Phlebology for the Internist not a vain effort
|
|
|
- Iris McBride
- 5 years ago
- Views:
Transcription

1 Phlebology for the Internist not a vain effort G. Davin Haraway DO,FACOI,FACCWS,RPhS Tulsa Vein Institute We are talking about veins but don t ever forget to check the arterial status 1 st thing! 1


2 The acute leg swelling and Painful Leg IF DVT on your mind think Wells score Send to the ER as this can be a life and/or limb threatening condition also If DVT is not found they may have another condition that may need emergent treatment i.e. acute cellulitis or Necrotizing fasciitis or Arterial occlusion I would recommend that you send them with an order for D-Dimer if referring them to the ER - most will draw but some do not. If they have Superficial thrombophlebitis they could have up to a 40% chance of having a concurrent DVT in the same OR THE OTHER LEG so get bilateral studies not just the symptomatic leg so same recommendation of ER. This could look like Cellulitis but typically along the course of a vein. Treatment of superficial thrombophlebitis typically would consist of NSAIDS and Compression hose at least 20-30mmhg (yes tender to get on but will typically provide relief rapidly) these patients typically have disease that will need treatment a vein center (and may not be their 1 st episode) This does not require antibiotics (unless substance was injected) A subset of Superficial thrombophlebitis may be best treated with anticoagulation if extensive (involves the SFJ), hypercoaguable state, or history of active cancer Stasis Eczema(dermatitis) Is typically a manifestation of advanced venous Disease and can be helped greatly by treatment of the underlying REFLUX Steroid creams mask the underlying real problem Hypercoaguable state factor V leiden,prothrombin G2021A,antithrombin III deficiency, Protein C and S deficiency, Lupus anticoagulant, Anticardiolipin syndrome, elevated Factor VIII levels Screening for this is not typically recommended with 1 st DVT IF it can be explained and no family history or recurrent fetal loss. Phlebology What s that about? Davin Haraway DO,FACOI,FACCWS,RPhS 2
3 Prevalence of Chronic Venous Disease 1 in 22 or 4.5% or 12.2 million people in the USA are affected by varicose veins Incidence increases with age and is more common in women with over 40% of women in their 50 s suffering from some sort of venous disorder Across all ages and gender, 60% of Americans suffer from venous disease and its sequelae National Heart Lung and Blood Institute (NHLBI) Population Tulsa County 603,403 Age ,512 Female 51% 73,191 Male 50% 71,756 Age % prevalence 23,106 Age % prevalence 16,833 Age % prevalence 13,260 Age % prevalence 7,096 50% pathologic reflux 11,553 50% pathologic reflux 8,416 50% pathologic reflux 6,630 50% pathologic reflux 3, % GSV reflux 1,964-5, % GSV reflux 1,430-3, % GSV reflux 1,127-3, % GSV reflux 603-1,632 Total patients that would potentially just need GSV treatment by endothermal ablation range from 5,124 to 13,866 if symptomatic. A portion of these patients will need Phlebectomy and /or Ultrasound guided sclerotherapy in addition to endothermal ablation all of which are reimbursable procedures by most Insurance carriers when symptomatic. This assumes that all patients were healthy on a population basis. Age years total 143,512 from Tulsa City Statistics 77% of this age group are years old and 23% age55 64 years old. 3
4 65 and older 50,508 Female 72% prevalence 31,007 x 0.72= 22,325 Male 43% prevalence 19,501 x 0.43 = 8, % GSV reflux 3,795-10, % GSV reflux 1, Medicare age patients with potential GSV reflux could be treated with endothermal ablation if symptomatic would range from 5,220 to 14,126. Medicare has coverage criteria for symptomatic patients. Patients from age group 35 to over 65 total 10,344 27,922 in the Tulsa County The Spectrum of Chronic Venous Disease telangiectasias superficial phlebitis varicose veins lipodermatosclerosis venous ulceration 4
5 Who should be screened? Patients with typical symptoms of venous disease with a constellation of symptoms and/or signs of: varicosities that are symptomatic; or a history of Venous Ulcerations; or no skin changes at all and symptoms could include: Aching Heaviness (#1complaint) or fatigue in legs usually better with ambulation (different from claudication) Pain: throbbing, burning, stabbing Cramping Swelling (peripheral edema) Itching Restless legs Numbness Leg ulcerations usually on the lower leg could be medial or lateral ( with acceptable arterial circulation) What s their ABI not to miss Arterial disease! THE UNIFYING EVENT THAT CAUSES SYMPTOMS AND SIGNS OF VENOUS DISEASE IS AMBULATORY VENOUS HYPTERTENSION What do you tell your patients about this? (30% risk of venous ulceration due to GSV distribution and already skin changes at the ankle) 5
6 Or this? And this is.. Lipoedema characteristic cut off sign at the ankles and no edema Of feet these patient typically complain of sensitive skin Weight loss only works to a certain degree usually hereditary Treatment Liposuction and mild compression (usually will help If they can stand it 6


7 7


8 4/25/2017 8


9 4/25/ years old 9

10 4/25/



11 4/25/
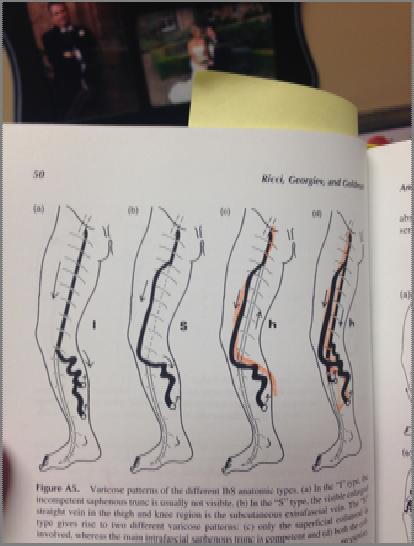
 to only superficial disease")
12 Frequently asked questions Aren t Vein Practices just cosmetic and spa centers? No - Phlebology practice encompasses a wide range of Services. As with other practices may deal with Deep system problems (such as May/Thurner syndrome thrombolytic therapy and stenting/coiling vascular malformation) to only superficial disease GSV/SSV/Perforator and or tributary disease to the reticular and telangiectasia OR both. Board Certification pathway in Phlebology is thru American Board of Venous and Lymphatic Medicine - Recognized by AOA and AMA as distinct primary or secondary specialty Certainly patients may initially present with the intent of a Cosmetic outcome but the evaluation always begins with a History/Physical AND a Duplex Ultrasound specifically for REFLUX (different protocol for DVT). Surprising Number of patients when carefully questioned about their leg discomfort have Symptoms that can be attributed to Venous Disease. 12
13 13
14 Perforator veins 14

15 Pelvic congestion syndrome Pelvic Congestion Syndrome Affects thousands of women in the U.S. More common in multiparous women Due to reflux in the ovarian veins, iliac veins, etc. May result in severe pelvic discomfort during the pre-menstrual period, after intercourse, and with prolonged standing May be effectively treated by blocking the reflux with embolization and/or pelvic vein sclerotherapy Venbrux AC et al J Vasc Interv Radiol 2002; 13:

16 4/25/
17 17
18 Venous Disease is a Hereditary Disorder 134 families were examined. The risk of developing varicose veins was: 89% if both parents had varicose veins 47% if one parent had varicose veins 20% if neither parent had varicose veins Cornu-Thenard, A, J Dermatol Surg Oncol 1994 May; 20(5): The beginnings of venous disease may be found as early as childhood Diagnosable Vein disease Actual Varicose Veins 740 pts y/o 518 pts y/o 459 pts y/o 2.5% 12.3% 19.8% 0 1.7% 3.3% Phlebologie Nov-Dec;43(4): Weindorf N, Schultz-Ehrenburg U. 18
19 Inactivity aggravates venous disease 2,854 patients with varicose veins, working in a factory 64.5% had jobs standing in one place 29.2% had jobs requiring prolonged periods of sitting 6.3% had jobs allowing frequent walking during their shift Santler, R Hautarzt 1956; 10:460 Each pregnancy worsens the condition 405 women with varicose veins 13% had one pregnancy 30% had two pregnancies 57% had three pregnancies Brand FN, et al The epidemiology of varicose veins: the Framingham Study Am J Prev Med 1988; 4:
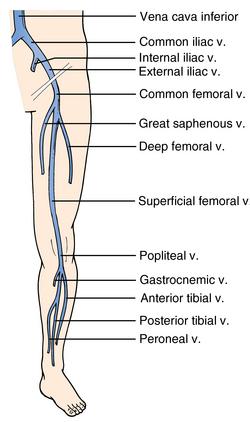
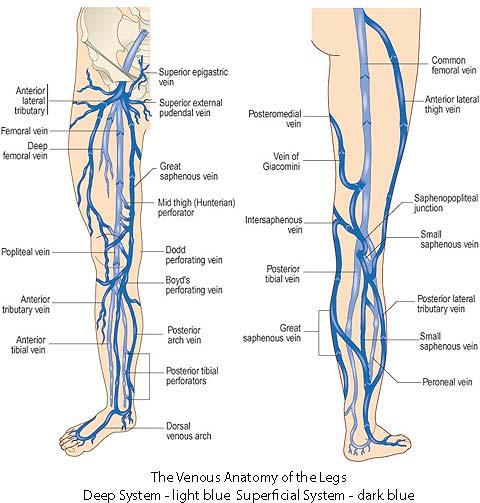
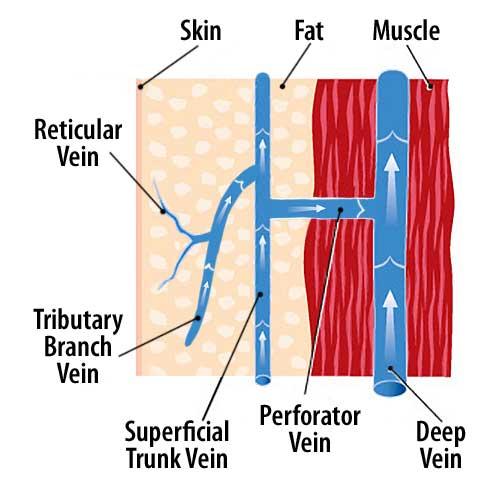
20 Anatomy and physiology of the venous system in the lower extremity Deep venous system: the channel through which 90% of venous blood is pumped out of the legs Superficial venous system: the collecting system of veins Perforating veins: the conduits for blood to travel from the superficial to the deep veins Musculovenous pump: Contraction of foot and leg muscles pumps the blood through one-way valves up and out of the legs 20


21 Venous Valvular Function Valve leaflets allow unidirectional flow, upward or inward Dilation of vein wall prevents opposition of valve leaflets, resulting in reflux Valvular fibrosis, destruction, or agenesis results in reflux 21

22 Doppler exam: Normal flow Illustration by Linda S. Nye Doppler: Reflux Illustration by Linda S. Nye 22

23 REFLUX: its contribution to varicose veins Illustration by Linda S. Nye Pathophysiology: 2 components REFLUX Dilatation of vein wall leads to valve insufficiency Monocytes may destroy vein valves Retrograde flow results in distal venous hypertension OBSTRUCTION Thrombosis and subsequent fibrosis obstruct venous outflow Damage to vein valves may also cause reflux Both contribute to venous hypertension The presence of both is far worse than either one alone 23

24 24




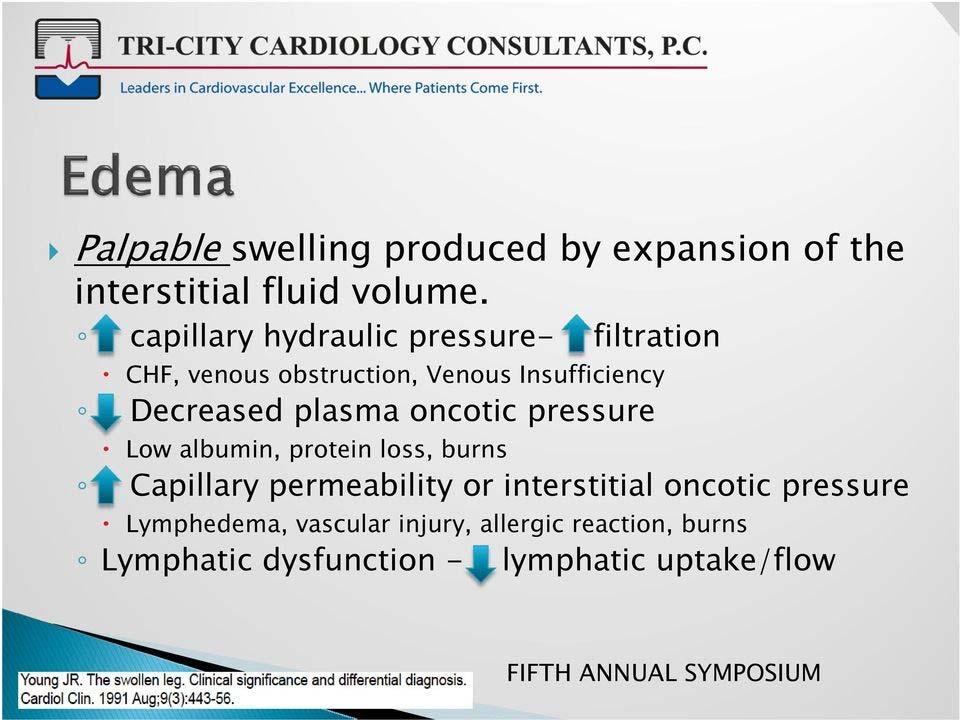
25 Frequently Asked Questions What does my poor circulation have to do with my swelling? We educate our patients on distinguishing between arterial and venous circulation and go over their particular factors for their swelling verbally and with a diagram. Draw Diagram How I educate patients on their Edema. 25
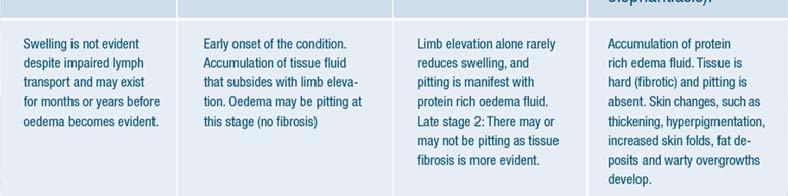
26 Edema All edema is lymphedema CHF Left and/or Right, cirrhosis, Renal failure = Diuretics + compression Venous insufficiency = compression not diuretics Lymphedema = manual decongestive therapy + compression Not diuretics Don t forget Thyroid Lipo Edema characteristic Cut off sign at ankle Can have all three PhleboLipoLymphedema Be sure to check ABI if compressing Caution if ABI <0.8 CHF (left and/or Right) Kidney disease Liver Disease Lymphedema Lipo edema Hypothyroidism Varicose Veins Exacerbating factors obesity/pulmonary hypertension 26


27 27

28 28

29 4/25/
30 30






31 Test Patient : What could be wrong with this guy??? I.e. would you send him for an ablation procedure? CHF (left and/or Right) Kidney disease Liver Disease Lymphedema Lipo edema Hypothyroidism Varicose Veins Exacerbating factors obesity/pulmonary hypertension What i see 31
32 CEAP Classification C = Clinical C0 - no visible venous disease C1 - telangiectasias or reticular veins C2 - varicose veins C3 - edema C4 - skin changes without ulceration C4a pigmentation or eczema C4b LDS or atrophie blanche C5 - skin changes with healed ulceration C6 - skin changes with active ulceration E = Etiology (primary vs. secondary) A = Anatomy (defines location of disease within superficial, deep and perforating venous systems) P = Pathophysiology (reflux, obstruction, or both) What to Expect Their 1 st appointment typically takes approximately hrs. depending on the complexity of their disease. After review of their condition You should receive the consult with my findings and recommendations to the patient. I Would like your help My typical recommendations would include exercise, weight loss, continue compression, and leg elevation when resting. NSAIDS or analgesic medication for discomfort and schedule for procedure /further testing or follow up. If there is another potential cause of their swelling or a condition that would exacerbate their condition then I may recommend they see their PCP for further evaluation of their Pulmonary status, Cardiovascular status, Endocrine status Lymphedema referral and/or wound clinic referral( if they have an ulceration). 32
33 History History of problem: onset, pregnancies, prior DVT, immobilization Associated symptoms and relationship to heat, menses, exercise and compression Current medications Family history Previous treatment and result Goals of patient Physical Examination Examine patient in the standing position, from the groin to the ankle Inspect and palpate for varicose and telangiectatic veins Check the medial and lateral malleolar areas for skin changes suggestive of chronic venous insufficiency (e.g., corona phlebectatica) Inspect the abdomen for enlarged superficial veins if ilio-femoral thrombosis is suspected 33


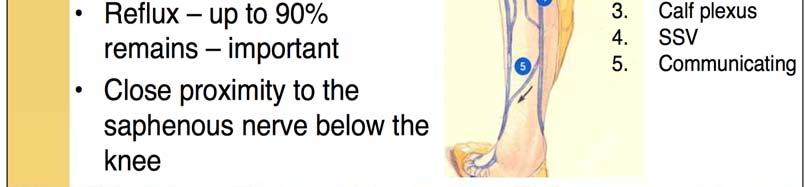
34 Telangiectasias Also known as spider veins due to their appearance Very common, especially in women Increase in frequency with age 85% of patients are symptomatic * May indicate more extensive venous disease * Weiss RA and Weiss MA J Dermatol Surg Oncol Apr;16(4): Lateral Subdermic Plexus Very common, especially in women Superficial veins with direct perforators to deep system Remnant of embryonic deep venous system 34


35 Reticular Veins Enlarged, greenish-blue appearing veins Frequently associated with clusters of telangiectasias May be symptomatic, especially in dependent areas of leg Varicose Veins Great Saphenous Distribution Most common finding in patients with varicose veins Varicosities most commonly along the medial thigh and calf but cannot assume location indicates origin At least 20% of patients are at risk of ulceration 35


36 Great Saphenous Insufficiency Skin changes are seen along the medial aspect of the ankle The presence of skin changes is a predictor of future ulceration * * Kirsner R et al. The Clinical Spectrum of Lipodermato-sclerosis, J Am Acad Derm, April 1993;28(4):623-7 Varicose Veins Small Saphenous Distribution Less frequent than Great Saphenous involvement Varicosities may be seen on the posterior calf and lateral ankle Skin changes are seen along the lateral ankle 36
 Atrophie blanche (C4b) Pigmentation")



37 Skin changes suggestive of chronic venous insufficiency Corona Phlebectatica (C1) Atrophie blanche (C4b) Pigmentation (C4a) Healed ulcer (C5) Venous Ulceration Over 50% of patients have only superficial venous disease; superficial venous disease may be primary factor in 50-85% of patients * <10% have only deep venous disease Results from ambulatory venous hypertension, which leads to WBC activation, TCpO2, local release of proteolytic enzymes * Shami SK et al. J Vasc Surg 1993; 17:
 of the GSV and or SSV and tributaries then Insurance will")

38 Venous Ulceration Impending ulceration Lipodermatosclerosis (C4a) Venous ulceration (C6) Are Vein procedures covered by my insurance? By and large if a patient has symptomatic venous disease with duplex findings of Reflux and enlarged size veins(variable to the insurance) of the GSV and or SSV and tributaries then Insurance will typically cover their treatment Of course some insurances are more strict. Insurance LCD Also dictate mostly that the axial Veins of the GSV/SSV must be treated first before tributary disease can be covered Foam and Liquid Sclerotherapy of veins less than 3mm and no reflux typically are not covered and are treated if symptomatic or at the desire of the patient for a more esthetic outcome on a Cash basis. (most SYMPTOMS are improved with treatment of the above however the end result is driven by the patient for cosmetic appearance). 38
39 Do I have to wear Compression stockings? Compression stockings are a very important part of treating chronic venous disease Depending on where the patient is on the spectrum of their particular disease process they may be recommended to always wear their compression hose(especially if Deep Reflux) or they may not need to wear their hose after their treatment if ALL reflux has been treated and no further symptoms. HOWEVER All insurance Carriers start with a period of conservative treatment which includes Compression hose NOT TED hose typically 20-30mmHg compression VENOUS DISEASE IS A CONDITION OF CHRONICITY AND MUST BE FOLLOWED NEW AREAS OF REFLUX WILL LIKELY DEVELOP IN THE FUTURE AND MAY BE DEALT WITH EXPECTANTLY to not notify a patient of this would disappoint the patient. CONSERVATIVE TREATMENT OF VENOUS DISORDERS 39

40 Compression Therapy Provides a gradient of pressure, highest at the ankle, decreasing as it moves up the leg Reduces reflux of blood Improves venous outflow Increases velocity of blood flow to reduce the risk of blood clots Photo courtesy of Juzo Compression Therapy Reduces symptoms of aching, fatigue, pain, and swelling Increases fibrinolytic activity Increases TCpO2 Mainstay of treatment for venous ulcers NOTE: Graduated compression therapy and wound care will heal venous stasis ulcers. Elimination of the reflux will reduce the recurrence. 40


41 Elastic compression stockings Must be graduated Calf high generally sufficient Replace q 6 months to assure proper pressure Available in a variety of strengths, styles, colors, and fabrics Graduated compression is not the same as T.E.D. hose T.E.D.s are meant for nonambulatory, supine patients T.E.D.s are indicated to decrease the incidence of thrombosis T.E.D.s do not provide sufficient pressure for ambulatory patients 41
42 Compression Strength 8-15mm Indications Leg fatigue, mild swelling, stylish 15-20mm Mild aching, swelling, stylish 20-30mm Aching, pain, swelling, mild varicose veins 30-40mm * Aching, pain, swelling, varicose veins, post-ulcer 40-50, 50-60mm * Recurrent ulceration, lymphedema * Requires a prescription Gradient compression hose At least Calf high 20-30mmhg Thigh high or panty hose may be more comfortable depending on the situation Open or closed toe depending on concurrent condition such as diabetes, neuropathy or concurrent arterial disease. The clock starts ticking when they began their compression so If you document it I can use that date for their insurance approval. Where can they get them? DME store LKM, Freeland Brown, Fidelity Lymphedema, can purchase over the counter ( typically sized by the calf and thigh circumference and outseam) Yes some fit better than others but if symptoms helped and continue despite their stockings and reflux found good chance they will respond to treatment. 42
43 If they have an Ulcer This is a good patient to send to both the wound center AND Tulsa Vein as the wound centers are great at getting them in compression, evaluating the wound for proper dressings/home health, debridement, biopsy, and education. We can work on the Cause of the Ulceration REFLUX -and try to get the ulcer healed faster and maintain skin integrity with intervention such as endovenous ablation and foam sclerotherapy or other techniques. Likely their Ultrasound will prognosticate if they have single, double or triple component disease meaning superficial or Deep or perforator disease or all three. 43
44 Evaluation and treatment of Venous Ulcerations We will get into this Summarize Compression mainstay of treatment of venous ulcerations showed no help of healing with ligation/stripping HOWEVER reoccurrence rate decreased with ligation/stripping with Evidence of Eschar Study Several flaws in methodology Society for Vascular Surgery and American venous Forum recommendations Grade 1B compression therapy for healing venous ulcers Grade 1B if patient is candidate for Ablation of symptomatic varicose veins without ulcers over chronic compression Grade 1A ablation of incompetent superficial veins in addition to compression therapy for reduced reoccurrence rates for Venous Ulcerations 44





")
")

45 Endothermal and Non thermal Ablation Venefit Procedure Coviden/Medtronic Endothermal Laser Ablation Mechanical Occlusion Chemical Assisted ablation (Clarivein) Venaseal (cyanoacrolate) Varithena Microchemical Foam ablation Steam ablation Foam ablation Stripping Local Microphlebectomy 45

46 91 CURRENT APPROACHES TO THE TREATMENT OF VARICOSE VEINS ALWAYS TREAT THE TRUNK FIRST IF REFLUX FOUND Radiofrequency Closure Technique Outpatient procedure approximately 60 min. long Local tumescent Temperature at vein wall controlled >90% closure at 2 yrs FDA-approved for RX of Great Saphenous Vein 46



47 93 Treatment of telangiectasias Sclerotherapy most effective Laser may be helpful Multiple treatments usually required Reduces symptoms in 85% of patients Improves quality of life Weiss RA and Weiss MA J Dermatol Surg Oncol Apr;16(4): Sclerotherapy of Telangiectasias: Technique Injection of sclerosant solution causes damage to endothelium which leads to fibrosis of vein 47

 visible Efficacy enhanced with foamed sclerosant Photo courtesy of")
48 Treatment of Reticular Veins Frequently associated with telangiectasias, their Rx may enhance results of sclerotherapy of telangiectasias Visualization may be improved with transillumination Ultrasound-guided Sclerotherapy Nearly any size vein can be treated Needle location inside vein, as well as movement of sclerosant and response of vein (spasm) visible Efficacy enhanced with foamed sclerosant Photo courtesy of CompuDiagnostics, Inc. 48


49 Sclerotherapy Results Before After Ultrasound-guided sclerotherapy of the Great Saphenous Vein and sclerotherapy of branches Photos courtesy of Steven Zimmet, MD, FACPh Surgical Treatment of Varicose Veins: Vein Stripping Vein stripping used to remove Great and Small saphenous veins Yields 60% long term improvement Neovascularization a problem Usually requires general anesthetic courtesy of John Bergan, MD Butler CM, et al Phlebology :

50 Surgical Treatment of Varicose Veins: Phlebectomy Very esthetic method of removing varicose veins Usually requires only local anesthetic Especially useful for tributaries of GSV, SSV 50





51 Treatment Results Before After Endovenous obliteration of the Great Saphenous Vein and phlebectomy of tributaries Photos courtesy of Steven Zimmet, MD, FACPh Superficial Thrombophlebitis: Management In the presence of varicose veins, DVT found in 10-20% Initial RX includes graduated compression and ambulation NSAID s for pain Antibiotics rarely needed 51
52 Thank You!!!! 52
53 Meet the Staff! Kelly Nichols Front office Reception Lori Bolman Medical assistant Tammy Haraway yep she s related Keeps track of everything/everyone And myself My Contact Information And a big thank you for attending! We hope to Grow with you! Tulsa vein Institute 81 st and Lewis office Fax My Cell phone number
54 Spectrum of Venous disease G. Davin Haraway DO, FACOI,FACCWS, RPhS Tulsa Vein Institute 26 y/o female with hx of port wine stain left leg from birth, as infant had varicose vein from knee down and "had checked out" but doesn't remember who. started having bulging noticeable vein in thigh when in college but non tender. past two years has been enlarging. this July went trip flying to California while there noted both legs and ankles swelling but subsided when she got back. and more bulging left leg vein. approx. 3 weeks ago went to Podiatrist and had cortisone shot left heel for plantar fasciitis. before shot had some local phlebitis left inside knee and now tender along the left leg knee and thigh. runs about 4 miles a day. now with restless legs. now has edema at end of day. elevation helps. has not worn compression stockings before. has taken ibuprophen and ice feels better. Podiatrist told to schedule appt here. Medical History 54




55 55
56 No DVT Mild Deep reflux on left Severe SFJ and GSV reflux left Isolated 4cm non compressibility and superficial phlebitis of Distal thigh Proximal Calf GSG Severe refluxing varicosities upper thigh and calf With port wine staining congenital syndrome diagnosis entertained Deep System: Duplex exam of the bilateral deep venous system demonstrates coaptation of vessel walls with compression and intact Doppler signals with distal augmentation, no intraluminal echoes are observed throughout the CFV, FV, POP, and tibial veins. No evidence of DVT. Mild evidence of deep venous reflux on left Superficial System: Largest Vein Diameter: RGSV:0.17 cm LGSV:_0.62_cm RT SFJ is intact without pathologic reflux. Right GSV is small and shows no pathologic reflux except for distal calf of 1812ms of reflux LT SFJ is enlarged at 0.67cm shows >2958ms of pathologic reflux and GSV is enlarged at 0.62cm with maximal reflux of 2352ms. severe reflux of the calf GSV is also present with >2292ms of pathologic reflux and large tributary disease. Active phlebitis of 4cm segment of the distal GSV present Impression: 1. No evidence of DVT. 2. mild left deep venous reflux. 3. NOSevere reflux of the Rt. GSV. (suitable for ablation) 4. NOSevere reflux of the Rt. SSV. (suitable for ablation) 5. Severe reflux of the Lt. GSV. (suitable for ablation) 6. NOSevere reflux of the Lt. SSV. (suitable for ablation) 7. Bilateral unremarkable PTV perforators. severe varicosities noted to the left medial calf amiable for phlebectomy Davin Haraway DO,FACOI,FACCWSResults 56
57 Long story HGB 5.8 at IR evaluation but plans for further eval once anemia evaluated most common Fe def from menorrhagia but risk if GI source Next visit clot extension despite NSAIDS and compression urgent RF ablation proximal to clot in GSV. And second opinion Saw popliteal clot at second opinion removable filter placed and Lovenox 40mg started. (abnormal Iliac anatomy suspected with filter placement) GI eval scheduled per PCP - HGB improving on Fe Eventual IVUS May Thurner anatomy and stent deployed No obvious Av malformations detected to thigh port wine stain. 3monnths Xarelto life long ASA saw GYN in between all this and had hypercoag panel neg Scheduled for RF ablation of residual GSV and Phlebectomy and US guided sclerotherapy in future. Diagnosis Klippel Trenaunay like syndrome (no bony over growth) and persistent lateral vein not apparent Parkes-weber (above plus av fistula) I do not feel she has but was discussed Some evidence of genetic translocation t(8;14)(q22.3;q13) Billy Corgan lead singer for the Smashing Pumpkins 57
58 dogma Do what is Only right in your God (attending s) eyes - or May you never pass with your Ass(etts) intact You could probably think up more Learn your basics well but Keep an open mind for improvement and Change! To learn you must realize that you do not know (that s mine) 58
PHLEBOLOGY. Venous Insufficiency. Presentation Use Information
 Disclosure of Conflict of Interest THE BASICS OF VENOUS INSUFFICIENCY: What You Should Know. An Introductory Lecture Donald Ives, MD, RVT, RPVI Board Certified Family Physician Diplomate of the American
Disclosure of Conflict of Interest THE BASICS OF VENOUS INSUFFICIENCY: What You Should Know. An Introductory Lecture Donald Ives, MD, RVT, RPVI Board Certified Family Physician Diplomate of the American
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
lipodermatosclerosis standards of medical practitioners and the quality of patient care related to the treatment of venous disorders.
 Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
AMERICAN PODIATRIC MEDICAL ASSOCIATION
 AMERICAN PODIATRIC MEDICAL ASSOCIATION THE NATIONAL ANNUAL SCIENTIFIC MEETING Friday, July 13 th 2018 Washington, D.C. CHRONIC VENOUS INSUFFICIENCY OF THE LOWER EXTREMITIES Clinical Pearls for the Podiatrist
AMERICAN PODIATRIC MEDICAL ASSOCIATION THE NATIONAL ANNUAL SCIENTIFIC MEETING Friday, July 13 th 2018 Washington, D.C. CHRONIC VENOUS INSUFFICIENCY OF THE LOWER EXTREMITIES Clinical Pearls for the Podiatrist
Additional Information S-55
 Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona
 Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona March 8, 2011 Varicose Vi Vein Market Approximately 40% of the US population has venous disease;
Expanding Your Vein Business Terri Morrison, RN, B.S., CEO Morrison Vein Institute Scottsdale/Tempe Arizona March 8, 2011 Varicose Vi Vein Market Approximately 40% of the US population has venous disease;
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat?
 Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Chronic Venous Insufficiency
 Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency
 The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency Thomas E. Eidson, DO Certified Venous Disease Specialist Board Certified Family Medicine Disclosure of Conflict of
The Vascular Disease Almost No One Teaches But Should!!! Chronic Venous Insufficiency Thomas E. Eidson, DO Certified Venous Disease Specialist Board Certified Family Medicine Disclosure of Conflict of
Superficial Varicose and Deep Vein Concerns - ACOI Chicago Hospitalist Meeting
 Superficial Varicose and Deep Vein Concerns - ACOI Chicago Hospitalist Meeting Davin Haraway DO,FACOI,FACCWS,RPhS Diplomate American Board of Venous and Lymphatic Medicine Vein issues encountered by Hospitalists
Superficial Varicose and Deep Vein Concerns - ACOI Chicago Hospitalist Meeting Davin Haraway DO,FACOI,FACCWS,RPhS Diplomate American Board of Venous and Lymphatic Medicine Vein issues encountered by Hospitalists
Patient Information. Venous Insufficiency and Varicose Veins
 Patient Information Venous Insufficiency and Varicose Veins What is a Varicose Vein? Gitter Vein Institute-revised 3/8/2016 2 Frequently Asked Questions What is the difference between varicose and spider
Patient Information Venous Insufficiency and Varicose Veins What is a Varicose Vein? Gitter Vein Institute-revised 3/8/2016 2 Frequently Asked Questions What is the difference between varicose and spider
PROVIDER POLICIES & PROCEDURES
 PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
PROVIDER POLICIES & PROCEDURES TREATMENT OF VARICOSE VEINS OF THE LOWER EXTREMITIES STAB PHLEBECTOMY AND SCLEROTHERAPY TREATMENT The primary purpose of this document is to assist providers enrolled in
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
How varicose veins occur
 Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Selection and work up for the right patients suspected of deep venous disease
 Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Selection and work up for the right patients suspected of deep venous disease R A G H U K O L L U R I, M S, M D, R V T S Y S T E M M E D I C A L D I R E C T O R V A S C U L A R M E D I C I N E / V A S
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
Vein Disease Treatment
 MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY
 RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
OHTAC Recommendation. Endovascular Laser Treatment for Varicose Veins. Presented to the Ontario Health Technology Advisory Committee in November 2009
 OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
OHTAC Recommendation Endovascular Laser Treatment for Varicose Veins Presented to the Ontario Health Technology Advisory Committee in November 2009 April 2010 Issue Background The Ontario Health Technology
Patient assessment and strategy making for endovenous treatment
 Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Clinical case. Symptomatic anterior accessory great saphenous vein (AAGSV) reflux
 reflux") Clinical case Symptomatic anterior accessory great saphenous vein (AAGSV) reflux A 70 year-old female presents with symptomatic varicose veins on left leg for more than 10 years. She complains of heaviness,
Clinical case Symptomatic anterior accessory great saphenous vein (AAGSV) reflux A 70 year-old female presents with symptomatic varicose veins on left leg for more than 10 years. She complains of heaviness,
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.
 to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN.") How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
How to choose which treatment method(s) to use for a particular varicose veins patient ESTABLISHING A TREATMENT PLAN Surgeon Dr G Mark Malouf Sydney Australia Following History and Physical examination
2017 Florida Vascular Society
 Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Medicare C/D Medical Coverage Policy
 Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Segmental GSV reflux
 Segmental GSV reflux History of presentation A 43 year old female presented with right lower extremity varicose veins and swelling. She had symptoms of aching, heaviness and tiredness in the right leg.
Segmental GSV reflux History of presentation A 43 year old female presented with right lower extremity varicose veins and swelling. She had symptoms of aching, heaviness and tiredness in the right leg.
Current Management of Varicose Veins
 Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Determine the patients relative risk of thrombosis. Be confident that you have had a meaningful discussion with the patient.
 Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
High Level Overview: Venous Anatomy of Lower Extremities. Anatomy of a Vein 5/11/2015. Barbara Deusterman, RN
 High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
High Level Overview: Venous Anatomy of Lower Extremities Barbara Deusterman, RN What does this anatomy lecture have to do with visually guided sclerotherapy (VGS)? May 11, 2015 2 Anatomy of a Vein Almeida,
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.066.MH Last Review Date: 11/08/2018 Effective Date: 01/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
Varicose Vein Information Sheet
 Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
Neil Goldstein, MD Joseph Hewett, MD Board- Certified Physicians in Interventional, Diagnostic, and Vascular Radiology, Surgery, Vascular Surgery and Phlebology Varicose Vein Information Sheet PREVALENCE
Recurrent Varicose Veins We All See Them
 We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
We All See Them November 4, 2017 Austin, TX Arlington Heights, IL No conflicts Terminology REVAS REcurrent Varices After Surgery PREVAIT PREsence of Varices After Interventional Treatment Recurrent varices
Introduction to Saphenous Vein Ablations: When/Why/How?
 John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
Prevalence. Definition. Chronic Venous Insufficiency. Overview of Chronic Venous Insufficiency
 Overview of Chronic Venous Insufficiency Steven M. Dean, DO, FACP, RPVI Vascular Medicine Specialist Assistant Professor of Internal Medicine Department of Cardiovascular Medicine The Ohio State University
Overview of Chronic Venous Insufficiency Steven M. Dean, DO, FACP, RPVI Vascular Medicine Specialist Assistant Professor of Internal Medicine Department of Cardiovascular Medicine The Ohio State University
COMMISSIONING POLICY
 Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
UNDERSTANDING VEIN PROBLEMS
 UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Epidemiology: Prevalence
 Epidemiology: Prevalence More than 30 million Americans suffer from varicose veins or a more serious form of venous disease called Chronic Venous Insufficiency (CVI). 1 Of the over 30 million Americans
Epidemiology: Prevalence More than 30 million Americans suffer from varicose veins or a more serious form of venous disease called Chronic Venous Insufficiency (CVI). 1 Of the over 30 million Americans
All you need to know about. Varicose Veins. & its treatments. in 10 mins
 All you need to know about Varicose Veins & its treatments in 10 mins Contents Symptoms and Causes...04 Risk Factors...05 Relief: The Top Five Tips...06 Compression Stockings or Bandages...08 New Surgery
All you need to know about Varicose Veins & its treatments in 10 mins Contents Symptoms and Causes...04 Risk Factors...05 Relief: The Top Five Tips...06 Compression Stockings or Bandages...08 New Surgery
Conflict of Interest. None
 Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Endovenous Radiofrequency and Laser Ablation
 Endovenous Radiofrequency and Laser Ablation [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr go to Comunicados a Proveedores, and click Cartas Circulares.]
Endovenous Radiofrequency and Laser Ablation [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr go to Comunicados a Proveedores, and click Cartas Circulares.]
Techniques and Specific Treatment Modalities for the Active Non-Healing Wound. Luke Maj, MD, MHA
 Techniques and Specific Treatment Modalities for the Active Non-Healing Wound Luke Maj, MD, MHA Assistant Professor of Radiology University of Miami, Miller School of Medicine Director of The Vein Center
Techniques and Specific Treatment Modalities for the Active Non-Healing Wound Luke Maj, MD, MHA Assistant Professor of Radiology University of Miami, Miller School of Medicine Director of The Vein Center
8/16/18. Chronic Venous Insufficiency. Financial Disclosure. Case Study. Prevalence. Risk Factors. Objectives
 Chronic Venous Insufficiency Financial Disclosure Unfortunately, I have no financial obligations to disclose. Kimberly Giberga MSN APRN FNP-C RPhS 2018 Objectives Describe Venous Anatomy Describe the pathophysiology
Chronic Venous Insufficiency Financial Disclosure Unfortunately, I have no financial obligations to disclose. Kimberly Giberga MSN APRN FNP-C RPhS 2018 Objectives Describe Venous Anatomy Describe the pathophysiology
Venous Disease and Leg Ulcers. Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL
 Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments
 1 Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments What are spider veins? Spider veins are dilated, small blood vessels that have a red or bluish color. They appear
1 Vein & Body Specialists at The Bellevue Hospital Spider Vein and Varicose Vein Treatments What are spider veins? Spider veins are dilated, small blood vessels that have a red or bluish color. They appear
Medical Affairs Policy
 Service: Varicose Vein Treatments PUM 250-0032 Medical Affairs Policy Medical Policy Committee Approval 12/01/17 Effective Date 04/01/18 Prior Authorization Needed Yes Disclaimer: This policy is for informational
Service: Varicose Vein Treatments PUM 250-0032 Medical Affairs Policy Medical Policy Committee Approval 12/01/17 Effective Date 04/01/18 Prior Authorization Needed Yes Disclaimer: This policy is for informational
UNDERSTANDING VEIN DISEASE. UC EN - For use in the U.S. only
 UNDERSTANDING VEIN DISEASE UC201706537 EN - For use in the U.S. only Do you need to sit down during your work day because your legs ache and/or swell? Do you miss out on doing the activities you love because
UNDERSTANDING VEIN DISEASE UC201706537 EN - For use in the U.S. only Do you need to sit down during your work day because your legs ache and/or swell? Do you miss out on doing the activities you love because
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
Management of Post-Thrombotic Syndrome
 Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Varithena 3 rd February 2015
 Varithena 3 rd February 2015 Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other forward-looking statements with respect to
Varithena 3 rd February 2015 Forward-looking statement This presentation and information communicated verbally to you may contain certain projections and other forward-looking statements with respect to
Sincerely, Michael R. Probstfeld, M.D., FACS Southern Arizona Laser & Vein Institute A MESSAGE ABOUT OUR PATIENT HISTORY FORM
 A MESSAGE ABOUT OUR PATIENT HISTORY FORM. Dear Patients, Thank you in advance for taking the time to accurately complete our SALVI patient questionnaire. This valuable tool helps us to help you. Due to
A MESSAGE ABOUT OUR PATIENT HISTORY FORM. Dear Patients, Thank you in advance for taking the time to accurately complete our SALVI patient questionnaire. This valuable tool helps us to help you. Due to
NCVH. Ultrasongraphy: State of the Art Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW
 Ultrasongraphy: State of the Art 2015 NCVH New Cardiovascular Horizons Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW Anil K. Chagarlamudi, M.D. Cardiovascular
Ultrasongraphy: State of the Art 2015 NCVH New Cardiovascular Horizons Vein Forum 2015 A Multidisciplinary Approach to Otptimizing Venous Circulation From Wounds to WOW Anil K. Chagarlamudi, M.D. Cardiovascular
Lower Extremity Venous Insufficiency Evaluation
 VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Venous Insufficiency Evaluation This Protocol was prepared by members of the Society for Vascular Ultrasound (SVU) as a template
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Lower Extremity Venous Insufficiency Evaluation This Protocol was prepared by members of the Society for Vascular Ultrasound (SVU) as a template
Varicose Vein Cyanoacrylate Glue treatment
 The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
Let s Take a Look Venous Insufficiency Ultrasound Techniques
 Let s Take a Look Venous Insufficiency Ultrasound Techniques Brent Wilkinson RVT, RDMS Steve Schomaker RVT, RDCS, RDMS Let s take a look Differentiate between normal venous flow and venous insufficiency
Let s Take a Look Venous Insufficiency Ultrasound Techniques Brent Wilkinson RVT, RDMS Steve Schomaker RVT, RDCS, RDMS Let s take a look Differentiate between normal venous flow and venous insufficiency
Endothermal Ablation for Venous Insufficiency. Dr. S. Kundu Medical Director The Vein Institute of Toronto
 Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy
Endothermal Ablation for Venous Insufficiency Dr. S. Kundu Medical Director The Vein Institute of Toronto Objective: remove the GSV from the circulation 1. Surgical - HL & stripping 2. Chemical sclerotherapy
Varicose Vein Surgery
 What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
What are varicose veins? Varicose veins are enlarged and twisted veins in your leg. Varicose veins are common, affecting up to 3 in 10 people. Varicose veins tend to run in families and are made worse
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015
 Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
Love your legs again Varicose Veins
 Love your legs again Varicose Veins Veins are the vessels that return blood to the heart once it has circulated through the body (as opposed to arteries, which carry oxygen-rich blood from the heart to
Love your legs again Varicose Veins Veins are the vessels that return blood to the heart once it has circulated through the body (as opposed to arteries, which carry oxygen-rich blood from the heart to
New Guideline in venous ulcer treatment: dressing, medication, intervention
 New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
Dr Peter Chapman-Smith
 Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
A treatment option for varicose veins. enefit" Targeted Endovenous Therapy. Formerly known as the VNUS Closure procedure E 3 COVIDIEN
 A treatment option for varicose veins. enefit" Targeted Endovenous Therapy Formerly known as the VNUS Closure procedure E 3 COVIDIEN THE VENOUS SYSTEM ANATOMY The venous system is made up of a network
A treatment option for varicose veins. enefit" Targeted Endovenous Therapy Formerly known as the VNUS Closure procedure E 3 COVIDIEN THE VENOUS SYSTEM ANATOMY The venous system is made up of a network
Deep Venous Pathology. Eberhard Rabe Department of Dermatology University of Bonn Germany
 Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Alberta Health. Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual
 Alberta Health Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual March 7, 2016 Revision History Description Date N-03, N 05 and N-07:
Alberta Health Alberta Aids to Daily Living Compression Stockings and Lymphedema Sleeves Ready Made Benefits Policy & Procedures Manual March 7, 2016 Revision History Description Date N-03, N 05 and N-07:
Treatment of Varicose Veins
 Treatment of Varicose Veins Policy Number: Original Effective Date: MM.06.016 04/15/2005 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 09/28/2018 Section: Surgery Place(s) of
Treatment of Varicose Veins Policy Number: Original Effective Date: MM.06.016 04/15/2005 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 09/28/2018 Section: Surgery Place(s) of
Microphlebectomy for Varicose Veins
 Microphlebectomy for Varicose Veins Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look?
Microphlebectomy for Varicose Veins Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look?
Deep Vein Thrombosis
 Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Ligation with Stripping
 Ligation with Stripping Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look? Vein problems
Ligation with Stripping Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look? Vein problems
Latmedical, LLC is the exclusive Caribbean distributor
 No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
FIND RELIEF FROM VARICOSE VEINS. VenaSeal Sapheon Closure System
 FIND RELIEF FROM VARICOSE VEINS VenaSeal Sapheon Closure System UNDERSTAND Varicose veins may be a sign of something more severe. Your doctor can help you understand if you have this condition. may cause
FIND RELIEF FROM VARICOSE VEINS VenaSeal Sapheon Closure System UNDERSTAND Varicose veins may be a sign of something more severe. Your doctor can help you understand if you have this condition. may cause
Interactive Learning Session
 Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Dr Paul Thibault. Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology
 Australasian College of Phlebology") Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Le varici recidive Recurrent varices: how to manage them?
 Le varici recidive Recurrent varices: how to manage them? Marianne De Maeseneer MD PhD, Vascular Surgeon Department of Dermatology, Rotterdam, Netherlands & Faculty of Medicine and Health Sciences University
Le varici recidive Recurrent varices: how to manage them? Marianne De Maeseneer MD PhD, Vascular Surgeon Department of Dermatology, Rotterdam, Netherlands & Faculty of Medicine and Health Sciences University
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction. Erin H. Murphy, MD Rane Center
 Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
Appendix 1 to Direct Vision Sclerotherapy AUSTRALASIAN COLLEGE OF PHLEBOLOGY CLINICAL PROCEDURES. CP Direct Vision Sclerotherapy Clinical procedure
 Appendix 1 to Direct Vision Sclerotherapy AUSTRALASIAN COLLEGE OF PHLEBOLOGY CLINICAL PROCEDURES CP Direct Vision Sclerotherapy Clinical procedure 1 PURPOSE This procedure summarises the actions required
Appendix 1 to Direct Vision Sclerotherapy AUSTRALASIAN COLLEGE OF PHLEBOLOGY CLINICAL PROCEDURES CP Direct Vision Sclerotherapy Clinical procedure 1 PURPOSE This procedure summarises the actions required
Occasional pain or other discomfort (ie, not restricting regular daily activity)
") Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Criteria For Medicare Members. Kaiser Foundation Health Plan of Washington
 Clinical Review Criteria Treatment of Varicose Veins Radiofrequency Catheter Closure Sclerotherapy Surgical Stripping Trivex System for Outpatient Varicose Vein Surgery VenaSeal Closure System VNUS Closure
Clinical Review Criteria Treatment of Varicose Veins Radiofrequency Catheter Closure Sclerotherapy Surgical Stripping Trivex System for Outpatient Varicose Vein Surgery VenaSeal Closure System VNUS Closure
FIND RELIEF FROM VARICOSE VEINS. VenaSeal Closure System
 FIND RELIEF FROM VARICOSE VEINS VenaSeal Closure System UNDERSTAND Varicose veins may be a sign of something more severe venous reflux disease Your doctor can help you understand if you have this condition.
FIND RELIEF FROM VARICOSE VEINS VenaSeal Closure System UNDERSTAND Varicose veins may be a sign of something more severe venous reflux disease Your doctor can help you understand if you have this condition.
TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY
 TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY TL LUK Consultant Vascular Surgeon Sarawak General Hospital HKL Vascular Conference 19/06/2013 PREVALENCE OF LOWER LIMB VENOUS DISEASE Affects half of
TREATMENT OPTIONS FOR CHRONIC VENOUS INSUFFICIENCY TL LUK Consultant Vascular Surgeon Sarawak General Hospital HKL Vascular Conference 19/06/2013 PREVALENCE OF LOWER LIMB VENOUS DISEASE Affects half of
Varicose Veins. These are abnormal veins in the legs that appear as unsightly or cause other problems.
 Varicose Veins What are varicose veins? These are abnormal veins in the legs that appear as unsightly or cause other problems. They develop due to abnormal valve function that allows the blood to travel
Varicose Veins What are varicose veins? These are abnormal veins in the legs that appear as unsightly or cause other problems. They develop due to abnormal valve function that allows the blood to travel
Endo-Thermal Heat Induced Thrombosis (E-HIT)
") Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis, Klippel- Trenaunay syndrome DVT CVD
 Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Venous Reflux Duplex Exam
 Venous Reflux Duplex Exam GWENDOLYN CARMEL, RVT PHYSIOLOGIST, DEPARTMENT OF VASCULAR SURGERY NEW JERSEY VETERANS HEALTHCARE CENTER EAST ORANGE, NJ PURPOSE: To identify patterns of incompetence and which
Venous Reflux Duplex Exam GWENDOLYN CARMEL, RVT PHYSIOLOGIST, DEPARTMENT OF VASCULAR SURGERY NEW JERSEY VETERANS HEALTHCARE CENTER EAST ORANGE, NJ PURPOSE: To identify patterns of incompetence and which
MEDICAL POLICY SUBJECT: SURGICAL STOCKINGS AND COMPRESSION GARMENTS. POLICY NUMBER: CATEGORY: Equipment/ Supplies
 MEDICAL POLICY SUBJECT: SURGICAL STOCKINGS AND PAGE: 1 OF: 7 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
MEDICAL POLICY SUBJECT: SURGICAL STOCKINGS AND PAGE: 1 OF: 7 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including
SAVE LIMBS SAVE LIVES! Endovenous Ablation for Chronic Wounds
 SAVE LIMBS SAVE LIVES! Endovenous Ablation for Chronic Wounds Frank J. Tursi, DPM, FACFS Clinical Associate Professor, University of Pennsylvania/Presbyterian Foot and Ankle Consultant, Philadelphia Flyers,
SAVE LIMBS SAVE LIVES! Endovenous Ablation for Chronic Wounds Frank J. Tursi, DPM, FACFS Clinical Associate Professor, University of Pennsylvania/Presbyterian Foot and Ankle Consultant, Philadelphia Flyers,
Varicose veins. Information for patients Sheffield Vascular Institute
 Varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins. This leaflet explains more about varicose veins and answers some of the most frequently
Varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins. This leaflet explains more about varicose veins and answers some of the most frequently
Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment.
 Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment. Approximately 1 in 5 adult Americans suffer from superficial
Varicose Veins are a Symptom of Vein Disease. Now you can treat the source of your varicose veins with non-surgical endovenous laser treatment. Approximately 1 in 5 adult Americans suffer from superficial
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.015.MH Last Review Date: 11/08/2018 Effective Date: 02/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Compression Garments and
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers Compression Garments and
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing?
 Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
ACP Phlebology Fellowship Curriculum 1
 ACP Phlebology Fellowship Curriculum 1 There are seven columns in the curriculum outline 1. Goals and objectives (G & O)- curriculum objectives are listed in this column. 2. Resources- text references
ACP Phlebology Fellowship Curriculum 1 There are seven columns in the curriculum outline 1. Goals and objectives (G & O)- curriculum objectives are listed in this column. 2. Resources- text references
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Find From Varicose Veins. VenaSeal
 Find Relief From Varicose Veins VenaSeal Closure System Understand Varicose veins may be a sign of something more severe venous reflux disease. Your doctor can help you understand if you have this condition.
Find Relief From Varicose Veins VenaSeal Closure System Understand Varicose veins may be a sign of something more severe venous reflux disease. Your doctor can help you understand if you have this condition.
PROCEDURES FOR SPIDER AND VARICOSE VEINS. Reducing Symptoms and Improving Appearance
 PROCEDURES FOR SPIDER AND VARICOSE VEINS Reducing Symptoms and Improving Appearance Understanding Leg Vein Problems Do your legs feel tired and achy at the end of the day? Are you unhappy about visible
PROCEDURES FOR SPIDER AND VARICOSE VEINS Reducing Symptoms and Improving Appearance Understanding Leg Vein Problems Do your legs feel tired and achy at the end of the day? Are you unhappy about visible
Varicose veins. Natural history, assessment and management. Arteries and veins. Why do people get varicose veins? Classification of venous disease
 Arteries and veins Neil Wright Rob Fitridge Varicose veins Natural history, assessment and management Background Varicose veins are a common condition. Presentations can range from those that are noticed
Arteries and veins Neil Wright Rob Fitridge Varicose veins Natural history, assessment and management Background Varicose veins are a common condition. Presentations can range from those that are noticed
Page 1. Ruling out deep venous obstruction prior to superficial vein treatment. Disclosures. Indications for saphenous vein ablation (SVA)
") 1 Ruling out deep venous obstruction prior to superficial vein treatment Deepak Sudheendra, MD, RPVI Assistant Professor of Clinical Radiology & Surgery Disclosures No financial disclosures Indications
1 Ruling out deep venous obstruction prior to superficial vein treatment Deepak Sudheendra, MD, RPVI Assistant Professor of Clinical Radiology & Surgery Disclosures No financial disclosures Indications
Step by step ultrasound examination of varicose veins. Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany
 Step by step ultrasound examination of varicose Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany Required technical setup: B-mode vessel imaging combined with color
Step by step ultrasound examination of varicose Dr. Özgün Sensebat Vascular Surgeon Private Vascular Clinic Dorsten & Borken, Germany Required technical setup: B-mode vessel imaging combined with color
Endovenous Laser Therapy INFORMATION & TREATMENT INSTRUCTIONS
 1324 Princess Street Kingston, ON K7M 3E2 Website: www.ucosmetic.com Email: nuyu@ucosmetic.com Phone: (613) 536-LASR (5277) Fax: (613) 536-5108 Dr. Kim Meathrel, MD, FRCSC, Plastic Surgeon, Associate Professor
1324 Princess Street Kingston, ON K7M 3E2 Website: www.ucosmetic.com Email: nuyu@ucosmetic.com Phone: (613) 536-LASR (5277) Fax: (613) 536-5108 Dr. Kim Meathrel, MD, FRCSC, Plastic Surgeon, Associate Professor