Pancreatic Adenocarcinoma
|
|
|
- Sylvia Walsh
- 5 years ago
- Views:
Transcription
1 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018

2 Percentage alive 5 years after diagnosis for men and women
3 Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death At diagnosis, 50% have metastatic disease, 30% locally advanced disease and 20% operable disease 1 year survival overall is 24% and 5 year is 5% Median age at diagnosis is 69 in men and 65 in women
4 Risk factors for pancreatic adenocarcinoma Genetic syndromes BRCA2 (Up to 10% in Ashkenazi Jews with pancreas ca) Lynch Syndrome (MSI-H) PALB2 Familial pancreatic adenocarcinoma Peutz Jeghers Syndrome p16ink4 (melanoma and pancreas ca) CF and SPINK1 mutations (familial pancreatitis and pancreatic adenocarcinoma) Smoking Chronic pancreatitis (GS and ETOH) Pancreatic Cystadenoma (mucinous and serous) IPMN. Intrapanctreatic mucinous neoplasia
: 495 501")
5 BRCAish and high levels of neo-antigen do better, studies ongoing with PARP inhibitors Nature February 26; 518(7540):
6 Presentation of pancreas adenocarcinoma Painless obstructive jaundice Most common (75% of adenocarcinomas are in head of pancreas) Due to obstruction of common bile duct Diabetes (often insulin dependent) or worsening/brittle diabetes Lipid malabsorption Metastatic disease symptoms Loss of weight Nausea Pain: Often poorly localized, epigastric back. May take a long time to make diagnosis.

7 Dilatation of the common bile duct PCPA Advanced Trainee Program 2018

8 Double duct sign PCPA Advanced Trainee Program 2018
9 Investigation imaging Pancreatic protocol CT (+staging CT) Most accurate way to stage pancreatic adenocarcinoma Double duct sign MRCP to delineate duct anatomy Not always necessary If unsure about stenting or site of obstruction Endoscopic ultrasound Allows staging as well as biopsy FNA only Increasingly commonly used for inoperable disease for biopsy or operable disease to stage Biopsy Increasingly EUS Not necessary if surgery is planned and CT highly suggestive
10 Other Investigation LFTs, if bilirubin not too high immediate surgery is favourable CA19.9 Definitions of operability vary widely Borderline operable no standard definition
11 Post-operative complications Anastomotic/bile leak Malabsorption Brittle diabetes Pancreatitis Failure to thrive May lead to long delays prior to adjuvant therapy and preclude some from receiving it.
12 Adjuvant therapy PCPA Advanced Trainee Program 2018
13 Adjuvant therapies in pancreatic adenocarcinoma Chemotherapy ESPAC 1 Chemotherapy vs chemoradiotherapy vs nil CONKO1 Gemcitabine vs nil ESPAC 3 Gemcitabine vs 5FU ESPAC 4 Gemcitabine vs Gemcitabine plus capecitabine Radiotherapy GITSG RTOG 9704 EORTC
14 20.1 vs 15.5 mo Final ESPAC1 results Original 2 x 2 randomisation only Chemoradiotherapy detrimental Lancet Nov 10;358(9293): JAMA Sep 8;304(10):
15 CONKO1 Oettle et al, JAMA, Vol. 297 No. 3, January 17, 2007
16 CONKO DFS Gemcitabine Observation Node months 11.2 months Node months 7.0 months R0 resection 14.0 months 7.9 months R1 resection 14.5 months 5.5 months Oettle et al, JAMA, Vol. 297 No. 3, January 17, 2007
17 ESPAC 3 Results Received no chemotherapy Completed chemotherapy Grade 3/4 diarrhoea Grade 3/4 stomatitis Grade 3/4 neutropenia Gemcitabine 5FU P value 10% 11% 60% 55% 2% 13% 0% 10% 22% 22% PFS 14.3 months 14.1 months 0.44 Median OS 23.6 months 23 months 0.39 JAMA Jul 11;308(2):147-56

18 ESPAC 3 PCPA Advanced Trainee Program 2018

19 106 sites, Not a highly selected population: 60% R1, 80% node +ve

20 2 drugs better than 1 PCPA Advanced Trainee Program year OS 28.8 v 16.3 months
21 ESPAC 4

22 ESPAC trials 5 year OS 8% => 17% => 29% PCPA Advanced Trainee Program 2018

23 Toxicity only moderately increased PCPA Advanced Trainee Program 2018
24 Chemoradiotherapy PCPA Advanced Trainee Program 2018 Trial GITSG 1985 Pt no. RT Chemotx Median OS P value 43 2 x 20Gy Bolus 5FU during and after RT 20 vs 11 months EORTC 1999 RTOG * x 20Gy CI 5FU only during RT Gy continuous CI 5FU during RT (all) 4 mo of gem vs 4 mo of CI 5FU 17.1 vs 12.6 months 18.8 vs.16.9 months Ann Surg Oncol May;18(5):
25 Is there a role for chemoradiotherapy post surgery for pancreatic adenocarcinoma today? Controversial No large randomised studies supporting the approach Study of National Cancer Data Base showed advantage in N+ and R1 resection Will not generally be curative in such patients (some anecdotes) Reduces local recurrence but not distant recurrence Increases toxicity compared to Chemotherapy alone? Save RT for treatment of symptoms due to local relapse Cancer Dec 1;121(23):4141-9
26 Neoadjuvant therapy PCPA Advanced Trainee Program 2018 Gillen et al PLoS Med April; 7(4)
27
28 Neo-adjuvant chemotherapy for operable pancreatic adenocarcinoma No randomised trials CT and CRT approaches in retrospective and small prospective series Not to be confused with downstaging to operability (operable vs borderline) May spare some major surgery Risks of sepsis/blockage due to stent
29 ASCO 2017 Recommendations Recommendation 2.1: Primary surgical resection of the primary tumor and regional lymph nodes is recommended for patients who meet all of the following criteria: no clinical evidence for metastatic disease, performance status and comorbidity profile appropriate for a major abdominal operation, no radiographic interface between primary tumor and mesenteric vasculature on high-definition cross-sectional imaging, and a CA 19-9 level (in absence of jaundice) suggestive of potentially curable disease (Type: evidence based, benefits outweigh harms; Evidence quality: intermediate; Strength of recommendation: strong). Recommendation 3.1: Preoperative therapy is recommended for patients with pancreatic cancer who meet any of the following criteria: radiographic findings suspicious but not diagnostic for extrapancreatic disease, a performance status or comorbidity profile not currently appropriate (but potentially reversible) for a major abdominal operation, a radiographic interface between primary tumor and mesenteric vasculature on cross-sectional imaging that does not meet appropriate criteria for primary resection or a CA 19-9 level (in absence of jaundice) suggestive of disseminated disease (Type: evidence based, benefits outweigh harms; Evidence quality: low; Strength of recommendation: strong). Recommendation 3.2: Preoperative therapy should be offered as an alternative treatment strategy for any patient who meets all criteria in Recommendation 2.1 (Type: evidence based, benefits outweigh harms; Evidence quality: low; Strength of recommendation: strong). JCO VOLUME 35 NUMBER 20 JULY 10, 2017
30 Locally Advanced/Inoperable pancreatic adenocarcinoma Heterogeneous presentations to the oncologist Failed resection ± surgical bypass Obviously inoperable on CT ± stent inserted Too old/infirm for surgery Symptomatic pain, LOW Completely asymptomatic and bypassed/stented One approach does not fit all
31 Locally advanced disease Chemotherapy Gemcitabine Paclitaxel NAB FOLFIRINOX and derivatives Chemoradiotherapy with 5FU, capecitabine or gemcitabine Both Currently chemotherapy is standard, use of radiotherapy decreasing Radiotherapy still used for pain control

32 LAP07 Study PCPA Advanced Trainee Program 2018
33 LAP 07 chemotherapy vs chemotherapy then chemoradiotherapy PCPA Advanced Trainee Program 2018
34 Metastatic pancreas ca For 10 years standard of care = gemcitabine FOLFIRINOX Oxaliplatin, irinotecan, 5FU. 5 months increased median overall survival Increased rate of sepsis (stents = cholangitis) 2013 Gemcitabine plus Paclitaxel NAB 3 month OS advantage compared to gemcitabine Need to balance toxicity/qol vs survival. In Australia Paclitaxel NAB only on the PBS for first line use Conroy T et al. NEJM 2011;;364: Von Hoff DD, et al. N Engl J Med Oct 16

35 Biologicals? PCPA Advanced Trainee Program 2018 = p>0.05 for biological
36 Overall Survival for All Patients HR = 0.81* 95%CI P=0.025 Gemcitabine + Erlotinib Median = 6.37 months 1 year survival = 24% Gemcitabine + Placebo Median = 5.91 months 1 year survival = 17% * Adjusted for PS, pain and disease extent at randomization

37 New Targets PARPi CD4/6 inhibitors CSFR1 inhibitors Pegylated recombinant Human hyaluronidase Immunotherapies

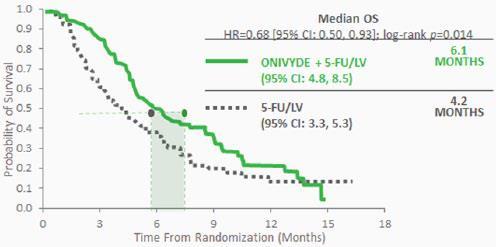
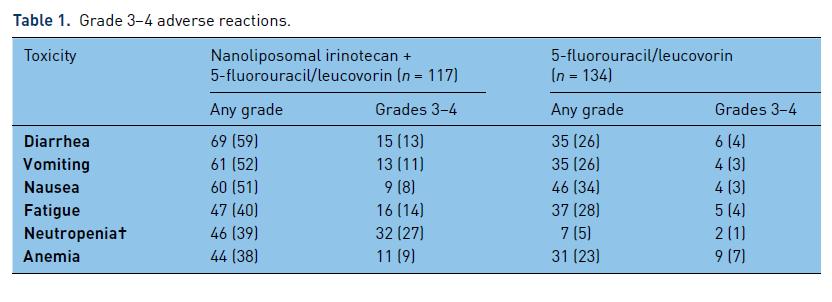
38 NAPOLI-1 study, liposomal irinotecan Ther Adv Gastroenterol 2017, Vol. 10(7)
39
40 Suggestion For ECOG 0-1 Clinical trial First line gemcitabine and paclitaxel NAB Second line FOLFOX or FOLFIRI 3 rd line (after FOLFOX) irinotecan BUT no data and likely very low RR For ECOG 2+ First line gemcitabine Second line capecitabine
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Reference No: Author(s) 12/05/16. Approval date: committee. June Operational Date: Review:
 12/05/16. Approval date: committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015
 What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
Pancreatic Ca Update
 Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Dr Roopinder Gillmore July 2017
 Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Pancreatic Cancer: Medical Therapeutic Approaches
 Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Disclosures
 Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD
 Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
Pancreatic Cancer Where are we?
 Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
Pancreatic Ductal Adenocarcinoma. Razvan Popescu Tumor Center Aarau Switzerland
 Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Adjuvant Treatment of Pancreatic Cancer in 2009: Where Are We? Highlights from the 45 th ASCO Annual Meeting. Orlando, FL, USA. May 29 - June 2, 2009
 HIGHLIGHT ARTICLE - Slide Show Adjuvant Treatment of Pancreatic Cancer in 2009: Where Are We? Highlights from the 45 th ASCO Annual Meeting. Orlando, FL, USA. May 29 - June 2, 2009 Muhammad Wasif Saif
HIGHLIGHT ARTICLE - Slide Show Adjuvant Treatment of Pancreatic Cancer in 2009: Where Are We? Highlights from the 45 th ASCO Annual Meeting. Orlando, FL, USA. May 29 - June 2, 2009 Muhammad Wasif Saif
ASCO Poster Review PANCREATIC CANCER
 ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
Pancreatic Cancer. Maribel Tirado Gomez, MD Hematology and Medical Oncology
 Pancreatic Cancer Maribel Tirado Gomez, MD Hematology and Medical Oncology Disclosures I have no actual or potential financial or commercial conflict of interest in relation to this presentation. Consulting
Pancreatic Cancer Maribel Tirado Gomez, MD Hematology and Medical Oncology Disclosures I have no actual or potential financial or commercial conflict of interest in relation to this presentation. Consulting
Tough to treat tumors in elderly. how far can we go? Jean-Luc Raoul Institut Paoli-Calmettes Marseille France
 Tough to treat tumors in elderly Pancreatic cancer: how far can we go? Jean-Luc Raoul Institut Paoli-Calmettes Marseille France Top 5 causes of cancer death / age Cancer Statistics in the USA 2008, CA
Tough to treat tumors in elderly Pancreatic cancer: how far can we go? Jean-Luc Raoul Institut Paoli-Calmettes Marseille France Top 5 causes of cancer death / age Cancer Statistics in the USA 2008, CA
Pancreas Cancer Update Systemic Treatments
 Pancreas Cancer Update Systemic Treatments Carlos R Becerra. Baylor University Medical Center Stage Distribution for Pancreas Cancer in the US (24-21) 1 9 8 7 Axis Title 6 5 4 53 3 28 2 1 9 11 Localized
Pancreas Cancer Update Systemic Treatments Carlos R Becerra. Baylor University Medical Center Stage Distribution for Pancreas Cancer in the US (24-21) 1 9 8 7 Axis Title 6 5 4 53 3 28 2 1 9 11 Localized
Cáncer de Páncreas: Optimización del tratamiento sistémico
 Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Cáncer de Páncreas: Optimización del tratamiento sistémico Alfredo Carrato Hospital Universitario Ramón y Cajal, Madrid 16 de Mayo de 2015 Pancreatic cancer screening There is a latency period of about
Pancreatic cancer from the past to the future
 Pancreatic cancer from the past to the future Darren Sigal, MD Scripps Clinic Pancreas and Bile Duct Cancer Group Division of Hematology/Oncology Scripps Clinic Pancreas and Bile Duct Cancer Group 1 Objectives
Pancreatic cancer from the past to the future Darren Sigal, MD Scripps Clinic Pancreas and Bile Duct Cancer Group Division of Hematology/Oncology Scripps Clinic Pancreas and Bile Duct Cancer Group 1 Objectives
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel
 Tunnel") Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
LA CHEMIOTERAPIA DI I LINEA
 DECIDERE LA CHEMIOTERAPIA ADIUVANTE E DELLA MALATTIA METASTATICA LA CHEMIOTERAPIA DI I LINEA Michele Reni Department of Medical Oncology IRCCS Ospedale San Raffaele Milan, Italy 1930 1940 1950 1960 1970
DECIDERE LA CHEMIOTERAPIA ADIUVANTE E DELLA MALATTIA METASTATICA LA CHEMIOTERAPIA DI I LINEA Michele Reni Department of Medical Oncology IRCCS Ospedale San Raffaele Milan, Italy 1930 1940 1950 1960 1970
Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid
 Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid Pancreatic Cancer Pancreatic Cancer Pancreatic Cancer Entity Resectable Borderline Resectable Locally advanced
Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid Pancreatic Cancer Pancreatic Cancer Pancreatic Cancer Entity Resectable Borderline Resectable Locally advanced
Systemic Cytotoxic Therapy in advanced HCC
 Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
State of the Art Management of Pancreatic Cancer. Laleh Melstrom, MD, MS, FACS
 State of the Art Management of Pancreatic Cancer Laleh Melstrom, MD, MS, FACS Nothing to disclose DISCLOSURE Pancreas Cancer Demographics/Risk Factors/Presentation Epidemiology 1 : 8 th most common malignancy
State of the Art Management of Pancreatic Cancer Laleh Melstrom, MD, MS, FACS Nothing to disclose DISCLOSURE Pancreas Cancer Demographics/Risk Factors/Presentation Epidemiology 1 : 8 th most common malignancy
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Concept to Practice: New Advances in the Treatment of GI Cancers
 Concept to Practice: New Advances in the Treatment of GI Cancers 2016 Community Oncology Alliance Conference Orlando, FL Thomas George, MD, FACP Director, GI Oncology Program Director, Experimental Therapeutics
Concept to Practice: New Advances in the Treatment of GI Cancers 2016 Community Oncology Alliance Conference Orlando, FL Thomas George, MD, FACP Director, GI Oncology Program Director, Experimental Therapeutics
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Reference No: Author(s) Approval date: 12/05/16. Committee. June Operational Date: Review:
 Approval date: 12/05/16. Committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Biliary Tract Cancer (BTC) Dr Colin Purcell, Consultant Medical Oncologist on behalf of the GI Oncologists Group, Cancer
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
SBRT in Pancreas Cancer Role of The Radiosurgery Society
 SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Pancreatic Cancer - Resected
 Pancreatic Cancer - Resected GI Practice Guideline Dr. Michael Sanatani, MD. FRCPC Dr. Francisco Perera, MD, FRCPC Dr. Brian Dingle, MD, FRCPC Approval Date: October 4, 2007 This guideline is a statement
Pancreatic Cancer - Resected GI Practice Guideline Dr. Michael Sanatani, MD. FRCPC Dr. Francisco Perera, MD, FRCPC Dr. Brian Dingle, MD, FRCPC Approval Date: October 4, 2007 This guideline is a statement
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
ARROCase: Borderline Resectable Pancreatic Cancer
 ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Pancreatic Ductal Adenocarcinoma. Razvan Popescu Tumor Center Aarau Switzerland
 Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Teaching aims Discuss role of palliative care in PDAC Metastatic or locally advanced irresectable disease First line Therapies
Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Teaching aims Discuss role of palliative care in PDAC Metastatic or locally advanced irresectable disease First line Therapies
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Upper Gastrointestinal. Friday, March 2, :00 p.m. 2:45 p.m.
 Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Perioperative versus adjuvant management of gastric cancer, update 2013
 Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
Pancreas SBRT. Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis
 Pancreas SBRT Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis December 19, 2018 Clinical Presentation 48 year old woman initially
Pancreas SBRT Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis December 19, 2018 Clinical Presentation 48 year old woman initially
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Update on Pancreatic Cancer
 Update on Pancreatic Cancer Farshid Dayyani, MD, PhD Associate Clinical Professor, Department of Medicine, UC Irvine School of Medicine February 2 nd, 2018 Overview Current Systemic Treatments Adjuvant
Update on Pancreatic Cancer Farshid Dayyani, MD, PhD Associate Clinical Professor, Department of Medicine, UC Irvine School of Medicine February 2 nd, 2018 Overview Current Systemic Treatments Adjuvant
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Pancreatic Cancer in adults:
 National Institute for Health and Care Excellence Version 1.0 Pancreatic Cancer in adults: diagnosis and management Appendix K 31 July 2017 Draft for Consultation Developed by the National Guideline Alliance,
National Institute for Health and Care Excellence Version 1.0 Pancreatic Cancer in adults: diagnosis and management Appendix K 31 July 2017 Draft for Consultation Developed by the National Guideline Alliance,
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER
 CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
Evidence-Based adjuvant treatment of resectable pancreatic adenocarcinoma. Adina Croitoru Fundeni Clinical Institute
 Evidence-Based adjuvant treatment of resectable pancreatic adenocarcinoma Adina Croitoru Fundeni Clinical Institute 1. Introduction 2. Borderline resectable-neoadjuvant CHT-RT 3. Adjuvant CHT 4. Adjuvant
Evidence-Based adjuvant treatment of resectable pancreatic adenocarcinoma Adina Croitoru Fundeni Clinical Institute 1. Introduction 2. Borderline resectable-neoadjuvant CHT-RT 3. Adjuvant CHT 4. Adjuvant
The Role of Radiation Therapy in Upper Gastrointestinal Cancers
 The Role of Radiation Therapy in Upper Gastrointestinal Cancers David H. Ilson, MD, PhD David H. Ilson, MD, PhD, is an attending physician at the Memorial Sloan Kettering Cancer Center and a professor
The Role of Radiation Therapy in Upper Gastrointestinal Cancers David H. Ilson, MD, PhD David H. Ilson, MD, PhD, is an attending physician at the Memorial Sloan Kettering Cancer Center and a professor
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m B a y e r
 EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
Is the Neo-adjuvant Approach Better than Adjuvant Approach? Comparative Levels of Evidence: Randomized Trials
 Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
L oncologo Alberto Zaniboni
 COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
GASTROINTESTINAL MALIGNANCIES
 Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
Outline GASTROINTESTINAL MALIGNANCIES Bassel F. El-Rayes Winship Cancer Institute Emory University Colorectal Cancer Pancreas Cancer Gastric Cancer Hepatobiliary Cancer Anal Cancer Introduction Epidemiology
ESMO 13th World Congress on Gastrointestinal Cancer
 ESMO 13th World Congress on Gastrointestinal Cancer 22-25 June, 2011 Barcelona, Spain INTRODUCTION The ESMO World Congress on Gastrointestinal Cancer took place in Barcelona from the 22nd until the 25th
ESMO 13th World Congress on Gastrointestinal Cancer 22-25 June, 2011 Barcelona, Spain INTRODUCTION The ESMO World Congress on Gastrointestinal Cancer took place in Barcelona from the 22nd until the 25th
Future Perspectives in mpca. Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France
 Future Perspectives in mpca Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France Number of Novel Therapies and Targets in Pancreatic Cancer Are Expanding Garrido-Laguna I, et al. Nat Rev Clin Oncol.
Future Perspectives in mpca Michel Ducreux, MD, PhD Gustave Roussy Villejuif, France Number of Novel Therapies and Targets in Pancreatic Cancer Are Expanding Garrido-Laguna I, et al. Nat Rev Clin Oncol.
Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma
 Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
Original Article Phase II trial of capecitabine plus nab-paclitaxel in patients with metastatic pancreatic adenocarcinoma Werner Scheithauer 1, Gabriela Kornek 1, Gerald Prager 1, Nadja Stranzl 1, Friedrich
HPB Clinical Guidelines for Pancreatic and Periampullary Cancer, Colorectal Liver Metastases and Primary Liver Cancers 2016 (Lancs & South Cumbria)
") HPB Clinical Guidelines for Pancreatic and Periampullary Cancer, Colorectal Liver Metastases and Primary Liver Cancers 2016 (Lancs & South Cumbria) 1 Pancreatic and Periampullary Cancer (ELHT Ver 5 2016)
HPB Clinical Guidelines for Pancreatic and Periampullary Cancer, Colorectal Liver Metastases and Primary Liver Cancers 2016 (Lancs & South Cumbria) 1 Pancreatic and Periampullary Cancer (ELHT Ver 5 2016)
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for