Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
|
|
|
- Darlene McDowell
- 6 years ago
- Views:
Transcription

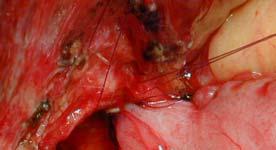
1 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation Strasbourg, IRCAD, October 2010 Bile Duct Injury during Lap Chole TOPICS 1. Prevalence, mechanisms, prevention and diagnosis 2. Treatment strategies: a. primary surgical repair b. postoperative biliary fistula c. biliary peritonitis d. biliary stricture
2 Local risk factors of BDI Multicenter Belgian Surveys Authors Period Patients type of clinical BDI rate procedure presentation Vereecken LC all type t 0.50 % Gigot < LC all type 0.50 % Vandesande LC all type 0.37 % all type all type 0.58 % Vandesande LC all typet 0.31 % all type all type 0.54 % Navez LC acute cholecystitis 1 % X 2 THE RISK FACTORS for BDI during LAP. CHOLE are MULTIFACTORIAL 1. factors inherent to the laparoscopic approach 2. inadequate training of the surgeon 3. local risk factors 4. Technical factors
 blind manipulation of instruments.")
 SURGEON EXPERIENCE and LOCAL RISK FACTORS * 15 10 5 0 50 100 150 200 250 300 350 400 450 Surgeon s s experience (Nb of LC)!")
3 1.RISK FACTORS INHERENT TO THE LAPAROSCOPIC APPROACH loss of depth perception loss of manual palpation surgeon's dependance to the equipment limited field easily obscured by bile or blood (loss of vision) blind manipulation of instruments. Nb of BDI anonymous survey on 9959 LC 65 patients with BDI (0.5 %) SURGEON EXPERIENCE and LOCAL RISK FACTORS * Surgeon s s experience (Nb of LC)! absent present < 50 cases : 55 % 45 % > 50 cases : 24 % 76 % p = 0.03 GIGOT, Surg Endosc 1997, 11 :





 3 large impacted i stone")

4 Laparoscopic belgian survey misidentification of cystic duct : the «classical» injury with CBD duct during IOC 6 % during dissection 35 % 43 % with cystic artery 1.5 % cystic duct avulsion CBD tenting Clipping during urgent haemostasis h DIFFICULT 3. LOCAL RISK FACTORSAND BILE DUCT INJURIES 3 acute or severe chronic inflammation!!! (65 %) 3 large impacted i stone in the Hartman pouch (16 %) 3 MIRIZZI syndrome +/- bilio-biliary biliary fistula (4%) 3 Morbid obesity 3 Anatomical anomalies complete cholangiogram!





5 In SEVERE CHOLECYSTITIS with anomalous RHD You can perform a Subtotal cholecystectomy leave a piece of gallbladder wall on the Calot triangle and at the level of the Hartman Pouch BDI during LC SEVERITY SITE ( BISMUTH classif. ) * lateral injury : 48% * complete transsection : 32% * resection : 10% * thermal : 11% * type I : 51% * type II : 28% * type III : 9% * type IV : 3% * type V : 9% 52% 21% GIGOT, Surg Endosc 1997; 11: 1171
6 BDI during LC : the Belgian Registry 65 patients CLINICAL PRESENTATION peroperative detection (29) : 44.5 % external biliary leak (8): 12% biliary peritonitis : - localized (biloma) (3): 6% - diffuse (19) : 29 %!!! biliary stricture : - early (3): 4.5% - late (3) : 4.5% 51 % Bile Duct Injury during Lap.Chole. TIMING of REPAIR * IMMEDIATE REPAIR : * small caliber of non dilated ducts (during the 1st op) * but absence of local inflammation * EARLY REPAIR : * non dilated ducts!!! (<2months) * local inflammation * sepsis and poor patients condition * LATE REPAIR : * optimized conditions (>2 months) * presence of ductal dilatation with fibrotic tissues




7 1.Early REPAIR of BDI risk factors for late stricture THERMAL INJURY In 1/3 of BDI VASCULAR INJURY 30-50% type IV : 60 % Stewart et al. Ann Surg 2003; 237: 460 Patients Mortality Biliary Reinterv. FU (mo) Recurrent complic. median Stricture. Perop. detect. : 7 % 24 % 14 % %. Peritonitis : 20 % 50 % 23 % % 29 % 47 % PHILOSOPHY of TREATMENT Laparoscopic cholecystectomy = minimally invasive procedure BDI = maximally invasive situation change your philosophy treat properly medico legal consequences
8 Bile Duct Injury during Lap.Chole. MANAGEMENT of BILE DUCT INJURY DIAGNOSED EARLY after LAPAROSCOPIC CHOLECYSTECTOMY 3 types of postoperative clinical presentations : external biliary fistula bile peritonitis obstructive jaundice from biliary stricture 1. Postoperative Biliary Fistula RADIOLOGICAL EVALUATION PURPOSE AVOID to REOPERATE before complete evaluation 1. to define site and severity of BDI 2. to evaluate the intraabdominal bile leakage 3. to detect coexistent injury TYPE of IMAGING STUDIES 1. CT with contrast injection is superior to US 2. MRI is a all-in exam (cholangio + angio-mri) to define lesions 3. ERCP is the most useful tool in partial injury (excepted if complete obstruction or transsection)
9 CT or (MRI) diffuse bile peritonitis SURGERY localized biloma Percut. RX drainage if - persistant > 1 week or worsening - LFTs elevated (obstruction?) - total biliary diversion * no o collection * good clinical condition WAIT - amount of bile / 24 h. - evolution of biliary leak ERCP to define ERCP type / site / severity cystic, Luchka * partial injury * complete transsection ducts * lat. clipping * resection ES + prosthesis ES + prosthesis or surgery SURGERY ENDOSCOPIC Efficient endoscopic MANAGEMENT management
10 2.POST- OPERATIVE BILIARY PERITONITIS! High suspicion s for BDI B should be maintained for any patient who do not recover normally and quickly after LC. The mean delay for reoperation in the Belgian registry was 11 days (1 21) MANAGEMENT of BILIARY PERITONITIS EMERGENCY TREATMENT * septic condition ( infected bile) * long standing peritonitis * good clinical condition * recent peritonitis ERCP LAPAROTOMY * peritoneal lavage * biliary drainage - bilio- digestive anastomosis.. if possible - otherwise, external diversion complete laceration partial laceration, cystic or Luchka duct 1. endoprosthesis 2. percutaneous or surgical drainage (lap or open) clinical improvement no residual bile collections on repeat CT examination


11 classification of injury by IOC -type - severity partial injury complete transsection wide resection thermal necrosis suture suture+ T tube HJA. excise and HJA + T tube T HJA. diversion partial laceration of the choledochus






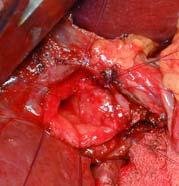
12 END-to to-end BILIARY REPAIR CAUSES of FAILURES * loss of ductal tissue * tension on the suture line * inadequate blood supply (thermal injury) * small caliber of the ducts * proximal location of BDIB BDI due to an ANOMALOUS R. HEPATIC DUCT lateral BDI to anomalous RLD during delayed LC for severe cholecystitis primary repair by suture with T-tube T insertion



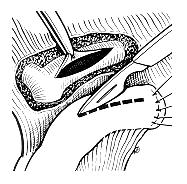
13 BDI due to to an ANOMALOUS R. R. HEPATIC DUCT STRATEGY OF TREATMENT do a selective cholangiography!! if limited biliary sector and thin duct if large biliary sector and large stoma if large biliary sector and thin duct then, close it permanently make a repair (suture + Tube or HJA) clip temporary and come back later, when dilated TOTAL BILIARY DIVERSION INDICATIONS when a biliary repair is impossible or unsafe - proximal thermal necrosis - severe inflammation - tiny proximal duct TECHNIQUE drain into the proximal biliary stump multiples large sub-hepatic drains.. NOT too close of the hepatoduodenal ligament.. risk of vascular injury! (large sub-hepatic omentoplasty)


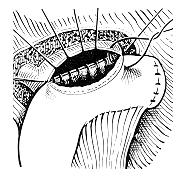
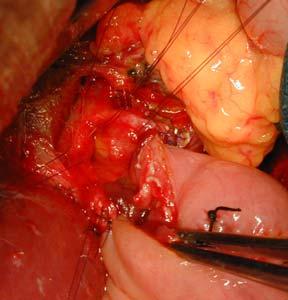

14 Hepatico-jejunal anastomosis: The HEPP-COUINAUD APPROACH Hepatico-jejunal anastomosis: The HEPP-COUINAUD APPROACH «mucosa-to to-mucosa» hepatico-jejunostomy
 is mandatory before")


15 BILE DUCT INJURY during LAP. CHOLE Long-term follow-up (at( least 10 years) is mandatory before definitive conclusions about the outcome of BDI. Female, 74y 1994: type IV BDI post lap chole Hepp Couinaud HJA FU once a year in outpatient clinic (biology and cholangiomri) Completely asymptomatic with normal follow up untill june 2009 April and June 2009: Cholangitis Normal LFT (after cholangitis) MRI:! Stenosis at the level of the LHD CLINICAL CASES


16 Clinical case : 1 CT SCAN ERCP Female, 35y D1: abdominal pain CRP: 22 WBC: Normal LFT WHAT SHOULD YOU DO? 1. Wait and see 2. Percutaneous drain alone 3. Endoprothesis alone 4. Percutaneous drain and endoprothesis 5. Open Hepatico-jejunostomy and peritoneal lavage




17 Clinical case : 1 Answer: 4.Endoprothesis and percutaneous drain Clinical case 2 * F 30 years-old * Lap chole 9 days ago Bile peritonitis Sepsis++ ERCP



18 1.Wait and see 2. Endoprothesis and percutaneous drain 3.Surgical exploration Answer: 3. Surgical exploration D9: Surgical exploration: excision ion of EHBD and main biliary convergence Diffuse Biliary peritonitis
19 1. Peritoneal lavage and direct end to end suture 2. Peritoneal lavage and suture with T-tube insertion 3. Peritoneal lavage and hepatico-jejunal anastomosis 4.Peritoneal lavage and external biliary diversion Clinical case : 2 Answer: 4.Peritoneal lavage and external biliary diversion
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Bile Duct Injuries. Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
, MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India") Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Common Bile Duct Injury: Recognition and Management
 Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
Biliary Anatomy in Living-related Liver Transplantation
 The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
LAPAROSCOPIC SPLENECTOMY
 LAPAROSCOPIC SPLENECTOMY Catherine HUBERT Jean François GIGOT Benoît NAVEZ Strasboug, IRCAD October 2011 Division of Hepato Bilio Pancreatic Surgery Department of Abdominal Surgery and Transplantation
LAPAROSCOPIC SPLENECTOMY Catherine HUBERT Jean François GIGOT Benoît NAVEZ Strasboug, IRCAD October 2011 Division of Hepato Bilio Pancreatic Surgery Department of Abdominal Surgery and Transplantation
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Bile duct injuries related to misplacement of T tubes
 Annals of Hepatology 2006; 5(1): January-March: 44-48 Original Article Annals of Hepatology Bile duct injuries related to misplacement of T tubes Miguel Ángel Mercado;* Carlos Chan; Héctor Orozco;* Alexandra
Annals of Hepatology 2006; 5(1): January-March: 44-48 Original Article Annals of Hepatology Bile duct injuries related to misplacement of T tubes Miguel Ángel Mercado;* Carlos Chan; Héctor Orozco;* Alexandra
Post Laparoscopic Cholecystectomy Biloma in a Child Managed by Endoscopic Retrograde Cholangio-Pancreatography and Stenting: A Case Report
 pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.281 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):281-285 Case Report PGHN Post Laparoscopic Cholecystectomy Biloma in
pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.281 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):281-285 Case Report PGHN Post Laparoscopic Cholecystectomy Biloma in
Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES
 Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES Yunfeng Cui, Hongtao Zhang, Naiqiang Cui, Zhonglian Li* Department of Surgery, Tianjin Nankai Hospital,
Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES Yunfeng Cui, Hongtao Zhang, Naiqiang Cui, Zhonglian Li* Department of Surgery, Tianjin Nankai Hospital,
LAPAROSCOPIC SPLENECTOMY
 LAPAROSCOPIC SPLENECTOMY Strasboug, IRCAD October 2010 Catherine HUBERT Jean François GIGOT Benoît NAVEZ Division of Hepato Bilio Pancreatic Surgery Department of Abdominal Surgery and Transplantation
LAPAROSCOPIC SPLENECTOMY Strasboug, IRCAD October 2010 Catherine HUBERT Jean François GIGOT Benoît NAVEZ Division of Hepato Bilio Pancreatic Surgery Department of Abdominal Surgery and Transplantation
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Laparoscopic Subtotal Cholecystectomy for Difficult Acute Calculous Cholecystitis
 Journal of Surgery 2017; 5(6): 111-117 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.15 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Laparoscopic Subtotal Cholecystectomy
Journal of Surgery 2017; 5(6): 111-117 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.15 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Laparoscopic Subtotal Cholecystectomy
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Gallstones & Other Biliary Disorders
 Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing
Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study
 Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
White Rose Research Online URL for this paper: Version: Accepted Version
 This is a repository copy of Delayed referral to specialist centre increases morbidity in patients with bile duct injury (BDI) after laparoscopic cholecystectomy (LC). White Rose Research Online URL for
This is a repository copy of Delayed referral to specialist centre increases morbidity in patients with bile duct injury (BDI) after laparoscopic cholecystectomy (LC). White Rose Research Online URL for
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article:
Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA ABSTRACT
, Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA ABSTRACT") Hiroshima J. Med. Sci. Vol. 64, No. 3, 45~49, September, 2015 HIJM 64 8 45 Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA Department
Hiroshima J. Med. Sci. Vol. 64, No. 3, 45~49, September, 2015 HIJM 64 8 45 Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA Department
Overview of PSC Making the Diagnosis
 Overview of PSC Making the Diagnosis Tamar Taddei, MD Assistant Professor of Medicine Yale University School of Medicine Overview Definition Epidemiology Diagnosis Modes of presentation Associated diseases
Overview of PSC Making the Diagnosis Tamar Taddei, MD Assistant Professor of Medicine Yale University School of Medicine Overview Definition Epidemiology Diagnosis Modes of presentation Associated diseases
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
cholangiopancreatography
 1250 Hepatopancreatic-Biliary Unit, Academic Medical Centre, University of Amsterdam, The Netherlands P H P Davids J Ringers E A J Rauws L Th de Wit K Huibregtse M N van der Heyde G N J Tytgat Correspondence
1250 Hepatopancreatic-Biliary Unit, Academic Medical Centre, University of Amsterdam, The Netherlands P H P Davids J Ringers E A J Rauws L Th de Wit K Huibregtse M N van der Heyde G N J Tytgat Correspondence
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
T-TUBE DRAINAGE VERSUS PRIMARY COMMON BILE DUCT CLOSURE AFTER OPEN CHOLEDOCHOTOMY
 T-TUBE DRAINAGE VERSUS PRIMARY COMMON BILE DUCT CLOSURE AFTER OPEN CHOLEDOCHOTOMY Khaled Ahmed El- Dabee, Abd Al-Lateif Ahmed, Mohamed Abdel Aziz Abdel Jawad, Taha Bahgat Salam, Ahmed Eisa Ahmed* and Saed
T-TUBE DRAINAGE VERSUS PRIMARY COMMON BILE DUCT CLOSURE AFTER OPEN CHOLEDOCHOTOMY Khaled Ahmed El- Dabee, Abd Al-Lateif Ahmed, Mohamed Abdel Aziz Abdel Jawad, Taha Bahgat Salam, Ahmed Eisa Ahmed* and Saed
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study
 Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
cholecystectomy Treatment of bile duct lesions after laparoscopic cholecystectomy does, however, carry an injuries.7 11 Comparatively few papers,9 12
 Gut 1996; 38: 141-147 Treatment of bile duct lesions after laparoscopic cholecystectomy 141 Departments of Gastroenterology J J G H M Bergman G R van den Brink E A J Rauws K Huibregtse G N J Tytgat and
Gut 1996; 38: 141-147 Treatment of bile duct lesions after laparoscopic cholecystectomy 141 Departments of Gastroenterology J J G H M Bergman G R van den Brink E A J Rauws K Huibregtse G N J Tytgat and
Arpit Amin, Yuriy Zhurov, George Ibrahim, Anthony Maffei, Jonathan Giannone, Thomas Cerabona, and Ashutosh Kaul
 Case Reports in Surgery Volume 2016, Article ID 1896368, 9 pages http://dx.doi.org/10.1155/2016/1896368 Case Report Combined Endoscopic and Management of Postcholecystectomy Mirizzi Syndrome from a Remnant
Case Reports in Surgery Volume 2016, Article ID 1896368, 9 pages http://dx.doi.org/10.1155/2016/1896368 Case Report Combined Endoscopic and Management of Postcholecystectomy Mirizzi Syndrome from a Remnant
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Bile duct injuries following laparoscopic cholecystectomy
 570088SJS0010.1177/1457496915570088A. Viste, et al. research-article2015 ORIGINAL ARTICLE Bile duct injuries following laparoscopic cholecystectomy A. Viste 1,2, A. Horn 1, K. Øvrebø 1, B. Christensen
570088SJS0010.1177/1457496915570088A. Viste, et al. research-article2015 ORIGINAL ARTICLE Bile duct injuries following laparoscopic cholecystectomy A. Viste 1,2, A. Horn 1, K. Øvrebø 1, B. Christensen
Repair 0ptions Following Iatrogenic Bile Duct Injuries
 Journal of Surgery 2015; 3(5): 50-55 Published online October 23, 2015 (http://www.sciencepublishinggroup.com/j/js) doi: 10.11648/j.js.20150305.12 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Repair
Journal of Surgery 2015; 3(5): 50-55 Published online October 23, 2015 (http://www.sciencepublishinggroup.com/j/js) doi: 10.11648/j.js.20150305.12 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Repair
IMPROVEMENT OF SURGICAL TREATMENT OF INTRAOPERATIVE
 Open Access Research Journal www.pradec.eu Medical and Health Science Journal, MHSJ ISSN: 1804-1884 (Print) 1805-5014 (Online) Volume 10, 2012, pp.41-46 IMPROVEMENT OF SURGICAL TREATMENT OF INTRAOPERATIVE
Open Access Research Journal www.pradec.eu Medical and Health Science Journal, MHSJ ISSN: 1804-1884 (Print) 1805-5014 (Online) Volume 10, 2012, pp.41-46 IMPROVEMENT OF SURGICAL TREATMENT OF INTRAOPERATIVE
A RARE EXTRAHEPATIC BILIARY ANOMALY
 HPB Surgery 1989, Vol. 1, pp. 353-358 Reprints available directly from the publisher Photocopying permitted by license only 1989 Harwood Academic Publishers GmbH Printed in Great Britain CASE REPORT A
HPB Surgery 1989, Vol. 1, pp. 353-358 Reprints available directly from the publisher Photocopying permitted by license only 1989 Harwood Academic Publishers GmbH Printed in Great Britain CASE REPORT A
Imaging of Biliary Tract Emergencies in Jorge A. Soto, MD Professor of Radiology Boston University Medical Center.
 Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing
 Focus on Surgical Techniques from Bench to Bedside Page 1 of 9 Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing Michail Karanikas 1, Ferdi Bozali 1, Vasileia Vamvakerou
Focus on Surgical Techniques from Bench to Bedside Page 1 of 9 Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing Michail Karanikas 1, Ferdi Bozali 1, Vasileia Vamvakerou
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
Mirizzi syndrome with an unusual type of biliobiliary fistula a case report
 Kawaguchi et al. Surgical Case Reports (2015) 1:51 DOI 10.1186/s40792-015-0052-2 CASE REPORT Mirizzi syndrome with an unusual type of biliobiliary fistula a case report Tsutomu Kawaguchi 1,2*, Tadao Itoh
Kawaguchi et al. Surgical Case Reports (2015) 1:51 DOI 10.1186/s40792-015-0052-2 CASE REPORT Mirizzi syndrome with an unusual type of biliobiliary fistula a case report Tsutomu Kawaguchi 1,2*, Tadao Itoh
Biliary MRI w Eovist
 Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
SUNY Downstate Medical Center Kings County Hospital
 Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
CHOLECYSTECTOMY CONSENT FORM
 1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
Cholecystectomy. Sarah Forsyth
 Cholecystectomy Sarah Forsyth History of Cholecystectomy First open cholecystectomy 1882 by Carl Langenbuch in Germany First lap cholecystectomy 1987, Philip Mouret (Gynaecologist) in Lyon, France 1990,
Cholecystectomy Sarah Forsyth History of Cholecystectomy First open cholecystectomy 1882 by Carl Langenbuch in Germany First lap cholecystectomy 1987, Philip Mouret (Gynaecologist) in Lyon, France 1990,
ISSN X (Print) Research Article. *Corresponding author Bikramjit Pal
 Research Article. *Corresponding author Bikramjit Pal") Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(5F):1900-1905 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(5F):1900-1905 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
No 72-hour pathological boundary for safe early laparoscopic cholecystectomy in acute cholecystitis: a clinicopathological study
 Original article Annals of Gastroenterology (2013) 26, 1-6 No 72-hour pathological boundary for safe early laparoscopic cholecystectomy in acute cholecystitis: a clinicopathological study Rachel M. Gomes
Original article Annals of Gastroenterology (2013) 26, 1-6 No 72-hour pathological boundary for safe early laparoscopic cholecystectomy in acute cholecystitis: a clinicopathological study Rachel M. Gomes
Surveillance proposal consultation document
 Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Comparison Between Primary Closure of Common Bile Duct and T- Tube Drainage After Open Choledocholithiasis: A Hospital Based Study
 Original article: Comparison Between Primary Closure of Common Bile Duct and T- Tube Drainage After Open Choledocholithiasis: A Hospital Based Study Kali CharanBansal Principal Specialist (General surgery)
Original article: Comparison Between Primary Closure of Common Bile Duct and T- Tube Drainage After Open Choledocholithiasis: A Hospital Based Study Kali CharanBansal Principal Specialist (General surgery)
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Guidelines for Laparoscopic CBD Exploration
 Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Stenting of the Cystic Duct in Benign Disease: A Definitive Treatment for the Elderly and Unwell
 Cardiovasc Intervent Radiol (2015) 38:964 970 DOI 10.1007/s00270-014-1014-y CLINICAL INVESTIGATION NON-VASCULAR INTERVENTIONS Stenting of the Cystic Duct in Benign Disease: A Definitive Treatment for the
Cardiovasc Intervent Radiol (2015) 38:964 970 DOI 10.1007/s00270-014-1014-y CLINICAL INVESTIGATION NON-VASCULAR INTERVENTIONS Stenting of the Cystic Duct in Benign Disease: A Definitive Treatment for the
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page
 Vol. 72 (9), Page") The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page 5153-5160 Role of Interventional Radiology in the Management of Postoperative Biliary Complications 1 Hana Hamdy Nasif, 1 Mennatallah
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (9), Page 5153-5160 Role of Interventional Radiology in the Management of Postoperative Biliary Complications 1 Hana Hamdy Nasif, 1 Mennatallah
Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy
 Gut and Liver, Vol. 7, No. 3, May 2013, pp. 352-356 ORiginal Article Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy Hosur Mayanna Lokesh,
Gut and Liver, Vol. 7, No. 3, May 2013, pp. 352-356 ORiginal Article Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy Hosur Mayanna Lokesh,
The Endoscopic Management of PSC
 The Endoscopic Management of PSC Raj J. Shah, M.D. Associate Professor of Medicine Director, Pancreaticobiliary Endoscopy Services University of Colorado at Denver and the Health Sciences Center Why did
The Endoscopic Management of PSC Raj J. Shah, M.D. Associate Professor of Medicine Director, Pancreaticobiliary Endoscopy Services University of Colorado at Denver and the Health Sciences Center Why did
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN VAN DER LEIJ, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+
 THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+ DISCLOSURES None 78 Y/O FEMALE Painful RUQ Fever Lab: Raised Leukocytes/CRP CHOLECYSTITIS 3-9% patients ER
THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+ DISCLOSURES None 78 Y/O FEMALE Painful RUQ Fever Lab: Raised Leukocytes/CRP CHOLECYSTITIS 3-9% patients ER
Comparison between primary closure and T-tube drainage after open choledocotomy
 ISSN: 2203-1413 Vol.03 No.04 Comparison between primary closure and T-tube drainage after open choledocotomy Alireza Barband 1, Farzad Kakaei 1, Morteza Ghojazadeh 2, Abdolhamid Chavoshi Khamneh 1*, Morteza
ISSN: 2203-1413 Vol.03 No.04 Comparison between primary closure and T-tube drainage after open choledocotomy Alireza Barband 1, Farzad Kakaei 1, Morteza Ghojazadeh 2, Abdolhamid Chavoshi Khamneh 1*, Morteza
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Gum O Jung and Dong Eun Park. Department of Surgery, Wonkwang University Hospital, Wonkwang University School of Medicine, Iksan, Korea
 Korean J Hepatobiliary Pancreat Surg 2012;16:110-114 Case Report Successful percutaneous management of bronchobiliary fistula after radiofrequency ablation of metastatic cholangiocarcinoma in a patient
Korean J Hepatobiliary Pancreat Surg 2012;16:110-114 Case Report Successful percutaneous management of bronchobiliary fistula after radiofrequency ablation of metastatic cholangiocarcinoma in a patient
LAPAROSCOPIC GALLBLADDER SURGERY
 LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
laparoscopic cholecystectomy
 Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
Technical Guidance for Surgical Workload Audit and Research Database: Cholecystectomy V1.0
 Technical Guidance for Surgical Workload Audit and Research Database: Cholecystectomy V1.0 Contents 1. The Indicators... 3 1.1. Activity Volume... 3 3.2. Average Length of Stay (Days)... 3 3.3. 2/7/30
Technical Guidance for Surgical Workload Audit and Research Database: Cholecystectomy V1.0 Contents 1. The Indicators... 3 1.1. Activity Volume... 3 3.2. Average Length of Stay (Days)... 3 3.3. 2/7/30
In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo Shin Choi 2, and Seung Eun Lee 2. Departments of Surgery, Dongguk University College of Medicine 2
 Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Systematic Review of Mirizzi's Syndrome's Management
 REVIEW ARTICLE Systematic Review of Mirizzi's Syndrome's Management Mallikarjuna Uppara, Ashraf Rasheed Gwent Centre for Digestive Diseases University of South Wales, United Kingdom ABSTRACT Background
REVIEW ARTICLE Systematic Review of Mirizzi's Syndrome's Management Mallikarjuna Uppara, Ashraf Rasheed Gwent Centre for Digestive Diseases University of South Wales, United Kingdom ABSTRACT Background
LAPAROSCOPIC CHOLECYSTECTOMY DON J. SELZER, MD, AND KEITH D. LILLEMOE, MD
 CHAPTER 130 LAPAROSCOPIC CHOLECYSTECTOMY DON J. SELZER, MD, AND KEITH D. LILLEMOE, MD Laparoscopic cholecystectomy, reported by Reddick in 1989, began a revolution in surgical practice. Improvements in
CHAPTER 130 LAPAROSCOPIC CHOLECYSTECTOMY DON J. SELZER, MD, AND KEITH D. LILLEMOE, MD Laparoscopic cholecystectomy, reported by Reddick in 1989, began a revolution in surgical practice. Improvements in
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 4/ Issue 42/ May 25, 2015 Page 7258
 LAPAROSCOPIC COMPLETION CHOLECYSTECTOMY FOR POST CHOLECYSTECTOMY SYNDROME Zahur Hussain 1, Himanshu Sharma 2, Vikrant Singh Chandail 3, Barinder Kumar 4, Suneel Mattoo 5, Ashufta Rasool 6, Anshuman Sharma
LAPAROSCOPIC COMPLETION CHOLECYSTECTOMY FOR POST CHOLECYSTECTOMY SYNDROME Zahur Hussain 1, Himanshu Sharma 2, Vikrant Singh Chandail 3, Barinder Kumar 4, Suneel Mattoo 5, Ashufta Rasool 6, Anshuman Sharma
Title. Author(s) Issue Date Right.
 Issue Date Right.") NAOSITE: Nagasaki University's Ac Title Author(s) Citation Results of elective laparoscopic ch following percutaneous transhepatic Kuroki, Tamotsu; Kitasato, Amane; T Hiroaki; Taniguchi, Ken; Maeda, Shi
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Results of elective laparoscopic ch following percutaneous transhepatic Kuroki, Tamotsu; Kitasato, Amane; T Hiroaki; Taniguchi, Ken; Maeda, Shi
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
Portal Vein in a Patient Undergoing Hepatic Resection
 HPB Surgery, 1997, Vol. 10, pp. 323-327 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
HPB Surgery, 1997, Vol. 10, pp. 323-327 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
Conversion to Open Cholecystectomy Implications of Decision Making. Mr.. Val Usatoff HPB Surgeon Alfred and Western Hospitals
 Conversion to Open Cholecystectomy Implications of Decision Making Mr.. Val Usatoff HPB Surgeon Alfred and Western Hospitals Open Cholecystectomy Born 1882 Unwell early 1990 s Fading fast late 1990 s 21st
Conversion to Open Cholecystectomy Implications of Decision Making Mr.. Val Usatoff HPB Surgeon Alfred and Western Hospitals Open Cholecystectomy Born 1882 Unwell early 1990 s Fading fast late 1990 s 21st
Pre-operative prediction of difficult laparoscopic cholecystectomy
 International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20151083 Pre-operative prediction of difficult laparoscopic
International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20151083 Pre-operative prediction of difficult laparoscopic
Postoperative Bile Duct Strictures: Management and Outcome in the 1990s
 ANNALS OF SURGERY Vol. 232, No. 3, 430 441 2000 Lippincott Williams & Wilkins, Inc. Postoperative Bile Duct Strictures: Management and Outcome in the 1990s Keith D. Lillemoe, MD, Genevieve B. Melton, MD,
ANNALS OF SURGERY Vol. 232, No. 3, 430 441 2000 Lippincott Williams & Wilkins, Inc. Postoperative Bile Duct Strictures: Management and Outcome in the 1990s Keith D. Lillemoe, MD, Genevieve B. Melton, MD,
Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis
 Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Quality & Safety Committee 17 th August 2017 Agenda item: 6.2
 SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
The role of cholangiography with t-tube in the liver transplantation
 The role of cholangiography with t-tube in the liver transplantation Poster No.: C-0362 Congress: ECR 2012 Type: Educational Exhibit Authors: S. Magalhães, I. Ferreira, A. B. Ramos, F. Reis, M. Ribeiro
The role of cholangiography with t-tube in the liver transplantation Poster No.: C-0362 Congress: ECR 2012 Type: Educational Exhibit Authors: S. Magalhães, I. Ferreira, A. B. Ramos, F. Reis, M. Ribeiro
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
JMSCR Vol 05 Issue 04 Page April 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i4.11 Post Cholecystectomy Stump Calculus Cholecystitis
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i4.11 Post Cholecystectomy Stump Calculus Cholecystitis