IBS. Dan Carter, M.D. Institute of Gastroenterology Sheba medical center
|
|
|
- Maud Carroll
- 5 years ago
- Views:
Transcription
1 IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center
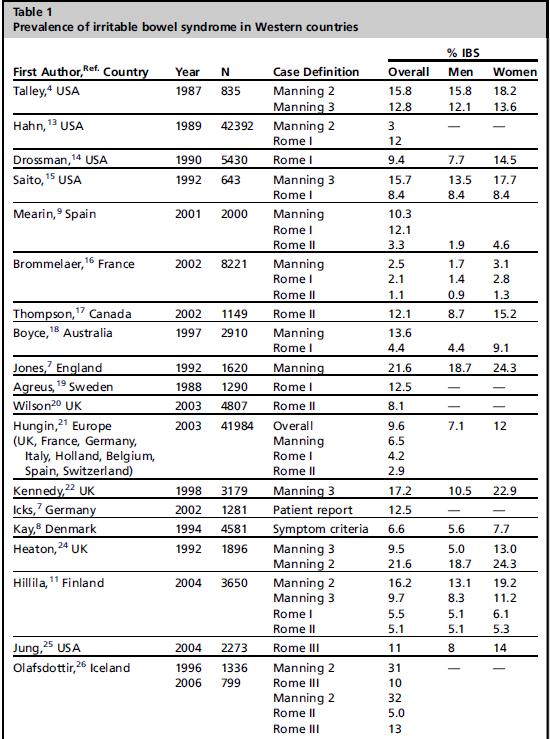
2 Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort and diarrhea or constipation, or both. The definition of IBS has evolved over time, from a diagnosis of exclusion to the symptom-based diagnostic criteria including Manning, Rome I, Rome II, and Rome III criteria.
3 Epidemiology IBS accounts for 10% to 15% of primary care visits 25% to 50% of gastroenterology referral visits Only limited proportion of subjects suffering from IBS seek medical attention for this condition. Prevalence rates in various studies have varied between 3 and 32 per 100.
4 Epidemiology
5 Epidemiology The incidence rate : cases per 100,000 person-years in study on American population to 300 per 100,000 people in a study from Europe. If only half seek care, the observed incidence can be doubled to 400 per 100,000 per year and then multiplied by a 20-year disease duration to get a prevalence of 12%.
6 Demographic predictors of IBS The odds of having IBS are higher in women. More prevalent in younger patients. More prevalent in lower socioeconomic groups.
7 Resource use in IBS Burden of illness studies estimate that there are 3.6 million physician visits in the United States annually for IBS IBS care consumes over $20 billion in both direct and indirect expenditures. Patients with IBS consume over 50% more health care resources than matched controls without IBS.
8 Resource use in IBS Much of the cost of care in IBS arises from sequential and redundant diagnostic tests, invasive procedures, and abdominal operations. patients with IBS are three times more likely than matched controls to undergo cholecystectomy Nearly 25% of colonoscopies performed in patients younger than 50 years of age are for IBS symptoms
9 Resource use in IBS Employees with IBS are absent 3% to 5% of the work-week, and report impaired productivity 26% to 31% of the week, rates that exceed those of non-ibs control employees by 20%. Patients with impaired productivity have more extraintestinal comorbidities : chronic fatigue syndrome, fibromyalgia, interstitial cystitis, and more disease-specific fears and concerns.
10 Quality of life IBS patients have the same physical HRQOL as patients with diabetes, and a lower physical HRQOL compared with patients who have depression or gastroesophageal reflux disease. The health utility of severe IBS is similar to that of Class 3 congestive heart failure and rheumatoid arthritis.
11 Quality of life This HRQOL decrement can be severe enough to raise the risk of suicidal behavior is some cases. Data from several studies indicate that in patients with IBS, HRQOL decreases in parallel with increasing symptom severity.
12 Overlap with Other Functional Gastrointestinal Disorders Many population-based and clinical studies have reported the associations with other diseases, specifically other FGIDs. GERD and symptomatic bronchial hyperresponsiveness occurred more frequently together with IBS than expected.
13 Overlap with Extra intestinal Disorders IBS patients make 2 or 3 times as many non- GI health care visits as control subjects. Non-GI nonpsychiatric disorders documented to be associated with IBS include: - chronic fatigue syndrome (51%) - chronic pelvic pain (50%) - temporomandibular joint disorders (64%(
14 Overlap with Extra intestinal Disorders In referred patients with IBS, psychiatric disorders have also been reported to be very common: especially major depression, anxiety, and somatoform disorders.

15 Natural history of IBS IBS is considered a chronic stable disorder that may wax and wane for years. Substantial symptom fluctuation among the GI symptom complexes with increasing prevalence over time. IBS is not associated with any increase in mortality.
16 Pathophysiology Multifactorial and varies from patient to patient. Disturbances of motor function in the small intestine and colon and smooth-muscle dysfunction in other gut and extraintestinal regions. Abnormalities of sensory function in visceral and somatic structures, which may relate to peripheral sensitization or altered central nervous system processing of afferent information.
17 Pathophysiology
18 Motor dysfunction
19 Altered visceral sensory activity Alterations in visceral and somatic perception are prevalent in IBS but have uncertain roles in inducing the different symptoms of this disorder. Some patients with IBS experience normal physiologic events, not normally perceived by healthy individuals, as being uncomfortable or painful
20 Pathophysiology
21 Brain-gut interactions Results from PET and fmri investigations taken suggest that patients with IBS show significant disruptions of CNS activity related to attention, arousal, emotional, and autonomic responses to gut stimulation. CNS imaging studies have shown alterations in brain structure in IBS Evoked potential recordings in functional dyspepsia and IBS show shorter waveform latencies and increased waveform amplitudes, consistent with defects in visceral afferent pathways.
22 Psychosocial distress Numerous studies confirm a high degree of psychosocial dysfunction in IBS. Psychiatric disturbances can be shown in most patients with IBS in tertiary practice, but also in patients managed in primary care and in individuals with IBS who do not seek care. Rates of suicidal behavior are increased 2- to 4-fold in IBS.
23 Psychosocial distress Exposure to wartime early in life increased the risk of developing IBS in another investigation. Increases in patients with IBS compared with healthy controls have been reported for: major depression phobias somatization disorder hypochondriasis generalized anxiety disorder hostility panic disorder concealed aggression neuroticism suppressed anger PTSD
24 Role of Stress Psychiatric disturbances usually predate or occur concurrently with the onset of bowel symptoms, indicating that emotional illness is not a consequence of IBS. IBS shows a strong association with reports of psychological stress. Previous stressful life events, such as loss of a parent, marital difficulties, maladaptive family interactions, and career changes, are more common in patients with IBS than in healthy individuals or patients with organic disease
25 Psychosocial distress Sleep disturbances are reported by most patients with IBS. IBS has been associated with histories of sexual and/or physical abuse including verbal aggression, exhibitionism, sexual harassment, sexual touching, and rape
26 The Role of Genetics in IBS
27 The Role of Genetics in IBS
28 Summary of positive gene associations, by IBS type and subtype
29 Food and IBS
30 Food and IBS Patients associate their symptoms with the ingestion of certain foods, combinations of foods, or a meal itself. More than 60% of IBS patients report worsening of symptoms after meals, 28% of these within 15 minutes after eating and 93% within 3 hours. Many patients identify specific trigger foods :most commonly dairy, fructose, wheat products, and caffeine. There is little evidence that IBS patients with foodrelated complaints are suffering from a true FA
31 Elimination diets Response rates to exclusion diets have ranged from 15% to 71%. Dairy products, wheat, and eggs the most commonly implicated food items.
32 Inflammation and Microflora The human intestinal tract is composed of more than 500 different species of bacteria. By adulthood most humans reach an established balance of type and numbers of bacteria that is unique to a given individual. There is growing evidence that supportes a new hypothesis for IBS based on alterations in intestinal bacterial composition.
33 Inflammation and Microflora Gut microbes interact with the gut mucosal immune system through innate and adaptive mechanisms. Altered flora can lead to changes in the intestinal epithelial barrier. Neuroimmune and pain modulation pathways may be influenced by the flora. Changing flora can increase food fermentation and subsequent intestinal gas production. Bile acid malabsorption can result from expansion of gut flora into the small bowel
34 Inflammation and Microflora Culture studies have consistently demonstrated a paucity of Lactobacillus and Bifidobacterium. Balb/c mice infected with a probiotic L acidophilus strain had elevated expression of several intestinal pain receptors that led to decreased visceral sensitivity.
35 Postinfectious IBS Numerous studies have shown that IBS can be precipitated by an episode of acute gastroenteritis. 10% of subjects who have AGE develop IBS, with a summary odds ratio of 6 to 7. The 2 most significant of these are duration/severity of gastroenteritis and female sex.
36 Antibiotic Treatment of IBS: Support for a Gut Flora Hypothesis TARGET 1 and TARGET 2: In these studies, rifaximin was effective in improving IBS based on abdominal pain, stool consistency, bloating, and the primary outcome measure of global relief.
37 Probiotics in IBS It seems reasonable that probiotics should restore a healthy gut microbiota and alleviate IBS symptoms. Unfortunately, the numerous controlled trials of probiotics in IBS have shown mixed results. The data are strongest for Bifidobacterium and Lactobacillus strains.
38 Diagnosing IBS
39 Symptom-Based Diagnostic Criteria for Irritable Bowel Syndrome
40 Diagnosing IBS Most patients who fulfill Rome III suffer with IBS. Because the condition is so common, there are likely many patients who do not fulfill symptom-based criteria but end up with a diagnosis of IBS.
41 Diagnosing IBS The most recent guidelines encourage clinicians to make a positive diagnosis of IBS based on a thorough history, using symptombased criteria and considering the presence or absence of specific alarm features. In the absence of alarm features, routine use of diagnostic imaging studies, blood tests, or stool studies are not advised.

42 Alarming clinical or historical features
43 Diagnosing IBS
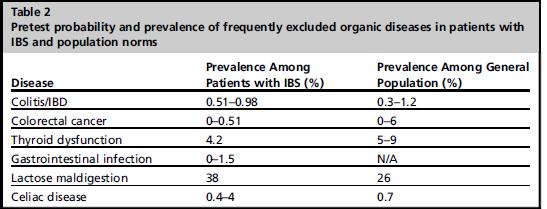
44 Routine Blood Tests CBC, CMP, TFT, ESR and CRP are often ordered on initial evaluation of patients with suspected IBS. In patients in tertiary centers, the likelihood of identifying organic disease with routine laboratory tests seems to be no greater in patients with IBS (and absent alarm features) than in the general population.
45 Testing for Celiac Disease The prevalence of celiac disease in individuals with suspected IBS was computed to be 4 times greater than in non-ibs controls. The ACG IBS Task Force recommended testing for celiac disease in patients presenting with nonconstipated IBS symptoms. The tests include EMA or TTG levels.
46 Colonoscopy Recommendations of the ACG IBS Task Force are to perform colonoscopy in patients with IBS older than 50 years and those with alarm features. When colonoscopy is performed in patients with suspected IBS-D random mucosal biopsies Should be preformed to rule out microscopic colitis.
47 Breath Testing SIBO or Carbohydrate Maldigestion Bloating is one of the most common symptoms associated with IBS, occurring in more than 75% of patients. Known symptom improvement from antibiotic and probiotic therapy. Association of IBS-like symptoms with lactose or fructose ingestion. Whether or not a correlation exists between IBS and SIBO remains controversial.
48 Breath Testing SIBO or Carbohydrate Maldigestion The ACG Task Force indicated that there is insufficient evidence to support the routine use of breath tests for SIBO. In patients reporting food-related symptoms, trials of lactose- or fructose-restricted diets are a rational and pragmatic therapeutic approach.
49 Stool Studies The ACG IBS Task Force does not recommend the routine use of stool studies to evaluate for infectious causes of IBS symptoms in the absence of a relevant travel history or specific alarm features (severe uncontrollable diarrhea, hematochezia, weight loss).
50 Stool Studies Several neutrophil-derived proteins excreted in the feces, such as lactoferrin and calprotectin, are highly sensitive and specific markers of inflammatory activity in the gut. Because of the high negative predictive value of these tests in ruling out intestinal inflammation, clinicians use them as a noninvasive screen for IBD in their patients with typical IBS symptoms.
51 Treatment
52 Gluten Restriction

53 FODMAP Restriction Fermentable Oligo-, Di-, and Monosaccharides And Polyols diet. Family of poorly absorbed, short-chain carbohydrates, which are highly fermentable in the presence of gut bacteria.
54 FODMAP Restriction The low FODMAP diet differs from most other elimination diets in that no initial attempts are made to identify specific culprit foods. In persons who respond to the full elimination phase, specific FODMAP food groups are sequentially reintroduced, allowing determination of the particular foods that the patient cannot tolerate.
55 Peripherally Acting Therapies for the Treatment of Irritable Bowel Syndrome Most of these peripheral acting agents are primarily targeted at individual symptoms. The evidence supporting the use of these agents in IBS is largely anecdotal. Serotonergic agents and the chloride channel activator lubiprostone have shown efficacy in treating symptoms of IBS.
56 Fiber supplements and laxatives Dietary fiber supplements represent a heterogeneous group of complex carbohydrates that are resistant to hydrolysis during digestion. These non-digested products result in increased stool bulk and water content, effectively decreasing stool consistency and increasing stool frequency.
57 Fiber supplements The results of the 6 trials comparing psyllium and ispaghula with placebo were pooled, yielding a total of 321 patients with IBS, with 161 in the treatment arm. 52% of patients treated with psyllium had persistent IBS symptoms after treatment compared with 64% of those receiving placebo RR of symptoms not improving with psyllium was 0.78 compared with placebo with a NNT of 6.
58 Laxatives The use of laxatives in the treatment of IBS-C has evolved from their known effect on the symptoms of constipation. Only polyethylene glycol PEG has been assessed in the treatment of IBS. laxatives were shown to improve stool frequency but not abdominal pain in one small sequential study in adolescents with IBS- C.( PEG).
59 Antidiarrheals Studies have reported accelerated small bowel and colon transit times as well as exaggerated motility patterns in those with IBS-D. Only loperamide has been evaluated in RCTs for the treatment of IBS.
60 Antidiarrheals The antidiarrheal agent loperamide is not more effective than placebo at reducing abdominal pain or global symptoms of IBS, but is an effective agent for treatment of diarrhea, improving stool frequency and stool consistency. RCTs with other antidiarrheal agents have not been performed. Safety and tolerability data on loperamide are lacking.
61 Antispasmodics Abdominal pain or discomfort is a cardinal feature of IBS. Observation and clinical studies have suggested that an exaggerated motility response of the small bowel and colon to environmental stimuli may be responsible for the symptoms experienced in IBS. For this reason antispasmodics have been and remain a mainstay of therapy for the symptoms of IBS.
62 Antispasmodics These agents are directed at those subgroups of IBS, with a predominant symptom of abdominal pain and stool patterns that are either mixed or more diarrheal in nature. The anticholinergic properties of these agents restrict their usefulness in clinical practice.
63 Antispasmodics ACG Task Force Certain antispasmodics (hyoscine, cimetropium, and pinaverium) may provide short-term relief of abdominal pain/discomfort in IBS. Evidence for long-term efficacy is not available. Evidence for safety and tolerability are limited.
64 Antispasmodics These agents are likely to be most effective in those patients with IBS with a predominant symptom of abdominal pain. These agents can worsen constipation and should therefore be used cautiously in patients with IBS with a predominance of constipation.
65 Serotonergic agents Serotonin (5-HT) is the neurotransmitter primarily produced and stored in enterochromaffin cells located throughout the intestinal epithelium. 95% of total body concentration of 5-HT resides in the gastrointestinal tract. Acting through the intrinsic and extrinsic afferent nervous system of the GIT, 5-HT plays an important role in various aspects of gastrointestinal sensory, secretory, absorptive, and motility function.
66 Serotonergic agents Receptor agonists of 5-HT 1 : improve gastric accommodation slow gastric emptying stimulate activity of the MMC Receptor antagonists of 5-HT 3 : slow small bowel transit decrease intestinal secretion decrease colonic tone and transit.
67 Serotonergic agents Agonists of the 5-HT 4 receptor: accelerate gastric emptying improve gastric accommodation accelerate small bowel transit accelerate colonic transit decrease visceral sensation No 5-HT 1 or 5-HT 4 receptor agents are approved for the treatment of IBS in the United States or Canada
68 Serotonergic agents Alosetron is more effective than placebo at relieving global IBS in male and female patients with IBS with diarrhea. Potentially serious side effects include constipation and colonic ischemia. The benefits and harms balance for alosetron is most favorable in women with IBS-D who have not responded to conventional therapies.
69 Chloride channel activator Lubiprostone is the only chloride channel activator with FDA approval for the management of IBS-C. Lubiprostone in a dose of 8μg twice daily is more effective than placebo in relieving global IBS symptoms in women with IBC-S Lubiprostone is contraindicated in patients with mechanical bowel obstruction and should be avoided in patients with preexisting diarrhea.
70 Centrally Acting Therapies for Irritable Bowel Syndrome The use of psychotropic agents for FGIDs has grown significantly in the past 2 decades. Every 1 in 8 patients with IBS is offered an antidepressant. A recent meta-analysis showed significantly decreased relative risk of persistent IBS symptoms with antidepressant treatment. On average, 3 to 4 patients needed to be treated with an antidepressant to improve 1 patient s symptom.

71 Centrally Acting Therapies
72 Psychotropic agents Four major classes of psychotropic agents of interest in IBS are : tricyclic antidepressants selective serotonin reuptake inhibitors serotonin-norepinephrine reuptake inhibitors atypical antipsychotics. TCAs and SSRIs have been most widely studied. SNRIs are gaining popularity for treatment for other chronic pain conditions such as fibromyalgia and are likely to be further explored in IBS and other FGIDs.
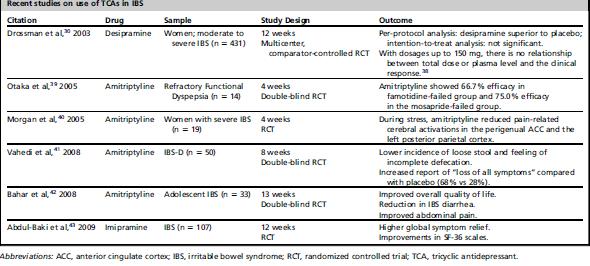
73 Tricyclic Antidepressants

74 Selective Serotonin Reuptake Inhibitors
75 Selective Serotonin Reuptake Inhibitors SSRI s improve global well-being and some GIspecific symptoms. SSRI s have anxiolytic properties and can target social phobia, agoraphobia, and symptom-related anxiety. may augment the analgesic effects of other agents (TCAs); Treat psychiatric comorbidities. Diarrhea may be a side effect, and SSRIs may benefit patients with constipation.
76 Serotonin-Norepinephrine Reuptake Inhibitors The SNRI s may potentially be as effective as the TCAs, owing to their dual blockade of reuptake of NE and 5HT receptors. Duloxetine is the only SNRI agent that has been studied for the treatment of IBS. Duloxetine (60 mg daily dosage) appeared to be effective for pain, severity of illness, quality of life, loose stool, work and family disability, and anxiety.
77 Atypical Antipsychotics Are beneficial in lower dosages for patients with FGIDs because of their analgesic properties (alone or in synergism with antidepressants) and their sedative and anxiolytic effects.

78 Centrally Acting Therapies
79 Behavioral therapies
80 Behavioral therapies Establish a rational model of illness: reframe maladaptive beliefs. Reduce overresponsiveness to stress, eg, stress and autonomic reactivity. Reduce or modify maladaptive psychological responses: catastrophizing, symptom-specific anxiety, shame/guilt. Reduce or modify maladaptive behaviors, eg, agoraphobia, seeking diagnostic studies.
81 Behavioral therapies CBT has a direct effect on global IBS symptom improvement, independent of its effects on distress. Symptom benefit with CBT may be mediated through changes in neural activity of corticallimbic regions that subserve hypervigilance and emotion regulation.
82 Relaxation Training Relaxation techniques are to train patients to counteract physiologic squeal of stress or anxiety. Five recent studies have assessed efficacy of relaxation therapy in IBS. Relaxation alone or in combination with CBT and other therapies can be beneficial for IBS symptoms.
83 Hypnotherapy Hypnotherapy has been shown to be effective for the treatment of IBS and a recent review concluded that hypnosis has a favorable impact on refractory IBS symptoms. The mechanism is unclear, although there is some evidence that it reduces gut contractility and normalizes pain thresholds after balloon rectal distension.
84 Complementary and Alternative Medicine for the Irritable Bowel Syndrome CAMs are commonly used by patients with IBS, particularly acupuncture and herbal medicines. Well-controlled clinical trials are lacking to support CAM use in IBS. Nevertheless, several treatments, particularly some probiotics and herbs (eg, peppermint oil), suggest that they may have a benefit in IBS.
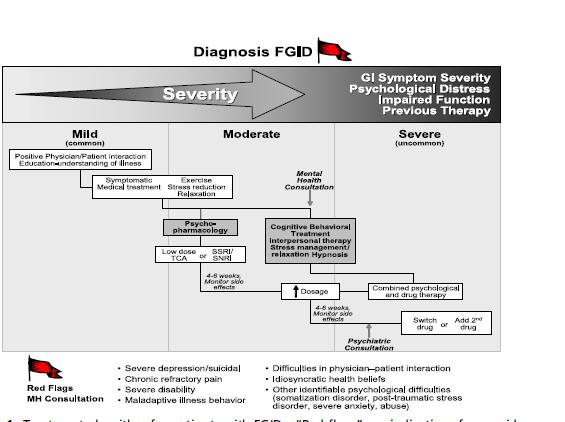
85 Treatment
Irritable Bowel Syndrome Now. George M. Logan, MD Friday, May 5, :35 4:05 PM
 Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Advancing gastroenterology, improving patient care
 American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
Is one of the most common chronic disorders. causing patients to seek medical treatment.
 ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
IBS Irritable Bowel syndrome Therapeutics II PHCL 430
 Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Presenter. Irritable Bowel Syndrome. Objectives. Introduction. Rome Criteria. Irritable Bowel Syndrome 2/28/2018
 Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
4) Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis
 Irritable Bowel Syndrome - Dr. Shaikhani. Epidemiology. Pathophysiology. Burden. Diagnosis") 4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
4) Irritable Bowel Syndrome - Dr. Shaikhani Epidemiology A common disorder, with a 7% prevalence. Women are 1.5 times more likely to be affected than men, most commonly between ages 20-40 years. Onset
IBS - Definition. Chronic functional disorder of GI generally characterized by:
 IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
Primary Management of Irritable Bowel Syndrome
 Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
 Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
Irritable Bowel Syndrome. Mustafa Giaffer March 2017
 Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence
 Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
IBS and Functional GI Disorders (FGIDs)
") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary
 Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Chronic Abdominal Pain. Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016
 Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
MANAGEMENT OF VISCERAL PAIN
 MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
IRRITABLE BOWEL SYNDROME
 DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 IRRITABLE BOWEL SYNDROME DEFINITION: *FUNCTIONAL GASTROINTESTINAL DISORDER CHARACTERIZED
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (403) 270-7479 IRRITABLE BOWEL SYNDROME DEFINITION: *FUNCTIONAL GASTROINTESTINAL DISORDER CHARACTERIZED
What is Irritable Bowel Syndrome (IBS)?
?") What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
Irritable Bowel Syndrome. Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016
 Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
Irritable Bowel Syndrome Paul Sheykhzadeh, DO, FACG Digestive Health Associates Reno, NV NAPNA Symposium March 5, 2016 Definition of Irritable Bowel Syndrome (IBS) Rome III Criteria Recurrent abdominal
IBS-D: The Role of Pathophysiology in Assessment and Treatment ReachMD Page 1 of 7
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Functional Dyspepsia
 Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
ROME IV CRITERIA FOR IBS
 PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
David Leff, DO. April 13, Disclosure. I have the following financial relationships to disclosure:
 David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
David Leff, DO AOMA 94 th Annual Convention April 13, 2016 Disclosure I have the following financial relationships to disclosure: Speaker s Bureau: Allergan Labs, Takeda Pharmaceutical, Valeant Pharmaceutical
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Bloating, Flatulence, and
 A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
A 45-Year-Old Man With Recurrent Abdominal Pain, Bloating, Flatulence, and Intermittent Loose Stools Anthony J. Lembo, MD Associate Professor of Medicine Harvard Medical School Director, GI Motility Laboratory
Irritable Bowel Disease. Dr. Alexandra Ilnyckyj MD
 Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
Irritable Bowel Disease Dr. Alexandra Ilnyckyj MD Exactly what is IBS? Common condition affecting mostly women Symptoms are variable but they reflect altered gut movement (motility) and sensation Commonly
... SELECTED ABSTRACTS...
 ... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
William D. Chey, MD Professor of Medicine University of Michigan
 Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
Management of Functional Bowel Disorders
 Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
Management of Functional Bowel Disorders Amy Foxx-Orenstein, DO, FACG, FACP Professor of Medicine Mayo Clinic Tucson Osteopathic Medical Foundation May 1, 2016 Objectives Review epidemiology and pathophysiology
Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome
 Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School What is the general
Current and Emerging Pharmacological Treatments in Irritable Bowel Syndrome Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School What is the general
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
Irritable Bowel Syndrome Irritable bowel syndrome (IBS) has a variety of symptoms, most commonly cramping, abdominal pain, bloating, constipation, and diarrhea. Symptoms can vary from person to person,
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Lower Gastrointestinal Tract KNH 406
 Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
Lower Gastrointestinal Tract KNH 406 Lower GI Tract A&P Small Intestine Anatomy Duodenum, jejunum, ileum Maximum surface area for digestion and absorption Specialized enterocytes from stem cells of crypts
IBS-D: What to Do When Typical Treatment Methods Fail
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Evolving Therapy in Irritable Bowel Syndrome (IBS)
") Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
Evolving Therapy in Irritable Bowel Syndrome (IBS) Dr. Syed Mohammad Arif MBBS, FCPS (Medicine), MD (Gastro) Associate Professor Department of Medicine Dhaka Medical College A good set of bowels is worth
Irritable Bowel Syndrome (IBS)
") Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Irritable Bowel Syndrome (IBS) Dr Rex J Polson 17 th January 2018 Overview Description of the condition Discussion of symptoms and investigations that may be required Discussion of management and treatment
Irritable bowel syndrome in adults
 Irritable bowel syndrome in adults NICE provided the content for this booklet which is independent of any company or product advertised Welcome In February 2008, NICE published a clinical guideline on
Irritable bowel syndrome in adults NICE provided the content for this booklet which is independent of any company or product advertised Welcome In February 2008, NICE published a clinical guideline on
At the outset, we want to clear up some terminology issues. IBS is COPYRIGHTED MATERIAL. What Is IBS?
 1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
Objectives. Pain Types Brief Review. Referred Pain. Chronic/Recurrent Abdominal Pain 1/12/2017. I have no conflicts of interest to disclose
 Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
IRRITABLE BOWEL SYNDROME
 IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
IRRITABLE BOWEL SYNDROME CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Here are some questions to ask your doctor. WHAT IS IRRITABLE BOWEL SYNDROME? 4
The Role of Food in the Functional Gastrointestinal Disorders
 The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
Low FODMAP Dietary Approach For FGD/IBS. Our Experience. Charlotte McCamphill 19 th February 2015
 Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Microbiome GI Disorders
 Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Functional gastrointestinal disorders Definition A variable combination of chronic or recurrent gastrointestinal symptoms (attributed to the pharynx, esophagus, stomach, biliary
Irritable Bowel Syndrome Functional gastrointestinal disorders Definition A variable combination of chronic or recurrent gastrointestinal symptoms (attributed to the pharynx, esophagus, stomach, biliary
Functional Nutrition Approaches to Gut Health 20 CPEU Module accredited by Nutrition Mission
 Topics Covered 1. Good Health Starts in the Gut 2. Microbiome Part 1 3. Microbiome Part 2 4. What Can Go Wrong 5. FODMAP Intolerance 6. GERD 7. Celiac Disease 8. Non-Celiac Gluten Sensitivity 9. Intestinal
Topics Covered 1. Good Health Starts in the Gut 2. Microbiome Part 1 3. Microbiome Part 2 4. What Can Go Wrong 5. FODMAP Intolerance 6. GERD 7. Celiac Disease 8. Non-Celiac Gluten Sensitivity 9. Intestinal
Nicholas J. Talley, MD University of Newcastle Callaghan, NSW Australia. Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA
 Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Nicholas J. Talley, MD University of Newcastle Callaghan, NSW Australia
Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Nicholas J. Talley, MD University of Newcastle Callaghan, NSW Australia
Dr. Melvyn Letier Constantiaberg Mediclinic October 2016
 Dr. Melvyn Letier Constantiaberg Mediclinic October 2016 This presentation will enable you to: Understand the pathophysiology of IBS Recognize the clinical manifestations of IBS Make a confident diagnosis
Dr. Melvyn Letier Constantiaberg Mediclinic October 2016 This presentation will enable you to: Understand the pathophysiology of IBS Recognize the clinical manifestations of IBS Make a confident diagnosis
with DIARRHEA (IBS-D)
") Understanding IRRITABLE BOWEL SYNDROME with DIARRHEA (IBS-D) What is Irritable Bowel Syndrome with Diarrhea (IBS-D)? Irritable Bowel Syndrome (IBS) is a common chronic gastrointestinal disorder that involves
Understanding IRRITABLE BOWEL SYNDROME with DIARRHEA (IBS-D) What is Irritable Bowel Syndrome with Diarrhea (IBS-D)? Irritable Bowel Syndrome (IBS) is a common chronic gastrointestinal disorder that involves
Disclosures. Objectives. Pre-Test Question 1. Pre-Test Question 2. Pre-Test Question 3 9/23/2016
 Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
Disclosures Beating the Bowel Blues: An Update on the Treatment of Irritable Bowel Syndrome Matthew Nelson, PharmDBCPS, Roosevelt University College of Pharmacy Matthew Nelson declares no conflicts of
Irritable Bowel Syndrome (IBS) Information Leaflet THE DIGESTIVE SYSTEM
 Information Leaflet THE DIGESTIVE SYSTEM") THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Irritable Bowel Syndrome (IBS) Irritable Bowel Syndrome (IBS) consists of a number of symptoms. The most
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Irritable Bowel Syndrome (IBS) Irritable Bowel Syndrome (IBS) consists of a number of symptoms. The most
Level 2. Non Responsive Celiac Disease KEY POINTS:
 Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
Level 2 Non Responsive Celiac Disease KEY POINTS: Celiac Disease (CD) is an autoimmune condition triggered by ingestion of gluten leading to intestinal damage and a variety of clinical manifestations.
Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61
 Irritable bowel syndrome in adults: diagnosis and management Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Irritable bowel syndrome in adults: diagnosis and management Clinical guideline Published: 23 February 2008 nice.org.uk/guidance/cg61 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Psycho-pharmacologic Therapy. Objectives
 Psycho-pharmacologic Therapy for Functional Bowel Disorders John J. Hutchings, M.D. Assistant Professor of Medicine and Psychiatry Louisiana i State t University it School of Medicine i Department of Medicine
Psycho-pharmacologic Therapy for Functional Bowel Disorders John J. Hutchings, M.D. Assistant Professor of Medicine and Psychiatry Louisiana i State t University it School of Medicine i Department of Medicine
The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome
 n The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome Information for patients Irritable bowel syndrome (IBS) is a common, long term condition of the digestive system (gut). It causes episodes
n The Leeds Teaching Hospitals NHS Trust Irritable Bowel Syndrome Information for patients Irritable bowel syndrome (IBS) is a common, long term condition of the digestive system (gut). It causes episodes
ROLE OF THE GUT BACTERIA
 ROLE OF THE GUT BACTERIA Our Good Bacteria In a perfect world, we would all have a proper ratio of good bacteria And what could this proper ratio do for us? The knowledge of the connections between our
ROLE OF THE GUT BACTERIA Our Good Bacteria In a perfect world, we would all have a proper ratio of good bacteria And what could this proper ratio do for us? The knowledge of the connections between our
DOWNLOAD OR READ : IRRITABLE BOWEL SYNDROME ONE DISEASE SEVERAL OR NONE PERSPECTIVES IN DIGESTIVE DISEASES VOL 5 PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : IRRITABLE BOWEL SYNDROME ONE DISEASE SEVERAL OR NONE PERSPECTIVES IN DIGESTIVE DISEASES VOL 5 PDF EBOOK EPUB MOBI Page 1 Page 2 irritable bowel syndrome one disease several or none perspectives
DOWNLOAD OR READ : IRRITABLE BOWEL SYNDROME ONE DISEASE SEVERAL OR NONE PERSPECTIVES IN DIGESTIVE DISEASES VOL 5 PDF EBOOK EPUB MOBI Page 1 Page 2 irritable bowel syndrome one disease several or none perspectives
Irritable bowel syndrome (IBS) is a chronic, potentially disabling
 is a chronic, potentially disabling") Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
Diagnosis and Treatment of Irritable Bowel Syndrome
 Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
Special Issue Diagnosis and Treatment of Irritable Bowel Syndrome Myung Gyu Choi, M.D. Department of Internal Medicine The Catholic University of Korea, College of Medicine Kangnam St. Mary's Hospital
Inflammatory or Irritable? (the bowel, not the speaker)
") South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
South GP CME Edgar Centre, Dunedin August 2014 Inflammatory or Irritable? (the bowel, not the speaker) Dr Jason Hill MBChB FRACP FRCP Edin Department of Gastroenterology, Southern DHB Dunedin School Of
Irritable Bowel Syndrome
 68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
68 TH ANNUAL MCGILL REFRESHER COURSE FOR FAMILY PHYSICIANS 2017 Irritable Bowel Syndrome Gad Friedman, MDCM, FRCPC Jewish General Hospital DISCLOSURES I have no disclosures LEARNING OBJECTIVES 1. Review
Elderly Man With Chronic Constipation
 Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
Elderly Man With Chronic Constipation Linda Nguyen, MD Director, Neurogastroenterology and Motility Clinical Assistant Professor Stanford University Overview Normal bowel function Defining Constipation:
Dietitian Connection Webinar: Dietary management of IBS the low FODMAP diet & other adjunct therapies. Presented by Shirley Webber and Dr Jane Varney
 Dietitian Connection Webinar: Dietary management of IBS the low FODMAP diet & other adjunct therapies Presented by Shirley Webber and Dr Jane Varney Q. When doing the challenges, does the patient have
Dietitian Connection Webinar: Dietary management of IBS the low FODMAP diet & other adjunct therapies Presented by Shirley Webber and Dr Jane Varney Q. When doing the challenges, does the patient have
Why does my stomach hurt? Exploring irritable bowel syndrome
 Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
IBS current status Peter Laszlo Lakatos
 IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
IBS current status Peter Laszlo Lakatos Semmelweis University 1st Department of Medicine Functional gastrointestinal disorders Chronic or fluctuating functional gastrointestinal symptoms that can not be
Understanding IRRITABLE BOWEL SYNDROME (IBS)
") Understanding IRRITABLE BOWEL SYNDROME (IBS) What is irritable bowel syndrome (IBS)? Irritable bowel syndrome (IBS) is a disorder affecting the intestine. IBS involves problems with motility (movement
Understanding IRRITABLE BOWEL SYNDROME (IBS) What is irritable bowel syndrome (IBS)? Irritable bowel syndrome (IBS) is a disorder affecting the intestine. IBS involves problems with motility (movement
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514
 Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
IBS: overview and assessment of pain outcomes and implications for inclusion criteria
 IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
5 Things to Know About Irritable Bowel Syndrome
 5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Chronic diarrhea. Dr.Nasser E.Daryani Professor of Tehran Medical University
 1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
1 Chronic diarrhea Dr.Nasser E.Daryani Professor of Tehran Medical University Timing Acute diarrhea: 4 weeks Definitions Derived from Greek
Tana's Habitat - Vim and Vigor - They Don t Call Them High Bars For Nothin
 http://www.tanashabitat.com/vim/0404151of6.asp Do you have a tummy ache that ver seems to go away? Do you wish your gu would just calm down and let you live your life? If so, you re not alo. You may suffer
http://www.tanashabitat.com/vim/0404151of6.asp Do you have a tummy ache that ver seems to go away? Do you wish your gu would just calm down and let you live your life? If so, you re not alo. You may suffer
The role of gut microbiome in IBS
 The role of gut microbiome in IBS Chung Owyang, MD H. Marvin Pollard Professor of Internal Medicine Professor of Molecular and Integrative Physiology Chief, Division of Gastroenterology Director, Pollard
The role of gut microbiome in IBS Chung Owyang, MD H. Marvin Pollard Professor of Internal Medicine Professor of Molecular and Integrative Physiology Chief, Division of Gastroenterology Director, Pollard
Tenapanor for irritable bowel syndrome with constipation
 NIHR Innovation Observatory Evidence Briefing: February 2018 Tenapanor for irritable bowel syndrome with constipation NIHRIO (HSRIC) ID: 6704 NICE ID: 9736 LAY SUMMARY Irritable bowel syndrome with constipation
NIHR Innovation Observatory Evidence Briefing: February 2018 Tenapanor for irritable bowel syndrome with constipation NIHRIO (HSRIC) ID: 6704 NICE ID: 9736 LAY SUMMARY Irritable bowel syndrome with constipation
Bacteriology. Mycology. Patient: SAMPLE PATIENT DOB: Sex: MRN: Rare. Rare. Positive. Brown. Negative *NG. Negative
 Patient: SAMPLE PATIENT DOB: Sex: MRN: 3.2 0.9-26.8 U/g 1.2 0.2-3.3 mg/g 2.2 1.3-8.6 micromol/g 1.1 1.3-23.7 mg/g 1.1 0.2-3.5 mg/g Rare 1.0 0.2-8.8 mg/g Rare 4.4 2.6-32.4 mg/g 64.6 >= 13.6 micromol/g Bacteriology
Patient: SAMPLE PATIENT DOB: Sex: MRN: 3.2 0.9-26.8 U/g 1.2 0.2-3.3 mg/g 2.2 1.3-8.6 micromol/g 1.1 1.3-23.7 mg/g 1.1 0.2-3.5 mg/g Rare 1.0 0.2-8.8 mg/g Rare 4.4 2.6-32.4 mg/g 64.6 >= 13.6 micromol/g Bacteriology
Ever wonder what s really happening on the inside?
 For Practitioners Ever wonder what s really happening on the inside? Are your patients suffering from diarrhea, constipation, bloating, gas or indigestion? Rocky Mountain Analytical is now offering Gut-Well
For Practitioners Ever wonder what s really happening on the inside? Are your patients suffering from diarrhea, constipation, bloating, gas or indigestion? Rocky Mountain Analytical is now offering Gut-Well
10/1/2016. Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD. Kimberly Kearns, APN. Mary Davitt, PMHNP.
 Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD Kimberly Kearns, APN Speakers Bureau: Medtronic Salix Pharmaceuticals Takeda Pharmaceuticals Mary Davitt, PMHNP None Rachel
Kimberly Kearns, MS, APN, ANP-BC Mary Davitt, MS, PMHNP-BC Rachel Richardson, RD Kimberly Kearns, APN Speakers Bureau: Medtronic Salix Pharmaceuticals Takeda Pharmaceuticals Mary Davitt, PMHNP None Rachel
Irritable bowel syndrome (IBS) is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome
 is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome") ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
William Chey, MD University of Michigan Ann Arbor, MI
 Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
Hompes Method. Practitioner Training Level II. Lesson Eight Part 1C SIBO Protocols
 Hompes Method Practitioner Training Level II Lesson Eight Part 1C SIBO Protocols Health for the People Ltd not for reuse without expressed permission Hompes Method is a trading name of Health For The People
Hompes Method Practitioner Training Level II Lesson Eight Part 1C SIBO Protocols Health for the People Ltd not for reuse without expressed permission Hompes Method is a trading name of Health For The People
IBS. Patient INFO. A Guide to Irritable Bowel Syndrome
 Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
REVIEWS. Diagnosis and management of IBs. Sarah Khan and Lin Chang
 REVIEWS Diagnosis and management of IBs Sarah Khan and Lin Chang abstract IBS is a common gastrointestinal condition characterized by chronic or recurrent abdominal pain associated with altered bowel habits.
REVIEWS Diagnosis and management of IBs Sarah Khan and Lin Chang abstract IBS is a common gastrointestinal condition characterized by chronic or recurrent abdominal pain associated with altered bowel habits.
Is Physical Activity Effective In Reducing The Gastrointestinal Symptoms Associated with Irritable Bowel Syndrome?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Physical Activity Effective In Reducing
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Physical Activity Effective In Reducing
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Thornton Natural Healthcare s Better Health News
 August, 2010 Volume 5, Issue 8 Thornton Natural Healthcare s Better Health News www.thornton-health.com Special Interest Articles: Vitamin K Probiotics and IBS IBS Food sensitivity and IBS Mercury and
August, 2010 Volume 5, Issue 8 Thornton Natural Healthcare s Better Health News www.thornton-health.com Special Interest Articles: Vitamin K Probiotics and IBS IBS Food sensitivity and IBS Mercury and
Efficacy and Safety of Lubiprostone. Laura Wozniak February 23, 2010 K30 Monthly Journal Club
 Efficacy and Safety of Lubiprostone Laura Wozniak February 23, 2010 K30 Monthly Journal Club Objectives Brief overview of constipation Review of article Discussion Constipation in Children 3-5% of all
Efficacy and Safety of Lubiprostone Laura Wozniak February 23, 2010 K30 Monthly Journal Club Objectives Brief overview of constipation Review of article Discussion Constipation in Children 3-5% of all
IBS CLOSED REFERRAL STATUS: Dear Dr.,
 Name: PHN/ULI: DOB: RHRN: RefMD: Dr. RefMD Fax: RefDate: Date Today: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS: Dear Dr., Referral Received Enhanced Primary Care Pathway CLOSED IBS The clinical and
Name: PHN/ULI: DOB: RHRN: RefMD: Dr. RefMD Fax: RefDate: Date Today: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS: Dear Dr., Referral Received Enhanced Primary Care Pathway CLOSED IBS The clinical and
Canadian Association of Gastroenterology Clinical Practice Guideline for the Management of Irritable Bowel Syndrome (IBS)
") Journal of the Canadian Association of Gastroenterology, 2019, XX(X), 1 24 doi: 10.1093/jcag/gwy071 Original Article Original Article Canadian Association of Gastroenterology Clinical Practice Guideline
Journal of the Canadian Association of Gastroenterology, 2019, XX(X), 1 24 doi: 10.1093/jcag/gwy071 Original Article Original Article Canadian Association of Gastroenterology Clinical Practice Guideline
Modulation of abdominal pain by probiotics. Anna Lyra, PhD DuPont Nutrition & Health
 Modulation of abdominal pain by probiotics Anna Lyra, PhD DuPont Nutrition & Health Functional gastrointestinal (GI) wellbeing Up to 70% suffer from functional GI symptoms - ¾ do not seek medical care
Modulation of abdominal pain by probiotics Anna Lyra, PhD DuPont Nutrition & Health Functional gastrointestinal (GI) wellbeing Up to 70% suffer from functional GI symptoms - ¾ do not seek medical care
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics. Dr. Alia Shatanawi
 GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
UKLIN1693a, date of preparation: March 2013.
 1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
อภ ชาต แสงจ นทร ภาคว ชาอาย รศาสตร คณะแพทย ศาสตร มหาว ทยาล ยขอนแก น
 อภ ชาต แสงจ นทร ภาคว ชาอาย รศาสตร คณะแพทย ศาสตร มหาว ทยาล ยขอนแก น Functional bowel disorder characterized by abdominal pain or discomfort and altered bowel habits in the absence of detectable structural
อภ ชาต แสงจ นทร ภาคว ชาอาย รศาสตร คณะแพทย ศาสตร มหาว ทยาล ยขอนแก น Functional bowel disorder characterized by abdominal pain or discomfort and altered bowel habits in the absence of detectable structural
Understanding probiotics and health
 Understanding probiotics and health Gemma Laws MSc Student Microbiology and Immunology Department The gut microbiota The name given to the total microbial population living in our intestine Bacteria, fungi,
Understanding probiotics and health Gemma Laws MSc Student Microbiology and Immunology Department The gut microbiota The name given to the total microbial population living in our intestine Bacteria, fungi,
Gastrointestinal Society 2016 SURVEY RESULTS
 Gastrointestinal Society 2016 SURVEY RESULTS Irritable Bowel Syndrome (IBS) The GI (Gastrointestinal) Society represents Canadians living with gastrointestinal diseases and disorders including those who
Gastrointestinal Society 2016 SURVEY RESULTS Irritable Bowel Syndrome (IBS) The GI (Gastrointestinal) Society represents Canadians living with gastrointestinal diseases and disorders including those who
Is Gut-Directed Hypnotherapy An Effective Treatment For Refractory IBS?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Gut-Directed Hypnotherapy An Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2018 Is Gut-Directed Hypnotherapy An Effective
Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R.
 UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version
UvA-DARE (Digital Academic Repository) Studies on inflammatory bowel disease and functional gastrointestinal disorders in children and adults Hoekman, D.R. Link to publication Citation for published version