CANCER SCREENING USPSTF AND BEYOND. DeAnn Cummings, MD March 3, 2018
|
|
|
- Claud Long
- 5 years ago
- Views:
Transcription


1 CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 3, 2018
2 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT primary prevention
3 CASE #1 40 year old African American male in your office for a physical. His wife made him come in. He feels well and has no complaints. ROS completely negative PMH none PSH none Meds - none
4 Social history Smokes ½ ppd for 20 years (trying to quit) No alcohol, no drugs He is an attorney. Married with 2 children CASE #1
5 CASE #1 Family history Father colon polyps at age 50, prostate CA age 60 Mother CAD, HTN, DM Paternal Grandfather colon CA at age 55 Brother age 50 HTN, DM, elevated PSA, has not yet had colonoscopy
6 Physical exam BMI = 33, BP = 130/80, HR = 90 Other than obesity, his exam is normal. Rectal and genital exam not done. CASE #1
7 His wife thinks he should get a PSA. What do you think? CASE #1
8 PROSTATE CANCER SCREENING
9 USPSTF 2017 DRAFT Recommendations Men age shared decision making Men age 70 or greater no screening 2012 Recommendations No screening D What changed their thinking? D C
10 USPSTF 2017 DRAFT Previously the harm of unnecessary testing and treatment outweighed the benefit of finding a cancer early and treating it. New study (ERSPC) Screening prevents 1-2/1000 men from dying from prostate CA and 3/1000 men from developing metastatic CA Urology guidelines now encourage active surveillance of elevated PSA rather than aggressive treatment.
11 AUA GUIDELINES 2013 Recommendations Men age 39 or less No screening Men age IF average risk, no screening. Shared decision making if African American or positive family hx Men age Shared decision making. Consider PSA every 2 years instead of yearly Men age 70 or greater If life expectancy < yrs, do not screen
12 AUA GUIDELINES 2013 Why start screening at 55? 99% deaths from prostate CA occur after age 54 Family history Men with one first degree relative with prostate CA have increased risk by 30%. 3 first degree relatives hereditary form If family member had advanced disease at diagnosis or died of prostate CA, there may be increased benefit from screening.
13 AUA GUIDELINES 2013 African American 44.1 deaths/100,000 vs 19.1 deaths/100,000 for white men Trials had small number of African American patients May be benefit to screening at < age 55 Probably no benefit to screening after age 70
14 AUA GUIDELINES 2013 PSA level and interval of screening If PSA < 1, could screen every 4 years If PSA is 1-4, screen every 2 years For men over 70, if PSA is < 3, can stop screening Rationale for every 2 year instead of yearly screen Less harm from unnecessary testing and treatment No sig reduction in benefit
15 AUA GUIDELINES 2013 Harm For every 1000 men screened 2 serious cardiovascular event 1 DVT or PE 29 erectile dysfunction 18 incontinence 1 death Less serious hematuria, pain, worry, prostatitis
16 CASE #1 Our patient Age 40 African American Father with prostate CA but don t know details Brother with elevated PSA but don t know details
17 How do we have a discussion with our patient? Will we sway him one way or the other? What if he had the same family history but was white? CASE #1
18 COLON CANCER SCREENING
19 USPSTF 2016 All patients age should be offered screening A For patient age consider life expectancy, ability to undergo treatment and hx previous screening. C More benefit in those who have not had regular screening. No point in screening if patient is not in good enough shape for surgery. ABOVE APPLIES TO AVERAGE RISK PATIENTS ONLY
20 US MULTI-SOCIETY TASK FORCE 2017 American College of Gastroenterology American Gastroenterological Association American Society for Gastrointestinal Endoscopy
21 MSTF 2017 Guidelines based on studies that did NOT include patients with inflammatory bowel disease, prior CRC or polyps, or hereditary CRC syndromes (familial polyposis, Lynch syndrome)
22 What are we looking for in screening? Advanced adenoma (70% of all CRC) Lesions 1 cm or more in size Lesions with high grade dysplasia Lesions with villous elements Serrated colorectal lesions (30% of all CRC) Sessile serrated polyps (SSPs) Often flat, less vascular and proximal MSTF 2017
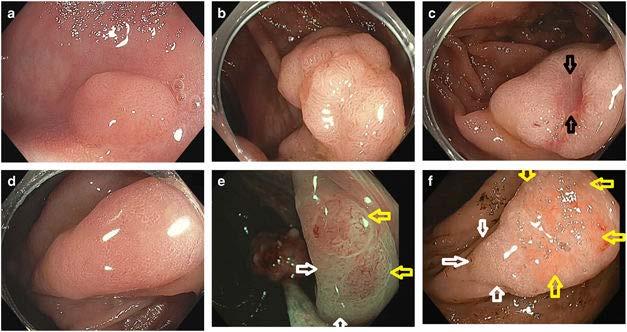
23
24 MSTF 2017 Offer CRC screening for average-risk patients at age 50 (Strong) 3 options for presenting screening test choices Offer multiple screening options (2 or more) Offer sequential ordering of screening tests Risk stratified approach encourage colonoscopy for higher risk patients
25 Screening test options Colonoscopy PROS Potential to diagnose and treat all in one test Won t need additional clean outs! Can find polyps in both right and left colon Can find sessile polyps Screening is less frequent MSTF 2017
26 Screening test options Colonoscopy CONS Need thorough bowel cleansing Risk of perforation (0.5/1000) Risk of bleeding (2.6/1000) Risk of aspiration if sedated Risk of death (2.9/100,000) MSTF 2017
27 MSTF 2017 Screening test options Colonoscopy CONS Operator dependence in performance Adenoma detection rate should be 25% or more Cecal intubation rate 90% or more overall Should use split dose bowel prep (half of prep given on day of colonoscopy) Report afterwards should include photos of the end of the colon and describe bowel prep quality
28 MSTF 2017 Fecal immunochemical test (FIT) PROS No prep! $20 Sensitivity for cancer of 79%, sensitivity for advanced adenoma of 30% FIT test CONS Need yearly testing Poor sensitivity for SSPs (once dysplastic or cancerous, more likely to be picked up
29 MSTF 2017 FIT-fecal DNA test (Cologuard) PROS No prep! Good sensitivity for CRC (92%) 40% sensitivity for SSPs Every 3 year testing FIT-fecal DNA test CONS Decrease in specificity vs FIT alone (86% vs 96%) High cost - $ Higher number of colonoscopies per test
30 MSTF 2017 CT Colonography PROS 82 92% sensitivity for adenomas > 1cm Lower risk of perforation than colonoscopy Testing every 5 years CT Colonography CONS Need for bowel prep (otherwise decreased sensitivity) Difficult to detect small and flat lesions (SSPs) Detection of extracolonic incidental findings Patients with polyps 6 mm or more will need colonoscopy
31 MSTF 2017 Flexible sigmoidoscopy PROS Decreases DISTAL cancer incidence and mortality No need for sedation, less bowel prep, less risk than colonoscopy Screen every 5-10 years (favor 10 years) Flexible sigmoidoscopy CONS Does not detect proximal disease Less patient satisfaction due to no sedation
32 MSTF 2017 Capsule colonoscopy PROS Can be done in patients who should not get sedation 88% sensitivity for adenomas 6 mm or more May avoid risks of colonoscopy Capsule colonoscopy CONS Extensive bowel prep required Cannot detect SSPs Poor reimbursement Will need colonoscopy anyway if positive
33 MSTF 2017 Septin9 serum assay Sensitivity of 48% for detection of CRC No sensitivity for detection of precancerous polyps NOT recommended
34 3 Tiers Tier 1 Colonoscopy every 10 years Annual FIT Tier 2 CT colonography every 5 years FIT-fecal DNA every 3 years Flex sig every 10 years (or every 5 years) Tier 3 Capsule colonoscopy every 5 years MSTF GUIDELINES
35 MSTF GUIDELINES Average risk patients should be offered screening at age 50 (Strong) What about higher risk patients? Family history of CRC or advanced adenomas Cig smoking Diabetes Obesity African American
36 MSTF GUIDELINES 2017 One first degree relative with CRC or a documented advanced adenoma at age < 60 OR two first degree relatives at any age Colonoscopy every 5 years beginning 10 years prior to diagnosis of family member or age 40, whichever is earlier. (Weak)
37 MSTF GUIDELINES 2017 One first degree relative diagnosed at age 60 or greater with CRC or advanced adenoma Colonoscopy every 10 years, starting at age 40 (Weak) One or more first degree relatives with an advanced serrated lesion Same as for advanced adenomas (Weak)
38 MSTF GUIDELINES 2017 Need additional study to know what to do with diabetics, smokers or obese patients African American (CRC at younger age, increased incidence) 2 of the member organizations endorse screening at age 45 even if average risk American College of Physicians endorse screening at age 40
39 MSTF GUIDELINES Increasing incidence of CRC in people < 50 Aggressive evaluation of patients with colorectal symptoms, especially bleeding (Strong) When to stop? Screening may be beneficial up to age 86 if there has not been previous screening but must consider comorbidities and life expectancy. (Weak) Consider stopping at age 75 if pt has had previous screening (Weak)
40 CASE #1 Our patient s father had colon polyps at age 50. He does not know what kind of polyps they were. Grandfather with CRC at age 55 Also a smoker and obese and African American What do you recommend?
41 CASE #2 Polly is a 50 year old white female who presents for a well visit. She, at least initially, has no complaints. She is married with 2 children who are both in college. She works as a nurse in a primary care office. She tells you she just turned 50 and wants to get checked out.
42
43 OUR PATIENT PMH GERD Mild depression PSH Appendectomy Meds Omeprazole x 10 years Prozac x 5 years Multivitamin, vitamin E, calcium, vitamin D, vitamin B12
44 OUR PATIENT Social History Smokes 1 ppd for 30 years Occasional glass of wine No drugs Family History Mom Living. Had MI at age 55. Dad Living. Has COPD. Sister Breast cancer at age 50. Maternal grandmother Ovarian cancer
45 OUR PATIENT GYN History G2P2 Both deliveries were vaginal and at term. First delivery was at age 24. She has used a copper IUD since the birth of her last child. She used oral contraceptives prior to having children. Menarche was at age 11. She has not had her period in 6 months.
46 OUR PATIENT EXAM BP = 120/70, HR = 92, RR = 16, Weight = 125 lbs, Height = 5 5 BMI = 20.8 HEENT unremarkable Skin unremarkable (How thorough are you?) Neck no adenopathy or thyromegaly Lungs decreased breath sounds at bases but clear Heart Regular S1S2, no murmurs Abdomen unremarkable Extremities good pulses, no edema
47 BREAST EXAM Will our patient benefit from a clinical breast exam?
48 BREAST EXAM All recommendations agree that clinical breast exam is not indicated for average-risk women. It may be valuable in high-risk women on a yearly basis. Is our patient high risk?
49 BREAST EXAM Gail assessment tool (IBIS, NCI) Age 50 Menarche 11 years First live birth at years old One first degree relative with breast CA No previous breast biopsy White 2.0% 5-year breast cancer risk compared to 1.3% for average 50 year old (high risk if > 1.7%) 17.9% lifetime risk (high risk if > 15-20%)
50 PELVIC EXAM AND PAP SMEAR Will our patient benefit from a pelvic exam? Does she need a pap smear? She has been seeing her OB-GYN who gets yearly pap smears. She is now coming to you for GYN care. Last pap was one year ago. She has no history of an abnormal pap smear.
51 CERVICAL CANCER SCREENING ASCCP, ACOG and ACS Recommendations Pap and HPV testing every 5 years (preferred) OR pap every 3 years for women 30 years old or more Stop screening at age 65 if adequate prior screening and no CIN 2 or 3 in the past 20 years USPSTF Pap every 3 years OR HPV test every 5 years for women Same recommendation as above for women over 65
52 CERVICAL CANCER SCREENING How do you convince her that she doesn t need pap smears every year? She tells you her GYN told her she is high risk from her family history.
53 CERVICAL CANCER SCREENING How do you convince her that she doesn t need pap smears every year? She tells you her GYN told her she is high risk from her family history.
54 OUR PATIENT You do a clinical breast exam which is normal. You convince her she does not need a pap and pelvic. However, she is very worried about her family history of breast and ovarian cancer. She would like any available tests to help detect these cancers. She has had yearly mammograms since age 40. Does she need genetic testing for BRCA?
55 GENETIC TESTING USPSTF recommends using a screening tool to determine who needs genetic testing Referral Screening Tool, FHS-7 2 first degree relatives with breast CA, one prior to age 50 3 or more first and second degree relatives with breast CA Combo of breast and ovarian CA in first and second degree relatives One first degree relative with bilateral breast CA 2 or more first or second degree relatives with ovarian CA One first or second degree relative with both breast and ovarian CA Breast CA in a male relative Women of Ashkenazi Jewish descent who have a first degree relative with either breast or ovarian CA
56 BREAST CANCER SCREENING Average- risk women Offer/discuss starting mammogram screening at age 40 ACS recommends starting at 45 years Mammogram every 1-2 years for all women yrs USPSTF recommends every 2 years ACS yearly screening more beneficial in women < 55 yrs and consider every other year screening in women over 55 Consider stopping mammograms at age 75 ACOG shared decision-making (July 2017)
57 BREAST CANCER SCREENING BRCA- positive women (ACOG) Clinical breast exam every 6-12 months Yearly MRI at ages After age 30, yearly MRI and mammo Consider prophylaxis (med or surgery) BRCA increases risk of breast CA by 45-65% BRCA increases risk of ovarian CA by 39%
58 BREAST CANCER SCREENING What about high risk women who have negative genetic testing? Recommend yearly mammogram, MRI and CBE if life-time breast CA risk is 20% or more (our patient is 17.9%) ACS consider above if life-time risk is 15-20% If 5 year risk is 1.7% or more, consider tamoxifen or raloxifene prophylaxis (decreases breast CA by 50%) Our patient has a 5 year risk of 2%
59 OVARIAN CANCER SCREENING Transvaginal pelvic ultrasound Sensitive but poor specificity CA 125 Elevated in 50% of early ovarian CA patients Elevated in 80% of advanced ovarian CA patients Specificity = 98-99% Human Epididymis Protein 4 (HE4) Positive in 32% of patients with CA125 negative ovarian CA Symptom Index
60 OVARIAN CANCER SCREENING Symptom Index Bloating or increased abdominal size Abdominal or pelvic pain Difficulty eating or early satiety These symptoms must be new within the last 12 months and occur 12x per month or more. If you have one of these symptoms, consider getting CA 125 and HE4. If either of these is positive, check TVUS.
61 OVARIAN CANCER SCREENING All groups do not recommend screening average-risk women for ovarian CA Ovarian CA has a low incidence (40/100,000) A screening test would need a specificity of 99.6% to get a PPV of 10%. Otherwise there will be too many false positives and therefore too many unnecessary procedures. High risk but BRCA negative High risk, BRCA positive
62 OVARIAN CANCER SCREENING High risk BRCA positive Encourage prophylactic salpingo-oophorectomy if done having children Otherwise expert opinion suggests yearly CA125 and transvaginal pelvic US starting at age 35 Studies are ongoing
63 OVARIAN CANCER SCREENING High risk BRCA negative Does not appear to be any benefit to screening however studies are ongoing.
64 OUR PATIENT She gets tested for BRCA and it is negative. You recommend she continue with yearly mammograms and no ovarian cancer screening. HOWEVER, her risk should be reassessed yearly. She is trying to quit smoking but is concerned about the possibility of lung CA. She has no concerning symptoms. She asks about a CXR or CT chest.
65 LUNG CANCER SCREENING USPSTF 2013 Low dose CT chest at ages for patients with 30 pack year history and currently smoke or quit in the past 15 years
66 OUR PATIENT You advise her to get low dose CT chest at age 55 and educate her about concerning symptoms. You advise her she should get colon CA screening and recommend a colonoscopy. She wants to avoid a colonoscopy at all costs!
CANCER SCREENING USPSTF AND BEYOND. DeAnn Cummings, MD March 9, 2019
 CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 9, 2019 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 9, 2019 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
CANCER SCREENING. Er Chaozer Department of General Medicine, Tan Tock Seng Hospital
 CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening I have no conflicts of interest. Principles of screening. Cancer in the World Page 1. Letting Evidence Be Our Guide
 Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer
 Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Selected Controversies. Cancer Screening. Breast Cancer Screening. Selected Controversies. Page 1. Using Best Evidence to Guide Practice
 Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Guidelines for the Early Detection of Cancer
 Guidelines for the Early Detection of Cancer The American Cancer Society recommends these cancer screening guidelines for most adults. Screening tests are used to find cancer before a person has any symptoms.
Guidelines for the Early Detection of Cancer The American Cancer Society recommends these cancer screening guidelines for most adults. Screening tests are used to find cancer before a person has any symptoms.
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Page 1. Controversies in Cancer Prevention and Screening. Disclosures. Screening. Principles of Screening. I have no conflicts of interest
 Controversies in Cancer Prevention and Screening Disclosures Using the Best Evidence in 2015 I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health
Controversies in Cancer Prevention and Screening Disclosures Using the Best Evidence in 2015 I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health
Screening tests. When you need them and when you don t
 Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Colorectal Cancer Screening
 Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Disclosures. Cancer Screening for Women. Topics for today. But what about? What works? What doesn t? I have no conflicts of interest
 Cancer Screening for Women Disclosures What works? What doesn t? I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health Center of Excellence University
Cancer Screening for Women Disclosures What works? What doesn t? I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health Center of Excellence University
Decoding the USPSTF. By: Dr Vikram Arora Heritage Valley Health System
 Decoding the USPSTF By: Dr Vikram Arora Heritage Valley Health System Objectives O Gain insight into function of USPSTF O Review grading system O Critically appraise key current recommendations of the
Decoding the USPSTF By: Dr Vikram Arora Heritage Valley Health System Objectives O Gain insight into function of USPSTF O Review grading system O Critically appraise key current recommendations of the
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program
 Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Cancer Screening 2009: Setting Evidence-based Priorities
 Cancer Screening 2009: Setting Evidence-based Priorities Eliseo J. Pérez-Stable, MD Professor of Medicine Department of Medicine Division of General Internal Medicine University of California, San Francisco
Cancer Screening 2009: Setting Evidence-based Priorities Eliseo J. Pérez-Stable, MD Professor of Medicine Department of Medicine Division of General Internal Medicine University of California, San Francisco
10/25/2011 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screenin
 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
CVIM s Cancer Screening Practices
 12-13-17 Professional Practice Minutes CVIM s Cancer Screening Practices At CVIM, preventative health care is very important! In these minutes you will find a review of our recommendations for cancer screening
12-13-17 Professional Practice Minutes CVIM s Cancer Screening Practices At CVIM, preventative health care is very important! In these minutes you will find a review of our recommendations for cancer screening
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer
 Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD, MACG 1, C. Richard Boland, MD 2, Jason A. Dominitz,
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD, MACG 1, C. Richard Boland, MD 2, Jason A. Dominitz,
Cancer Facts for Women
 Cancer Facts for Women Some of the cancers that most often affect women are breast, colorectal, endometrial, lung, cervical, skin, and ovarian cancers. Knowing about these cancers and what you can do to
Cancer Facts for Women Some of the cancers that most often affect women are breast, colorectal, endometrial, lung, cervical, skin, and ovarian cancers. Knowing about these cancers and what you can do to
A senior s guide for preventative healthcare services Ynolde F. Smith D.O.
 A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Grand Rounds. Des Moines University. May 5, Durado Brooks, MD, MPH Director, Cancer Control Intervention American Cancer Society
 Grand Rounds Des Moines University May 5, 2016 Durado Brooks, MD, MPH Director, Cancer Control Intervention American Cancer Society Case Summary Mrs. J is a 56 y o w female complaining of always tired;
Grand Rounds Des Moines University May 5, 2016 Durado Brooks, MD, MPH Director, Cancer Control Intervention American Cancer Society Case Summary Mrs. J is a 56 y o w female complaining of always tired;
Screening and Detection in Cancer Survivors. Jose W. Avitia, MD Oncology/Hematology
 Screening and Detection in Cancer Survivors Jose W. Avitia, MD Oncology/Hematology Breast Cancer Summary of 2012 ASCO guideline recommendations for surveillance after breast cancer treatment History/physical
Screening and Detection in Cancer Survivors Jose W. Avitia, MD Oncology/Hematology Breast Cancer Summary of 2012 ASCO guideline recommendations for surveillance after breast cancer treatment History/physical
Cancer Screenings and Early Diagnostics
 Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Cancer Screening & Prevention. Dr. Jamey Burton, MD, FAAFP
 Cancer Screening & Prevention Dr. Jamey Burton, MD, FAAFP Cervical Cancer Breast Cancer Colon Cancer Prostate Cancer Lung Cancer How common is cervical cancer? What causes it? What screening is needed?
Cancer Screening & Prevention Dr. Jamey Burton, MD, FAAFP Cervical Cancer Breast Cancer Colon Cancer Prostate Cancer Lung Cancer How common is cervical cancer? What causes it? What screening is needed?
Evidence-based Cancer Screening & Surveillance
 Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Optima Health. Adult Health Maintenance Guidelines. Guideline History Original Approve Date 04/93
 Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
ONCOLOGY OUTCOMES REPORT
 2017 EVANGELICAL COMMUNITY HOSPITAL ONCOLOGY OUTCOMES REPORT One Hospital Drive, Lewisburg, PA 17837 570-522-2000 evanhospital.com Cancer Screening The Commission on Cancer requires annual dissemination
2017 EVANGELICAL COMMUNITY HOSPITAL ONCOLOGY OUTCOMES REPORT One Hospital Drive, Lewisburg, PA 17837 570-522-2000 evanhospital.com Cancer Screening The Commission on Cancer requires annual dissemination
Colon Cancer Screening and Surveillance. Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011
 Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Updates in Colorectal Cancer Screening & Prevention
 Updates in Colorectal Cancer Screening & Prevention Swati G. Patel, MD MS Assistant Professor of Medicine Division of Gastroenterology & Hepatology Gastrointestinal Cancer Risk and Prevention Clinic University
Updates in Colorectal Cancer Screening & Prevention Swati G. Patel, MD MS Assistant Professor of Medicine Division of Gastroenterology & Hepatology Gastrointestinal Cancer Risk and Prevention Clinic University
Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE
 Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE A key mission for family medicine is preserving health and maximizing
Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE A key mission for family medicine is preserving health and maximizing
Genetic Risk Evaluation and Testing Program
 INSTRUCTIONS: Please complete this form to the best of your ability PRIOR to your appointment. Please remember to list ALL relatives, both living and deceased, regardless of if they have had cancer or
INSTRUCTIONS: Please complete this form to the best of your ability PRIOR to your appointment. Please remember to list ALL relatives, both living and deceased, regardless of if they have had cancer or
10/20/2015. Valerie Ballard, DNP Women s Health Nurse Practitioner
 S.Storm - Dementia Valerie Ballard, DNP Women s Health Nurse Practitioner A WELL VISIT IS PART OF A JOURNEY TO WELLNESS AND HEALTH FOR OUR PATIENTS. As a provider, take the opportunity to listen, teach
S.Storm - Dementia Valerie Ballard, DNP Women s Health Nurse Practitioner A WELL VISIT IS PART OF A JOURNEY TO WELLNESS AND HEALTH FOR OUR PATIENTS. As a provider, take the opportunity to listen, teach
Colorectal Cancer Screening and Surveillance
 1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
Cancer Facts for Men FOR REVIEW ONLY
 Cancer Facts for Men Prostate cancer The chance of getting prostate cancer goes up as a man gets older. Most prostate cancers are found in men over the age of 65. For reasons that are still unknown, African
Cancer Facts for Men Prostate cancer The chance of getting prostate cancer goes up as a man gets older. Most prostate cancers are found in men over the age of 65. For reasons that are still unknown, African
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana
 GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Colorectal Cancer Screening. Paul Berg MD
 Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
THE MODERN GYNECOLOGIC EXAMINATION & SCREENING FOR GYNECOLOGIC MALIGNANCIES
 THE MODERN GYNECOLOGIC EXAMINATION & SCREENING FOR GYNECOLOGIC MALIGNANCIES Denise Uyar, MD Associate Professor OB/GYN Chief Gynecologic Oncology Medical College of Wisconsin April 12, 2019 NO DISCLOSURES
THE MODERN GYNECOLOGIC EXAMINATION & SCREENING FOR GYNECOLOGIC MALIGNANCIES Denise Uyar, MD Associate Professor OB/GYN Chief Gynecologic Oncology Medical College of Wisconsin April 12, 2019 NO DISCLOSURES
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Colon Cancer Screening Past, Present & Future
 Colon Cancer Screening Past, Present & Future Steve Lanspa, MD August 25, 2018 Dr. Lanspa has listed no financial interest/arrangement that would be considered a conflict of interest. Learning Objectives
Colon Cancer Screening Past, Present & Future Steve Lanspa, MD August 25, 2018 Dr. Lanspa has listed no financial interest/arrangement that would be considered a conflict of interest. Learning Objectives
Cancer in Women. Lung cancer. Breast cancer
 Cancer in Women You can get cancer at any age, but it is more likely as you get older. The types of cancer people get and the risk of dying from cancer are not the same for all ethnic groups. Here are
Cancer in Women You can get cancer at any age, but it is more likely as you get older. The types of cancer people get and the risk of dying from cancer are not the same for all ethnic groups. Here are
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
GENERAL COLORECTAL CANCER INFORMATION. What is colorectal cancer?
 GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
AMSER Rad Path Case of the Month: December 2018
 AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
Protect & Detect: What Women should Know about cancer. The American College of Obstetricians and Gynecologists
 Protect & Detect: What Women should Know about cancer The American College of Obstetricians and Gynecologists A Message From ACOG President Kenneth L. Noller, MD Dr. Noller is the Louis E. Phaneuf professor
Protect & Detect: What Women should Know about cancer The American College of Obstetricians and Gynecologists A Message From ACOG President Kenneth L. Noller, MD Dr. Noller is the Louis E. Phaneuf professor
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D
 Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Colorectal Cancer Screening
 Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Cancer Screening 2009: New Tests, New Choices
 Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Financial Disclosers
 Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
11/9/2015 OUTLINE. Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist
 Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Preventive Services Explained
 Preventive Services Explained Medicare covers many preventive care services without charge. Most of these services have been recommended by the U.S. Preventive Services Task Force. However, which beneficiaries
Preventive Services Explained Medicare covers many preventive care services without charge. Most of these services have been recommended by the U.S. Preventive Services Task Force. However, which beneficiaries
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer
 1016 CLINICAL GUIDELINES CME Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD 1, C. R i chard B ol
1016 CLINICAL GUIDELINES CME Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer Douglas K. Rex, MD 1, C. R i chard B ol
Cancer Prevention and Early Detection Worksheet for Women
 Page 1 of 8 Cancer Prevention and Early Detection Worksheet for Women While a tremendous amount of progress has been made in cancer research, we still don t understand exactly what causes most cancers.
Page 1 of 8 Cancer Prevention and Early Detection Worksheet for Women While a tremendous amount of progress has been made in cancer research, we still don t understand exactly what causes most cancers.
Medicare Wellness. Meggan Robinson, DO MAOFP Spring Update 4/23/16
 Medicare Wellness Meggan Robinson, DO MAOFP Spring Update 4/23/16 Objectives History of Medicare Wellness Exam Identify the goals of the Wellness exam Differentiate the different types of Wellness exams
Medicare Wellness Meggan Robinson, DO MAOFP Spring Update 4/23/16 Objectives History of Medicare Wellness Exam Identify the goals of the Wellness exam Differentiate the different types of Wellness exams
The Guidelines Guide: Routine Adult Screening Created March 2009 by Alana Benjamin, MD Last updated: June 29 th, 2010
 The Guidelines Guide: Routine Adult Screening Created March 2009 by Alana Benjamin, MD Last updated: June 29 th, 2010 Table of Contents Topic Page Introduction 2 Abbreviations 2 USPSTF Grades of Recommendations
The Guidelines Guide: Routine Adult Screening Created March 2009 by Alana Benjamin, MD Last updated: June 29 th, 2010 Table of Contents Topic Page Introduction 2 Abbreviations 2 USPSTF Grades of Recommendations
This information explains the advice about familial breast cancer (breast cancer in the family) that is set out in NICE guideline CG164.
 that is set out in NICE guideline CG164.") Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Let s look a minute at the evidence supporting current cancer screening recommendations.
 I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
What is Colorectal Cancer?
 COLORECTAL CANCER (CRC) What is Colorectal Cancer? Colorectal cancer (also known as colon cancer) is cancer of the colon and/or rectum and occurs when a growth in the lining of the colon or rectum becomes
COLORECTAL CANCER (CRC) What is Colorectal Cancer? Colorectal cancer (also known as colon cancer) is cancer of the colon and/or rectum and occurs when a growth in the lining of the colon or rectum becomes
SIGNS, SYMPTOMS AND SCREENING GUIDELINES
 SIGNS, SYMPTOMS AND SCREENING GUIDELINES SIGNS AND SYMPTOMS You may think it s normal, but it could be a sign or symptom of an illness or cancer-related disease. If you are experiencing any of these signs
SIGNS, SYMPTOMS AND SCREENING GUIDELINES SIGNS AND SYMPTOMS You may think it s normal, but it could be a sign or symptom of an illness or cancer-related disease. If you are experiencing any of these signs
The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening
 The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening By Marsha Fountain, RN, MSN The
The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening By Marsha Fountain, RN, MSN The
Member Newsletter Vol. 1, What cancer screenings should I get? AETNA BETTER HEALTH OF MISSOURI. Early detection can lower your risk
 AETNA BETTER HEALTH OF MISSOURI Member Newsletter Vol. 1, 2016 What cancer screenings should I get? Early detection can lower your risk Cancer screenings can help detect cancer in the early stages. Early
AETNA BETTER HEALTH OF MISSOURI Member Newsletter Vol. 1, 2016 What cancer screenings should I get? Early detection can lower your risk Cancer screenings can help detect cancer in the early stages. Early
A patient s guide to understanding. Cancer. Screening
 A patient s guide to understanding Cancer Screening Contents 04 06 10 12 Cancer Screening Who Should Go For Cancer Screening 05 Nasopharyngeal Carcinoma Colorectal Cancer 08 Lung Cancer Liver Cancer Breast
A patient s guide to understanding Cancer Screening Contents 04 06 10 12 Cancer Screening Who Should Go For Cancer Screening 05 Nasopharyngeal Carcinoma Colorectal Cancer 08 Lung Cancer Liver Cancer Breast
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64
 Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
Preventive Care Guideline for Asymptomatic Low Risk Adults Age 18 through 64 1. BMI - Documented in patients medical record on an annual basis. Screen for obesity and offer intensive counseling and behavioral
Improving Outcomes in Colorectal Cancer: The Science of Screening. Colorectal Cancer (CRC)
") Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families
 Information for individuals and families") Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast and Ovarian Cancer is a genetic condition which
Hereditary Breast and Ovarian Cancer (HBOC) Information for individuals and families What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast and Ovarian Cancer is a genetic condition which
Removing Unnecessary Barriers to Contraceptive Services
 Title X Grantee Meeting July 31, 2013 Seattle, WA Removing Unnecessary Barriers to Contraceptive Services Michael Policar, MD, MPH Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine policarm@obgyn.ucsf.edu
Title X Grantee Meeting July 31, 2013 Seattle, WA Removing Unnecessary Barriers to Contraceptive Services Michael Policar, MD, MPH Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine policarm@obgyn.ucsf.edu
WALNUT CREEK FAMILY PRACTICE 4303 JODECO ROAD MCDONOUGH, GA
 WALNUT CREEK FAMILY PRACTICE 4303 JODECO ROAD MCDONOUGH, GA 30253 770-898-7840 Dear Walnut Creek Family Practice Patient, Your physical appointment is scheduled for you and no one else at that time. If
WALNUT CREEK FAMILY PRACTICE 4303 JODECO ROAD MCDONOUGH, GA 30253 770-898-7840 Dear Walnut Creek Family Practice Patient, Your physical appointment is scheduled for you and no one else at that time. If
2019 Adult Preventive Health Guidelines
 1 2019 Adult Preventive Health Guidelines Important Note Health Net s Preventive Health Guidelines provide Health Net members and practitioners with recommendations for preventive care services for the
1 2019 Adult Preventive Health Guidelines Important Note Health Net s Preventive Health Guidelines provide Health Net members and practitioners with recommendations for preventive care services for the
Summary of Cancer Prevention and Screening Benefits of the Affordable Care Act (ACA) in Kentucky (includes kynect)
 in Kentucky (includes kynect)") Summary of Cancer Prevention and Screening Benefits of the Talk with patients about ü Potential benefits, harms, and uncertainties of cancer screening ü Identify family history ü Cancer prevention, early
Summary of Cancer Prevention and Screening Benefits of the Talk with patients about ü Potential benefits, harms, and uncertainties of cancer screening ü Identify family history ü Cancer prevention, early
Name: Today s Date: Address: State, Zip Code
 New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
New Patient Health History Questionnaire Name: Today s Date: Address: City State, Zip Code Email Address: Date of Birth: Home Telephone #: Cell Number: Work Number: Emergency Contact name & number: Referred
Medicare Preventive Services Calendar. Please punch hole to hang calendar
 2016 Printer Medicare Preventive Services Calendar instructions: Please punch hole to hang calendar Welcome to Medicare Visit During the first 12 months that you have Part B, you can get a Welcome to Medicare
2016 Printer Medicare Preventive Services Calendar instructions: Please punch hole to hang calendar Welcome to Medicare Visit During the first 12 months that you have Part B, you can get a Welcome to Medicare
Chapter 7 Section 2.2. Clinical Preventive Services - TRICARE Prime
 Medicine Chapter 7 Section 2.2 Issue Date: May 15, 1996 Authority: 32 CFR 199.17 1.0 POLICY 1.1 TRICARE Prime enrollees may receive Prime Clinical Preventive Services from any network provider without
Medicine Chapter 7 Section 2.2 Issue Date: May 15, 1996 Authority: 32 CFR 199.17 1.0 POLICY 1.1 TRICARE Prime enrollees may receive Prime Clinical Preventive Services from any network provider without
History and Physical Description References
 : Ages 19 through 64 Years The Patient Protection and Affordable Care Act (PPACA, P.L. 111-148, March 23, 2010, as amended) requires, among other things, coverage of all A and B Recommendations as promulgated
: Ages 19 through 64 Years The Patient Protection and Affordable Care Act (PPACA, P.L. 111-148, March 23, 2010, as amended) requires, among other things, coverage of all A and B Recommendations as promulgated
Colorectal Cancer Screening in Ohio CHCs. Ohio Association of Community Health Centers
 Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Increasing Colorectal Cancer Screening in Wyoming. Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program
 Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
PREVENTION CARE IN ADULTS
 PREVENTION CARE IN ADULTS Hong Xiao, M.D. Department of Family & Community Medicine Weight and BMI Abdominal Aortic Aneurysm (AAA) Blood Pressure Breast Exam Breast Cancer Mammogram Breast Cancer BRCA
PREVENTION CARE IN ADULTS Hong Xiao, M.D. Department of Family & Community Medicine Weight and BMI Abdominal Aortic Aneurysm (AAA) Blood Pressure Breast Exam Breast Cancer Mammogram Breast Cancer BRCA
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond.
 HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
1. USPSTF (1996) Updated The expert consensus opinion of the 2004 PH Committee. 3. ACOG (2006)
 Updated The expert consensus opinion of the 2004 PH Committee. 3. ACOG (2006)") : Ages 19 through 64 Years The Patient Protection and Affordable Care Act (PPACA, P.L. 111-148, March 23, 2010, as amended) requires, among other things, coverage of all A and B Recommendations as promulgated
: Ages 19 through 64 Years The Patient Protection and Affordable Care Act (PPACA, P.L. 111-148, March 23, 2010, as amended) requires, among other things, coverage of all A and B Recommendations as promulgated
However, I sometimes hike in Kapu areas.!
 Cancer Screening for Women: Updates and Controversies Rebecca Jackson, MD Professor, Ob/Gyn & Reproductive Sciences Epidemiology & Biostatistics University of California, San Francisco Disclosures I have
Cancer Screening for Women: Updates and Controversies Rebecca Jackson, MD Professor, Ob/Gyn & Reproductive Sciences Epidemiology & Biostatistics University of California, San Francisco Disclosures I have
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 7 Section 2.1. Clinical Preventive Services - TRICARE Standard
 Medicine Chapter 7 Section 2.1 Issue Date: April 19, 1983 Authority: 32 CFR 199.4(e)(28) and (f)(12), 10 USC 1079(a), Public Law 110-471, Section 711 1.0 CPT 1 PROCEDURE CODES 45300-45305, 45308-45315,
Medicine Chapter 7 Section 2.1 Issue Date: April 19, 1983 Authority: 32 CFR 199.4(e)(28) and (f)(12), 10 USC 1079(a), Public Law 110-471, Section 711 1.0 CPT 1 PROCEDURE CODES 45300-45305, 45308-45315,
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
HEALTH HISTORY QUESTIONNAIRE. Family Risk Assessment Program
 HEALTH HISTORY QUESTIONNAIRE Family Risk Assessment Program Name DOB Current Age Address Home Phone Cell Phone Business Phone Best time to contact you Day Evening E-mail Address (Email will only be used
HEALTH HISTORY QUESTIONNAIRE Family Risk Assessment Program Name DOB Current Age Address Home Phone Cell Phone Business Phone Best time to contact you Day Evening E-mail Address (Email will only be used
Summary of Cancer Prevention and Screening Benefits of the Affordable Care Act (ACA) in Kentucky for health professionals
 in Kentucky for health professionals") Summary of Cancer Prevention and Screening Benefits of the Affordable Care Act (ACA) in Kentucky for health professionals Talk with patients about ü Cancer Prevention & Early Detection ü Benefits, harms
Summary of Cancer Prevention and Screening Benefits of the Affordable Care Act (ACA) in Kentucky for health professionals Talk with patients about ü Cancer Prevention & Early Detection ü Benefits, harms
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
2017 Preventive Health Care Guidelines Free preventive care to help you be your healthiest.
 2017 Preventive Health Care Guidelines Free preventive care to help you be your healthiest. Guidelines may change throughout the year based on new research and recommendations. Get the most up-to-date
2017 Preventive Health Care Guidelines Free preventive care to help you be your healthiest. Guidelines may change throughout the year based on new research and recommendations. Get the most up-to-date