Communicating Pain Assessment Effectively
|
|
|
- Amberly Floyd
- 5 years ago
- Views:
Transcription




1 ASCO International Palliative Care Course Jakarta, March 08 10, 2017 Communicating Pain Assessment Effectively Janet Abrahm, MD, FAAHPM, FACP Palliative Care Interdisciplinary Curriculum
2 Pain assessment Objectives Listening Model to guide symptom assessment Communicating effectively PAINAD
3 Imagine
4 How will you feel if I don t ask about your concerns?
5 Listening Exercise Pairs 1, 2 Speaker, listener Speaker describe a significant event in your life Person, pet, object, etc 3 minutes Listener silent
6 Group debrief The biggest communication problem We do not listen to understand We listen to reply
7 Pain assessment is a model for symptom assessment...

8 Video Hector 67 year old male Colon cancer Bone metastases Listen for important elements of the pain assessment...

9
10 Video Debrief What were the important elements of the pain assessment...
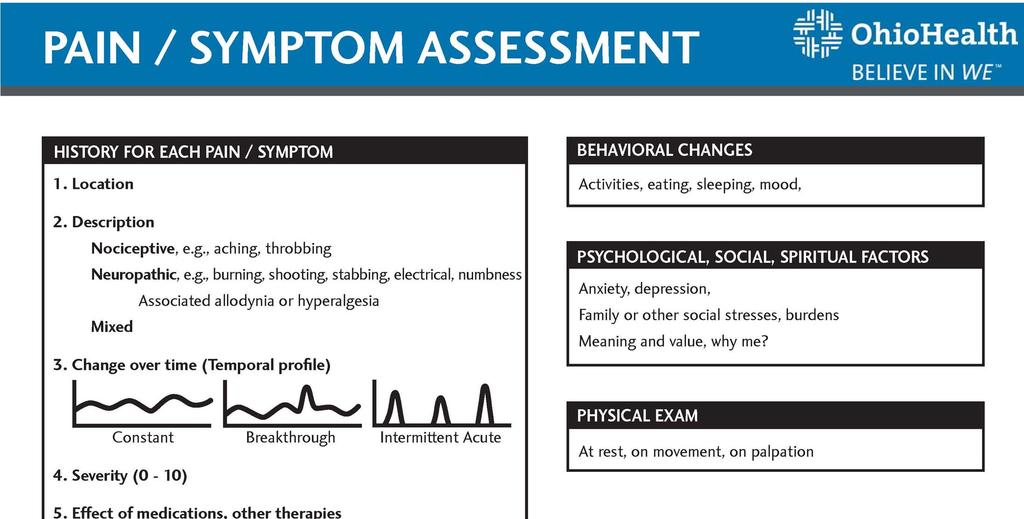
11 Pain Assessment 1. Location 2. Description ( type ) 3. Change over time 4. Severity ( 0 10 ) 5. Effect of treatments Benefit ( + ) Side effects ( - )
12 Where is it? Does it move? 1. Location
13 2. Description What does the pain feel like? Does it ever feel burning or shooting? How does the pain impact your life?
14 Nociceptive Pain Somatic pain Described as... Skin, soft tissue, bone Easy to describe, localize Visceral pain Organs Difficult to describe, localize Sharp Aching Throbbing Wolf CJ. Ann Intern Med
15 Neuropathic Pain Described as Burning Electrical Shooting Stabbing Tingling Associated numbness Pain may be > observable injury Wolf CJ. Ann Intern Med
16 3. Change over time Constant Breakthrough Intermittent acute

17 4. Pain Severity = 5th Vital Sign 17
18 5. Effect of treatments Medications, therapies tried What worked? What didn t work? Any effects you didn t like?
19 Pain Assessment Psychological social spiritual concerns Anxiety, depression Family or other social stresses, burdens Meaning and value, Why me? Behavioral changes Activities, mood
20 General exam Focused exam Examination Guarding? Pain with motion? Masses, tenderness? Psychological exam Anxious, withdrawn, depressed?
21
22 Communicating pain assessment effectively
23 Communication The wrong way The right way
24 Communication Exercise Pairs 1, 2 Same case study Clinician 1 give report Clinician 2 receive report, listen
25 Communicating Assessment Brief description of the patient 1. Location 2. Description ( type ) 3. Change over time 4. Severity ( 0 10 ) 5. Effect of treatments Benefit ( + ) Side effects ( - )
26 Repeat Communication Exercise Same pairs 1, 2 Same case study Clinician 2 give report Clinician 1 receive report, listen
27 Communicating Assessment Brief description of the patient 1. Location: Leg 2. Description ( type ): Dull 3. Change over time: no 4. Severity ( 0 10 ): Average 3, Worst 4 5. Effect of treatments: Meds, cream Benefit ( + ) Side effects ( - )
28 Group Discussion Is structure helpful? Take-home messages?
29 Pain assessment in the cognitively impaired

30 Warden V, Hurley AC, Volicer V. J Am Med Dir Assoc, 2003; 4 :9-15.
31 Other Symptom Assessment 1. Location 2. Description ( type ) 3. Change over time 4. Severity ( 0 10 ) 5. Effect of treatments Benefit ( + ) Side effects ( - )

32 Summary Listen Assess Communicate effectively Pain is a model for symptom assessment and communication...



33 Gandhi You need to be the change you want to see in the world Kobacker House Columbus, Ohio ASCO International Palliative Care Course Jakarta, March 08 10, 2017
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
May 2015 Clinical Nurse Educator Arohanui Hospice
 May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
May 2015 Clinical Nurse Educator Arohanui Hospice End of Life Care, what s on top? Feedback from last session (Physiology of Dying) Volunteer to present at August meeting Presentation: Breaking Bad News
VAO PAIN RELIEF HANDOUT
 HANDOUT AMBULANCE TASMANIA 1 Clinical Field Protocols To complete this module, you will need to become familiar with the following clinical protocols: Clinical Approach to a Patient VAO CFP03 Pain Relief
HANDOUT AMBULANCE TASMANIA 1 Clinical Field Protocols To complete this module, you will need to become familiar with the following clinical protocols: Clinical Approach to a Patient VAO CFP03 Pain Relief
Geriatric Pain Assessment and Management. Robin Arends, DNP, CNP, FNP-BC
 + Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
+ Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
Location of initiative York Region Chronic Kidney Disease Program, Mackenzie Richmond Hill Hospital, Richmond Hill, ON
 Story # CSHP 015 objective Objective.1 - In 70% of ambulatory and specialized care clinics providing clinic care, pharmacists will manage medication therapy for clinic patients with complex and high-risk
Story # CSHP 015 objective Objective.1 - In 70% of ambulatory and specialized care clinics providing clinic care, pharmacists will manage medication therapy for clinic patients with complex and high-risk
PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM NAME: D.O.B AGE: SEX: STREET: CITY: STATE: ZIP: SS #: ETHNICITY: RACE: LANGUAGE: PHONE # TO LEAVE A PERSONAL MESSAGE: HOME PHONE #: WORK #: CELL #: E MAIL ADDRESS: EMERGENCY CONTACT:
PATIENT REGISTRATION FORM NAME: D.O.B AGE: SEX: STREET: CITY: STATE: ZIP: SS #: ETHNICITY: RACE: LANGUAGE: PHONE # TO LEAVE A PERSONAL MESSAGE: HOME PHONE #: WORK #: CELL #: E MAIL ADDRESS: EMERGENCY CONTACT:
Where is your pain located? Please use the diagram below to indicate where most of your pain is located.
 Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
Patient Comfort Assessment Guide. To facilitate your assessment of your patients pain and its effect on their daily activities
 Patient Comfort Assessment Guide To facilitate your assessment of your patients pain and its effect on their daily activities Patient Comfort Assessment Guide Pharmacologic management of pain, as a component
Patient Comfort Assessment Guide To facilitate your assessment of your patients pain and its effect on their daily activities Patient Comfort Assessment Guide Pharmacologic management of pain, as a component
DOCTOR DISCUSSION GUIDE
 DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
DOCTOR DISCUSSION GUIDE BE PREPARED For the best outcome from a visit with your doctor, it s important to be prepared. The more completely and clearly you describe the pain you re experiencing, the easier
The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes
 The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes 1 Medical Hypothesis 2007, Vol. 69, pp. 1169 1178 Sota Omoigui
The biochemical origin of pain: The origin of all pain is inflammation and the inflammatory response: Inflammatory profile of pain syndromes 1 Medical Hypothesis 2007, Vol. 69, pp. 1169 1178 Sota Omoigui
tain PHow o Manage Your This patient guide will help you understand:
 tain PHow o Manage Your This patient guide will help you understand: What is cancer-related pain? pg 2 What causes cancer-related pain? pg 3 What can I do to manage my pain? pg 4 When should I talk to
tain PHow o Manage Your This patient guide will help you understand: What is cancer-related pain? pg 2 What causes cancer-related pain? pg 3 What can I do to manage my pain? pg 4 When should I talk to
Get Help for. Cancer Pain
 Get Help for Cancer Pain Pain does not have to be part of cancer. If you have cancer, you may have pain. But you can do something about it. Treating pain is a key part of cancer treatment. There are many
Get Help for Cancer Pain Pain does not have to be part of cancer. If you have cancer, you may have pain. But you can do something about it. Treating pain is a key part of cancer treatment. There are many
HISTORY OF PRESENT ILLNESS A. TELL US ABOUT YOUR PAIN PROBLEM
 1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
RESEARCH STUDY: RELATIONSHIP BETWEEN PAIN AND SLEEP IN SPINAL CORD INJURY PATIENTS Pain perception : McGill Pain Questionnaire
 RESEARCH STUDY: RELATIONSHIP BETWEEN PAIN AND SLEEP IN SPINAL CORD INJURY PATIENTS Pain perception : McGill Pain Questionnaire Participants Name: Date: Time: PRI: S A E M PRI (TOTAL) PPI (1-10) (11-15)
RESEARCH STUDY: RELATIONSHIP BETWEEN PAIN AND SLEEP IN SPINAL CORD INJURY PATIENTS Pain perception : McGill Pain Questionnaire Participants Name: Date: Time: PRI: S A E M PRI (TOTAL) PPI (1-10) (11-15)
BRIEF PAIN INVENTORY LONG FORM
 BRIEF PAIN INVENTORY LONG FORM Date: Name: 1) Marital Status (at present) Single Widowed Married Separated/Divorced 2) Education (Circle only the highest grade or degree completed) Grade 0 1 2 3 4 5 6
BRIEF PAIN INVENTORY LONG FORM Date: Name: 1) Marital Status (at present) Single Widowed Married Separated/Divorced 2) Education (Circle only the highest grade or degree completed) Grade 0 1 2 3 4 5 6
NECK PAIN QUESTIONNAIRE
 NECK PAIN QUESTIONNAIRE This questionnaire is designed by your doctor to answer specific questions. Please answer each question as completely as possible. Name: Date: 1. How long have you had neck pain?
NECK PAIN QUESTIONNAIRE This questionnaire is designed by your doctor to answer specific questions. Please answer each question as completely as possible. Name: Date: 1. How long have you had neck pain?
Orofacial Pain Examination Form
 ADVANCED ORAL AND FACIAL SURGERY OF THE MAIN LINE, PC G. JOEL FUNARI, M.S., D.M.D. Orofacial Pain Examination Form Please complete pages 1 through 4. Circle choices whenever available. Name Date SSN DOB
ADVANCED ORAL AND FACIAL SURGERY OF THE MAIN LINE, PC G. JOEL FUNARI, M.S., D.M.D. Orofacial Pain Examination Form Please complete pages 1 through 4. Circle choices whenever available. Name Date SSN DOB
New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification
 Certification") Name Social Security Number Address: Street: _ New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification Date of Birth Gender: Male Female City: State Zip Code E-mail: Home Phone:
Name Social Security Number Address: Street: _ New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification Date of Birth Gender: Male Female City: State Zip Code E-mail: Home Phone:
Evaluation and Management of Pain in Children
 Evaluation and Management of Pain in Children What is pain? Is a very complex experience Affects psychology and physiology of the person experiencing it Is a response for self preservation Depends on many
Evaluation and Management of Pain in Children What is pain? Is a very complex experience Affects psychology and physiology of the person experiencing it Is a response for self preservation Depends on many
Name: (Last) (First) (Middle) Address: (City) (State) (Zip) Home: ( ) Work: ( ) Cell: ( ) Age: DOB: SS#: Height: Weight: Occupation:
 (First) (Middle) Address: (City) (State) (Zip) Home: ( ) Work: ( ) Cell: ( ) Age: DOB: SS#: Height: Weight: Occupation:") 2124 Route 35, Tel: (732) 788-0349 Holmdel, Fax: (877) 211-6276 NJ, E-mail: info@gramercypaincenter.com 07733. www.gramercypaincenter.com Date: Name: (Last) (First) (Middle) Home: ( ) Work: ( ) Cell: (
2124 Route 35, Tel: (732) 788-0349 Holmdel, Fax: (877) 211-6276 NJ, E-mail: info@gramercypaincenter.com 07733. www.gramercypaincenter.com Date: Name: (Last) (First) (Middle) Home: ( ) Work: ( ) Cell: (
Foundations of Palliative Care Series
 Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Foundations of Palliative Care Series Developed by: Tim Sakaluk MD, Ingrid See CPL, Tammy Dyson SW, Sharon Salomons SCP!!!!!! This course was developed in collaboration with the UBC Learning Circle to
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Eastern Shore MediCann Clinic, LLC
 Eastern Shore MediCann Clinic, LLC New Patient Medical History and Intake Form Medical Marijuana Certification Name Date of Birth Social Security Number Gender: Male Female Address: Street: City: State
Eastern Shore MediCann Clinic, LLC New Patient Medical History and Intake Form Medical Marijuana Certification Name Date of Birth Social Security Number Gender: Male Female Address: Street: City: State
Pain Management: Overview of A Practical Approach
 Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
NEW PATIENT INFORMATION
 OrthoNeuro For every motion in life. NEW PATIENT INFORMATION NAME: AGE: DATE: REFERRING DOCTOR/THERAPIST: SELF REFERRAL (if so, circle) Are you: Male Female Right handed Left handed Ambidextrous CHIEF
OrthoNeuro For every motion in life. NEW PATIENT INFORMATION NAME: AGE: DATE: REFERRING DOCTOR/THERAPIST: SELF REFERRAL (if so, circle) Are you: Male Female Right handed Left handed Ambidextrous CHIEF
Introduction To Pain Management In Palliative Care
 Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Pain. Fears and Facts. What is pain? Factors that Affect People with Pain. Symptom Management
 Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
CNA Training Advisor
 CNA Training Advisor Volume 12 Issue No. 1 January 2014 Pain management Pain affects many nursing home residents. It often results from injury or sensory stimulation. A variety of factors affect recognition,
CNA Training Advisor Volume 12 Issue No. 1 January 2014 Pain management Pain affects many nursing home residents. It often results from injury or sensory stimulation. A variety of factors affect recognition,
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Elements for a public summary
 VI.2 Elements for a public summary Part VI.2 Elements for a public summary is applicable for all products that are covered by this RMP, except from the important potential risk of Medication error with
VI.2 Elements for a public summary Part VI.2 Elements for a public summary is applicable for all products that are covered by this RMP, except from the important potential risk of Medication error with
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN
 Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Elbow and Forearm Pain Form
 Elbow and Forearm Pain Form Last Name First Name Date RIGHT LEFT My dominant hand? Right Left Does your elbow hurt? Yes No Yes No Does your forearm hurt? Yes No Yes No When did the problem start? Did you
Elbow and Forearm Pain Form Last Name First Name Date RIGHT LEFT My dominant hand? Right Left Does your elbow hurt? Yes No Yes No Does your forearm hurt? Yes No Yes No When did the problem start? Did you
(Patients complete on initial consult)
") Person Completing the Form: Primary Care Physician and phone number: Referring Physician and phone number: Please list all other physicians involved in your care: Current Medical History: What is the health
Person Completing the Form: Primary Care Physician and phone number: Referring Physician and phone number: Please list all other physicians involved in your care: Current Medical History: What is the health
Recognizing & Treating Pain
 Recognizing & Treating Pain Making a Difference in the Lives of your Residents Presented by: Demi Haffenreffer, RN, MBA demi@consultdemi.net www.consultdemi.net Pain Assessment & Management in Long Term
Recognizing & Treating Pain Making a Difference in the Lives of your Residents Presented by: Demi Haffenreffer, RN, MBA demi@consultdemi.net www.consultdemi.net Pain Assessment & Management in Long Term
Name (First, Middle initial, Last): Mailing Address: Home phone: Cell Gender identification: M F Birthdate: Age: Birthplace:
: Mailing Address: Home phone: Cell Gender identification: M F Birthdate: Age: Birthplace:") General Information Name (First, Middle initial, Last): Mailing Address: Home phone: Cell Email Gender identification: M F Birthdate: Age: Birthplace: Nationality: Religion: Marital Status: Ages of children
General Information Name (First, Middle initial, Last): Mailing Address: Home phone: Cell Email Gender identification: M F Birthdate: Age: Birthplace: Nationality: Religion: Marital Status: Ages of children
COMPREHENSIVE PAIN MANAGEMENT INTAKE FORM. Home Phone: Other Contact: Other Contact: Address: City: State: Zip: Address: City: State: Zip:
 COMPREHENSIVE PAIN MANAGEMENT INTAKE FORM Last Name: First Name: Middle: Home Phone: Other Contact: Other Contact: DOB: Age: Sex: Name of Referring Physician: Phone: Fax: Address: City: State: Zip: Name
COMPREHENSIVE PAIN MANAGEMENT INTAKE FORM Last Name: First Name: Middle: Home Phone: Other Contact: Other Contact: DOB: Age: Sex: Name of Referring Physician: Phone: Fax: Address: City: State: Zip: Name
PAIN RELIEF CENTER SPECIFIC FORM
 PAIN RELIEF CENTER SPECIFIC FORM Legal Name: Referring Specialist: CONCERNS Thank you for taking the time to fill out this intake form. We know it is comprehensive, but by gathering this information about
PAIN RELIEF CENTER SPECIFIC FORM Legal Name: Referring Specialist: CONCERNS Thank you for taking the time to fill out this intake form. We know it is comprehensive, but by gathering this information about
Aspire Pain Medical Center
 Aspire Pain Medical Center Welcome to Aspire Pain Medical Center. We are looking forward to providing you with the best care to manage your needs. Please take the time to complete the following questionnaire
Aspire Pain Medical Center Welcome to Aspire Pain Medical Center. We are looking forward to providing you with the best care to manage your needs. Please take the time to complete the following questionnaire
PATIENT HISTORY FORM
 PATIENT HISTORY FORM NAME: DATE: DATE OF BIRTH/AGE: Name of the physician who referred you to see a neurosurgeon: City and State of referring physician: Is your referring physician a chiropractor? Yes
PATIENT HISTORY FORM NAME: DATE: DATE OF BIRTH/AGE: Name of the physician who referred you to see a neurosurgeon: City and State of referring physician: Is your referring physician a chiropractor? Yes
Pain. Types of Pain. Types of Pain 8/21/2013
 Pain 1 Types of Pain Acute Pain Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus Mediated by rapidly conducting nerve pathways & associated with increased
Pain 1 Types of Pain Acute Pain Complex combination of sensory, perceptual, & emotional experiences as a result of a noxious stimulus Mediated by rapidly conducting nerve pathways & associated with increased
Pain Notebook NAME PHONE. Three Hole Punch Here Three Hole Punch Here. Global Pain Initiative 2018 Ver 1.0
 Pain Notebook Three Hole Punch Here Three Hole Punch Here NAME EMAIL PHONE Global Pain Initiative 2018 Ver 1.0 What is pain? Pain is a bad sensation that tells you something is wrong. Pain falls into two
Pain Notebook Three Hole Punch Here Three Hole Punch Here NAME EMAIL PHONE Global Pain Initiative 2018 Ver 1.0 What is pain? Pain is a bad sensation that tells you something is wrong. Pain falls into two
**PLEASE NOTE OUR NEW ADDRESS** The Spine Center 159 Wells Ave, Newton, MA Ph: Fax:
 Helpful Telephone Numbers Pre-Registration 855-890-9241 Hospital Billing (NWH) 617-726-3884 Physician/Provider Billing (MGPO) 617-726-3884 Web Address nwh.org Pre-Registration Please call up to 7 days
Helpful Telephone Numbers Pre-Registration 855-890-9241 Hospital Billing (NWH) 617-726-3884 Physician/Provider Billing (MGPO) 617-726-3884 Web Address nwh.org Pre-Registration Please call up to 7 days
HEADACHE QUESTIONNAIRE
 HEADACHE QUESTIONNAIRE 1. How long have you experienced headaches (include all types)? 2. How old were you when you first had headaches (of any type)? 3. When was your last headache? 4. How severe are
HEADACHE QUESTIONNAIRE 1. How long have you experienced headaches (include all types)? 2. How old were you when you first had headaches (of any type)? 3. When was your last headache? 4. How severe are
Standardized Evaluation of Pain (StEP) Neuropathic Pain
 Neuropathic Pain") Standardized Evaluation of Pain (StEP) Neuropathic Pain Patient s name: Date of birth: / / Patient ID Examiner s name: Date of the examination: / / Introduction (please read to the patient) To get a better
Standardized Evaluation of Pain (StEP) Neuropathic Pain Patient s name: Date of birth: / / Patient ID Examiner s name: Date of the examination: / / Introduction (please read to the patient) To get a better
Palliative Care and End of Life Care
 Palliative Care and End of Life Care 8/2012 Palliative Care Palliative care is specialized medical care for people with serious illness. This type of care is focused on providing patients with relief from
Palliative Care and End of Life Care 8/2012 Palliative Care Palliative care is specialized medical care for people with serious illness. This type of care is focused on providing patients with relief from
New Patient Pain Evaluation
 New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
Identification of Painful Tissue Orthopaedic Examination DX 612. James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic
 Identification of Painful Tissue Orthopaedic Examination DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Generalized Pain Description Joint pain may be constant
Identification of Painful Tissue Orthopaedic Examination DX 612 James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Generalized Pain Description Joint pain may be constant
WellnessPro. - Test booklet -
 WellnessPro - Test booklet - It's clear that pain is understood by anyone and that everyone feels it a bit differently. Overall, pain is an unpleasant sensation that occurs in varying degrees of severity
WellnessPro - Test booklet - It's clear that pain is understood by anyone and that everyone feels it a bit differently. Overall, pain is an unpleasant sensation that occurs in varying degrees of severity
Welcome to NHS Highland Pain Management Service
 Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
Personal &Work Information Date: Patient Name: Age: City: State: Zip: Primary Care Physician: PCP Phone:
 Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Loyola University Medical Center Female Pelvic Medicine & Reconstructive Surgery
 Loyola University Medical Center Female Pelvic Medicine & Reconstructive Surgery Medical History Questionnaire Name: Date: Age: D.O.B. Race: What is the nature of your current gynecologic or urologic medical
Loyola University Medical Center Female Pelvic Medicine & Reconstructive Surgery Medical History Questionnaire Name: Date: Age: D.O.B. Race: What is the nature of your current gynecologic or urologic medical
What is your present motivation for consulting our office? Vital Information (Adult)
") What is your present motivation for consulting our office? Heal disease, symptoms and infirmities (ill-health) Preventing disease, symptoms and infirmities (ill-health) Improving family and/or community
What is your present motivation for consulting our office? Heal disease, symptoms and infirmities (ill-health) Preventing disease, symptoms and infirmities (ill-health) Improving family and/or community
Improving Health, Enriching Life. Pain Management. Altru HEALTH SYSTEM
 Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
Improving Health, Enriching Life altru.org Pain Management Altru HEALTH SYSTEM There are many different causes and kinds of pain. Pain can be caused by injury, illness, sickness, disease or surgery. Treating
A Letter From Home February 2016
 More than two thirds of all Americans suffer from multiple, chronic conditions. An estimated 60-70% of people over 65 report at least some persistent pain (Centers for Disease Control and Prevention, 2013).
More than two thirds of all Americans suffer from multiple, chronic conditions. An estimated 60-70% of people over 65 report at least some persistent pain (Centers for Disease Control and Prevention, 2013).
Dear Patient, Sincerely, South Texas Bone & Joint Physical Therapy & Rehabilitation Team
 Physical Therapy & Rehabilitation 601 Texan Trail, Suite 250 Corpus Christi, Texas 78411 Telephone: (361)854-0811 EXT 221 Fax: (361)561-0609 www.southtexasboneandjoint.com Dear Patient, South Texas Bone
Physical Therapy & Rehabilitation 601 Texan Trail, Suite 250 Corpus Christi, Texas 78411 Telephone: (361)854-0811 EXT 221 Fax: (361)561-0609 www.southtexasboneandjoint.com Dear Patient, South Texas Bone
PAIN HISTORY. Please describe your pain:
 Name: Date: PAIN HISTORY Please describe your pain: List surgeries/hospital admissions and dates (Skip if you have already provided this information on Medical History Questionnaire): Please list current
Name: Date: PAIN HISTORY Please describe your pain: List surgeries/hospital admissions and dates (Skip if you have already provided this information on Medical History Questionnaire): Please list current
DEPARTMENT OF NEUROSURGERY Spine Center New Patient Intake Form
 DEPARTMENT OF NEUROSURGERY Spine Center New Patient Intake Form Today's date: Your name: Date of birth: Email address: CHIEF COMPLAINT What is the main reason that you are seeking medical attention? Please
DEPARTMENT OF NEUROSURGERY Spine Center New Patient Intake Form Today's date: Your name: Date of birth: Email address: CHIEF COMPLAINT What is the main reason that you are seeking medical attention? Please
Thank you for choosing Holy Cross Outpatient Rehabilitation
 Thank you for choosing Holy Cross Outpatient Rehabilitation Please complete the attached paperwork prior to your arrival. Ensure you know which facility you are scheduled for. Please arrive 30 minutes
Thank you for choosing Holy Cross Outpatient Rehabilitation Please complete the attached paperwork prior to your arrival. Ensure you know which facility you are scheduled for. Please arrive 30 minutes
Date: Can we leave messages on voice mail at home/work/cell? Yes No. Sex: Male Female SS#: If yes, what type? Auto Work Other.
 1 Patient Information : Name: Last First MI Email address: Mailing Address: Phone # (H) (W) (Other) Can we call you at work? Yes No of Birth: Can we leave messages on voice mail at home/work/cell? Yes
1 Patient Information : Name: Last First MI Email address: Mailing Address: Phone # (H) (W) (Other) Can we call you at work? Yes No of Birth: Can we leave messages on voice mail at home/work/cell? Yes
Emad F. Abdallah, DMD, MS Member, American Association of Orthodontists Diplomate, American Board of Orofacial Pain
 Patient s Date: Age: Sex: Date of Birth: Home Occupation: Chief Complaint: Duration of the problem: Problem most severe: Morning Afternoon Evening Sleeping Eating No pattern SYMPTOMS Left Right Face Pain
Patient s Date: Age: Sex: Date of Birth: Home Occupation: Chief Complaint: Duration of the problem: Problem most severe: Morning Afternoon Evening Sleeping Eating No pattern SYMPTOMS Left Right Face Pain
Arresting Pain without Getting Arrested
 G. Jay Westbrook, M.S., R.N., CHPN - Clinical Director Compassionate Journey: An End-of-Life Clinical & Education Service CompassionateJourney@hotmail.com 818/773-3700 Arresting Pain without Getting Arrested
G. Jay Westbrook, M.S., R.N., CHPN - Clinical Director Compassionate Journey: An End-of-Life Clinical & Education Service CompassionateJourney@hotmail.com 818/773-3700 Arresting Pain without Getting Arrested
Family First Chiropractic
 Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
Family First Chiropractic Personal Information Title: (Check one) Mr. Mrs. Ms. Miss Other First Name Middle Initial Last Name Street City State Zip Code Email Home Phone ( ) - Cell Phone ( ) - Date of
NEW PATIENT DEMOGRAPHICS QUESTIONNAIRE
 NEW PATIENT DEMOGRAPHICS QUESTIONNAIRE Today s : Patient Name: DOB: Race White/Caucasian Black/African American Asian Native American Alaskan Native Native Hawaiian Pacific Islander Other: Preferred Language:
NEW PATIENT DEMOGRAPHICS QUESTIONNAIRE Today s : Patient Name: DOB: Race White/Caucasian Black/African American Asian Native American Alaskan Native Native Hawaiian Pacific Islander Other: Preferred Language:
History of Present Condition
 Name: Date: Address: City: Province: Postal Code: Home Phone: Cell Phone: Work Phone: Email: Marital Status: Name Of Family Physician (MD): Age: Occupation: Employer: Extended Health Care Company: Policy
Name: Date: Address: City: Province: Postal Code: Home Phone: Cell Phone: Work Phone: Email: Marital Status: Name Of Family Physician (MD): Age: Occupation: Employer: Extended Health Care Company: Policy
Pain In Primary Care. Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant
 Pain In Primary Care Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant Outline è Definition of pain è Prevalence and significance è Causes è Assessment
Pain In Primary Care Dr. Chris Frank Dr. John Puxty Deanna Abbott-McNeil, GiiC Consultant Susanne Murphy, GiiC Consultant Outline è Definition of pain è Prevalence and significance è Causes è Assessment
New Patient Evaluation Form
 New Patient Evaluation Form Alfred Tennant, DDS TMJ, Facial Pain, Dental Sleep Medicine 33 Davis Blvd Tampa, FL 33606 Fax (813)658-6254 Phone (813)743-2352 Please complete pages 1-8 and circle choices
New Patient Evaluation Form Alfred Tennant, DDS TMJ, Facial Pain, Dental Sleep Medicine 33 Davis Blvd Tampa, FL 33606 Fax (813)658-6254 Phone (813)743-2352 Please complete pages 1-8 and circle choices
ELNEC. Module 2 Pain Assessment & Management. Geriatric Curriculum ELNEC- END-OF-LIFE NURSING EDUCATION CONSORTIUM. Geriatric Curriculum
 ELNEC END-OF-LIFE NURSING EDUCATION CONSORTIUM Module 2 Pain Assessment & Management Part I: Module 2 General pain assessment Assessment of pain in nonverbal residents Part II: Pharmacological management
ELNEC END-OF-LIFE NURSING EDUCATION CONSORTIUM Module 2 Pain Assessment & Management Part I: Module 2 General pain assessment Assessment of pain in nonverbal residents Part II: Pharmacological management
Integrated Care for Depression, Anxiety and PTSD. Introduction: Overview of Clinical Roles and Ideas
 Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
Integrated Care for Depression, Anxiety and PTSD University of Washington An Evidence-based d Approach for Behavioral Health Professionals (LCSWs, MFTs, and RNs) Alameda Health Consortium November 15-16,
New Patient Pain History Form
 New Patient Pain History Form Name: Date of Birth: / / Today s Date: / / Date the Pain Began: / / Reason for visit: Describe what caused the pain (accident, injury, etc.): Pain 1. Pain/Symptom Description
New Patient Pain History Form Name: Date of Birth: / / Today s Date: / / Date the Pain Began: / / Reason for visit: Describe what caused the pain (accident, injury, etc.): Pain 1. Pain/Symptom Description
PAIN MANAGEMENT IN CHILDREN
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Non-prescription pain relievers
 John Bell Counter says Connection Non-prescription pain relievers Pharmacy assistant s education Module 225 Non-prescription pain relievers By Madeline Thompson This education module is independently researched
John Bell Counter says Connection Non-prescription pain relievers Pharmacy assistant s education Module 225 Non-prescription pain relievers By Madeline Thompson This education module is independently researched
Re-Exam Questionnaire
 Re-Exam Questionnaire Patient Name: Date: The following hi-lighted symptoms are what brought you into our office originally. DIRECTIONS: Please rate ALL hi-lighted symptoms: S = same; B = better; W = worse
Re-Exam Questionnaire Patient Name: Date: The following hi-lighted symptoms are what brought you into our office originally. DIRECTIONS: Please rate ALL hi-lighted symptoms: S = same; B = better; W = worse
The UW Pain Treatment and Research Center takes a holistic approach to your pain care.
 Pain Treatment and Research Center 5249 East Terrace Drive Madison, WI 53718 Phone: (608) 263-9550 Dear Patient: The UW Pain Treatment and Research Center takes a holistic approach to your pain care. You
Pain Treatment and Research Center 5249 East Terrace Drive Madison, WI 53718 Phone: (608) 263-9550 Dear Patient: The UW Pain Treatment and Research Center takes a holistic approach to your pain care. You
Name: Date: Street Address: Referring Physician: How long have you had your current problem?
 3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
Parent Pain Questionnaire Understanding your child s pain
 Parent Pain Questionnaire Understanding your child s pain This questionnaire is to help us learn about your child's pain problems. All information obtained from this questionnaire and in interviews will
Parent Pain Questionnaire Understanding your child s pain This questionnaire is to help us learn about your child's pain problems. All information obtained from this questionnaire and in interviews will
NEW CHIROPRACTIC PATIENT INFORMATION Dr. Bryan Mock, LLC 2101 Greentree Rd Pittsburgh, PA
 NEW CHIROPRACTIC PATIENT INFORMATION Dr. Bryan Mock, LLC 2101 Greentree Rd Pittsburgh, PA 15220 412-668-2089 Allergies: WELCOME The doctor and staff would like to welcome you and want to provide you with
NEW CHIROPRACTIC PATIENT INFORMATION Dr. Bryan Mock, LLC 2101 Greentree Rd Pittsburgh, PA 15220 412-668-2089 Allergies: WELCOME The doctor and staff would like to welcome you and want to provide you with
Liberty Chiropractic Clinic Scarsdale Blvd., Houston, TX
 Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Liberty Chiropractic Clinic, -6154 Patient's Name Patient's Address City State Zip Code Age D.O.B. Single Married Divorced Widowed No. of children Occupation Employer Home Phone Work Phone Cell Phone Email
Beyond Cancer Moving On
 Beyond Cancer Moving On Today, people with cancer have a better chance at living a normal life than ever before in history. In fact, there are more than 10 million survivors people who have, or are living
Beyond Cancer Moving On Today, people with cancer have a better chance at living a normal life than ever before in history. In fact, there are more than 10 million survivors people who have, or are living
INFORMATION SHEET FOR THE DEPARTMENT OF PAIN AND PALLIATIVE CARE
 INFORMATION SHEET FOR THE DEPARTMENT OF PAIN AND PALLIATIVE CARE Please review the following instructions as it contains important information regarding the management of your pain. Once reviewed, our
INFORMATION SHEET FOR THE DEPARTMENT OF PAIN AND PALLIATIVE CARE Please review the following instructions as it contains important information regarding the management of your pain. Once reviewed, our
Interventional Pain Outcome Study
 ssmhealth.com/pain White Paper Interventional Pain Outcome Study Introduction Pain commonly presents as a complex process and is equally as difficult to manage and treat. Acute or chronic, pain differs
ssmhealth.com/pain White Paper Interventional Pain Outcome Study Introduction Pain commonly presents as a complex process and is equally as difficult to manage and treat. Acute or chronic, pain differs
HealthPartners Inspire Special Needs Basic Care Clinical Care Planning and Resource Guide CHRONIC PAIN
 The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Institute of Neurological Disorders and Stroke), Mount Sinai Beth Israel
The following evidence based guideline was used in developing this clinical care guide: National Institute of Health (NIH National Institute of Neurological Disorders and Stroke), Mount Sinai Beth Israel
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
MOTOR IMAGERY. for the Treatment of. Patient Information Booklet
 MOTOR IMAGERY This booklet was produced by Marielle Blain, nurse clinician and Dr. François Gobeil, anesthesiologist Pain Management Consultation Unit, CSSS Pierre Boucher In collaboration with DSIPP CSSS
MOTOR IMAGERY This booklet was produced by Marielle Blain, nurse clinician and Dr. François Gobeil, anesthesiologist Pain Management Consultation Unit, CSSS Pierre Boucher In collaboration with DSIPP CSSS
PAIN QUESTIONNAIRE. Patient Name: Patient Date of Birth: Appointment Date:
 Patient Name: Patient Date of Birth: Appointment Date: Please mark and/or notate the areas of your body which are affected by pain. RIGHT RIGHT LEFT LEFT RIGHT LEFT RIGHT RIGHT LEFT LEFT RIGHT LEFT For
Patient Name: Patient Date of Birth: Appointment Date: Please mark and/or notate the areas of your body which are affected by pain. RIGHT RIGHT LEFT LEFT RIGHT LEFT RIGHT RIGHT LEFT LEFT RIGHT LEFT For
NEW PATIENT INFORMATION FORM
 NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
Thank you for choosing Holy Cross Outpatient Rehabilitation
 Thank you for choosing Holy Cross Outpatient Rehabilitation Please complete the attached paperwork prior to your arrival. Ensure you know which facility you are scheduled for. Please arrive 30 minutes
Thank you for choosing Holy Cross Outpatient Rehabilitation Please complete the attached paperwork prior to your arrival. Ensure you know which facility you are scheduled for. Please arrive 30 minutes
A Personalized Approach to Assessing and Managing Pain in Patients With Cancer David Hui and Eduardo Bruera
 VOLUME 32 NUMBER 16 JUNE 1 2014 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E A Personalized Approach to Assessing and Managing Pain in Patients With Cancer David Hui and Eduardo Bruera All authors:
VOLUME 32 NUMBER 16 JUNE 1 2014 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E A Personalized Approach to Assessing and Managing Pain in Patients With Cancer David Hui and Eduardo Bruera All authors:
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
LIST RESTRICTED ACTIVITY: CURRENT ACTIVITY LEVEL USUAL ACTIVITY LEVEL
 Whom may we thank for referring you to this office Today s Date: PATIENT DEMOGRAPHICS? HRN: Name: Birth Date: Age: Male Female Address: City: State: Zip: E mail Address: Home Phone: Mobile Phone: Marital
Whom may we thank for referring you to this office Today s Date: PATIENT DEMOGRAPHICS? HRN: Name: Birth Date: Age: Male Female Address: City: State: Zip: E mail Address: Home Phone: Mobile Phone: Marital
Primary Health Concerns Please use the following to best describe the primary reason you are seeking medical care today.
 Patient Intake Form 30 E. 60 th Street #302 - New York, NY 10022 New Patient Special Consultation Notes: For: (OFFICE USE ONLY) Full Name (First, Last) Date Referral: How did you hear about us? Who should
Patient Intake Form 30 E. 60 th Street #302 - New York, NY 10022 New Patient Special Consultation Notes: For: (OFFICE USE ONLY) Full Name (First, Last) Date Referral: How did you hear about us? Who should
Medical History. Instructions. My telephone number is: 1 Tools Medical History
 Medical History Instructions To do the best possible job with your pain, your doctor needs details about your history, including current and past medical problems, medications, health habits, and family
Medical History Instructions To do the best possible job with your pain, your doctor needs details about your history, including current and past medical problems, medications, health habits, and family
New Patient Intake Form. Please List All Current Medications. Please shade in the areas where you have pain
 New Patient Intake Form Name: Date: Referring Physician Primary Care Physician Please List All Current Medications Do you take Coumadin/Warfarin/Plavix/Lovonox or Aspirin? Yes No Last dose? Please shade
New Patient Intake Form Name: Date: Referring Physician Primary Care Physician Please List All Current Medications Do you take Coumadin/Warfarin/Plavix/Lovonox or Aspirin? Yes No Last dose? Please shade
Individual Planning: A Treatment Plan Overview for Adult with Chronic Pain Problems
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Adult with Chronic Pain Problems A Treatment Plan Overview for Individuals for Adult with Chronic Pain Problems. Duration:
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Adult with Chronic Pain Problems A Treatment Plan Overview for Individuals for Adult with Chronic Pain Problems. Duration:
PEDIATRIC PAIN QUESTIONNAIRE Form A (Adolescent)
") PEDIATRIC PAIN QUESTIONNAIRE Form A (Adolescent) Daniel P. Kohen, M.D. Developmental-Behavioral Pediatrics Partners-in-Healing of Minneapolis 10505 Wayzata Blvd - Suite 200 Minnetonka, MN 55305 763-546-5797
PEDIATRIC PAIN QUESTIONNAIRE Form A (Adolescent) Daniel P. Kohen, M.D. Developmental-Behavioral Pediatrics Partners-in-Healing of Minneapolis 10505 Wayzata Blvd - Suite 200 Minnetonka, MN 55305 763-546-5797
Carriage House Chiropractic and Acupuncture
 Chiropractic Patient History Questionnaire Date: Name: Date of birth: Address: City: St: Zip: Phone: (home) (cell) (work) May we send appointment reminders to you via text messages on your cell phone Email:
Chiropractic Patient History Questionnaire Date: Name: Date of birth: Address: City: St: Zip: Phone: (home) (cell) (work) May we send appointment reminders to you via text messages on your cell phone Email:
NUMBNESS EVALUATION FORM Date: Name: Last First Initial Date of Birth SS # - - Age: Dominant Hand: Right Left Height: Weight:
 NUMBNESS EVALUATION FORM Date: Name: Last First Initial Date of Birth SS # - - Age: Dominant Hand: Right Left Height: Weight: I Referring Doctor Complete Name of Referring Doctor Last Complete Address
NUMBNESS EVALUATION FORM Date: Name: Last First Initial Date of Birth SS # - - Age: Dominant Hand: Right Left Height: Weight: I Referring Doctor Complete Name of Referring Doctor Last Complete Address
Patient # (assigned by office) Full Name: Social Security # Address: City: State: Zip: address: Home Phone Cell Phone:
 Full Name: Social Security # Address: City: State: Zip: address: Home Phone Cell Phone:") We appreciate the opportunity to help you get back to the health. The more accurate and complete the information you give us, the better service we can give you. Date: Patient # (assigned by office) Full
We appreciate the opportunity to help you get back to the health. The more accurate and complete the information you give us, the better service we can give you. Date: Patient # (assigned by office) Full