Superficial Varicose and Deep Vein Concerns - ACOI Chicago Hospitalist Meeting
|
|
|
- August Terry
- 5 years ago
- Views:
Transcription
1 Superficial Varicose and Deep Vein Concerns - ACOI Chicago Hospitalist Meeting Davin Haraway DO,FACOI,FACCWS,RPhS Diplomate American Board of Venous and Lymphatic Medicine
2 Vein issues encountered by Hospitalists Cellulitis Infected venous stasis ulcerations Leg ulcers consultations for evaulation and treatment Lymphedema Lymphangitis Superficial thrombophlebitis Post phlebetic syndrome Pulmonary Embolus Acute DVT at or above Common femoral vein Acute DVT below the Common femoral vein Upper extremity DVT Phlegmesia Cerula Dolens Venous malformations Stasis dermatitis vs Cellulitis vs hemosiderosis, vs calciphylaxis
3 Who do you hand off when the patient is discharged and what do you recommend? Sleep study Education on lymphedema treatment Referral to OP wound care/hbo Referral to phlebologist Who is going to manage their DVT/Anticoagulants/Stents Who is going to manage their wound care Do you have local support and know providers in the community to help the PCP?
4 Impact on venous disease outside the hospital


5 Davin Haraway DO,FACOI,FACCWS,RPhS Diplomate Certified American Board of Venous and Lymphatic Medicine

6 Outline Incidence and prevalence Anatomy Function and Physiology diagnosis Classification Conservative tx Intervention treatment Special considerations




7 What I see
8 What I do
9






10 The Spectrum of Chronic Venous Disease telangiectasias superficial phlebitis varicose veins lipodermatosclerosis venous ulceration


11


12
13 Prevalence of Chronic Venous Disease 1 in 22 or 4.5% or 12.2 million people in the USA are affected by varicose veins Incidence increases with age and is more common in women with over 40% of women in their 50 s suffering from some sort of venous disorder Across all ages and gender, 60% of Americans suffer from venous disease and its sequelae National Heart Lung and Blood Institute (NHLBI)
14 Population Tulsa County 603,403 Age ,512 Female 51% 73,191 Male 50% 71,756 Age % prevalence 23,106 Age % prevalence 16,833 Age % prevalence 13,260 Age % prevalence 7,096 50% pathologic reflux 11,553 50% pathologic reflux 8,416 50% pathologic reflux 6,630 50% pathologic reflux 3, % GSV reflux 1,964-5, % GSV reflux 1,430-3, % GSV reflux 1,127-3, % GSV reflux 603-1,632 Total patients that would potentially just need GSV treatment by endothermal ablation range from 5,124 to 13,866 if symptomatic. A portion of these patients will need Phlebectomy and /or Ultrasound guided sclerotherapy in addition to endothermal ablation all of which are reimbursable procedures by most Insurance carriers when symptomatic. This assumes that all patients were healthy on a population basis. Age years total 143,512 from Tulsa City Statistics 77% of this age group are years old and 23% age55 64 years old.
15 65 and older 50,508 Female 72% prevalence 31,007 x 0.72= 22,325 Male 43% prevalence 19,501 x 0.43 = 8, % GSV reflux 3,795-10, % GSV reflux 1, Medicare age patients with potential GSV reflux could be treated with endothermal ablation if symptomatic would range from 5,220 to 14,126. Medicare has coverage criteria for symptomatic patients. Patients from age group 35 to over 65 total 10,344 27,922 in the Tulsa County
16
17 Who should be screened? Patients with typical symptoms of venous disease with a constellation of symptoms of Big varicosities that are symptomatic or a history of Venous Ulcerations or no skin changes at all could include: Aching Fatigue, heaviness in legs Pain: throbbing, burning, stabbing Cramping Swelling (peripheral edema) Itching Restless legs Numbness Leg ulcerations usually on the lower leg could be medial or lateral with typically acceptable arterial circulation What s their ABI not to miss Arterial disease
18 Are Vein procedures covered by my insurance? By and large if a patient has symptomatic venous disease with duplex findings of Reflux and enlarged size veins(variable to the insurance) of the GSV and or SSV and tributaries then Insurance will typically cover their treatment Of course some insurances are more strict. Insurance LCD Also dictate mostly that the axial Veins of the GSV/SSV must be treated first before tributary disease can be covered Foam and Liquid Sclerotherapy of veins less than 3mm and no reflux typically are not covered and are treated if symptomatic or at the desire of the patient for a more esthetic outcome on a Cash basis. (most SYMPTOMS are improved with treatment of the above however the end result is driven by the patient for cosmetic appearance).
19 Frequently Asked Questions What does my poor circulation have to do with my swelling? We educate our patients on distinguishing between arterial, venous, and lymphatic circulation and go over their particular factors for their swelling verbally and with a diagram. I have stasis eczema what is that I use hydrocortisone on my legs for years why is that? Draw Diagram How I educate patients on their Edema.
20 Do I have to wear Compression stockings? Compression stockings are a very important part of treating chronic venous disease Depending on where the patient is on the spectrum of their particular disease process they may be recommended to always wear their compression hose(especially if Deep Reflux) or they may not need to wear their hose after their treatment if ALL reflux has been treated and no further symptoms. HOWEVER All insurance Carriers start with a period of conservative treatment which includes Compression hose NOT TED hose typically 20-30mmHg compression VENOUS DISEASE IS A CONDITION OF CHRONICITY AND MUST BE FOLLOWED NEW AREAS OF REFLUX WILL LIKELY DEVELOP IN THE FUTURE AND MAY BE DEALT WITH EXPECTANTLY to not notify a patient of this would disappoint the patient.
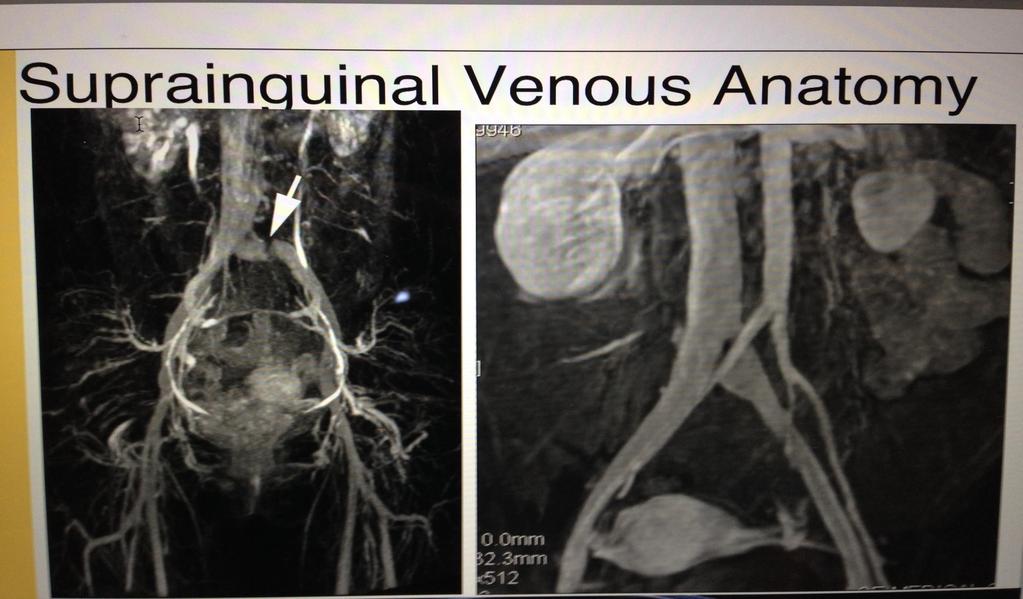
21 Anatomy
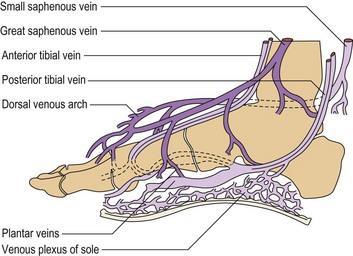
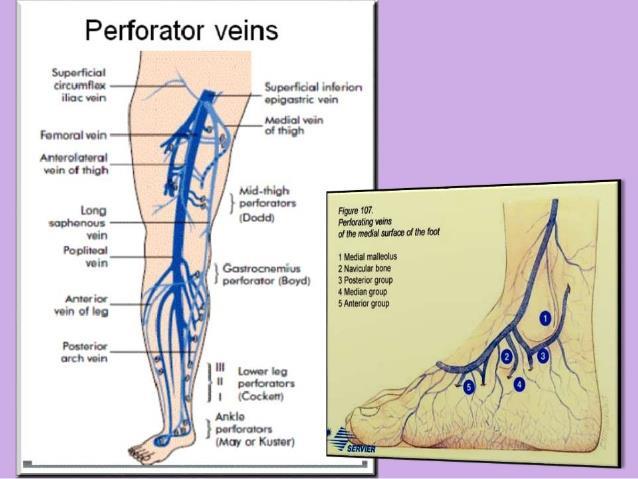
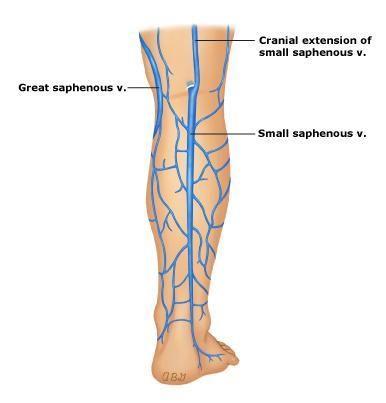
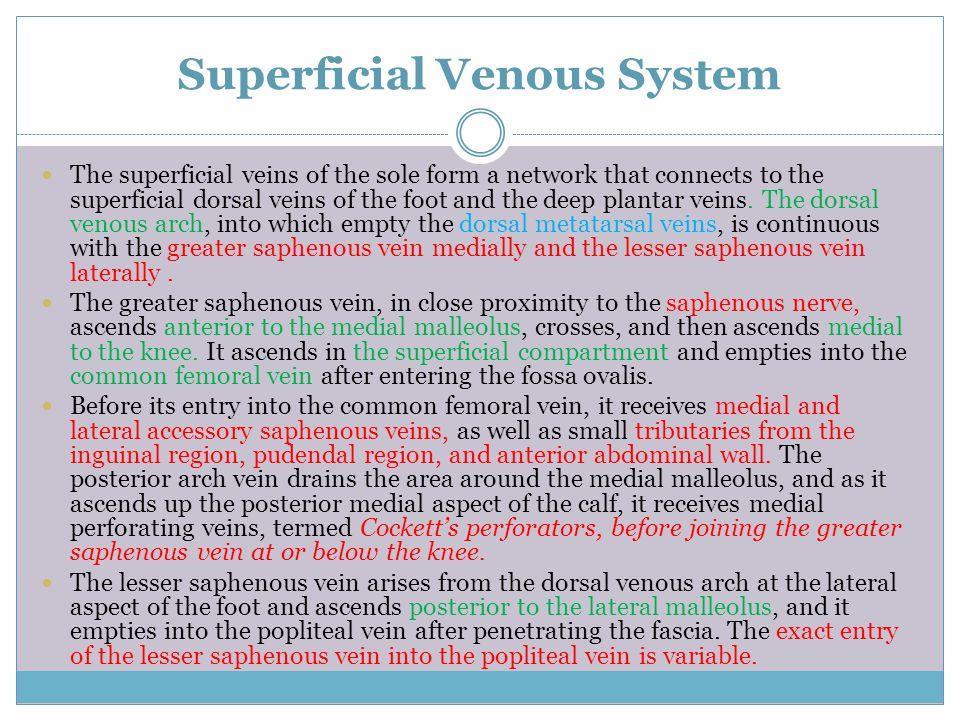
22 It all begins in the feet Vein anatomy that is In general venous flow should be from superficial to deep in the lower extremity the exception is the foot where there are general lack of valves in the deep veins of the foot that have outward flow thru perforators into the superficial venous arch that constitute the origins of the GSV and SSV. And otherwise directly communicate with the Posterior tibial and peroneal/anterior tibial veins.

23
24


25 Covered by muscle Not covered by muscle
26
27
28

29

30
31

32 What do you tell your patients about this?




33

34

35

36


37



38

39



40
41 Physiology
42

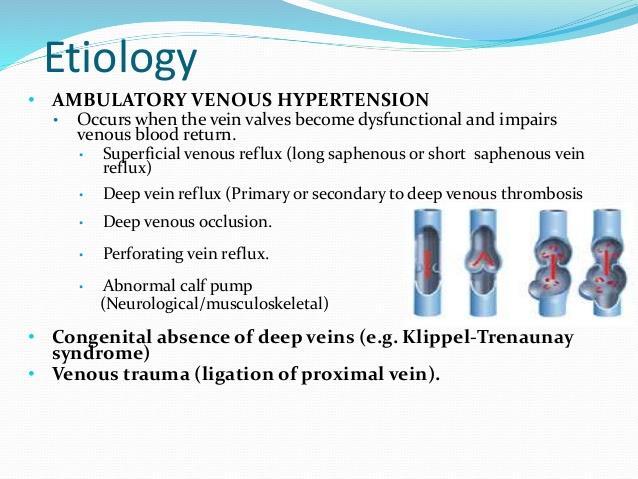
43 Ambulatory Venous Hypertension
44
45
46

47 Venous Valvular Function Valve leaflets allow unidirectional flow, upward or inward Dilation of vein wall prevents opposition of valve leaflets, resulting in reflux Valvular fibrosis, destruction, or agenesis results in reflux
48 A DVT Doppler study is NOT the same as Doppler study for Venous Reflux!

49 Doppler exam: Normal flow Illustration by Linda S. Nye

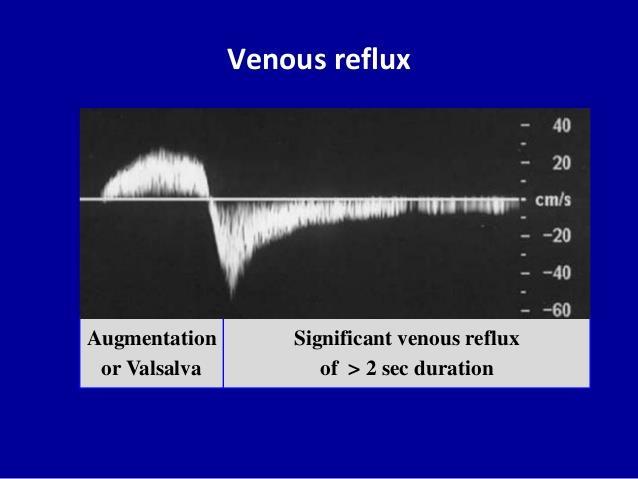
50 Doppler: Reflux Illustration by Linda S. Nye


51 REFLUX: its contribution to varicose veins Illustration by Linda S. Nye
52 Pathophysiology: 2 components REFLUX Dilatation of vein wall leads to valve insufficiency Monocytes may destroy vein valves Retrograde flow results in distal venous hypertension OBSTRUCTION Thrombosis and subsequent fibrosis obstruct venous outflow Damage to vein valves may also cause reflux Both contribute to venous hypertension The presence of both is far worse than either one alone
53 Venous Disease is a Hereditary Disorder 134 families were examined. The risk of developing varicose veins was: 89% if both parents had varicose veins 47% if one parent had varicose veins 20% if neither parent had varicose veins Cornu-Thenard, A, J Dermatol Surg Oncol 1994 May; 20(5):
54 The beginnings of venous disease may be found as early as childhood 740 pts y/o 518 pts y/o 459 pts y/o Diagnosable Vein disease Actual Varicose Veins 2.5% 12.3% 19.8% 0 1.7% 3.3% Phlebologie Nov-Dec;43(4): Weindorf N, Schultz-Ehrenburg U.
55 Inactivity aggravates venous disease 2,854 patients with varicose veins, working in a factory 64.5% had jobs standing in one place 29.2% had jobs requiring prolonged periods of sitting 6.3% had jobs allowing frequent walking during their shift Santler, R Hautarzt 1956; 10:460
56 Each pregnancy worsens the condition 405 women with varicose veins 13% had one pregnancy 30% had two pregnancies 57% had three pregnancies Brand FN, et al The epidemiology of varicose veins: the Framingham Study Am J Prev Med 1988; 4:96-101
57

58
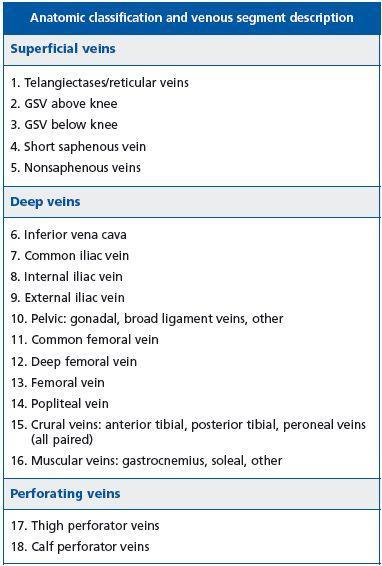
59 CEAP Classification C = Clinical C0 - no visible venous disease C1 - telangiectasias or reticular veins C2 - varicose veins C3 - edema C4 - skin changes without ulceration C4a pigmentation or eczema C4b LDS or atrophie blanche C5 - skin changes with healed ulceration C6 - skin changes with active ulceration E = Etiology (primary vs. secondary) A = Anatomy (defines location of disease within superficial, deep and perforating venous systems) P = Pathophysiology (reflux, obstruction, or both)

60
61 History History of problem: onset, pregnancies, prior DVT, immobilization Associated symptoms and relationship to heat, menses, exercise and compression Current medications Family history Previous treatment and result Goals of patient
62 Physical Examination Examine patient in the standing position, from the groin to the ankle Inspect and palpate for varicose and telangiectatic veins Check the medial and lateral malleolar areas for skin changes suggestive of chronic venous insufficiency (e.g., corona phlebectatica) Inspect the abdomen for enlarged superficial veins if ilio-femoral thrombosis is suspected
:333-6.")
63 Telangiectasias Also known as spider veins due to their appearance Very common, especially in women Increase in frequency with age 85% of patients are symptomatic * May indicate more extensive venous disease * Weiss RA and Weiss MA J Dermatol Surg Oncol Apr;16(4):333-6.

64 Lateral Subdermic Plexus Very common, especially in women Superficial veins with direct perforators to deep system Remnant of embryonic deep venous system

65 Reticular Veins Enlarged, greenish-blue appearing veins Frequently associated with clusters of telangiectasias May be symptomatic, especially in dependent areas of leg

66 Most common finding in patients with varicose veins Varicosities most commonly along the medial thigh and calf but cannot assume location indicates origin At least 20% of patients are at risk of ulceration Varicose Veins Great Saphenous Distribution

67 Great Saphenous Insufficiency Skin changes are seen along the medial aspect of the ankle The presence of skin changes is a predictor of future ulceration * * Kirsner R et al. The Clinical Spectrum of Lipodermato-sclerosis, J Am Acad Derm, April 1993;28(4):623-7

68 Less frequent than Great Saphenous involvement Varicosities may be seen on the posterior calf and lateral ankle Skin changes are seen along the lateral ankle Varicose Veins Small Saphenous Distribution



")
69 Skin changes suggestive of chronic venous insufficiency Corona Phlebectatica (C1) Atrophie blanche (C4b) Pigmentation (C4a) Healed ulcer (C5)
70 Frequently Asked Questions What does my poor circulation have to do with my swelling? We educate our patients on distinguishing between arterial, venous, and lymphatic circulation and go over their particular factors for their swelling verbally and with a diagram. I have stasis eczema what is that I use hydrocortisone on my legs for years why is that? Draw Diagram How I educate patients on their Edema.

71
")
72 CHF (left and/or Right) Kidney disease Liver Disease Lymphedema Lipo edema Hypothyroidism Varicose Veins Exacerbating factors obesity/pulmonary hypertension (too many bags of frito s- True story!!!)
73 Inverted tree Pure Superficial Venous Edema is usually from the knee down If there is edema extends into the thigh and above think additional systemic factors and/or deep venous involvement
74
75 Edema All edema is lymphedema CHF Left and/or Right, cirrhosis, Renal failure = Diuretics + compression Venous insufficiency = compression/ablation/procedure if indicated not diuretics Lymphedema = manual decongestive therapy + compression Not diuretics Don t forget Thyroid Lipo Edema characteristic Cut off sign at ankle Can have all three PhleboLipoLymphedema Be sure to check ABI if compressing Caution if ABI <0.8
76


77
78
79

80
81 Frequently asked questions Aren t Vein Practices just cosmetic and spa centers? No - Phlebology practice encompasses a wide range of Services. As with other practices may deal with Deep system problems (such as May/Thurner syndrome thrombolytic therapy and stenting/coiling vascular malformation) to only superficial disease GSV/SSV/Perforator and or tributary disease to the reticular and telangiectasia OR both. Certainly patients may initially present with the intent of a Cosmetic outcome but the evaluation always begins with a History/Physical AND a Duplex Ultrasound specifically for REFLUX (different protocol for DVT). Surprising Number of patients when carefully questioned about their leg discomfort have Symptoms that can be attributed to Venous Disease.
82 Guidance for the treatment of deep vein thrombosis and pulmonary embolism J Thromb Thrombolysis (2016) 41:32 67 DOI /s Michael B. Streiff1 Giancarlo Agnelli2 Jean M. Connors3 Mark Crowther4 Sabine Eichinger5 Renato Lopes6 Robert D. McBane7 Stephan Moll8 Jack Ansell9 Published online : 16 January 2016 O The Author(s) This article is published with open access at Springerlink.com
83 Who should be screened? Patients with typical symptoms of venous disease with a constellation of symptoms of Big varicosities that are symptomatic or a history of Venous Ulcerations or no skin changes at all could include: Aching Fatigue, heaviness in legs Pain: throbbing, burning, stabbing Cramping Swelling (peripheral edema) Itching Restless legs Numbness Leg ulcerations usually on the lower leg could be medial or lateral with typically acceptable arterial circulation What s their ABI not to miss Arterial disease
84 Evaluation and treatment of Venous Ulcerations We will get into this Summarize Compression mainstay of treatment of venous ulcerations. Eschar Study showed no help of healing with ligation/stripping HOWEVER reoccurrence rate decreased with ligation/stripping with Evidence of Eschar Study Several flaws in methodology (delay of 4-7 weeks before surgery was performed) Society for Vascular Surgery and American venous Forum recommendations Grade 1B compression therapy for healing venous ulcers Grade 1B if patient is candidate for Ablation of symptomatic varicose veins without ulcers over chronic compression Grade 1A ablation of incompetent superficial veins in addition to compression therapy for reduced reoccurrence rates for Venous Ulcerations

85
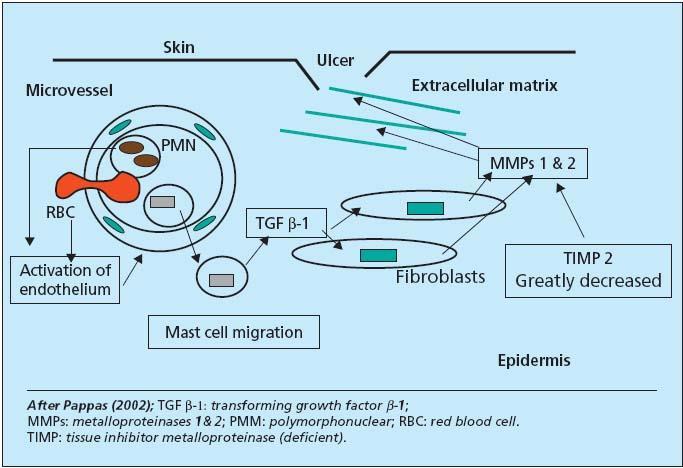
86 Venous Ulceration Over 50% of patients have only superficial venous disease; superficial venous disease may be primary factor in 50-85% of patients * <10% have only deep venous disease Results from ambulatory venous hypertension, which leads to WBC activation, TCpO2, local release of proteolytic enzymes * Shami SK et al. J Vasc Surg 1993; 17:487-90

 Venous")
87 Venous Ulceration Impending ulceration Lipodermatosclerosis (C4a) Venous ulceration (C6)
88 Unique issues Hemorrhage of varicosity Can be scary for the patient Usually story is in the shower and look down and blood just pours Education to get their leg UP and put compression on it not lean over and apply compression (just increasing the hydrostatic pressure to the vein) This is usually an insurance automatic for an intervention especially if recurrent for some type of intervention whether it be ablation, phlebectomy, sclerotherapy or some combination of treatments of course with venous reflux exam to determine the source of reflux. Active or healed venous ulcerations usually an insurance automatic for intervention must have an outlined plan for compression however before I will treat an active ulceration Recurrent Phlebitis this will typically accelerate authorization
89 Who should be screened? Patients with typical symptoms of venous disease with a constellation of symptoms of Big varicosities that are symptomatic or a history of Venous Ulcerations symptoms could include: Aching Fatigue, heaviness in legs Pain: throbbing, burning, stabbing Cramping Swelling (peripheral edema) Itching Restless legs Numbness Leg ulcerations usually on the lower leg could be medial or lateral with typically acceptable arterial circulation What s their ABI not to miss Arterial disease
90 Do I have to wear Compression stockings? Compression stockings are a very important part of treating chronic venous disease Depending on where the patient is on the spectrum of their particular disease process they may be recommended to always wear their compression hose(especially if Deep Reflux) or they may not need to wear their hose after their treatment if ALL reflux has been treated and no further symptoms. HOWEVER All insurance Carriers start with a period of conservative treatment which includes Compression hose NOT TED hose typically 20-30mmHg compression VENOUS DISEASE IS A CONDITION OF CHRONICITY AND MUST BE FOLLOWED NEW AREAS OF REFLUX WILL LIKELY DEVELOP IN THE FUTURE AND MAY BE DEALT WITH EXPECTANTLY to not notify a patient of this would disappoint the patient.
91 CONSERVATIVE TREATMENT OF VENOUS DISORDERS

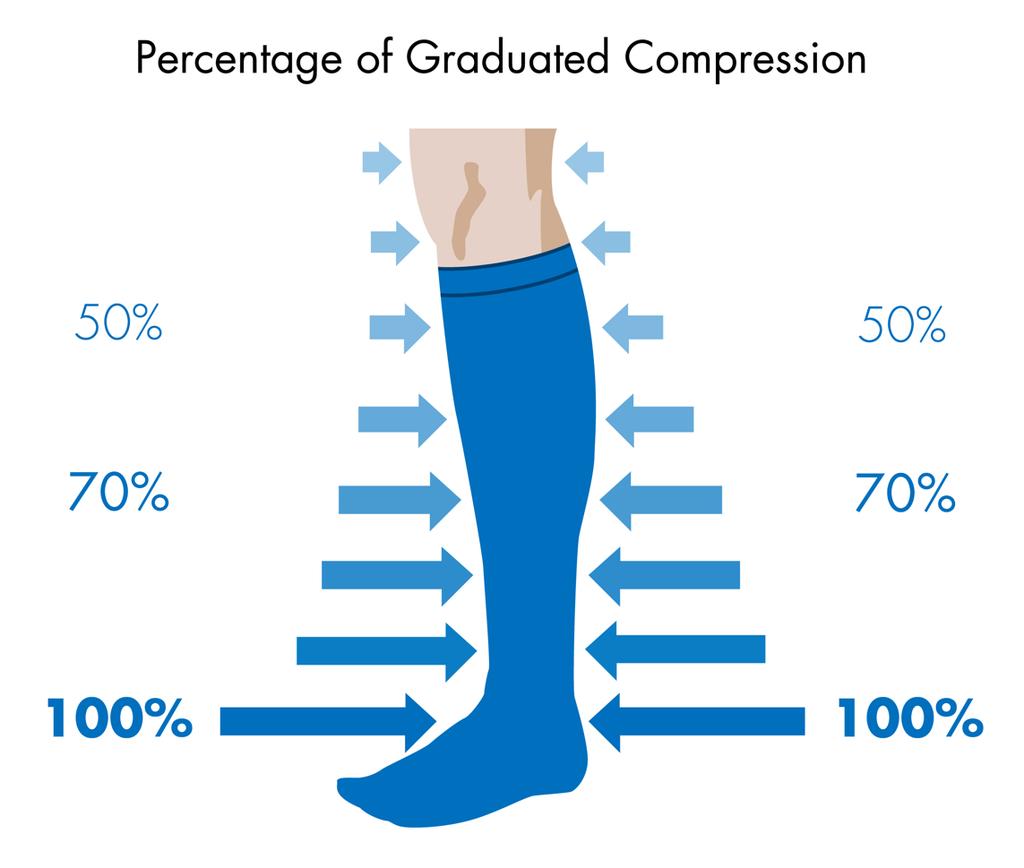
92 Compression Therapy Provides a gradient of pressure, highest at the ankle, decreasing as it moves up the leg Reduces reflux of blood Improves venous outflow Increases velocity of blood flow to reduce the risk of blood clots Photo courtesy of Juzo
93 Compression Therapy Reduces symptoms of aching, fatigue, pain, and swelling Increases fibrinolytic activity Increases TCpO2 Mainstay of treatment for venous ulcers NOTE: Graduated compression therapy and wound care will heal venous stasis ulcers. Elimination of the reflux will reduce the recurrence. Note Tubigrip is variable in patients with ulcerations depending on their anatomy and ankle pressure

94 Elastic compression stockings Must be graduated Calf high generally sufficient Replace q 6 months to assure proper pressure Available in a variety of strengths, styles, colors, and fabrics


95

96 Graduated compression is not the same as T.E.D. hose T.E.D.s are meant for nonambulatory, supine patients T.E.D.s are indicated to decrease the incidence of thrombosis T.E.D.s do not provide sufficient pressure for ambulatory patients
97 Compression Strength 8-15mm Indications Leg fatigue, mild swelling, stylish 15-20mm Mild aching, swelling, stylish 20-30mm Aching, pain, swelling, mild varicose veins 30-40mm * Aching, pain, swelling, varicose veins, post-ulcer 40-50, 50-60mm * Recurrent ulceration, lymphedema * Requires a prescription
98 Gradient compression hose At least Calf high 20-30mmhg Thigh high or panty hose may be more comfortable depending on the situation Open or closed toe depending on concurrent condition such as diabetes, neuropathy or concurrent arterial disease. The clock starts ticking when they began their compression so If you document it I can use that date for their insurance approval. Where can they get them? DME store LKM, Freeland Brown, Fidelity Lymphedema, can purchase over the counter ( typically sized by the calf and thigh circumference and outseam) Yes some fit better than others but if symptoms helped and continue despite their stockings and reflux found good chance they will respond to treatment.
99 If they have an Ulcer This is a good patient to send to both the wound center AND Tulsa Vein as the wound centers are great at getting them in compression, evaluating the wound for proper dressings/home health, debridement, biopsy, and education. Waiting on complete healing before a referral for ablation need not occur as this may just delay getting the patient the needed treatment - even if heals will likely need referral to keep it closed. We can work on the Cause of the Ulceration REFLUX -and try to get the ulcer healed faster and maintain skin integrity with intervention such as endovenous ablation and foam sclerotherapy or other techniques. Likely their Ultrasound will prognosticate if they have single, double or triple component disease meaning superficial or Deep or perforator disease or all three.
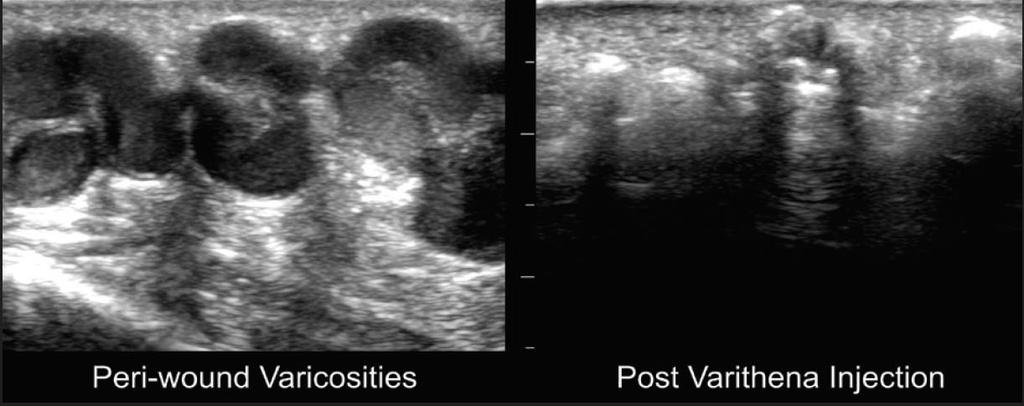
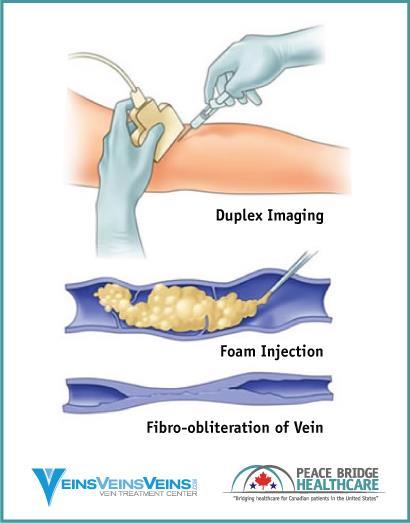
100 Endothermal and Non thermal Ablation Venefit Procedure Endothermal Radiofrequency Ablation Coviden/Medtronic Endothermal Laser Ablation Mechanical Occlusion Chemical Assisted ablation (Clarivein) Venaseal (cyanoacrolate) Varithena Microchemical Foam ablation Steam ablation (Europe) Foam ablation (polidocanol or sotradecol) Stripping Local Microphlebectomy
101
102



103
104 Things I did not talk about due to time- not that they are unimportant Type of compression bandaging - Inelastic vs elastic ie unna boot vs multilayer compression both work Types of dressings follow best wound care protocols Types of Cellular tissue products I ve used most all and have spoken on most - some have advantages over others but wont work at all if poor wound bed preparation Again thank you Osiris Therapeutics for sponsoring this lecture with a grant. Lymphedema treatment as a component of venous ulcer healing Lymphedema pumps and ambulatory lymphedema pump -Acti-touch Medications for Venous disease trental for venous ulcers and other meds such as horse chestnut,pycnogenol,ketoprophen,resveratrol,tumeric,vasculera, diosmen complex etc. Ambulatory Venous Hypertension MUST be addressed to have optimal outcome and sustained healing
105 Guidance for the treatment of deep vein thrombosisand pulmonary embolism J Thromb Thrombolysis (2016) 41:32 67 Summary Guidelines
106 Contraindications to outpatient treatment of venous thromboembolism Active or high risk of bleeding Recent surgery (within 7 days) Cardiopulmonary instability Severe symptomatic venous obstruction High risk pulmonary embolism* Thrombocytopenia (platelets<50,000/ll) Other medical or surgical condition requiring inpatient management Medical non-compliance Geographical or telephone inaccessibility Poor hepatic function (International Normalized Ratio (INR)C1.5)Unstable renal function (e.g. rising serum creatinine) Poor home health care support environment * High risk PE is characterized by systolic blood pressure< 90 mmhg or a systolic blood pressure drop ofc40 mmhg for>15 min not due to an arrhythmia, hypovolemia or sepsis
107 Wells clinical DVT model Clinical characteristic Active cancer (patient receiving treatment for cancer within 6 months or currently receiving palliative 1 treatment) Paralysis, paresis, or recent plaster cast immobilization of the lower extremities 1 Recently bedridden for 3 days or more, or major surgery within the previous 12 weeks requiring general or regional anesthesia 1 Localized tenderness along the distribution of the deep venous system 1 Entire leg swollen 1 Calf swelling at least 3 cm larger than the asymptomatic side (measured 10 cm below the tibial tuberosity 1 Pitting edema confined to the symptomatic leg 1 Collateral superficial veins (non-varicose) 1 Previously documented deep vein thrombosis 1 Alternative diagnosis at least as likely as deep vein thrombosis -2 Score A score of 0 indicates that a low pretest probability of deep vein thrombosis. A score of 1 or 2 points indicates a moderate risk of DVT and a score of 3 or higher indicates a high risk of deep vein thrombosis [152]
108 Wells clinical pulmonary embolism model Clinical characteristic Score Active cancer (patient receiving treatment for cancer within 6 months or currently receiving palliative treatment) 1 Surgery or bedridden for 3 days or more during the past 4 weeks 1.5 History of deep venous thrombosis or pulmonary embolism 1.5 Hemoptysis 1Heart rate[100 beats/min 1.5 Pulmonary embolism judged to be the most likely diagnosis 3 Clinical signs and symptoms compatible with deep venous thrombosis 3 A score of<2 indicates a low probability of pulmonary embolism. A score of 2 6 indicates an intermediate probability of PE. A score of more than 6 indicates a high probability of pulmonary embolism. Kearon C, Ginsberg JS, Douketis J, et al. (2006) An evaluation of D-dimer in thediagnosis of pulmonary embolism: a randomized trial. Ann Intern Med Jun 6; 144(11):812-21
109 Simplified PESI (pulmonary embolism severity index) score Predictors Age >80 years 1 History of cancer 1 History of heart failure 1 Pulse>110 beats/min 1 Systolic blood pressure<100 mmhg 1 Arterial oxygen saturation<90 % 1 Low risk=total point score 0 Management of outpatients vs Inpatients
110 How is the diagnosis of deep vein thrombosis and pulmonary embolism established? We suggest the use of validated pre -test probability models in conjunction with D dimer testing and selective use of objective diagnostic imaging to increase the cost-efficiency and accuracy of VTE diagnosis
111 Which patients require hospitalization versus initial outpatient therapy for the management of VTE? We suggest that most patients with DVT and many patients with PE can be managed as outpatients. PE patients should be risk stratified to determine appropriate management. A variety of laboratory tests and imaging modalities a swell as clinical risk prediction models are available to identify PE patients who are suitable for outpatient management. Further research is needed to identify the optimal approach to risk stratification of PE patients
112 What are the therapeutic options for the acute treatment of venous thromboembolism? With the variety of treatment options available, we recommend that the acute therapy of VTE should be customized to suit the unique clinical circumstances of the individual patient. We suggest that unfractionated heparin may be preferable for inpatients with planned invasive procedures, recent major bleeding episode s or impaired renal function as well as underweight and morbidly obese patients although several members of panel felt there were insufficient data to support this suggestion. LMWHs are convenient options for inpatient and outpatient therapy. DOACs are optimized for outpatient therapy of VTE We suggest that systemic and catheter-directed pharmacomechanical thrombolytic therapy are effective options for treatment of acute extensive proximal DVT and massive PE that can rapidly reduce thrombus burden. Given the greater risks of bleeding associated with these approaches, we recommend that a careful assessment of the risks and benefits of therapy should be performed in each patient prior to the initiation of thrombolytic therapy
113 Which patients are candidates for a DOAC? Dabigatran When used after a 5 10 day initial course of parenteral anticoagulation, dabigatran is as effective as warfarin in the acute and short term treatment of VTE. We suggest dabigatran as an alternative to vitamin K antagonists for the short term therapy of VTE. In some studies, dabigatran has been associated with an increased risk of acute coronary syndrome and gastrointestinal bleeding compared with vitamin K antogonists Rivaroxaban Rivaroxaban is as effective as LMWH/VKA in the treatment of DVT and PE. We suggest rivaroxaban as an alternative to LMWH/VKA for the acute and short term treatment of VTE in appropriate patients. No increase in acute coronary syndrome or gastrointest inal bleeding has been seen with rivaroxaban, however GI bleeding may be more common in patients age 75 and older Apixaban Apixaban is as effective as LMWH/VKA in the treatment of DVT and PE and associated with less major bleeding and major or clinically relevant non-major bleeding. We suggest apixaban as an alternative to LMWH/VKA in the acute andshort term treatment of VTE in appropriately selected patients. No increase in acute coronary syndrome or gastrointestinal bleeding has been seen with apixaban Edoxaban After an initial 5 10 days of LMWH or UFH, edoxaban is as effective as LMWH/VKA in the treatment of acute DVT and PE but associated with less major or clinically relevant non-major bleeding. We suggest edoxaban as an alternative to VKA for the shortterm treatment of VTE in appropriately selected candidates
114 What is the role of vena cava filters if the patient is not a candidate for anticoagulation? We suggest that vena cava filters should be considered in any patient with acute VTE (within 4 weeks) who cannot be treated with anticoagulation. We suggest that retrievable filters are strongly preferred as most patients have only temporary contraindications to anticoagulation. Filters should be retrieved once anticoagulation can be reinitiated preferably within 6 months of placement. Patients with filters should be closely monitored in a structured program to facilitate retrieval and minimize the number of patients lost to follow up Following anticoagulation-associated gastrointestinal bleeding, we suggest that anticoagulation can be re-initiated as early as 7 days after cessation of bleeding and treatment of causal lesions. Following anticoagulation associated ICH, we suggest resumption of anticoagulation no sooner than 10 weeks post-bleed. Further investigation of this topic is warranted
115 How is upper extremity VTE treated? Identification and elimination of trigger factors when feasible is important to reduce the incidence of recurrent upper extremity DVT. For CVC-associated DVT, we suggest that anticoagulation without CVC removal is the treatment of choice. If symptoms fail to resolve, CVC removal can be considered. We suggest that anticoagulation should be continued for at least 3 months or the duration ofthe CVC whichever is longer. At least 3 months of anticoagulation is appropriate for pacemaker wire-associated VTE The committee was divided as to the optimal approach to treatment of TOS/PSSassociated upper extremity DVT. The benefits of rib resection/scalenectomy following thrombolysis and anticoagulation remain to be rigorously demonstrated. Therefore, providers should consider therapy for TOS/PSS on a case-by-case basis until higher quality data are available. We suggest that TOS/PSS-associated upper extremity DVT warrants anticoagulation for at least 3 months. Treatment of upper extremity DVT associated with extrinsic compression due to cancer or infection should include treatment of the underlying disease in addition to anticoagulation
116 When is ambulation/exercise safe after DVT/PE? We suggest that ambulation is safe in patients with acute DVT±PE after initiation of anticoagulation
117 Is the use of graduated compression stockings safe after acute DVT/PE? We suggest that GCS do not increase the risk of recurrent thromboembolism inpatients with acute VTE. We suggest that GCS do not have any beneficial effect on leg discomfort associated with acute DVT
118 What is the recommended duration of therapy for a patient with distal DVT? We suggest treatment of distal DVT with anticoagulation versus observation. We suggest a duration of therapy of 3 months. In patients with contraindications to anticoagulation, we favour repeat duplex surveillance in 1 week rather than vena cava filter insertion
119 What is the recommended duration of therapy for a patient with a surgically provoked VTE? We suggest that 3 months of anticoagulation is adequate for surgical risk factor-associated VTE unless risk factors for recurrence persist
120 What is the recommended duration of therapy for a pregnancy or estrogen-associated VTE? We suggest that patients with pregnancy-associated VTE should be treated for the duration of the pregnancy and the post-partum period (up to 12 weeks postpartum) or as long as dictated by the VTE, whichever is longer. Patients with pregnancy-associated VTE are at high risk for recurrent VTE with subsequent pregnancies, therefore we suggest that thromboprophylaxis for the duration of the pregnancy and post-partum period should be strongly considered Patients with hormone-associated VTE appear to be at lower risk for recurrent VTE particularly if their D dimer is negative at the end of therapy and 1 month after discontinuing anticoagulation. Therefore, we suggest that long term anticoagulation beyond 3 6 months may not be associated with a favorable risk:benefit balance if hormonal therapy has been discontinued. If hormonal therapy is medically necessary, we suggest that anticoagulation should be continued as these patients are at high risk for recurrent VTE
121 What is the recommended duration of therapy for a medical illness-associated VTE? We suggest that patients with medical-illness associated VTE should be treated for at least 3 months or as long as the medical risk factors for VTE remain present
122 What is the recommended duration of therapy for a travel-associated VTE? Travel ([ 4 h duration) is a modest and transient risk factor for VTE. Therefore, VTE should only be ascribed to air travel if it presents within 4 weeks of travel and is not associated with other concomitant triggers. In the absence of other precipitants, we suggest that travelassociated VTE should be treated for at least3 months. We suggest that travel thromboprophylaxis be considered for future travel in these patients
123 What is the recommended duration of therapy for a malignancy-associated VTE? Active cancer is a potent risk factor for VTE that varies with the type and extent of cancer and its treatment. Therefore, we suggest anticoagulation be continued as long as the underlying cancer is active or under treatment
124 What is the recommended duration of therapy for a patient with unprovoked VTE? Patients with unprovoked VTE are at high risk for recurrence so we suggest long term anticoagulation. As there is limited information on the risks and benefits of anticoagulation beyond 2 years, we suggest that providers reassess patients on long term anticoagulation on an annual basis
125 What are the therapeutic options for long term treatment of DVT/PE? Vitamin K antagonists Adjusted dose vitamin K antagonists (INR 2 3) reduce the relative risk of recurrent VTE by 88 %, but they are associated with 2.6 fold increase in major bleeding compared with placebo. Consequently, it is important to assess the risksand benefits of long term anticoagulation on a case-by-case basis. Since lowintensity (INR 1.5 2) anticoagulation is associated with a similar risk of major bleeding, we prefer standard intensity anticoagulation for long term therapy o VTE LMWH/Fondaparinux Evidence indicates that LMWH is as effective as VKA in the reduction of recurrent VTE but associated with a reduced risk of m ajor bleeding. Limited experience with fondaparinux in the long term treatment of VTE suggests that itis as effective as LMWH in the prevention of recurrent VTE. Fondaparinux may cause more bleeding than VKA in patients without cancer. We suggest that LMWH and fondaparinux are acceptable alternatives to VKA for treatment ofvte Direct Oral Anticoagulants Dabigatran In long term therapy of VTE, dabigatran was as effective as warfarin and superior to placebo in prevention of recurrent thromboembolism. There was a trend toward reduced major bleeding with dabigatran compared with warfarin but major bleeding was 3-fold higher with dabigatran than placebo. We suggest tha t these data establish dabigatran as a viable option to vitamin K antagonists for long term therapy of VTE Rivaroxaban In long term treatment of VTE (after 3 6 months of therapy), rivaroxaban wa smore effective than placebo but associated with 5 fold increase in major o rclinically relevant nonmajor bleeding. We suggest that these data support the use of rivaroxaban in the long term treatment of VTE in candidates sui table for anticoagulation Apixaban In long term treatment of VTE (after 6 months of therapy), apixaban was more effective than placebo and associated with a similar risk of major or clinically relevant non-major bleeding. We suggest that these data support the use ofapixaban for the long term treatment of VTE in patients who are appropriate candidates. The option of a reduced dose for long term secondary prevention maybe attractive for some patients Aspirin After an initial 6 18 months of anticoagulation, aspirin 100 mg daily was associated with a 34 % reduction in the relative risk of recurrent VTE (from 7.5to 5.1 %) compared with placebo. Major bleeding was similar in both groups. Therefore, we suggest that aspirin should be considered an option for patients atrisk for recurrent VTE who are not considered appropriate candidates for longt erm anticoagulation or who chose to discontinue anticoagulation
126 What is the best treatment of patients who have recurrent VTE in spite of anticoagulation? In patients with recurrent VTE despite anticoagulation, we suggest that it is important for providers to assess adherence to therapy and identify clinical conditions associated with anticoagulation failure including cancer, antiphospholipid syndrome, heparin-induced thrombocytopenia and vascular compression syndromes (May- Thurner syndrome, thoracic outlet syndrome). We suggest that higher-intensity anticoagulation (VKA INR or 3 4 or based upon chromogenic factor X activity or escalated dose [125 % dose] LMWH),alternative forms of parenteral anticoagulation and therapies directed at restoring adequate blood flow are effective strategies to consider
127 How can you assess the risk of recurrent VTE and anticoagulant-associated bleeding? We suggest that patients with unprovoked VTE should be considered intrinsically thrombophilic and long term anticoagulation should be considered. When assessing the risk of recurrent VTE in patients with provoked VTE, it is important to determine whether provoking factors persist. If such factors are still present, we suggest that continued anticoagulation should be considered if bleeding risk is not excessive We suggest that D dimer testing represents a promising global measure of pro-thrombotic potential that can be used to risk stratify patients for their future risk of VTE. However, we believe it is important to recognize that different D dimer assays may have different performance characteristics in regards to VTE risk assessment. In addition, the impact of age on the D dimer results and VTE risk prediction remains incompletely characterized. The value of other global laboratory measures (endogenous thrombin potential) and imaging studies remains to be established. Multimodality risk assessment models appear to be effective approach to risk stratification of patients with unprovoked VTE. Further validation of these risk assessment tools is underway Anticoagulation-associated bleeding While a bleeding risk assessment is important to the decision on the duration of anticoagulation, we suggest that it is premature to use formal bleeding risk assessment models to identify patients who should discontinue anticoagulation. Development of better risk prediction models remains a priority
128 Thank You! It is always an Honor to be invited to speak to colleagues in medicine!
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
lipodermatosclerosis standards of medical practitioners and the quality of patient care related to the treatment of venous disorders.
 Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
PHLEBOLOGY. Venous Insufficiency. Presentation Use Information
 Disclosure of Conflict of Interest THE BASICS OF VENOUS INSUFFICIENCY: What You Should Know. An Introductory Lecture Donald Ives, MD, RVT, RPVI Board Certified Family Physician Diplomate of the American
Disclosure of Conflict of Interest THE BASICS OF VENOUS INSUFFICIENCY: What You Should Know. An Introductory Lecture Donald Ives, MD, RVT, RPVI Board Certified Family Physician Diplomate of the American
Phlebology for the Internist not a vain effort
 Phlebology for the Internist not a vain effort G. Davin Haraway DO,FACOI,FACCWS,RPhS Tulsa Vein Institute We are talking about veins but don t ever forget to check the arterial status 1 st thing! 1 The
Phlebology for the Internist not a vain effort G. Davin Haraway DO,FACOI,FACCWS,RPhS Tulsa Vein Institute We are talking about veins but don t ever forget to check the arterial status 1 st thing! 1 The
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Additional Information S-55
 Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
AMERICAN PODIATRIC MEDICAL ASSOCIATION
 AMERICAN PODIATRIC MEDICAL ASSOCIATION THE NATIONAL ANNUAL SCIENTIFIC MEETING Friday, July 13 th 2018 Washington, D.C. CHRONIC VENOUS INSUFFICIENCY OF THE LOWER EXTREMITIES Clinical Pearls for the Podiatrist
AMERICAN PODIATRIC MEDICAL ASSOCIATION THE NATIONAL ANNUAL SCIENTIFIC MEETING Friday, July 13 th 2018 Washington, D.C. CHRONIC VENOUS INSUFFICIENCY OF THE LOWER EXTREMITIES Clinical Pearls for the Podiatrist
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency
 The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency Thomas E. Eidson, DO Certified Venous Disease Specialist Board Certified Family Medicine Disclosure of Conflict of
The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency Thomas E. Eidson, DO Certified Venous Disease Specialist Board Certified Family Medicine Disclosure of Conflict of
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Chronic Venous Insufficiency
 Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
OHTAC Recommendation. Endovascular Laser Treatment for Varicose Veins. Presented to the Ontario Health Technology Advisory Committee in November 2009
 OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
Patient Information. Venous Insufficiency and Varicose Veins
 Patient Information Venous Insufficiency and Varicose Veins What is a Varicose Vein? Gitter Vein Institute-revised 3/8/2016 2 Frequently Asked Questions What is the difference between varicose and spider
Patient Information Venous Insufficiency and Varicose Veins What is a Varicose Vein? Gitter Vein Institute-revised 3/8/2016 2 Frequently Asked Questions What is the difference between varicose and spider
Medicare C/D Medical Coverage Policy
 Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
How varicose veins occur
 Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Determine the patients relative risk of thrombosis. Be confident that you have had a meaningful discussion with the patient.
 Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
UNDERSTANDING VEIN PROBLEMS
 UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat?
 Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Dr Paul Thibault. Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology
 Australasian College of Phlebology") Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
Current Management of Varicose Veins
 Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona
 Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona March 8, 2011 Varicose Vi Vein Market Approximately 40% of the US population has venous disease;
Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona March 8, 2011 Varicose Vi Vein Market Approximately 40% of the US population has venous disease;
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range
 Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range") Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.066.MH Last Review Date: 11/08/2018 Effective Date: 01/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
Prevalence. Definition. Chronic Venous Insufficiency. Overview of Chronic Venous Insufficiency
 Overview of Chronic Venous Insufficiency Steven M. Dean, DO, FACP, RPVI Vascular Medicine Specialist Assistant Professor of Internal Medicine Department of Cardiovascular Medicine The Ohio State University
Overview of Chronic Venous Insufficiency Steven M. Dean, DO, FACP, RPVI Vascular Medicine Specialist Assistant Professor of Internal Medicine Department of Cardiovascular Medicine The Ohio State University
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
UNDERSTANDING VEIN DISEASE. UC EN - For use in the U.S. only
 UNDERSTANDING VEIN DISEASE UC201706537 EN - For use in the U.S. only Do you need to sit down during your work day because your legs ache and/or swell? Do you miss out on doing the activities you love because
UNDERSTANDING VEIN DISEASE UC201706537 EN - For use in the U.S. only Do you need to sit down during your work day because your legs ache and/or swell? Do you miss out on doing the activities you love because
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Love your legs again Varicose Veins
 Love your legs again Varicose Veins Veins are the vessels that return blood to the heart once it has circulated through the body (as opposed to arteries, which carry oxygen-rich blood from the heart to
Love your legs again Varicose Veins Veins are the vessels that return blood to the heart once it has circulated through the body (as opposed to arteries, which carry oxygen-rich blood from the heart to
Vein Disease Treatment
 MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
Varicose Vein Cyanoacrylate Glue treatment
 The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
Management of Post-Thrombotic Syndrome
 Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Varicose Vein Information Sheet
 Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
Deep Vein Thrombosis
 Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Selection and work up for the right patients suspected of deep venous disease
 Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Patient assessment and strategy making for endovenous treatment
 Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY
 RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Dr Peter Chapman-Smith
 Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Endovenous Radiofrequency and Laser Ablation
 Endovenous Radiofrequency and Laser Ablation [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr go to Comunicados a Proveedores, and click Cartas Circulares.]
Endovenous Radiofrequency and Laser Ablation [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr go to Comunicados a Proveedores, and click Cartas Circulares.]
Epidemiology: Prevalence
 Epidemiology: Prevalence More than 30 million Americans suffer from varicose veins or a more serious form of venous disease called Chronic Venous Insufficiency (CVI). 1 Of the over 30 million Americans
Epidemiology: Prevalence More than 30 million Americans suffer from varicose veins or a more serious form of venous disease called Chronic Venous Insufficiency (CVI). 1 Of the over 30 million Americans
Endo-Thermal Heat Induced Thrombosis (E-HIT)
") Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
A A U
 PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
Rapid Fire-Top Articles You Need to Know
 Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Rapid Fire-Top Articles You Need to Know TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Suspected Deep Vein Thrombosis (DVT) Assessment
 Assessment") CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
New Guideline in venous ulcer treatment: dressing, medication, intervention
 New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL
 PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
Deep Venous Pathology. Eberhard Rabe Department of Dermatology University of Bonn Germany
 Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Alberta Health. Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual
 Alberta Health Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual March 7, 2016 Revision History Description Date N-03, N 05 and N-07:
Alberta Health Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual March 7, 2016 Revision History Description Date N-03, N 05 and N-07:
Varithena 3 rd February 2015
 Varithena 3 rd February 2015 Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other forward-looking statements with respect to
Varithena 3 rd February 2015 Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other forward-looking statements with respect to
Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments
 1 Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments What are spider veins? Spider veins are dilated, small blood vessels that have a red or bluish color. They appear
1 Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments What are spider veins? Spider veins are dilated, small blood vessels that have a red or bluish color. They appear
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Conflict of Interest. None
 Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Varicose Vein Surgery
 What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.
 to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.") How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES
 DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment.
 Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment. Approximately 1 in 5 adult Americans suffer from superficial
Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment. Approximately 1 in 5 adult Americans suffer from superficial
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Occasional pain or other discomfort (ie, not restricting regular daily activity)
") Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Recurrent Varicose Veins We All See Them
 We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
A treatment option for varicose veins. enefit" Targeted Endovenous Therapy. Formerly known as the VNUS Closure procedure E 3 COVIDIEN
 A treatment option for varicose veins. enefit" Targeted Endovenous Therapy Formerly known as the VNUS Closure procedure E 3 COVIDIEN THE VENOUS SYSTEM ANATOMY The venous system is made up of a network
A treatment option for varicose veins. enefit" Targeted Endovenous Therapy Formerly known as the VNUS Closure procedure E 3 COVIDIEN THE VENOUS SYSTEM ANATOMY The venous system is made up of a network
Endovenous Laser Therapy INFORMATION & TREATMENT INSTRUCTIONS
 1324 Princess Street Kingston, ON K7M 3E2 Website: www.ucosmetic.com Email: nuyu@ucosmetic.com Phone: (613) 536-LASR (5277) Fax: (613) 536-5108 Dr. Kim Meathrel, MD, FRCSC, Plastic Surgeon, Associate Professor
1324 Princess Street Kingston, ON K7M 3E2 Website: www.ucosmetic.com Email: nuyu@ucosmetic.com Phone: (613) 536-LASR (5277) Fax: (613) 536-5108 Dr. Kim Meathrel, MD, FRCSC, Plastic Surgeon, Associate Professor
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
All you need to know about. Varicose Veins. & its treatments. in 10 mins
 All you need to know about Varicose Veins & its treatments in 10 mins Contents Symptoms and Causes...04 Risk Factors...05 Relief: The Top Five Tips...06 Compression Stockings or Bandages...08 New Surgery
All you need to know about Varicose Veins & its treatments in 10 mins Contents Symptoms and Causes...04 Risk Factors...05 Relief: The Top Five Tips...06 Compression Stockings or Bandages...08 New Surgery
Superficial Thrombophlebitis Treatment Guideline Review
 Superficial Thrombophlebitis Treatment Guideline Review Suman M. Wasan, MD, MS Regents Professor Director, Vascular Medicine College of Medicine University of Oklahoma Health Sciences Center Disclosure
Superficial Thrombophlebitis Treatment Guideline Review Suman M. Wasan, MD, MS Regents Professor Director, Vascular Medicine College of Medicine University of Oklahoma Health Sciences Center Disclosure
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015
 Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
Venous interventions in DVT
 Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Venous interventions in DVT Sriram Narayanan Chief of Vascular and Endovascular Surgery, Tan Tock Seng Hospital A/Prof of Surgery, National University of Singapore ANTI-COAGULATION LMWH Warfarin x 6m Acute
Current issues in the management of Superficial Vein Thrombosis - SVT
 Current issues in the management of Superficial Vein Thrombosis - SVT Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health Sciences,
Current issues in the management of Superficial Vein Thrombosis - SVT Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health Sciences,
High Level Overview: Venous Anatomy of Lower Extremities. Anatomy of a Vein 5/11/2015. Barbara Deusterman, RN
 High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention
 TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention") A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
A VENOUS THROMBOEMBOLISM (VTE) TOWN HALL: Answering Your Top Questions on Treatment and Secondary Prevention This handout is a supplemental resource to an educational video activity released on Medscape
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Discussion Leader: Doug Bias, M.D.
 In low-risk patients with isolated calf DVT (IDDVT), what is the morbidity risk of treating with repeat ultrasound/observation versus anticoagulation? Discussion Leader: Doug Bias, M.D. Clinical Scenario:
In low-risk patients with isolated calf DVT (IDDVT), what is the morbidity risk of treating with repeat ultrasound/observation versus anticoagulation? Discussion Leader: Doug Bias, M.D. Clinical Scenario:
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.015.MH Last Review Date: 11/08/2018 Effective Date: 02/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Compression Garments and
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Compression Garments and
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
PATIENT EDUCATION HANDBOOK
 PATIENT EDUCATION HANDBOOK Welcome from Our Founder and CEO 1 What is Venous Insufficiency 2 What Factors Can Cause Varicose Veins? 2 Our Procedures 3 Pre- and Post-Operative Instructions 4 Sclerotherapy
PATIENT EDUCATION HANDBOOK Welcome from Our Founder and CEO 1 What is Venous Insufficiency 2 What Factors Can Cause Varicose Veins? 2 Our Procedures 3 Pre- and Post-Operative Instructions 4 Sclerotherapy
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies