Efficacy and Safety of Treatment for Pediatric IBD
|
|
|
- Whitney Barker
- 6 years ago
- Views:
Transcription


1 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
2 Treatment of Pediatric IBD Goals Improve growth and nutrition Improve quality of life Maximize therapeutic response Minimize toxicity Prevent disease complications Mucosal healing Promote psychological health

3 5-ASA Delivery Systems PENTASA ASACOL/DELZICOL/LIALDA/APRISO COLAZAL/AZULFIDINE/DIPENTUM ENEMA SUPP JEJUNUM / ILEUM / ASCENDING / DESCENDING / SIGMOID / RECTUM SMALL BOWEL COLON
4 Efficacy of 5-ASA s Ulcerative Colitis Oral therapy effective for induction and maintenance of remission Rectal, oral + rectal More effective than just oral for distal disease Crohn s disease Efficacy unclear for induction or maintenance of remission


5 Antibiotics Decrease inflammation by changing or eliminating bacteria in GI tract Multiple indications for Crohn s Perianal disease Abscess Prevent post-operative recurrence Treatment of mild or moderate disease Flagyl (metronidazole) Cipro (ciprofloxacin) Ulcerative colitis Triple or quadruple antibiotics for refractory severe UC* *Turner D, et al. J Crohns Colitis 2014; 8:

6 Probiotics Live microorganisms Alter flora of gut Promote more favorable bacteria inflammation Many different preparations UC Effective, particularly for pouchitis Crohn s Not proven effective
7 Systemic Corticosteroids Oral (prednisone), IV (Solumedrol), or rectal Suppress active inflammation Indication: Acute UC or Crohn s flare Provide immediate symptomatic relief Do not promote healing of GI tract Not indicated for maintenance therapy Lose efficacy, side effects
8 Corticosteroids Common Side Effects Growth retardation Contribution to bone mineral density Excessive weight gain Cosmetic Acne, moon facies, hirsutism Psychological Sleep disturbance, mood instability Increased risk of infection
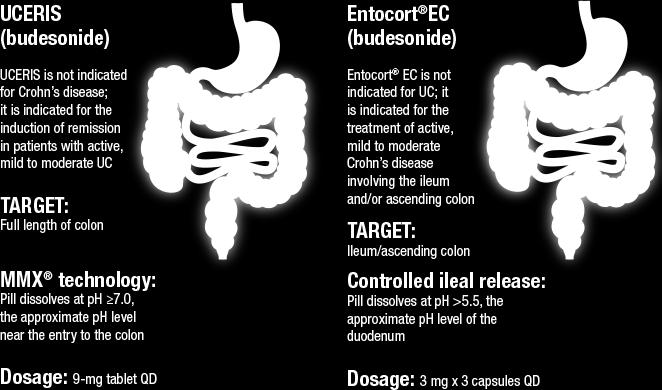
9 Budesonide



 Methotrexate No")
10 Immunomodulators Suppress immune response that triggers intestinal damage in IBD Require longer period of time for efficacy Steroid sparing effects Used alone and in combination with biological therapies Imuran (azathioprine) Purinethol (6-MP) Methotrexate No live vaccines
11 6-MP/Imuran Oral medication administered every night Requires 3-4 months for maximal efficacy Effective for Crohn s Disease and UC Maintenance of remission Decrease in steroid requirements Perianal disease? Prevention/treatment of post-operative recurrence
12 Methotrexate Better studied in Crohn s disease May improve growth, perianal disease Administered once weekly Subcutaneous injection vs. oral Laboratory monitoring required Requires 6-8 weeks for efficacy Faster onset of action compared to 6-MP Does not require monitoring of metabolites
13 6-MP/AZA and MTX Adverse Effects Nausea 6-MP/AZA white blood cell count Liver toxicity Pancreatitis Increased infection risk Increased skin cancer risk Slightly increased lymphoma risk Methotrexate Nausea white blood cell count Liver toxicity Poor appetite Increased infection risk Reaction at injection site No documented increased cancer risk Teratogenic

14 Enteral Nutritional Therapy TO BE DISCUSSED LATER!
15 Biologic Therapies Pro-inflammatory cytokines contribute to inflammation in IBD Remicade (infliximab) TNFα is elevated in IBD patients Biologics block and neutralize cytokines Used to treat moderate to severe Crohn s disease and ulcerative colitis 75% Human Humira (adalimumab) 100% Human
16 Remicade (infliximab) Humira (adalimumab) Moderate to severe Crohn s disease Decreases steroid requirement Mucosal healing Healing of perianal disease Improvement of growth Bone health Prevention of post-operative recurrence Ulcerative colitis Treatment of moderate to severe disease Prevention of surgery

17 REACH Improved Growth with Infliximab Hyams, et al. Gastroenterology 2007;132:863-73
18 Anti-TNF α Therapy Remicade (infliximab) Intravenous infusion Loading dose 0, 2, 6 weeks Maintenance dose Every 8 weeks Can escalate if necessary Humira (adalimumab) SQ injection Loading dose Multiple injections wk 0,2 Maintenance dose Every 2 weeks Can escalate if necessary Need to pre-screen for tuberculosis No live vaccines

19 Anti-TNF Therapeutic Monitoring Measure trough level/antibodies against medicine Sub-therapeutic drug level Less likely to be effective Increase dose and/or decrease interval Antibodies against medication Less likely to be effective Can optimize dose Might have to switch agents Add immunomodulator
20 Vedolizumab (Entyvio) Gut specific anti-adhesion molecule 2014: Approved for adult Crohn and UC CHOP: ~30 patients have received Currently studying results
21 % Remission Remission (PCDAI < 10 or PUCAI <10) Baseline Week 6 Week 14 Week 22 n=21


22 Ustekinumab (Stelara ) for Active Crohn Disease Prevents binding of IL-12 and IL-23 to receptors Showed promise for adult CD patients with anti-tnf failure 09/2016: Approved for treatment of Crohn disease Side effect profile seems favorable Induction: Single IV weight-based dose Maintenance: 90 mg SQ q8 weeks Sandborn WJ et al. N Engl J Med 2012; 367:
23 Traditional Pediatric IBD Step-Up Algorithm Severe Surgery Moderate Mild Prednisone Steroids Budesonide Antibiotics Aminosalicylates Infliximab/ Adalimumab 6-MP/AZA Methotrexate Enteral Nutrition Probiotics
24 Does Early Use of Biological Therapy Improve Efficacy? Growth? Early Biologic therapy 6-MP/AZA/Methotrexate Steroids Late Surgery
25 Percent of patients (%) SONIC Trial Corticosteroid-Free Clinical Remission at Week p=0.025 p<0.001 p= /170 67/169 94/169 AZA + placebo IFX + placebo IFX+ AZA Colombel JF et al. N Eng J Med. 2010; 362:
 Early immunomodulator Neither 100 80 60")

26 Early Anti-TNF Therapy in Pediatric Crohn Disease Observational cohort of pediatric CD patients (inflammatory) Propensity score analysis matched patients on baseline characteristics in 68 triads Early anti-tnf (<3 mo) Early immunomodulator Neither Steroid-free Remission* at 1 Year p= p= % p= % 54.4% Early anti-tnf Higher remission rate Improved height z-score *Remission: PCDAI 10, steroid free, no surgery 20 0 Anti-TNF IM Neither Walters TD et al. Gastroenterology 2014; 146:383-91
27 Risk of Treating vs. Not Treating Risk of Treatment Risk of Disease Risk of Treatment
28 Long-Term Evolution of Pediatric Crohn Disease is Structural Damage Inflammatory Stricturing Penetrating Vernier-Massouille G et al. Gastroenterology 2008
29 What we (parents, patients and physicians) are most concerned about: Infection Lymphoma


30 Pediatric IBD Risk of Serious Infection: A Systematic Review Serious Infections per 10,000 Patient-Years P<0.001 P<0.001 P= Ped Anti-TNF Ped IM Adult Anti-TNF Ped Steroids Dulai PS et al. Clin Gastroenterol Hepatol 2014; 12:
31 Meta-Analysis: Biological Therapies and Risk of Infection 49 randomized, placebo controlled trials 14,590 participants For all studies, patients on biological therapy: 19% increased risk of all infections Serious infections not increased Higher risk of opportunistic infections (including Tb) For studies deemed low risk of bias Serious infections decreased in biologic exposed Bononvas S et al. Clin Gastroenterol Hepatol 2016; 14:
32 Vaccination Ensure that vaccines are up to date at time of diagnosis All non-live vaccines should be given Annual flu shot HPV vaccine Consider pneumococcal vaccine Avoid live vaccines if immunosuppressed MMR, Varicella, intranasal flu, others Try to confirm Varicella immunity prior

33 Risk versus Benefit of Biologics and Immune Suppressants in IBD Adapted from Siegel CA. Comprehensive approach to patient risk. Risk versus benefit of biologics and immune suppressants. In: Targan S, Shanahan F, Karp L, eds. Inflammatory Bowel Disease: Translating basic science into clinical practice

34 Risk of Developing NHL No immune suppression
35 Risk of Developing NHL -- Immunomodulator

36 Risk of Developing NHL Immunomodulator & Anti- TNF
37 Pediatric Develop Registry Largest prospective pediatric IBD safety cohort Patients assessed every 6 months, followed for 20 years 5,691 patients enrolled with > 20,000 PY of F/U Infliximab exposed do not have higher rate of malignancy than non-exposed Statistically significant slightly increased rate of malignancy in thiopurine exposed Hyams J et al. Gastroenterology 2017; epub ahead of press.

38 Less Risk of Malignancy with Biologic Monotherapy? Lichtenstein GR et al. Am J Gastroenterol 2014; 109:
39 Risk of Disease Often Greater than Risk of Treatment Risk of Treatment Risk of Disease

40 Thank you
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Medical therapies and IBD
 Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
Medical therapies and IBD Although there is no cure for IBD, there are many treatment options available. There is no standard treatment for IBD that is effective in all situations or for all patients,
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Practical Risk Management Tools for Patients with IBD. Garth Swanson MD Rush University Medical Center
 Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
Practical Risk Management Tools for Patients with IBD Garth Swanson MD Rush University Medical Center IBD Therapy Severity Tysabri Surgery Infliximab, i Adalimumab, Certilizumab Corticosteroids, Immunomodulators
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
My Child Has Inflammatory Bowel Disease : Why? What now? What s next?
 My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
My Child Has Inflammatory Bowel Disease : Why? What now? What s next? George M. Zacur, M.D., M.S. Clinical Assistant Professor Department of Pediatrics and Communicable Diseases Division of Gastroenterology
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Improving outcome of Inflammatory Bowel Disease in children
 Improving outcome of Inflammatory Bowel Disease in children Dinesh Pashankar, MD Pediatric Gastroenterologist Director- Pediatric IBD program Yale University School of Medicine Pediatric Gastroenterology
Improving outcome of Inflammatory Bowel Disease in children Dinesh Pashankar, MD Pediatric Gastroenterologist Director- Pediatric IBD program Yale University School of Medicine Pediatric Gastroenterology
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
COPYRIGHT. Inflammatory Bowel Disease What Every Clinician Needs to Know. Adam S. Cheifetz, MD. Director, Center for Inflammatory Bowel Disease
 Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Of Treatment For Inflammatory Bowel Diseases
 Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Outline. Biologic Drugs in Inflammatory Bowel Disease Dr. Jason Etzel MD The Vancouver Clinic. Biologic Drugs. Biologic Drugs. Biologic Drugs Anti-TNF
 Outline Biologic Drugs in Inflammatory Bowel Disease Dr. Jason Etzel MD The Vancouver Clinic Types of biologic drugs How do they work? How effective are they? Safety/Toxicity concerns with biologics Biologic
Outline Biologic Drugs in Inflammatory Bowel Disease Dr. Jason Etzel MD The Vancouver Clinic Types of biologic drugs How do they work? How effective are they? Safety/Toxicity concerns with biologics Biologic
Ulcerative Colitis Therapy. Faculty Disclosure. Acknowledgements 28/11/2013. Amy Morse November 30/13
 Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Latest Meds Approved for IBD: What are they and how do they work?
 Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Treatment of Pediatric IBD: What is Different?
 Treatment of Pediatric IBD: What is Different? January 13, 2017 Michael Kappelman MD, MPH University of North Carolina at Chapel Hill Overview Is Pediatric IBD the same disease? Treatment considerations
Treatment of Pediatric IBD: What is Different? January 13, 2017 Michael Kappelman MD, MPH University of North Carolina at Chapel Hill Overview Is Pediatric IBD the same disease? Treatment considerations
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
I B D. etter than this. isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES
 I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
IBD in teenagers Biological and Transition
 IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
Drug Level Monitoring in IBD. Objectives
 Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
New Perspectives on the Diagnosis and Management of IBD. Disclosures
 New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
Preventive Care and Monitoring of the IBD Patient
 Preventive Care and Monitoring of the IBD Patient Francis A. Farraye, MD, MSc, FACG Clinical Director, Section of Gastroenterology Director, Inflammatory Bowel Disease Center Boston Medical Center Professor
Preventive Care and Monitoring of the IBD Patient Francis A. Farraye, MD, MSc, FACG Clinical Director, Section of Gastroenterology Director, Inflammatory Bowel Disease Center Boston Medical Center Professor
Addressing Risks and Benefits In IBD
 Addressing Risks and Benefits In IBD Gil Y. Melmed, MD, MS Assistant Professor of Medicine, Cedars-Sinai Medical Center David Geffen School of Medicine at UCLA www.nomorecrohnsdisease.com "Jaw Dropping
Addressing Risks and Benefits In IBD Gil Y. Melmed, MD, MS Assistant Professor of Medicine, Cedars-Sinai Medical Center David Geffen School of Medicine at UCLA www.nomorecrohnsdisease.com "Jaw Dropping
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL
 NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
NEW CONCEPTS IN CROHN S DISEASE GLENDON BURRESS, MD PEDIATRIC GASTROENTEROLOGY ROCKFORD, IL CROHN S DISEASE Chronic disease of uncertain etiology Etiology- genetic, environmental, and infectious Transmural
Treatment Options. Suresh Pola, MD Kaiser San Diego
 Treatment Options Suresh Pola, MD Kaiser San Diego Overview of Treatments! Medications! Diet! Complementary and Alternative Medicines! How to treat Pain Treatment Goals and Target! Goals of Treatment should
Treatment Options Suresh Pola, MD Kaiser San Diego Overview of Treatments! Medications! Diet! Complementary and Alternative Medicines! How to treat Pain Treatment Goals and Target! Goals of Treatment should
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
IBD Module 2: Medication and Patient Management. Kami Roake, PharmD Rheumatology & Gastroenterology Pharmacist University of Utah Hospitals & Clinics
 IBD Module 2: Medication and Patient Management Kami Roake, PharmD Rheumatology & Gastroenterology Pharmacist University of Utah Hospitals & Clinics Objectives Describe current treatment guidelines and
IBD Module 2: Medication and Patient Management Kami Roake, PharmD Rheumatology & Gastroenterology Pharmacist University of Utah Hospitals & Clinics Objectives Describe current treatment guidelines and
Dr. Elmer Schabel, MD. Bundesinstitut für Arzneimittel und Medizinprodukte, Bonn, Germany (No conflicts of interest)
") EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Risk = probability x consequence
 Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
Explaining Risks of IBD Therapy to Parents and Patients December 4, 2009 CCFA Advances in IBD Hollywood, FL Corey A. Siegel Assistant Professor of Medicine, Dartmouth Medical School Director, Dartmouth-Hitchcock
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA
 Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Epidemiology / Morbidity
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments
 INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments Phillip Minar, MD Pediatric Gastroenterologist Cincinnati Children s Hospital Medical Center Objectives of Session What
INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments Phillip Minar, MD Pediatric Gastroenterologist Cincinnati Children s Hospital Medical Center Objectives of Session What
DENOMINATOR: All patients aged 18 and older with a diagnosis of inflammatory bowel disease
 Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Speaker Introduction
 Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
Speaker Introduction Stephen B. Hanauer, MD Professor of Medicine and Clinical Pharmacology University of Chicago Pritzker School of Medicine Chief of Gastroenterology, Hepatology, and Nutrition University
Effective Health Care Program
 Comparative Effectiveness Review Number 131 Effective Health Care Program Pharmacologic Therapies for the Management of Crohn s Disease: Comparative Effectiveness Executive Summary Description of Crohn
Comparative Effectiveness Review Number 131 Effective Health Care Program Pharmacologic Therapies for the Management of Crohn s Disease: Comparative Effectiveness Executive Summary Description of Crohn
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review)
") Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments
 INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments Phillip Minar, MD, MS Pediatric Gastroenterologist Cincinnati Children s Hospital Medical Center 3.3.2019 Objectives
INFLAMMATORY BOWEL DISEASE 101: From Hurdling New Diagnosis to Optimizing Treatments Phillip Minar, MD, MS Pediatric Gastroenterologist Cincinnati Children s Hospital Medical Center 3.3.2019 Objectives
This program is supported by an educational grant from Janssen Biotech Inc., Shire, Inc., and a sponsorship from Takeda
 This program is supported by an educational grant from Janssen Biotech Inc., Shire, Inc., and a sponsorship from Takeda Today s Presenter Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease
This program is supported by an educational grant from Janssen Biotech Inc., Shire, Inc., and a sponsorship from Takeda Today s Presenter Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease
Carefirst.+.V Family of health care plans
 Carefirst.+.V Family of health care plans CVS care mark POLICY Document for ENTYVIO The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Carefirst.+.V Family of health care plans CVS care mark POLICY Document for ENTYVIO The overall objective of this policy is to support the appropriate and cost effective use of the medication, specific
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Garrick Brown, MD. Digestive Health Specialists Tacoma Gig Harbor
 Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
Garrick Brown, MD Digestive Health Specialists Tacoma Gig Harbor Today s Objectives Define IBD, its potential causes and diagnosis Discuss management and treatment Discuss complementary and alternative
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM
 CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Crohn s
 Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
FOR UK NURSING MEDIA Embargoed until: 00:01 GMT, Friday 13 March 2015
 Contact: Ross Selby Takeda UK Ltd Email ross.selby@takeda.com News Release FOR UK NURSING MEDIA Embargoed until: 00:01 GMT, Friday 13 March 2015 World s first gut-selective treatment for ulcerative colitis
Contact: Ross Selby Takeda UK Ltd Email ross.selby@takeda.com News Release FOR UK NURSING MEDIA Embargoed until: 00:01 GMT, Friday 13 March 2015 World s first gut-selective treatment for ulcerative colitis
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Inflammatory Bowel Diseases
 Objectives Today s discussion will address the following topics: Similarities and differences between Crohn s disease (CD) and ulcerative colitis (UC) Risks and benefits of medication, surgery, and integrative
Objectives Today s discussion will address the following topics: Similarities and differences between Crohn s disease (CD) and ulcerative colitis (UC) Risks and benefits of medication, surgery, and integrative
IBD Biologicals and Novel therapeutic regimes. Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh
 IBD Biologicals and Novel therapeutic regimes Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh 1 Treatment aims in IBD Traditional treatment goals of IBD Control of symptoms?improvement
IBD Biologicals and Novel therapeutic regimes Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh 1 Treatment aims in IBD Traditional treatment goals of IBD Control of symptoms?improvement
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Biologic Therapy for Ulcerative Colitis in 2015
 5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease
 Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
INFLAMMATORY BOWEL DISEASE. Brittany Palasik, PharmD, BCPS University of North Texas System College of Pharmacy
 INFLAMMATORY BOWEL DISEASE Brittany Palasik, PharmD, BCPS University of North Texas System College of Pharmacy Pharmacist learning objectives By the end of this presentation, the pharmacist should be able
INFLAMMATORY BOWEL DISEASE Brittany Palasik, PharmD, BCPS University of North Texas System College of Pharmacy Pharmacist learning objectives By the end of this presentation, the pharmacist should be able
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,