PAIN CLINIC PATIENT INTAKE FORM
|
|
|
- Dwain McKinney
- 5 years ago
- Views:
Transcription
: Insurance Provider: As a professional courtesy, we would like to keep your primary care provider up to date regarding your injury or treatment.")
1 PAIN CLINIC PATIENT INTAKE FORM PAITNET INFORMATION Name: Date of Birth: Health Card# Version Code: Gender: Male Female Address: Home Phone: City: Postal Code: Cell Phone: Work Phone: Who is your primary care provider (Physician/NP, etc.): Insurance Provider: As a professional courtesy, we would like to keep your primary care provider up to date regarding your injury or treatment. Is it Ok to provide them with a consultation note and updates related to your injury?: YES NO Who may we contact in case of an emergency? Relationship: Phone 1: Phone 2: Please list below all individuals with whom we may talk to about your health concerns: Name: Relationship: Name: Relationship: Do you have any allergies? (Medications, foods, environmental) Are you currently taking any medications (prescription or over the counter, or supplements?) MEDICAL HISTORY Weight Loss / Gain Loss of Energy Unusual Fatigue Headaches Severe Migraine Dizziness or Fainting Decreased Hearing Ringing in Ears(s) Failing Vision Blurred or Double Vision Eye Pain Frequent Ear Infections Glaucoma Cataracts Sinus Pain Frequent Sore Throats Teeth/Gum Pain/Bleeding Hoarseness Chronic Cough Hay Fever Allergies Pneumonia / Pleurisy Bronchitis / Emphysema (COPD) Asthma / Wheezing Shortness of Breath Chest Pain or Tightness Heart Murmur Irregular Pulse Past and Present Medical History Palpitations High Cholesterol / Fat Swollen Ankles Calf Pain (while walking) Varicose Veins / Phlebitis Loss of Appetite (Recent) Difficulty Swallowing Indigestion or Heartburn Frequent Nose Bleeds Difficulty Sleeping Eczema Insomnia Peptic Ulcer Abdominal Pains Gall Bladder Troubles Jaundice / Hepatitis Change in Bowel Habits Diarrhea Constipation Bowel Polyps Crohn s or Colitis Hernia Hemorrhoids Frequent Urinary Tract Infections Anemia Urinary Painful, Bloody, No Control Decrease in force or flow of urine Kidney Stones
2 STD s / Genital Warts Urethral Discharge Circulatory Problems Bruise Easily Cancer (Type: ) Diabetes Excessive Thrust Thyroid Disease Seizures / Convulsions Stroke Tremor/Hands Shaking Muscle Weakness Numbness / Tingling Sensations Arthritis / Rheumatism Back Pain Frequent Bone Fracture/Joint Injury Gout Osteoporosis Foot Pain Cold/Numb Feet Rashes Hives Psoriasis Drug Abuse Depression Nervousness Memory Loss Phobias Moodiness Stress Excessive Mental Illness Chicken Pox Polio Mumps Measles Rheumatic Fever Tuberculosis Exposure to blood/bodily fluids Blood Transfusions Sexual Problems Women Only Last Menstrual Period (Date: ) Was the flow Regular, Irregular, Pain/Cramps Are you currently Pregnant: Yes No Number of Pregnancies: Number of Abortions: Number of Miscarriages: Number of Live Births: Are you currently on Birth Control Method: Date of last mammogram: History of Communicable Diseases? (I.e. HIV, Hep B, etc. Please specify: MEDICAL HISTORY CONTINUED Condition Glaucoma Thyroid Problems Hay Fever Asthma Anaemia Bleeds Easily Osteoporosis Stroke Diabetes Heart Disease Depression High/Low Blood Pressure Family Medical History (please specify relationship) High Cholesterol Alcoholism Genetic Disease Migraine Epilepsy Psoriasis Arthritis Mental Illness Eczema Cancer (Type) Atherosclerosis Other: Condition Habits and Health Access (please specify relationship) Do you Smoke Cigarettes? /day # Years Last Routine Physical (Date): Alcohol: Drinks/week: Last Blood Test (Date): Street Drugs: Last Urine Test (Date): Caffeine Drinks: Last Eye Exam (Date): Sleep Pattern: satisfactory occasionally disturbed Last Dental Exam (Date): Mostly disturbed Last Pap (Women) (Date): Last Prostate/Rectal(Date): Last Electrocardiogram (Date): Hospitalizations and Surgeries (Please indicate the year and reason not including normal pregnancies) Hospitalizations Surgeries Year Illness / Injury Year Illness / Injury

3 Date of Injury: Was this a workplace injury? YES NO WISB Claim? YES NO Claim# Please describe your injury/illness: Please describe how it happened: Has the injury got Better or Worse since it occurred On a Scale of 0-10, with 10 being the worst pain you have ever experienced, what would the pain on average be? Currently be? Would you describe the pain as: constant dull sharp throbbing tight burning tingling INJURY INFORRMATION Is there anything that makes it feel better? Is there anything that makes it feel worse? Have you received care from anyone yet for this injury? Has it helped? On the diagram, please mark with an X where the injury is, and where you are feeling the most pain. You may also mark on this diagram any pain that is radiating around by using the following: S = Sharp/Stabbing Pain B = Burning Pain N = Numbness P = Pins and Needles Check the words that best describe the pain Tingling Cramping Exausting Radiating Boring Continuous Sheeting Heavy Penetrating Stabbing Tender Nagging Burning Splitting Exerueiating Deep Piercing Unbearable Numb Aching Throbbing Laneinating Cutting Gnawing Teraing Sharp Are you doing anything to help with the pain? Warm Compress Cold Compress Relaxation Techniques Distraction Biofeedback Hypnosis
4 MEDICATION HISTORY Are you currently taking any pain medications? If so, how long does it take for the pain to return? List (name, dose and frequency) 1 hour 2 hours 3 hours 4 hours 5-12 hours More than 12 hours Do not take any pain medications I prefer to take pain medications: I take my pain medications (in a 24 hour period) On a regular basis Not every day Only when necessary 1-2 times a day I do not take pain medications 3-4 times a day 5-6 times a day 6+ times a day Do you feel you need a stronger type of pain Do you feel that you need to take more of the pain medication? medication then your provider prescribed? YES NO Why? Are you concerned that you use too much pain medication? YES NO Not Sure Why? Do you feel you need more information about your pain medication? YES NO Not Sure Is there something specific you are concerned about? YES NO Not Sure Why? Are you having any side effects caused by your pain medication YES NO Not Sure Explain: Is there anything you are taking/doing for pain that your provider has not provided you? PAIN INVENTORY 1. When does the pain usually begin? 2. How long does it usually last? 3. How often does it occur? Is there any side effects (depression, headaches, etc)? 4. Have you tried Chiropractic? Was it helpful? 5. Have you tried Physiotherapy? Was it helpful? 6. Have you had any x-rays, MRIs,etc yet? Is there anything else we should know about your injury/pain?

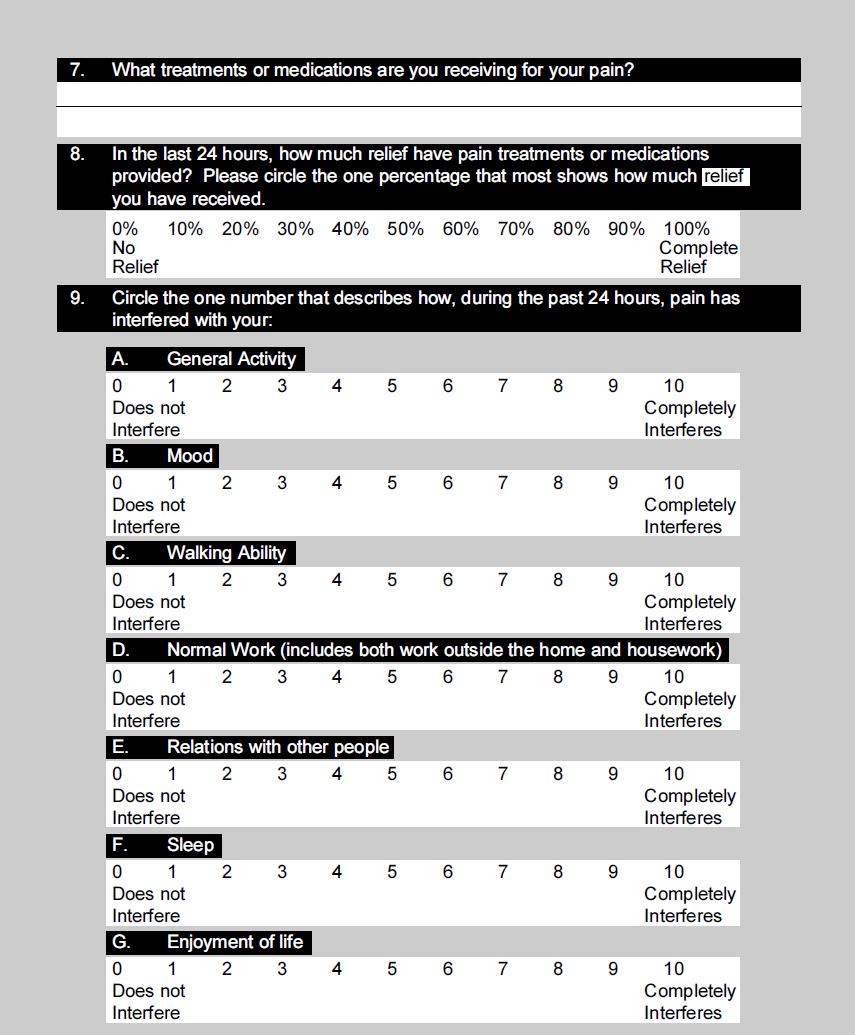
5 BRIEF PAIN INVENTORY
6
7 In this document I, my, me and you refer to the patient Health Care Provider refers to any clinician employed or student employed or under the fellowship of our clinicians with Algoma Sports Medicine and Physical Injuries Clinic Medical History and Consent to Assessment I certify that the information contained in this patient intake form is accurate, complete and true. I hereby request and consent to the performance of the required physical examinations and tests be completed in order to diagnose my condition. I understand that the health care provider will attempt to explain the procedures, and will attempt to provide appropriate privacy measures throughout the evaluation of my injury or illness. Treatment Consent CONSENT FORM Algoma Sports Medicines health care providers are trained to assess and treat many different conditions related to sports injuries. Our health care providers are trained in various manual and sports medicine techniques through various organizations in North America, and Europe as part of their medical training. This necessitates hands on techniques when diagnosing and treating various areas of the body. The treatment hypothesis and supportive research entails utilizing whole body muscle balance approach. The health care provider providing care for you will attempt to explain to you each time what they are doing, and you should advise the practitioner if there is any component of the examination or treatment that you are not comfortable with (i.e. feeling a muscle, ribs, body positioning, etc.). The use of manual therapy is a very safe and effective treatment for many sports injuries. There is a probable 1 to 3 in a million chance of catastrophic vascular problems (stroke) with cervical manipulation. The health care provider will inform you that they would like to perform cervical manipulation, and if you wish not to have this technique performed, please advise the health care provider. Manual therapy also carries a small probability of causing a compression fracture in the spine in predisposed individuals with spinal cancers, severe osteoporosis, bony problems, bleeding disorders, or severe degenerative diseases. All of the above can utilize very gentle manual therapy. The most common side effects are pain for a couple of days if the treatment is not aggressive, strain/sprain syndromes can also occur in 1% of cases. Privacy Consent This office may share my health information with other agencies/persons in accordance with current legislation and office policy. I also understand that if desired, someone can be in the room with me while being assessed and treated. Please note that the door may be open at all times during the history, physical or treatment. By signing below I understand that my consent may be withdrawn at any time, except for actions already taken, I release the health care provider providing any assessment or treatment, the facility, directors, officers, and successors from any liabilities, claims, and causes of action, known or unknown, contingent or fixed, that may result from the treatment and/or assessment. I agree not to file a lawsuit or other action to assert a claim. Signature: Date: Witness: Date:
CHRISTOPHER BROWN D.O. - TRADITIONAL OSTEOPATHY
 CHRISTOPHER BROWN D.O. - TRADITIONAL OSTEOPATHY REGISTRATION PAGE Date: Name: Tel: 510-526-5256 (Albany) 415-334-1010 (San Francisco) Fax: 510-526-5547 christopherbrowndo@gmail.com DOB: Age: Sex: Address:
CHRISTOPHER BROWN D.O. - TRADITIONAL OSTEOPATHY REGISTRATION PAGE Date: Name: Tel: 510-526-5256 (Albany) 415-334-1010 (San Francisco) Fax: 510-526-5547 christopherbrowndo@gmail.com DOB: Age: Sex: Address:
Our staff will need to make a photocopy of the following: Insurance Card (front and back) Driver's License or picture identification
 Driver's License or picture identification") Long Island Pulmonary and Sleep Medicine Associates, PLLC Louis Saffran, MD FCCP Frank S. Coletta, MD FCCP Karen Mrejen-Shakin, MD FCCP Aviva Kamath, MD FCCP Sepideh Sedgh DO 200 North Village Avenue Suite
Long Island Pulmonary and Sleep Medicine Associates, PLLC Louis Saffran, MD FCCP Frank S. Coletta, MD FCCP Karen Mrejen-Shakin, MD FCCP Aviva Kamath, MD FCCP Sepideh Sedgh DO 200 North Village Avenue Suite
DEPARTMENT OF MEDICINE Outpatient Intake Form
 NAME: Last First Middle Initial Date of Birth: ADDRESS: HOME PHONE: WORK PHONE: Did someone refer you here? Yes No If yes, please give name: Main reason for your visit today: MEDICAL HISTORY: (Please check
NAME: Last First Middle Initial Date of Birth: ADDRESS: HOME PHONE: WORK PHONE: Did someone refer you here? Yes No If yes, please give name: Main reason for your visit today: MEDICAL HISTORY: (Please check
Address: City: Postal Code: Emergency Contact: Phone# Relationship: Who may we thank for referring you to this office?
 CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
CLAYTON PARK CHIROPRACTIC CENTRE INC. Suite 11-117 Kearney Lake Road Halifax, Nova Scotia B3M 4N9 (902) 443-5669 phone (902) 443-9419 fax info@claytonparkchiro.ca For Office Use Only: Bilaterals L R PERSONAL
DEPARTMENT OF MEDICINE Outpatient Intake Form
 NAME: Last First Middle Initial Date of Birth: ADDRESS: HOME PHONE: WORK PHONE: Did someone refer you here? Yes No If yes, please give name: Main reason for your visit today: MEDICAL HISTORY: (Please check
NAME: Last First Middle Initial Date of Birth: ADDRESS: HOME PHONE: WORK PHONE: Did someone refer you here? Yes No If yes, please give name: Main reason for your visit today: MEDICAL HISTORY: (Please check
Personal &Work Information Date: Patient Name: Age: City: State: Zip: Primary Care Physician: PCP Phone:
 Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
Personal &Work Information Date: Patient Name: Age: Birth Date: / / Preferred Name: Gender: Home Phone: Address: Mobile Phone: City: State: Zip: Occupation: Employer: Work Phone: Email: Emergency Contact:
LAKES INTERNAL MEDICINE
 LAKES INTERNAL MEDICINE HEALTH HISTORY QUESTIONNAIRE Please print this and complete and bring to your initial appointment. Today's Date Last Name First Name Middle Initial Date of Birth Male Female Education
LAKES INTERNAL MEDICINE HEALTH HISTORY QUESTIONNAIRE Please print this and complete and bring to your initial appointment. Today's Date Last Name First Name Middle Initial Date of Birth Male Female Education
PATIENT INFORMATION Please print clearly and complete all blanks
 PATIENT INFORMATION Please print clearly and complete all blanks DATE: REFERRED BY: SEX: NAME: LAST FIRST MIDDLE BIRTHDATE: MAILING ADDRESS: CITY STATE ZIP TELEPHONE: CELL PHONE: WORK NUMBER: SS # MARITAL
PATIENT INFORMATION Please print clearly and complete all blanks DATE: REFERRED BY: SEX: NAME: LAST FIRST MIDDLE BIRTHDATE: MAILING ADDRESS: CITY STATE ZIP TELEPHONE: CELL PHONE: WORK NUMBER: SS # MARITAL
PATIENT INFORMATION FORM (WOMEN ONLY)
") PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
Laser Vein Center Thomas Wright MD Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
Demographics Laser Vein Center Thomas Wright MD Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Insurance Information Primary Insurance ID# Group# Subscriber
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
CASE HISTORY. Address: City: State: Zip: Date of Birth: Age: address: Occupation: Employer: Spouse's Employer: Referred by:
 CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
CASE HISTORY Account #: Please complete this form using your keyboard, then print it using the print function of your browser. You can then sign the form and bring it with you to your first appointment.
Laser Vein Center Thomas Wright MD RVT Page 1 of 4
 Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
Demographics Laser Vein Center Thomas Wright MD RVT Page 1 of 4 Patient Name: Address: City, St, Zip Primary Phone: Alternate: DOB: Social Security #: Marital Status: Married Single Other Emergency Contact:
Patient History Form
 Patient Personal Information Name: Date: Age: Occupation: Employer's name: Briefly describe your daily activities at work: Sex: male female Marital Status: single married divorced widowed Spouse's name:
Patient Personal Information Name: Date: Age: Occupation: Employer's name: Briefly describe your daily activities at work: Sex: male female Marital Status: single married divorced widowed Spouse's name:
INFORMATION/APPLICATION FOR CARE
 INFORMATION/APPLICATION FOR CARE The following information is needed in order to better serve you. Please complete all questions. If you need help please ask. Name Home Phone Work Phone Cell Phone E-Mail
INFORMATION/APPLICATION FOR CARE The following information is needed in order to better serve you. Please complete all questions. If you need help please ask. Name Home Phone Work Phone Cell Phone E-Mail
RHEUMATOLOGY PATIENT HISTORY FORM
 !! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
!! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
Personal Health Risk Appraisal
 Today s Date: Premier Arthritis and Osteoporosis Center 722 North Fairfield Road Beavercreek, OH 45434 Phone (937) 208-7000 Fax (937) 208-7010 Personal Health Risk Appraisal Last Name: First Name: MI:
Today s Date: Premier Arthritis and Osteoporosis Center 722 North Fairfield Road Beavercreek, OH 45434 Phone (937) 208-7000 Fax (937) 208-7010 Personal Health Risk Appraisal Last Name: First Name: MI:
Application For Admission Jersey Shore Low Back Center DRX 9000 Severe Back Pain Solution Program
 Application For Admission Jersey Shore Low Back Center DRX 9000 Severe Back Pain Solution Program If you are reading this you have been fortunate enough to qualify for a consultation with Dr. Zammito at
Application For Admission Jersey Shore Low Back Center DRX 9000 Severe Back Pain Solution Program If you are reading this you have been fortunate enough to qualify for a consultation with Dr. Zammito at
HIGH$ROCK$INTERNAL$MEDICINE,$PA$PATIENT$PAYMENT$POLICY!
 Patient HIGH$ROCK$INTERNAL$MEDICINE,$PA$PATIENT$PAYMENT$POLICY WelcometoHighRockInternalMedicine.Asapatientofours,westrivetoprovideyouwiththebest medicalcarepossibleatthelowestcost.thefollowinginformationwillhelpustodothis.ifyouhave
Patient HIGH$ROCK$INTERNAL$MEDICINE,$PA$PATIENT$PAYMENT$POLICY WelcometoHighRockInternalMedicine.Asapatientofours,westrivetoprovideyouwiththebest medicalcarepossibleatthelowestcost.thefollowinginformationwillhelpustodothis.ifyouhave
Medical History Form
 General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
General: Medical History Form 1. Chief Complaint: What are the main health concerns you wish to address? 2. Current and Past Treatment: Have you received treatment for these problems? Yes No, if yes, which:
Name: Date: Sex: Male Female Date of Birth(DD/MM/YY): Address: City: Postal Code: Phone #: (Home) (Work) (Cell) (Other) Address:
: Address: City: Postal Code: Phone #: (Home) (Work) (Cell) (Other) Address:") Name: Date: Sex: Male Female Date of Birth(DD/MM/YY): Address: City: Postal Code: Phone #: (Home) (Work) (Cell) (Other) Email Address: Emergency Contact Name and Phone Number: Family Doctor Name and Address:
Name: Date: Sex: Male Female Date of Birth(DD/MM/YY): Address: City: Postal Code: Phone #: (Home) (Work) (Cell) (Other) Email Address: Emergency Contact Name and Phone Number: Family Doctor Name and Address:
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic th Avenue Surrey BC V4A 2H9 Tel: Fax:
 Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
Dr. Sereena Uppal DC Michael Herrewig DC Doctor of Chiropractic 690 15355 24 th Avenue Surrey BC V4A 2H9 Tel: 604.541.9336 Fax: 604.541.9308 I. Patient Information Thank you for choosing our practice for
Placer Private Physicians: Patient Health Questionnaire [2]
![Placer Private Physicians: Patient Health Questionnaire [2]](/thumbs/87/96006031.jpg "Placer Private Physicians: Patient Health Questionnaire [2]") Dr.Br own 7. Do you feel you eat a healthy diet? 8. Please describe why or why not? 9. Do you exercise regularly? Yes No 10. If yes, what type of exercises and how many days per week? 11. Have you ever
Dr.Br own 7. Do you feel you eat a healthy diet? 8. Please describe why or why not? 9. Do you exercise regularly? Yes No 10. If yes, what type of exercises and how many days per week? 11. Have you ever
Date of Birth: Age: Sex: Male Female Marital. Driver's Lic S M D. Status: Address:
 Houston Weight Loss and Lipo Centers Patient Name: Address: City, State : Apt: Zip: Email*: *By providing your email address you are agreeing to communication via email. Home Phone Primary contact Work
Houston Weight Loss and Lipo Centers Patient Name: Address: City, State : Apt: Zip: Email*: *By providing your email address you are agreeing to communication via email. Home Phone Primary contact Work
NEW CHILD PATIENT INTAKE FORM
 Today's Date: Carmen Hering D.O. NEW CHILD PATIENT INTAKE FORM Patient Name: Please print Date of Birth - - Age: Please list primary caregiver(s) and relationship to child: Number of households: Address(s):
Today's Date: Carmen Hering D.O. NEW CHILD PATIENT INTAKE FORM Patient Name: Please print Date of Birth - - Age: Please list primary caregiver(s) and relationship to child: Number of households: Address(s):
WELCOME TO THE MILLER CHIROPRACTIC CLINIC
 WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
WELCOME TO THE MILLER CHIROPRACTIC CLINIC We are pleased that you have chosen to consult us regarding your health. In order to help us evaluate your condition thoroughly, please complete the following
New Patient Documentation. Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )
 (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( )") New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
New Patient Documentation Name: (Last) (First) (Middle) Address: (Street) (Apt#) (City) (State) (Zip) Home Phone: ( ) Cell: ( ) Work: ( ) Age: Birthdate: E Email: Social: Sex: Male Female Height: Weight:
Joseph S. Weiner, MD, PC Patient History Form
 Date: / / NAME: Last First M. I. Age: Sex: q F q M Birthdate: / / What specific questions or goals do you have for this appointment? Please list the names of other clinicians you have seen for this problem:
Date: / / NAME: Last First M. I. Age: Sex: q F q M Birthdate: / / What specific questions or goals do you have for this appointment? Please list the names of other clinicians you have seen for this problem:
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History
 Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
Capital Health Medical Center - Hopewell NEUROSURGICAL-ONCOLOGY Patient History Please take a few minutes and complete the following questions before you see the doctors so that we may learn a bit more
COMPREHENSIVE HEALTH & WELLNESS PROFILE
 Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
Patient Name DOB COMPREHENSIVE HEALTH & WELLNESS PROFILE The human body is designed to be healthy. Throughout life, events occur which damage your natural health expression. As a full spectrum Chiropractic
Employed? Yes No Employer Name. Occupation. Problem Onset Frequency Severity E.g. Headaches June times per week Mild / Moderate / Severe
 PLEASE NOTE: This file must be saved to your desktop before and after completing! PATIENT INFORMATION Date First Name SSN Sex Marital Status Middle Name Birth Date Last Name Height Spouse Name Address
PLEASE NOTE: This file must be saved to your desktop before and after completing! PATIENT INFORMATION Date First Name SSN Sex Marital Status Middle Name Birth Date Last Name Height Spouse Name Address
Johanna M. Hoeller, DC PS
 ENTRANCE FORM Birth date: Height: Weight: Emergency Contact: Emergency Contact Phone: ( ) Spouse/Partner or Parent s name: Children s names: Occupation (Your): Employer: Address: City/State/Zip: Phone:
ENTRANCE FORM Birth date: Height: Weight: Emergency Contact: Emergency Contact Phone: ( ) Spouse/Partner or Parent s name: Children s names: Occupation (Your): Employer: Address: City/State/Zip: Phone:
MEDICAL DATA SHEET For Patients 18 years of age and older
 MEDICAL DATA SHEET For Patients 18 years of age and older NAME: DATE: / / AGE: DOB: / / 1. What is the main reason you are seeking a physician s advice? 2. Please list all allergies: Drug Allergies: Other
MEDICAL DATA SHEET For Patients 18 years of age and older NAME: DATE: / / AGE: DOB: / / 1. What is the main reason you are seeking a physician s advice? 2. Please list all allergies: Drug Allergies: Other
MEDICAL HISTORY (To be filled in by patient)
") MEDICAL HISTORY Reason for Visit or Chief Complaint: Referred By: Present Illness: (To be filled in by Physician) I. Have you had any reactions, allergies or bad effects from any of the following: Serum
MEDICAL HISTORY Reason for Visit or Chief Complaint: Referred By: Present Illness: (To be filled in by Physician) I. Have you had any reactions, allergies or bad effects from any of the following: Serum
PATIENT INTRODUCTION
 PATIENT INTRODUCTION Personal History: Mr. Mrs. Miss Ms. Dr. Name: First Middle Last Your Address: _ City: Prov: Postal Code: Telephone: Home: Bus: Cell: E-Mail: Check this box if we may contact you via
PATIENT INTRODUCTION Personal History: Mr. Mrs. Miss Ms. Dr. Name: First Middle Last Your Address: _ City: Prov: Postal Code: Telephone: Home: Bus: Cell: E-Mail: Check this box if we may contact you via
Inner Balance Acupuncture
 Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Welcome to About Women by Women
 Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
Welcome to About Women by Women Today s Date New Patient Questionnaire Name: Birth Date: / / Home Phone: Address: Cell Phone: Work Phone: Occupation: Employer: Marital Status: Married Living w/ Partner
New Patient Intake Form 4 Market Place, PO Box 1585, Hollis, NH p: f:
 New Patient Intake Form 4 Market Place, PO Box 1585, Hollis, NH 03049 p: 603.465.2235 f: 603.465.2236 About You Last Name: First Name: Middle Initial: Nickname: Date of Birth: Age: Gender: [ ] M [ ] F
New Patient Intake Form 4 Market Place, PO Box 1585, Hollis, NH 03049 p: 603.465.2235 f: 603.465.2236 About You Last Name: First Name: Middle Initial: Nickname: Date of Birth: Age: Gender: [ ] M [ ] F
New Patient Intake Form
 New Patient Intake Form Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name _ Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
New Patient Intake Form Title: (Check one) Mr. Mrs. Ms. Miss Dr. Other First Name Middle Initial Last Name _ Address City State Zip Code Leave Messages on: (Circle one) Home Cell Work Don t leave messages
City State Zip Code. Ethnic Background: Caucasian African-American Asian Hispanic Native American. Previous. Hobbies/Leisure activities:,,,
 History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
Patient Name Date of Birth MALE / FEMALE Date. Left handed or Right handed. Marital Status: Single Married Divorced Widowed Children?
 PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
PH NEW PATIENT HISTORY Patient Name Date of Birth MALE / FEMALE Date Occupation: Left handed or Right handed Marital Status: Single Married Divorced Widowed Children? Y or N # Previous Treating Physician:
Address Street Address City State Zip Code. Address Street Address City State Zip Code
 Male Initial Visit Intake Form PATIENT INFORMATION Today s Date Last Name Mid Initial First Name Date of Birth Address Home Phone Social Security Number Street Address City State Zip Code Cell Phone E-mail
Male Initial Visit Intake Form PATIENT INFORMATION Today s Date Last Name Mid Initial First Name Date of Birth Address Home Phone Social Security Number Street Address City State Zip Code Cell Phone E-mail
PLEASE NOTE: This file must be saved to your desktop before and after completing!
 PATIENT INFORMATION PLEASE NOTE: This file must be saved to your desktop before and after completing! Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number
PATIENT INFORMATION PLEASE NOTE: This file must be saved to your desktop before and after completing! Date First Name Middle Name Last Name SSN Sex Birth Date Height Weight Marital Status Spouse Name Number
Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: Fax: Peter Robertson Blvd, Brampton ON L6R 1T4
 Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: 905-793- 8868 Fax: 905-793- 8957 630 Peter Robertson Blvd, Brampton ON L6R 1T4 ADULT INTAKE FORM Name: (Last) (First) (Preferred Name) Address:
Dr. Andrea Gri B.Kin, ND Doctor of Naturopathic Medicine Phone: 905-793- 8868 Fax: 905-793- 8957 630 Peter Robertson Blvd, Brampton ON L6R 1T4 ADULT INTAKE FORM Name: (Last) (First) (Preferred Name) Address:
New Patient Specialty Intake Form Department of Surgery
 This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
WELCOME TO THE BURLINGTON NATURAL HEALTH CENTRE PLEASE FILL IN THESE FORMS AS COMPLETELY AS POSSIBLE. THANKYOU!
 WELCOME TO THE BURLINGTON NATURAL HEALTH CENTRE PLEASE FILL IN THESE FORMS AS COMPLETELY AS POSSIBLE. THANKYOU! NAME DATE ADDRESS Gender CITY, PROVINCE HOME PHONE E MAIL POSTAL CODE DATE OF BIRTH (D/M/Y)
WELCOME TO THE BURLINGTON NATURAL HEALTH CENTRE PLEASE FILL IN THESE FORMS AS COMPLETELY AS POSSIBLE. THANKYOU! NAME DATE ADDRESS Gender CITY, PROVINCE HOME PHONE E MAIL POSTAL CODE DATE OF BIRTH (D/M/Y)
UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT
 APPLICANT NAME: UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT REACTION ACCOM. LIGHT PUPILS EQUAL UNEQUAL FUNDI FIELDS OF VISION COLOUR (TEST USED) WITHOUT GLASSES NEAR FAR WITH GLASSES RIGHT
APPLICANT NAME: UCCM ANISHNAABE POLICE SERVICE EMPLOYMENT VISION REPORT REACTION ACCOM. LIGHT PUPILS EQUAL UNEQUAL FUNDI FIELDS OF VISION COLOUR (TEST USED) WITHOUT GLASSES NEAR FAR WITH GLASSES RIGHT
Patient Medical History Form
 Patient Medical History Form Name: DOB: Sex: M F Street Address: City: State: Zip: Home Phone: Work Phone: Cell Phone:_ Email: Emergency Contact: Phone: Primary Care Physician: Phone: How did you hear
Patient Medical History Form Name: DOB: Sex: M F Street Address: City: State: Zip: Home Phone: Work Phone: Cell Phone:_ Email: Emergency Contact: Phone: Primary Care Physician: Phone: How did you hear
Eastern Body Therapy
 2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
2310 Eastern Body Therapy 6th Avenue San Diego, CA 92101 (619)772-4002 Personal Information Name Date of injury/illness Address: Apt. City State Zip Home phone: ( ) Work Phone: ( ) E-mail: Social Security
Eastern Shore MediCann Clinic, LLC
 Eastern Shore MediCann Clinic, LLC New Patient Medical History and Intake Form Medical Marijuana Certification Name Date of Birth Social Security Number Gender: Male Female Address: Street: City: State
Eastern Shore MediCann Clinic, LLC New Patient Medical History and Intake Form Medical Marijuana Certification Name Date of Birth Social Security Number Gender: Male Female Address: Street: City: State
California Chiropractic Boshears, Inc Yucaipa Blvd., Yucaipa Ca Phone: (909) Fax : (909)
 Fax : (909)") California Chiropractic Boshears, Inc. 35191 Yucaipa Blvd., Yucaipa Ca. 92399 Phone: (909) 790-5005 Fax : (909) 790-5009 Patient Information Date: Name: Address: Home Phone: Work Phone: Sex: Male or Female
California Chiropractic Boshears, Inc. 35191 Yucaipa Blvd., Yucaipa Ca. 92399 Phone: (909) 790-5005 Fax : (909) 790-5009 Patient Information Date: Name: Address: Home Phone: Work Phone: Sex: Male or Female
Patient Name: Date: Address: Primary Care Physician: Online Website On TV In print On the radio
 927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
927 W. Myrtle St. Boise, ID 83702 (208) 947-0100 NEW PATIENT INTAKE Patient Name: Date: Email Address: Primary Care Physician: How did you hear about AVT? (Please mark all that apply) Online Website On
Accompanied by Relationship MEDICAL BACKGROUND INFORMATION. Please name the professionals that you have seen for this condition:
 Name: Age: Date: Accompanied by Relationship E-mail: @ MEDICAL BACKGROUND INFORMATION Please name the professionals that you have seen for this condition: Name Specialty Town Phone Who is your primary
Name: Age: Date: Accompanied by Relationship E-mail: @ MEDICAL BACKGROUND INFORMATION Please name the professionals that you have seen for this condition: Name Specialty Town Phone Who is your primary
Name Age Date. Address Phone. Name of Physician. Address Street Address City State Zip Code
 Name Age Date Address Phone What is the reason for your visit today? Where have you been receiving your medical care? Name of Physician Address Street Address City State Zip Code PAST MEDICAL HISTORY:
Name Age Date Address Phone What is the reason for your visit today? Where have you been receiving your medical care? Name of Physician Address Street Address City State Zip Code PAST MEDICAL HISTORY:
Please fill out the following form in as much detail as possible. Please Print. Name. Address. City State Zip. Home Phone Office Phone.
 CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
CASE NO. Please fill out the following form in as much detail as possible. Please Print Date Name Address City State Zip Home Phone Office Phone E-mail Address Age Date of Birth Occupation Sex (M) (F)
CHIROPRACTIC ASSOCIATES CLINIC
 CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM PATIENT INFORMATION Last
CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM PATIENT INFORMATION Last
New Patient Information
 Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
Geoffrey G Glidden MD PA New Patient Information Name Address City/State/Zip Cell Phone Home Phone DL# SSN# Age of Birth Sex: Male / Female Your employer Occupation Work Phone E-Mail Referring Physician
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
REVIEWED DATE / INITIALS Safety: Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: If YES, please list medication allergies: Do you have
PATIENT HEALTH QUESTIONNAIRE Radiation Oncology
 REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
REVIEWED DATE / INITIALS Safety: Yes No Are you at risk for falls? Do you have a Pacemaker? Females; Is there a possibility you may be pregnant? Allergies: Yes No If YES, please list medication allergies:
PATIENT INFORMATION FILL OUT ALL ITEMS
 PATIENT INFORMATION FILL OUT ALL ITEMS FAILURE TO COMPLETELY FILL OUT THIS FORM MAY RESULT IN YOU BEING BILLED IN FULL Patient Last Name: First: MI:. Address:. Date of Birth: Gender: M or F Marital Status:
PATIENT INFORMATION FILL OUT ALL ITEMS FAILURE TO COMPLETELY FILL OUT THIS FORM MAY RESULT IN YOU BEING BILLED IN FULL Patient Last Name: First: MI:. Address:. Date of Birth: Gender: M or F Marital Status:
Caspian Acupuncture -- Health History Form Anita Tayyebi EAMP, LAc. 652 SW 150 th St Burien WA 98166
 Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
Patient History Form
 Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
* CC* PATIENT QUESTIONNAIRE
 Pain Center of Michigan *0290341CC* PATIENT QUESTIONNAIRE Patient Name Birthdate Age Home Address City State Zip Home Phone Alternate Phone Referring Physician Primary Care Physician MEDICAL HISTORY Please
Pain Center of Michigan *0290341CC* PATIENT QUESTIONNAIRE Patient Name Birthdate Age Home Address City State Zip Home Phone Alternate Phone Referring Physician Primary Care Physician MEDICAL HISTORY Please
HEALTH INFORMATION FORM
 #102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
#102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
Rockwood Natural Medicine Clinic
 Rockwood Natural Medicine Clinic 9755 N. 90 th St., Suite A-210 Scottsdale, Arizona 85258 480-767-7119 Date: Name: Age: Sex: M F Are you: Married Separated Divorced Widowed Single How did you hear about
Rockwood Natural Medicine Clinic 9755 N. 90 th St., Suite A-210 Scottsdale, Arizona 85258 480-767-7119 Date: Name: Age: Sex: M F Are you: Married Separated Divorced Widowed Single How did you hear about
Medical History Form
 Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
Medical History Form NAME DOB / / TODAY S DATE MEDICAL HISTORY What medical Conditions do you have? Select all that apply, or write in if not listed: Diabetes High Blood Pressure Thyroid Disorder Heart
Please list any medications you currently taking along with dosage and directions (including birth control, vitamins and OTC medications):
:") Name: DOB: Date of Appointment: Please list all doctors you currently see (Primary Care Physician and Specialists i.e. Cardiologist): Please list any medications you currently taking along with dosage
Name: DOB: Date of Appointment: Please list all doctors you currently see (Primary Care Physician and Specialists i.e. Cardiologist): Please list any medications you currently taking along with dosage
HEALTH INFORMATION FORM
 #102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
#102, 506-71 Ave SW Calgary AB T2V 4V4 Ph 587.352.9199 Fax 1.888.501.1724 info@fullcirclecalgary.ca www.fullcirclecalgary.ca Part 1: BASIC INFORMATION HEALTH INFORMATION FORM Name: Date: Address: City:
DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N)
") Medical History: Patient: DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N) List the names of prescription
Medical History: Patient: DOB: / / Please list the names and telephone numbers of the other physicians involved in your care: Name Specialty Phone Address Receive Report (Y/N) List the names of prescription
Chiropractic Registration and History
 Chiropractic Registration and History 1. Patient Information Name: Birthdate: SS/HIC/Patient ID #: Address: City: State: Zip: Phone: Cell: E-Mail: Sex: M F (Circle) Minor Single Married Divorced Separated
Chiropractic Registration and History 1. Patient Information Name: Birthdate: SS/HIC/Patient ID #: Address: City: State: Zip: Phone: Cell: E-Mail: Sex: M F (Circle) Minor Single Married Divorced Separated
Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address
 Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
Today s Date Contact Information Name Age DOB Sex M F Your relationship status: Single Married Life partner Widowed Address Phone numbers and E-mail (please check numbers to call or leave a message) Home
New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification
 Certification") Name Social Security Number Address: Street: _ New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification Date of Birth Gender: Male Female City: State Zip Code E-mail: Home Phone:
Name Social Security Number Address: Street: _ New Patient Medical History and Intake Form Medical Marijuana ( MMJ ) Certification Date of Birth Gender: Male Female City: State Zip Code E-mail: Home Phone:
PATIENT INFORMATION FILL OUT ALL ITEMS
 PATIENT INFORMATION FILL OUT ALL ITEMS FAILURE TO COMPLETELY FILL OUT THIS FORM MAY RESULT IN YOU BEING BILLED IN FULL Patient Last Name: First: MI:. Address:. City: State: Zip:. Date of Birth: Gender:
PATIENT INFORMATION FILL OUT ALL ITEMS FAILURE TO COMPLETELY FILL OUT THIS FORM MAY RESULT IN YOU BEING BILLED IN FULL Patient Last Name: First: MI:. Address:. City: State: Zip:. Date of Birth: Gender:
Amarillo Surgical Group Doctor: Date:
 Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
Office Visit Information (General Surgery) Amarillo Surgical Group Doctor: Date: Patient s Information Name: Last First Middle Social Security #: Date of Birth: Age Gender: [ Male / Female ] Marital Status:
55 S. Main Street, Driggs, ID (208)
") Elements of Health 55 S. Main Street, Driggs, ID 83422 (208) 920-0312 Name: (first) (middle) (last) Date: / / Address: Phone: / street address city zipcode home / cell Date of Birth: / / Age: Gender: M/F
Elements of Health 55 S. Main Street, Driggs, ID 83422 (208) 920-0312 Name: (first) (middle) (last) Date: / / Address: Phone: / street address city zipcode home / cell Date of Birth: / / Age: Gender: M/F
MedStar Medical Group at Forest Hill 1517 Rock Spring Road, Suite C Forest Hill, Maryland Phone (410) Fax (410)
 Fax (410)") MedStar Medical Group at Forest Hill 1517 Rock Spring Road, Suite C Forest Hill, Maryland 21050 Phone (410) 838-6358 Fax (410) 838-6750 Name Last First MI Preferred Address Street Number Road Apt Number
MedStar Medical Group at Forest Hill 1517 Rock Spring Road, Suite C Forest Hill, Maryland 21050 Phone (410) 838-6358 Fax (410) 838-6750 Name Last First MI Preferred Address Street Number Road Apt Number
PATIENT MEDICAL HISTORY INTAKE FORM
 Northgate Professional Center 1985 Main Street, Suite 209 Springfield, Massachusetts 01103 Tel; 413-455-1081 Fax; 413-391-7489 www.marimedconsults.com PATIENT MEDICAL HISTORY INTAKE FORM Patient Information:
Northgate Professional Center 1985 Main Street, Suite 209 Springfield, Massachusetts 01103 Tel; 413-455-1081 Fax; 413-391-7489 www.marimedconsults.com PATIENT MEDICAL HISTORY INTAKE FORM Patient Information:
Sydney Chiropractic, DR. DAVID DUNN
 PERSONAL HISTORY Name: Address: City: Province: Postal Code: Home Phone: Birthdate: Age: Sex: M F # of Children Business/Employer: Business Phone: Type of Work You Do: E-mail: Emergency Contact: Phone
PERSONAL HISTORY Name: Address: City: Province: Postal Code: Home Phone: Birthdate: Age: Sex: M F # of Children Business/Employer: Business Phone: Type of Work You Do: E-mail: Emergency Contact: Phone
NEW PATIENT INFORMATION FORM
 UNIT NUMBER PT. NAME UCSF Medical Center AMBULATORY SERVICES BIRTHDATE LOCATION DATE Today s Date / / What is the reason for your visit today? Where have you been receiving your medical care? Name of Physician
UNIT NUMBER PT. NAME UCSF Medical Center AMBULATORY SERVICES BIRTHDATE LOCATION DATE Today s Date / / What is the reason for your visit today? Where have you been receiving your medical care? Name of Physician
CHIROPRACTIC ASSOCIATES CLINIC
 CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM Which Chiropractor are
CHIROPRACTIC ASSOCIATES CLINIC 1127 LAKEWOOD COURT NORTH, REGINA, SK S4X 3S3 PH: (306) 924-5300 FAX: (306) 924-5252 EMAIL: cac.north@accesscomm.ca CHIROPRACTIC INITIAL HEALTH FORM Which Chiropractor are
New Adult Intake Form
 New Adult Intake Form Please complete the following form in order to provide us with the background information we require to ensure you receive comprehensive care. Name: Today s Date: Age: Date of Birth
New Adult Intake Form Please complete the following form in order to provide us with the background information we require to ensure you receive comprehensive care. Name: Today s Date: Age: Date of Birth
Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left HISTORY OF PRESENT ILLNESS
 CAPS PAINCARE Page 1 of 5 Today s : / / SSN (last 4 digits): xxx-xx - Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left Type of Accident/Injury: Auto Work Personal Injury
CAPS PAINCARE Page 1 of 5 Today s : / / SSN (last 4 digits): xxx-xx - Patient Name: DOB: Age: Sex: Male Female Height: Weight: Dominant Hand: Right Left Type of Accident/Injury: Auto Work Personal Injury
PATIENT PERSONAL / CONFIDENTAL DATA
 PATIENT PERSONAL / CONFIDENTAL DATA Address: City: State: Zip Code : H. Phone: W. Phone: Cell Phone: Date of Birth: Age: Sex: M F Marital Status: M S D W Email Address: Social Security # Name of Spouse:
PATIENT PERSONAL / CONFIDENTAL DATA Address: City: State: Zip Code : H. Phone: W. Phone: Cell Phone: Date of Birth: Age: Sex: M F Marital Status: M S D W Email Address: Social Security # Name of Spouse:
New Patient Form Welcome!
 New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
New Patient Form Welcome! Last First Middle Initial DOB Address City ST ZIP Phone (H) (C) Email Occupation Employer Relationship Status S M W D Spouse s Name DOB Children s Names and Ages Have you had
Adult Health History Summary
 Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Adult Health History Summary Name Age Date of Birth Address City Province Postal Code Phone (home) (cell) Occupation Email May we contact you via email? YES NO Emergency Contact Phone # How did you hear
Health History. Personal Health History. Institute of Complementary Medicine. FOC Health History - ICM
 Reason for office visit today FOC Health History - ICM Health History Whom may we thank for referring you today? Do you have another primary care provider? Date of last physical exam Previous or referring
Reason for office visit today FOC Health History - ICM Health History Whom may we thank for referring you today? Do you have another primary care provider? Date of last physical exam Previous or referring
CONSULTATION ADMITTANCE FORM
 CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
CONSULTATION ADMITTANCE FORM Last Name: First Name: Address: City Postal Code: Home Phone: Work Phone: Age: Birth date (dd/mm/yr): Sex: M / F Height Weight Occupation: Alberta Health Care #: PLEASE CHECK
Questionnaire for Lipedema Patients
 Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Questionnaire for Lipedema Patients Name Date of diagnosis Date Name of physician making diagnosis Do you also have lymphedema? What areas of the body are affected? Outside of thighs Inner thighs Knees
Address: Yes! I would like to receive your Monday Morning Health Tips.
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
What is your occupation? Company Name Do you have extended healthcare benefits? Yes No Benefits are personal or from work
 Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Welcome to our Office! New Patient Intake Form Date Name Preferred Name Birthdate (D/M/Y) Age Sex F M Address Unit City Province Postal Code Home # Cell # May we contact you at work? Yes No Work # Extension
Medical Intake Form. Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip:
 Date: Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: E-mail: Person to Contact in Case of Emergency: Relationship
Date: Patient Name: Age : Date of Birth: Gender: Female Male Marital Status: #Children: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: E-mail: Person to Contact in Case of Emergency: Relationship
Pure Health Natural Medicine
 Pure Health Natural Medicine Female Intake Date: Personal Information Name: (first, last) Maiden: Preferred Name: Sex: M F Date of Birth: Age: Street Address: City: State: Zip: E-mail Home Phone: Cell
Pure Health Natural Medicine Female Intake Date: Personal Information Name: (first, last) Maiden: Preferred Name: Sex: M F Date of Birth: Age: Street Address: City: State: Zip: E-mail Home Phone: Cell
Patient First Name Patient Middle Initial Patient Last Name. Primary Care Physician Primary Care Physician Phone Pharmacy Name
 NP Hagans Walk-In Clinic * 9135 Piscataway Rd. # 320 Clinton, MD 20735 * (240)-412-5093 (Office) Patient Information Patient First Patient Middle Initial Patient Last Sex Marital Status Date of Birth Social
NP Hagans Walk-In Clinic * 9135 Piscataway Rd. # 320 Clinton, MD 20735 * (240)-412-5093 (Office) Patient Information Patient First Patient Middle Initial Patient Last Sex Marital Status Date of Birth Social
Chiropractic Case History/Patient Information. Social Security # Home Phone: Address: City: State: Zip: address: Fax # Cell Phone:
 Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Tassin Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
Chiropractic Case History/Patient Information 1 Date: Patient # Doctor: Tassin Name: Social Security # Home Phone: Address: City: State: Zip: E-mail address: Fax # Cell Phone: Age: Birth Date: Race: Marital:
HILL PARK MEDICAL CENTER PATIENT REGISTRATION FORM
 PATIENT REGISTRATION FORM Address: City: Contact: State: Zip: Home Phone: Email: Work: Cell: Date of Birth: SSN#: Age: Gender: I am: q Married q In a Partnership q Separated q Divorced q Widowed q Single
PATIENT REGISTRATION FORM Address: City: Contact: State: Zip: Home Phone: Email: Work: Cell: Date of Birth: SSN#: Age: Gender: I am: q Married q In a Partnership q Separated q Divorced q Widowed q Single
1. Have you ever had or now have: 2. Have you ever had or now have:
 1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
Providence Neurosurgery PATIENT INFORMATION SHEET
 Date: Staff only: Weight: Height: BP: Pain Age Patient Name Date of Birth Street Address City State Zip Code Home Phone Work Phone Cell Phone Right handed Left handed Please mark one Referring Physician
Date: Staff only: Weight: Height: BP: Pain Age Patient Name Date of Birth Street Address City State Zip Code Home Phone Work Phone Cell Phone Right handed Left handed Please mark one Referring Physician
McLaren Cardiothoracic and Vascular PATIENT HISTORY FORM
 McLaren Cardiothoracic and Vascular PATIENT HISTORY FORM Please complete this form and bring it with you to your appointment Appointment Date Appointment Time Name Referring Physician Date of Birth Please
McLaren Cardiothoracic and Vascular PATIENT HISTORY FORM Please complete this form and bring it with you to your appointment Appointment Date Appointment Time Name Referring Physician Date of Birth Please