Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant
|
|
|
- Rodger Washington
- 6 years ago
- Views:
Transcription
1 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant

2 All medical RCC transfusions (but only 1 in 3 haematology or oncology cases) in 3 x one week periods Medical specialties include: haematology, oncology, acute medicine, general medicine, care of the elderly, cardiology, gastro-intestinal medicine, endocrinology, renal medicine, neurology, rheumatology, respiratory medicine
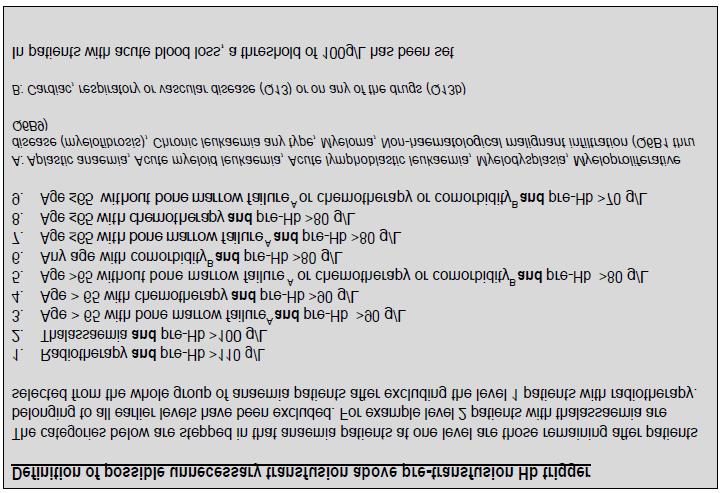
3 Audit standards 1. Pre-transfusion haemoglobin (Hb) taken within 3 days of transfusion (and preferably the same day) 2. No non-radiotherapy patient should have a pre-transfusion Hb >10g/dl 3. Post-transfusion Hb taken within 3 days of transfusion (and preferably the same day) 4. No non-radiotherapy patient should have a post-transfusion Hb >12 g/dl

4 Other parameters developed for the audit:
5

6
 2% - prophylaxis pre-procedure Median age was 73 yrs 53% M / 47% F 32% were haematology")
7 Results 9126 cases Primary reason for transfusion: 78% - anaemia (n=7128) 19% - blood loss (n=1773) 2% - prophylaxis pre-procedure Median age was 73 yrs 53% M / 47% F 32% were haematology cases
8 RCC units transfused per case
9 Results - audit standards 1. Pre-transfusion haemoglobin (Hb) taken within 3 days of transfusion (and preferably the same day) 93% compliance 2. No non-radiotherapy patient should have a pre-transfusion Hb >10g/dl 96.4% compliance 3. Post-transfusion Hb taken in within 3 days of transfusion (and preferably the same day) Within 3 days 84%, same day 12% 4. No non-radiotherapy patient should have a post-transfusion Hb >12 g/dl 94.1% compliance
10 Potentially avoidable transfusions 53% (4818/9126) of transfusions were considered potentially avoidable: 1. 20% (1791/9126) had a possible potentially reversible anaemia 2. 29% (2533/8820) were above the pre-transfusion Hb trigger(s) 3. 33% (2451/7437) were transfused to more than 2g/dl over the Hb threshold(s) 5% (403/8820) of cases fell in to both 1. & 2. above
11 Possible reversible anaemia Out of the 1791 identified as possible potentially reversible anaemia : 13% (n=1201) was possible iron deficiency 16% of F cases, 11% of M cases 3% was B12/folate deficiency 1.5% had positive direct antiglobulin test [possible autoimmune haemolytic anaemia] 3.2 % was egfr 30 [possible renal anaemia]
12 Transfusion above Hb trigger 34% of pt.s with anaemia 10% (n=106) of pt.s with blood loss [10g/dl]
13 Transfusion to >2g/dl above Hb trigger 40% of patients with anaemia 7% (n=116) of patients with blood loss [12g/dl]

14 3138 of the 4818 potentially avoidable transfusions were then randomly selected for further investigation Hospital based auditors asked to review patient notes to collect additional information, and conclude if the transfusion could have been avoided, or whether it was appropriate Further data was actually submitted on 1592 cases (51%)
15 Possible reversible anaemia 747 cases (out of the 1592 cases reported for part 2) 71% (n=527) had a documented reason for transfusion in the case notes:
 transfusion could have been")
16 Possible reversible anaemia 25% (n=187) transfusion could have been avoided:

17 Possible reversible anaemia Which service first noted the anaemia:
18 Possible reversible anaemia 372 patients had definite iron deficiency anaemia (out of the 552 possible cases identified in part 1) (64%) had a low ferritin - 37 (10%) had a transferrin saturation of <20% - 96 (26%) had a low MCV alone and no haematinic results Treatment of iron deficiency anaemia - 75% prescribed iron therapy (252 oral / 20 parenteral / 8 NK) - 37 (15%) of the 252 were intolerant to oral iron, but only 8 (22%) of these were given parenteral iron Also: - 63 patients were given dietary advice patient had treatment for an underlying GI disorder - 18 female patients received treatment for menorrhagia
19 Transfusion above Hb trigger 808 cases (32% of the 2533 cases identified in part 1) 438 (54%) had a documented reason for transfusion in the case notes and 338 (42%) did not [it was unclear in 32 cases]:
20 Transfusion above Hb trigger Transfusion was not appropriate in 220 (27%) of cases: - Of the 438 cases with a documented reason for transfusion, 365 (83%) were appropriately transfused - Of the 338 cases with no documented reason for transfusion, 156 (46%) were appropriately transfused
 Hb increment per unit transfused by ranges of body weight for patients transfused to more than 20g/L above")
21 Transfused to more than 2g/dl over Hb threshold 439 cases (18% of the 2451 cases identified in part 1) Significant correlation between body weight and Hb increment per unit transfused was found: the lower the body weight the larger the Hb increment Median (IQR) Hb increment per unit transfused by ranges of body weight for patients transfused to more than 20g/L above threshold
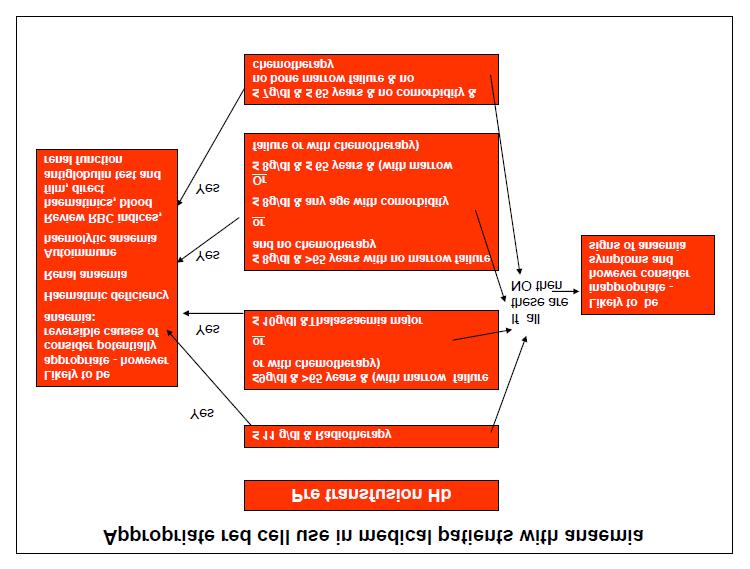
22 Conclusion [part 2] There is evidence of inappropriate use of blood in medical patients due to transfusion of patients with reversible anaemia, transfusion at a higher trigger threshold than required and over-transfusion. Unnecessary transfusion could be avoided by: - Recognising anaemia earlier and instituting appropriate investigation and management - Ensuring that the patient s symptoms and signs and the Hb level are taken into account and that this is documented in the notes - Introduction of more cautious use of multi-unit transfusion especially in those with low bodyweight; Clinical re-assessment and laboratory checks after each unit in smaller patients in particular would help to prevent over-transfusion; - An individualised approach to chronic transfusion-dependent patients
23 Recommendations [part 2] 1. Patients with medical conditions such as low grade chronic bleeding, malabsorption syndromes, and chronic renal impairment should be checked for anaemia. 2. Anaemia should be investigated for an underlying cause. 3. Patients should receive appropriate and timely treatment for anaemia to avoid unnecessary transfusion, e.g. parenteral iron for treatment of iron deficiency anaemia if it is not possible to use oral iron. 4. Patients should give valid consent to receive a transfusion which includes having the risks and benefits of transfusion explained and being offered alternatives to transfusion where relevant.
24 Recommendations [part 2] 5. The decision to transfuse must take into account the laboratory findings, the patient s symptoms and signs and the underlying cause for the anaemia. The decision must be fully documented in the patient notes with the justification for the use of transfusion rather than alternatives and the expected outcome of the transfusion. 6. Clinicians must be made aware that the expected increment following transfusion of a unit of red cells is dependent upon the patient s weight. In medical patients with anaemia, there should be clinical reassessment after each unit transfused and a re-check of the blood count. 7. Further research is required to provide the evidence for appropriate transfusion decision making in medical patients with anaemia


25 National Survey Red Cell Use 2014
26 National Survey Red Cell Use 2014
27 Clinical scenarios
28 TRUE OR FALSE? A GP refers in an asymptomatic 30 year old female with a history of menorrhagia and a Hb 44g/L. Initial treatment should include a 2 unit transfusion of red cells. 50% 50% A. True B. False True False 10
29 TRUE OR FALSE? A GP refers in an asymptomatic 30 year old female with a history of menorrhagia and a Hb 44g/L. Initial treatment should include a 2 unit transfusion of red cells. FALSE In chronic anaemia transfusion is based on symptoms, not Hb. Iron deficiency anaemia secondary to menorrhagia is easily treated with oral iron supplements. Hb should increase by approximately 15g/L per week.
30 TRUE OR FALSE? An 82 year old male with known diabetes and hypertension has a repeat Hb of 101g/L following admission for recurrent chest pain. It is appropriate to transfuse him red cells. 50% 50% A.True B.False True False 10
31 TRUE OR FALSE? An 82 year old male with known diabetes and hypertension has a repeat Hb of 101g/L following admission for recurrent chest pain. It is appropriate to transfuse him red cells. FALSE There is no evidence to support transfusing patients with an Hb>100g/L. In acute blood loss transfusion is indicated after 30-40% loss of blood volume (> mls in adult). Peri-operative transfusion may be indicated if Hb<70g/L or <80g/L in elderly patients with known cardiovascular disease, although a full clinical assessment must first be made.
32 Case studies
33 1. A 78 year old man felt unwell and had a Hb 58g/L. He was otherwise asymptomatic and was known to have iron deficiency anaemia. The attending doctor authorised a 3 unit red cell transfusion. The post transfusion Hb was 76g/L.
34 Appropriate or inappropriate transfusion? A. Appropriate pt. unwell (but also should be started on iron) B. Inappropriate number of units for the pt. s age C. Appropriate pt. had Hb >20g/l below transfusion trigger D. Inappropriate pt. asymptomatic of anaemia
35 Inappropriate transfusion of red cells to an asymptomatic iron deficient patient A 78 year old man felt unwell and had a Hb 58g/L. He was otherwise asymptomatic and was known to have iron deficiency anaemia. The attending doctor authorised a 3 unit red cell transfusion. The post transfusion Hb was 76g/L. from the SHOT 2013 report
36 2. A patient weighing 35.1kg with small bowel angiodysplasia and anaemia received 6 red cell transfusions over a 3 month period.
37 What are the clinical issues here? Multiple transfusions over short time period Low patient body weight RCC transfusion not indicated for this condition Oral iron is first line treatment
38 A patient of low body weight repeatedly over-transfused A patient weighing 35.1kg with small bowel angiodysplasia and anaemia received 6 red cell transfusions over a 3 month period. A fall precipitated her admission and her Hb was then found to be 222 g/l and she was generally deteriorating. She was dyspnoeic with a tachycardia and had symptoms consistent with polycythaemia. A haematology specialist registrar noted the patient was plethoric and she then required repeated venesection. She developed renal impairment with long term morbidity. from the SHOT 2012 report
39 3. A 78 year old female, weight 63.3kg, with a possible allergic transfusion reaction. On assessment, there was no evidence of an allergic reaction and a diagnosis of TACO was made. The patient had been admitted to the emergency department (ED) unwell and feeling faint. All vital signs were within normal limits, Hb 59g/L with a microcytic blood picture, likely cause chronic iron deficiency. Two units of red cells were ordered by the ED doctor. The first unit was begun at 14:12 and she was transferred to the AMU. During a consultant led ward round, 2 more red cell units were prescribed.
40 What do you think was the outcome? Required a further 2 RCC units 24 hours later Reviewed again tx. withheld in favour of iron therapy Continued with management plan Good Hb increment with first 2 units with poor outcome other 2 withheld
41 Fatal TACO following red cell transfusion for probable chronic iron deficiency anaemia A 78 year old female, weight 63.3kg, was brought to the attention of a transfusion practitioner as a possible allergic transfusion reaction. On assessment, there was no evidence of an allergic reaction and a diagnosis of TACO was made. The patient had been admitted to the emergency department (ED) unwell and feeling faint. All vital signs were within normal limits, Hb 59g/L with a microcytic blood picture, likely cause chronic iron deficiency. Two units of red cells were ordered by the ED doctor. The first unit was begun at 14:12 and she was transferred to the AMU. During a consultant led ward round, 2 more red cell units were prescribed. She received 3 red cell units and approximately 290mL of the fourth unit when she developed massive pulmonary oedema and left ventricular failure. Her pulse and blood pressure at baseline and at the time of the reaction were 98 and 82bpm and 120/75mmHg and 152/111 respectively. An electrocardiograph showed atrial fibrillation and T wave changes. She was admitted to ITU where she received continuous positive airway pressure (CPAP) and a furosemide infusion, however she subsequently died. from the SHOT 2013 report
42 4. A middle-aged woman with known alcoholic liver disease presented with haematemesis estimated to be more than 500 ml and was urgently transfused 7 units of red cells without monitoring of the Hb. The Hb on the previous day was 11.3 g/dl. The patient was not reviewed regularly during transfusion. Appropriate to transfuse? YES NO
43 Appropriate to transfuse? A.Yes B.No 50% 50% 10 Yes No
44 How would you dose RCCs? Against initial Hb Against initial Hb and estimated blood loss (ongoing) Against regular Hbs and symptoms Against regular Hbs check
45 Haematemesis with excessive transfusion and TACO A middle-aged woman with known alcoholic liver disease presented with haematemesis estimated to be more than 500 ml and was urgently transfused 7 units of red cells without monitoring of the Hb. The Hb on the previous day was 11.3 g/dl. The patient was not reviewed regularly during transfusion. Her Hb rose to 16.4 g/dl post-transfusion requiring venesection of 2 units and admission to high dependency unit (HDU) for ventilation because of pulmonary oedema. She later died of multi-organ failure. It was felt that death was related to the excessive transfusion. from the SHOT 2011 report
46 Summary of transfusion of adult medical patients Anaemia was the primary reason for transfusion in 78% of cases. Most commonly 2 units of red cells were given (67% of cases). Transfusion at above Hb trigger (29%) and to >2g.dl above Hb trigger (33%) 20% of transfusions had a possible potentially reversible anaemia - 13% of were possible iron deficiency Patients should receive appropriate and timely treatment for anaemia to avoid unnecessary transfusion
47 Thank you Alister Jones
National Comparative Audit of red cell transfusion in Medical Patients Part Two
 National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
National Comparative Audit of red cell transfusion in Medical Patients Part Two Dr. Kate Pendry, Project Clinical Lead John Grant-Casey, Project Manager August 2013 Part One 9216 cases from 181 sites (90%
Julie Ball SHOT Clinical Incidents Specialist
 Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
Julie Ball SHOT Clinical Incidents Specialist Surveillance procedures from the collection of blood and its components to the follow up of the recipients To collect and assess information on unexpected
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
2017 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients
 07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
Single unit transfusion audit PE Smith B Ferguson
 Single unit transfusion audit PE Smith B Ferguson Brief introduction Method: A retrospective audit performed in November 2015 Standards: All stable, normovolaemic adult inpatients who require transfusion
Single unit transfusion audit PE Smith B Ferguson Brief introduction Method: A retrospective audit performed in November 2015 Standards: All stable, normovolaemic adult inpatients who require transfusion
Pulmonary complications in the Elderly. Paula Bolton-Maggs Medical Director
 Pulmonary complications in the Elderly Paula Bolton-Maggs Medical Director What does SHOT do? Serious Hazards of Transfusion Collect data on serious adverse reactions and events related to transfusion
Pulmonary complications in the Elderly Paula Bolton-Maggs Medical Director What does SHOT do? Serious Hazards of Transfusion Collect data on serious adverse reactions and events related to transfusion
Management of Anaemia
 Management of Anaemia Janet Birchall Consultant Haematologist North Bristol Trust and NHS Blood & Transplant Case History - DW age 86 years 14.30 FBC by GP Hb 58 g/l, ferritin 3microg/L. Hospital review
Management of Anaemia Janet Birchall Consultant Haematologist North Bristol Trust and NHS Blood & Transplant Case History - DW age 86 years 14.30 FBC by GP Hb 58 g/l, ferritin 3microg/L. Hospital review
National Comparative Audit of Blood Transfusion
 National Comparative Audit Of Blood Transfusion National Comparative Audit of Blood Transfusion 2011 Audit of Use of Blood in Adult Medical Patients Part 1 St. Elsewhere's Hospital ACKNOWLEDGEMENTS We
National Comparative Audit Of Blood Transfusion National Comparative Audit of Blood Transfusion 2011 Audit of Use of Blood in Adult Medical Patients Part 1 St. Elsewhere's Hospital ACKNOWLEDGEMENTS We
27/01/2019. Anaemia, Transfusion and TACO Lise Estcourt. Anaemia. What is anaemia?
 Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
Anaemia, Transfusion and TACO Lise Estcourt 1 Anaemia 2 What is anaemia? 3 1 Anaemia according to WHO 4 Anaemia in palliative care Common (77% men 68% women) Symptoms often non-specific Some causes potentially
Pre-operative Anaemia Colorectal and Orthopaedic Surgery
 Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Pre-operative Anaemia Colorectal and Orthopaedic Surgery Dr Simon Rang Consultant Anaesthetist East Kent Hospitals NHS Trust Dreamland Pre-operative Anaemia Anaemia is a perioperative risk factor Perioperative
Dr Charlie Baker Consultant Anaesthetist UHNM. Being a place our f amilies would choose
 Dr Charlie Baker Consultant Anaesthetist UHNM Being a place our f amilies would choose The story so far: Anaemia is associated with transfusion. The more anaemic you are pre op the more likely you are
Dr Charlie Baker Consultant Anaesthetist UHNM Being a place our f amilies would choose The story so far: Anaemia is associated with transfusion. The more anaemic you are pre op the more likely you are
Management of Anaemia reduces Red cell Transfusion in NI. Dr Susan Atkinson NI Transfusion Committee
 Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
Management of Anaemia reduces Red cell Transfusion in NI Dr Susan Atkinson NI Transfusion Committee BBTS September 2014 Patient and Client Council Department of Health Chief Medical Officer Expert Professionals
Blood Transfusion. Dr William Dooley
 Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
Blood Transfusion Dr William Dooley Plan Cases Blood groups / Indications Procedure Monitoring / Reactions Cases For following cases: - Would you give them a blood transfusion? - How many units you would
National Comparative Audit of Blood Transfusion
 National Comparative Audit Of Blood Transfusion National Comparative Audit of Blood Transfusion 2011 Audit of Use of Blood in Adult Medical Patients Part Two July 2013 1 ACKNOWLEDGEMENTS We wish to thank
National Comparative Audit Of Blood Transfusion National Comparative Audit of Blood Transfusion 2011 Audit of Use of Blood in Adult Medical Patients Part Two July 2013 1 ACKNOWLEDGEMENTS We wish to thank
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Patient Blood Management and alternatives to transfusion
 Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
Patient Blood Management and alternatives to transfusion Patient Blood Management and the alternatives to transfusion and when these should be used Learning Outcomes Explain techniques that can be used
National Comparative Audit of Blood Transfusion
 National Comparative Audit of Blood Transfusion National Comparative Audit of Blood Transfusion 2017 Transfusion Associated Circulatory Overload Audit 0 1 Acknowledgements We wish to thank all those who
National Comparative Audit of Blood Transfusion National Comparative Audit of Blood Transfusion 2017 Transfusion Associated Circulatory Overload Audit 0 1 Acknowledgements We wish to thank all those who
Cancer associated thrombosis palliative care and the end of life. Tracy Anderson May 2017
 Cancer associated thrombosis palliative care and the end of life Tracy Anderson May 2017 Treatment at the end of life Can be challenging to know what treatments are appropriate Benefit vs burden Patients
Cancer associated thrombosis palliative care and the end of life Tracy Anderson May 2017 Treatment at the end of life Can be challenging to know what treatments are appropriate Benefit vs burden Patients
Laboratory Empowerment. Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance
 Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Laboratory Empowerment Debbie Asher Adrian Ebbs Transfusion Laboratory Managers, Eastern Pathology Alliance Why? Electronic ICE requesting was in use for requesting red cells NBTC Indication Codes were
Transfusion reactions. Jim Taylor Haematology SpR Sheffield
 Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Transfusion reactions Jim Taylor Haematology SpR Sheffield Pre questions 1. Platelet transfusions are more prone to bacterial contamination compared to red cells. T/F 2. Common causes of an acute transfusion
Northern Treatment Advisory Group
 Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
Northern Treatment Advisory Group Ferric Maltol (Feraccru ) for the treatment of iron deficiency Lead author: Daniel Hill Regional Drug & Therapeutics Centre (Newcastle) September 2018 2018 Summary Iron
HOSPITAL MEDICINE BECOMING A PHYSICIAN
 HOSPITAL MEDICINE BECOMING A PHYSICIAN DR MIKE MASDING Consultant Physician & Diabetologist Poole Hospital NHS Foundation Trust 24 September 2010 Hospital Medicine Becoming a Physician What is a Physician?
HOSPITAL MEDICINE BECOMING A PHYSICIAN DR MIKE MASDING Consultant Physician & Diabetologist Poole Hospital NHS Foundation Trust 24 September 2010 Hospital Medicine Becoming a Physician What is a Physician?
National Comparative Audit of Blood Transfusion Audit of Red Cell & Platelet Transfusion in Adult Haematology Patients.
 National Comparative Audit of Blood Transfusion 2016 Audit of Red Cell & Platelet Transfusion in Adult Haematology Patients South West RTC Why was this audit necessary? Up to 65% of all platelet transfusions
National Comparative Audit of Blood Transfusion 2016 Audit of Red Cell & Platelet Transfusion in Adult Haematology Patients South West RTC Why was this audit necessary? Up to 65% of all platelet transfusions
Administration of blood components. Tina Parker - Transfusion Practitioner
 . Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
. Administration of blood components Tina Parker - Transfusion Practitioner Red Cells Each unit contains 250-350mls Preserved with glucose and Mannitol to keep the correct tension Lasts 35 days from midnight
Tranexamic acid and Iron in Haematology. Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital
 Tranexamic acid and Iron in Haematology Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital Why consider an alternative? Can t we just give blood? Why consider an alternative? Can t we
Tranexamic acid and Iron in Haematology Andy King-Venables Transfusion Practitioner Hinchingbrooke Hospital Why consider an alternative? Can t we just give blood? Why consider an alternative? Can t we
Overview of session. Blood transfusions in advanced disease 3/21/18. Why am I interested in blood transfusions?
 Blood transfusions in advanced disease Dr Karen Neoh Registrar in Palliative Medicine, Leeds Teaching Hospital Trust and the Academic Unit of Palliative Care, University of Leeds Dr Jason Boland Senior
Blood transfusions in advanced disease Dr Karen Neoh Registrar in Palliative Medicine, Leeds Teaching Hospital Trust and the Academic Unit of Palliative Care, University of Leeds Dr Jason Boland Senior
RAPID REFERRAL ANEMIA CLINICS
 RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
RAPID REFERRAL ANEMIA CLINICS REDUCING INAPPROPRIATE TRANSFUSION AND OPTIMIZING PATIENT CARE ALAN TINMOUTH ORBCON APRIL 11, 2018 www.ohri.ca Affiliated with Affilié à OBJECTIVES 1. Review rationale for
Low risk upper GI bleeding pathway
 Low risk upper GI bleeding pathway Background Low risk upper GI bleeding may be safely managed without an emergency admission to NUH following presentation to the ED. NUH uses the Glasgow Blatchford score
Low risk upper GI bleeding pathway Background Low risk upper GI bleeding may be safely managed without an emergency admission to NUH following presentation to the ED. NUH uses the Glasgow Blatchford score
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare?
 1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
Have you ever managed patients who have experienced an adverse reaction to transfusion?
 Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Have you ever managed patients who have experienced an adverse reaction to transfusion? A. Yes, often B. Yes, occasionally C. No A. 1 in 30 units? B. 1 in 100? C. 1 in 1000? D. 1 in 10,000? SHOT collects
Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital
 Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital Primary aim to reduce the need for red blood cell transfusion, in those patients where transfusion can be avoided, through the use
Mr John Faulds Blood Conservation Co-ordinator Royal Cornwall Hospital Primary aim to reduce the need for red blood cell transfusion, in those patients where transfusion can be avoided, through the use
PREOPERATIVE ANAEMIA PATHWAY
 PREOPERATIVE ANAEMIA PATHWAY Surname: Patient ID No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: Next of Kin: Name GP Name: GP Practice: Planned Operation:
PREOPERATIVE ANAEMIA PATHWAY Surname: Patient ID No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: Next of Kin: Name GP Name: GP Practice: Planned Operation:
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
An Audit of Poor Response To Erythropoeitin Therapy. September 1998
 1 An Audit of Poor Response To Erythropoeitin Therapy September 1998 Prepared By: Nicola Austerberry Renal Audit Facilitator Phil Kalra Consultant Nephrologist 2 1 Introduction The topic for this audit
1 An Audit of Poor Response To Erythropoeitin Therapy September 1998 Prepared By: Nicola Austerberry Renal Audit Facilitator Phil Kalra Consultant Nephrologist 2 1 Introduction The topic for this audit
GP refresher course Anaemia. Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018
 GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
Update on the management of iron deficiency
 Update on the management of iron deficiency Outline Need to improve management & avoid transfusion Diagnosis & investigation Oral iron & IV iron Tools & resources No conflicts of interest All natural
Update on the management of iron deficiency Outline Need to improve management & avoid transfusion Diagnosis & investigation Oral iron & IV iron Tools & resources No conflicts of interest All natural
Blood Transfusion. Dr Will Dooley
 Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
Blood Transfusion Dr Will Dooley Plan Cases OSCE practice scenario Blood groups Monitoring / Reactions Miss Irene Bleede, 23yo Asymptomatic, healthy woman with menorrhagia Hb 78 g/l, MCV 73fl Would you
PREOPERATIVE ANAEMIA PATHWAY
 PREOPERATIVE ANAEMIA PATHWAY Surname: Unit No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: GP Name: GP Practice: Planned Operation: Postcode: Mobile
PREOPERATIVE ANAEMIA PATHWAY Surname: Unit No. Forename: DOB: / / Age: NHS Number: Likes to be called: Address: Tel. No. Religion/Spirituality: GP Name: GP Practice: Planned Operation: Postcode: Mobile
EFFECTIVE SHARE CARE AGREEMENT
 Specialist details Patient identifier Name: Tel: EFFECTIVE SHARE CARE AGREEMENT For the specialist use of Erythropoietin Stimulating Agent (ESA) Therapy (formerly known as EPO) for the correction of Anaemia
Specialist details Patient identifier Name: Tel: EFFECTIVE SHARE CARE AGREEMENT For the specialist use of Erythropoietin Stimulating Agent (ESA) Therapy (formerly known as EPO) for the correction of Anaemia
Dr Marina Karakantza Consultant Haematologist, NHSBT
 Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
Dr Marina Karakantza Consultant Haematologist, NHSBT Overview Definition of transfusion thresholds Mechanisms of adaptation to anaemia How RBC transfusion affect adaptation mechanisms to anaemia Triggers
A review of paediatric and neonatal prescribing practice. Tracey Shackleton Alder Hey Children s NHS Trust 24 th September 2014
 A review of paediatric and neonatal prescribing practice. Tracey Shackleton Alder Hey Children s NHS Trust 24 th September 2014 SHOT report 2013 The overall pattern of errors reported to SHOT for the 2013
A review of paediatric and neonatal prescribing practice. Tracey Shackleton Alder Hey Children s NHS Trust 24 th September 2014 SHOT report 2013 The overall pattern of errors reported to SHOT for the 2013
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON
 IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
IRON DEFICIENCY / ANAEMIA ANTHONY BEETON HYPOXIA 1-2 mg IRON Labile iron Body iron ± 3 4 g Liver and the reticuloendothelial system and spleen (approximately 200 300 mg in adult women and 1 g in adult
Pre-operative Assessment
 Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Pre-operative Assessment Dr Craig Taylor Andrea Harris On behalf of the WM RTC Audit Group A good example of an audit cycle...... or is it!!?? Identify Better Blood Transfusion 2002 2007 West Midlands
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant. Lab Matters study day Oake Manor, Taunton, 8 th July 2015
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios
 Education package for GPs and Nurse Practitioners Case scenarios") NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios How to use the case scenarios The case scenarios can be used in a training
NICE guideline on Suspected cancer: recognition and referral (2015) Education package for GPs and Nurse Practitioners Case scenarios How to use the case scenarios The case scenarios can be used in a training
Top tips for surviving your first on call Dr Maleeha Rizvi
 Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Top tips for surviving your first on call Dr Maleeha Rizvi Specialist Registrar in Cardiology University Hospital Lewisham Overview Practical points The Bleep and prioritising on call Cardiac arrests Prescribing
Haematology dilemma s to refer or not to refer?
 Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia. Ioannis Griveas, MD, PhD
 Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Efficacy and tolerability of oral Sucrosomial Iron in CKD patients with anemia Ioannis Griveas, MD, PhD Anaemia is a state in which the quality and/or quantity of circulating red blood cells are below
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease
 Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Guideline for the Management of Acute Chest Syndrome in Children with Sickle Cell Disease Definition Acute chest syndrome (ACS) is defined as an acute illness characterized by fever and/or respiratory
Blood Transfusions in Children with Haemoglobinopathies
 Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Blood Transfusions in Children with Haemoglobinopathies Version: 2 Date: 22 nd April 2010 Authors: Responsible committee or Director: Review date: Target audience: Stakeholders/ committees involved in
Atrial Fibrillation. A guide for Southwark General Practice. Key Messages. Always work within your knowledge and competency
 Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
CAUTION: You must refer to the intranet for the most recent version of this procedural document.
 Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
Procedure for the use of Intravenous Iron Dextran (CosmoFer ) Sharepoint Location Sharepoint Index Directory Clinical Policies and Guidelines General Policies and Guidelines/ Haematology And blood transfusion
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
NZBS HAEMOCHROMATOSIS & THERAPEUTIC VENESECTION POLICY
 REASON FOR ISSUE: New Document for TV Clinic 1. INTRODUCTION NZBS will provide a venesection service for people in New Zealand who require venesection for conditions that are known to benefit from therapeutic
REASON FOR ISSUE: New Document for TV Clinic 1. INTRODUCTION NZBS will provide a venesection service for people in New Zealand who require venesection for conditions that are known to benefit from therapeutic
9 Diabetes care. Back to contents
 Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Definition Aetiology
 Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
ferric carboxymaltose 50mg iron/ml solution for injection/infusion (Ferinject ) SMC No. (463/08) Vifor Pharmaceuticals
 SMC No. (463/08) Vifor Pharmaceuticals") ferric carboxymaltose 50mg iron/ml solution for injection/infusion (Ferinject ) SMC No. (463/08) Vifor Pharmaceuticals 17 December 2010 The Scottish Medicines Consortium (SMC) has completed its assessment
ferric carboxymaltose 50mg iron/ml solution for injection/infusion (Ferinject ) SMC No. (463/08) Vifor Pharmaceuticals 17 December 2010 The Scottish Medicines Consortium (SMC) has completed its assessment
NHS North of Tyne Guidelines on Iron Deficiency Anaemia & Referral Form v2
 Clinical Guidelines Guideline Number: T 02 NHS rth of Tyne Guidelines on Iron Deficiency Anaemia & Referral Form v2 Ratified by: NHS rth of Tyne Pathways & Guidelines Group Date ratified: July 2010 Date
Clinical Guidelines Guideline Number: T 02 NHS rth of Tyne Guidelines on Iron Deficiency Anaemia & Referral Form v2 Ratified by: NHS rth of Tyne Pathways & Guidelines Group Date ratified: July 2010 Date
DETECTION, INVESTIGATION AND MANAGEMENT OF ANAEMIA
 From the Chief Medical Officer Dr Michael McBride HSS(MD) 22/2012 Circulation list: For Action: Chief Executives of HSC Trusts Medical Directors of HSC Trusts (for onward distribution to All Hospital Doctors)
From the Chief Medical Officer Dr Michael McBride HSS(MD) 22/2012 Circulation list: For Action: Chief Executives of HSC Trusts Medical Directors of HSC Trusts (for onward distribution to All Hospital Doctors)
Transfusion Challenges. - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016
 Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
Transfusion Challenges - Transfusion Reactions - Do they need platelets? Dr. Eoghan Molloy Haem SpR 2016 Guidance on Transfusion Hospital transfusion guidelines and procedures Irish Blood Transfusion Service
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary
 Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO
 POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO Selection Examination for Enrolment to the in-service Training Programme in Postgraduate Certificate in Basic Laboratory Sciences leading to the
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO Selection Examination for Enrolment to the in-service Training Programme in Postgraduate Certificate in Basic Laboratory Sciences leading to the
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Managing peri-operative anaemiathe Papworth way. Dr Andrew A Klein Royal Papworth Hospital Cambridge UK
 Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Managing peri-operative anaemiathe Papworth way Dr Andrew A Klein Royal Papworth Hospital Cambridge UK Conflicts of interest: Unrestricted educational grants/honoraria from CSL Behring, Brightwake Ltd,
Policy for the use of intravenous Iron Dextran (CosmoFer )
") Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
Policy for the use of intravenous Iron Dextran (CosmoFer ) Sharepoint Location Clinical Policies and Guidelines Sharepoint Index Directory General Policies and Guidelines Sub Area Haematology and Blood
Oxford Kidney Unit A guide to conservative kidney management. Information for Healthcare Professionals
 Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
Prescribing Framework for Methotrexate for Immunosuppression in ADULTS
 Hull & East Riding Prescribing Committee Prescribing Framework for Methotrexate for Immunosuppression in ADULTS Patient s Name:.. NHS Number: Patient s Address:... (Use addressograph sticker) GP s Name:...
Hull & East Riding Prescribing Committee Prescribing Framework for Methotrexate for Immunosuppression in ADULTS Patient s Name:.. NHS Number: Patient s Address:... (Use addressograph sticker) GP s Name:...
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
 Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Interpreting Blood Tests Part 1. Dr Andrew Smith
 Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*
 and Strategies for Prevention. Khalid Abdulla Sharif, MD, MRCP (UK)*") Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
Bahrain Medical Bulletin, Vol. 29, No.4, December 2007 Transfusion-Related Acute Lung Injury (TRALI) and Strategies for Prevention Khalid Abdulla Sharif, MD, MRCP (UK)* Background: Transfusion-Related
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Iron Deficiency Anaemia but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service
 Iron Deficiency but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service 1 3 Questions 1. Is anaemia incurable in my patient? 2. Is anaemia unavoidable in my bleeding patient? 3. Is
Iron Deficiency but Why? Dr LAU Ching-wa Specialist in Haematology Blood Transfusion Service 1 3 Questions 1. Is anaemia incurable in my patient? 2. Is anaemia unavoidable in my bleeding patient? 3. Is
BMS Education Day 28 th January and 4th February 2013
 BMS Education Day 28 th January and 4th February 2013 Category of Reaction 24 hours from the transfusion = DELAYED Infectious Bacterial contamination Viral HIV,
BMS Education Day 28 th January and 4th February 2013 Category of Reaction 24 hours from the transfusion = DELAYED Infectious Bacterial contamination Viral HIV,
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings
 Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Trust Guideline for the Management and Administration of Intravenous Iron in Adults under the Gastroenterology Directorate
 A clinical guideline recommended for use For Use in: The Gastroenterology Directorate By: Registered nurses competent in the administration of intravenous therapy and medical staff For: Adult patients
A clinical guideline recommended for use For Use in: The Gastroenterology Directorate By: Registered nurses competent in the administration of intravenous therapy and medical staff For: Adult patients
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
2:39 2: Dizziness and nausea Cerebral. 2:57 1: Vomiting Gastro-intestinal
 Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
Supplemental: Table B: Detailed description of adverse events by time, treatment group and procedure T-spinal to incident T-spinal to PACU discharge Group THA/TKA Adverse event description Adverse event
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010
 Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN MEDICAL PHYSIOLOGY EXAMINATION - APRIL 2015 FOUNDATION MODULE
 POSTGRADUATE INSTITUTE OF MEDICINE FOUNDATION MODULE Date :- 25 th April 2015 Time 9.30 a.m. - 10.30 a.m. STRUCTURED ESSAY QUESTION (SEP) PAPER 1. Using diagrams, describe the sequence of events by which
POSTGRADUATE INSTITUTE OF MEDICINE FOUNDATION MODULE Date :- 25 th April 2015 Time 9.30 a.m. - 10.30 a.m. STRUCTURED ESSAY QUESTION (SEP) PAPER 1. Using diagrams, describe the sequence of events by which
Anaemia in Pregnancy
 Anaemia in Pregnancy Definition :anaemia is a pathological condition in which the oxygen-carrying capacity of red blood cells is insufficient to meet the body needs. The WHO : haemoglobin concentration
Anaemia in Pregnancy Definition :anaemia is a pathological condition in which the oxygen-carrying capacity of red blood cells is insufficient to meet the body needs. The WHO : haemoglobin concentration
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth
 Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
Laboratory diagnosis of iron deficiency: The interpretation of automated counting parameters. Dr Wayne Thomas Derriford Hospital, Plymouth Why does it matter? Over 30% of the Worlds population are anaemic,
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery
 2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery 2017 Re-Audit of Red Cell & Platelet Transfusion in Adult Haematology patients South West RTC 2016 Re-Audit of
2016 Re-Audit of Patient Blood Management in adults undergoing elective, scheduled surgery 2017 Re-Audit of Red Cell & Platelet Transfusion in Adult Haematology patients South West RTC 2016 Re-Audit of
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Patient Blood Management. Peter Freeman Patient Blood Management Officer Clinical Operations Hunter New England LHD.
 Patient Blood Management Peter Freeman Patient Blood Management Officer Clinical Operations Hunter New England LHD. 1 National Standard 7: Blood & Products To ensure that the patients who receive blood
Patient Blood Management Peter Freeman Patient Blood Management Officer Clinical Operations Hunter New England LHD. 1 National Standard 7: Blood & Products To ensure that the patients who receive blood
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Venesection Nursing Guidelines
 Venesection Nursing Guidelines Rationale Patients requiring venesection on the Day Treatment Unit (DTU) fall into 3 main categories; patients diagnosed with: Polycythemia Rubra Vera Haemachromatosis Transfusion
Venesection Nursing Guidelines Rationale Patients requiring venesection on the Day Treatment Unit (DTU) fall into 3 main categories; patients diagnosed with: Polycythemia Rubra Vera Haemachromatosis Transfusion
SMR Palliative Care Forum The Intersection: Chronic disease and Palliative Care. Chronic Heart Failure
 SMR Palliative Care Forum The Intersection: Chronic disease and Palliative Care. Chronic Heart Failure Bruce Jackson Physician (General Medicine, Nephrology, Cardiology) Inpatient ward service in General
SMR Palliative Care Forum The Intersection: Chronic disease and Palliative Care. Chronic Heart Failure Bruce Jackson Physician (General Medicine, Nephrology, Cardiology) Inpatient ward service in General
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University
 Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
Intravenous Iron: A Good Thing Made Better? Marilyn Telen, MD Wellcome Professor of Medicine Duke University Use of IV Iron There are increasing data regarding safety of IV iron. IV iron is superior to
Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD)
") Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD) This guideline is for use in adult patients with an estimated Glomerular Filtration Rate (egfr) of less than 60ml/min/1.73m
Guidelines on Anaemia Management in Patients with Chronic Kidney Disease (CKD) This guideline is for use in adult patients with an estimated Glomerular Filtration Rate (egfr) of less than 60ml/min/1.73m
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Palliative Care for Heart Failure. Service Development in West Hertfordshire
 1 Palliative Care for Heart Failure. Service Development in West Hertfordshire Dr Sharon Chadwick, Medical Director &Consultant in Palliative Medicine Hospice of St Francis, Berkhamsted. Consultant in
1 Palliative Care for Heart Failure. Service Development in West Hertfordshire Dr Sharon Chadwick, Medical Director &Consultant in Palliative Medicine Hospice of St Francis, Berkhamsted. Consultant in