Follow up The way ahead. John Griffith
|
|
|
- Ethan Booker
- 5 years ago
- Views:
Transcription



1 Follow up The way ahead John Griffith
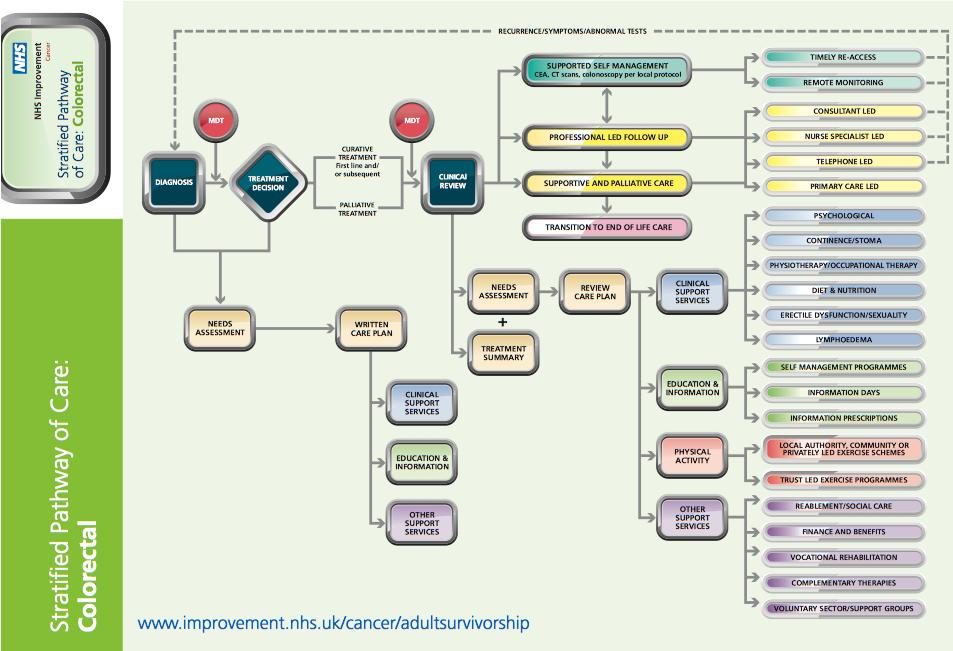
2 Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring Care coordination with open access

")
3 One Size Fits All established follow-up No metastases picked up by the 5 year CT in 79 patients The one year colonoscopy detected 1 cancer (ba enema pre-op) 13 patients with polyps 8 known incomplete or not removed pre-op 5 new (one adenoma)


4 CRC Recurrence Retrospective study Included colorectal cancer AND surgical resection Excluded those who had de-functioning stomas only Period between Ensures a full 5 year follow-up cycle completed 1000 Case-notes 600 Bradford (60%) 250 Calderdale and Huddersfield (25%) 150 York (15%) Data collected: Patient Demographic Tumour Features Recurred? If so, where, when and how was it detected?

 6.61 Rectum (Mid 6-12cm) 11.")
5 Final Analysis: 1001 Cases 877 adenocarcinomas undergoing curative resection Location 71.0% Colon 29.0% Rectum Dukes Stage Dukes A = 15.6% Dukes B = 45.1% Dukes C = 39.0% Dukes C1 = 34.9% Dukes C 2 = 4.1% Location % Caecum/Right/Ascending Hepatic flexure 2.39 Transverse/Splenic flexure 6.73 Left/Descending 4.33 Sigmoid/RSJ Rectum (High >12cm) 6.61 Rectum (Mid 6-12cm) Rectum (Low <6cm) Anal 0.23
6 Mortality and Recurrences Mortality 40.9% Mortality Rate Cancer Related Deaths (51.3%) Recurrence Rate 232 recurrences (26.5%) No significant difference between centres Recurrence YES Recurrence NO Total Cases % age Recurrence Bradford C&H York Total



7 Recurrence Location Most common site of recurrence is multiple followed closely by: Liver Anastamosis/Pelvis Lung Location of Recurrences Bones Brain Lymph node Other Lung Anastomosis/Pelvis Liver Multiple

 Significantly greater likelihood of recurring in")

8 Location of Recurrence: Colon vs. Rectal Primary %'age Rectum %'age Colon Colonic primary - Isolated liver metastasis (28.9%) Significantly greater likelihood of recurring in liver p-value = 0.09 Rectal primary - Isolated lung metastasis (30.0%) Significantly greater likelihood of recurring in lung p-value =

9 Recurrence Mode of Detection Mode of Detection vs. Location of Recurrence CEA Endoscopy CT USS Other Eg. MRI/PET CT Isolated Anastomosis/Pelvis Recurrences: Endoscopy detected 37.4% CT detected 46.5% Isolated Liver Recurrences: CT detected: 69.4%

10 Management of Recurrence 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Lung Anastomosis/Pelvis Liver Multiple Proceed to Intervention 82.93% 81.40% 71.18% 50.82% Proceed to Resection 53.66% 44.18% 47.46% 9.84%

: 49.")




11 Impact of Resected Recurrence Of those who had their recurrence resected (n=81): 49.3% Completed 5 year follow-up 2.5% Died of non-cancer related causes eg. MI However, 46.9% had a cancer related death Count Percentage Not died during follow-up % Death not cancer related % Cancer related death % Unknown Cause %
 Dukes Stage of Primary No recurrence Recurrence Recurrence Rate (%) A 129 8 5.84 B 309 87 21.97 C1 195 111 36.")
12 Tumour Features if Recurred Dukes Stage Significant difference in recurrence rate depending on Dukes Stage (p<0.001) Dukes Stage of Primary No recurrence Recurrence Recurrence Rate (%) A B C C D
 EMVI Present 139 111 44.")


13 EMVI Status EMVI Status of Primary No recurrence Recurrence Recurrence Rate (%) EMVI Present No EMVI Significantly increased risk of recurrence if EMVI from primary: P-value = <0.001 Location of recurrence if EMVI present: EMVI & Recurrence Percentage (%) Liver Anastomosis/Pelvis Lung Multiple Lymph Node/Other


14 CRM Status Increased risk of recurrence if primary was CRM positive (p<0.001) 51.4% CRM positive vs. 25.3% not CRM positive Location of recurrence if CRM positive: Anastamosis/Pelvis recurrences most likely p = 0.04 CRM Positive & Recurrence % Liver Anastomosis/Pelvis Lung Multiple Lymph Node/Other
15 Survival Curve vs. Dukes Stage Kaplan-Meier survival estimates, by dukes analysis time dukes = A dukes = C1 dukes = D dukes = B dukes = C2
16 Time to Recurrence Time to Recurrence (Days) Percentage of Total Recurrences (%) Cumulative Total of Recurrences (%) (1 year) (2 years) (3 years) (4 years) (5 years) Greater than 5 years By 3 years, we have 84.5% of our recurrences.

17 Time to Recurrences vs. Primary Tumour Site Smoothed hazard estimates, by primary_tumour_site analysis time primary_tumour_site = Caecum/Rightprimary_tumour_site = Hepatic flexure to Left primary_tumour_site = Sigmoid primary_tumour_site = Rectum
18 Building Our Model of Recurrence Level of Significance p = Age 0.69 Primary Tumour Site Rectum = Hepatic Flex to Desc = Sigmoid = Duke s Stage <0.001 Grade * EMVI <0.001 CRM <0.001 Mucinous ** Sex 0.67 Ethnicity NS * When controlled for Duke s Stage ** When controlled for Duke s Stage, EMVI and CRM



19 The next steps Risk stratified follow up Remote follow up Survivorship programmes Late effects of treatment Life with recurrence
20 Success!
21 Where can we deliver this? Increasing number of survivors Increasing number of new referrals Reduction in staff Primary care budgets! NHS Improvement Remote monitoring tool
22 Criteria for CRC risk stratification Disease Treatment or effects of treatment Individual Supported Self Management pathway (green) Dukes A, B, C T1-3 N0-2 Curative intent After closure of temporary stoma After completion of adjuvant therapy Good understanding of care pathway Good general fitness Willingness to self manage Clinically Supervised Pathway (amber) Unstable CEA T4 Trial Patients N1N2 Palliative Intent Post op bowel or urological dysfunction Temporary stoma in place Poor symptom control High anxiety scores (>5 on DT score) Poor compliance Social isolation Significant comorbidity Complex Care pathway (red) Dukes D M1 Liver metastases High score EMVI patients Post hepatic surgery Severe side effects of treatment On active treatment Multiagency support FOR TESTING January to December 2011(V.3 revised December 2011)
23
24 % patients stratified to each pathway % Salford NBT Guys Red complex pathway Amber shared pathway Green Self Management Pathway Red Amber Green Number % Number % Number % Salford Bristol Guys
25 No:patients Time since treatment combined data Combined - Time since end of treatment months 6months 12 months 18 months 2 years 3 years 4 years 5 years Of these 45 (20%) suitable at 12 months or before Question: Where does it leave the 18 month suggested time point before risk stratification occurs
26 Annual Saving Estimates (based on data submitted by sites) Bristol Guys Salford Average slots/month Projected slots saved /annum Projected savings*/ annum ,092 37,440 62,400 87,360 *Outpatients slots calculated at 80 per appointment Estimated savings across all three sites in year 1 = 187K NB longer term savings will be less as backlog is cleared
27 Outcome measures Laparoscopic surgery CRM involvement? Personalised care pathways Survivorship events PROMS data Survival!
28
29
30
31
32




33 Suvivorship and Education Programmes Symptoms Benefits and finance Group care and well being Dietetics Exercise (local councils) Follow-up regime
34 What are the late effects? Low anterior resection syndrome Sexual dysfunction Urinary symptoms Chemotherapy toxicity

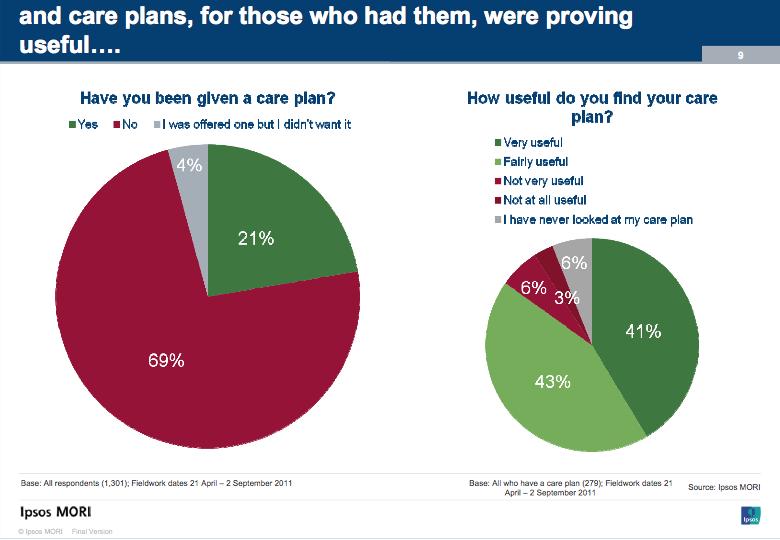
35 Main findings from Ipsos Mori baseline survey Information deficit about providing information on symptoms & signs of recurrence. 45% did not feel they had enough. 45% of patients with ED since treatment continue to have problems. 53% noticed a change of interest in sex and 35% say they have not had any advice relating to this 20% currently have a care plan
36 Questions we must answer What is the unmet need of our patients? What services do we need to provide for them and when? What is life like living with recurrence: duration, treatment, side effects, visits.
37 Low risk Medium risk Risk stratification Tumour Dukes A & B (-ve EMV & CRM) Dukes B (Either +ve EMV OR +ve CRM) Dukes C1 (-ve EMV & CRM) High risk Dukes B (+ve EMV & + ve CRM) Dukes C1 (Either +ve EMV OR +ve CRM) Dukes C2 Patients receiving neoadjuvant treatments
38 Diagnosis CT, MRI, Colonoscopy Low risk 6 weeks post op CEA 4 months CEA, Colonoscopy (if not performed preop) 8 months CEA Low risk time of recurrence patients (cumulative) 12 months CEA 16 months CEA number of patients Op Chemo/Radio Palliative 18 months CT months CEA 5 24 months CEA 30 months CEA, CT years 36 months CEA, Colonoscopy Follow-up to 5 years 6 monthly CEA
39 Diagnosis CT, MRI, Colonoscopy Medium risk 6 weeks post op CEA 4 months CEA, Colonoscopy (if not performed preop) 8 months CEA 12 months CEA Medium risk time of recurrence (cumulative) 16 months CEA 18 months CT 20 months CEA 15 number of patients 10 5 OP Chemo/Radi o 24 months CEA 30 months CEA, CT years 36 months CEA, Colonoscopy Follow-up to 5 years 6 monthly CEA
40 Diagnosis CT, MRI, Colonoscopy High risk 6 weeks post-op CEA 4 months CEA, Colonoscopy (if not performed preop) 8 months CEA High risk time of recurrence (cumulative) 12 months CEA, CT, Flexible sigmoidoscopy months CEA 20 months CEA number of patients OP Chemo/Radio Palliative 24 months CEA, CT months CEA 36 months CEA, CT & Colonoscopy years Follow-up to 5 years 6 monthly CEA, 5 year CT


41 What follow-up & When? Low and medium risk: Regular CEA, CT at 18 & 36 months, Colon 3yrs High risk: Regular CEA, CT 12, 24 & 36 months, Colon 3yrs

42 Conclusion There is currently a lot of interest in the overall package of the care our patients receive. Many of the indices which care will be assessed by are currently not being measured, and we probably have no idea as to the services we need for many of the problems. Follow up regimes should be patient specific.
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Bowel Cancer in England and Wales A summary report about the management and outcomes of people with bowel cancer
 Bowel Cancer in England and Wales A summary report about the management and outcomes of people with bowel cancer Based on findings from the National Bowel Cancer Audit Background How are patients diagnosed?
Bowel Cancer in England and Wales A summary report about the management and outcomes of people with bowel cancer Based on findings from the National Bowel Cancer Audit Background How are patients diagnosed?
Northern Ireland Cancer Network (NICaN) Colorectal Cancer follow-up Workshop Report. 18 th October 2013 Antrim Enterprise Agency
 Colorectal Cancer follow-up Workshop Report. 18 th October 2013 Antrim Enterprise Agency") Northern Ireland Cancer Network (NICaN) Colorectal Cancer follow-up Workshop Report 18 th October 2013 Antrim Enterprise Agency Report compiled November 2013 Contents 1. Summary of Key Messages... 2 2.
Northern Ireland Cancer Network (NICaN) Colorectal Cancer follow-up Workshop Report 18 th October 2013 Antrim Enterprise Agency Report compiled November 2013 Contents 1. Summary of Key Messages... 2 2.
Ghosts in the Machine: Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand
 Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131
 Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer
 Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Caring for a Patient with Colorectal Cancer. Objectives. Poll question. UNC Cancer Network Presented on 10/15/18. For Educational Use Only 1
 Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Colorectal Cancer Comparative Audit Report
 SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER
 CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER 1. a. If you are retired, or do not perform such surgery, please check the box at the right, answer questions
CURRENT PRACTICE OF FOLLOW-UP MANAGEMENT AFTER POTENTIALLY CURATIVE RESECTION OF RECTAL CANCER 1. a. If you are retired, or do not perform such surgery, please check the box at the right, answer questions
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2016 March Published: March 2018
 Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
The CREST Trial. Funded by Cancer Research UK and developed by the National Cancer Research Institute
 The CREST Trial A randomised phase III study of stenting as a bridge to surgery in obstructing colorectal cancer. Results of the UK ColoRectal Endoscopic Stenting Trial (CREST). Funded by Cancer Research
The CREST Trial A randomised phase III study of stenting as a bridge to surgery in obstructing colorectal cancer. Results of the UK ColoRectal Endoscopic Stenting Trial (CREST). Funded by Cancer Research
Northern Ireland Bowel Cancer Screening Programme. Pathways. Version 4 1 st October 2013
 Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
ANNUAL REPORT. Figure 2 displays the distribution of the number of these diagnoses in 2013 by age (along the X axis) and by gender.
 and by gender.") One ANNUAL REPORT Colorectal Cancer Colorectal cancer affects 14, Americans annually, making it the fourth most frequently diagnosed cancer in the US. It is also the second leading cause of cancer death
One ANNUAL REPORT Colorectal Cancer Colorectal cancer affects 14, Americans annually, making it the fourth most frequently diagnosed cancer in the US. It is also the second leading cause of cancer death
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Bowel Cancer Information Leaflet THE DIGESTIVE SYSTEM
 THE DIGESTIVE SYSTEM This factsheet is about bowel cancer Throughout our lives, the lining of the bowel constantly renews itself. This lining contains many millions of tiny cells, which grow, serve their
THE DIGESTIVE SYSTEM This factsheet is about bowel cancer Throughout our lives, the lining of the bowel constantly renews itself. This lining contains many millions of tiny cells, which grow, serve their
COLORECTAL CANCER Quality Performance Indicators (QPI) Comparative Report
 Comparative Report") SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2016 2017 Quality Performance Indicators (QPI) Comparative Report Mr S Yalamarthi, NHS Fife, Lead Colorectal Cancer Clinician,
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2016 2017 Quality Performance Indicators (QPI) Comparative Report Mr S Yalamarthi, NHS Fife, Lead Colorectal Cancer Clinician,
COLORECTAL CANCER COMPARATIVE AUDIT REPORT SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT. Mr B.J. Mander SCAN Group Chair
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Colorectal Cancer Quality Performance Indicators
 Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
On-going and planned colorectal cancer clinical outcome analyses
 On-going and planned colorectal cancer clinical outcome analyses Eva Morris Cancer Research UK Bobby Moore Career Development Fellow National Cancer Data Repository Numerous routine health data sources
On-going and planned colorectal cancer clinical outcome analyses Eva Morris Cancer Research UK Bobby Moore Career Development Fellow National Cancer Data Repository Numerous routine health data sources
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial
 Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial ANNUAL REPOR T (562) 933-0900 MemorialCare.org/TCI 2810 Long Beach Blvd. Long Beach, CA 90806 #3 Colorectal cancer is
Colorectal Cancer at the MemorialCare Todd Cancer Institute at Long Beach Memorial ANNUAL REPOR T (562) 933-0900 MemorialCare.org/TCI 2810 Long Beach Blvd. Long Beach, CA 90806 #3 Colorectal cancer is
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2014 March Published: July 2016
 NORTH OF SCOTLAND PLANNING GROUP Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2014 March 2015 Published: July 2016 Mr
NORTH OF SCOTLAND PLANNING GROUP Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2014 March 2015 Published: July 2016 Mr
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer
 Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
COLON CANCER FOLLOW UP GUIDELINES
 COLON CANCER FOLLOW UP GUIDELINES CAGPO Dr. Raziya Mia October 1, 2016 1 DISCLOSURES NONE 2 MITIGATING POTENTIAL BIAS Recommendations are consistent with published guidelines American Society of Clinical
COLON CANCER FOLLOW UP GUIDELINES CAGPO Dr. Raziya Mia October 1, 2016 1 DISCLOSURES NONE 2 MITIGATING POTENTIAL BIAS Recommendations are consistent with published guidelines American Society of Clinical
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
BOWEL CANCER. Cancer information.
 BOWEL CANCER Cancer information www.cancervic.org.au What is bowel cancer? Bowel cancer is the second most common cancer in both men and women in Australia1 and is more common in people over the age of
BOWEL CANCER Cancer information www.cancervic.org.au What is bowel cancer? Bowel cancer is the second most common cancer in both men and women in Australia1 and is more common in people over the age of
BOWEL CANCER. Causes of bowel cancer
 A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Shore Medical Center Site-Specific Study: Colorectal Cancer 2013
 Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
NHS Wirral Clinical Commissioning Group Old Market House Hamilton Street Birkenhead Wirral CH41 5AL Tel:
 Our Ref: ID 834 NHS Wirral Clinical Commissioning Group Old Market House Hamilton Street Birkenhead Wirral CH41 5AL Tel: 0151 541 5830 Re: Freedom of Information Request Thank you for your request for
Our Ref: ID 834 NHS Wirral Clinical Commissioning Group Old Market House Hamilton Street Birkenhead Wirral CH41 5AL Tel: 0151 541 5830 Re: Freedom of Information Request Thank you for your request for
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
Advances in Imaging Technology In The Management of Colorectal Cancer
 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative
 Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
CARCINOMA DEL COLON-RETTO: COSA DICONO LE LINEE GUIDA. Dr.ssa Foltran Luisa Oncologia medica Pordenone
 CARCINOMA DEL COLON-RETTO: COSA DICONO LE LINEE GUIDA Dr.ssa Foltran Luisa Oncologia medica Pordenone Convegno Regionale AIOM FVG, Palmanova, 14 Maggio 2016 COLORECTAL CANCER FOLLOW-UP Objectives Intensive
CARCINOMA DEL COLON-RETTO: COSA DICONO LE LINEE GUIDA Dr.ssa Foltran Luisa Oncologia medica Pordenone Convegno Regionale AIOM FVG, Palmanova, 14 Maggio 2016 COLORECTAL CANCER FOLLOW-UP Objectives Intensive
UK Bowel Cancer screening Dr Voi Shim Wong BsC MD FRCP. Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals
 UK Bowel Cancer screening 2017 Dr Voi Shim Wong BsC MD FRCP Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals Bowel Cancer Contents UK Bowel Cancer Screening Programme
UK Bowel Cancer screening 2017 Dr Voi Shim Wong BsC MD FRCP Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals Bowel Cancer Contents UK Bowel Cancer Screening Programme
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Colorectal Cancer Dashboard
 Process Risk Assessment Presence or absence of cancer in first-degree blood relatives documented for patients with colorectal cancer Percent of patients with colorectal cancer for whom presence or absence
Process Risk Assessment Presence or absence of cancer in first-degree blood relatives documented for patients with colorectal cancer Percent of patients with colorectal cancer for whom presence or absence
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit
 NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit NBOCA: Feasibility Study Date of publication: Thursday 9 th August
NATIONAL BOWEL CANCER AUDIT The feasibility of reporting Patient Reported Outcome Measures as part of a national colorectal cancer audit NBOCA: Feasibility Study Date of publication: Thursday 9 th August
The Binational Colorectal Cancer Audit. A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017
 The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance
 Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana
 GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
NEWTON-WELLESLEY HOSPITAL. Standard 4.6: Assessment and Evaluation of Treatment Planning Rectal Cancer
 NEWTON-WELLESLEY HOSPITAL Standard 4.6: Assessment and Evaluation of Planning Rectal Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic evaluation and
NEWTON-WELLESLEY HOSPITAL Standard 4.6: Assessment and Evaluation of Planning Rectal Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic evaluation and
GREATER MANCHESTER EXPERIENCE
 Greater Manchester Cancer Vanguard Innovation Remote Monitoring / Stratified Pathways GREATER MANCHESTER EXPERIENCE NADEEM AHMED - INFORMATICS ENTERPRISE ARCHITECT, DIGITAL PROJECTS @ The Christie Previously
Greater Manchester Cancer Vanguard Innovation Remote Monitoring / Stratified Pathways GREATER MANCHESTER EXPERIENCE NADEEM AHMED - INFORMATICS ENTERPRISE ARCHITECT, DIGITAL PROJECTS @ The Christie Previously
Stage III Colon Cancer Susquehanna Cancer Center Warren L Robinson, MD, FACP May 9, 2007
 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Warren L Robinson, MD, FACP May 9, 27 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Colorectal cancer is the third most common cancer
Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Warren L Robinson, MD, FACP May 9, 27 Stage III Colon Cancer Susquehanna Cancer Center 1997-21 Colorectal cancer is the third most common cancer
What you need to know about Radiation Therapy for Colorectal Cancer
 What you need to know about Radiation Therapy for Colorectal Cancer Questions and Answers CR Lund MSc MD FRCPC Radiation Oncologist Clinical Assistant Professor Overview I. Description of Radiation II.
What you need to know about Radiation Therapy for Colorectal Cancer Questions and Answers CR Lund MSc MD FRCPC Radiation Oncologist Clinical Assistant Professor Overview I. Description of Radiation II.
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE
 SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Transforming Cancer Services for London
 Programme Director Paul Roche Status Draft Owner Laura Boyd Version 0.4 Author Jennifer Layburn Date 15/05/13 Transforming Cancer Services for London Best Practice Commissioning Pathway for the early detection
Programme Director Paul Roche Status Draft Owner Laura Boyd Version 0.4 Author Jennifer Layburn Date 15/05/13 Transforming Cancer Services for London Best Practice Commissioning Pathway for the early detection
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital