Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
|
|
|
- Chloe Caldwell
- 5 years ago
- Views:
Transcription
1 Mark slides
2 Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
3 Hyperlipidemia is a common problem Nearly 50% of men in the over the age of 20 in the US have an LDL > 130 mg/dl (~45% for women) Approximately 20% of men and 17% of women have an LDL cholesterol > 160 mg/dl An estimated 40 million Americans have CHD, PVD, CVD, or DM
4 Topics for Today What should our targets be for cholesterol lowering a review of the NCEP guidelines What are the data supporting use of medications to lower cholesterol in primary prevention and secondary prevention What do we still need to know? unanswered questions
5
6 Evolution of the NCEP Guidelines ATP I 1970s 1988 ATP II ATP III MRFIT LRC-CPPT Coronary Drug Project Helsinki Heart Study Framingham Angiographic Trials (FATS, POSCH, SCOR, STARS, Ornish, MARS) Meta-Analyses (Holme, Rossouw) 4S, WOSCOPS, CARE, LIPID, AFCAPS/TexCAPS, VA-HIT, others CLAS (angio)
7 LDL Cholesterol Goals and Cutpoints for Therapeutic Lifestyle Changes (TLC) and Drug Therapy in Different Risk Categories 6 Risk Category LDL Goal (mg/dl) LDL Level at Which to Initiate Therapeutic Lifestyle Changes (TLC) (mg/dl) LDL Level at Which to Consider Drug Therapy (mg/dl) CHD or CHD Risk Equivalents (10-year risk >20%) < ( : drug optional) 2+ Risk Factors (10-year risk 20%) < year risk 10 20%: year risk <10%: Risk Factor < ( : LDLlowering drug optional)
8 CHD risk equivalents Patients with known CHD have a 10 year risk of recurrent events of >20% Patients with CHD risk equivalents -- symptomatic carotid disease, peripheral arterial disease, AAA, diabetes -have a similar risk of >20% for hard CHD ( CHD death or MI)
9 Assessing 10 year CHD risk Estimated CHD risk is based on Framingham Data Patients with known CHD or CHD equivalent have a 10 yr risk of >20% Patients with 0-1 risk factors have a 10 year risk of <10% Patients with 2 or more risk factors have a 10 year risk between 0 and 20%
10 Reaching treatment goals: TLC or Drug therapy Therapeutic Lifestyle Changes ( TLC) are recommended as the initial treatment step for all individuals not at their treatment goal Drug therapy should be promptly initiated for all patients whose LDL is 30 mg/dl greater than goal, except for very low risk individuals
11 Case 1 A 64 y/o male patient presents for an initial clinic visit. PMH is notable for CHD ( s/p IMI 2 years ago) HTN, smoking Current Meds :ASA 81 mg po qd, atenolol 50 mg po qd, lisinopril 10 mg po qd, omeprazole 20 mg po qd. Fasting lipid profile LDL 95, HDL 45, TG 150, Total cholesterol 185 Should he be on a statin?
12 How should we go? Low Two distinct issues 1) Should patients with low baseline LDL (<100) and known CHD be treated? 2) For patients on lipid lowering medication, what should our treatment target be? 130 mg/dl, 100 mg/dl, 75mg/dl
13 How Low should we go? ( continued) Major lipid lowering trials have generally compared a single statin dose vs. placebo rather than comparing specific treatment target LDL levels Target LDL levels have been inferred based upon 1)epidemiological data demonstrating a curvilinear relationship between LDL and CHD; 2)baseline and post-treatment LDL levels that have been associated with reduction in clinical endpoints in lipid lowering trials
14 My Drug Study Sounds Catchier 4S CARE LIPID WOSCOPS REVERSAL PROVE-IT SEARCH TNT TOAST than Yours
15 Prevention Strategies Primary Prevention Prevention of events in patients without known heart disease Mortality of acute MI approaches 25% Secondary prevention Prevention of recurrent events in individuals with known disease
16 The Pyramid of Recent Trials Relative Size of the Various Segments of the Population Very high cholesterol with CHD or MI Moderately high cholesterol in high risk CHD or MI Normal cholesterol with CHD or MI 4S LIPID CARE High cholesterol without CHD or MI WOSCOPS No history of CHD or MI AFCAPS/TexCAPS
17 Summary Data Statin Trials Trial Initial LDL Final LDL LDL% Change Event Rate Statin Event Rate- Placebo RRR % ARR % NNT 4S LIPID CARE WOSCOPS AFCAPS/ TEXCAPS
18 Endpoint Trials with the Statins Trial Primary Prevention AFCAPS/TexCAPS WOSCOPS Secondary Prevention 4S CARE LIPID Ischemia MIRACL AVERT Drug Lovastatin Pravastatin Simvastatin Pravastatin Pravastatin Atorvastatin Atorvastatin CHD Risk Reduction 40%* 31%* 34%* 24%* 24%* 26%** 36%** *Nonfatal MI or CHD death; **ischemic events Downs JR et al. JAMA 1998;279: Shepherd J et al. N Engl J Med 1999;333: Scandinavian Simvastatin Study Group. Lancet 1994;344: Sacks FM et al. N Engl J Med 1996;335: LIPID Study Group. N Engl J Med 1998;339: Schwartz GG et al. JAMA 2001;285: Pitt B et al. N Engl J Med 1999;341:70-76.
 Shepherd J et al. N Engl J Med. 1995;333:1301-1307. 4S Study Group. Lancet.")
19 Relation Between CHD Events and LDL-C in Recent Statin Trials 30 4S-PI 25 2 Prevention 20 4S-Rx % with CHD event LIPID-Rx CARE-Rx LIPID-PI CARE-PI AFCAPS/TexCAPS-PI AFCAPS/TexCAPS-Rx WOSCOPS-Rx 1 Prevention WOSCOPS-PI PI=placebo; Rx=treatment Mean LDL-C level at follow-up (mg/dl) Shepherd J et al. N Engl J Med. 1995;333: S Study Group. Lancet. 1995;345: Sacks FM et al. N Engl J Med. 1996;335: Downs JR et al. JAMA. 1998;279: Tonkin A. Presented at AHA Scientific Sessions, TM 1999 Professional Postgraduate Services
20 Heart Protection Study Secondary prevention study in the UK 20,356 adults Age at entry, 5 year follow up PMH + for CHD, PVD, DM or Males> 65 with HTN Total cholesterol>135 mg/dl (3500 had baseline LDL <100) 40 mg simvastatin vs. placebo
21 Heart Protection Study Endpoints Coronary events: MI, coronary death Stroke Revascularization Cause specific mortality All cause mortality
22 Simvastatin: Cause-Specific Mortality Cause of Death Vascular Coronary Other vascular ANY VASCULAR Nonvascular Neoplastic Respiratory Other medical Nonmedical NONVASCULAR ALL CAUSES Simvastatin (10,269) (7.6%) (5.3%) 1328 (12.9%) Placebo (10,267) (9.1%) (5.6%) 1507 (14.7%) Risk ratio and 95% CI STATIN Better PLACEBO Better 17% SE 4 reduction (2P<0.0001) 5% SE 6 reduction (NS) 13% SE 4 reduction (2P<0.001) Heart Protection Study Collaborative Group. Lancet 2002;360: Reprinted with permission from Elsevier Science.
23 People Suffering Events (%) Simvastatin: Major Vascular Events by Year Placebo Years of Follow-up Simvastatin Benefit/1000 (SE): 5 (3) 20 (4) 35 (5) 46 (5) 54 (7) 60 (18) 6
24 HPS: Major Vascular Events by LDL Lipid Levels at Entry LDL cholesterol (mg/dl) Simvastatin (10,269) Cholesterol Placebo (10,267) Risk ratio and 95% CI STATIN Better PLACEBO Better < (16.4%) 358 (21.0%) 100 < (18.9%) 871 (24.7%) (21.6%) 1356 (26.9%) ALL PATIENTS 2033 (19.8%) 2585 (25.2%) 24% SE 3 reduction (2P< )
25 Age < Sex Baseline Feature 75 Male Female ALL PATIENTS Simvastatin: Major Vascular Events by Age and Sex Simvastatin (10,269) 831 (16.9%) 512 (20.9%) 548 (23.8%) 142 (23.1%) 1666 (21.6%) 367 (14.4%) 2033 (19.8%) Placebo (10,267) 1091 (22.1%) 665 (27.2%) 620 (27.7%) 209 (32.3%) 2135 (27.6%) 450 (17.7%) 2585 (25.2%) 0.4 Risk ratio and 95% CI STATIN Better PLACEBO Better 24% SE 3 reduction (2P< ) Heart Protection Study Collaborative Group. Lancet 2002;360:
26 The CHD Risk of HPS and ATP III CHD and CHD Risk Equivalent Patients Based on risk of CHD death or nonfatal MI HPS (5-yr risk) ATP III CHD and Risk Equivalents (10-yr risk) All Patients 25% LDL-C % LDL-C % LDL-C <100 21% Acute MI 26 51% Revascularization 25 30% Stable angina 20% Unstable angina 20 26% 26% *CHD death only PAD 20 29%* 29%* CVA 14 20%* Diabetes 15 25%* 10-yr estimated risk >20%
27 Heart Protection Study Conclusions Patients at high risk for recurrent events benefit from treatment with simvastatin even with low baseline LDL levels Relative risk reduction remains relatively constant across LDL levels Absolute risk reduction depends on baseline risk rather than on baseline LDL alone
28 Case #2 CD is a 72 y/o female pt with known CHD who presents for a follow-up visit Current Meds: Pravastatin 80 mg po qd, Toprol XL 200 mg po qd, ASA 81 mg po qd, Lisinopril 20 mg po qd Lipid Profile LDL 104, HDL 44, TG 170? Changes in Rx
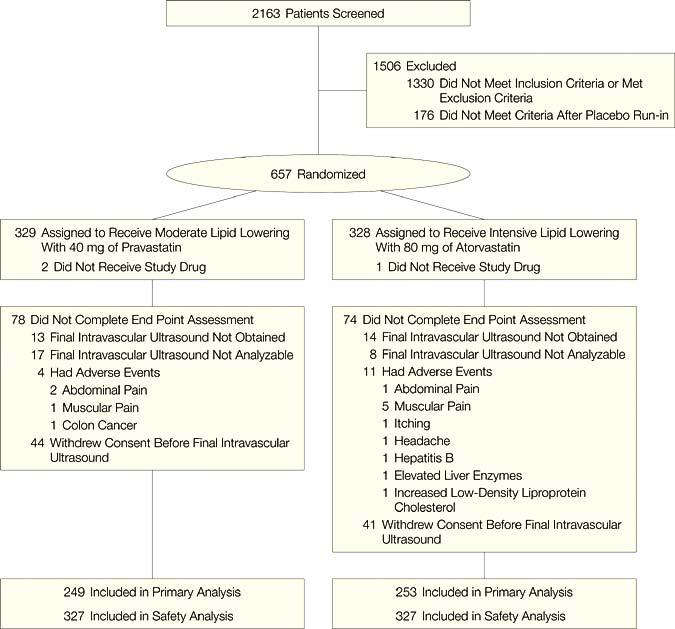
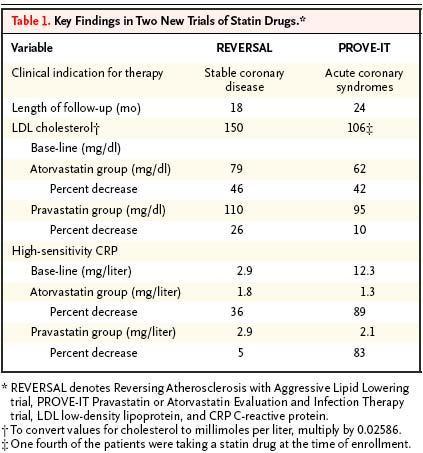
29 Reversal of Atherosclerosis with Aggressive Lipid Lowering ( REVERSAL) 654 patients with stable CHD randomized to Atorvastatin 80 mg/day vs. Pravastatin 40 mg po qd 18 month f/u Primary endpoint progression progression of atherosclerosis by endovascular ultrasound
30

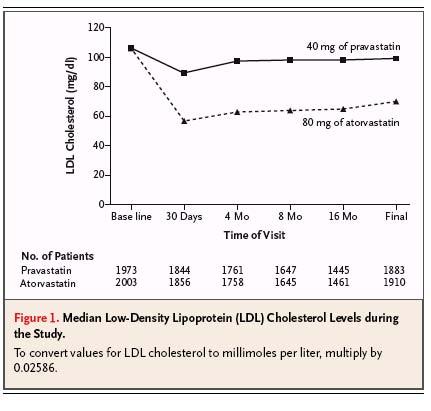
31 REVERSAL cholesterol results
32
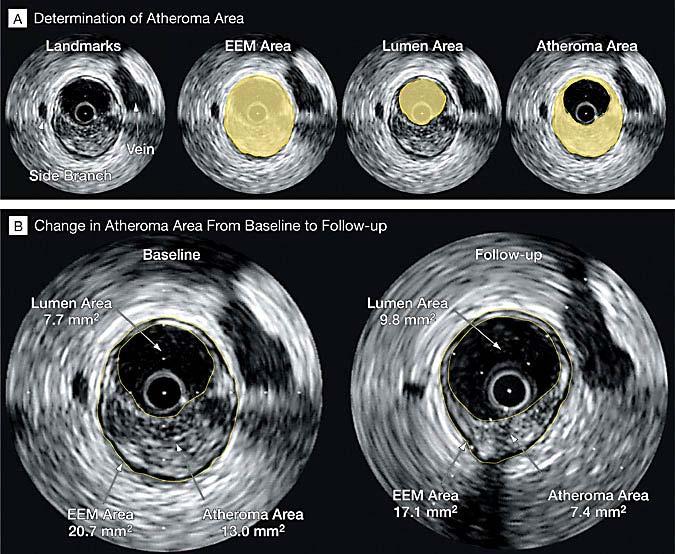
33 REVERSAL Results Atheroma volume increased 2.7% in the pravastatin group ( P=0.001) Atheroma volume remained unchanged in the atorvastatin group ( -0.4% decrease from baseline, p=0.98 NS)
34 REVERSAL Conclusions High dose atorvastatin was superior to medium dose pravastatin in preventing progression of atheroma high dose atorvastatin was well tolerated Benefit of high dose atorvastatin on clinical endpoints MI, death, recurrent angina, need for revascularization is not known
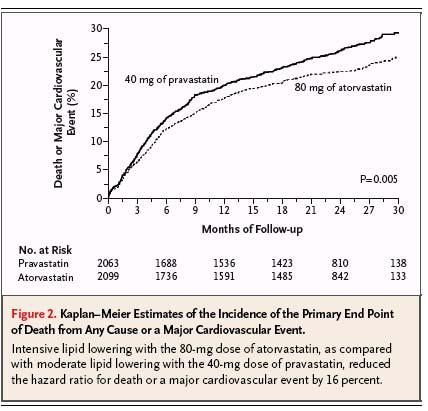
35 Pravastatin or Atorvastatin Evaluation and Infection Therapy ( PROVE-IT) Randomized controlled trial of Pravastatin 40 mg vs. Atorvastatin 80 mg in patients with an acute coronary syndromes ( STEMI, NSTEMI, Unstable Angina) month follow-up Primary endpoint: composite of death,mi, unstable angina, revascularization and stroke
36 PROVE-IT ( continued Eligibility: age>18, ACS within past 10 days PCI completed ( if planned) Cholesterol <240, or <200 if on statin Exclusion criteria: PCI in past 6 months planned CABG or CABG in past 2 months Liver disease or Cr >2.0
37 PROVE-IT Patient characteristics Age: 58 ( mean) Gender 78% men DM 18% HTN 50% Smoking 37% PCI 69% ( for index event)
38 PROVE IT patient characteristics ( Cont.) On statin therapy 25% Baseline LDL 106 mg/dl Interquartile range Baseline HDL 38 mg/dl
39 LDL levels on treatment (mg/dl) Pre Post Atorvastatin 80 mg Pravastatin 40 mg
40
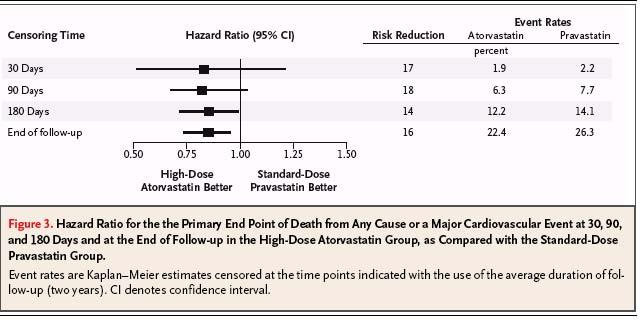
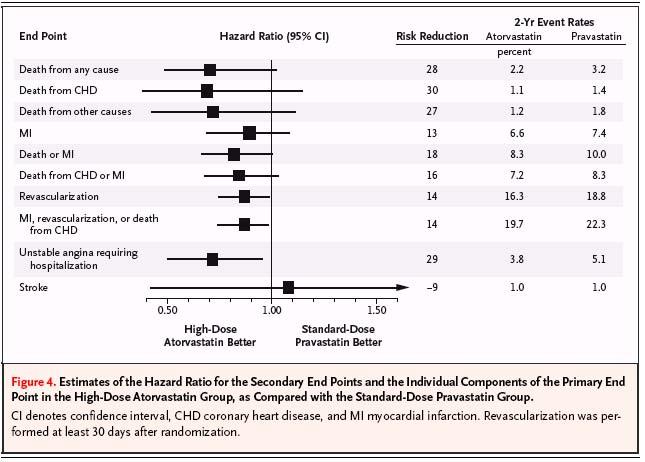
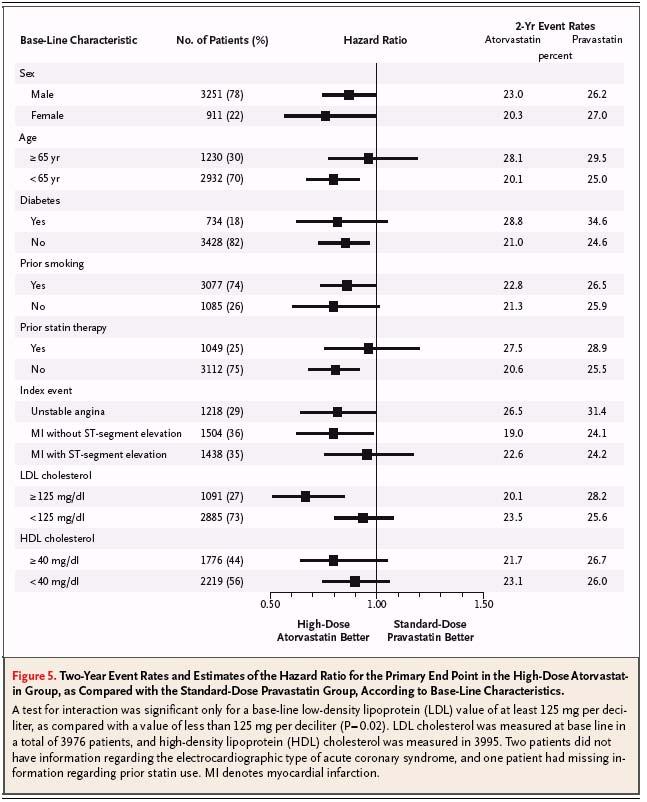
41 PROVE-IT Results 16 percent relative reduction in primary endpoint at 2 years ( death,mi, revascularization, or unstable angina) 26.3% in the pravastatin group vs. 22.4% in the atorvastatin group Revascularization ( 16.3% vs. 18.8%) and unstable angina ( 3.8% vs. 5.15%) were the only individual endpoints to achieve statistical significance
42
43
44
45
46 REVERSAL, PROVE IT Summary In patients with an ACS,, aggressive lipid lowering results in reduction in clinically important endpoints ( PROVE-IT) In patients with stable CHD, aggressive lipid lowering appears to halt progression of atheroma, but the effect on clinical endpoints is not known ( REVERSAL)
47 Ongoing Clinical Trials SEARCH Study Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine, 80 mg simvastatin vs. 20 mg simvastatin Report due ~ 2005 TNT Treating Treating to New Targets 10 mg atorvastatin vs. 80 mg atorvastatin
48 Case #3 54 y/o male pt s/p anterior MI in 1998, ex- smoker here for routine f/u visit Feels well, no angina, active, fit Meds: ASA, atenolol Lipid Profile HDL 28, LDL 95, TG 160 Treatment recommendations?
49 Isolated Low HDL 11% of US men have isolated low HDL 30% of men have an HDL <40 mg/dl Each 1% drop in HDL is associated with a 2-3% increase in CHD risk
50 Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial (VA-HIT) Double-blind study Gemfibrozil (600 mg BID) versus placebo 2,531 men with CHD, LDL-C 140 mg/dl dl,, and HDL-C 40 mg/dl Mean age: 64 y (76.5% aged > 60 y) Study duration: 7 y Median follow-up: 5.1 y Primary end point: nonfatal MI or coronary death Rubins HB et al. N Engl J Med 1999;341:
51 Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial (VA-HIT) Effects on Lipid Levels at 1 Year % change with gemfibrozil versus placebo No change LDL-C HDL-C TC TG Rubins HB et al. N Engl J Med 1999;341:

52 VA-HIT: Major Coronary Events in Gemfibrozil vs. Placebo Groups 25 Cumulative Incidence (%) % reduction P = Placebo Gemfibrozil Year Rubins HB et al. N Engl J Med 1999;341: Copyright 1999, Massachusetts Medical Society. All rights reserved.
53 Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial (VA-HIT) Effects of Fibrate on CVD Events in CHD Patients With Isolated Low HDL-C 0-5 Nonfatal MI/CHD death CHD All-cause death Stroke * mortality % decrease ** Placebo/Treated: 275/ /93 88/64 220/198 * Investigator-designated P = 0.006; ** P = 0.04 Rubins HB et al. N Engl J Med 1999;341:
54 HDL-Atherosclerosis Treatment Study ( HATS) RCT of 160 patients with baseline HDL<35, LDL <145 Simvastatin mg + Niacin 2-4 g vs. placebo Target LDL <90, HDL increase of > 5 mg/dl 3 year follow-up Endpoints-angiographic progression or MI, death, stroke, revascularization
55 HDL-Atherosclerosis Treatment Study (HATS) Niacin and Statin Outcome Trial Composite Event Rate, % % Reduction * *P<.05 vs. Placebo Placebo S + N AV S + N + AV Coronary Death, MI, Stroke, or Revascularization Brown BG et al. N Engl J Med 2001;345:
56 Comparison of Trials in Which Statin Therapy Ablated Coronary Risk Associated With Low HDL-C Coronary events (%) S LIPID CARE WOSCOPS AFCAPS/ TexCAPS Statin Placebo < 39 > 44 < < HDL-C (mg/dl) Adapted from Ballantyne CM et al. Circulation 1999;99:
57 Case #4 An inquisitive, well educated, 65 y/o recently retired patient s you after reading in the paper about hscrp. She is in excellent health, has no cardiac risk factors except her age, and has an LDL of 120, HDL 50, and normal triglycerides She wants to know if she should have her hscrp checked and whether she should be on a statin if it is elevated?
58 C-Reactive Protein Hepatically derived pentraxin five 23kDa subunits Marker and mediator of atherosclerosis Associated with increased risk for vascular events in numerous epidemiological studies Increases with infection, trauma, hospitalization
59

60

61 LDL and hscrp Relative Risk
62 HsCRP and Statin Treatment: AFCAPS Data Subgroup Event Rate % Statin Placebo Relative Risk Reduction% Number Needed to Treat (NNT) Chol/HDL<median CRP< median Chol/HDL<median CRP>median Chol/HDL>median CRP<median Chol/HDL>median CRP>median % % % % 62
63
64 AHA/CDC recommendations those patients at intermediate risk (e.g., 10% to 20% risk of coronary heart disease (CHD) over 10 years), in whom the physician may need additional information to guide considerations of further evaluation (e.g., imaging, exercise testing) or therapy (e.g., drug therapies with lipid-lowering, antiplatelet, or cardioprotective agents), may benefit from measurement of hs-crp.
65 JUPITER Trial recently recently started Justification for Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin 15,000 patients ( M>55, W>65) hscrp>2 mg/l, LDL < 130, TG<500 No CHD history or CHD risk equivalents Randomized to placebo vs. rosuvastatin 20 mg
66 Role of hscrp Testing Patients at high risk for recurrent events should be treated with a statin regardless of CRP level Primary prevention---consider treatment of patients with high CRP, normal LDL at intermediate risk (10-20%) for CHD
67 Monthly Costs of Common Statins at Drugstore.com Atorvastatin Simvastatin Pravastatin Lovastatin 10 mg $ mg $ mg $ mg $ mg $62.99 Rosuvastatin 5mg $69.99 Niacin 2gm $15
68 Cost- Effectiveness of Statins (per QALYs Gained) 10 yr CHD risk Annual Statin Cost $ $1000 $500 $250 $125 35% 25% 15% 10% 5% 10,
69 PROVE-IT Safety and tolerability Tolerability: : ~ 22% of patients discontinued treatment because of adverse events or patient preference or other reasons LFT abnormalities- - ALT > 3x normal in 1.1% pravastatin patients vs. 3.1 % in the atorvastatin group ( p <0.001) Myalgias or CK elevations: : 2.7 % pravastatin vs. 3.3 % atorvastatin
70 Summary Patients at high risk for CHD appear to benefit from statin therapy even with baseline LDL levels <100 The optimal target for lipid lowering is not yet known, but may be well less than 100 mg/dl in some patient populations Patients with low HDL benefit from treatment with gemfibrozil or simvastatin-niacin Biomarkers such as hscrp may play a key role in identifying candidates for lipid lowering, but definitive studies have not yet been performed
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Preventing Cardiovascular Disease With Lipid Management: Matching Therapy to Risk
 PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Disclosures. Objectives. Cardiovascular Risk. Patient Case. JUPITER: The final frontier in statin utilization or an idea from outer space?
 Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Medical evidence suggests that
 COMBINATION THERAPY TO ACHIEVE LIPID GOALS David G. Robertson, MD* ABSTRACT Coronary heart disease (CHD) remains the leading cause of death in the United States despite recent advances in treatment and
COMBINATION THERAPY TO ACHIEVE LIPID GOALS David G. Robertson, MD* ABSTRACT Coronary heart disease (CHD) remains the leading cause of death in the United States despite recent advances in treatment and
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipid Management: Beyond LDL
 Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
Lipid Management: Beyond LDL Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine University of Kentucky Overview Discuss the concept of residual risk Review current evidence-based medicine
The updated guidelines from the National
 BEYOND NCEP ATP III: LESSONS LEARNED AND FUTURE DIRECTIONS * Benjamin J. Ansell, MD, FACP ABSTRACT The National Cholesterol Education Program (NCEP) Third Adult Treatment Panel (ATP III) guidelines provide
BEYOND NCEP ATP III: LESSONS LEARNED AND FUTURE DIRECTIONS * Benjamin J. Ansell, MD, FACP ABSTRACT The National Cholesterol Education Program (NCEP) Third Adult Treatment Panel (ATP III) guidelines provide
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Coronary artery disease remains the leading
 UNMET NEEDS IN THE TREATMENT OF ATHEROSCLEROSIS: WHY ARE WE NOT DONE YET? * Evan A. Stein, MD, PhD ABSTRACT Heart disease remains the leading cause of death in the United States. Despite advances in surgical,
UNMET NEEDS IN THE TREATMENT OF ATHEROSCLEROSIS: WHY ARE WE NOT DONE YET? * Evan A. Stein, MD, PhD ABSTRACT Heart disease remains the leading cause of death in the United States. Despite advances in surgical,
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
The American Diabetes Association estimates
 DYSLIPIDEMIA, PREDIABETES, AND TYPE 2 DIABETES: CLINICAL IMPLICATIONS OF THE VA-HIT SUBANALYSIS Frank M. Sacks, MD* ABSTRACT The most serious and common complication in adults with diabetes is cardiovascular
DYSLIPIDEMIA, PREDIABETES, AND TYPE 2 DIABETES: CLINICAL IMPLICATIONS OF THE VA-HIT SUBANALYSIS Frank M. Sacks, MD* ABSTRACT The most serious and common complication in adults with diabetes is cardiovascular
RECOGNITION OF THE METABOLIC SYNDROME
 THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
THE METABOLIC SYNDROME IN CLINICAL PRACTICE Michael H. Davidson, MD* ABSTRACT Patients with the metabolic syndrome remain at significantly elevated risk of morbidity and mortality associated with coronary
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Supplementary Online Content
 Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
The Clinical Debates
 The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
The Metabolic Syndrome
 The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
LAMIS (Livalo in AMI Study)
") JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
JAMA. 2011;305(24): Nora A. Kalagi, MSc
: Nora A. Kalagi, MSc") JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
Tailored Statin Treatment for Type 2 Diabetes. Han, Ki Hoon Asan Medical Center University of Ulsan
 Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Drug Class Review on HMG-CoA Reductase Inhibitors (Statins)
") Drug Class Review on HMG-CoA Reductase Inhibitors () Final Report June 2004 Mark Helfand, MD, MPH Susan Carson, MPH Cathy Kelley, PharmD Oregon Evidence-based Practice Center Oregon Health & Science University
Drug Class Review on HMG-CoA Reductase Inhibitors () Final Report June 2004 Mark Helfand, MD, MPH Susan Carson, MPH Cathy Kelley, PharmD Oregon Evidence-based Practice Center Oregon Health & Science University
COURAGE to Leave Diseased Arteries Alone
 COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Calculating RR, ARR, NNT
 Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Low HDL and Diabetic Dyslipidemia
 The Lowdown: Low HDL and Diabetic Dyslipidemia Patients with diabetes commonly have a low-density lipoprotein cholesterol (LDL-C) no higher than that of the general population. What treatment is warranted
The Lowdown: Low HDL and Diabetic Dyslipidemia Patients with diabetes commonly have a low-density lipoprotein cholesterol (LDL-C) no higher than that of the general population. What treatment is warranted
Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
REAL-CAD. : Cardiovascular benefit of pitavastatin in stable coronary artery disease
 REAL-CAD : Cardiovascular benefit of pitavastatin in stable coronary artery disease Soo-Joong Kim M.D., PhD. Department of Cardiology, Internal Medicine, Kyung Hee University Hospital I have nothing to
REAL-CAD : Cardiovascular benefit of pitavastatin in stable coronary artery disease Soo-Joong Kim M.D., PhD. Department of Cardiology, Internal Medicine, Kyung Hee University Hospital I have nothing to
STATINS FOR PAD Long - term prognosis
 STATINS FOR PAD Long - term prognosis Prof. Pavel Poredos, MD, PhD Department of Vascular Disease University Medical Centre Ljubljana Slovenia DECLARATION OF CONFLICT OF INTEREST No conflict of interest
STATINS FOR PAD Long - term prognosis Prof. Pavel Poredos, MD, PhD Department of Vascular Disease University Medical Centre Ljubljana Slovenia DECLARATION OF CONFLICT OF INTEREST No conflict of interest
10/15/2012. Lessons Learned from Tim Russert: Investigating Residual Risk. Tim Russert: Residual CV Risk?
 Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
LIST OF ABBREVIATIONS
 Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Lipid Studies That Rocked My World Gabor Gyenes Medicine Grand Rounds May 27, 2011
 Lipid Studies That Rocked My World Gabor Gyenes Medicine Grand Rounds May 27, 2011 Disclosure of Conflicts of Interest I have received travel grants and honoraria from sanofi-aventis, Pfizer, Servier,
Lipid Studies That Rocked My World Gabor Gyenes Medicine Grand Rounds May 27, 2011 Disclosure of Conflicts of Interest I have received travel grants and honoraria from sanofi-aventis, Pfizer, Servier,
2/23/2018. Management of Hyperlipidemia Update on Guidelines and Novel Therapies. Burden of Heart Disease in U.S.
 Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Management of Hyperlipidemia Update on Guidelines and Novel Therapies SHARATH SUBRAMANIAN, MD, FACC February 24, 2018 Disclosures : None Burden of Heart Disease in U.S. https://www.cdc.gov/nchs/images/databriefs/251
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical