrr, It s Cold In Here Kate Grogan, MD Transfusion Medicine Fellow Physician, BloodworksNW 4/24/15 Patient 20 year old female Viral illness Presents one week later with severe hemolysis Hgb 5.6 Increased
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY
 THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY INTRODUCTION TO ANEMIA Third year medical students First semester 2018/2019 Dr. RBC DISORDERS Lecturer: Dr. Tariq Al-Adaily Email: TNALADILY@ju.edu.jo
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY INTRODUCTION TO ANEMIA Third year medical students First semester 2018/2019 Dr. RBC DISORDERS Lecturer: Dr. Tariq Al-Adaily Email: TNALADILY@ju.edu.jo
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Bor-Sheng Ko. Hematology Division, Department of Internal Medicine, National Taiwan University Hospital
 Bor-Sheng Ko Hematology Division, Department of Internal Medicine, National Taiwan University Hospital On behalf of Members of Aplastic Anemia Consensus Meeting Diagnosis and classification: Treatment
Bor-Sheng Ko Hematology Division, Department of Internal Medicine, National Taiwan University Hospital On behalf of Members of Aplastic Anemia Consensus Meeting Diagnosis and classification: Treatment
PATTERNS TO EASILY IDENTIFY AND TESTING TO EFFECTIVELY CONFIRM
 PATTERNS TO EASILY IDENTIFY AND TESTING TO EFFECTIVELY CONFIRM WHERE DOES THIS DATA COME FROM? MY EXPERIENCE 3 YEARS REVIEWING CHARTS AT SMMH LITERATURE GUIDELINES PROLOGUE >1000 SMMH BLOOD REVIEWS /YEAR
PATTERNS TO EASILY IDENTIFY AND TESTING TO EFFECTIVELY CONFIRM WHERE DOES THIS DATA COME FROM? MY EXPERIENCE 3 YEARS REVIEWING CHARTS AT SMMH LITERATURE GUIDELINES PROLOGUE >1000 SMMH BLOOD REVIEWS /YEAR
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Challenges in the Laboratory Diagnosis of Anemia
 Challenges in the Laboratory Diagnosis of Anemia Dr. Behzad Poopak, DCLS PhD. Associate Professor of Hematology Islamic Azad University, Tehran Medical Branch Objectives I will review following topics
Challenges in the Laboratory Diagnosis of Anemia Dr. Behzad Poopak, DCLS PhD. Associate Professor of Hematology Islamic Azad University, Tehran Medical Branch Objectives I will review following topics
The Complete Blood Count
 The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
5/5/2010. Goldilocks picture from
 Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Sometimes platelet counts are TOO LOW; Goldilocks and the Three Platelets Robert T. Means, Jr., M.D. Professor & Senior Associate Chair Department of Internal Medicine University of Kentucky Lexington
Evaluation of the Inpatient with Anemia
 Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia
 Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
Evaluation of the Inpatient with Anemia Camila Masias, M.D. Assistant Professor Division of Hematology The Ohio State University Wexner Medical Center Case 1 22 yo woman presents to the ED with fatigue
The University of Mississippi Medical Center The University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 The University of Mississippi Medical Center The University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation June 2012 Objective The goal of this medication use
The University of Mississippi Medical Center The University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation June 2012 Objective The goal of this medication use
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Aplastic Anemia: Understanding your Disease and Treatment Options
 Aplastic Anemia: Understanding your Disease and Treatment Options No financial relationships or commercial interest related to the content of this presentation Josh Sasine, MD, PhD Hematopoietic Cell Transplant
Aplastic Anemia: Understanding your Disease and Treatment Options No financial relationships or commercial interest related to the content of this presentation Josh Sasine, MD, PhD Hematopoietic Cell Transplant
11. An acute leukemia causing. 12. An adult patient presents with acute. 13. Anemia due to renal failure may be
 Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
INVESTIGATION OF ADVERSE TRANSFUSION REACTIONS TABLE OF RECOMMENDED TESTS. Type of Reaction Presentation Recommended Tests Follow-up Tests
 Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Minor Allergic (Urticarial) Urticaria, pruritis, flushing, rash If skin reaction only and mild hives/ rash
Aplastic anamia & Sideroblastic anemia
 Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Diagnostic Approach to Patients with Anemia
 J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Latest updates in Myeloproliferative Neoplasms. Elizabeth Hexner, MD, MSTR
 Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Latest updates in Myeloproliferative Neoplasms Elizabeth Hexner, MD, MSTR Disclosures Nothing to disclose Agenda/Goals Treatment goals in PV Indications for cytoreduction in patients polycythemia vera
Anemia. Tong Chen Department of Hematology Huashan Hospital
 Anemia Tong Chen Department of Hematology Huashan Hospital 1 Content General information of anemia Iron-Deficiency Anemia Aplastic Anemia Hemolytic Anemia 2 Key Points Definition and classification of
Anemia Tong Chen Department of Hematology Huashan Hospital 1 Content General information of anemia Iron-Deficiency Anemia Aplastic Anemia Hemolytic Anemia 2 Key Points Definition and classification of
Pathophysiology 7/18/2012 PAROXYSMAL NOCTURNAL HEMOGLOBINURIA
 PAROXYSMAL NOCTURNAL HEMOGLOBINURIA OUTLINE OF DISCUSSION WHAT IS IT WHO GETS IT NATURAL HISTORY TYPES RISKS COURSE TREATMENTS SYMPTOMS PREGNANCY Pathophysiology Acquired hematopoietic stem cell disorder
PAROXYSMAL NOCTURNAL HEMOGLOBINURIA OUTLINE OF DISCUSSION WHAT IS IT WHO GETS IT NATURAL HISTORY TYPES RISKS COURSE TREATMENTS SYMPTOMS PREGNANCY Pathophysiology Acquired hematopoietic stem cell disorder
When Selfies Go Bad!
 When Selfies Go Bad! Decoding Autoantibodies and Autoimmune Hemolytic Anemia D. Joe Chaffin, MD April 17, 2017 Outline Background Warm autoantibodies and WAIHA Cold autoantibodies and CAD Paroxysmal Cold
When Selfies Go Bad! Decoding Autoantibodies and Autoimmune Hemolytic Anemia D. Joe Chaffin, MD April 17, 2017 Outline Background Warm autoantibodies and WAIHA Cold autoantibodies and CAD Paroxysmal Cold
Aplastic Anemia. is a bone marrow failure disease 9/19/2017. What you need to know about. The 4 major components of blood
 What you need to know about Aplastic Anemia Stuart Goldberg MD Aplastic Anemia is a bone marrow failure disease The bone marrow is the factory that makes blood The 4 major components of blood Red Blood
What you need to know about Aplastic Anemia Stuart Goldberg MD Aplastic Anemia is a bone marrow failure disease The bone marrow is the factory that makes blood The 4 major components of blood Red Blood
MORPHOLOGY IN ACTION. Description MINI-CASE ONE OBJECTIVES. Differential Diagnosis. Laboratory Results
 MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
HOVON 141 CLL. Version 3, 25JUL2018. Table Required investigations at entry, during treatment and during follow up.
 Table 10.2.1 Required investigations at entry, during treatment and during follow up At entry 1 each induction cycle cycle 2 Cycle 3 day 8 and 15 Cycle 4 day1 and 6 cycle 9 day 15 of cycle 15 9 cycle 15:
Table 10.2.1 Required investigations at entry, during treatment and during follow up At entry 1 each induction cycle cycle 2 Cycle 3 day 8 and 15 Cycle 4 day1 and 6 cycle 9 day 15 of cycle 15 9 cycle 15:
Investigation and Management of Chronic Lymphocytic Leukemia. James Johnston
 Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Investigation and Management of Chronic Lymphocytic Leukemia James Johnston Site Specific Clinics CLL Clinic (787-4454) Erin Elphee BN James Johnston Rajat Kumar Matt Seftel (transplant) Myeloma Clinic
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Management of anemia in CKD
 Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
ASPEN MOUNTAIN MEDICAL CENTER. Lab Health Fair
 ASPEN MOUNTAIN MEDICAL CENTER Lab Health Fair GENERAL HEALTH PANEL: CMP CMP The Comprehensive Metabolic Panel is used as a broad screening tool to evaluate organ function and check for conditions such
ASPEN MOUNTAIN MEDICAL CENTER Lab Health Fair GENERAL HEALTH PANEL: CMP CMP The Comprehensive Metabolic Panel is used as a broad screening tool to evaluate organ function and check for conditions such