Sports Medicine Policy and Procedures Try-Out Checklist
|
|
|
- Myra Strickland
- 6 years ago
- Views:
Transcription
, a nurse practitioner (APRN), or a physician s assistant (PA), stating that you have been")
1 Try-Out Checklist WHAT MEDICAL INFORMATION DO I NEED TO PROVIDE BEFORE TRYING OUT FOR AN ATHLETIC TEAM AT THE UNIVERSITY OF CONNECTICUT? The NCAA requires you to have a note signed by a licensed medical practitioner, either a doctor (MD, DO), a nurse practitioner (APRN), or a physician s assistant (PA), stating that you have been examined in the past six months and have been cleared to try out for an intercollegiate athletic team. This note can come in any form, as long as it is signed by the licensed practitioner and has their license number on it. It can come from a practitioner back home who has recently seen you or it can be done by someone locally. A sample history and physical is attached to this checklist. THIS EXACT FORM IS NOT REQUIRED. It is only there for your practitioner to use, if they so desire. The NCAA requires you to show proof of a test for sickle cell trait before you can begin trying out. You need to do one of the following: Provide evidence of a previous test. All newborns are now tested, and your doctor at home may have the results. Have the test performed. This is available at Student Health Services. You will need to have it ordered by a practitioner there. There is a fee for it. Sign a waiver declining the test. This can only be done after reading the educational material about sickle cell trait that is attached to the waiver. All of this information will need to be turned in to the coach responsible for organizing try-outs for your team. Once it has been determined that you have made the team, you will need to see one of the team physicians for a complete sports physical.
2 Medical Clearance for Try-Out DOCUMENTATION OF MEDICAL CLEARANCE TO TRY-OUT FOR INTERCOLLEGIATE ATHLETICS I have examined _ and (patient s name) document that I have found no evidence of a medical condition that would prohibit them from trying out for the following intercollegiate sports at the University of Connecticut. All sports All sports except Only the following sports of Examination (must be within 6 months of try-out): Practitioner s Name: Title: M.D. DO PA APRN Signature: Street City State Zip Phone License# State
3 Try-Out Policy Statement Name: : People Soft#: Team: DOB: Year: I do hereby release the University of Connecticut and its employees from liability due to injury or illness arising as the result of my participation as a walk-on of the above stated University of Connecticut athletic team. I also will provide proof of medical clearance to participate in athletics by a qualified health care practitioner that has been performed within 6 months prior to trying out. Within 14 days of making the team, a complete physical has to be done by a University of Connecticut Team Physician. I understand that I have to schedule an appointment at Print Name Signature Emergency Contact Information Name: Relationship: Phone Number(s):

4 Sickle Cell Fact Sheet
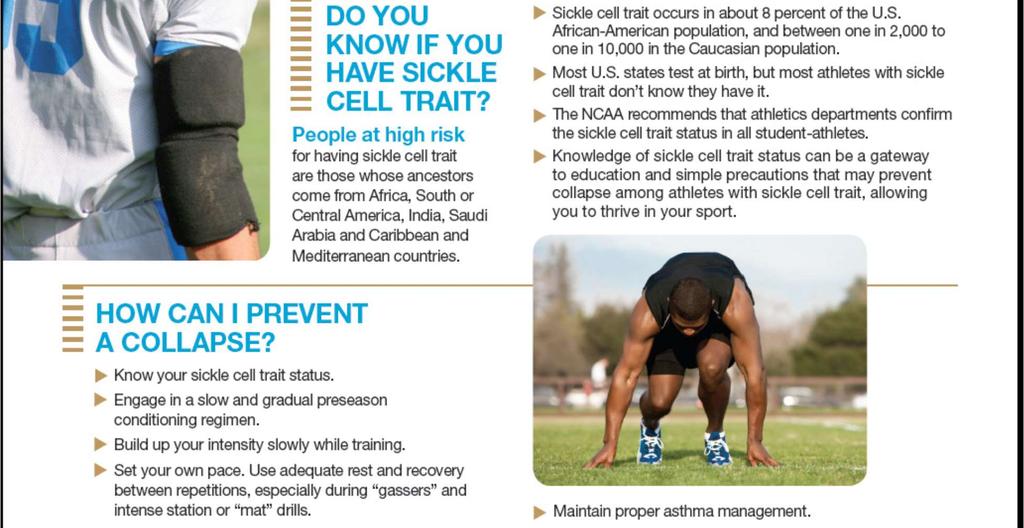
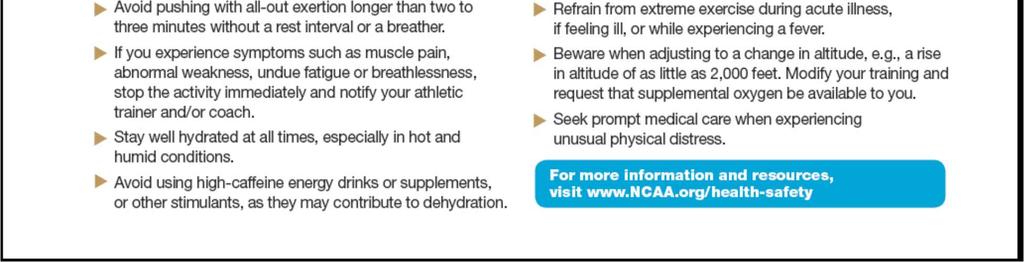
5 Sickle Cell Fact Sheet About Sickle Cell Trait- Sickle cell trait is an inherited condition of the oxygen-carrying protein, hemoglobin, in the red blood cells. Sickle cell trait is a common condition (> three million Americans) Although Sickle cell trait is most predominant in African-Americans and those of Mediterranean, Middle Eastern, Indian, Caribbean, and South and Central American ancestry, persons of all races and ancestry may test positive for sickle cell trait. Sickle cell trait is usually benign, but during intense, sustained exercise, hypoxia (lack of oxygen) in the muscles may cause sickling of red blood cells (red blood cells changing from a normal disc shape to a crescent or sickle shape), which can accumulate in the bloodstream and logjam blood vessels, leading to collapse from the rapid breakdown of muscles starved of blood. Sickle Cell Trait Testing- The NCAA mandates that all student-athletes have knowledge of their sickle cell trait status, show proof of a prior test or sign a testing waiver before the student-athlete participates in any intercollegiate athletics event, including strength and conditioning sessions, practices, competitions, etc. SICKLE CELL TRAIT TESTING WAIVER I,, understand and acknowledge that the NCAA mandates that all studentathletes have knowledge of their sickle cell trait status. Additionally, I have read and fully understand the aforementioned facts and the University policy about sickle cell trait and sickle cell trait testing. Recognizing that my true physical condition is dependent upon an accurate medical history and a full disclosure of any symptoms, complaints, prior injuries, ailments, and/or disabilities experienced, I hereby affirm that I have fully disclosed in writing any prior medical history and/or knowledge of sickle cell trait status to University of Connecticut Department of Sports Medicine personnel. I do not wish to undergo sickle cell trait testing and I voluntarily agree to release, discharge, indemnify and hold harmless the State of Connecticut, the University, its officers, employees, agents and their successors and assigns from any and all costs, claims, damages or expenses, including attorneys fees, arising from any loss or personal injury that might result from my non-compliance with the mandate of the NCAA. I have read and signed this document with full knowledge of its significance. I further state that I am at least 18 years of age and competent to sign this waiver. Student-Athlete Signature Parent/Guardian Signature (if under 18 years of age) Parent/Guardian Print Name Witness Sport Sport
The University of Michigan
 Tryout Directions and Information: The University of Michigan This packet contains the following forms that must be completed before your tryout can begin: Tryout clearance form You only need to fill out
Tryout Directions and Information: The University of Michigan This packet contains the following forms that must be completed before your tryout can begin: Tryout clearance form You only need to fill out
SICKLE CELL TRAIT DOCUMENTATION (6/11)
") SICKLE CELL TRAIT DOCUMENTATION Because of the health related issues stemming from possible outcomes of blood cell sickling in the athletic population, the NCAA is recommending documentation of testing
SICKLE CELL TRAIT DOCUMENTATION Because of the health related issues stemming from possible outcomes of blood cell sickling in the athletic population, the NCAA is recommending documentation of testing
University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS
 Name (Last, First, MI) University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS of Birth Address Sex M / F Sport Phone City State Zip
Name (Last, First, MI) University of Nebraska Omaha Athletic Performance Pre-Participation Medical History & Physical Examination Form TEAM TRYOUTS of Birth Address Sex M / F Sport Phone City State Zip
INTERCOLLEGIATE ATHLETICS RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST
 RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, Welcome back to Aberdeen. We are excited to see you return to continue your pursuit of athletic excellence and academic success.
RETURNING STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, Welcome back to Aberdeen. We are excited to see you return to continue your pursuit of athletic excellence and academic success.
CONTENTS ALL PARTS OF THIS PACKET ARE IMPORTANT, AND IT MUST BE COMPLETED IN ITS ENTIRETY!
 2017-18 Point Park University Athletics Medical Packet Enclosed you will find many of the necessary forms needed to compete in intercollegiate athletics during the 2017-18 year. Please return all completed
2017-18 Point Park University Athletics Medical Packet Enclosed you will find many of the necessary forms needed to compete in intercollegiate athletics during the 2017-18 year. Please return all completed
Spring Hill College Athletic Training Department NCAA Division II Tryout
 Dear Parent/Guardian: Spring Hill College Athletic Training Department NCAA Division II Tryout I want to first welcome you to Spring Hill College and its athletic department; this is an exciting time for
Dear Parent/Guardian: Spring Hill College Athletic Training Department NCAA Division II Tryout I want to first welcome you to Spring Hill College and its athletic department; this is an exciting time for
TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT
 TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT To be completed by Student prior to tryout Name Date Date of Birth Sport School Currently Attending Registered with NCAA Eligibility Center o Yes o No
TRYOUT REQUEST COVERSHEET FOR PROSPECTIVE STUDENT To be completed by Student prior to tryout Name Date Date of Birth Sport School Currently Attending Registered with NCAA Eligibility Center o Yes o No
NCAA Sports. Participation Forms. Required for Participation in NCAA Sports BRYN ATHYN COLLEGE HEALTH SERVICES 2945 COLLEGE DRIVE, BRYN ATHYN PA 19009
 NCAA Sports Participation Forms Required for Participation in NCAA Sports BRYN ATHYN COLLEGE HEALTH SERVICES 2945 COLLEGE DRIVE, BRYN ATHYN PA 19009 (Page 1 of 6) Athletic Department Participation Agreement,
NCAA Sports Participation Forms Required for Participation in NCAA Sports BRYN ATHYN COLLEGE HEALTH SERVICES 2945 COLLEGE DRIVE, BRYN ATHYN PA 19009 (Page 1 of 6) Athletic Department Participation Agreement,
ETSU Athletic Training Jerry Robertson BucSports Athletic Medicine Center
 To: Potential ETSU Student Athlete From: Nathan Barger, MA, ATC Assistant Athletic Trainer for Football Re: Athletic Training Room Physical Paperwork Thank you for your interest in East Tennessee State
To: Potential ETSU Student Athlete From: Nathan Barger, MA, ATC Assistant Athletic Trainer for Football Re: Athletic Training Room Physical Paperwork Thank you for your interest in East Tennessee State
FRESHMEN/TRANSFER STUDENT CHECKLIST
 FRESHMEN/TRANSFER STUDENT CHECKLIST Pre Participation Questionnaire Medical Consent Form Insurance Form Please include a copy of the FRONT and BACK of your insurance card. Pre Participation Physical Form
FRESHMEN/TRANSFER STUDENT CHECKLIST Pre Participation Questionnaire Medical Consent Form Insurance Form Please include a copy of the FRONT and BACK of your insurance card. Pre Participation Physical Form
MEDICAL CLEARANCE FOR ATHLETIC TRYOUTS
 MEDICAL CLEARANCE FOR ATHLETIC TRYOUTS "Tryouts" are individuals whose athletic skills are being evaluated by the coaching staff. BEFORE YOU TRY OUT: A general physical examination by a physician is required.
MEDICAL CLEARANCE FOR ATHLETIC TRYOUTS "Tryouts" are individuals whose athletic skills are being evaluated by the coaching staff. BEFORE YOU TRY OUT: A general physical examination by a physician is required.
DON T WAIT: SUBMIT YOUR HEALTH FORMS AND COMPLETE YOUR ONLINE HEALTH INSURANCE WAIVER!
 DON T WAIT: SUBMIT YOUR HEALTH FORMS AND COMPLETE YOUR ONLINE HEALTH INSURANCE WAIVER! A critical next step in becoming a student at Western New England University is making sure you have submitted all
DON T WAIT: SUBMIT YOUR HEALTH FORMS AND COMPLETE YOUR ONLINE HEALTH INSURANCE WAIVER! A critical next step in becoming a student at Western New England University is making sure you have submitted all
We are looking for personality, strong pom, jazz, and hip hop backgrounds and mature, natural expression through dance.
 Our team is made up of talented, dynamic dancers from diverse backgrounds. We are looking for dancers that are well-rounded in different styles, understand and appreciate MSU Athletics and want to be an
Our team is made up of talented, dynamic dancers from diverse backgrounds. We are looking for dancers that are well-rounded in different styles, understand and appreciate MSU Athletics and want to be an
Send Completed Forms:
 Health Forms Due: August 1 (Spring Registration, January 3) DON T WAIT: SUBMIT YOUR HEALTH FORMS AND COMPLETE YOUR ONLINE HEALTH INSURANCE WAIVER! A critical next step in becoming a student at Western
Health Forms Due: August 1 (Spring Registration, January 3) DON T WAIT: SUBMIT YOUR HEALTH FORMS AND COMPLETE YOUR ONLINE HEALTH INSURANCE WAIVER! A critical next step in becoming a student at Western
NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies
 NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies INSTRUCTIONS Instructions for the Educational Organization (Applicant)
NCAA, NAIA, or NJCAA Intercollegiate Football: Traumatic Brain Injury Supplemental Warranty Application for New and Renewal Policies INSTRUCTIONS Instructions for the Educational Organization (Applicant)
Radford Athletic Department Tryout Clearance Form
 Radford Athletic Department Tryout Clearance Form This form is to be utilized for all student-athletes who are not on the official team roster after reporting for the fall team meetings. The student-athlete
Radford Athletic Department Tryout Clearance Form This form is to be utilized for all student-athletes who are not on the official team roster after reporting for the fall team meetings. The student-athlete
NAME: SEX: AGE: DATE OF BIRTH: CLASSIFICATION SPORT(S): HOME ADDRESS: PRIMARY PHONE:
: HOME ADDRESS: PRIMARY PHONE:") BETHEL UIVERSITY PREPARTICIPATIO EVALUATIO DATE OF EXAM: HISTORY FORM AME: SEX: AGE: DATE OF BIRTH: CLASSIFICATIO SPORT(S): HOME ADDRESS: PRIMARY PHOE: PERSOAL PHYSICIA: PROVIDER PHOE UMBER STATE/ COUTRY
BETHEL UIVERSITY PREPARTICIPATIO EVALUATIO DATE OF EXAM: HISTORY FORM AME: SEX: AGE: DATE OF BIRTH: CLASSIFICATIO SPORT(S): HOME ADDRESS: PRIMARY PHOE: PERSOAL PHYSICIA: PROVIDER PHOE UMBER STATE/ COUTRY
Waiver, Release and Hold Harmless Agreement Personal Training Services
 Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
Intercollegiate Athletics Pre-Participation Packet
 Intercollegiate Athletics Pre-Participation Packet The sports medicine staff is comprised of athletic trainers who are members of the National Athletic Trainers, certified by the Board of Certification,
Intercollegiate Athletics Pre-Participation Packet The sports medicine staff is comprised of athletic trainers who are members of the National Athletic Trainers, certified by the Board of Certification,
PROGRAM YEAR 2018 REGISTRATION PACKAGE
 PROGRAM YEAR 2018 REGISTRATION PACKAGE Full Stride Track Club is a competitive track club for Contra Costa and Solano County youth ages 5 to 18 years old. We are committed to providing our youth with a
PROGRAM YEAR 2018 REGISTRATION PACKAGE Full Stride Track Club is a competitive track club for Contra Costa and Solano County youth ages 5 to 18 years old. We are committed to providing our youth with a
P: F: balance. Some exercise equipment will be used such as treadmills, NuSteps and resistance devices.
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
P: F: Session Information Sessions are held quarterly, registration is ongoing. Monday, Wednesday 2:00PM 3:00PM
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
P: F:
 Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
Intercollegiate Athletics Pre-Participation Packet
 Intercollegiate Athletics Pre-Participation Packet The sports medicine staff is comprised of athletic trainers who are members of the National Athletic Trainers, certified by the Board of Certification,
Intercollegiate Athletics Pre-Participation Packet The sports medicine staff is comprised of athletic trainers who are members of the National Athletic Trainers, certified by the Board of Certification,
EXTERNAL TRAINER AGREEMENT. THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and -
 - and -") EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - 2566588 Ontario Ltd. operating as Fortis Fitness West (2566588 Ontario Ltd. operating as Fortis
EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - 2566588 Ontario Ltd. operating as Fortis Fitness West (2566588 Ontario Ltd. operating as Fortis
City of Carson 701 E. Carson St., Carson, CA Telephone: (310) ; ci.carson.ca.us
 ; ci.carson.ca.us") OFFICE USE ONLY Case No. City of Carson 701 E. Carson St., Carson, CA 90745 Telephone: (310) 830-7600; ci.carson.ca.us Application Submittal Date Fee Accepted By SUPPLEMENTAL APPLICATION FOR COMMERCIAL
OFFICE USE ONLY Case No. City of Carson 701 E. Carson St., Carson, CA 90745 Telephone: (310) 830-7600; ci.carson.ca.us Application Submittal Date Fee Accepted By SUPPLEMENTAL APPLICATION FOR COMMERCIAL
EXTERNAL TRAINER AGREEMENT. THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and -
 - and -") EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - Fortis Fitness Inc. (Fortis Fitness Inc. or Fortis Fitness or the Companies ) This Agreement
EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - Fortis Fitness Inc. (Fortis Fitness Inc. or Fortis Fitness or the Companies ) This Agreement
Tomorrow s SMILES Program
 Do you know a promising teen whose future is at-risk due to lack of dental treatment? Would your teen and his or her family understand, appreciate, and value pro-bono dental care? If so, your teen may
Do you know a promising teen whose future is at-risk due to lack of dental treatment? Would your teen and his or her family understand, appreciate, and value pro-bono dental care? If so, your teen may
Rhode Island College Student-Athletes, Parents or Guardians. FROM: Athletic Training/Sports Medicine Department. Athletic Insurance Information
 TO: Rhode Island College Student-Athletes, Parents or Guardians FROM: Athletic Training/Sports Medicine Department RE: Athletic Insurance Information We are pleased to have you/your son/daughter participating
TO: Rhode Island College Student-Athletes, Parents or Guardians FROM: Athletic Training/Sports Medicine Department RE: Athletic Insurance Information We are pleased to have you/your son/daughter participating
A Tradition of Excellence
 A Tradition of Excellence November 7 2017 Via Electronic Mail Donald P O Neil RE: 17-77 Response to FOIA Request Thank you for writing to Hinsdale Township High School District 86 with your request for
A Tradition of Excellence November 7 2017 Via Electronic Mail Donald P O Neil RE: 17-77 Response to FOIA Request Thank you for writing to Hinsdale Township High School District 86 with your request for
JDRF Oklahoma. Youth Ambassador Program 2017 Promise Ball 20 th Anniversary. Information Packet
 JDRF Oklahoma Youth Ambassador Program 2017 Promise Ball 20 th Anniversary Information Packet Dear Prospective JDRF Youth Ambassador: I am writing to invite you to participate in the 2017 JDRF Youth Ambassador
JDRF Oklahoma Youth Ambassador Program 2017 Promise Ball 20 th Anniversary Information Packet Dear Prospective JDRF Youth Ambassador: I am writing to invite you to participate in the 2017 JDRF Youth Ambassador
Administering Medicines to Students Asthma Inhaler Exemption
 Administering Medicines to Students Asthma Inhaler Exemption Any school employee authorized in writing by the district administrator or school principal: 1. May assist in the self-administration of any
Administering Medicines to Students Asthma Inhaler Exemption Any school employee authorized in writing by the district administrator or school principal: 1. May assist in the self-administration of any
Student Wellness Services-Health
 Student Wellness Services-Health Welcome Varsity Athlete, As your health and safety are of the utmost importance you must receive medical clearance from our office, CCSU Student Wellness Services-Health,
Student Wellness Services-Health Welcome Varsity Athlete, As your health and safety are of the utmost importance you must receive medical clearance from our office, CCSU Student Wellness Services-Health,
Please complete the medical history section below so that we can be sure to respond to any
 200hr Yoga Teacher Training Application Please fill out this form and email it to teachertraining@ahamyoga.com with Teacher training application 2016 as the subject line. Any enrollments without this form
200hr Yoga Teacher Training Application Please fill out this form and email it to teachertraining@ahamyoga.com with Teacher training application 2016 as the subject line. Any enrollments without this form
Jumpstart, Fitness Assessment, & Body Composition
 Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Client Intake Form - Therapeutic Massage
 Client Intake Form - Therapeutic Massage Personal Information: Date: Name: Phone #: Address: City/State/Zip: Email: DOB: Occupation: Emergency Contact: Phone #: HOW DID YOU HEAR ABOUT US? The following
Client Intake Form - Therapeutic Massage Personal Information: Date: Name: Phone #: Address: City/State/Zip: Email: DOB: Occupation: Emergency Contact: Phone #: HOW DID YOU HEAR ABOUT US? The following
Personal Training Information Packet
 Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event**
 Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event** The Autism Society of Greater Orlando is hosting its 13 th Annual Autism Walk & Family Fun Day inside
Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event** The Autism Society of Greater Orlando is hosting its 13 th Annual Autism Walk & Family Fun Day inside
Release & Waiver Synergy Studio
 Release & Waiver Synergy Studio I,, have enrolled in a program of physical activity, including but not limited to, body conditioning machinery used during the workouts offered by Synergy Studio. I affirm
Release & Waiver Synergy Studio I,, have enrolled in a program of physical activity, including but not limited to, body conditioning machinery used during the workouts offered by Synergy Studio. I affirm
4. ADD/ADHD Medical Documentation Athlete is responsible for reading, completing, and providing required documentation.
 LAST NAME FIRST SPORT Returning Student-Athlete Health Information ONLY complete this booklet if you play varsity men s or women s soccer, women s volleyball, men s golf, men s or women s swimming, men
LAST NAME FIRST SPORT Returning Student-Athlete Health Information ONLY complete this booklet if you play varsity men s or women s soccer, women s volleyball, men s golf, men s or women s swimming, men
Talisman Therapeutic Riding, Inc. PO Box 300, Grasonville, MD
 Volunteer Application (Page 1 of 6) General Information Form - Please Print Clearly and Complete Fully (Last Name) (First Name) (Middle Initial) (Nickname) Street Address: City: State: Zip Code: Home Phone:
Volunteer Application (Page 1 of 6) General Information Form - Please Print Clearly and Complete Fully (Last Name) (First Name) (Middle Initial) (Nickname) Street Address: City: State: Zip Code: Home Phone:
VARSITY AND CLUB SPORTS PACKET
 VARSITY AND CLUB SPORTS PACKET If you are planning to participate or feel that there is a possibility that you might participate in a Varsity or Club Sports you must submit all the documents listed below.
VARSITY AND CLUB SPORTS PACKET If you are planning to participate or feel that there is a possibility that you might participate in a Varsity or Club Sports you must submit all the documents listed below.
Please everything to the address below: ITEMS TO MAIL. 1. Copy of the athletes immunization record
 In order to participate in the Syracuse Indoor Showcase each player will need to EMAIL all the items below upon completion of their online registration. Your registration/spot in the showcase is not complete
In order to participate in the Syracuse Indoor Showcase each player will need to EMAIL all the items below upon completion of their online registration. Your registration/spot in the showcase is not complete
Increase Your Speed!!!
 www.ashevillephysicaltherapy.com Increase Your Speed!!! (Mon Thur) June 20-23 July 18-21 Aug 1-4 Ages: 10 13 Ages: 14 18+ 9:00 10:30 am 4:00 5:30 pm Early Registration: $69! Contrary to popular belief,
www.ashevillephysicaltherapy.com Increase Your Speed!!! (Mon Thur) June 20-23 July 18-21 Aug 1-4 Ages: 10 13 Ages: 14 18+ 9:00 10:30 am 4:00 5:30 pm Early Registration: $69! Contrary to popular belief,
Personal Training Health Screening Questionnaire
 RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
Operation Screen Your Athlete Medical Questionnaire
 Operation Screen Your Athlete Medical Questionnaire PLEASE PRINT Athlete s Name: DOB: / / Male Female Street Address: School Attending: Parent/Guardian Name: Parent/Guardian Email: Parents please fill
Operation Screen Your Athlete Medical Questionnaire PLEASE PRINT Athlete s Name: DOB: / / Male Female Street Address: School Attending: Parent/Guardian Name: Parent/Guardian Email: Parents please fill
CITY OF PINOLE TINY TOTS PROGRAM REGISTRATION AND EMERGENCY FORM
 CITY OF PINOLE TINY TOTS PROGRAM REGISTRATION Child's Name Date of Birth Parent/Guardian's Full Name Address Street: Address Line 2: City, State, Zip: Phone ( ) - Email EMERGENCY CONTACT INFORMATION OTHER
CITY OF PINOLE TINY TOTS PROGRAM REGISTRATION Child's Name Date of Birth Parent/Guardian's Full Name Address Street: Address Line 2: City, State, Zip: Phone ( ) - Email EMERGENCY CONTACT INFORMATION OTHER
Department of Campus Recreation: SouthFit Personal Training
 Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Washington County-Johnson City Health Department Christen Minnick, MPH, Director 219 Princeton Road Johnson City, Tennessee Phone:
 Washington County-Johnson City Health Department Christen Minnick, MPH, Director 219 Princeton Road Johnson City, Tennessee 37601 Phone: 423-975-2200 Dear Parent: The Washington County Health Department
Washington County-Johnson City Health Department Christen Minnick, MPH, Director 219 Princeton Road Johnson City, Tennessee 37601 Phone: 423-975-2200 Dear Parent: The Washington County Health Department
Grasso Technical High School Athlete Eligibility Packet Sign-off. Student Name: Grade: Sport:
 Grasso Technical High School Athlete Eligibility Packet Sign-off Student Name: Grade: Sport: All students and parents must read and sign all attached documents and parents must sign this cover sheet in
Grasso Technical High School Athlete Eligibility Packet Sign-off Student Name: Grade: Sport: All students and parents must read and sign all attached documents and parents must sign this cover sheet in
Baby-Sitting - $20 Per Day/Per Nanny (local clients) Less than 24 hours notice $30 Per Day/Per Nanny. Hotel Overnight Sitting - $35 per Day/Per Nanny
 Less than 24 hours notice $30 Per Day/Per Nanny. Hotel Overnight Sitting - $35 per Day/Per Nanny") ALL ABOUT NANNIES BUSINESS PHONE: 602-266-9116 BUSINESS FACSIMILE: 602-266-9787 BUSINESS EMAIL: ADMIN@ALLABOUTNANNIESINC.COM TEMPORARY, BABY-SITTING, HOTEL & ON-CALL AS NEEDED Mother s Full Name: Place
ALL ABOUT NANNIES BUSINESS PHONE: 602-266-9116 BUSINESS FACSIMILE: 602-266-9787 BUSINESS EMAIL: ADMIN@ALLABOUTNANNIESINC.COM TEMPORARY, BABY-SITTING, HOTEL & ON-CALL AS NEEDED Mother s Full Name: Place
APPLICATION INSTRUCTIONS
 APPLICATION INSTRUCTIONS TEACHER TRAINING PROGRAMS Application Deadlines To process your application, please send your complete application no later than one week prior to the program start date. However,
APPLICATION INSTRUCTIONS TEACHER TRAINING PROGRAMS Application Deadlines To process your application, please send your complete application no later than one week prior to the program start date. However,
East Stroudsburg University Athletic Training Medical Forms Information and Directions
 East Stroudsburg University Athletic Training Medical Forms Information and Directions 2013 2014 All student athletes must complete all medical information forms on the ATS Webportal by July 27 th, 2013.
East Stroudsburg University Athletic Training Medical Forms Information and Directions 2013 2014 All student athletes must complete all medical information forms on the ATS Webportal by July 27 th, 2013.
Celebration Lutheran School
 Celebration Lutheran School Wisconsin Interscholastic Athletic Association Athletic History and Physical Examination Approval for TWO YEARS of Competition All students participating in interscholastic
Celebration Lutheran School Wisconsin Interscholastic Athletic Association Athletic History and Physical Examination Approval for TWO YEARS of Competition All students participating in interscholastic
Cougar Employee Wellness Program WASHINGTON STATE UNIVERSITY
 Cougar Employee Wellness Program WASHINGTON STATE UNIVERSITY Participant Waiver I,, a WSU employee, wish to voluntarily participate in the WSU Cougar Employee Wellness Program (CEWP). In consideration
Cougar Employee Wellness Program WASHINGTON STATE UNIVERSITY Participant Waiver I,, a WSU employee, wish to voluntarily participate in the WSU Cougar Employee Wellness Program (CEWP). In consideration
Participant Information Exercise Equivalent Chart Weekly Activity Log Participation Agreement Waiver and Indemnity Agreement
 Participant Information Email Exercise Equivalent Chart Weekly Activity Log Participation Agreement Waiver and Indemnity Agreement PLEASE POST THIS EMAIL ON COMMON USE AREA BULLETIN BOARDS AT YOUR UNIT
Participant Information Email Exercise Equivalent Chart Weekly Activity Log Participation Agreement Waiver and Indemnity Agreement PLEASE POST THIS EMAIL ON COMMON USE AREA BULLETIN BOARDS AT YOUR UNIT
*To reserve your place in the training, you must submit the completed application along with a minimum
 APPLICATION INSTRUCTIONS The Epídavros Teacher Training programs includes a vigorous two-hour asana practice. We strongly recommend that applicants have one year of consistent asana practice. If your yoga
APPLICATION INSTRUCTIONS The Epídavros Teacher Training programs includes a vigorous two-hour asana practice. We strongly recommend that applicants have one year of consistent asana practice. If your yoga
Mount Morris Central School. Fitness Room. Procedures, Rules, and Required Forms
 Mount Morris Central School Fitness Room Procedures, Rules, and Required Forms Where is the Fitness Room Located? The Mount Morris Central School fitness room is located across from the new gymnasium.
Mount Morris Central School Fitness Room Procedures, Rules, and Required Forms Where is the Fitness Room Located? The Mount Morris Central School fitness room is located across from the new gymnasium.
City of Norwalk Recreation Department. Concussion Guidelines for Youth Athletics
 City of Norwalk Recreation Department Concussion Guidelines for Youth Athletics I. INTRODUCTION. In recognition of the dangers posed to youth athletes as a result of sports related head injuries, the City
City of Norwalk Recreation Department Concussion Guidelines for Youth Athletics I. INTRODUCTION. In recognition of the dangers posed to youth athletes as a result of sports related head injuries, the City
Application for Cadet Membership
 Application for Cadet Membership 275 West Main Street P.O. Box 309 Braidwood, IL 60408 815-458-2000 Name: (Print Neatly) Introduction The Braidwood Fire Department consists of dedicated men and women who
Application for Cadet Membership 275 West Main Street P.O. Box 309 Braidwood, IL 60408 815-458-2000 Name: (Print Neatly) Introduction The Braidwood Fire Department consists of dedicated men and women who
DIOCESE OF CORPUS CHRISTI
 Office of Youth Ministry DIOCESE OF CORPUS CHRISTI PO Box 2620 Corpus Christi, Texas 78403 (361) 882-6191 Fax (361) 693-6787 www.diocesecc.org/youth YouthOffice@diocesecc.org DIOCESAN CONFIRMATION RETREATS
Office of Youth Ministry DIOCESE OF CORPUS CHRISTI PO Box 2620 Corpus Christi, Texas 78403 (361) 882-6191 Fax (361) 693-6787 www.diocesecc.org/youth YouthOffice@diocesecc.org DIOCESAN CONFIRMATION RETREATS
1 st Thursday Participation Benefits
 Participation Benefits 1 st Thursday was started by Downtown Santa Barbara (DSB) in February 2007 and has since significantly grown in popularity and visibility in the community and beyond. 1 st Thursday
Participation Benefits 1 st Thursday was started by Downtown Santa Barbara (DSB) in February 2007 and has since significantly grown in popularity and visibility in the community and beyond. 1 st Thursday
CAMP LOCATIONS CAMP STAFF. You can be young, have diabetes and still have FUN. Exercise and a good diet should be part of your life
 ELIGIBILITY Moses E. Cheeks Slam Dunk for Diabetes Basketball Camp is for children and young adults ages 5-18 years old who have been medically diagnosed with diabetes and prediabetes. Please submit your
ELIGIBILITY Moses E. Cheeks Slam Dunk for Diabetes Basketball Camp is for children and young adults ages 5-18 years old who have been medically diagnosed with diabetes and prediabetes. Please submit your
APPLICATION FOR SERVICES
 APPLICATION FOR SERVICES CLIENT - PERSONAL INFORMATION First Name M.I. Last Name Today s Street Address City State Zip Birth date Home phone (ok to leave msg? Y - N) Cell phone (ok to leave msg? Y - N
APPLICATION FOR SERVICES CLIENT - PERSONAL INFORMATION First Name M.I. Last Name Today s Street Address City State Zip Birth date Home phone (ok to leave msg? Y - N) Cell phone (ok to leave msg? Y - N
Personal Training Intake Form
 Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Phlebotomy Health Requirements Checklist
 Phlebotomy Health Requirements Checklist The applicant must: 1). Upload the original completed form to your CertifiedBackground profile. 2). Retain a copy for your records. www.certifiedbackground.com
Phlebotomy Health Requirements Checklist The applicant must: 1). Upload the original completed form to your CertifiedBackground profile. 2). Retain a copy for your records. www.certifiedbackground.com
The Society of St. Vincent de Paul. Riverwalk. San Marcos, TX
 The Society of St. Vincent de Paul Riverwalk San Marcos, TX Saturday October 1, 2016 The Society of St. Vincent de Paul 624 East Hopkins Street San Marcos, Texas 78666 512-353-7394 River Walk for the Poor
The Society of St. Vincent de Paul Riverwalk San Marcos, TX Saturday October 1, 2016 The Society of St. Vincent de Paul 624 East Hopkins Street San Marcos, Texas 78666 512-353-7394 River Walk for the Poor
Notre Dame of Maryland University Athletics Concussion Management Protocol
 Notre Dame of Maryland University Athletics Concussion Management Protocol Neuropsychological (NP) Baseline Testing: All NCAA sports will utilize baseline NP testing. All athletes will receive baseline
Notre Dame of Maryland University Athletics Concussion Management Protocol Neuropsychological (NP) Baseline Testing: All NCAA sports will utilize baseline NP testing. All athletes will receive baseline
(City, State, Zip Code)
") This Partner Agency Agreement, dated this day of, 2015, is between COMMUNITY FOOD SHARE, INC. (CFS), whose address is 650 South Taylor Avenue, Louisville, CO 80027, and (Partner Agency) whose address is
This Partner Agency Agreement, dated this day of, 2015, is between COMMUNITY FOOD SHARE, INC. (CFS), whose address is 650 South Taylor Avenue, Louisville, CO 80027, and (Partner Agency) whose address is
Summer Youth Institute Packet
 Dear Prospective Youth Volunteer, Summer Youth Institute Packet Thank you for your interest in the Volunteers of America s Youth Volunteer Summer Institute! Volunteers of America is a national, non-profit,
Dear Prospective Youth Volunteer, Summer Youth Institute Packet Thank you for your interest in the Volunteers of America s Youth Volunteer Summer Institute! Volunteers of America is a national, non-profit,
Baa Hózhó Navajo Prep Math Summer Camp 2017
 Math Summer Camp 2017 Application Packet Grades 7-12 May 30-June 3, 2017 Navajo Preparatory School, Farmington, NM Residential Camp Application Checklist A complete application must include the following:
Math Summer Camp 2017 Application Packet Grades 7-12 May 30-June 3, 2017 Navajo Preparatory School, Farmington, NM Residential Camp Application Checklist A complete application must include the following:
Trees Hall. Bellefield Hall
 Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
2010 Sharing Hope Program for men
 2010 Sharing Hope Program for men Criteria and Application Made possible by participating sperm banks and fertility centers Program Overview Goal Cancer patients have little opportunity to save for the
2010 Sharing Hope Program for men Criteria and Application Made possible by participating sperm banks and fertility centers Program Overview Goal Cancer patients have little opportunity to save for the
AFFILIATION PROGRAM AGREEMENT
 AFFILIATION PROGRAM AGREEMENT This AFFILIATION PROGRAM AGREEMENT (this Agreement ) is made and entered into by and between FACULTY PHYSICIANS & SURGEONS OF LLUSM dba LOMA LINDA UNIVERSITY FACULTY MEDICAL
AFFILIATION PROGRAM AGREEMENT This AFFILIATION PROGRAM AGREEMENT (this Agreement ) is made and entered into by and between FACULTY PHYSICIANS & SURGEONS OF LLUSM dba LOMA LINDA UNIVERSITY FACULTY MEDICAL
INTERCOLLEGIATE ATHLETICS NEW STUDENT-ATHLETE MEDICAL FORMS CHECKLIST
 NEW STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, On behalf of the Athletic Training Department, I would like to welcome to Aberdeen and the Presentation College campus. We are excited
NEW STUDENT-ATHLETE MEDICAL FORMS CHECKLIST Dear PC Student-Athletes, On behalf of the Athletic Training Department, I would like to welcome to Aberdeen and the Presentation College campus. We are excited
Jones Co. Jr. College Sports Medicine Medical History Questionairre
 Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
Jones Co. Jr. College Sports Medicine Medical History Questionairre DEMOGRAPHIC INFORMATION Full Name: Social Security #: - - Date of Birth: Sport: Year in School: Home Phone #: Cell Phone #: Parent/Guardian
OAKLAND UNIVERSITY INTERCOLLEGIATE ATHLETIC MEDICAL INSURANCE
 OAKLAND UNIVERSITY INTERCOLLEGIATE ATHLETIC MEDICAL INSURANCE We are extremely pleased to have your son/daughter as a student-athlete at Oakland University and hope that he/she will achieve academic, social,
OAKLAND UNIVERSITY INTERCOLLEGIATE ATHLETIC MEDICAL INSURANCE We are extremely pleased to have your son/daughter as a student-athlete at Oakland University and hope that he/she will achieve academic, social,
Checklist Creating an Athletics Concussion Management Plan
 Checklist Creating an Athletics Concussion Management Plan Intro text No athletic safety issue has garnered more attention recently than concussions, a type of mild traumatic brain injury (TBI). The potential
Checklist Creating an Athletics Concussion Management Plan Intro text No athletic safety issue has garnered more attention recently than concussions, a type of mild traumatic brain injury (TBI). The potential
Exhibitor/Vendor Prospectus
 Sickle Cell Disease Association of America, Inc. 5th Annual National Sickle Cell Walk with the Stars & Move-a-thon Canton Waterfront Park, Baltimore, MD August 18, 2018 Exhibitor/Vendor Prospectus SCDAA
Sickle Cell Disease Association of America, Inc. 5th Annual National Sickle Cell Walk with the Stars & Move-a-thon Canton Waterfront Park, Baltimore, MD August 18, 2018 Exhibitor/Vendor Prospectus SCDAA
(FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:
 (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE:") PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
PATIENT INFORMATION EMAIL: MARITAL STATUS: [ ]MARRIED [ ]SINGLE [ ]DIVORCED [ ]WIDOWED NAME: (FIRST) (MIDDLE) (LAST) STREET: CITY: STATE: ZIP CODE: DOB: PHONE: [ ]Home [ ]Work [ ]Cell PHONE: [ ]Home [
TEACHER TRAINING APPLICATION
 Introduction TEACHER TRAINING APPLICATION Thank you for your interest in the Hot 8 Yoga Teacher Training Program! Below you will find detailed instructions on how to apply. Please be aware that the Hot
Introduction TEACHER TRAINING APPLICATION Thank you for your interest in the Hot 8 Yoga Teacher Training Program! Below you will find detailed instructions on how to apply. Please be aware that the Hot
Completed applications can be submitted either by mail or to:
 Dear Sir or Madam: Thank you for your interest in the Feldenkrais Foundation s Low Fee Clinic. This popular clinic provides individual Feldenkrais Functional Integration sessions at a reduced rate for
Dear Sir or Madam: Thank you for your interest in the Feldenkrais Foundation s Low Fee Clinic. This popular clinic provides individual Feldenkrais Functional Integration sessions at a reduced rate for
WV Address WV Phone # Father / Male Guardian Information (required) Work Phone # Home Phone # Cell Phone # Home Address (if different)
 Work Phone # Home Phone # Cell Phone # Home Address (if different)") 2016 Freestyle/Freeski BagJump/Trampoline Skills Training Sessions & 6 Day Camp Application For each athlete, please complete, sign and return all pages of this application and include payment in full
2016 Freestyle/Freeski BagJump/Trampoline Skills Training Sessions & 6 Day Camp Application For each athlete, please complete, sign and return all pages of this application and include payment in full
th Street Urbandale, IA YOST
 YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
YfC 3993 100th Street Urbandale, IA 50322 515.278.YOST www.yostfamilychiropractic.com Demographics: Language (Primary) Race: Unspecified American Indian or Alaska Native Black or African American Other
Personal Training Registration Packet
 Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
GAH Elite Performance Adult Personal Training Registration Date:
 GAH Elite Performance Adult Personal Training Registration : Name: Address: First Middle Last Street # City State Zip of Birth: Sex (M/F) Home Phone E-mail: Emergency contact name: phone: Are you training
GAH Elite Performance Adult Personal Training Registration : Name: Address: First Middle Last Street # City State Zip of Birth: Sex (M/F) Home Phone E-mail: Emergency contact name: phone: Are you training
Trees Hall. Bellefield Hall. Add a Fitness Center Membership for a small additional price!
 Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
Application to Livingston Robotics Club Season Part A: Student information. Name: (Student) Home Address:
 Home Address:") Due s: July 30, 2017 for FLL and FTC Mail to: P.O. Box 771, Livingston, NJ 07039 Email to info@livingstonrobotics.org Application to Livingston Robotics Club Part A: Student information Name: (Student)
Due s: July 30, 2017 for FLL and FTC Mail to: P.O. Box 771, Livingston, NJ 07039 Email to info@livingstonrobotics.org Application to Livingston Robotics Club Part A: Student information Name: (Student)
Part I: Concern About Sickle Cell and NCAA Testing
 Part I: Concern About Sickle Cell and NCAA Testing You are encouraged to work with other students, but each person must submit the assignment individually. There will be no group assessment on this assignment.
Part I: Concern About Sickle Cell and NCAA Testing You are encouraged to work with other students, but each person must submit the assignment individually. There will be no group assessment on this assignment.
Kairos 79 November (Seniors) Kairos 80 February19-22 (Seniors)
 Kairos 80 February19-22 (Seniors)") Kairos Retreats 2017-2018 There are 40 spaces available on each retreat, 20 for girls and 20 for boys. Don t delay! Sign up for the Kairos of your choice now! Kairos 79 November 19-22 (Seniors) Kairos
Kairos Retreats 2017-2018 There are 40 spaces available on each retreat, 20 for girls and 20 for boys. Don t delay! Sign up for the Kairos of your choice now! Kairos 79 November 19-22 (Seniors) Kairos
SMITH PHYSICAL THERAPY AND RUNNING ACADEMY, LLC PHYSICAL THERAPY PATIENT INFORMATION CITY: STATE: ZIP CODE:
 PHYSICAL THERAPY PATIENT INFORMATION DATE: NAME: DATE OF BIRTH: ADDRESS: CITY: STATE: ZIP CODE: *E-MAIL: HOW DID YOU HEAR ABOUT SMITH PHYSICAL THERAPY AND RUNNING ACADEMY? EMERGENCY CONTACT: REFERRING
PHYSICAL THERAPY PATIENT INFORMATION DATE: NAME: DATE OF BIRTH: ADDRESS: CITY: STATE: ZIP CODE: *E-MAIL: HOW DID YOU HEAR ABOUT SMITH PHYSICAL THERAPY AND RUNNING ACADEMY? EMERGENCY CONTACT: REFERRING
Health Unit Coordinator
 Health Unit Coordinator Health Requirements Checklist All MATC Health Science students are required to complete and upload health requirements prior to petitioning for courses which contain a clinical
Health Unit Coordinator Health Requirements Checklist All MATC Health Science students are required to complete and upload health requirements prior to petitioning for courses which contain a clinical
EMPLOYMENT APPLICATION
 15205 41 st Ave. SE, Bothell, WA 98012-6114 - P.O. Box 13888, Mill Creek, WA 98082-1888 Telephone (425) 337-3647 Facsimile (425) 337-4399 EMPLOYMENT APPLICATION An incomplete application may delay action
15205 41 st Ave. SE, Bothell, WA 98012-6114 - P.O. Box 13888, Mill Creek, WA 98082-1888 Telephone (425) 337-3647 Facsimile (425) 337-4399 EMPLOYMENT APPLICATION An incomplete application may delay action
City State Zip. Home Phone Mobile Phone. Can we text you appointment reminders? Yes / No If yes, who is your wireless carrier?
 CryoBoost Lubbock 5206 82 nd St., Suite 15 (inside Austin Chiropractic) CryoBoost Allen 801 S Greenville Ave., Suite 115 (inside Wellness) Physical Readiness Questionnaire Name Date Address City State
CryoBoost Lubbock 5206 82 nd St., Suite 15 (inside Austin Chiropractic) CryoBoost Allen 801 S Greenville Ave., Suite 115 (inside Wellness) Physical Readiness Questionnaire Name Date Address City State
Presbyterian Night Shelter Volunteer Application
 Presbyterian Night Shelter Volunteer Application Thank you for your interest in the Presbyterian Night Shelter (PNS). Please complete this application as well as the attached documents and return to: Presbyterian
Presbyterian Night Shelter Volunteer Application Thank you for your interest in the Presbyterian Night Shelter (PNS). Please complete this application as well as the attached documents and return to: Presbyterian
Personal Training New Client Packet Personal Training/Fit for Hire
 Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with
Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with