Current Trends in Pain Management: Guidelines, Standards and Approaches
|
|
|
- Gerard Holland
- 6 years ago
- Views:
Transcription
1 Current Trends in Pain Management: Guidelines, Standards and Approaches Kim Spinelli MSN, APRN, BC, CNS Pain Management Clinical Nurse Specialist Memorial Hospital; University of Colorado Health Colorado Springs, CO


2 My Work

3 My Home

4
5 The Opioid Epidemic More Americans die each year from drug overdoses than motor vehicle crashes At least 50% of all opioid overdoses involved a prescribed medicine Sales of prescription opioids in the U.S. nearly quadrupled from 1999 to 2014, but the overall amount of pain Americans report has not changed Heroin-related overdose deaths have more than tripled since 2010 and continue to increase 2016 ANA, CDC guidelines 2016, IOM relieving pain in America 2011, National pain strategy 2016
. Results from the 2009 National Survey on Drug Use and Health: National Findings. 2010.")
6 Emergency Room (ER) Visits Nonmedical Use of Narcotic Pain Relievers Estimated number of ER visits involving nonmedical use of narcotic pain relievers increased 111% from 2004 to Office of Applied Studies, Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2009 National Survey on Drug Use and Health: National Findings
.")
7 Sources of Non-medically Used Analgesics 1 >60% of opioids used by non-patients are obtained from friends or family members 1. Office of Applied Studies, Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2009 National Survey on Drug Use and Health: National Findings
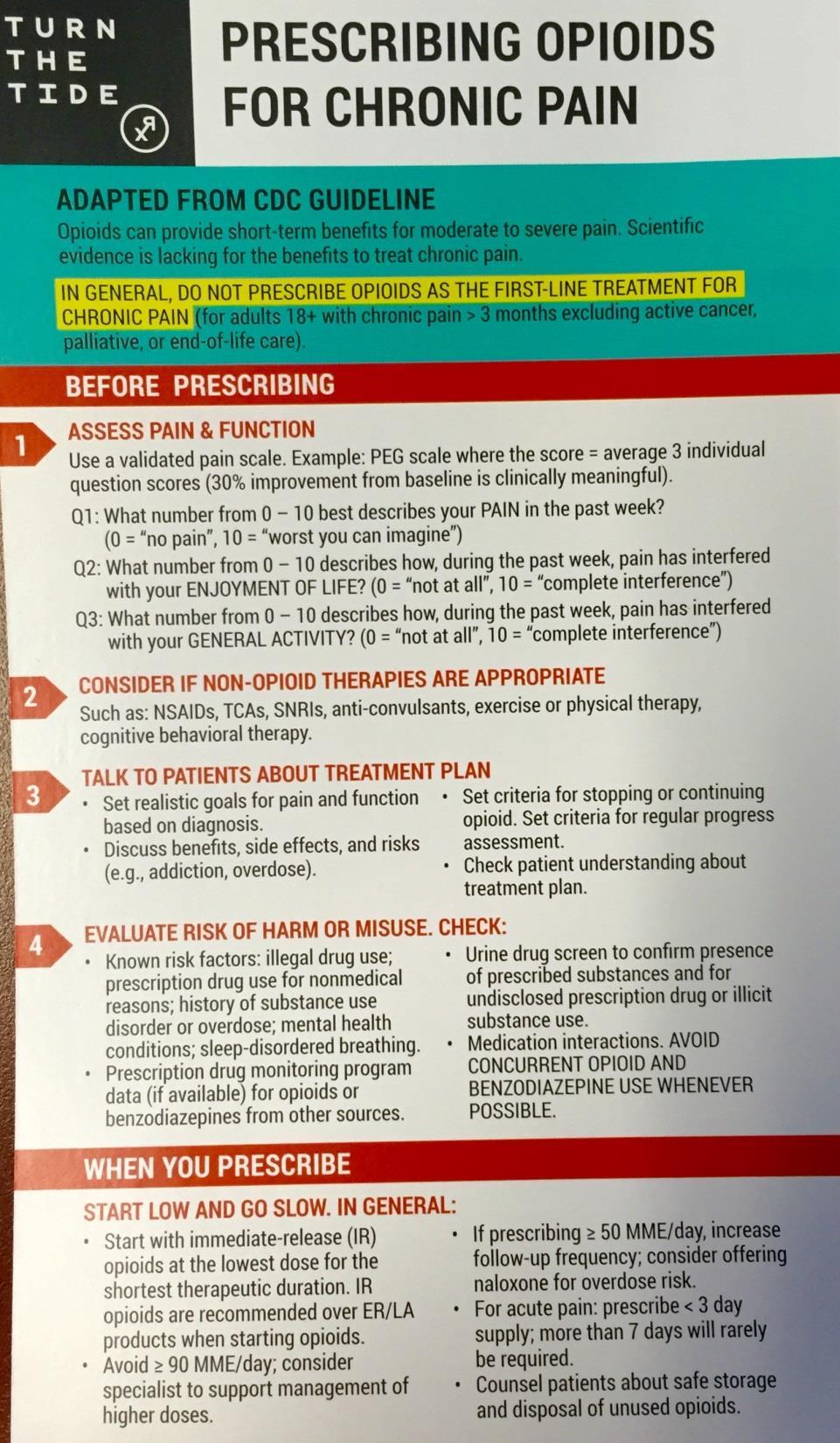
8 Centers for Disease Control and Prevention (CDC) Guideline for Prescribing Opioids for Chronic Pain Published in JAMA March 2016 Purpose, Use, and Primary Audience: Primary Care Providers Treating patients >18 years with Chronic pain Outpatient settings Does NOT include active cancer treatment, palliative care, and end-of-life care
9 CDC Guideline for Prescribing Opioids for Chronic Pain 12 Recommendations grouped into 3 conceptual areas: Determining when to initiate or continue opioids for chronic pain Opioid selection, dosage, duration, follow-up, and discontinuation Assessing risk and addressing harms of opioid use
10 CDC Guideline Recommendations: Determining when to initiate or continue opioids for chronic pain 1. Opioids not first-line or routine therapy for chronic pain Emphasis on non-pharm, non-opioid preferred Interventional approaches, Multimodal therapies 2. Establish and measure progress toward goals 3. Discuss benefits and risks of opioid therapy with patients
11 CDC Guideline Recommendations: Opioid selection, dosage, duration, follow-up, and discontinuation 4. Use immediate-release opioids when starting 5. Use caution at any dose and avoid increasing to high dosages 6. Prescribe no more than needed 7. Offer a taper if opioids cause harm or are not helping
12 CDC Guideline Recommendations: Assessing risk and addressing harms of opioid use 8. Evaluate and address risks for opioid-related harms 9. Check PDMP for high dosages and dangerous combinations 10. Test urine for prescribed opioid and other drugs 11. Avoid concurrent opioid and benzodiazepine prescribing 12. Treat patients for opioid use disorder (OUD) if needed
13
14
15
16 Ending the Opioid Epidemic Increase access to treatment: Train physicians and other clinicians who will provide treatment for opioid use disorders Continue to train healthcare professionals in safe and appropriate use of opioids and alternatives to use of opioids for pain Continue to educate the public about the dangers of misuse of pain medications and safe use when necessary including safe storage and disposal Use PDMPs, treatment agreements, and toxicology screens to increase safety Provide evidence-based treatment to all who need it for as long as it is clinically indicated Treatment of pain Treatment of Substance Use Disorder and Addiction
17 Pain by the Numbers Acute and chronic pain affect large numbers of Americans 2011 IOM report concluded that 100 million adults have chronic pain 2012 survey found 126 million had pain in the previous 3 months More than 73 million surgeries each year in U.S. >80% have moderate to severe pain during first 2 weeks after surgery 2014 survey found that 74% had moderate to severe pain after discharge Pain is common in persons with cancer: 30-40% at diagnosis; 50% at all stages; 70-90% with advanced disease More than a third of those cured of cancer report pain Pain is common in older persons 20% of general public >65 y/o report pain Almost half of nursing home residents report pain that is of moderate or greater intensity
18 The Pain Epidemic Institute of Medicine (IOM) comprehensive report: Relieving Pain In America Pain represents a public health crisis of epidemic proportions 100 million adults with chronic pain Annual cost of chronic pain to American economy is over $500 billion each year Medical treatment Lost productivity
19 Chronic pain affects more Americans than diabetes, heart disease and cancer COMBINED IOM REPORT 2011
20 Consequences of Unrelieved Pain: Societal Costs Unnecessary suffering Annual cost to American economy: over $500 billion 50 million lost work days/year in U.S. Unrelieved post-operative pain can increase length of stay
21 The Problem of Pain Pain is a uniquely individual and subjective experience with biological, psychological, and social factors Treatment is inadequate: Uncertain diagnoses Societal stigma Shortcomings in the availability of effective treatments Inadequate patient and clinician knowledge Unrelieved pain is harmful: Interferes with healing Interferes with immunity Interferes with functioning Puts patients at risk for developing complications
22 Consequences of Pain Poor pain control can lead to the development of chronic/persistent pain Acute pain can evolve directly into chronic pain from Wind Up of the nervous system (hyper excitability as a result of repeated, prolonged noxious stimuli) leading to neuronal plasticity. (APS, 2003, 2008) Post thoracotomy syndrome Post mastectomy syndrome Stimuli that are normally innocuous produce pain (allodynia)
23 Optimal Pain Management Care is individualized Mutual goals to balance comfort/function/safety Care is collaborative: Interdisciplinary in conjunction with patient & family Pain assessment is consistent Across different shifts, disciplines and settings Systematic reassessment & interventions evaluated Findings & plan are well documented Ineffective treatment plan revised
24 National Pain Strategy Developed in response to the IOM report calling to increase the recognition of pain as a significant public health problem in the U.S. Released in March 2016 by the Dept of Health and Human Services Created by a diverse team of experts from around the nation Roadmap toward achieving a system of care in which all people receive appropriate, high quality and evidence-based care for pain
25 National Pain Strategy Recommendations for Key Areas Population research Prevention and care Disparities Service delivery and payment Professional education and training Public education and communication
26 Pain Management in the Hospital: Joint Commission Standards The hospital educates all licensed independent practitioners on assessing and managing pain The hospital respects the patient s right to pain management The hospital assesses and manages the patient s pain Consistent with its scope of care, treatment, and services and the patient s condition Methods used are consistent with the patient s age, condition and ability to understand Reassessment and response to the patient s pain are done based on its reassessment criteria The hospital either treats the patient s pain or refers the patient for treatment. Treatment may include pharm and/or nonpharmacologic approaches.
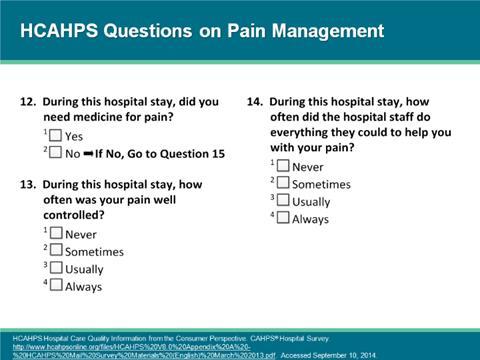
27 Patient Satisfaction

28 Guidelines on the Management of Postoperative Pain- Feb 2016
29 The Problem Patients still experiencing acute post op pain >75% report the pain severity as moderate, severe, or extreme >50% report relief as inadequate Inadequately controlled postoperative pain Increases the risk of postsurgical complications Negatively affects quality of life, function, and functional recovery Increases the risk of persistent postsurgical pain
30 Postoperative Pain Clinical Guidelines Based on underlying premise: Optimal pain management begins pre op with assessment and development of a plan tailored to the individual and surgery Preoperative education Perioperative pain management planning Use of pharm and nonpharm modalities (utilize multimodal therapies) Organizational policies Transition to outpatient care
31 Perioperative Techniques for Post Operative Pain Management IV bolus or IV PCA with systemic opioids Epidural or intrathecal opioid analgesia Indwelling catheter or single shot Regional techniques Single shot nerve block Continuous peripheral nerve block (cpnb) Post incisional infiltration with local anesthetics Multimodal analgesia The use of a variety of analgesic medications and techniques that target different mechanisms of action in the nervous system to take advantage of additive or synergistic effects and achieve more effective pain relief compared with singl-modality interventions Non-pharmacologic modalities PT/OT, TENS, Ice, Heat, Music, Relaxation, Breathing, Imagery, ect
32 Multimodal Treatment Physical Medicine and Rehabilitation Assistive devices, electrotherapy Complementary and Alternative Medicine Massage, supplements Pharmacotherapy Opioids, nonopioids, adjuvant analgesics Strategies for Pain and Associated Disability Lifestyle Change Exercise, weight loss Interventional Approaches Injections, neurostimulation Psychological Support Psychotherapy, group support Fine PG, et al. J Support Oncol. 2004;2(suppl 4):5-22. Portenoy RK, et al. In: Lowinson JH, et al, eds. Substance Abuse: A Comprehensive Textbook. 4th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2005:
33
34 Multimodal Techniques for Perioperative Pain Management Postoperative Pain Clinical Guidelines recommendations: Unless contraindicated, all patients should receive an around-theclock regimen of a non-opioid agent Non-steroidal anti-inflammatory drugs (NSAIDs) post op Cyclooxygenase-2 specific drugs (COXIBs) OK to give pre op Acetaminophen post op Gabapentin or pregabalin- start pre op Use regional blocks wherever possible and consider catheter placement for prolonged pain Use continuous epidural analgesia Major thoracic and abdominal procedures with increased risk of cardiac and pulmonary complications or prolonged ileus Provide appropriate RN monitoring of patients sedation and respiratory status Specifically in first 24 hours after surgery, and with dose changes Assess for risk factors warranting increased monitoring (continuous pulse ox, capnography) American Society of Anesthesiologists (ASA) Task Force. Anesthesiology 2012; 116(2):
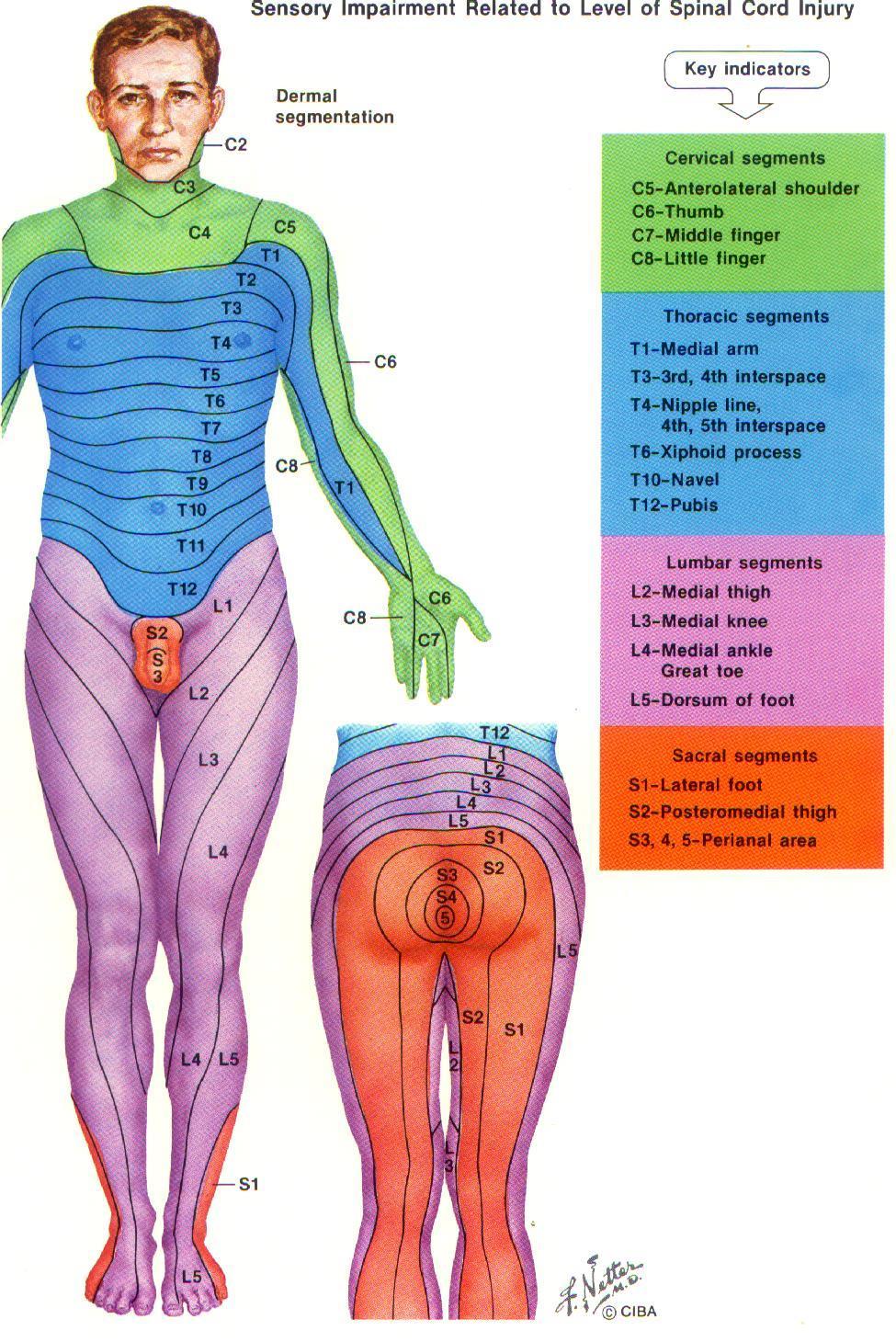
35 Epidural Analgesia Widely used for post op and post trauma Blunts the stress response Targeted therapy (placement of catheter at spinal cord level appropriate to the level of surgery or injury) Much lower systemic effect of the opioids Can be up to 10 times less than IV route Earlier return of bowel function Utilize opioid with local anesthetic for synergistic effect, and opioid sparing (allows less to be used of each) Restoration of respiratory mechanics after multiple rib fractures. Can speed recovery Earlier ambulation- Decreased incidence of DVT

36 Epidural Placement May be placed in the thoracic, lumbar or caudal spaces. Thoracic management of upper abdominal and thoracic sites of pain (ie. rib fractures) Lumbar and caudal used for lower abdominal and lower extremity pain
37

38
39 Continuous Peripheral Nerve Blocks -Catheter placed by an anesthesiologist near a peripheral nerve that allows for the continuous infusion of local anesthetic (i.e. ropivacaine). -Rate can be adjusted Most common sites: Lower Extremity Femoral, Adductor Canal, Fascia Iliaca, Lumbar Plexus, Sciatic, Popliteal, Saphenous Upper Extremity Brachial plexus, Interscalene, Infra/supra clavicular, Axillary Thorax (rib fx, thoracotomy, VATS, breast surgery) Paravertebral, Intercostal Abdominal- (Midline and transverse abd incisions) Transversus Abdominis Plane (TAP) Can be used safely for an extended period of time More effective pain management and fewer side effects than traditional opioid methods Opioid sparing Has specific order set and discharge instructions

40 Paravertebral placement

41 Paravertebral Catheter


42 Disposable Elastomeric pump for Incisional and Continuous Peripheral Nerve Blocks


43 Implantable Pain Therapies Neurostimulation Intrathecal Drug Delivery
44 Indications for Interventional Pain Management- Implantable Pain Therapies Neurostimulation Radiculopathies Phantom Limb/Stump Pain Neuralgias Intrathecal Drug Delivery Diffuse Cancer Pain Osteoporotic Pain Axial Somatic Pain
45 Indications for Interventional Pain Management Implantable Pain Therapies Neurostimulation OR Intrathecal Drug Delivery Failed Back Syndrome Complex Regional Pain Syndrome (CRPS) Arachnoiditis Painful Neuropathies
46 Patient Selection Criteria for Implanted Devices (SCS & ITDD) Objective pathology is concordant with the pain complaint More conservative therapies have failed Further surgical intervention is not indicated No serious drug habituation problem exists untreated Psychological clearance No contraindications to implantation are present

47 Neurostimulation A pain treatment that delivers low voltage electrical stimulation to the spinal cord to inhibit or block the sensation of pain. Totally implantable system, preceded by a screening test that allows for qualification of patients likely to benefit. Two types of fully implantable systems: rechargeable and nonrechargeable. First used 30 years ago.

48 Effective method of pain control. Non-destructive versus neuroablation. Minimally invasive surgical procedure. Reduction or elimination of pain medications May have long-term cost-effectiveness Advantages of Neurostimulation


49 Intrathecal Drug Delivery A pain management therapy that uses a drug delivery system to deliver medication directly into the fluid surrounding the spinal cord. Typically used when oral opioids do not deliver enough pain relief or side effects are intolerable. System consists of a pump and catheter, both of which are surgically placed under the skin. Pump Intraspinal Catheter
50 Key Benefits of Neurostimulation and Intrathecal Drug Delivery Efficacy can be tested in a screening test procedure Pain relief in at least 50% of carefully selected Neurostim patients, at least 80% of those receiving Intrathecal Drug Delivery Decreased oral medication usage Effective pain relief with lower dose levels and fewer central side effects than oral opioids Increased activity Improved quality of life Cost-effective, reversible therapy

51 Reduce Dose Reduce Side Effects 1 mg intrathecal morphine = 300 mg oral morphine Krames ES. J Pain Symptom Manage Jun;11(6):



52 Personal Therapy Manager- PTM 8840 N Vision Programmer 8835 Personal Therapy Manager SynchroMed II Programmable Pump Enables Patient-Activated Dosing Initiates Patient-Activated Dose Delivers Patient-Activated Dose
53 SO How Can We Address the Opioid Epidemic AND Help Those Suffering In Pain? Maintain a balance among compassionate prescribing, ethical clinical strategies and societal obligations Easy Right???
54 Optimal Paradigm for Patient Care Quality Patient Safety Experience of Care Liang BA, Mackey T. Arch Pathol Lab Med. 2011; 135(11):
55
56


57 Thank you

58 And Just for fun
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Pain Management at Stony Brook Medicine
 Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Pain Management at Stony Brook Medicine Pain Management Policy All patients must have effective pain management Appropriate screening and pain assessment Documentation Care and treatment Pain education
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons. Karol A Gutowski, MD, FACS
 Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Balanced Analgesia With NSAIDS and Coxibs. Raymond S. Sinatra MD, Ph.D
 Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Acute Peri-Operative Pain Management Strategies
 Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
POST-OP MULTIMODAL PAIN MANAGEMENT. Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management
 POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Opioid Prescribing for Acute Pain. Care for People 15 Years of Age and Older
 Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Summary This quality standard provides guidance on the appropriate prescribing, monitoring, and tapering of opioids to treat
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society
 Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Oregon Opioid Overdose Prevention Initiative
 Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Current evidence in acute pain management. Jeremy Cashman
 Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY. Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group
 IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group Who Am I? Avid equestrian Trained in Physical Medicine & Rehabilitation
IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group Who Am I? Avid equestrian Trained in Physical Medicine & Rehabilitation
Objectives. Conflict of Interest Disclosure. Neuraxial and Regional Anesthesia in the Pediatric Population
 Neuraxial and Regional Anesthesia in the Pediatric Population Lauren Renner, MS, RN-BC, PNP Sharon Wrona, DNP, RN-BC, PNP, PMHS, AP- PMN.... Conflict of Interest Disclosure Conflicts of Interest for ALL
Neuraxial and Regional Anesthesia in the Pediatric Population Lauren Renner, MS, RN-BC, PNP Sharon Wrona, DNP, RN-BC, PNP, PMHS, AP- PMN.... Conflict of Interest Disclosure Conflicts of Interest for ALL
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
DORIS DUKE MEDICAL STUDENTS JOURNAL Volume V,
 Continuous Femoral Perineural Infusion (CFPI) Using Ropivacaine after Total Knee Arthroplasty and its Effect on Postoperative Pain and Early Functional Outcomes Eric Lloyd Scientific abstract Total Knee
Continuous Femoral Perineural Infusion (CFPI) Using Ropivacaine after Total Knee Arthroplasty and its Effect on Postoperative Pain and Early Functional Outcomes Eric Lloyd Scientific abstract Total Knee
I. Chronic Pain Information Page 2-3. II. The Role of the Primary Care Physician in Chronic Pain Management Page 3-4
 SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
Anesthesia Processing Guidelines
 Anesthesia Processing Guidelines Policy Number: 10.01.511 Last Review: 5/2014 Origination: 10/1988 Next Review: 5/2015 Policy The following guidelines are utilized in processing anesthesia claims: 1) Anesthesia
Anesthesia Processing Guidelines Policy Number: 10.01.511 Last Review: 5/2014 Origination: 10/1988 Next Review: 5/2015 Policy The following guidelines are utilized in processing anesthesia claims: 1) Anesthesia
Guidelines on the Safe Practice of Acute Pain Management
 Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
Analgesia for ERAS programs. Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital
 Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Peripheral Nerve Blocks
 Peripheral Nerve Blocks N U R S I N G E D U C A T I O N JPS Acute Pain Service Peripheral nerve blocks are used as part of a multimodal analgesic program which provides the patient with safe and effective
Peripheral Nerve Blocks N U R S I N G E D U C A T I O N JPS Acute Pain Service Peripheral nerve blocks are used as part of a multimodal analgesic program which provides the patient with safe and effective
6/6/2017. First Do No Harm SECTION 1 THE OPIOID CRISIS. Implementing an Opioid Stewardship Program in a HealthCare System OBJECTIVES
 First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
Dr P.W.Buczkowski. Consultant in Anaesthesia & Pain Medicine. Royal Derby Hospital
 Dr P.W.Buczkowski Consultant in Anaesthesia & Pain Medicine Royal Derby Hospital INTERVENTIONAL PAIN MANAGEMENT III Neuroaxial Drug Delivery KYIV May 2010 Dr J Azzopardi MD FRCA FFPMANZCA FFPMRCA Consultant
Dr P.W.Buczkowski Consultant in Anaesthesia & Pain Medicine Royal Derby Hospital INTERVENTIONAL PAIN MANAGEMENT III Neuroaxial Drug Delivery KYIV May 2010 Dr J Azzopardi MD FRCA FFPMANZCA FFPMRCA Consultant
Clinical Fellowship Regional Anesthesia
 Anesthesia and Perioperative Medicine Western University Regional Anesthesia Fellowship Program Directors Dr. Kevin Armstrong & Dr. Shalini Dhir Clinical Fellowship Regional Anesthesia The regional anesthesia
Anesthesia and Perioperative Medicine Western University Regional Anesthesia Fellowship Program Directors Dr. Kevin Armstrong & Dr. Shalini Dhir Clinical Fellowship Regional Anesthesia The regional anesthesia
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces
 16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Pre-op Interventions to Mitigate Post-op Acute and Chronic Pain
 Pre-op Interventions to Mitigate Post-op Acute and Chronic Pain H A R S H A S H A N T H A N N A. M D, M S C A S S O C I A T E P R O F E S S O R D E P A R T M E N T O F A N E S T H E S I A C H R O N I C
Pre-op Interventions to Mitigate Post-op Acute and Chronic Pain H A R S H A S H A N T H A N N A. M D, M S C A S S O C I A T E P R O F E S S O R D E P A R T M E N T O F A N E S T H E S I A C H R O N I C
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Complex Regional Pain Syndrome Evidence Based Care Synopsis
 Complex Regional Pain Syndrome Evidence Based Care Synopsis A COMPREHENSIVE PAIN MANAGEMENT APPROACH HOWARD KONOWITZ, MD BOARD CERTIFICATION: INTERNAL MEDICINE, ANESTHESIOLOGY, PAIN MANAGEMENT National
Complex Regional Pain Syndrome Evidence Based Care Synopsis A COMPREHENSIVE PAIN MANAGEMENT APPROACH HOWARD KONOWITZ, MD BOARD CERTIFICATION: INTERNAL MEDICINE, ANESTHESIOLOGY, PAIN MANAGEMENT National
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Management of Acute Pain in the Chronic Pain Patient. Eric Cannon, MD Mountain West Anesthesia December 1, 2017
 Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics
 Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
Dr Kelly Jones Anesthesiologist at Northwest Orthopedics Decrease narcotic use in the immediate post operative period. Better Pain Control Less side effects then General Anesthesia Sedation Post operative
44th Annual CME Conference for Physician Assistants. Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine
 44th Annual CME Conference for Physician Assistants Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine Fifth Vital Sign: 15 years later Opioid Epidemic Relevant Disclosure and
44th Annual CME Conference for Physician Assistants Alexander Bautista, MD Assistant Professor Anesthesiology and Pain Medicine Fifth Vital Sign: 15 years later Opioid Epidemic Relevant Disclosure and
Pain Management and Opioid Abuse in the Surgical Patient
 The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Pain Management and Opioid Abuse in the Surgical Patient Darin J. Correll, M.D. Department of Anesthesiology, Perioperative and Pain
The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Pain Management and Opioid Abuse in the Surgical Patient Darin J. Correll, M.D. Department of Anesthesiology, Perioperative and Pain
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intrathecal Opioid Therapy for Management of Chronic Pain
 Intrathecal Opioid Therapy for Management of Chronic Pain Date of Origin: 01/2000 Last Review Date: 09/27/2017 Effective Date: 09/27/2017 Dates Reviewed: 11/2002, 12/2003, 12/2004, 12/2005, 12/2006, 12/2007,
Intrathecal Opioid Therapy for Management of Chronic Pain Date of Origin: 01/2000 Last Review Date: 09/27/2017 Effective Date: 09/27/2017 Dates Reviewed: 11/2002, 12/2003, 12/2004, 12/2005, 12/2006, 12/2007,
Digital RIC. Rhode Island College. Linda M. Green Rhode Island College
 Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 1-1-2013 The Relationship
Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 1-1-2013 The Relationship
A Gathering Storm: Evaluating Perioperative Opioids
 A Gathering Storm: Evaluating Perioperative Opioids Michael Bottros, MD Disclosure Nothing to disclose 1 Learning Objectives Describe the history of opioid prescribing practices in the United States Describe
A Gathering Storm: Evaluating Perioperative Opioids Michael Bottros, MD Disclosure Nothing to disclose 1 Learning Objectives Describe the history of opioid prescribing practices in the United States Describe
BUPIVACAINE LIPOSOME (EXPAREL): Adjunct to Regional Anesthesia
: Adjunct to Regional Anesthesia") BUPIVACAINE LIPOSOME (EXPAREL): Adjunct to Regional Anesthesia NEBRASKA ASSOCIATION OF NURSE ANESTHETISTS Spring Meeting: April 27-29, 2018 Sallie Poepsel, PhD, MSN, CRNA, APRN Director, AANA Region IV
BUPIVACAINE LIPOSOME (EXPAREL): Adjunct to Regional Anesthesia NEBRASKA ASSOCIATION OF NURSE ANESTHETISTS Spring Meeting: April 27-29, 2018 Sallie Poepsel, PhD, MSN, CRNA, APRN Director, AANA Region IV
Anesthesia Processing Guidelines
 Anesthesia Processing Guidelines Policy Number: 10.01.511 Last Review: 5/2018 Origination: 10/1988 Next Review: 5/2019 Policy The following guidelines are utilized in processing anesthesia claims: 1) Anesthesia
Anesthesia Processing Guidelines Policy Number: 10.01.511 Last Review: 5/2018 Origination: 10/1988 Next Review: 5/2019 Policy The following guidelines are utilized in processing anesthesia claims: 1) Anesthesia
Opioids Are Seniors at Risk? (April 26, 2018)
") Opioids Are Seniors at Risk? (April 26, 2018) Seniors are living longer and, with age, they become vulnerable to health challenges and the pain that may accompany them. Thus, it is perhaps not surprising
Opioids Are Seniors at Risk? (April 26, 2018) Seniors are living longer and, with age, they become vulnerable to health challenges and the pain that may accompany them. Thus, it is perhaps not surprising
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Objectives 9/7/2012. Optimizing Analgesia to Enhance the Recovery After Surgery CME FACULTY DISCLOSURE
 Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Achieving Optimal Therapeutic Outcomes in Pain Management from a Pharmacist's Perspective
 Achieving Optimal Therapeutic Outcomes in Pain Management from a Pharmacist s Perspective Chris Herndon, PharmD, BCPS, CPE Assistant Professor Southern Illinois University Edwardsville Clinical Pharmacy
Achieving Optimal Therapeutic Outcomes in Pain Management from a Pharmacist s Perspective Chris Herndon, PharmD, BCPS, CPE Assistant Professor Southern Illinois University Edwardsville Clinical Pharmacy
Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
 Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Pharmacist s Role In Pain Management. Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017
 Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Baptist Health Lexington. ERAS Protocols
 Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
Pain Management and Opioid Treatment Services
 Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
Pain Management and Opioid Treatment Services Davis, CA (530) 753-4300; Voice mail: (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net www.trainforchange.net www.tipsntopics.com www.asamcriteria.org
A Gathering Storm: Evaluating Perioperative Opioids
 A Gathering Storm: Evaluating Perioperative Opioids Michael Bottros, MD Disclosure Nothing to disclose 1 Objectives Describe the history of opioid prescribing practices in the United States Describe the
A Gathering Storm: Evaluating Perioperative Opioids Michael Bottros, MD Disclosure Nothing to disclose 1 Objectives Describe the history of opioid prescribing practices in the United States Describe the
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Enhanced Recovery to Optimize Perioperative Alternatives to Opioids
 Enhanced Recovery to Optimize Perioperative Alternatives to Opioids Women in Government, Annual Healthcare Summit Th 05 November 2017, Washington DC Timothy E. Miller, MB, ChB, FRCA Duke University Department
Enhanced Recovery to Optimize Perioperative Alternatives to Opioids Women in Government, Annual Healthcare Summit Th 05 November 2017, Washington DC Timothy E. Miller, MB, ChB, FRCA Duke University Department
Reimbursement Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1
 GE Healthcare Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for ultrasound
GE Healthcare Information for Ultrasound-guided Procedures Performed by Anesthesiologists 1 January, 2013 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for ultrasound
Light Solutions for wellness. Solutions for wellness. Patient information
 - NEURIMPULSE - NEURIMPULSE - NEURIM Light Solutions for wellness Solutions for wellness rimpulse.com Patient information - www.neurimpulse.com - www.neurimpulse.com - www.neurimpulse.com - www.neurimpulse.com
- NEURIMPULSE - NEURIMPULSE - NEURIM Light Solutions for wellness Solutions for wellness rimpulse.com Patient information - www.neurimpulse.com - www.neurimpulse.com - www.neurimpulse.com - www.neurimpulse.com
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
ICD-9-CM Diagnosis Code options
 ICD-9-CM Diagnosis Code options Diagnosis codes are used by both physicians and facilities to document the indication for the procedure. Intrathecal drug delivery is directed at managing chronic, intractable
ICD-9-CM Diagnosis Code options Diagnosis codes are used by both physicians and facilities to document the indication for the procedure. Intrathecal drug delivery is directed at managing chronic, intractable
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Treating Pain in Pediatrics: Safety First. Nicole Ralston, RN Jamie Sperduto, RN, BSN
 Treating Pain in Pediatrics: Safety First Nicole Ralston, RN Jamie Sperduto, RN, BSN Background Information Due to the current opioid crisis that most states are experiencing, it is necessary to institute
Treating Pain in Pediatrics: Safety First Nicole Ralston, RN Jamie Sperduto, RN, BSN Background Information Due to the current opioid crisis that most states are experiencing, it is necessary to institute
Opioids: What You Should Know About Opioid Prescribing. Denis G. Patterson, DO Nevada State Medical Association October 19, 2016
 Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
FACULTY OF PAIN MEDICINE
 PM4 (2005) FACULTY OF PAIN MEDICINE AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 GUIDELINES FOR PATIENT ASSESSMENT AND IMPLANTATION OF INTRATHECAL CATHETERS, PORTS AND PUMPS FOR
PM4 (2005) FACULTY OF PAIN MEDICINE AUSTRALIAN AND NEW ZEALAND COLLEGE OF ANAESTHETISTS ABN 82 055 042 852 GUIDELINES FOR PATIENT ASSESSMENT AND IMPLANTATION OF INTRATHECAL CATHETERS, PORTS AND PUMPS FOR
UCSF Pain Summit Multidisciplinary Approach to Acute and Chronic Pain
 Multidisciplinary Approach to Acute and Chronic Pain UCSF NIH Center of Excellence in Pain Education (CoEPE) UCSF Pain Research Group May 16, 2013, 8:30am-3:30pm Millberry Union, City Lights and Golden
Multidisciplinary Approach to Acute and Chronic Pain UCSF NIH Center of Excellence in Pain Education (CoEPE) UCSF Pain Research Group May 16, 2013, 8:30am-3:30pm Millberry Union, City Lights and Golden
Overview of Pain Types and Prevalence
 Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
Reimbursement Guidelines for Pain Management Procedures 1
 GE Healthcare Reimbursement Guidelines for Pain Management Procedures 1 April 2015 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for pain management procedures
GE Healthcare Reimbursement Guidelines for Pain Management Procedures 1 April 2015 www.gehealthcare.com/reimbursement This overview addresses coding, coverage, and payment for pain management procedures
Australian and New Zealand Registry of Regional Anaesthesia (AURORA)
") Australian and New Zealand Registry of Regional Anaesthesia (AURORA) Overview of Results First 4000 procedures recorded to - www.anaesthesiaregistry.org June 1st 2011 to February 2012 Background Australian
Australian and New Zealand Registry of Regional Anaesthesia (AURORA) Overview of Results First 4000 procedures recorded to - www.anaesthesiaregistry.org June 1st 2011 to February 2012 Background Australian
Cape Town Pain Clinic
 Cape Town Pain Clinic An Interdisciplinary approach to pain management Dr. Ché Venter Neurorehabilitation and Pain Practitioner Medico legal and RAF4 Independent medical Examiner MBChB (UCT) CIME MP 0686328
Cape Town Pain Clinic An Interdisciplinary approach to pain management Dr. Ché Venter Neurorehabilitation and Pain Practitioner Medico legal and RAF4 Independent medical Examiner MBChB (UCT) CIME MP 0686328
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Pain and patient experience: A business partnership Managing patients pain is no longer just a clinical goal it s a business necessity.
 Performance improvement Pain and patient experience: A business partnership Managing patients pain is no longer just a clinical goal it s a business necessity. The Centers for Medicare and Medicaid Services
Performance improvement Pain and patient experience: A business partnership Managing patients pain is no longer just a clinical goal it s a business necessity. The Centers for Medicare and Medicaid Services
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
The Team. Regional Anesthesia for Postoperative Pain Management. How Can We Reduce Pain? Understanding the Principles of Pain Process
 Regional Anesthesia for Postoperative Pain Management Chris Peltier, DNP, RN-BC, FNP-BC The Team Regional Anesthesia Pain Service (RAPS) University of Minnesota M-Health University of Minnesota Masonic
Regional Anesthesia for Postoperative Pain Management Chris Peltier, DNP, RN-BC, FNP-BC The Team Regional Anesthesia Pain Service (RAPS) University of Minnesota M-Health University of Minnesota Masonic
A Patient s Guide to Transcutaneous Electrical Stimulation (TENS) for Cervical Spine Pain
 for Cervical Spine Pain") A Patient s Guide to Transcutaneous Electrical Stimulation (TENS) for Cervical Spine Pain 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information
A Patient s Guide to Transcutaneous Electrical Stimulation (TENS) for Cervical Spine Pain 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information
Treatment of Pain in an Emergent Setting
 Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Updated: October 22, 2018 Prescribing Guidelines for Pennsylvania Treatment of Pain in an Emergent Setting Opioids, including heroin and fentanyl, contribute to thousands of overdose deaths in Pennsylvania
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO A. SUBJECT: Pediatric Pain Assessment and Management
 Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0318 A. SUBJECT: Pediatric Pain Assessment and Management B. EFFECTIVE DATE: April 1, 2014 This policy applies to all neonatal and pediatric
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0318 A. SUBJECT: Pediatric Pain Assessment and Management B. EFFECTIVE DATE: April 1, 2014 This policy applies to all neonatal and pediatric
PERIPHERAL REGIONAL BLOCKS. by Mike DeBroeck, DNP, CRNA
 PERIPHERAL REGIONAL BLOCKS by Mike DeBroeck, DNP, CRNA Why am I bothering with this topic at all? Do CRNAs REALLY even do peripheral regional anesthetics? YES!!!!!!! TOPICS GENERAL INFO SUCCESS RATES
PERIPHERAL REGIONAL BLOCKS by Mike DeBroeck, DNP, CRNA Why am I bothering with this topic at all? Do CRNAs REALLY even do peripheral regional anesthetics? YES!!!!!!! TOPICS GENERAL INFO SUCCESS RATES
Pain Management and Safe use of opioids in hospitals. Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN
 Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Clinical guideline Published: 27 June 2012 nice.org.uk/guidance/cg143
 Sickle cell disease: managing acute painful episodes in hospital Clinical guideline Published: 27 June 2012 nice.org.uk/guidance/cg143 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Sickle cell disease: managing acute painful episodes in hospital Clinical guideline Published: 27 June 2012 nice.org.uk/guidance/cg143 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Pain Management Clinic ISIC
 Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
Pain Management Clinic ISIC Let us rebuild a pain free life Pain is one of the commonest symptoms in patients attending OPDs of various hospitals and clinics. Chronic pain is any pain that has persisted
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
MOA: Practice Managers Program. Presented by: Kimber Debelak, CMC, CMOM, CMIS. May 17, zpain Management. & New Opioid Laws
 MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Index. Note: Page numbers of article titles are in boldface type. Pain Management in Critical Care
 Pain Management in Critical Care Index Note: Page numbers of article titles are in boldface type. Acetaminophen, for pain, 215 dosage of, 216 in children, 287-288 Addiction, to medication, defined, 277
Pain Management in Critical Care Index Note: Page numbers of article titles are in boldface type. Acetaminophen, for pain, 215 dosage of, 216 in children, 287-288 Addiction, to medication, defined, 277
Innovative Approaches and New Technology to Gain Access
 Innovative Approaches and New Technology to Gain Access The following is intended only for presentation to the Reimbursement and Access 2017 audience, August 17, 2017. This information is not for promotional
Innovative Approaches and New Technology to Gain Access The following is intended only for presentation to the Reimbursement and Access 2017 audience, August 17, 2017. This information is not for promotional
AVENUE THERAPEUTICS, INC. NASDAQ: ATXI JANUARY 2018
 AVENUE THERAPEUTICS, INC. NASDAQ: ATXI JANUARY 2018 Forward Looking Statements Statements in this presentation that are not descriptions of historical facts are forward-looking statements within the meaning
AVENUE THERAPEUTICS, INC. NASDAQ: ATXI JANUARY 2018 Forward Looking Statements Statements in this presentation that are not descriptions of historical facts are forward-looking statements within the meaning
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Pain Management. University of Illinois at Chicago College of Nursing
 Pain Management University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this module, participants will be better able to: 1. Define pain management 2. Explore various
Pain Management University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this module, participants will be better able to: 1. Define pain management 2. Explore various