Flow cytometry for MRD detec1on: Focus on AML. Sindhu Cherian University of Washington, Sea6le, WA, USA
|
|
|
- Trevor Wood
- 5 years ago
- Views:
Transcription
1 Flow cytometry for MRD detec1on: Focus on AML Sindhu Cherian University of Washington, Sea6le, WA, USA

2 Residual disease in hematopoie1c malignancy Residual disease has tradi:onal been defined by morphology in hematopoie:c neoplasms Minimal residual disease (MRD) is defined as disease present at a level below the sensi:vity of morphologic detec:on Performed using a method more sensi:ve and specific than morphology Flow cytometry Molecular methods

3 Focus of this talk will be on AML Tradi:onal criteria for response in AML were created in the mid 1950s and included Morphologic criteria blast <5% Clinical criteria count recovery, no evidence of extramedullary disease We have had the ability to detect MRD using different methods for >20 years Flow cytometry Molecular methods Increasing sensi1vity 10X flow Standard PCR 100X flow Next genera:on sequencing
4 Molecular methods: MRD in AML Molecular methods: PCR for reduc:on in over expressed genes (eg WT1) Sensi:vity ~0.01% Applicable in ~50% of AML Directed PCR for a muta:on or transloca:on Sensi:vity % Highest sensi*vi*es using next genera*on sequencing methods Current targets include Muta:ons: NPM1, MLL, CEBPa Transloca:ons such as t(8;21), inv(16), t(15;17) Currently applicable ~50-70% of cases Poten:al is unknown and growing as we detect new markers with next genera:on sequencing plaaorms The role of molecular diagnos:cs for MRD detec:on in AML is likely to grow in the future
5 Flow cytometry for MRD in AML Sensi:vity ~0.01% Reported to be informa:ve in ~85-95% of cases in most studies Several variables underlie the success of flow cytometry for MRD detec:on in AML Number of events collected 500,000 to 1,000,000 More events more sensi:ve Number of colors used More informa:ve if more colors are used in the same tube Ideally 6 Experience of operator Immunophenotype of blasts and difference from normal may impact ease of detec*on Familiarity with normal an:gen expression pa6erns is cri:cal
6 Comparison of flow and PCR for MRD Detec1on in AML Flow cytometry is currently more widely applicable Flow cytometry is applicable in 85-95% of cases when using at least 6 colors Molecular methods apply in 50-70% of cases Molecular methods, when applicable are more sensi:ve Molecular (PCR for transloca:on or gene muta:on) Sensi:vity ~0.001% Next genera:on sequencing methods even more sensi:ve Flow Sensi:vity 0.01%
7 Impact of MRD on survival in AML Regardless of method used to measure MRD, the impact of MRD post therapy is clear MRD holds up in mul:variable analysis as a predictor of survival and relapse in mul:ple studies Some (including Buccisano et al and Loken et al. 2012) suggest including AML MRD in designing risk adapted therapeu:c regimens It is clear that MRD will be an important part of monitoring in pa:ents with AML post therapy and that flow cytometry has an important role in establishing MRD
8 Clinical impact of MRD in AML Author Publica1on year Clinically significant 1me point: level of MRD with clinical significance San Miguel et al End I: 0.5% End Int: 0.2% Vendif et al End C: 0.035% Sievers et al End I: 0.5% Kern et al End C: LD Al-Mawali et al End I: 0.15% Rubnitz et al End I: 1% Bucciscano et al Post C: 0.035% Loken et al Post I: Any, similarly bad if >0%/<1% or 1% Walter et al. 2011, 2012 Any MRD at CR1 and CR2 pre transplant predicted increased overall mortality and likelihood of relapse Chen et al 2015 Any MRD, end induc:on I=induc:on, Int=intensifica:on, C=consolida:on, CR-complete remission
9 245 adults in CR post induc1on for AML Cumula1ve incidence of relapse Overall survival Chen et al. JCO 2015;33(11):
10 359 consecu1ve adults with AML who underwent myeloabla1ve allogeneic HCT: MRD pre transplant was associated with poorer outcomes Overall survival Cumula1ve incidence of relapse Araki et al. J Clin Oncol Feb 1; 34(4):
11 Open ques1ons regarding MRD detec1on by flow cytometry in AML What is the best :me point to assess for MRD Controversial as to whether post induc:on or post consolida:on in most informa:ve Kern et al pose a role for early blast clearance (Day 16) Pre and post transplant MRD seems informa:ve What is the most important threshold Range of 1% to any level of MRD (no lower threshold) Most groups use WBC as the denominator while occasional groups use mononuclear cells Kern et al recommend using degree of reduc:on in abnormal blasts (log difference) rather than a percentage
12 Strategies for flow cytometric iden1fica1on of MRD Difference from normal Iden:fying a leukemia associated phenotype Best strategies combine the two
13 Difference from normal In our laboratory we focus on the difference from normal approach to define MRD. 10 color flow cytometry >500,000 events collected for MRD analysis This relies on a thorough understanding of pa6erns of an:gen expression on normal blasts. In the next few slides we will review normal an:gen expression on blasts and discuss how an:gen expression can be altered in the face of a myeloid stem cell neoplasm (in this case AML)
 Allows assessment of 10 colors")
14 Panel used in our laboratory LSR II with 4 lasers (Becton Dickinson) Allows assessment of 10 colors
 Be aware: Some neoplas2c popula2ons may be overlooked if")

15 Iden1fying progenitors Progenitor iden:fica:on generally begins with the CD45 vs SSC defined blast gate (progenitors) can be posi:vely iden:fied using a progenitor marker (CD34 +/- CD117) Be aware: Some neoplas2c popula2ons may be overlooked if you use only this strategy AML with monocy2c differen2a2on, acute promyelocy2c leukemia Viable cells CD45 versus SSC defined blast gate Viable cells Blast gate "Blast gate" In most plots you see in this presenta:on, CD34+ blasts will be colored red



16 The CD45 vs SSC defined blast gate contains more than just progenitors When undertaking AML MRD tes:ng, it is important to recognize other cells that reside in the CD45 vs SSC defined blast gate so these are not confused for an abnormal blast popula:on Basophils, A panel for AML MRD detec:on would allow reliable differen:a:on of these popula:ons from normal progenitors and abnormal blasts Viable "Blast gate" "Blast gate" Viable cells Blast Blast gate Blast gate CD 123 PE

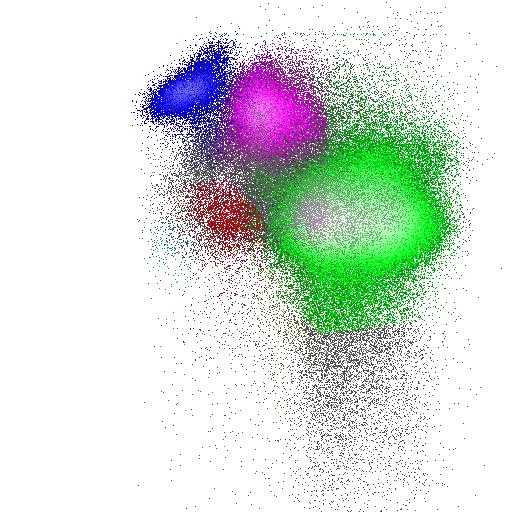
17 Normal progenitor development CD34 APC HLA-DR PB CD34 APC CD33 PE CD13 PE-Cy7

18
19 Progenitor abnormali1es Abnormali:es on myeloid progenitors (blasts) seen in myeloid stem cell neoplasms usually fall into one of 4 categories Abnormal intensity of an:gen expression (increased, decreased or absent). Asynchronous expression of an:gens associated with maturity with an:gens deno:ng immaturity Homogeneous expression of an an:gen usually expressed at varying levels with matura:on Expression of an:gens from other lineages. Recogni:on of such abnormali:es requires a thorough understanding of normal pa6erns of an:gen expression


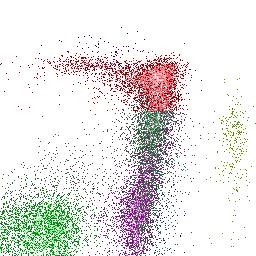
20 Abnormal intensity of an1gen expression Normal AML CD33 PE CD33 PE

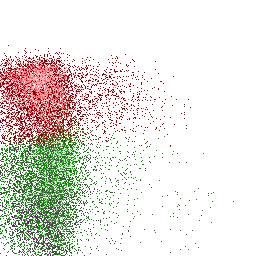
21 Asynchronous expression of an1gens associated with maturity and an1gens associated with immaturity Normal AML CD34+


22 Homogeneous expression of an an1gen usually expressed at varying levels through blast matura1on Normal AML CD34 APC




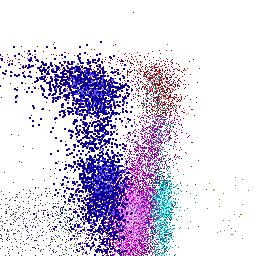
23 Expression of non-lineage an1gens Normal Blast gate AML CD5 PE-Cy5 CD7 PE Blast gate CD5 PE-Cy5 CD7 PE
24 Leukemia associated immunophenotype Using a different from normal strategy to iden:fy abnormal blast popula:ons in AML, leukemia associated immunophenotypes (LAIP) can be detected in most cases Most studies using 6 colors detect LAIP in 85-95% of AML For a sample list of specific LAIPS that have been described in AML in the literature see the following references Al-Mawali et al AJCP Olaru et al Cytometry Part B (Clinical Cytometry) In our laboratory (using 10 colors) we are able to define an abnormal immunophenotype in almost all cases of AML In the next few slides we will review some challenges in AML MRD detec:on by flow cytometry through a series of cases
25 Challenge 1: Blast phenotype in AML can be heterogeneous It has been long observed that abnormal blasts present in AML can have a very heterogeneous immunophenotype More than one LAIP may characterize a blast popula:on in AML At relapse or during/ater therapy, it is possible that the dominant clone will recede and that a minor clone will dominate Popula:on changes described in 31% of cases at relapse compared to diagnosis (Baer et al. 2001)




26 Example 1 Diagnosis WBCs Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 Normal WBCs Myeloblasts CD13 PE-Cy7 CD5 PE
27 Myeloid CD34+.tc s. re s. WBCs in The immunophenotype of the blasts is not homogeneous CD13 PE-Cy7 CD5 PE-Cy5 Myeloid CD34+ w w w WBCs CD13 PE-Cy7 CD5 PE-Cy5
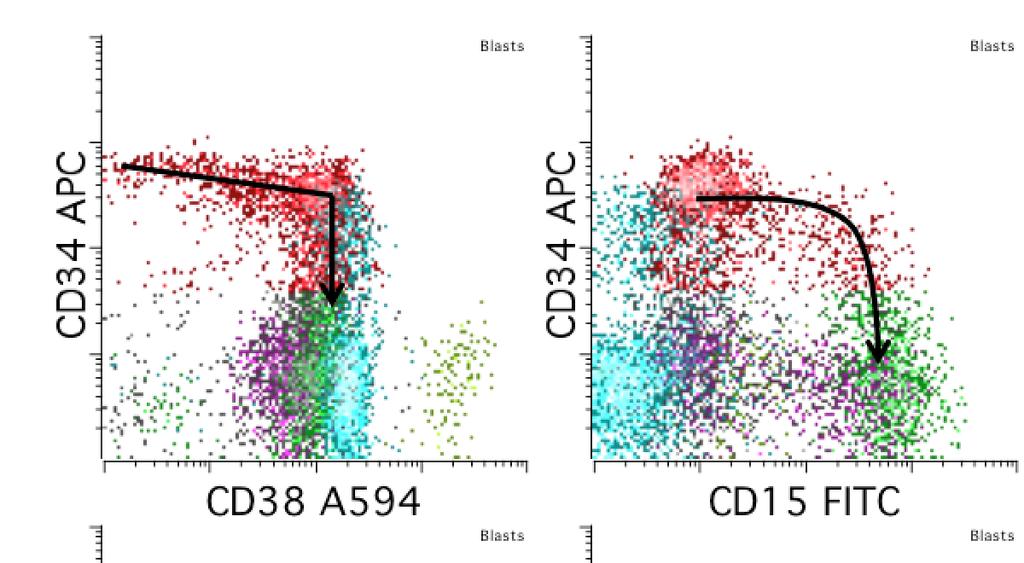
28 WBCs Abnormali1es in this case Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 Abnormal intensity of an1gen expression (increased, decreased or absent). Dominant red popula:on: Increased CD34, CD33, CD13 Variably decreased CD38 Minor orange popula:on Decreased CD38 Asynchronous expression of an1gens associated with maturity with an1gens deno1ng immaturity CD15 expression on a minor subset of CD34++ blasts Homogeneous expression of an an1gen usually expressed at varying levels with matura1on Uniform CD13, CD33, and CD34 Expression of an1gens from other lineages. Minor orange popula:on CD5 expression
29 Post transplant peripheral blood, day % circula:ng CD34+ blasts WBCs Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 Normal WBCs Myeloblasts CD13 PE-Cy7 CD5 PE The blasts in the peripheral blood are: A. Normal B. Abnormal
30 Post transplant peripheral blood, day 24 WBCs Myeloid CD34+ Diagnosis CD13 PE-Cy7 CD5 PE-Cy5 WBCs Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 The blasts in the peripheral blood resemble: A. The dominant popula:on seen at diagnosis (red) B. The minor popula:on seen at diagnosis (orange) C. A combina:on of the two

31 Post transplant peripheral blood, day 24 WBCs Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 Day 28 post transplant marrow 0.8% CD34+ blasts WBCs CD13 PE-Cy7 CD5 PE-Cy5 Normal for comparison WBCs Myeloblasts CD13 PE-Cy7 CD5 PE

32 Post transplant peripheral blood, day 24 WBCs Myeloid CD34+ CD13 PE-Cy7 CD5 PE-Cy5 Day 28 post transplant marrow 0.8% CD34+ blasts WBCs CD13 PE-Cy7 CD5 PE-Cy5 Day 28 post transplant sample with abnormal blasts highlighted in orange (0.2% of the WBC), normal background regenera:ng blasts present in red WBCs CD13 PE-Cy7 CD5 PE-Cy5




33 Myeloid CD34+ s. re s. WBCs in Diagnosis CD13 PE-Cy7 CD5 PE-Cy5.tc Relapse post transplant day 100 Myeloid CD34+ w w w WBCs CD13 PE-Cy7 CD5 PE-Cy5 The blast popula:on seen at recurrence has immunophenotypic features that overlap between the 2 dominant popula:ons present at diagnosis
34 Challenge 2: Prac1cal considera1ons How many events does it take to cons:tute and abnormal popula:on? What is the benefit of more colors?






35 Example 2 65 year old male with cytopenias Diagnos:c marrow for flow cytometry CD7 APC CD117 PE-Cy5 CD33 PE Normal for comparison CD7 APC CD117 PE-Cy5 CD33 PE
36 Abnormali1es in this case CD7 APC CD117 PE-Cy5 CD33 PE Abnormal intensity of an1gen expression (increased, decreased or absent). Decreased CD117 Increased CD34 Variably decreased CD38 Variably decreased HLA-DR Asynchronous expression of an1gens associated with maturity with an1gens deno1ng immaturity CD15 expression on CD34++ blasts Homogeneous expression of an an1gen usually expressed at varying levels with matura1on Bright homogeneous CD34 Homogeneous CD33 Expression of an1gens from other lineages. CD7 co-expression on a subset

37 Post-therapy, pre transplant specimen CD7 PE At first glance looks Normal for comparison ok but CD7 PE
 A small")



38 Although, most blasts look normal and regenera1ng (red) A small abnormal blast popula1on is highlighted in purple with similar features to that seen at diagnosis CD7 PE CD117 PE-Cy5 CD33 PE Diagnosis CD7 CD7 APC APC CD15 FITC CD117 CD117 PE-Cy5 PE-Cy5 CD33 CD33 PE PE
39 Popula1on iden1fica1on Ga1ng strategy 1. CD45 vs SSC defined blast gate 2. CD34+ blasts colored red CD19 PE-CF total events collected WBC (viable only, nrbc excluded)
40 Popula1on iden1fica1on Ga1ng strategy 1. CD45 vs SSC defined blast gate 2. CD34+ blasts colored red 3. CD34 bright vs CD38 low CD19 PE-CF594 CD total events collected WBC (viable only, nrbc excluded)
41 Popula1on iden1fica1on Ga1ng strategy 1. CD45 vs SSC defined blast gate 2. CD34+ blasts colored red 3. CD34 bright vs CD38 low 4. CD34 vs CD15 demonstrates dysschronous an:gen expression 5. HLA-DR VS CD117 CD117 remains low, HLA-DR is even lower than was seen at diagnosis CD19 PE-CF594 CD34+ CD117 PE-Cy total events collected WBC (viable only, nrbc excluded) Abnormal cells are 37 total events 0.01% of the WBC
42 Popula1on iden1fica1on Ga1ng strategy 1. CD45 vs SSC defined blast gate 2. CD34+ blasts colored red 3. CD34 bright vs CD38 low 4. CD34 vs CD15 demonstrates dysschronous an:gen expression 5. HLA-DR VS CD117 CD117 remains low, HLA-DR is even lower than was seen at diagnosis CD19 PE-CF594 CD34+ CD117 PE-Cy total events collected WBC (viable only, nrbc excluded) Abnormal cells are 37 total events 0.01% of the WBC
43 How many events does it take to cons1tute an abnormal popula1on? Controversial Most studies required at least events that cluster :ghtly together with mul:ple an:body combina:ons. More colors increases your specificity as you have more an:body combina:ons to evaluate To detect an event occurring at 0.01% (1/10,000) CV of 5% if you collect 400 events/4 X 10 6 CV of 10% if you collect 100 events/1 X 10 6 CV of 20% if you collect 25 events/2.5 X 10 5 Sta*s*cal versus analy*c sensi*vity See Hedley and Keeney 2012 for a discussion of rare event analysis


44 What if you had fewer events in this case? total events viable WBC 200,000 total 100,000 total 50,000 total CD117 PE-Cy5 CD117 PE-Cy5 CD117 PE-Cy5 CD117 PE-Cy5
45 How many colors are adequate Studies evalua:ng MRD by flow have been reported to evaluate between 3 and 10 colors simultaneously In general, the more colors u:lized, the higher the sensi:vity for picking up an abnormal popula:on Olaru et al demonstrated that by increasing the number of colors form 4 to 6, a greater number of LAIPs could be detected. 6 color tube allowed detec:on of 47 different LAIPS All of the 53 AML samples studies had at least one LAIP 4 color tube allowed detec:on of only 30 LAIPS
 to confirm.")
46 What if you had fewer colors? Consider a tube with CD45, CD34, CD38 and CD15 2. CD34++/CD38 low progenitors 3. CD34++/CD15 variable abnormal progenitors 1. CD45 vs SSC defined blast gate With 4 colors, you can get partly there but cannot check expression of other markers (CD7, CD13, CD33, CD117, HLA-DR) to confirm. Albeit, 4 colors would probably work in this case with a well chosen an:body panel. We will explore this ques:on further in a later case
47 Challenge 3: Blast immunophenotype may shig Blast popula:ons may change immunophenotype with treatment failure or at relapse Reported in over half of AML cases in some studies Described in 91% of cases in one study Changes described include A shit in an:gen expression on a blast popula:on A change in the dominant popula:on seen (perhaps related to challenge 1) Markers reported to shit commonly include CD13, CD33, CD34 may be gained at relapse Loss of CD56 and CD19 has been reported at relapse The changes may prevent you from iden:fica:on of an abnormal blast popula:on if you are strictly direc:ng your search to find a LAIP seen at diagnosis Abnormal popula:ons can usually s:ll be iden:fied by using a different from normal approach. References: Baer et al. 2001, Oelschlagel et al 2000, Macedo et al. 1996






48 Diagnosis 3 months later Early MRD + sample post treatment CD38 CD15 A594 FITC HLA-DR PB HLA-DR PB Overt relapse CD38 CD15 A594 FITC HLA-DR PB
49 Challenge 4: Understanding normal in res1ng and regenera1ve seings is cri1cal Understanding immunophenotypic changes that can arise with marrow regenera:on is cri:cal in dis:nguishing MRD from marrow regenera:on in the post chemotherapy sefng Several studies have detailed common LAIPS seen in AML and dis:nguished these from changes seen in normal and regenera:ng marrow Al-Mawali et al AJCP Olaru et al Cytometry Part B (Clinical Cytometry) Also important is understanding other normal popula:ons present in the blast gate so these are not confused for abnormal blasts Remember basophils and plasmacytoid dendri:c cells? Understanding how the AML MRD panels in your lab perform with normal specimens and with regenera:ng marrow is cri:cal before undertaking AML MRD tes:ng

 Monocy:c cells and increased overall (68%)")

50 60 year old female with history of chemotherapy for breast cancer, now with cytopenias and circula:ng blasts Bone marrow flow cytometry was performed Increased cells in the blast gate (CD117+ blasts comprise 6.5% of the WBC and aberrantly lack CD34) Monocy:c cells and increased overall (68%) and include an expanded (34%, yellow) immature subset with decreased to absent CD14 and par:al CD56 Of note, concurrent molecular tes:ng demonstrates the NPM1 muta:on WBCs WBCs WBCs CD117 PE-Cy5 CD14 PE-Cy55




51 Focus on the CD117+ component Pa:ent CD33 PE HLA-DR PB Normal Abnormal intensity of an:gen expression (increased, decreased or absent). Absent CD34, bright CD33 Mildly decreased CD38 Decreased to absent HLA-DR Asynchronous expression of an:gens associated with maturity with an:gens deno:ng immaturity Decreased CD38 with absent CD34, bright CD33 CD33 PE HLA-DR PB Homogeneous expression of an an:gen usually expressed at varying levels with matura:on Homogeneous, increased CD33 Expression of an:gens from other lineages. None NPM1+


52 Day 28 post therapy Normal CD33 PE HLA-DR PB CD33 PE HLA-DR PB As compared to a normal control, progenitor matura:on remains on the expected spectrum but is shited to the right and rela:vely homogeneous


53 Day 28 post therapy No blast popula1on similar to that seen at diagnosis is iden1fied Diagnosis HLA-DR PB Blast CD33 PE HLA-DR PB HLA-DR PB CD33 PE HLA-DR PB What is the purple highlighted by blue arrows? A. Hypogranular neutrophil? B. Basophil? C. Subset of normal blasts? D. Plasmacytoid dendri:c cell? NPM1-

54 Day 50 post transplant Pa:ent Begin by evalua:ng the following plots: Normal for comparison CD34 vs CD38 CD34 vs CD15 Diagnos:c Diagnosis specimen Nothing drama1c is apparent at first glance...



55 Day 50 post transplant However, in looking at other projec1ons, a popula1on is evident that expresses bright CD33 without HLA-DR that is absent in normal specimens. basophils Normal HLA-DR PB HLA-DR PB CD33 PE CD117 PE-Cy5 HLA-DR PB? GATING STRATEGY: 1. CD45 vs SSC defined blast gate 2. CD33 bright HLA-DR nega:ve cells 3. Bright CD117 with intermediate CD38 4. Note that CD34 is now posi:ve on a subset (was absent at diagnosis total events WBC HLA-DR PB HLA-DR PB HLA-DR PB 171 abnormal blasts 0.03% abnormal blasts



56 What if you had fewer colors? Consider the 4 color tube with CD45, CD34, CD38 and CD15 we tried in case 1 WBCs Iden:fying the abnormal popula:on would not be possible with this tube in this case CD38 CD15 A594 FITC





57 Follow up-day 80 post transplant WBCs CD38 A594 Relapsed AML with 15% CD117+ blasts CD33 PE HLA-DR PB Pa:ent at diagnois CD33 PE HLA-DR PB
58 Summary MRD is useful for prognos:ca:on in many hematopoie:c neoplasms including AML In AML, MRD has been proven to provide powerful prognos:c informa:on in both adult and pediatric popula:ons As we move forward MRD may impact risk adjusted therapeu:c strategies in AML Flow cytometry is currently applicable in most cases for MRD detec:on Currently applicable in more cases than molecular tes:ng although this may be shiting in the future Strategies include a difference from normal approach combined with iden:fying a LAIP
59 Summary Several unanswered ques:ons remain in AML MRD tes:ng by flow cytometry What is the best :me point to assess for MRD Controversial: Induc:on versus Consolida:on What is the most important threshold Range of 1% to any MRD Log reduc:on in abnormal cells What do you need to do if you want to bring AML MRD tes:ng into your lab Develop panels for MRD tes:ng At minimum 6 color: more colors=greater sensi:vity and specificity Must collect >500,000 events for adequate sensi:vity Get familiar with normal At bare minimum normal and 5-10 marrow regenera:on samples
60 References Utility of flow for MRD in AML Wood. Clinical Cytometry 2016;90(1): Araki et al. J Clin Oncol Feb 1; 34(4): Chen et al. JCO 2015;33(11): Bastos-Oreiro et al. European Jorunal of Haematology. 2014;93 (3): Walter et al. Significance of MRD before myeloablative allogeneic hematopoietic cell transplantation for AML in first and second complete remission. Blood. Pre-published online July 2013 Hourigan and Karp. Minimal residual disease in acute myeloid leukemia. Nature reviews in clinical oncology 2013;10: Loken et al. Residual disease detected by multidimentional flow cytometry signifies high relapse risk in patient s with de novo AML: a report from COG. Blood. 2013;120(8): Buccisano et al. Prognostic and therapeutic implications of minimal residual disease detection in acute myeloid leukemia. Blood. 2012;119(2): Walter et al. Impact of pre-transplant minimal residual disease, as detected by MFC, on outcome of myeloablative hematopoietic cell transplant for AML. Journal of Clinical Oncology. 2011;29: Buccisano et al. Cytogenetic and molecular diagnostic characterization combined to post consolidation MRD assessment by flow cytometry improves risk stratification in adult AML. Blood. 2010;116(13): Rubinitz et al. MRD directed therapy for childhood AML: results of the AML02 multicentre trial. Lancet Oncology. 2010;11:
61 References Utility of flow for MRD in AML Al-Mawali et al. The role of multiparameter flow cytometry for detection of MRD in AML. AJCP. 2009;131: Al-Mawali et al. The use of ROC analysis for detection of MRD using 5 color multiparameter flow cytometry in AML identifies patients with high risk of relapse. Cytometry Part B (Clinical Cytometry). 2009;76B: Al-Mawali et al. Incidence, sensitivity, and specificity of leukemia associated phenotypes in AML using specific 5 color multiparameter flow cytometry. AJCP. 2008;129: Olaru et al. Multiparametric analysis of normal and postchemotherapy bone marrow: implication for the detection of leukemia-associated immunophenotypes. Cytometry part B 2008;74b: Wood BL. Myeloid malignancies: myelodysplastic syndromes, myeloproliferative disorders, and acute myeloid leukemia. Clin Lab Med. Sep 2007;27(3): , vii. Kern et al. Determination of relapse risk based on assessment of MRD during complete remission by MPFC in unselected patients with acute myeloid leukemia. Blood 2004;104: Sievers et al. Immunophenotypic evidence of leukemia after induction therapy predicts relapse: results from a prospective Children s Cancer Group study of 353 patients with AML. Blood. 2003;101(9):
62 References Cont. Rare event analysis: Hedley and Keeney. Technical issues: flow cytometry and rare event analysis. International Journal of Laboratory Hematology. 2013;35: Immunophenotypic changes Baer et al. High frequency of immunophenotypic changes in acute myeloid leukemia at relapse: implications for residual disease detection. Blood 2001;97: Oleschlagel et al. Shift of aberrant antigen expression at relapse or at treatment failure in Acute leukemia. Cytometry. 2000;42: Macedo et al. Phenotypic changes in acute myeloid leukemia: implications in the detection of minimal residual disease. Journal of Clinical Pathology. 1996;49: Flow versus molecular MRD testing Rossi et al. Comparison between muiltiparameter flow cytometry and WT1-RNA quantification in monitoring MRD in AML without specific molecular targets. 2012;36: Inaba et al. Comparative analysis of different approaches to measure treatment response in AML. Journal of Clinical Oncology. 2012;30:




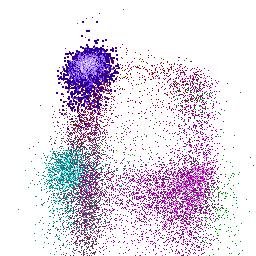
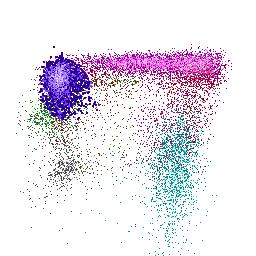
63 AML MRD normal WBCs CD19 PE-CF594 CD117 PE-Cy5 CD33 PE CD117 PE-Cy5 CD33 PE




64 AML MRD Normal, CD34+ myeloid blasts WBCs CD34+ CD34+ CD34+ CD34+ CD34+ CD34+ CD19 PE-CF594 CD34+ CD117 PE-Cy5 CD33 PE CD117 PE-Cy5 CD33 PE
Tools for MRD in AML: flow cytometry
 ACUTE MYELOID LEUKEMIA MEETING Ravenna - October 27, 2017 Tools for MRD in AML: flow cytometry Francesco Buccisano Can MRD improve outcome determina3on? No. of leukemic cells 10 12 10 10 10 8 10 6 10 4
ACUTE MYELOID LEUKEMIA MEETING Ravenna - October 27, 2017 Tools for MRD in AML: flow cytometry Francesco Buccisano Can MRD improve outcome determina3on? No. of leukemic cells 10 12 10 10 10 8 10 6 10 4
Multiparameter flow cytometry can be used to
 Minimal residual disease testing in Acute Leukemia Anjum Hassan MD Assistant Professor of Pathology and Immunology, Director FISH laboratory in Anatomic Pathology, Washington University in St Louis, School
Minimal residual disease testing in Acute Leukemia Anjum Hassan MD Assistant Professor of Pathology and Immunology, Director FISH laboratory in Anatomic Pathology, Washington University in St Louis, School
Minimal residual disease (MRD) in AML; coming of age. Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital
 in AML; coming of age. Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital") Minimal residual disease (MRD) in AML; coming of age Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital 1. The logistics of MRD assessment in AML 2. The clinical
Minimal residual disease (MRD) in AML; coming of age Dr. Mehmet Yılmaz Gaziantep University Medical School Sahinbey Education and Research hospital 1. The logistics of MRD assessment in AML 2. The clinical
VUmc Basispresentatie
 Clinical diagnostic cytometry Gerrit J Schuurhuis Dept of Hematology VU University Medical Center Amsterdam, Netherlands Use of immunophenotyping at diagnosis to trace residual disease after therapy 1.
Clinical diagnostic cytometry Gerrit J Schuurhuis Dept of Hematology VU University Medical Center Amsterdam, Netherlands Use of immunophenotyping at diagnosis to trace residual disease after therapy 1.
Reac%ve and Benign Flow Cytometry findings
 Reac%ve and Benign Flow Cytometry findings Lymph nodes and other /ssues Sindhu Cherian, MD University of Washington, Sea
Reac%ve and Benign Flow Cytometry findings Lymph nodes and other /ssues Sindhu Cherian, MD University of Washington, Sea
SUPPLEMENTARY FIG. S3. Kaplan Meier survival analysis followed with log-rank test of de novo acute myeloid leukemia patients selected by age <60, IA
 Supplementary Data Supplementary Appendix A: Treatment Protocols Treatment protocols of 123 cases patients were treated with the protocols as follows: 110 patients received standard DA (daunorubicin 45
Supplementary Data Supplementary Appendix A: Treatment Protocols Treatment protocols of 123 cases patients were treated with the protocols as follows: 110 patients received standard DA (daunorubicin 45
Meeting VAKB 8 februari 2011 Nancy Boeckx, MD, PhD
 Meeting VAKB 8 februari 2011 Nancy Boeckx, MD, PhD What is it? clonal expansion of myeloid precursor cells with reduced capacity to differentiate as opposed to ALL/CLL, it is limited to the myeloid cell
Meeting VAKB 8 februari 2011 Nancy Boeckx, MD, PhD What is it? clonal expansion of myeloid precursor cells with reduced capacity to differentiate as opposed to ALL/CLL, it is limited to the myeloid cell
Minimal Residual Disease as a Surrogate Endpoint in Acute Myeloid Leukemia Clinical Trials
 Minimal Residual Disease as a Surrogate Endpoint in Acute Myeloid Leukemia Clinical Trials Fda.gov Adriano Venditti Hematology, University Tor Vergata, Rome, Italy Minimal Residual Disease 10 12 Relapse
Minimal Residual Disease as a Surrogate Endpoint in Acute Myeloid Leukemia Clinical Trials Fda.gov Adriano Venditti Hematology, University Tor Vergata, Rome, Italy Minimal Residual Disease 10 12 Relapse
N Engl J Med Volume 373(12): September 17, 2015
: September 17, 2015") Review Article Acute Myeloid Leukemia Hartmut Döhner, M.D., Daniel J. Weisdorf, M.D., and Clara D. Bloomfield, M.D. N Engl J Med Volume 373(12):1136-1152 September 17, 2015 Acute Myeloid Leukemia Most
Review Article Acute Myeloid Leukemia Hartmut Döhner, M.D., Daniel J. Weisdorf, M.D., and Clara D. Bloomfield, M.D. N Engl J Med Volume 373(12):1136-1152 September 17, 2015 Acute Myeloid Leukemia Most
MRD detection in AML. Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome
 MRD detection in AML Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome Determinants of Treatment Response Leukemia Tumor burden Growth potential Drug resistance Karyotype Genetics Host
MRD detection in AML Adriano Venditti Hematology Fondazione Policlinico Tor Vergata Rome Determinants of Treatment Response Leukemia Tumor burden Growth potential Drug resistance Karyotype Genetics Host
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
CME. The Role of Multiparameter Flow Cytometry for Detection of Minimal Residual Disease in Acute Myeloid Leukemia
 Hematopathology / Minimal Residual Disease in AML The Role of Multiparameter Flow Cytometry for Detection of Minimal Residual Disease in Acute Myeloid Leukemia Adhra Al-Mawali, PhD, 1-3 David Gillis, MBBS,
Hematopathology / Minimal Residual Disease in AML The Role of Multiparameter Flow Cytometry for Detection of Minimal Residual Disease in Acute Myeloid Leukemia Adhra Al-Mawali, PhD, 1-3 David Gillis, MBBS,
Acute Lymphoblastic and Myeloid Leukemia
 Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Acute Lymphoblastic and Myeloid Leukemia Pre- and Post-Disease Form Acute Lympoblastic Leukemia Mary Eapen MD, MS Acute Lymphoblastic Leukemia SEER Age-adjusted incidence rate 1.6 per 100,000 men and women
Dr Prashant Tembhare
 Dr Prashant Tembhare docprt@gmail.com FCM very powerful technology in Identification and characterization of neoplastic plasma cells as it allows - simultaneous assessment of multiple antigens large numbers
Dr Prashant Tembhare docprt@gmail.com FCM very powerful technology in Identification and characterization of neoplastic plasma cells as it allows - simultaneous assessment of multiple antigens large numbers
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Journal of the Egyptian Nat. Cancer Inst., Vol. 13, No. 3, September: , 2001
 Journal of the Egyptian Nat. Cancer Inst., Vol. 13, No. 3, September: 191-201, 2001 Expression of the C-KIT Molecule in Acute Myeloid Leukemias: Implications of the Immunophenotypes CD117 and CD15 in the
Journal of the Egyptian Nat. Cancer Inst., Vol. 13, No. 3, September: 191-201, 2001 Expression of the C-KIT Molecule in Acute Myeloid Leukemias: Implications of the Immunophenotypes CD117 and CD15 in the
First relapsed childhood ALL Role of chemotherapy
 First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
First relapsed childhood ALL Role of chemotherapy Thirachit Chotsampancharoen, M.D. Division of Pediatric Hematology/Oncology Department of Pediatrics Prince of Songkla University Hat-Yai, Songkhla 25
PETHEMA; 2 HOVON; 3 PLAG and 4 GATLA Groups.
 Clinical significance of complex karyotype at diagnosis in Pa7ents with Acute Promyelocy7c Leukemia Treated with ATRA and chemotherapy based PETHEMA trials Labrador J 1, Montesinos P 1, Bernal T 1, Vellenga
Clinical significance of complex karyotype at diagnosis in Pa7ents with Acute Promyelocy7c Leukemia Treated with ATRA and chemotherapy based PETHEMA trials Labrador J 1, Montesinos P 1, Bernal T 1, Vellenga
Successful flow cytometric immunophenotyping of body fluid specimens
 Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
Successful flow cytometric immunophenotyping of body fluid specimens Fiona E. Craig, MD Division of Hematopathology Mayo Clinic Arizona 2017 MFMER slide-1 Financial disclosure No conflicts 2017 MFMER slide-2
Corporate Medical Policy. Policy Effective February 23, 2018
 Corporate Medical Policy Genetic Testing for FLT3, NPM1 and CEBPA Mutations in Acute File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_flt3_npm1_and_cebpa_mutations_in_acute_myeloid_leukemia
Corporate Medical Policy Genetic Testing for FLT3, NPM1 and CEBPA Mutations in Acute File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_flt3_npm1_and_cebpa_mutations_in_acute_myeloid_leukemia
Incidental Absolute Leukocytosis Connie Shen, MS2
 Incidental Absolute Leukocytosis Connie Shen, MS2 Clinical History An otherwise healthy 73-year-old Caucasian man presents for a rou=ne physical. Review of systems is nega=ve. A CBC was obtained and reveals
Incidental Absolute Leukocytosis Connie Shen, MS2 Clinical History An otherwise healthy 73-year-old Caucasian man presents for a rou=ne physical. Review of systems is nega=ve. A CBC was obtained and reveals
Molecular Advances in Hematopathology
 Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
V. Acute leukemia. Flow cytometry in evaluation of hematopoietic neoplasms: A case-based approach
 V. Acute leukemia Evaluating a sample for an acute leukemia Acute leukemia is a neoplasm of immature myeloid or lymphoid cells characterized by a block in maturation, usually at the stage of an early progenitor
V. Acute leukemia Evaluating a sample for an acute leukemia Acute leukemia is a neoplasm of immature myeloid or lymphoid cells characterized by a block in maturation, usually at the stage of an early progenitor
NUMERATOR: Patients who had baseline cytogenetic testing performed on bone marrow
 Quality ID #67 (NQF 0377): Hematology: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow National Quality Strategy Domain: Effective Clinical Care
Quality ID #67 (NQF 0377): Hematology: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow National Quality Strategy Domain: Effective Clinical Care
Mast Cell Disease Case 054 Session 7
 Mast Cell Disease Case 054 Session 7 Rodney R. Miles, M.D., Ph.D. Lauren B. Smith, M.D. Cem Akin, M.D. Diane Roulston,, Ph.D. Charles W. Ross, M.D. Departments of Pathology and Internal Medicine University
Mast Cell Disease Case 054 Session 7 Rodney R. Miles, M.D., Ph.D. Lauren B. Smith, M.D. Cem Akin, M.D. Diane Roulston,, Ph.D. Charles W. Ross, M.D. Departments of Pathology and Internal Medicine University
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Kerrie Clerici, Michael Swain, Dominic Fernandez, Julia Schulz, Matthew Archer, Janine Campbell
 Minimal Residual Disease (MRD) Testing by Flow Cytometry for childhood Precursor B Cell Acute Lymphoblastic Leukaemia Royal Children s Hospital experience. Kerrie Clerici, Michael Swain, Dominic Fernandez,
Minimal Residual Disease (MRD) Testing by Flow Cytometry for childhood Precursor B Cell Acute Lymphoblastic Leukaemia Royal Children s Hospital experience. Kerrie Clerici, Michael Swain, Dominic Fernandez,
MRD in ALL: Correct interpretation in clinical practice. Deepak Bansal Prof., Pediatric Hematology-Oncology unit PGIMER, Chandigarh
 MRD in ALL: Correct interpretation in clinical practice Deepak Bansal Prof., Pediatric Hematology-Oncology unit PGIMER, Chandigarh Minimal residual disease Subclinical level of residual leukemia Below
MRD in ALL: Correct interpretation in clinical practice Deepak Bansal Prof., Pediatric Hematology-Oncology unit PGIMER, Chandigarh Minimal residual disease Subclinical level of residual leukemia Below
AML Genomics 11/27/17. Normal neutrophil maturation. Acute Myeloid Leukemia (AML) = block in differentiation. Myelomonocy9c FAB M5
 = block in differentiation. Myelomonocy9c FAB M5") AML Genomics 1 Normal neutrophil maturation Acute Myeloid Leukemia (AML) = block in differentiation AML with minimal differen9a9on FAB M1 Promyelocy9c leukemia FAB M3 Myelomonocy9c FAB M5 2 1 Principle
AML Genomics 1 Normal neutrophil maturation Acute Myeloid Leukemia (AML) = block in differentiation AML with minimal differen9a9on FAB M1 Promyelocy9c leukemia FAB M3 Myelomonocy9c FAB M5 2 1 Principle
ETP - Acute Lymphoblastic Leukaemia
 ETP - Acute Lymphoblastic Leukaemia Dr Sally Campbell - Royal Children s Hospital Melbourne 24 February 2017 T-ALL 12-15% of all newly diagnosed ALL cases in pediatrics are T-ALL T-ALL behaves differently
ETP - Acute Lymphoblastic Leukaemia Dr Sally Campbell - Royal Children s Hospital Melbourne 24 February 2017 T-ALL 12-15% of all newly diagnosed ALL cases in pediatrics are T-ALL T-ALL behaves differently
Na#onal Neutropenia Network Family Conference July 12, 2014
 Na#onal Neutropenia Network Family Conference July 12, 2014 Jim Connelly, MD Assistant Professor of Pediatrics and Communicable Diseases Blood and Marrow Transplant Program University of Michigan Transplant
Na#onal Neutropenia Network Family Conference July 12, 2014 Jim Connelly, MD Assistant Professor of Pediatrics and Communicable Diseases Blood and Marrow Transplant Program University of Michigan Transplant
Standard risk ALL (and its exceptions
 Mahshid Mehdizadeh Standard risk ALL (and its exceptions WBC at diagnosis below 50 109/L - age 1 year - no central nervous system (CNS) involvement - ETV6/RUNX1 positivity - MRD at Day
Mahshid Mehdizadeh Standard risk ALL (and its exceptions WBC at diagnosis below 50 109/L - age 1 year - no central nervous system (CNS) involvement - ETV6/RUNX1 positivity - MRD at Day
Flow cytometry leukocyte differential : a critical appraisal
 Flow cytometry leukocyte differential : a critical appraisal Francis Lacombe Flow cytometry department University Hospital of Bordeaux, Pessac, France francis.lacombe@chu-bordeaux.fr 2008 HORIBA ABX, All
Flow cytometry leukocyte differential : a critical appraisal Francis Lacombe Flow cytometry department University Hospital of Bordeaux, Pessac, France francis.lacombe@chu-bordeaux.fr 2008 HORIBA ABX, All
The Hierarchical Organization of Normal and Malignant Hematopoiesis
 The Hierarchical Organization of Normal and Malignant Hematopoiesis NORMAL Hematopoie2c Stem Cell (HSC) Leukemia Stem Cells (LSC) MPP MLP CMP Leukemic Progenitors MEP GMP B/NK ETP Leukemic Blasts Erythrocytes
The Hierarchical Organization of Normal and Malignant Hematopoiesis NORMAL Hematopoie2c Stem Cell (HSC) Leukemia Stem Cells (LSC) MPP MLP CMP Leukemic Progenitors MEP GMP B/NK ETP Leukemic Blasts Erythrocytes
Mixed Phenotype Acute Leukemias
 Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow
 and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow") Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Personalized Therapy for Acute Myeloid Leukemia. Patrick Stiff MD Loyola University Medical Center
 Personalized Therapy for Acute Myeloid Leukemia Patrick Stiff MD Loyola University Medical Center 708-327-3216 Major groups of Mutations in AML Targets for AML: Is this Achievable? Chronic Myeloid Leukemia:
Personalized Therapy for Acute Myeloid Leukemia Patrick Stiff MD Loyola University Medical Center 708-327-3216 Major groups of Mutations in AML Targets for AML: Is this Achievable? Chronic Myeloid Leukemia:
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Dana-Farber Cancer Institute, Boston, MA; 2 City of Hope National Medical Center, Duarte, CA; 3 Roswell Park Cancer Institute, Buffalo, NY; 4
 Results from Ongoing Phase 2 Trial of SL-401 As Consolidation Therapy in Patients with Acute Myeloid Leukemia (AML) in Remission with High Relapse Risk Including Minimal Residual Disease (MRD) Andrew A.
Results from Ongoing Phase 2 Trial of SL-401 As Consolidation Therapy in Patients with Acute Myeloid Leukemia (AML) in Remission with High Relapse Risk Including Minimal Residual Disease (MRD) Andrew A.
Trapianto allogenico convenzionale
 Il trapianto nella leucemia acuta mieloide a rischio intermedio Trapianto allogenico convenzionale Trapianto allogenico nelle Leucemie Acute Mieloidi in I RC D. Pastore Ematologia con Trapianto-Bari Domenico
Il trapianto nella leucemia acuta mieloide a rischio intermedio Trapianto allogenico convenzionale Trapianto allogenico nelle Leucemie Acute Mieloidi in I RC D. Pastore Ematologia con Trapianto-Bari Domenico
Recommended Timing for Transplant Consultation
 REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
PDF of Trial CTRI Website URL -
 Clinical Trial Details (PDF Generation Date :- Wed, 19 Dec 2018 02:45:15 GMT) CTRI Number Last Modified On 25/12/2017 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Clinical Trial Details (PDF Generation Date :- Wed, 19 Dec 2018 02:45:15 GMT) CTRI Number Last Modified On 25/12/2017 Post Graduate Thesis Type of Trial Type of Study Study Design Public Title of Study
Regulatory Aspects - AML & CLL
 Regulatory Aspects - AML & CLL Dr Beatriz Flores November 2018 Disclaimer The views and opinions expressed in the following PowerPoint slides are those of the individual presenter and should not be attributed
Regulatory Aspects - AML & CLL Dr Beatriz Flores November 2018 Disclaimer The views and opinions expressed in the following PowerPoint slides are those of the individual presenter and should not be attributed
Acute Myeloid Leukemia: A Patient s Perspective
 Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
Acute Myeloid Leukemia: A Patient s Perspective Patrick A Hagen, MD, MPH Cardinal Bernardin Cancer Center Loyola University Medical Center Maywood, IL Overview 1. What is AML? 2. Who gets AML? Epidemiology
THE USE OF WT1-QPCR TO MEASURE AND DETECT MINIMAL RESIDUAL DISEASE IN ACUTE MYELOID LEUKEMIA. Ava Greco
 THE USE OF WT1-QPCR TO MEASURE AND DETECT MINIMAL RESIDUAL DISEASE IN ACUTE MYELOID LEUKEMIA Ava Greco REVIEW OF LITERATURE What is Leukemia? Abnormal growth of cells in the blood stream Progresses rapidly
THE USE OF WT1-QPCR TO MEASURE AND DETECT MINIMAL RESIDUAL DISEASE IN ACUTE MYELOID LEUKEMIA Ava Greco REVIEW OF LITERATURE What is Leukemia? Abnormal growth of cells in the blood stream Progresses rapidly
FLOW CYTOMETRIC ANALYSIS OF NORMAL BONE MARROW
 XI International Conference Hematopoiesis Immunology Budapest, June 6-7, 2014 FLO CYTOMETRIC ANALYSIS OF NORMAL BONE MARRO Bruno Brando and Arianna Gatti Hematology Laboratory and Transfusion Center Legnano
XI International Conference Hematopoiesis Immunology Budapest, June 6-7, 2014 FLO CYTOMETRIC ANALYSIS OF NORMAL BONE MARRO Bruno Brando and Arianna Gatti Hematology Laboratory and Transfusion Center Legnano
Multi-color flow cytometric immunophenotyping for detection of minimal residual disease in AML: past, present and future
 Bone Marrow Transplantation (2014) 49, 1129 1138 2014 Macmillan Publishers Limited All rights reserved 0268-3369/14 www.nature.com/bmt REVIEW Multi-color flow cytometric immunophenotyping for detection
Bone Marrow Transplantation (2014) 49, 1129 1138 2014 Macmillan Publishers Limited All rights reserved 0268-3369/14 www.nature.com/bmt REVIEW Multi-color flow cytometric immunophenotyping for detection
Acute myeloid leukemia: prognosis and treatment. Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg
 Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
Acute myeloid leukemia: prognosis and treatment Dimitri A. Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Campus Stuivenberg Patient Female, 39 years History: hypothyroidism Present:
Correspondence should be addressed to Anas Khanfar;
 Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Measurable/Minimal Residual Disease in Patients with Acute Myeloid Leukemia Undergoing Transplantation
 Measurable/Minimal Residual Disease in Patients with Acute Myeloid Leukemia Undergoing Transplantation June 9, 2018 Dave Sanford The Leukemia/Bone Marrow Transplant Program of British Columbia Disclosures
Measurable/Minimal Residual Disease in Patients with Acute Myeloid Leukemia Undergoing Transplantation June 9, 2018 Dave Sanford The Leukemia/Bone Marrow Transplant Program of British Columbia Disclosures
MUD SCT for Paediatric AML?
 7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
7 th South African Symposium on Haematopoietic Stem Cell Transplantation MUD SCT for Paediatric AML? Alan Davidson Haematology / Oncology Service Red Cross Children s Hospital THE SCENARIO A 10 year old
Multidimensional Flow Cytometry for Detection of Rare Populations in Hematological Malignancies
 TZU CHI MED J March 2009 Vol 21 No 1 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Original Article Multidimensional Flow Cytometry for Detection of Rare Populations in Hematological
TZU CHI MED J March 2009 Vol 21 No 1 available at http://ajws.elsevier.com/tcmj Tzu Chi Medical Journal Original Article Multidimensional Flow Cytometry for Detection of Rare Populations in Hematological
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Case #1. 65 yo man with no prior history presented with leukocytosis and circulating blasts: Bone marrow biopsy was performed
 Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD
 Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Photo by Tynan Studio Johann Hitzler, MD, FRCPC, FAAP Jacqueline Halton, MD, FRCPC Jason D. Pole, PhD 96 Atlas of Childhood Cancer in Ontario (1985-2004) Chapter 6: Leukemia 6 Leukemia Atlas of Childhood
Evolving Targeted Management of Acute Myeloid Leukemia
 Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
Evolving Targeted Management of Acute Myeloid Leukemia Jessica Altman, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Learning Objectives Identify which mutations should be assessed
STEM CELL TRANSPLANTATION FOR ACUTE MYELOID LEUKEMIA
 STEM CELL TRANSPLANTATION FOR ACUTE MYELOID LEUKEMIA Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
STEM CELL TRANSPLANTATION FOR ACUTE MYELOID LEUKEMIA Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
Indication for unrelated allo-sct in 1st CR AML
 Indication for unrelated allo-sct in 1st CR AML It is time to say! Decision of allo-sct: factors to be considered Cytogenetic risk status Molecular genetics FLT3; NPM1, CEBPA. Response to induction Refractoriness
Indication for unrelated allo-sct in 1st CR AML It is time to say! Decision of allo-sct: factors to be considered Cytogenetic risk status Molecular genetics FLT3; NPM1, CEBPA. Response to induction Refractoriness
Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute leukemia
 Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
New drugs in Acute Leukemia. Cristina Papayannidis, MD, PhD University of Bologna
 New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia
 Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
CSP04 Topics in Hematopathology: Flow Cytometry and Molecular Genetics as Tools for Understanding, Diagnosing, and Treating Hematolymphoid Malignancy
 CSP04 Topics in Hematopathology: Flow Cytometry and Molecular Genetics as Tools for Understanding, Diagnosing, and Treating Hematolymphoid Malignancy William Morice MD, PhD Horatiu Olteanu MD, PhD Andrew
CSP04 Topics in Hematopathology: Flow Cytometry and Molecular Genetics as Tools for Understanding, Diagnosing, and Treating Hematolymphoid Malignancy William Morice MD, PhD Horatiu Olteanu MD, PhD Andrew
23/10/2017. Analysis of bone marrow for MDSrelated. Approach used at Hematopathology, Lund
 Approach used at Hematopathology, Lund Analysis of bone marrow for MDSrelated aberrancies According to International/ELN Flow Cytometry Working Group (IMDSFlow) Anna Porwit Lund, Sweden 1. new patients
Approach used at Hematopathology, Lund Analysis of bone marrow for MDSrelated aberrancies According to International/ELN Flow Cytometry Working Group (IMDSFlow) Anna Porwit Lund, Sweden 1. new patients
NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia
 Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Case 24 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Aliyah Rahemtullah 1, Martin K Selig 1, Paola Dal Cin 2 and Robert P Hasserjian 1 Departments of Pathology,
Welcome and Introductions
 Information for Patients With Acute Myeloid Leukemia (AML) Welcome and Introductions Information for Patients With Acute Myeloid Leukemia (AML) Mark B. Juckett, MD Vice Chair for Clinical Affairs and Quality
Information for Patients With Acute Myeloid Leukemia (AML) Welcome and Introductions Information for Patients With Acute Myeloid Leukemia (AML) Mark B. Juckett, MD Vice Chair for Clinical Affairs and Quality
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Form 2011 R4.0: Acute Lymphoblastic Leukemia (ALL) Pre-HCT Data
 Pre-HCT Data") Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Key Fields Sequence Number: Date Received: - - CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: - - HCT type: (check all that apply) Autologous Allogeneic,
Test Name Results Units Bio. Ref. Interval. Positive
 LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
LL - LL-ROHINI (NATIONAL REFERENCE 135091533 Age 28 Years Gender Male 1/9/2017 120000AM 1/9/2017 105415AM 4/9/2017 23858M Ref By Final LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE, ANY 6 MARKERS t (1;19) (q23
Early Clearance of Peripheral Blood Blasts Predicts Response to Induction Chemotherapy in Acute Myeloid Leukemia
 Early Clearance of Peripheral Blood Blasts Predicts Response to Induction Chemotherapy in Acute Myeloid Leukemia Martha Arellano, MD 1 ; Suchita Pakkala, MD 1 ; Amelia Langston, MD 1 ; Mourad Tighiouart,
Early Clearance of Peripheral Blood Blasts Predicts Response to Induction Chemotherapy in Acute Myeloid Leukemia Martha Arellano, MD 1 ; Suchita Pakkala, MD 1 ; Amelia Langston, MD 1 ; Mourad Tighiouart,
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
CLINICAL USE OF CELLULAR SUBPOPULATION ANALYSIS IN BM
 CLINICAL USE OF CELLULAR SUBPOPULATION ANALYSIS IN BM CANCER RESEARCH CENTRE, UNIVERSITY AND UNIVERSITY HOSPITAL OF SALAMANCA (SPAIN)( Sao Paulo, 18th of April, 2009 IDENTIFICATION OF HPC (I) 1.- In vivo
CLINICAL USE OF CELLULAR SUBPOPULATION ANALYSIS IN BM CANCER RESEARCH CENTRE, UNIVERSITY AND UNIVERSITY HOSPITAL OF SALAMANCA (SPAIN)( Sao Paulo, 18th of April, 2009 IDENTIFICATION OF HPC (I) 1.- In vivo
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
MDS/MPN: What it is and How it Should be Treated?
 MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Myelodysplastic scoring system with flow cytometry. G Detry B Husson
 Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Significant CD5 Expression on Normal Stage 3 Hematogones and Mature B Lymphocytes in Bone Marrow
 Hematopathology / CD5 Expression on Normal B Cells Significant CD5 Expression on Normal Stage 3 Hematogones and Mature B Lymphocytes in Bone Marrow Franklin S. Fuda, DO, Nitin J. Karandikar, MD, PhD, and
Hematopathology / CD5 Expression on Normal B Cells Significant CD5 Expression on Normal Stage 3 Hematogones and Mature B Lymphocytes in Bone Marrow Franklin S. Fuda, DO, Nitin J. Karandikar, MD, PhD, and
New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke
 University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
ACUTE LYMPHOBLASTIC LEUKEMIA
 ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
ACUTE LYMPHOBLASTIC LEUKEMIA YOUNG ADULT PATIENT Highlights clonoseq Tracking (MRD) Testing in the peripheral blood revealed early signs of relapse post-transplant Patient achieved remission after CAR-T
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Standard immunophenotyping of leukemia cells in acute myeloid leukemia (AML)
") Clinical immunology Standard immunophenotyping of leukemia cells in acute myeloid leukemia (AML) ` JOLANTA WOZNIAK, JOANNA KOPEÆ-SZLÊZAK Department of Haematological Cytobiology, Institut of Haematology
Clinical immunology Standard immunophenotyping of leukemia cells in acute myeloid leukemia (AML) ` JOLANTA WOZNIAK, JOANNA KOPEÆ-SZLÊZAK Department of Haematological Cytobiology, Institut of Haematology
Chronic lymphocytic leukemia is eradication feasible and worthwhile?
 Chronic lymphocytic leukemia is eradication feasible and worthwhile? Gianluca Gaidano, MD, PhD Division of Hematology Department of Clinical and Experimental Medicine Amedeo Avogardo University of Eastern
Chronic lymphocytic leukemia is eradication feasible and worthwhile? Gianluca Gaidano, MD, PhD Division of Hematology Department of Clinical and Experimental Medicine Amedeo Avogardo University of Eastern
A pediatric patient with acute leukemia of ambiguous lineage with a NUP98-NSD1 rearrangement SH
 A pediatric patient with acute leukemia of ambiguous lineage with a NUP98NSD1 rearrangement SH20170203 Rebecca LeemanNeill, Ronald Rice, Anita Malek, Patricia Raciti, Susan Hsiao, Mahesh Mansukhani, Bachir
A pediatric patient with acute leukemia of ambiguous lineage with a NUP98NSD1 rearrangement SH20170203 Rebecca LeemanNeill, Ronald Rice, Anita Malek, Patricia Raciti, Susan Hsiao, Mahesh Mansukhani, Bachir
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328
 Rearrangement Following Therapy for APL Case 0328") Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Therapy-related MDS/AML with KMT2A (MLL) Rearrangement Following Therapy for APL Case 0328 Kenneth N. Holder, Leslie J. Greebon, Gopalrao Velagaleti, Hongxin Fan, Russell A. Higgins Initial Case: Clinical
Leukine. Leukine (sargramostim) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Leukine Page: 1 of 6 Last Review Date: November 30, 2018 Leukine Description Leukine (sargramostim)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Leukine Page: 1 of 6 Last Review Date: November 30, 2018 Leukine Description Leukine (sargramostim)
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Acute Myeloid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_acute_myeloid_leukemia
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Acute Myeloid File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_acute_myeloid_leukemia
Normal & Leukaemic haematopoiesis. Dr. Liu Te Chih Dept of Haematology / Oncology National University Health Services Singapore
 Normal & Leukaemic haematopoiesis 2010 Dr. Liu Te Chih Dept of Haematology / Oncology National University Health Services Singapore Use of Immunophenotyping today Lineage assignment Differentiation of
Normal & Leukaemic haematopoiesis 2010 Dr. Liu Te Chih Dept of Haematology / Oncology National University Health Services Singapore Use of Immunophenotyping today Lineage assignment Differentiation of
Pacharapan Surapolchai, MD Associate Professor Department of Pediatrics, Faculty of Medicine, Thammasat University, Thailand October 2018
 Pacharapan Surapolchai, MD Associate Professor Department of Pediatrics, Faculty of Medicine, Thammasat University, Thailand October 2018 Outline Case study Introduction of Current management of infantile
Pacharapan Surapolchai, MD Associate Professor Department of Pediatrics, Faculty of Medicine, Thammasat University, Thailand October 2018 Outline Case study Introduction of Current management of infantile
GENETIC TESTING FOR FLT3, NPM1 AND CEBPA VARIANTS IN CYTOGENETICALLY NORMAL ACUTE MYELOID LEUKEMIA
 CYTOGENETICALLY NORMAL ACUTE MYELOID LEUKEMIA Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,
CYTOGENETICALLY NORMAL ACUTE MYELOID LEUKEMIA Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures,
Test Name Results Units Bio. Ref. Interval. Positive
 Lab No 135091548 Age 35 Years Gender Female 1/9/2017 120000AM 1/9/2017 103420AM 4/9/2017 23753M Ref By Dr UNKNWON Final Test Results Units Bio Ref Interval LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE 3 t (1;19)
Lab No 135091548 Age 35 Years Gender Female 1/9/2017 120000AM 1/9/2017 103420AM 4/9/2017 23753M Ref By Dr UNKNWON Final Test Results Units Bio Ref Interval LEUKEMIA DIAGNOSTIC COMREHENSIVE ROFILE 3 t (1;19)
Hevylite assays de - convoluted. Dr Karthik Ramasamy Oxford University Hospitals
 Hevylite assays de - convoluted Dr Karthik Ramasamy Oxford University Hospitals Overview Hevylite assay Introduction Clinical utility of Hevylite 2 Hevylite specifici.es Hevylite specifici.es Hevylite
Hevylite assays de - convoluted Dr Karthik Ramasamy Oxford University Hospitals Overview Hevylite assay Introduction Clinical utility of Hevylite 2 Hevylite specifici.es Hevylite specifici.es Hevylite
Disclosures of Massimo Breccia
 Disclosures of Massimo Breccia Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Novar
Disclosures of Massimo Breccia Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Novar
Risk-adapted therapy of AML in younger adults. Sergio Amadori Tor Vergata University Hospital Rome
 Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
Risk-adapted therapy of AML in younger adults Sergio Amadori Tor Vergata University Hospital Rome Pescara 11/2010 AML: treatment outcome Age CR % ED % DFS % OS %
Medical Policy. MP Hematopoietic Cell Transplantation for Acute Myeloid Leukemia
 Medical Policy MP 8.01.26 BCBSA Ref. Policy: 8.01.26 Last Review: 01/30/2018 Effective Date: 01/30/2018 Section: Therapy Related Policies 2.04.124 Genetic Testing for FLT3, NPM1, and CEBPA Variants in
Medical Policy MP 8.01.26 BCBSA Ref. Policy: 8.01.26 Last Review: 01/30/2018 Effective Date: 01/30/2018 Section: Therapy Related Policies 2.04.124 Genetic Testing for FLT3, NPM1, and CEBPA Variants in
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Research Article Myeloid Sarcoma: Clinicopathologic, Cytogenetic, and Outcome Analysis of 21 Adult Patients
 SAGE-Hindawi Access to Research Leukemia Research and Treatment Volume 2011, Article ID 523168, 4 pages doi:10.4061/2011/523168 Research Article Myeloid Sarcoma: Clinicopathologic, Cytogenetic, and Outcome
SAGE-Hindawi Access to Research Leukemia Research and Treatment Volume 2011, Article ID 523168, 4 pages doi:10.4061/2011/523168 Research Article Myeloid Sarcoma: Clinicopathologic, Cytogenetic, and Outcome