Specialty Care National Program
|
|
|
- Domenic Greene
- 5 years ago
- Views:
Transcription

1 Specialty Care National Program Mini-Residency Pain Management February 10-12, 2015 Myofascial Techniques for Back and Neck Pain Presented by: Edward S. Lee MD National Program Faculty: Edward S. Lee MD Director, Interdisciplinary Pain Rehabilitation Program VA Pittsburgh Healthcare System Part 1
2 Disclosures Instructor, Medical Acupuncture for Physicians Course, Helms Medical Institute
3 Learning Objectives Know the differences between Myofascial Pain Syndrome (MPS) and Fibromyalgia (FM). Understand the anatomy and pathophysiology of myofascial pain. Appreciate the importance of diagnosing and managing MPS. Develop clinical skills in treating MPS. Utilize a multimodal, integrative, interdisciplinary approach to pain management.
4 Myofascial Pain Syndrome (MPS) Regional soft tissue pain commonly involving the neck, shoulders, trunk, arms, low back, hips and lower extremities Painful muscle dysfunction in one or several muscles in a region of the body with loss of range of motion Trigger points Central sensitization hypersensitivity, allodynia Referred pain Described as burning, stabbing, aching, nagging
5 Fibromyalgia (FM) Systemic somatic condition Widespread musculoskeletal tenderness and pain Tender points, may coincide with trigger points Central sensitization and augmentation Not excluded by Myofascial Pain Syndrome
6 FM Diagnostic Criteria, ACR 2010 Widespread Pain Index 7 and Symptom Severity scale score 5 OR Widespread Pain Index of 3-6 and Symptom Severity scale score 9
7 FM Widespread Pain Index Bilateral sites (total of 14) Jaw Shoulder Upper arm Lower arm Hips Upper leg Lower leg Unilateral sites (total of 5) Neck Upper back Chest/breast Abdomen Lower back
8 FM Symptom Severity Scale Fatigue, Cognitive Difficulties, and Sleep Disturbances Score each domain: 0 = No problem 1 = Slight or mild problems; generally mild or intermittent 2 = Moderate; considerable problems; often present and/or at a moderate level 3 = Severe: pervasive, continuous, life disturbing problems Somatic Symptoms 0 = 0 symptoms 1 = 1 to 10 2 = 11 to 24 3 = 25 or more
9 Muscle pain Irritable bowel syndrome Thinking or remembering problems Muscle weakness Headache Pain/cramps in the abdomen Numbness/tingling Dizziness Depression Constipation Pain in the upper abdomen Nausea Nervousness Somatic Symptoms Chest pain Blurred vision Fever Diarrhea Dry mouth Itching Wheezing Raynaud's phenomenon Hives/welts Ringing in ears Vomiting Heartburn Oral ulcers Loss of/change in taste Seizures Dry eyes Shortness of breath Loss of appetite Hair loss Frequent urination Painful urination Bladder spasms Rash Sun sensitivity Hearing difficulties Easy bruising Hair loss Frequent urination Painful urination Bladder spasm
10 Comorbid Conditions Found with Both FM and MPS Migraine headache Tension-type headache Temporomandibular joint disorder Hypermobility syndromes Painful bladder syndrome Irritable bowel syndrome Pelvic pain syndrome Vulvovaginitis Prostatitis Endometriosis Dysmenorrhea Hypothyroidism check TSH
11 Conditions More Commonly Associated with MPS Malabsorption Vitamin D deficiency Vitamin B12 deficiency Iron deficiency Parasitic infection Check stools x3 for O&P if significant GI symptoms Celiac disease Candida overgrowth
12 MPS: Epidemiology Prevalence up to 95% in patients with chronic pain disorders Overall prevalence: 37% of middle-aged men (30-60 years) 65% of middle-aged women 85% of elderly (>65 years) Costs up to $47 billion/year
13 MPS History Clinical studies of trigger points conducted by four separate investigators in the 1930 s and 40 s J. H. Kellgren at University College Hospital, London Hypertonic saline injection in healthy volunteers gave rise to zones of referred extremity pain. Michael Gutstein in Berlin Michael Kelly in Australia Janet G. Travell in New York Trigger point research and treatment of John F. Kennedy's back pain led to her becoming the first female Personal Physician to the President.
14 Osteopathic Medicine Founded by A.T. Still, Civil War surgeon, at a time when allopathic medicine had few safe and effective treatments. Holistic approach to health, on the premise that the body s capacity to heal can be optimized by assessing and manipulating the musculoskeletal system. Identified musculoskeletal pain and dysfunction as a manifestation of general health. Still and his successors developed numerous approaches for somatic dysfunction, including myofascial pain syndrome.
15 Myofascial Pain Syndrome: Etiology Often presents after an injury or with occupational repetitive activity/overuse. TrPs may develop when muscle use exceeds muscle capacity and normal recovery is disturbed. Local muscle metabolic stress may produce energy crisis. Dehydration may precipitate myofascial dysfunction Fascia plays central role. Shortened muscles lead to enthesopathy, tendonitis, postural changes, limited range of motion and limited flexibility, ie somatic dysfunction.

16 Myofascial Trigger Point Pathophysiology Fascial injury: tightness, restriction, compression, disruption, due to edema, hematoma, inflammation, tear etc. Adapted from Simons model of myofascial pain syndrome
17 Anatomy Revisited Musculoskeletal system is not simply a system of pulleys and levers. Bones are living, dynamic compressive elements that float in a sea of soft tissue. Muscles are incompressible, fluid-filled, contractile elements found in pockets of fascia, attached to bones via connective tissues.
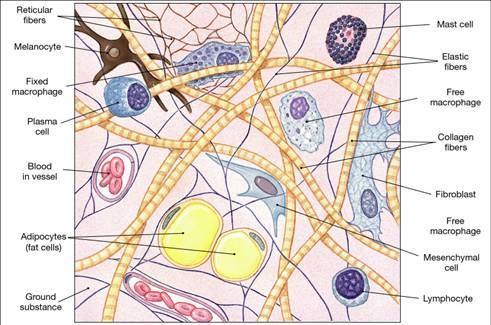
18 Fascia Originates from embryonic mesodermal mesenchymal cells. Is a continuous network of living, dynamic connective tissue that surrounds, connects, and penetrates every organ and structure in the body. Is populated by fibroblasts, as well as adipocytes, reticulocytes and other immune cells. Is richly innervated. Imparts tensile strength. Is the target of manual therapies, including acupuncture.

19




20 Dr. Jean Claude Guimberteau: Strolling Under the Skin

21 Tensegrity Buckminster Fuller Tension + Integrity Global balance between compression and tension

22 Artifact vs. Reality
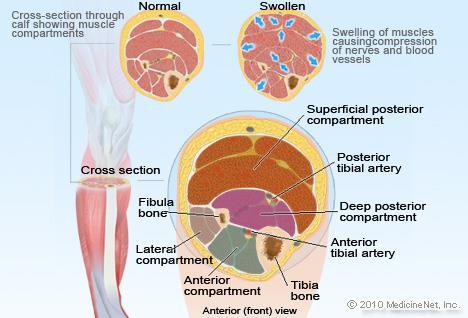
23 Compartment Syndrome

24 Mechanotransduction in Fibroblasts Integrin family Link between ECM and cell interior Physical and informational Triggers gene expression Regulates protein synthesis Changes extracellular matrix composition Change in connective tissue around nerve terminals Cytoskeletal reorganization

25 Mechanotransduction Stretch fibroblast, focal adhesions serve as force sensors, Rho signals a remodel message to relax itself Cytoskeletal remodeling, influences connective tissue tension Prevent with Colchicine

 Inhibited in animal models by injection of collagenase.")
26 Acupuncture affects fibroblasts several cm. away Reorganize their cytoskeleton, change shape Become larger and flatter Similar with sustained stretch(30 min.) Inhibited in animal models by injection of collagenase. Mechanotransduction

27 Fibroblast Response to Injury Production of collagen and ECM Matrix degrading enzymes when chronic Fibroblast myofibroblast Chronic; excess collagen, tissue tension, fibrosis


28 Wound Healing and Fibrosis
 have thicker connective")

29 Connective Tissue Fibrosis Patients with chronic low back pain (LBP) have thicker connective tissues. Usually dense and areolar tissue alternate, allowing lamellar gliding. LBP has decreased gliding.

30 Sensory Innervation of Fascia Connective tissues have sensory innervation, including pain afferents that respond to stretch of inflamed connective tissue.
31 Trigger Points Palpable muscle nodules, characterized by shortened sarcomeres. Found within taut bands of muscle. Associated with tenderness that reproduces patient s pain. Typically causes referred pain in a predictable distribution. Twitch response elicited with palpation or needling the affected muscle; variable, low inter-rater reliability.

32 Taut Band and Trigger Point
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital
 Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Fibromyalgia. November 3, 2018 Raymond Hong, MD, MBA
 Fibromyalgia November 3, 2018 Raymond Hong, MD, MBA The following report is proprietary information and constitutes trade secrets of The MetroHealth System and may not be disclosed in whole or part to
Fibromyalgia November 3, 2018 Raymond Hong, MD, MBA The following report is proprietary information and constitutes trade secrets of The MetroHealth System and may not be disclosed in whole or part to
HISTORY OF PRESENT ILLNESS A. TELL US ABOUT YOUR PAIN PROBLEM
 1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
1 UT Health Austin Comprehensive Pain Management New Patient Questionnaire Thank you for scheduling a visit with the Comprehensive Pain Management Care Team. The responses you provide to these questions
Emotional Relationships Social Life Sexually Recreation
 Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Manual Therapy Techniques
 Manual Therapy Techniques manual therapy: the use of hands-on techniques to evaluate, treat, and improve the status of neuromusculoskeletal conditions massage: the systematic and scientific manipulation
Manual Therapy Techniques manual therapy: the use of hands-on techniques to evaluate, treat, and improve the status of neuromusculoskeletal conditions massage: the systematic and scientific manipulation
New Patient Pain Evaluation
 New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
New Patient Pain Evaluation Name: Date: Using the following symbols, mark the areas of the body diagrams which are affected by your pain: \\ = Stabbing * = Electrical X = Aching N = Numbness 0 = Dull S
Chiropractic Applied Kinesiology Vitamins Herbs Homeopathy Health Education Classes PATIENT REGISTRATION
 Chiropractic Applied Kinesiology Vitamins Herbs Homeopathy Health Education Classes PATIENT REGISTRATION Name Date Address City State Zip Home Phone Cell Phone # Work: Email Address Occupation Employer
Chiropractic Applied Kinesiology Vitamins Herbs Homeopathy Health Education Classes PATIENT REGISTRATION Name Date Address City State Zip Home Phone Cell Phone # Work: Email Address Occupation Employer
ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION. Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security #: - -
 ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security : - - Home Address: City, State, Zip: Home Phone: ( ) Work Phone:
ABUNDANT HEALTH CHIROPRACTIC New Patient Form PERSONAL INFORMATION Name: Gender: M F Today's Date: / / Birth Date: / / Age: Social Security : - - Home Address: City, State, Zip: Home Phone: ( ) Work Phone:
Acupuncture & Myofascial Pain
 Acupuncture & Myofascial Pain Uncovering the Central Map of Physiological Homeostasis Joseph F. Audette, M.A., M.D. Spaulding Rehabilitation Hospital Department of PM&R, Harvard Medical School INTRODUCTION
Acupuncture & Myofascial Pain Uncovering the Central Map of Physiological Homeostasis Joseph F. Audette, M.A., M.D. Spaulding Rehabilitation Hospital Department of PM&R, Harvard Medical School INTRODUCTION
Amarillo Surgical Group Doctor: Date:
 Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop.
, by mouth, or as an eye drop.") Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Extended Health Care Company Do you need any help retaining information about your health insurance coverage? Yes No
 PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
PATIENT ENTRANCE FORM Date Circle: Male Female Name Birth Date (dd/mm/yy) Age Address Apt # City Province Postal Code Home # Cell # Work # E-MAIL Occupation Employer Name of Emergency Contact Contact #
CONSULTATION ADMITTANCE FORM
 CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
Pain Management Questionnaire
 In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
In order to make the most of your visit, we require this form to be completed to the best of your ability and sent to the Pain Management Clinic a copy should be shared with your Primary Care Provider
RHEUMATOLOGY PATIENT HISTORY FORM
 !! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
!! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
Post-op / Pre-op Page (ALREADY DONE)
") Post-op / Pre-op Page (ALREADY DONE) We offer individualized treatment plans based on your physician's recommendations, our evaluations, and your feedback. Most post-operative and preoperative rehabilitation
Post-op / Pre-op Page (ALREADY DONE) We offer individualized treatment plans based on your physician's recommendations, our evaluations, and your feedback. Most post-operative and preoperative rehabilitation
New Patient Specialty Intake Form Department of Surgery
 This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
Personal &Work Information Date: Patient Name: Age: City: State: Zip: Primary Care Physician: PCP Phone:
 Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Please fill out the following form in as much detail as possible. Please Print. Name. Address. City State Zip. Home Phone Office Phone.
 CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
Patient Health History Questionnaire
 Patient Health History Questionnaire Manitou Springs Acupuncture Randall Johnson, L.Ac., LLC Certified Seitai Shinpo Acupuncturist License Number: Acu-0002072 Phone: (719) 237-4547 Email: 719acupuncture@gmail.com
Patient Health History Questionnaire Manitou Springs Acupuncture Randall Johnson, L.Ac., LLC Certified Seitai Shinpo Acupuncturist License Number: Acu-0002072 Phone: (719) 237-4547 Email: 719acupuncture@gmail.com
Name: Date: Street Address: Referring Physician: How long have you had your current problem?
 3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
3851 Piper Street, Suite U464 Anchorage, AK 99508 p 907.339.4800 f 907.339.4801 New Patient Health Questionnaire Name: Date: Street Address: City: State Zip Sex: Age: Birth Date: Insurance: SS# Home Phone:
Symptom Review (page 1) Name Date
 Name Date") v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
Medical History Form
 General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
OU Children s Physicians Pediatric Arthritis Center
 Please complete the following questionnaire for your child: Patient Name: Birth Date: Parent/Caretaker Name: Primary Care Physician (Full Name, City, & State) Mother s Occupation: Fathers Occupation: Name
Please complete the following questionnaire for your child: Patient Name: Birth Date: Parent/Caretaker Name: Primary Care Physician (Full Name, City, & State) Mother s Occupation: Fathers Occupation: Name
Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire
 Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire First Name: M.I. Last Name: Date of Birth: Phone: Marital Status: Married Divorced Separated Widowed Single Work Status: Employed
Emory Clinic Department of Neurological Surgery Second Opinion Questionnaire First Name: M.I. Last Name: Date of Birth: Phone: Marital Status: Married Divorced Separated Widowed Single Work Status: Employed
Interventional Pain Medicine. P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C
 Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
Interventional Pain Medicine P. Tennent Slack, M.D. Dr. Greg Jackson, M.D. Ben Fleming, PA-C Gainesville Braselton Medical Park 1, Suite 300 Medical Plaza B, Suite 402 1315 Jesse Jewell Parkway 1404 River
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET
 SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
SECTION OF NEUROSURGERY PATIENT INFORMATION SHEET EC#: (for office use only) Patient s Name: Today s Date: Age: Date of Birth: Height: Weight: Physician you are seeing today: Marital Status: Married Work
725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA (770) (770) (facsimile)
 (770) (facsimile)") Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
Inner Balance Acupuncture
 Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
NEW PATIENT INFORMATION FORM
 NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
NEW PATIENT INFORMATION FORM Name: LAST FIRST MIDDLE Date of Birth: Sex: Marital Status: SS Number: Address: City: State: Zip Phone: Home Cell Work Email: Communication Preference: Patient Portal Phone
PRODUCT MONOGRAPH. FLOCTAFENINE Floctafenine Tablets 200 mg and 400 mg THERAPEUTIC CLASSIFICATION. Anti-inflammatory, Analgesic
 0 PRODUCT MONOGRAPH FLOCTAFENINE Floctafenine Tablets 200 mg and 400 mg THERAPEUTIC CLASSIFICATION Anti-inflammatory, Analgesic INFORMATION FOR THE PATIENT FLOCTAFENINE, which has been prescribed to you
0 PRODUCT MONOGRAPH FLOCTAFENINE Floctafenine Tablets 200 mg and 400 mg THERAPEUTIC CLASSIFICATION Anti-inflammatory, Analgesic INFORMATION FOR THE PATIENT FLOCTAFENINE, which has been prescribed to you
+ Color Change - + Hearing Loss - + Apnea - + Enuresis (urine - + Tremors - + Rash -
 Review of Systems: 0-1 year old Constitution neg Eyes neg GI neg Neurological neg + Activity Change - + Eye Discharge - + Reflux - + Facial Asymmetry - + Appetite Change - + Eye Redness - + Vomiting -
Review of Systems: 0-1 year old Constitution neg Eyes neg GI neg Neurological neg + Activity Change - + Eye Discharge - + Reflux - + Facial Asymmetry - + Appetite Change - + Eye Redness - + Vomiting -
MYOFASCIAL PAIN. Dr. Janet Travell ( ) credited with bringing MTrPs to the attention of healthcare providers.
 credited with bringing MTrPs to the attention of healthcare providers.") Myofascial Trigger Points background info Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT History lesson Dr. Janet Travell (1901 1997) credited with bringing MTrPs to the attention of healthcare
Myofascial Trigger Points background info Laurie Edge-Hughes BScPT, MAnimSt (Animal Physio), CAFCI, CCRT History lesson Dr. Janet Travell (1901 1997) credited with bringing MTrPs to the attention of healthcare
Trigger Point Injections TRIGGER POINT INJECTIONS HS-184. Policy Number: HS-184. Original Effective Date: 7/1/2010
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
GUPTA SPORTS & SPINE CENTER
 GUPTA SPORTS & SPINE CENTER NEW PATIENT INFORMATION FORM -ORTHO Please print all information. Thank you for your cooperation. Patient Name: Date of Birth: _ Social Security # Address: City: _ State: Zip
GUPTA SPORTS & SPINE CENTER NEW PATIENT INFORMATION FORM -ORTHO Please print all information. Thank you for your cooperation. Patient Name: Date of Birth: _ Social Security # Address: City: _ State: Zip
Specialty Care National Program
 Specialty Care National Program Mini-Residency Pain Management February 10-12, 2015 Myofascial Techniques for Back and Neck Pain Presented by: Edward S. Lee MD National Program Faculty: Edward S. Lee MD
Specialty Care National Program Mini-Residency Pain Management February 10-12, 2015 Myofascial Techniques for Back and Neck Pain Presented by: Edward S. Lee MD National Program Faculty: Edward S. Lee MD
Athens Rheumatology Clinic, LLC Sana Makhdumi, MD
 Athens Rheumatology Clinic, LLC Sana Makhdumi, MD Phone: 706-850-8322 Fax: 706-850-8322 PATIENT HISTORY FORM Date of first appointment: / / Time of appointment: Birthdate: Name LAST FIRST MIDDLE INITIAL
Athens Rheumatology Clinic, LLC Sana Makhdumi, MD Phone: 706-850-8322 Fax: 706-850-8322 PATIENT HISTORY FORM Date of first appointment: / / Time of appointment: Birthdate: Name LAST FIRST MIDDLE INITIAL
CECILIA P MARGRET MD PhD MPH Child, Adolescent and Adult Psychiatry NE 24th ST Suite 104, Bellevue WA 98007, Phone / Fax: +1 (425)
") IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
Silver Child Development Center New Patient Questionnaire. Relation (circle) Biological Mother Stepmother Adoptive Mother
 Biological Mother Stepmother Adoptive Mother") Silver Child Development Center New Patient Questionnaire Today s Date Mother s Name First Last Date of Birth Relation (circle) Biological Mother Stepmother Adoptive Mother Foster Mother Other Father s
Silver Child Development Center New Patient Questionnaire Today s Date Mother s Name First Last Date of Birth Relation (circle) Biological Mother Stepmother Adoptive Mother Foster Mother Other Father s
Bend Surgical Associates. Michael J. Mastrangelo, MD, FACS. Medication Name Dosage Frequency Medication Name Dosage Frequency
 Bend Surgical Associates Michael J. Mastrangelo, MD, FACS PATIENT NAME: DATE F BIRTH: MEDICATINS Please list all of your current prescription, non-prescription medications, vitamins, minerals, and supplements.
Bend Surgical Associates Michael J. Mastrangelo, MD, FACS PATIENT NAME: DATE F BIRTH: MEDICATINS Please list all of your current prescription, non-prescription medications, vitamins, minerals, and supplements.
Alivia Acupuncture Clinic, LLC. Address. City State Zip. . Occupation Employer. Emergency contact Relationship. Primary Care provider Phone
 Alivia Acupuncture Clinic, LLC Karla Sourasky Olmos, L. Ac Patient Information Name Age Date of birth Address City State Zip Email Home Phone Work phone Cell Phone Marital Status Single Married Divorced
Alivia Acupuncture Clinic, LLC Karla Sourasky Olmos, L. Ac Patient Information Name Age Date of birth Address City State Zip Email Home Phone Work phone Cell Phone Marital Status Single Married Divorced
Pathway for management of chronic widespread pain Diagnosis of fibromyalgia 8
 Pathway for management of chronic widespread pain Diagnosis of fibromyalgia 8 A patient satisfies diagnostic criteria for fibromyalgia if the following 3 conditions are met: 1. Widespread pain index (WPI)
Pathway for management of chronic widespread pain Diagnosis of fibromyalgia 8 A patient satisfies diagnostic criteria for fibromyalgia if the following 3 conditions are met: 1. Widespread pain index (WPI)
New Patient Intake Form
 New Patient Intake Form Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name _ Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
New Patient Intake Form Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name _ Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
Laser Vein Center Thomas Wright MD RVT Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): address: Occupation: Who referred you/how did you hear about us?
 (evening): (cell): address: Occupation: Who referred you/how did you hear about us?") Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): Email address: Occupation: Who referred you/how did you hear about us? Your primary health care provider: Phone: Emergency
Name: Date of birth: Address: City: State: Zip: Phone: (day) (evening): (cell): Email address: Occupation: Who referred you/how did you hear about us? Your primary health care provider: Phone: Emergency
Medical Information. (office use) MRN: CMRN: Last Name: First Name: Middle Initial: Date of birth: Age: Sex: M F Height: Weight:
 MRN: CMRN: Last Name: First Name: Middle Initial: Date of birth: Age: Sex: M F Height: Weight:") 1835 W. County Rd C, Suite 80, Roseville, MN 55113 P: 651-797-6880 F: 651-797-6881 info@spartzvein.com spartzvein.com Medical Information Date of consultation: (office use) MRN: CMRN: Last Name: First
1835 W. County Rd C, Suite 80, Roseville, MN 55113 P: 651-797-6880 F: 651-797-6881 info@spartzvein.com spartzvein.com Medical Information Date of consultation: (office use) MRN: CMRN: Last Name: First
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
Pain Differential Diagnosis - Enrico Dellacà M.D Ph.D. Extensor digitorum brevis muscle of the foot Myofascial Pain Syndrome
 Overview Extensor digitorum brevis muscle of the foot Myofascial Pain Syndrome Definition Pain Differential Diagnosis - Enrico Dellacà M.D Ph.D. Pain Differential Diagnosis - Enrico Dellacà M.D Ph.D. The
Overview Extensor digitorum brevis muscle of the foot Myofascial Pain Syndrome Definition Pain Differential Diagnosis - Enrico Dellacà M.D Ph.D. Pain Differential Diagnosis - Enrico Dellacà M.D Ph.D. The
Where is your pain located? Please use the diagram below to indicate where most of your pain is located.
 Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
The information you provide us will greatly help us provide the highest quality and most comprehensive care for you.
 Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information
Rheumatology (circle location of appointment) 111 Hundertmark Rd. Suite 115N 560 S. Maple St. Suite 400 place patient label here Chaska, MN 55318 Waconia, MN 55387 952-361-2450 952-361-2450 The information
NEW PATIENT HEALTH HISTORY
 NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
stoneburner acupuncture
 STONEBURNER ACUPUNCTURE, LLC Erin K. Stoneburner, LAc, MAcOM 1135 SE Salmon St, Suite 211 503.784.1660 stoneburner@gmail.com Date: Name: (First) (Middle) (Last) DOB: _ Age: Sex: Address: City/State: ZIP:
STONEBURNER ACUPUNCTURE, LLC Erin K. Stoneburner, LAc, MAcOM 1135 SE Salmon St, Suite 211 503.784.1660 stoneburner@gmail.com Date: Name: (First) (Middle) (Last) DOB: _ Age: Sex: Address: City/State: ZIP:
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History
 Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
TRIGGER POINT DRY NEEDLING
 TRIGGER POINT DRY NEEDLING Sadie Newman PT DPT Cox Health What is it? 1 A skilled intervention that uses a thin filiform needle to penetrate the skin and stimulate underlying myofascial trigger points,
TRIGGER POINT DRY NEEDLING Sadie Newman PT DPT Cox Health What is it? 1 A skilled intervention that uses a thin filiform needle to penetrate the skin and stimulate underlying myofascial trigger points,
COMPREHENSIVE HEALTH & WELLNESS PROFILE
 Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
For the Patient: USMAVNIV
 For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
Scottsdale Family Health
 Please list pharmacy you would like us to use for your medications. Pharmacy Phone Number Fax Number Since your last visit: 1. Have you been diagnosed with any new medical conditions? Yes No If Yes (give
Please list pharmacy you would like us to use for your medications. Pharmacy Phone Number Fax Number Since your last visit: 1. Have you been diagnosed with any new medical conditions? Yes No If Yes (give
Address City State Zip. Home Phone Cell Work. (For SHPT use only) Emergency Contact Phone
 Emergency Contact Phone") Somerset Hills Physical Therapy, PC 180 Mount Airy Road, Suite 103 Basking Ridge, NJ 07920 Phone (908) 766-1407 Fax (908) 953-8454 wwwsomersethillsptcom Patient Information: Name Sex M F Date of Birth
Somerset Hills Physical Therapy, PC 180 Mount Airy Road, Suite 103 Basking Ridge, NJ 07920 Phone (908) 766-1407 Fax (908) 953-8454 wwwsomersethillsptcom Patient Information: Name Sex M F Date of Birth
T- Timing- concise vs. complete and thorough, depending on need of presenter and audience. E- Elicit- ask for feedback- more information needed? Less?
 Review of STAGE presentation framework (from umass.macy.edu, revised Alicia Monroe, MD from 2005 STFM) S- style organization, sequencing adequate to build a case for your diagnosis or a story T- Timing-
Review of STAGE presentation framework (from umass.macy.edu, revised Alicia Monroe, MD from 2005 STFM) S- style organization, sequencing adequate to build a case for your diagnosis or a story T- Timing-
This Session by Simon Strauss
 This Session by Simon Strauss Myofascial Pain. Part A Myofascial Pain. Part B Pain Assessment Tools. Part C Definitions and Language of Pain Allodynia- 1. A lower than normal pain threshold. 2. A clinical
This Session by Simon Strauss Myofascial Pain. Part A Myofascial Pain. Part B Pain Assessment Tools. Part C Definitions and Language of Pain Allodynia- 1. A lower than normal pain threshold. 2. A clinical
Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?
![Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?](/thumbs/87/97078208.jpg "Name: [Type text] Date of Birth: ENDOCRINOLOGY HEALTH HISTORY. What is the reason for your visit?") ENDOCRINOLOGY HEALTH HISTORY What is the reason for your visit? MEDICATIONS List current prescription and over-the-counter medications. Also list current vitamin, herbal, and nutritional supplements: MEDICATION/SUPPLEMENT
ENDOCRINOLOGY HEALTH HISTORY What is the reason for your visit? MEDICATIONS List current prescription and over-the-counter medications. Also list current vitamin, herbal, and nutritional supplements: MEDICATION/SUPPLEMENT
NEW PATIENT HEALTH HISTORY
 NEW PATIENT HEALTH HISTORY Patient Name Today s Date Age Birth Date Date of last physical examination What is your reason for initial visit? Pharmacy Name & Telephone # NOTE: If you have prior records
NEW PATIENT HEALTH HISTORY Patient Name Today s Date Age Birth Date Date of last physical examination What is your reason for initial visit? Pharmacy Name & Telephone # NOTE: If you have prior records
The New Mexico Refugee Symptom Checklist-121 (NMRSCL-121)
") The New Mexico Refugee Symptom Checklist-121 (NMRSCL-121) Michael Hollifield, MD 2007 New Mexico Refugee Symptom Checklist-121 Instructions: Using the scale beside each symptom, please indicate the degree
The New Mexico Refugee Symptom Checklist-121 (NMRSCL-121) Michael Hollifield, MD 2007 New Mexico Refugee Symptom Checklist-121 Instructions: Using the scale beside each symptom, please indicate the degree
Coastal Digestive Diseases, P.C. MA New Pt Ht
 Coastal Digestive Diseases, P.C. MA New Pt Ht Interview Form Limited Use Only Estab Pt Wt Name Nickname DOB Address Occupation Social Security # Married Single Email Address: Divorced Widowed Check Contact
Coastal Digestive Diseases, P.C. MA New Pt Ht Interview Form Limited Use Only Estab Pt Wt Name Nickname DOB Address Occupation Social Security # Married Single Email Address: Divorced Widowed Check Contact
For the Patient: Fludarabine injection Other names: FLUDARA
 For the Patient: Fludarabine injection Other names: FLUDARA Fludarabine (floo-dare-a-been) is a drug that is used to treat many types of cancer. It is a clear liquid that is injected into a vein. Tell
For the Patient: Fludarabine injection Other names: FLUDARA Fludarabine (floo-dare-a-been) is a drug that is used to treat many types of cancer. It is a clear liquid that is injected into a vein. Tell
Other physician #1. #(p) List any allergies to medications. Please list below all other current medical conditions or previous surgeries
 List any allergies to medications. Please list below all other current medical conditions or previous surgeries") Dept. of Obstetrics and Gynecology Division of Gynecological Pain and Minimally Invasive Surgery Frank Tu, MD, MPH Sangeeta Senapati, MD, MS Howard Topel, MD Name: New Patient Intake Questionnaire Names
Dept. of Obstetrics and Gynecology Division of Gynecological Pain and Minimally Invasive Surgery Frank Tu, MD, MPH Sangeeta Senapati, MD, MS Howard Topel, MD Name: New Patient Intake Questionnaire Names
For the Patient: ULUAVPMB
 For the Patient: ULUAVPMB Other Names: Treatment of Advanced Non-Small Cell Lung Cancer Using Pembrolizumab U = Undesignated (requires special approval) LU = LUng AV = AdVanced PMB = PeMBrolizumab ABOUT
For the Patient: ULUAVPMB Other Names: Treatment of Advanced Non-Small Cell Lung Cancer Using Pembrolizumab U = Undesignated (requires special approval) LU = LUng AV = AdVanced PMB = PeMBrolizumab ABOUT
Chiropractic Glossary
 Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Patient Intake Form for Acupuncture Treatment at Infinite Healing
 Section A: Your Information Patient Intake Form for Acupuncture Treatment at Infinite Healing Last Name: First Name: Middle Initial: Mailing Address: _ City: Postal Code: E-mail: Birth date: M D YR Age:
Section A: Your Information Patient Intake Form for Acupuncture Treatment at Infinite Healing Last Name: First Name: Middle Initial: Mailing Address: _ City: Postal Code: E-mail: Birth date: M D YR Age:
2. Have your symptoms affected your ability to carry out your daily activities? YES NO
 QUESTIONNAIRE Page 1 of 5 Date: Referring MD (Name, Address, Phone Number): Primary Care Physician (Name and Address, Phone Number): Reason for visit: 1. How long have you had symptoms? Describe your symptoms?
QUESTIONNAIRE Page 1 of 5 Date: Referring MD (Name, Address, Phone Number): Primary Care Physician (Name and Address, Phone Number): Reason for visit: 1. How long have you had symptoms? Describe your symptoms?
Address: Yes! I would like to receive your Monday Morning Health Tips.
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
What is your occupation? Company Name Do you have extended healthcare benefits? Yes No Benefits are personal or from work
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Patient Interview Form
 Page 1 of 5 Patient Interview Form Patient Information First Name: MRN: Last Name: Date Of Birth: Contact Preference Email Telephone call- Work Telephone call - Home Email Please check one as your preferred
Page 1 of 5 Patient Interview Form Patient Information First Name: MRN: Last Name: Date Of Birth: Contact Preference Email Telephone call- Work Telephone call - Home Email Please check one as your preferred
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O.
 HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
HISTORY PAPERWORK FOR APPOINTMENTS WITH DAVID A. PROPST, D.O. Name: Age: Room Number: Sex: MALE or FEMALE Dominant Hand: RIGHT or LEFT Height Weight Blood pressure HISTORY 1. Did your first symptoms begin
Symptom Questionnaire
 Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
2. Approx. Date of Onset: 3. Approx. Date of Onset:
 Healthy Balance Lisa A. Dulac, L.Ac. Acupuncture Patient Intake Form Present Health Concerns: Please list your most important health concerns in order of their significance. 1. Approx. Date of Onset: 2.
Healthy Balance Lisa A. Dulac, L.Ac. Acupuncture Patient Intake Form Present Health Concerns: Please list your most important health concerns in order of their significance. 1. Approx. Date of Onset: 2.
NORTHWEST PROFESSIONAL OBSTETRICS & GYNECOLOGY, LTD. GYNECOLOGIC INTAKE AND HISTORY FORM
 NORTHWEST PROFESSIONAL OBSTETRICS & GYNECOLOGY, LTD. GYNECOLOGIC INTAKE AND HISTORY FORM Today s Date: Name: Date of Birth: Race: American Indian or Alaskan Native Asian Black or African-American More
NORTHWEST PROFESSIONAL OBSTETRICS & GYNECOLOGY, LTD. GYNECOLOGIC INTAKE AND HISTORY FORM Today s Date: Name: Date of Birth: Race: American Indian or Alaskan Native Asian Black or African-American More
Brisbin Family Chiropractic
 Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
Information reviewed with patient: Dr. Initials Today s Date Brisbin Family Chiropractic Name: Sex: Male Female Address: City: Postal Code: Home Ph# Work# Ext# Cell# Preferred number (circle one) Home
For the Patient: USMAVPEM
 For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
For the Patient: Cyclosporine injection Other names: SANDIMMUNE I.V.
 For the Patient: Cyclosporine injection Other names: SANDIMMUNE I.V. Cyclosporine (sye kloe spor een) is a drug that may be used to treat certain types of cancer. It may also be used to suppress your immune
For the Patient: Cyclosporine injection Other names: SANDIMMUNE I.V. Cyclosporine (sye kloe spor een) is a drug that may be used to treat certain types of cancer. It may also be used to suppress your immune
Myofascial Pain Syndrome and Trigger Points. Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine
 Myofascial Pain Syndrome and Trigger Points Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine Objectives Discuss why this topic is pertinent to our practices Review diagnostic criteria
Myofascial Pain Syndrome and Trigger Points Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine Objectives Discuss why this topic is pertinent to our practices Review diagnostic criteria
ABOUT YOU (Please print clearly) Name Birth Date Age Sex: Male Female Referring MD Mailing Address: Address
 Name Birth Date Age Sex: Male Female Referring MD Mailing Address: Address") ABOUT YOU (Please print clearly) Name Birth Date Age Sex: Male Female Referring MD Mailing Address: Address Home phone number MD Phone number Work number Any other MD you request we send information to?
ABOUT YOU (Please print clearly) Name Birth Date Age Sex: Male Female Referring MD Mailing Address: Address Home phone number MD Phone number Work number Any other MD you request we send information to?
Eastern Body Therapy
 2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
Mast Cell Activation Syndrome
 Mast Cell Activation Syndrome Clinical Questionnaire Description Today s Date: Patient Name: Please indicate yes or no for the following symptoms and traits: (If you are not familiar with a particular
Mast Cell Activation Syndrome Clinical Questionnaire Description Today s Date: Patient Name: Please indicate yes or no for the following symptoms and traits: (If you are not familiar with a particular
Bridges Family Wellness PC. New Patient Intake. Bridges Family Wellness Intake Form SE Lake Rd, Suite 102 Milwaukie, OR
 New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
HEALTH INFORMATION FORM
 #102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
#102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
Wisconsin Integrative Pain Specialists
 Patient Information Today s Date: Patient s Name: DOB: Age: Gender: Marital Status: M S D What would you like us to call you? Address: City, State, Zip: Home Phone: Cell Phone: Work Phone: Email: Preferred
Patient Information Today s Date: Patient s Name: DOB: Age: Gender: Marital Status: M S D What would you like us to call you? Address: City, State, Zip: Home Phone: Cell Phone: Work Phone: Email: Preferred
Trigger Point Injection. Objectives. What is a Trigger Point (TrP)? 3/19/2019
? 3/19/2019") Trigger Point Injection Brian Shian, MD, FHM Department of Family Medicine University of Iowa Hospitals and Clinics Objectives Discuss the definition and diagnosis criterial Explore possible pathophysiology
Trigger Point Injection Brian Shian, MD, FHM Department of Family Medicine University of Iowa Hospitals and Clinics Objectives Discuss the definition and diagnosis criterial Explore possible pathophysiology
Referring Physician/Therapist. Primary Care Physician. Reason for Visit
 Name Age Date Referring Physician/Therapist Primary Care Physician Reason for Visit If you are having pain, use the diagram and symbols to indicate where it is. Ache: AAA Burning:XXX Numbness:OOO Pins/Needles:
Name Age Date Referring Physician/Therapist Primary Care Physician Reason for Visit If you are having pain, use the diagram and symbols to indicate where it is. Ache: AAA Burning:XXX Numbness:OOO Pins/Needles:
Using Foam Rollers & various other tools. for self myofascial release
 Using Foam Rollers & various other tools for self myofascial release Why roll? reducing tone of overactive muscles via trigger point release MAY help reduce scar tissue, adhesions improve circulation increased
Using Foam Rollers & various other tools for self myofascial release Why roll? reducing tone of overactive muscles via trigger point release MAY help reduce scar tissue, adhesions improve circulation increased
Patient Name: Date: Address: Primary Care Physician: Online Website On TV In print On the radio
 927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
For the Patient: Bendamustine Other names: TREANDA
 For the Patient: Bendamustine Other names: TREANDA Bendamustine (ben'' da mus' teen) is a drug that is used to treat some types of cancer (lymphoma). It is a clear liquid that is injected into a vein.
For the Patient: Bendamustine Other names: TREANDA Bendamustine (ben'' da mus' teen) is a drug that is used to treat some types of cancer (lymphoma). It is a clear liquid that is injected into a vein.
Patient Information. Marital Status (Single, Married, Life Partner, Divorced, Widowed) CHIEF COMPLAINT
 CHIEF COMPLAINT") Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
WELCOME TO THE MILLER CHIROPRACTIC CLINIC
 WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
For the Patient: USMAVFIPI
 For the Patient: USMAVFIPI Other Names: First-Line Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced F =
For the Patient: USMAVFIPI Other Names: First-Line Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced F =
Adult Health Questionnaire
 Health for Life Chiropractic At Cloverdale Mall Unit #143-250 The East Mall Etobicoke, ON, M9B 3Y8 416-232-1822 416-232-0060 Dr. Chrystopher Sly B.Sc, D.C. Dr. Jesse Cracknell B.A., D.C. Adult Health Questionnaire
Health for Life Chiropractic At Cloverdale Mall Unit #143-250 The East Mall Etobicoke, ON, M9B 3Y8 416-232-1822 416-232-0060 Dr. Chrystopher Sly B.Sc, D.C. Dr. Jesse Cracknell B.A., D.C. Adult Health Questionnaire
NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE. Name (Last, First, M.I.) Address. City State Zip Code. Phone ( ) Work ( ) Cell ( )
 Address. City State Zip Code. Phone ( ) Work ( ) Cell ( )") NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE Date Name (Last, First, M.I.) Address City State Zip Code Phone ( ) Work ( ) Cell ( ) Date of Birth Age Marital Status SSN Employer Employer
NEW PATIENT REGISTRATION PLEASE COMPLETE ALL ITEMS ON EACH PAGE Date Name (Last, First, M.I.) Address City State Zip Code Phone ( ) Work ( ) Cell ( ) Date of Birth Age Marital Status SSN Employer Employer