TB, or NOT TB? A Tough Question in Kids!
|
|
|
- Dale Robbins
- 5 years ago
- Views:
Transcription

1 TB, or NOT TB? A Tough Question in Kids! Brian Lee, MD Pediatric Tuberculosis Program Division of Infectious Diseases Ken Martin, MD Division of Radiology
2 Overview Illustrate the range of clinical scenarios that present to pediatric ID/TB specialists Highlight clinical and radiographic features that are unique to pediatric TB Highlight common mistakes in the reading of pediatric radiographs Exchange ideas about approaches to management
3 Children are not little adults Children Primary Any lobe Rare Common Paucity Low Low Disease Type Location Cavitation Adenopathy Symptoms AFB Load Contagion Adults/Teens Reactivation Apical Common Rare Consistent High High
4 Diagnosis of Active TB in Children is Tough Clinical & radiographic findings are often nonspecific (due to immune response rather than AFB load) so can overlap with other diagnoses Low yield on AFB smears and cultures so microbiologic confirmation is not the norm (negative AFB smears and cultures NEVER rule out active tuberculosis) Diagnosis often based on epidemiologic risk and ruling out other causes
5 2-year old boy Arrived from Guatemala 3 months ago and was referred to TB clinic because of positive PPD (10 mm) and CXR showing right hilar adenopathy No significant past medical history Family denies any TB contact Symptom review: negative Physical exam: normal
6
7 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain gastric aspirates and start multidrug TB therapy D. Another approach?
8
9 What would you do? A. Treat patient for LTBI B. Obtain IGRA and base LTBI treatment decision on this result
10 Pearls To evaluate for TB disease in children, CXR should include both frontal and lateral views (lateral view helps with evaluation of the hilum) Expiratory films can give the appearance of adenopathy around the hilum or infiltrate in the parenchyma (in some cases, repeating CXR with better inspiration can be helpful)
11 5-year old boy Arrived from Yemen over a year ago and referred to TB clinic because of positive PPD (17 mm) and CXR showing right hilar adenopathy Patient and family (parents, 2 sisters) all PPD negative 1 year ago (3 month old brother not yet tested) Family denies any TB contact Symptom review: cough and rhinorrhea for 1-2 months Physical exam: normal
12
13 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain gastric aspirates and start multidrug TB therapy D. Another approach?
14 Evaluation of Household Members 3- and 7-year old sisters: PPD positive (conversion) Parents and 3-month old brother: PPD negative

15
16
17 What would you do? Gastric aspirates were obtained, and RIPE therapy was initiated No source case was identified and AFB cultures of gastric aspirates all negative after 8 weeks A. Stop treatment for active TB B. Change to INH/RIF and complete 4 more months of treatment for active TB C. Continue RIPE therapy for 4 more months
18 Pearls Negative AFB smears and cultures never rule out active TB In general, if there is enough concern to initiate treatment for active TB in a child, the full treatment course should be completed, unless an alternative diagnosis is identified Because of the paucibacillary nature of pediatric TB, many experts are comfortable with INH/RIF for the continuation phase of treatment in the setting of culture-negative disease
19 2-week old boy Admitted to the hospital because of right upper lobe consolidation noted on CXR (obtained because pediatrician noted right clavicular fracture in clinic) Born in US to Hmong family PPD negative Family denies any TB contact Symptom review: negative Physical exam: normal
20
21 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain gastric aspirates and start multidrug TB therapy D. Another approach?

22
23 Pearls In children, thymus often mistaken as a pathologic process Thymus has variable appearance in both size and shape Normally prominent in newborn Increases in size during the first few months of life Less prominent between 5-10 year of age
24 8-month old boy Admitted to hospital with cough, diffuse wheezing, and increased work of breathing no improvement with albuterol and corticosteroids History of reactive airway disease and multiple clinic/ed visits over past 2 months for asthma, bronchiolitis, and/or pneumonia Born in US but mother and multiple family members from Cambodia Family denies any TB contact but aunt on treatment for LTBI PPD positive (15 mm)
25

26
27 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain gastric aspirates and start multidrug TB therapy D. Another approach?
28 Evaluation of Household Members Mother: CXR with right lung infiltrates and pleural effusion Father: PPD positive (20 mm), CXR normal 2-year old brother: PPD positive (10 mm), CXR right hilar adenopathy 5-year old brother: PPD positive (12 mm), CXR normal



29
30 Pearl: Pediatric TB = Sentinel Event Active TB (and recent TB test conversion) in a young child represents recent infection and therefore active transmission in the community (usually due to a contagious adult)
31 Pearl: Pediatric TB Infection = High Risk of Active TB Healthy adults: 5-10% (over a lifetime) Children: age-related risk (over 24 months) Age Pulmonary CNS/Miliary <1 year 30-40% 10-20% 1-2 years 10% 2-5% 2-5 years 5% 0.5% 5-10 years 2% <0.5% >10 years 10-20% <0.5% Marais BJ et al. Int J Tuberc Lung Dis 2004; 8: Powell DA, Hunt WG. Advances in Pediatrics 2006;53:
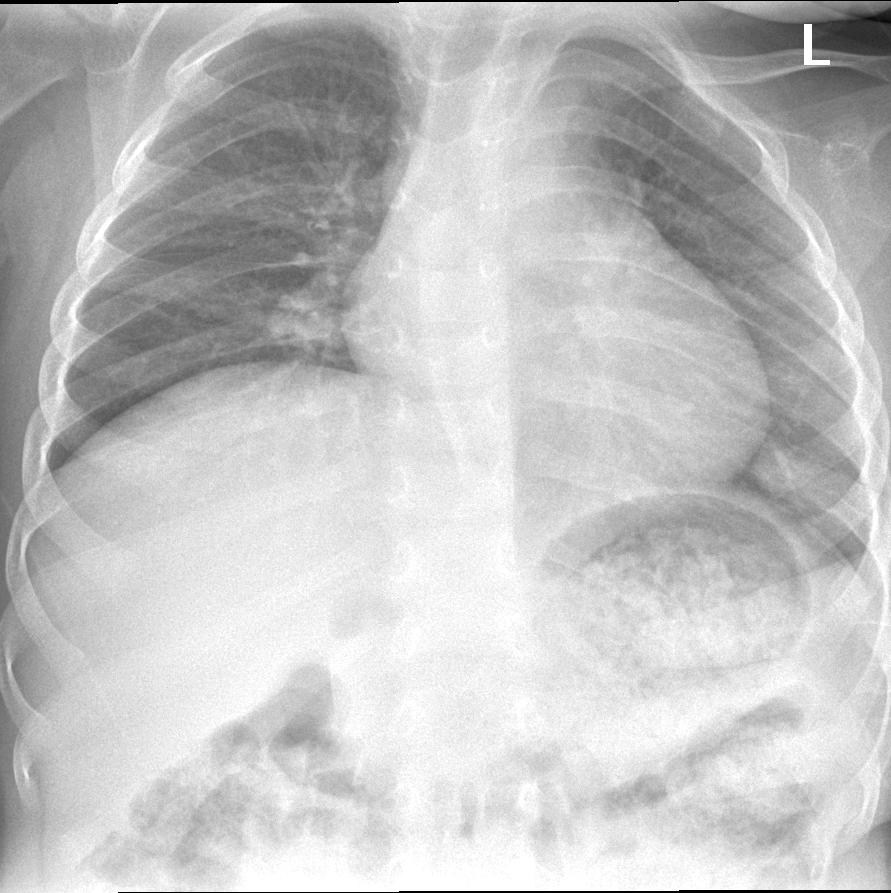
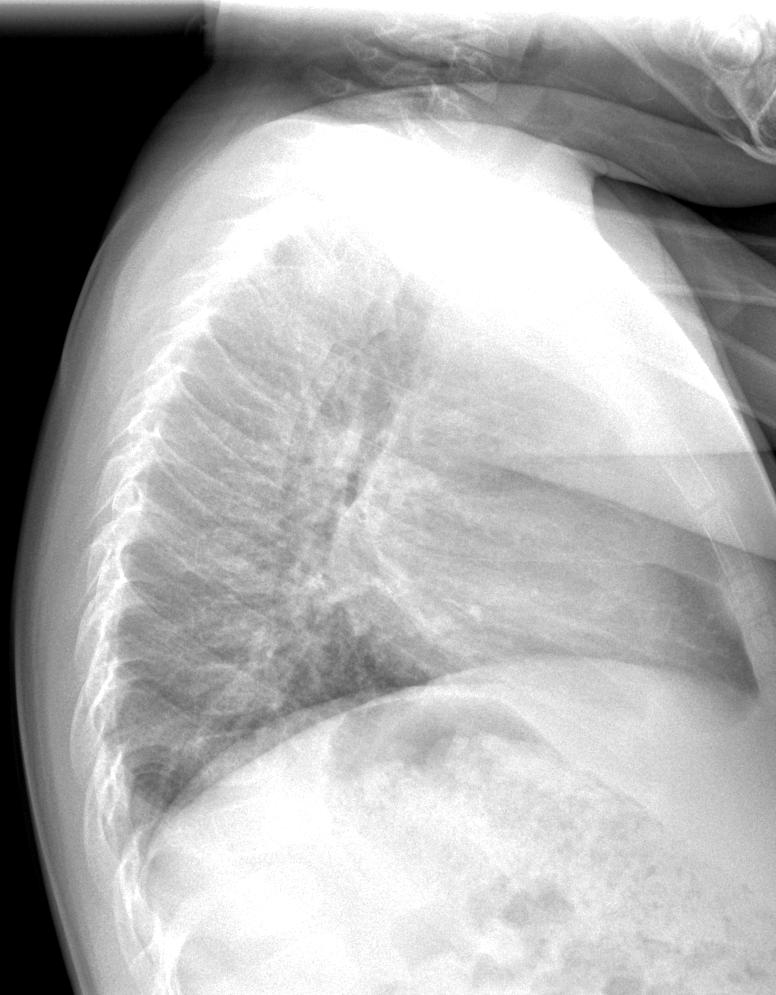
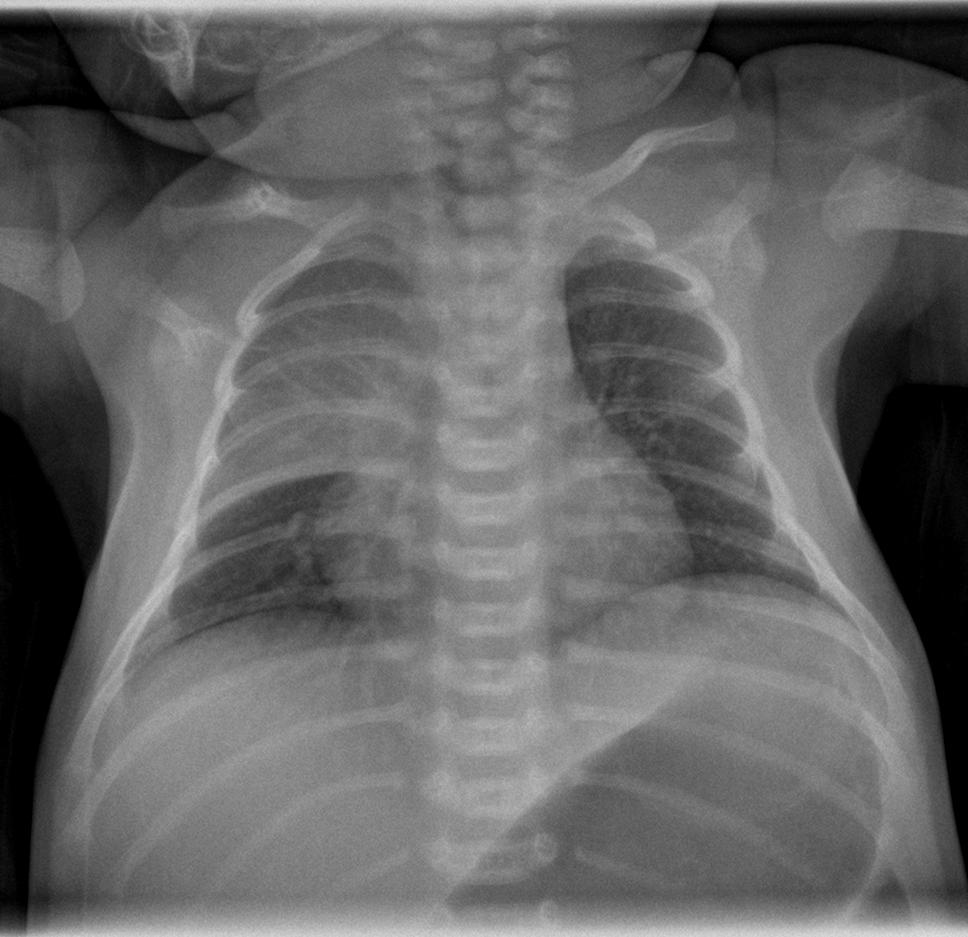
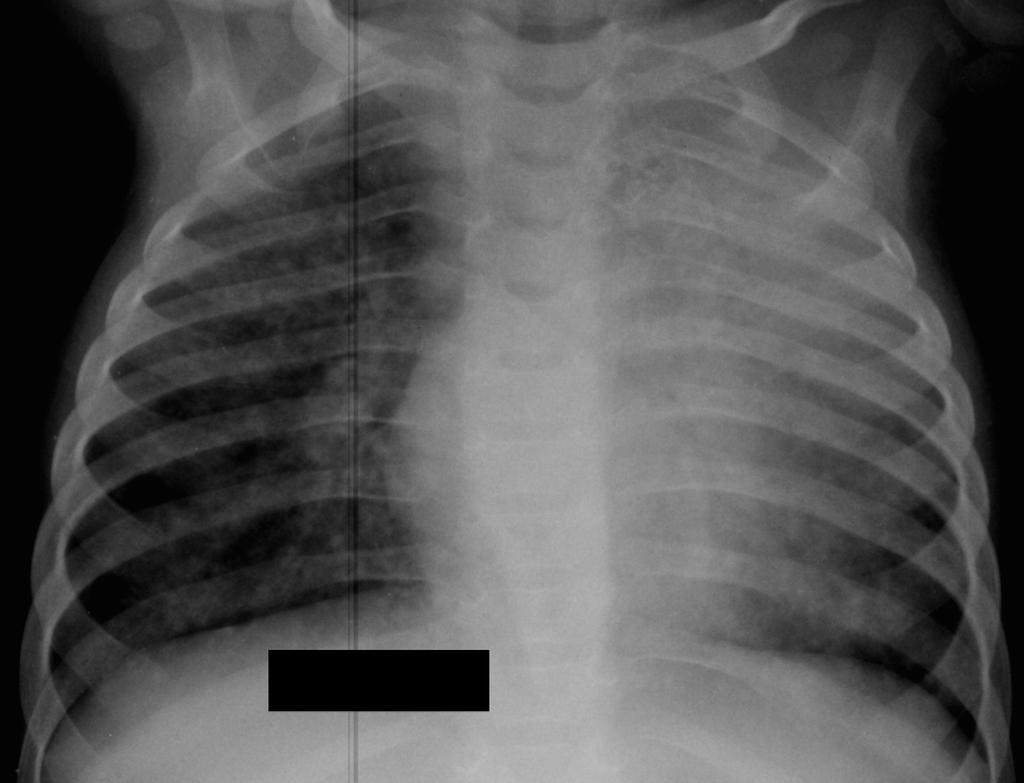
32 10-month old girl Referred to TB clinic because of exposure to the same family in the previous case (who was culture positive for pan-susceptible TB) No significant past medical history Symptom review: cough and fevers for 3-4 days Physical exam: normal PPD positive (12 mm)
")
33 Initial CXR (PA)

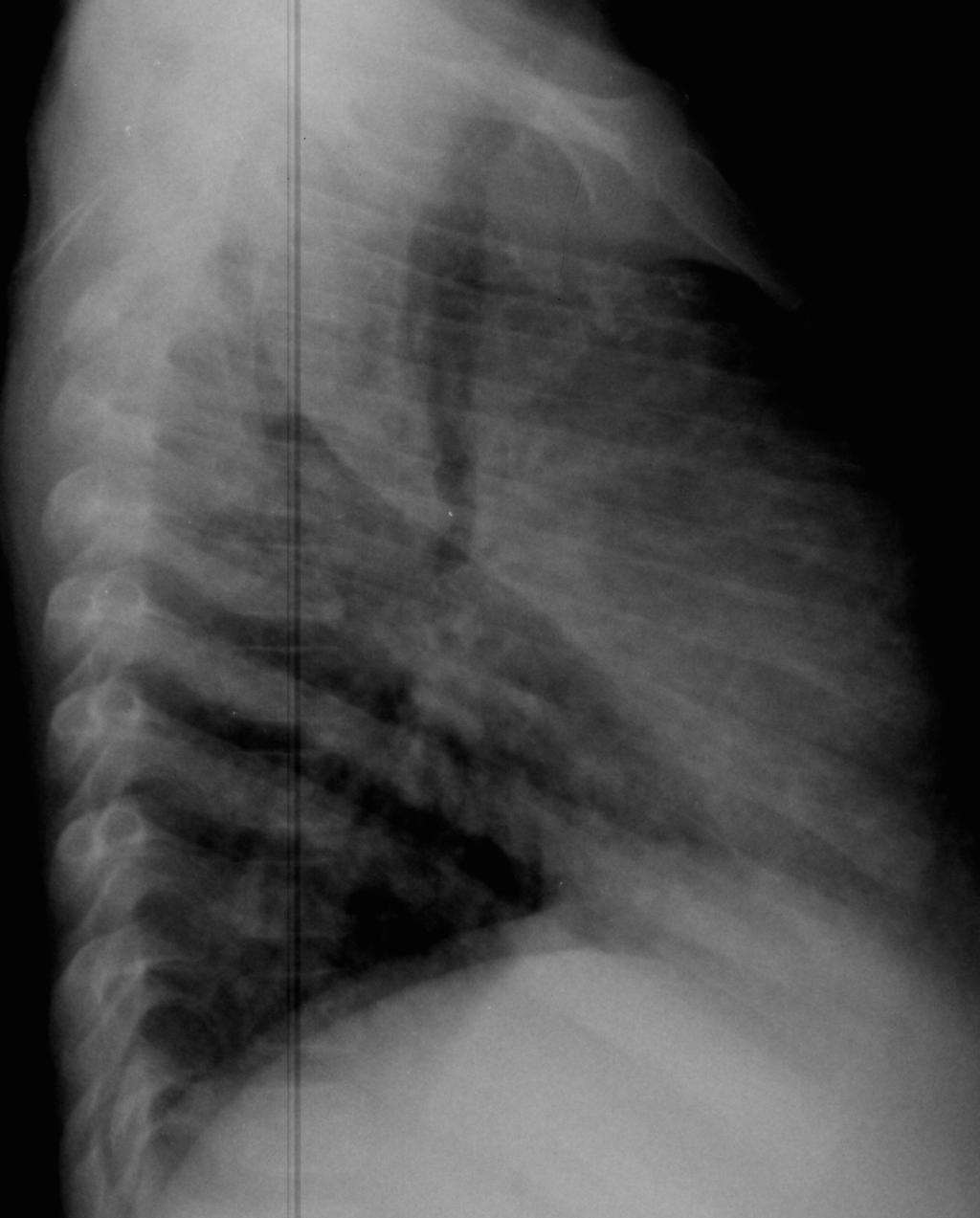
34 Initial CXR (Lateral)
35 What would you do? A. Obtain gastric aspirates and start multidrug TB therapy B. Forego gastric aspirates and start multidrug TB therapy C. Another approach?

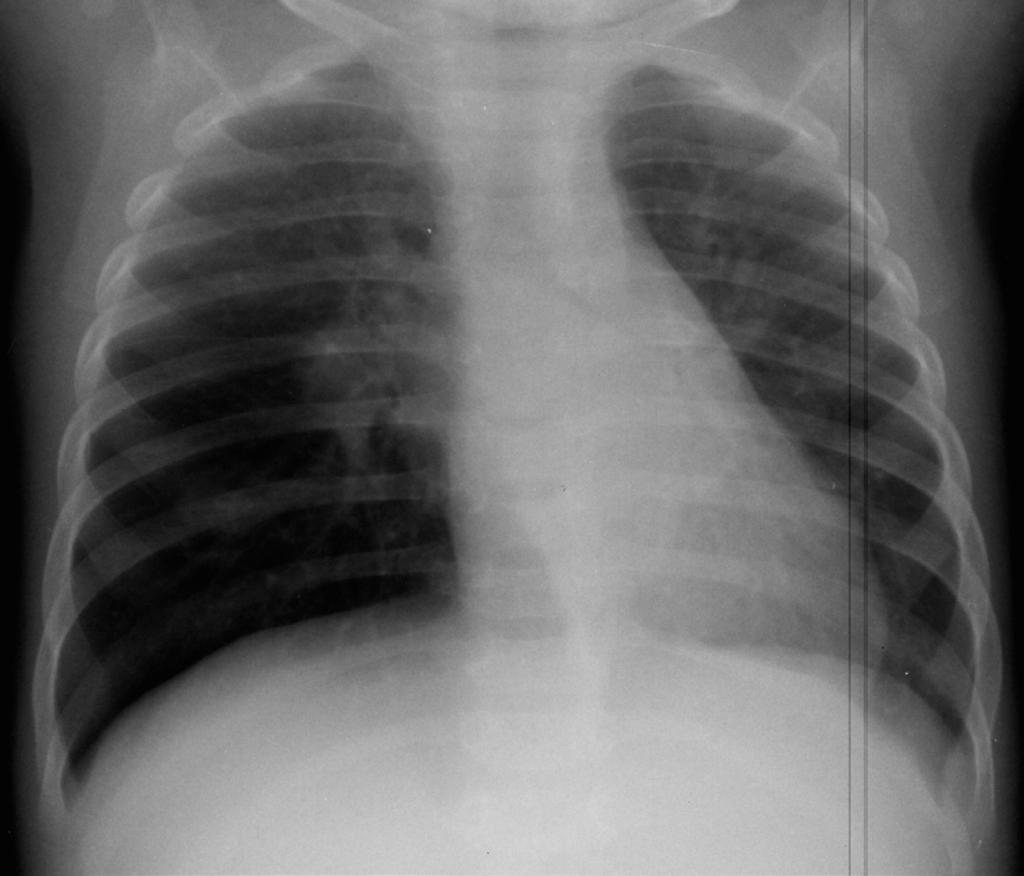
36 2 months into 3-drug therapy
37 What would you do? A. Continue current 3-drug TB therapy B. Change to 4-drug TB therapy C. Obtain gastric aspirates and add 2 new TB drugs D. Another approach?

38 1-week after prednisolone
39 Pearls Hilar adenopathy can manifest in multiple ways, including airway compression and ball-valve obstruction Worsening adenopathy (paradoxical reaction) after start of TB therapy is not uncommon and does not necessarily indicate treatment failure or drug resistance Rarely, corticosteroid therapy may be indicated in TB, such as for airway compression/obstruction
40 11-year old girl Referred to TB clinic because of positive PPD (19 mm) and abnormal CXR Born and raised in Japan until age 7 (h/o BCG), though parents originally from Sweden Past medical history: pectus excavatum Family denies any TB contact Review of symptoms: negative Physical exam: normal except pectus excavatum
41
42 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain induced sputum samples and start multidrug TB therapy D. Another approach?
43 Evaluation of Household Members Parents: PPD negative 10-year old brother: PPD positive in past (h/o BCG), CXR normal


44

45
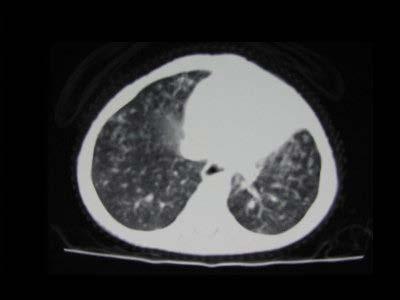
46 Pearls Chest wall deformities can cause increased density on CXR that can be mistaken for parenchymal disease CT scan can at times provide additional information when CXR findings are equivocal, but risks/benefits must be weighed
47 16-year old male Referred to TB clinic with 1 week of fevers and productive cough, h/o positive PPD, and CXR showing right lung disease Born in China and arrived in US 4 years ago Past medical history: PPD positive with normal CXR 1 year ago, but completed <1 month of INH Family denies any TB contact Symptom review: night sweats Physical exam: crackles over right lung
48
49 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain induced sputum samples and start multidrug TB therapy D. Another approach?
50 Additional information Evaluation of household members: Parents: h/o positive PPDs, CXRs normal 9-year old sister: PPD negative Induced sputum samples: all AFB smear negative and TB PCR negative
51 What would you do? A. Treat for community-acquired pneumonia B. Start multidrug TB therapy C. Obtain IGRA and based decision on this result D. Another approach?
52 Pearls When symptoms are acute, trial of treatment for community-acquired pneumonia is reasonable as long as: Initial sputum studies do show evidence of tuberculosis Reliable follow up assured BUT avoid using fluoroquinolone Normalization of CXR without TB therapy provides good evidence against active TB
53 16-year old male Referred to TB clinic due to productive cough over 3 weeks (despite course of azithromycin and amoxicillin), positive PPD, and CXR with RML/RLL infiltrates Born in China and arrived in US 2 years ago Past medical history: unremarkable Family denies any TB contact Review of systems: fever, cough, fatigue Physical exam: rales at right lung base
54
55 What would you do? A. Test household members for TB and then decide what to do based on these results B. Obtain IGRA on patient and then decide what to do based on this result C. Obtain induced sputum samples and start multidrug TB therapy D. Another approach?
56 Additional Information Evaluation of household members Father: PPD positive (15 mm), normal CXR Mother: PPD positive (10 mm), normal CXR Sputum samples AFB smear 2+ positive, TB PCR positive


57
58 Pearls When symptoms are more chronic and has not responded to treatment for common entities, TB must be considered higher on the differential diagnosis Teenagers, like adults with TB, are more likely than young children to have higher AFB load and contagion so early testing of sputum samples can be helpful
59 15-month old girl Admitted with cough and respiratory distress, marked weight loss, diffuse adenopathy, and hepatosplenomegaly Born in the US, no foreign travel Past medical history: bullous pemphigoid requiring chronic prednisone and mycophenalate therapy Family denies any TB contact PPD negative (0 mm)
60
61

62
63 What would you do? A. Obtain gastric aspirates B. Perform bronchoscopy C. Perform lymph node biopsy D. Perform urine studies E. Perform lumbar puncture F. All of the above
64 Results BAL fluid: AFB stain positive Lymph node pathology: caseating granulomas CSF: normal AFB cultures from gastric aspirates, BAL, lymph node, and urine all positive for M. tuberculosis
65 What later emerged Prior to her birth: Father diagnosed/treated for active pulmonary TB Contact investigation identified LTBI in mother and 3 siblings, all of whom completed INH 3 months after birth: Adult cousin diagnosed with active pulmonary TB Contact investigation never identified baby as a contact Prior to immunosuppression for skin condition, patient was never screened/tested for TB
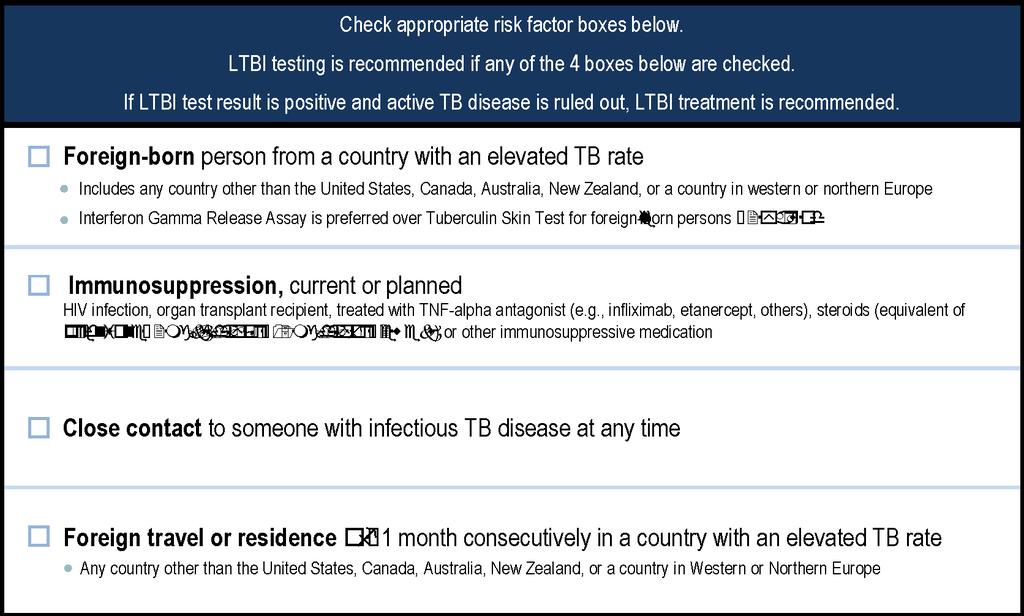
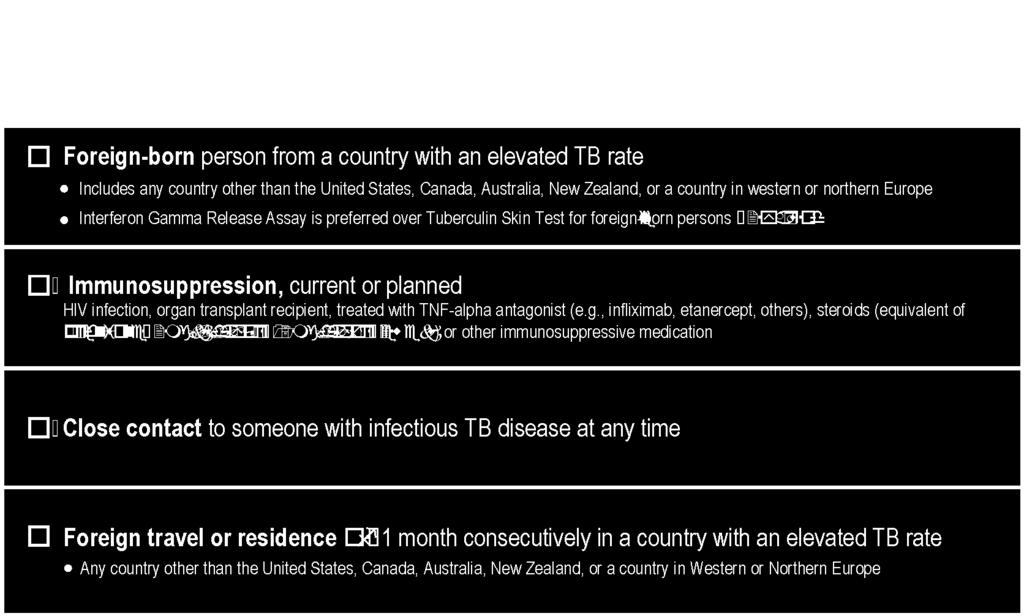
66 California Pediatric TB Risk Assessment
67 Pearls Families not always forthcoming with regards to TB history/exposure Risk assessment must include current/planned immunosuppression, which was not emphasized in prior TB risk assessments
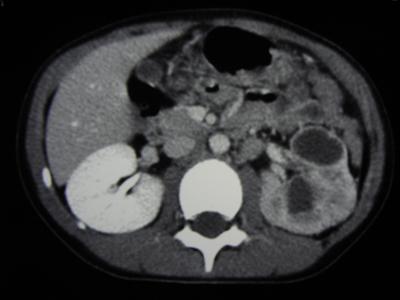
68 7-year old girl Referred to nephrology clinic because of several months of urinary discomfort and urinalysis showed Protein 100, WBC>2250, and RBC 360 with negative urine culture Born in US; family originally from China Past medical history: h/o positive PPD Review of systems: unremarkable except for urinary complaints Physical exam: normal CXR and renal imaging obtained

69

70
71 Additional information obtained after referral to ID/TB clinic History of exposure to uncle with active TB several years ago Patient had positive PPD at that time but never completed INH Urine AFB cultures obtained and positive for pansusceptible TB

72 After 9-months of TB therapy
73 What would you do? A. Stop TB treatment B. Continue 2-drug TB therapy C. Add 2 new drugs to TB therapy D. Recommend resection of nonfunctional kidney
74 After 16 months of TB therapy kidney was resected Upper pole kidney: 3+ AFB, TB PCR negative Lower pole kidney: AFB negative, TB PCR positive Ureter: 2+ AFB, TB PCR positive ALL AFB cultures negative Molecular beacon testing: no INH/rifampin resistance mutations detected What would you do?
75 Pearls I hope you can tell me some for this case
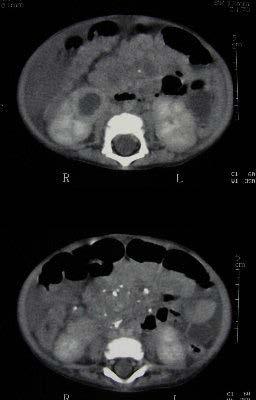
76 10-year old girl Admitted with fevers and severe abdominal pain and emesis Born in Philippines but arrived in US 3 years ago Past medical history: negative Review of systems: negative other than above Physical exam: acute abdomen Taken to OR due to concern for ruptured appendix

77
78 Hospital Course OR findings Cloudy peritoneal fluid Gross pus draining from mesenteric lymph nodes Periappendiceal inflammation Pathologic findings Necrotizing granulomatous inflammation AFB stain positive Additional testing PPD negative (0 mm) CXR normal
79 Evaluation of Household Members Mother: PPD negative Brother: PPD positive (15 mm), CXR normal
80 Pearls TB can mimic almost any disease Extrapulmonary involvement is not uncommon among children with active TB Extrapulmonary 22% Both 7% Pulmonary 71% Any extrapulmonary involvement* (totaling 29.5%) Extrapulmonary site (%) Lymphatic (18.8) Meningeal (3.6) Miliary (1.3) Bone & Joint (1.5) Other (4.3)
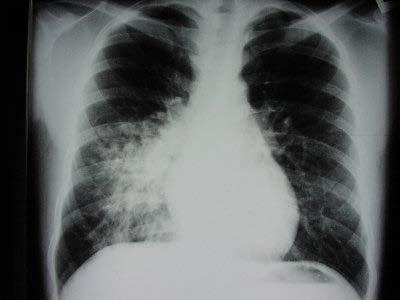
81 Cavitary Lung Cases Case 1: 14-year old female with cough and fevers for 1 month despite course of azithromycin. Patient born in US and no foreign travel but met missionaries from Uruguay. PPD negative. Case 2: 16-year old male with fever, cough, and weight loss over 10 days. Born in US and no foreign travel but parents both from Liberia. PPD negative. Case 3: 17-year old female with fever, chest pain, and cough for 2-3 weeks despite course of azithromycin. Born in Ethiopia and arrived in US 3 months ago. PPD negative.


82 Case 1: 14-year old female



83 Case 2: 16-year old male


84 Case 3: 17-year old female
85 Who has TB? A. Case 1 B. Case 2 C. Case 3 D. Case 1 & 2 E. Case 2 & 3 F. Case 1 & 3 G. All of the above
86 Epidemiologic Risk? Case 1: Lives in Tuolumne, CA. Both parents PPD negative years ago, contact with visitors from Uruguay Case 2: Lives in Antioch, CA. Parents from Liberia. Father (medical transport) PPD negative. Mother (LVN) PPD positive but CXR normal. Case 3: Lives in San Leandro, CA. Born in Ethiopia. Parents and 2 siblings TB cleared for immigration 3 months prior.
87 Alternative Causes? Case 1: Induced sputums with negative AFB smears. Fevers and cough improved on IV Unasyn and then PO Augmentin. CXR normal 2 weeks later. Case 2: Induced sputums with negative AFB smears. Coccidioidomycosis suspected. Fever and cough improved with fluconazole. Case 3: Symptoms not improving on ceftriaxone/clindamycin. Induced sputums with positive AFB smears and positive TB PCR.
88 Pearls Early testing of sputum samples for AFB and TB PCR can be helpful in older children with adult-type disease When negative, there should be careful consideration of other causes of cavitary disease
89 Summary Abnormal radiographs should be reviewed carefully, ideally with a pediatric radiologist Consider what else could be causing CXR finding (overlying clothing/jewelry, nipple, poor inspiration, thymus, etc.) Consider repeat CXR (sometimes with additional views) In some cases, consider CT scan to provide better definition of the abnormality Consider treatment of common infections first (as long as no evidence of contagion risk) Use TB infection/disease around child as surrogate for risk this may require active investigation
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Pediatric TB Radiology: It s Not Black and White Part 2
 Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Experiencing technical difficulties? Please call Adobe Connect for technical assistance at 1-800-422-3623 Pediatric TB Radiology: It s Not Black and White Part 2 June 18, 2018 A National Webinar June 18,
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
3/25/2012. numerous micro-organismsorganisms
 Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Congenital & Neonatal TB A Case of Tuberculosis Congenital or Acquired? Felicia Dworkin, MD NYC DOHMH Bureau TB Control World TB Day March 23, 2012 Congenital TB: acquired by the fetus during pregnancy
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Theresa Barton, MD
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Pediatric TB Theresa Barton, MD December 9, 2009 Pediatric Tuberculosis Tess Barton, MD Assistant Professor of Pediatrics UT Southwestern
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Diagnosis of tuberculosis in children H Simon Schaaf
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB in Children. The diagnostic challenge. Ralph Diedericks Red Cross Hospital
 TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
TB in Children The diagnostic challenge Ralph Diedericks Red Cross Hospital TB in children Brief epidemiology Clinical issues in primary TB Cases Rates of TB infection 2005 TST survey reported a TB prevalence
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
TB in Foreign Born and High Risk Populations
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 TB in Foreign Born and High Risk Populations John J. Nava, M.D. December 9, 2009 Tuberculosis in High Risk Populations and the Foreign Born
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis in Children Kim Connelly Smith, MD, MPH October 16, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Pediatric Drug-Resistant TB in China
 Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
Pediatric Drug-Resistant TB in China Shuihua Lu,Tao Li Shanghai Public Health Clinical Center Jan.18,2013 A MDR-TB CASE A four and a half years old boy, spent 4 yeas of his life in hospital. His childhood
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS
 MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
MANAGEMENT OF TUBERCULOSIS IN NEONATES AND YOUNG INFANTS A Bekker FIDSSA Conference, 2017 OUTLINE Case Perinatal TB Approach to the TB-exposed newborn MOM AND BABY S Born by NVD at peripheral hospital
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Pediatric TB Basics and Evaluation and Management of Exposed Neonates
 Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Pediatric TB Basics and Evaluation and Management of Exposed Neonates Ann M. Loeffler, MD Randall Children s Hospital, Portland OR & Curry International TB Center, Oakland CA September, 2017 No Disclosures
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015
 Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
Treatment of TB Infection Lisa Y. Armitige, MD, PhD April 7, 2015 Tuberculosis Infection Diagnosis and Treatment April 7, 2015 El Paso, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has
PEDIATRIC TUBERCULOSIS. Objectives. Children are not just small adults. Pediatric Tuberculosis 1
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
PEDIATRIC TUBERCULOSIS
 PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
PEDIATRIC TUBERCULOSIS Ann M. Loeffler, M.D. Faculty Consultant Curry International Tuberculosis Center Objectives At the end of this session, participants will be able to describe: how pediatric patients
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Disclosures. Current Issues and Controversies in Child and Adolescent Tuberculosis 02/24/2016. NSTC 2016 Annual Meeting
 Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
Current Issues and Controversies in Child and Adolescent Tuberculosis Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [With great thanks to Andrea Cruz, M.D.] Disclosures Dr.
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Contact Investigation and Prevention in the USA
 Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Contact Investigation and Prevention in the USA George D. McSherry, MD Division of Infectious Disease Penn State Children s Hospital Pediatric Section TB Center of Excellence Rutgers Global Tuberculosis
Enlarging TB Lymph Node Improving or Deteriorating? History. History. Physical examination. Distribution of lymph nodes
 Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
Enlarging TB Lymph Node Improving or Deteriorating? Dr. Lilian Lee Dr. Hamilton Hui Department of Paediatrics & Adolescent Medicine United Christian Hospital 30 August 2006 Enlarging TB lymph node - Improving
TB Intensive San Antonio, Texas
 TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
TB Intensive San Antonio, Texas August 2-5, 2011 Pediatric TB Jeffrey Starke, MD August 5, 2011 Jeffrey Starke, MD has the following disclosures to make: Is on a data safety monitoring board for Hoffman
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal
 Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Latent Tuberculosis Infection Reporting Instructions for Civil Surgeons Using CalREDIE Provider Portal Civil surgeons are required to report tuberculosis (TB) screening outcomes that result in latent TB
Summary Statistics of Reported and Verified Cases of Tuberculosis in San Joaquin County in 2012, (N=44) County Rate = 6.3 Cases per 100,000 Population
 County Rate = 6.3 Cases per 100,000 Population") I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES Male 29 65.9% Female 15 34.1% AGE GROUP NUMBER OF CASES PERCENT OF CASES 04 3 6.8% 514 2 4.5% 1524 3 6.8% 2544 6 13.6% 4564 15 34.1% 65+
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES Male 29 65.9% Female 15 34.1% AGE GROUP NUMBER OF CASES PERCENT OF CASES 04 3 6.8% 514 2 4.5% 1524 3 6.8% 2544 6 13.6% 4564 15 34.1% 65+
Contact Investigation
 Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Tuberculosis Ann Raftery, RN, PHN, MSc GHS Learning Objectives Upon completion of this session, participants will be able to: Describe the criteria used and method for determining the infectious period
Pulmonary TB aspects
 Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
Pulmonary TB aspects Nodule & infiltrate Cavern Pneumonia Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Nodules and infiltrates
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Pediatric Tuberculosis
 Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
Pediatric Tuberculosis Kim Connelly Smith, MD, MPH April 7, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Kim Connelly Smith, MD, MPH has the following disclosures to
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Algorithmic Approaches to Child TB Management in Resource-limited Settings
 Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Algorithmic Approaches to Child TB Management in Resource-limited Settings Steve Graham Centre for International Child Health University of Melbourne Department of Paediatrics Royal Children s Hospital
Case Study: TB-HIV co-infection
 Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
Case Study: TB-HIV co-infection Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County With guest appearance by Julie Tans-Kersten, MS, BSMT (ASCP) Director, WI TB Program 33
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
Management of Pediatric Tuberculosis in New Jersey
 Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
Management of Pediatric Tuberculosis in New Jersey Helen Aguila, MD NJMS Global TB Institute December 15, 2011 This presentation is in part adapted from Pediatric Tuberculosis by Ann Loeffler, MD : Francis
The Public Health Impact of TB in the Correctional System. Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer
 The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
The Public Health Impact of TB in the Correctional System Sarah Bur, RN, MPH Federal Bureau of Prisons Infection Prevention and Control Officer The Public Health Impact of TB in the Correctional System
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TB Intensive San Antonio, Texas December 1-3, 2010 TB Case Presentations Doug Hornick, MD; Iowa U Medical School December 1, 2010 Pulmonary Fascinomas with a Tuberculous Attitude Douglas B. Hornick, MD
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Case presentation. Dr REESAUL R
 Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Case presentation Dr REESAUL R Mr S. 25 years old Case 1 Ref on 06/ April /2006 to Chest Clinic from a private GP of Port Louis for : Cough + haemoptysis and dyspnoea Case 1(6/April/2006) Mr S Single 25
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Tuberculosis in the Traveler
 Tuberculosis in the Traveler Waterloo-Wellington Cardiovascular Respiratory Conference April 27 th, 2016 The Beat on Breathing Watch, Treat or Admit? disclosures No Potential for conflict of interest Staffed
Tuberculosis in the Traveler Waterloo-Wellington Cardiovascular Respiratory Conference April 27 th, 2016 The Beat on Breathing Watch, Treat or Admit? disclosures No Potential for conflict of interest Staffed
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Case Study: TB-HIV co-infection
 Case Study: TB-HIV co-infection Sarah Dietz, BSW Linkage to Care Specialist AIDS Resource Center of Wisconsin Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County The speakers
Case Study: TB-HIV co-infection Sarah Dietz, BSW Linkage to Care Specialist AIDS Resource Center of Wisconsin Julia Greenleaf, RN, MPH Public Health Nurse Public Health Madison & Dane County The speakers
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
BGS Spring Conference 2015
 TB in the elderly Dr Anna Rich Respiratory Consultant, Nottingham University Hospitals Outline Why relevant? Elderly vs young adults Diagnosis Treatment Side effects TB in the 21 st century Stats 2013;
TB in the elderly Dr Anna Rich Respiratory Consultant, Nottingham University Hospitals Outline Why relevant? Elderly vs young adults Diagnosis Treatment Side effects TB in the 21 st century Stats 2013;
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!