Pregabalin Prescribing in Primary Care Audit Results 2012/13
|
|
|
- Sandra Bryant
- 5 years ago
- Views:
Transcription
 and ABHB has the highest cost per 1000 patients in Wales, 37% greater than the National")
1 Executive summary Pregabalin Prescribing in Primary Care Audit Results 2012/13 Pregabalin is extensively used across Aneurin Bevan Health Board (ABHB). It is the second highest medicine in terms of primary care prescribing expenditure ( 794k per quarter Dec 12) and ABHB has the highest cost per 1000 patients in Wales, 37% greater than the National average. An audit of pregabalin usage was therefore included within the Clinical Effectiveness and Prescribing Programme (CEPP) within primary care, to audit this medicine s use in relation to: Which conditions were being treated? Adherence to local and National guidance Source of Initiation Dosage regimes and dosage optimisation This audit was completed in 84 GP practices and included 3266 patients taking pregabalin. 69% of prescribing was for neuropathic pain, 22% for generalised anxiety disorder (GAD) and 9% for diabetic neuropathic pain (DNP). The results are summarised in the table below. Generally across all indications there were relatively low levels of documented adherence to local and National guidelines, and within the treatment indications for neuropathic pain and diabetic neuropathic pain there was poor documented evidence of assessment of efficacy at maximally tolerated doses. Indication % Initiated in % Adherence % Initiated in % Adherence % Initiation (n=3266) Secondary Care to Guidance Primary Care to Guidance Unknown Neuropathic 52% 34% 46% 35% 2% Pain (69%) GAD (22%) 67% 38% 32% 16% 1% DNP (9%) 45% 19% 52% 11% 3% Dosage optimisations led by Prescribing Support technicians aiding the completion of the audit resulted in savings in excess of 139K, which indicated a lack of awareness on the flat, twice daily, pricing structure of this product. There was evidence, from completion of audit summary sheets in GP practices by the clinicians, that practices were made more aware of the issues around pregabalin prescribing, especially in relation to adherence with NICE guidelines, dose optimisation strategies and medication reviews for patients
2 taking pregabalin. 92% of GP practices intended to discuss these issues within their practice meetings. In summary, this was an extensive primary care audit which raised the awareness of clinicians of National and local guidelines. It is clear that implementation of guidance needs to be improved across the whole Health Board, in order that the prescribing of pregabalin reflects the positioning of the drug within existing guidance. It is intended to repeat this audit to assess any improvements in prescribing in 2013/14. Sponsored by: Prepared by: Jonathan Simms Clinical Director of Pharmacy Mike Curson Senior Primary Care Pharmacist Date 28 th February
")

3 Introduction The objective of this review is to measure current prescribing of pregabalin for neuropathic pain and generalised anxiety disorder against the Aneurin Bevan Health Board (ABHB) Guidelines for the diagnosis and management of Neuropathic Pain 4, ABHB guidelines for Diabetic Peripheral Neuropathic Pain 4 and the National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 113: Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults 9. ABHB spent 2.7 million on pregabalin in primary and secondary care during 2011, an increase of 25% compared to 2010, Although the trend in pregabalin prescribing has increased across all of the Welsh Health Localities, ABHB has the highest cost per 1000 patients in Wales and is 37% greater than the Welsh national average. 3
4 Method and Results. Data was collected, utilising the audit pack Appendix 1, for 3,266 patients taking pregabalin over 84 GP Practices in Aneurin Bevan Health Board who were receiving the treatment for the following conditions: Neuropathic Pain 2,264 patients Diabetic Neuropathic Pain 282patients Generalised Anxiety Disorder 720 patients 11% of patients were on a three times a day (TDS) dosage which was changed to an equivalent twice a day (BD) dosage along with other dose optimisations e.g. 25mg 2 BD to 50mg 1BD which collectively realised annual savings in excess of 139,000. ABHB Pregabalin Prescribing 2012/13 Neuropathic pain Diabetic Neuropathic pain Generalised Anxiety Disorder 22% 9% 69% Pregabalin for Neuropathic Pain In March 2010 NICE published guidance for the pharmacological management of neuropathic pain CG96 1 specifying pregabalin as one of the first-line treatment options. However in June 2010 the Drug and Therapeutics Bulletin 2 published an article questioning the validity of this recommendation stating that gabapentin was excluded as a treatment option based on indirect comparisons suggesting that, in relation to pregabalin, it offers less net benefit, is less cost-effective and requires more complex dosing and titration. Furthermore there were concerns over the economic modelling, on which CG96 was based to conclude that pregabalin was more cost-effective than gabapentin. It has been suggested that the drug costs used in the Health Technology Assessment (HTA) 3 were based exclusively on gabapentin generic tablets rather than the less expensive generic capsules and the costs of pregabalin assumed twice daily (rather than the more costly three times daily) dosing. As a result of this in July 2011, NICE in collaboration with the 4
5 HTA group were due to publish a review of the economic modelling but have recently announced the clinical guideline will now be fully revised in order to address ongoing uncertainties of cost effectiveness of some of the recommended treatment options. In September 2010 the Gwent Partnership Medicines and Therapeutics Committee discussed local implementation of NICE CG96 and based on the concerns above produced interim local guidance for the pharmacological management of neuropathic pain in a non-specialist setting 4 which reflects the current recommendations from the NHS Clinical Knowledge Summaries 5. This was supported by a letter to all prescribers in September 2010 from the Medical Director and the GPMTC chair 6. The Scottish Medicines Consortium has also restricted pregabalin for the treatment of peripheral neuropathic pain in adults to patients who have not achieved adequate pain relief from, or have not tolerated, conventional first and second line treatments for peripheral neuropathic pain. There is also a recommendation that treatment should be stopped if the patient has not shown sufficient benefit within 8 weeks of reaching the maximally tolerated therapeutic dose. 7 Of the 2,264 patients prescribed pregabalin for neuropathic pain 46% were initiated by the GP, 52% initiated by secondary care and 2% unknown due to limited documentation recorded as the patients are new to the practice. 35% of those initiated by the GP were prescribed in line with the local guidance compared to 34% of those initiated in secondary care. In both cases the majority of patients had no documentation of previous gabapentin use. Although it was not a requirement of the audit it was observed that there was a high incidence of side effects documented for those patients who had previously taken gabapentin. Diabetic Peripheral Neuropathic pain (DPN) NICE CG96 1 for the pharmacological management of neuropathic pain in adults recommends duloxetine as first line treatment for people with painful diabetic neuropathy with pregabalin and amitriptyline recommended as second line treatment options. However due to the concerns regarding the exclusion of gabapentin, ABHB have produced local guidance 8 which includes gabapentin and places pregabalin as a 4 th line treatment option. Of the 282 patients prescribed pregabalin for diabetic neuropathic pain 52% were initiated by the GP, 45% initiated by secondary care and 3% unknown due to limited documentation recorded as the patients are new to the practice. 11% of those initiated by the GP were prescribed in line the local guidance compared to 19% of those initiated in secondary care. In both cases the majority of patients had no documentation of previous duloxetine or gabapentin use. For both neuropathic pain and DPN, it was difficult to ascertain whether a true assessment of efficacy at maximal tolerated dose had been carried out. Reviews had been carried out but not systematically. 5
6 Pregabalin for generalised anxiety disorder (GAD) In January 2011 NICE published guidance for the management of generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults in primary, secondary and community care CG The guidance recommends offering drug treatment or a high-intensity psychological intervention for patients with GAD and marked functional impairment or those whose symptoms have not responded adequately to step 2 psychological interventions. If a patient chooses drug treatment a selective serotonin reuptake inhibitor (SSRI) should be used first-line and although it does not have a UK marketing authorisation NICE recommends sertraline as a cost-effective choice. The guidance goes on to state that if sertraline is ineffective offer an alternative SSRI or a serotonin noradrenaline reuptake inhibitor (SNRI). If the person cannot tolerate SSRIs or SNRIs then pregabalin could be considered. Of the 720 patients prescribed pregabalin for generalised anxiety disorder 32% were initiated by the GP, 67% initiated by secondary care and 1% unknown due to limited documentation recorded. 16% of patients initiated by the GP were prescribed in line with the local guidance compared with 38% of those initiated in secondary care with the remainder having no documentation of having being prescribed an SSRI or an SNRI previously although very few patients had neither before being initiated on pregabalin. Audit Summary Sheet (Part 2) (Comments) Within the review Practices were asked to: identify anything that they could do to improve pregabalin prescribing in neuropathic pain and generalised anxiety disorder; explain how the audit data will be discussed and relevant changes to practice taken forward. Of the 84 Practices who returned the completed summary results are as follows: 1. Is there anything that the practice has identified that they can do to improve prescribing in this area? No of practices Adhere to NICE / ABHB Guidelines 46 Dose optimise from TDS to BD 36 Consider using LANSS pain assessment tool 7 Issue on acute prescriptions only 4 Medication reviews for Pregabalin patients 25 Stop prescribing for anxiety disorder 3 Lack of information from Secondary Care pain clinics as to why Gabapentin is not used first line (More information required from Secondary Care) 3 6
7 Poor information from Mental Health clinics as to why SSRis and SNRIs are unsuitable for anxiety disorders (More information required from Secondary Care) Pregabalin added without tricyclic being stopped. No documented reason for the concomitant therapies. Would like Health Board to query with Secondary Care on behalf of practice). Use specific directions not as directed 1 Inform new GPs of audit results and Guidance 1 Carry out 4 weeks assessment on new patients 14 Re-audit in 12 months 5 Improve documentation on PMR 5 Contact Secondary Care where ABHB guidance has not been adhered to 1 Patient education on use of drug Individual GPs given list of patients where prescribing was not in accordance with guidelines for review and reflection Would like enhanced service with shared care protocol for monitoring Secondary Care prescribing 2 1 Discuss guidelines within the practice 1 Alerts added to PMR to discuss pregabalin 2 Stop initiation of Pregabalin 1 Switch Pregabalin patients to Gabapentin 3 Attempt to switch new patients initiated in Secondary Care from Pregabalin to Gabapentin 1 2. How will this information be discussed with all relevant members of the practice team and any relevant changes to practice taken forward? No of practices Discuss at practice meeting 77 Distribute copy of audit results to all partners 12 Agree pain management strategy 1 Formulary adjustments (dosage defaults) 1 ABHB / NICE Guidance to all clinicians 23 ABHB prescribing support team to assist in dose optimisation 2 Template made with guidelines for all doctors 1 Practice to arrange local pain specialist to talk at clinical meeting 1 Acknowledgements to GP practice staff and Medicines Management Technicians for their help and support in carrying out this audit. 7
8 References: DTB 2010;48:61 doi: /dtb HTA Report 05/30/03 - The Efficacy and Cost-Effectiveness of Different Treatment Pathways for Neuropathic Pain: systematic review and economic modelling of postherpetic neuralgia and painful diabetic neuropathy 4. ABHBsept2010.pdf 5. opathic_pain_drug_treatment/management 6. MDLetterSept10.pdf 7. Lyric a_/pregabalin Lyrica_
9 Appendix 1 Review of Pregabalin Prescribing in Primary Care Aim The objective of this review is to measure current prescribing of Pregabalin for neuropathic pain and generalised anxiety disorder against the Aneurin Bevan Health Board (ABHB) Guidelines for the diagnosis and management of Neuropathic Pain, ABHB guidelines for Diabetic Peripheral Neuropathic Pain and the National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 113: Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults. Process Run a search to identify all patients over 18 years who have been prescribed Pregabalin or Lyrica in the last 6 months. Exclude those patients with a read code for Epilepsy (F25%) Collect data for patients prescribed Pregabalin for neuropathic pain on data collection sheet (appendix A) Collect data for patients prescribed Pregabalin for diabetic peripheral neuropathic pain on data collection sheet (appendix B) Collect data for patients prescribed Pregabalin for generalised anxiety disorder on data collection sheet (appendix C) Complete the audit summary table (appendix D) The practice should submit a copy of the audit summary sheet to the locality Prescribing Advisor, as evidence of completion by 31st December Dose Optimisation ABHB has a standard operating procedure for changing pregabalin TDS dose regimes to BD regimes when prescribed for neuropathic pain or generalised anxiety disorder This is a separate cost saving scheme which may have already been implemented in your practice with support from the locality prescribing teams Following data collection if patients are identified with a TDS regime and have not previously been offered a BD regime please contact your locality prescribing team for support with the switch. 9
10 Rationale for Audit ABHB spent 2.7 million on pregabalin in primary and secondary care during 2011, an increase of 25% compared to 2010, Although the trend in pregabalin prescribing has increased across all of the Welsh Health Localities, ABHB has the highest cost per 1000 patients in Wales and is 37% greater than the Welsh national average. Pregabalin for Neuropathic Pain In March 2010 NICE published guidance for the pharmacological management of neuropathic pain CG96 1 specifying pregabalin as one of the first-line treatment options. However in June 2010 the Drug and Therapeutics Bulletin 2 published an article questioning the validity of this recommendation stating that gabapentin was excluded as a treatment option based on indirect comparisons suggesting that, in relation to pregabalin, it offers less net benefit, is less costeffective and requires more complex dosing and titration. Furthermore there were concerns over the economic modelling, on which CG96 was based to conclude that pregabalin was more costeffective than gabapentin. It has been suggested that the drug costs used in the Health Technology Assessment (HTA) 3 were based exclusively on gabapentin generic tablets rather than the less expensive generic capsules and the costs of pregabalin assumed twice daily (rather than the more costly three times daily) dosing. As a result of this in July 2011, NICE in collaboration with the HTA group were due to publish a review of the economic modelling but have recently announced the clinical guideline will now be fully revised in order to address ongoing uncertainties of cost effectiveness of some of the recommended treatment options. In September 2010 the Gwent Partnership Medicines and Therapeutics Committee discussed local implementation of NICE CG96 and based on the concerns above produced interim local guidance for the pharmacological management of neuropathic pain in a non-specialist setting 4 which reflects the current recommendations from the NHS Clinical Knowledge Summaries 5. (Reproduced overleaf). This was supported by a letter to all prescribers in September 2010 from the Medical Director and the GPMTC chair 6. The Scottish Medicines Consortium has also restricted pregabalin for the treatment of peripheral neuropathic pain in adults to patients who have not achieved adequate pain relief from, or have not tolerated, conventional first and second line treatments for peripheral neuropathic pain. There is also a recommendation that treatment should be stopped if the patient has not shown sufficient 10
11 benefit within 8 weeks of reaching the maximally tolerated therapeutic dose. 7 Diabetic Peripheral Neuropathic pain NICE CG96 1 for the pharmacological management of neuropathic pain in adults recommends duloxetine as first line treatment for people with painful diabetic neuropathy with pregabalin and amitriptyline recommended as second line treatment options. However due to the concerns regarding the exclusion of gabapentin mentioned above, ABHB have produced local guidance 8 which includes gabapentin and places pregabalin as a 4 th line treatment option. The increased level of pregabalin prescribing within ABHB seems to suggest that local guidance is not being followed. A review of prescribing will establish if this is the case. Recognising and Treating Neuropathic Pain in Primary and Secondary Care The LANSS Scoring Tool should be used to assist diagnosis and hence make a decision whether a treatment for neuropathic pain should be initiated. 11
12 RECOGNISING AND TREATING NEUROPATHIC PAIN IN PRIMARY & SECONDARY CARE SIGNS AND SYMPTOMS Can be spontaneous, continuous, intermittent, superficial or evoked Pain will often be described as burning, sharp, shooting, lanciating, itching, pins and needles, indescribable in terms of normal reference (patients often get distressed as they are not voice their pain in a way that they think is normal and are therefore worried they will not be believed). Can be made worse by temperature, or touch USE OF LANSS SCORING TOOL TO ASSIST DIAGNOSIS 1. Do you have pins and needles / numbness / tingling? 2. Does painful area change colour? 3. Does skin in painful area feel sensitive to touch? 4. Do you get feelings like an electric shock? 5. Do you get a feeling of burning where the pain is? 1. Test with cotton wool for allodynia 2. Is there an altered sensation to a needle prick? Yes (5) No (0) Yes (5) No (0) Yes (3) No (0) Yes (2) No (0) Yes (1) No (0) Yes (5) No (0) Yes (3) No (0) Total score < 12 = neuropathic pain unlikely. > 12 = likely neuropathic pain. USE OF PHARMACOLOGICAL AGENTS FOR NEUROPATHIC PAIN ONLY IF LANSS SCORE > 12 NON FOCAL NEUROPATHIC PAIN DIABETIC PERIPHERAL NEURALGIA FOCAL NEUROPATHIC PAIN AMITRIPTYLINE GABAPENTIN capsules PREGABALIN IF NO BENEFIT REFER FOR PAIN CLINIC REVIEW DULOXETINE NB: Consider CARBAMAZEPINE for trigeminal neuralgia CAPSAICIN cream 0.075% (Axsain) LIDOCAINE PLASTER (Versatis ) Post Herpetic Neuralgia ONLY Other off label uses should be initiated by ABHB Pain Clinic GPs may initiate as rescue analgesic (while waiting for a referral to Pain Clinic) in a very small subgroup of people with localised pain who are unable to take oral medication because of medical conditions and/or disability ANY VARIATION FROM THIS FLOWCHART REQUIRES THE REASON(S) TO BE CLEARLY DOCUMENTED IN THE PATIENT NOTES AND COMMUNICATED WHERE APPROPRIATE Full guidance with dose regimes can be found at: ABHBsept2010.pdf RevisedALOGORITHM%5B21June2011%5D.pdf 12
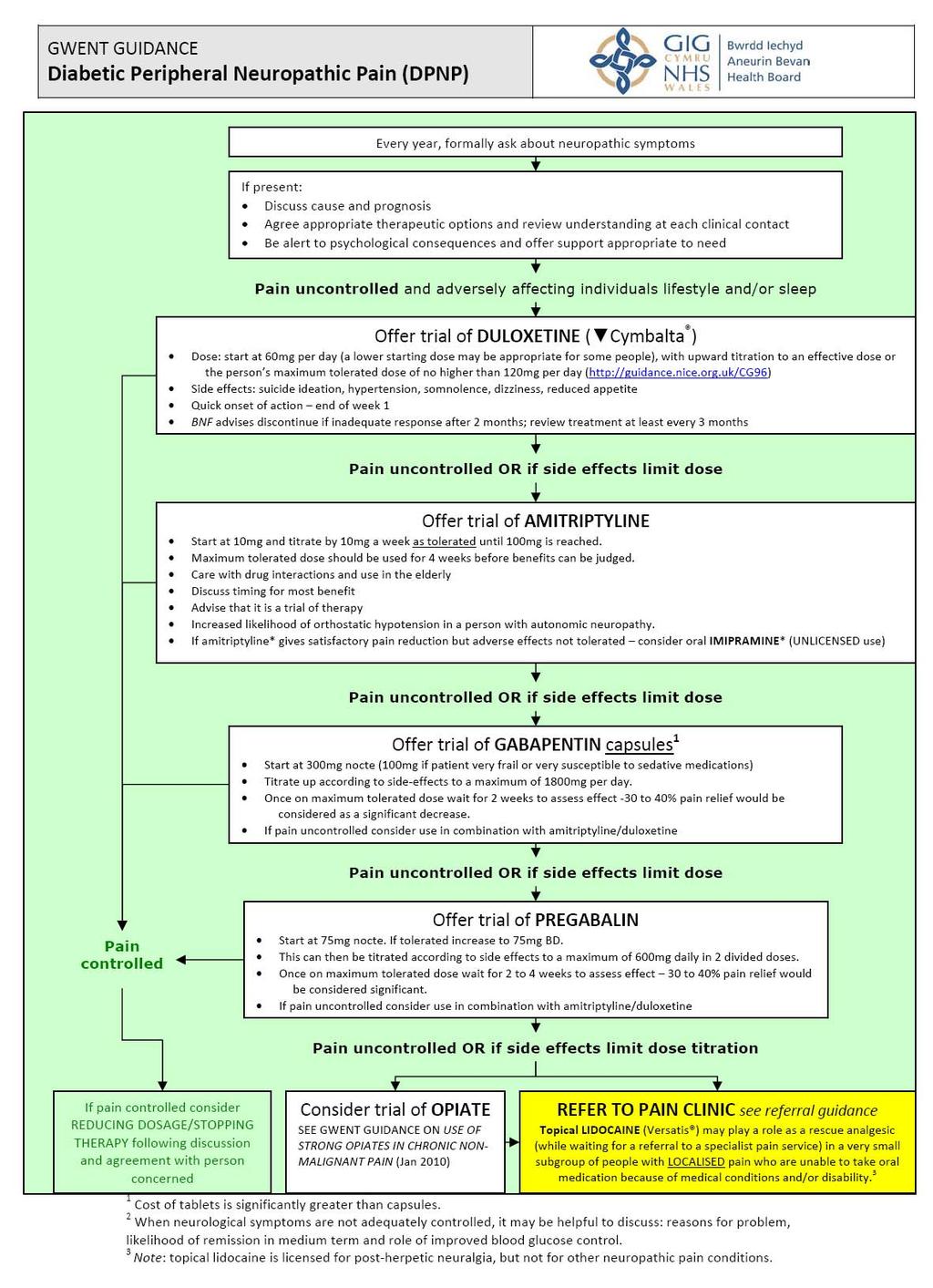
13 NON FOCAL NEUROPATHIC PAIN FOCAL NEUROPATHIC PAIN AMITRIPTYLINE * start at 10mg and titrate by 10mg a week until 75mg daily (in divided doses or as a single dose at bedtime) is reached. Maximum tolerated dose should be used for 4 weeks before benefits can be judged. Care with drug interactions and use in the elderly If satisfactory improvement continue the treatment; improvement sustained consider reducing dose If amitriptyline* gives satisfactory pain reduction but adverse effects not tolerated consider oral imipramine* STOP IF NO BENEFIT slowly over 4 weeks CAPSAICIN cream 0.075% (Axsain) GABAPENTIN capsules start at 300mg nocte (100mg if patient very frail or very susceptible to sedative medications).titrate up according to side effects to a maximum of 1800mg per day. Once on maximum tolerated dose wait for 2 weeks to assess effect 30 to 40% pain relief would be considered as a significant decrease. IF NO BENEFIT LIDOCAINE PLASTER (Versatis ) licensed for post herpetic neuralgia used 12 hours on and 12 hours off Can be cut to cover area (possibly allowing more economic use) No more than 3 patches should be applied an any one time Do not use on broken skin One month trial required before assessing efficacy NB: Consider CARBAMAZEPINE for trigeminal neuralgia IF NO BENEFIT or NOT TOLERATED (due to adverse effects or difficulty adhering to dosage schedule) PREGABALIN start at 75mg nocte. If tolerated increase to 75mg BD. This can then be titrated according to side effects to a maximum of 600mg daily in two divided doses. Once on maximum tolerated dose wait for 2 to 4 weeks to assess effect 30 to 40% pain relief would be considered significant. IF NO BENEFIT REFER FOR PAIN CLINIC REVIEW Topical lidocaine (Versatis ) may play a role as a rescue analgesic (while waiting for a referral to a specialist pain service) in a very small subgroup of people with localised pain who are unable to take oral medication *In these recommendations, drug names are marked with an asterisk if they do not have UK marketing authorisation for the indication in question. Informed consent should be obtained and documented. 13
14 14
15 Pregabalin for generalised anxiety disorder (GAD) In January 2011 NICE published guidance for the management of generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults in primary, secondary and community care CG The guidance recommends offering drug treatment or a high-intensity psychological intervention for patients with GAD and marked functional impairment or those whose symptoms have not responded adequately to step 2 psychological interventions. If a patient chooses drug treatment a selective serotonin reuptake inhibitor (SSRI) should be used first-line and although it does not have a UK marketing authorisation NICE recommends sertraline as a cost-effective choice. The guidance goes on to state that if sertraline is ineffective offer an alternative SSRI or a serotonin noradrenaline reuptake inhibitor (SNRI). If the person cannot tolerate SSRIs or SNRIs then pregabalin could be considered. ABHB guidance for drug treatment of GAD is reproduced on the following pages. Anecdotally GPs have seen an increase in pregabalin prescribing requests for GAD from secondary care. A review of prescribing will establish if prescribing is compliant with current guidance. 15
16 GWENT GUIDANCE (BASED ON NICE CG113 Drug Treatment for Generalised Anxiety Disorder (GAD) If a person with GAD chooses drug treatment Discuss the treatment options and any concerns the person with GAD has about taking medication. Explain fully the reasons for prescribing and provide written and verbal information on: the likely benefits of different treatments the gradual development, over 1 week or more, of the full anxiolytic effect importance of taking medication as prescribed and the need to continue treatment after remission to avoid relapse differences in drug side effect, withdrawal syndrome and drug interaction profiles the risk of activation with SSRIs and SNRIs, with symptoms such as increased anxiety, agitation and problems sleeping BENZODIAZEPINES SHOULD ONLY BE USED AS A SHORT TERM MEASURE (10 TO 14 DAYS) DURING CRISES. DO NOT OFFER AN ANTIPSYCHOTIC FOR THE TREATMENT OF GAD IN PRIMARY CARE Offer trial of SSRI (see ABHB options below) Note increased risk of bleeding in elderly and those on NSAIDs/aspirin consider a gastro protective drug. Advise those <30yrs of age of risks of suicidal ideation and self harm monitor weekly for first month. Review the effectiveness and side effects every 2 to 4 weeks during the first 3 months of treatment and every 3 months thereafter. If effective advise the person to continue for at least 1 year to avoid relapse. SSRI INEFFECTIVE SSRI NOT TOLERATED Offer trial of alternate SSRI (see ABHB options on page 2 Offer trial of SNRI (see ABHB options on page 2) Provide information and consider one of the following strategies: monitoring the person s symptoms closely (if the side effects are mild and acceptable to the person) OR reducing the dose of the drug OR stopping the drug and, according to the person s preference, offering either an alternative DRUG OR a high intensity psychological intervention m/r venlafaxine INAPPROPRIATE, INEFFECTIVE or NOT TOLERATED Consider trial of PREGABALIN initially 150mg daily in 2 divided doses, increased if necessary at 7 day intervals in steps of 150mg daily; max. 600mg daily in 2 divided doses Pregabalin INEFFECTIVE or NOT TOLERATED Consider SPECIALIST REFERRAL if the person with GAD has severe anxiety with marked functional impairment in conjunction with: a risk of self harm or suicide OR significant comorbidity, such as substance misuse, personality disorder or complex physical health problems OR self neglect OR an inadequate response to the drug pathway above. 16
17 SSRIs in ABHB Formulary SERTRALINE Licensed status for GAD OFF LABEL obtain & document informed consent CITALOPRAM OFF LABEL obtain & document informed consent. FLUOXETINE OFF LABEL obtain & document informed consent. Dose in adults over 18 years Initially 25mg daily increased after 1 week to 50mg daily; if response is partial and if drug tolerated, dose increased in steps of 50mg at intervals of at least 1 week to max. 200mg daily. Initially 10mg once daily increased gradually if necessary in steps of 10mg daily, usual dose 20 30mg once daily; max. 40mg once daily (20mg once daily in the elderly) Initially 20mg daily, increased after 3 4 weeks if necessary, and at appropriate intervals thereafter; max 60mg daily (elderly usual max 40mg) PAROXETINE LICENSED CSM advise that the recommended dose for GAD is 20mg daily. There is no evidence that a higher dose is more effective. SNRIs in ABHB Formulary VENLAFAXINE 28 day cost (Oct 2011) 50mg mg mg mg mg 1.74 GAD License Dose 28 day cost (Oct 2011) Only M/R capsules (XL) LICENSED for moderate to severe GAD. 75mg once daily, increased if necessary at intervals of at least 2 weeks. Discontinue if no response after 8 weeks; max 225mg once daily. DULOXETINE LICENSED Initially 30mg once daily, increased if necessary to 60mg once daily; max 120mg daily. 75mg M/R mg M/R mg mg Comment Recommended by NICE as the SSRI to try first as it had the lowest probability of discontinuation due to side effects and the second highest in terms of achieving a conditional response (among the drugs considered by NICE). Licensed for depressive illness, OCD, Panic disorder, PTSD and social anxiety disorder. Caution advised in patients susceptible to QTinterval prolongation. Licensed for depressive illness and Panic disorder. Long duration of action due to long half life. Treatment break of 2 weeks recommended if switching from fluoxetine to another SSRI. Licensed for major depression & OCD. Associated with a withdrawal syndrome, gradual dose reduction is advised on cessation of treatment. Also licensed for major depression, OCD, Panic disorder, Social anxiety disorder & PTSD. Comment Caution advised in patients with heart disease. Associated with a withdrawal syndrome, gradual dose reduction is advised on cessation of treatment. Also licensed for major depression. 17
18 References: DTB 2010;48:61 doi: /dtb HTA Report 05/30/03 - The Efficacy and Cost-Effectiveness of Different Treatment Pathways for Neuropathic Pain: systematic review and economic modelling of post-herpetic neuralgia and painful diabetic neuropathy nt/management Lyrica_/pregabalin Lyrica_
19 Appendix A: Data collection sheet Pregabalin for Neuropathic Pain Patient ID Strength & Dose Initiated by GP 2nd ry care TDS dose which could be switched to BD Previously tried or is currently prescribed Previously tried Gabapentin Efficacy Reviewed after 4 weeks of max Pregabalin prescribed in line with (Exclude patients who Amitriptyline tolerated dose? ABHB have previously been Neuropathic offered this switch and declined Read code Pain Guideline 8B30) Yes No Yes No Yes No Yes No Yes No 19
20 Appendix B: Data collection sheet Pregabalin for Diabetic Neuropathic Pain Patient ID Strength & Dose Initiated by GP 2nd ry care TDS dose which could be switched to BD Previously tried or is currently prescribed Previously tried Gabapentin Efficacy Reviewed after 4 weeks at max Pregabalin prescribed in line with (Exclude patients who Duloxetine tolerated dose? ABHB have previously been Neuropathic offered this switch and declined Read code Pain Guideline 8B30) Yes No Yes No Yes No Yes No Yes No 20
21 Appendix C: Data collection sheet Pregabalin for Generalised Anxiety Disorder Patient ID Strength & Dose Initiated by GP 2nd ry care TDS dose which could be switched to BD Previously tried SSRI Previously tried SNRI Documented reason for not prescribing Pregabalin prescribed in line with NICE (Exclude patients who SSRI / SNRI Guideline have previously been (if no previous CG113 offered this switch and declined Read code trial) 8B30) Yes No Yes No Yes No Yes No 21
22 Appendix D: Audit Summary Sheet (Part 1) Review of Pregabalin in neuropathic pain and generalised anxiety disorder Practice Name Date of data collection No. Patients % of Patients Pregabalin for Neuropathic Pain Number of patients reviewed Number of patients with TDS dose which could be switched to BD dose Number initiated by GP Number initiated by secondary care (SC) Number where prescribing is line with ABHB guidance Number where pregabalin used before other recommended treatments Number where pregabalin has not been assessed after 4 weeks of max tolerated dose GP SC GP SC Pregabalin for Diabetic Neuropathic Pain Number of patients reviewed Number of patients with TDS dose which could be switched to BD dose Number initiated by GP Number initiated by secondary care (SC) Number where prescribing is line with ABHB guidance Number where pregabalin used before other recommended treatments Number where pregabalin has not been assessed after 4 weeks of max tolerated dose GP SC GP SC 22
23 Pregabalin for generalised anxiety disorder Number of patients reviewed Number of patients with TDS dose which could be switched to BD dose Number initiated by GP Number initiated by secondary care (SC) Number of patients where pregabalin has been initiated in line with NICE CG 113 Number of patients where pregabalin has been used before other recommended treatments and no reason provided GP SC GP SC Submit a copy of audit summary sheet part 1 and 2 to the locality pharmacy team by 31 st December
24 Appendix D: Audit Summary Sheet (Part 2) 1. Is there anything that the practice has identified that they can do to improve prescribing in this area? (Please specify below) 2. How will this information be discussed with all relevant members of the practice team and any relevant changes to practice taken forward? (Please specify below) Practice: Date: Signed: Designation: 24
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
Step 3: GAD with marked functional impairment or that has not improved after step 2 interventionsentions bring together everything NICE says on a topic in an interactive flowchart. are interactive and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
Document Title Pharmacological Management of Generalised Anxiety Disorder
 Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Document Title Pharmacological Management of Generalised Anxiety Disorder Document Description Document Type Policy Service Application Trust Wide Version 1.1 Policy Reference no. POL 201 Lead Author(s)
Volume 9; Number 3 March 2015 PRESCRIBING AND DISPENSING PREGABALIN FOR NEUROPATHIC PAIN
 Arden and Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and
Arden and Greater East Midlands Commissioning Support Unit in association with Lincolnshire Clinical Commissioning Groups, Lincolnshire Community Health Services, United Lincolnshire Hospitals Trust and
Neuropathic pain MID ESSEX LOCALITY
 Neuropathic pain Neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory nervous system. A. Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) i Read questions to
Neuropathic pain Neuropathic pain is defined as pain caused by a lesion or disease of the somatosensory nervous system. A. Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) i Read questions to
7 th November % of patients had lidocaine plasters prescribed for the licensed indication of post herpatic neuralgia
 Directorate of Integrated Care Health and Social Care Board 12-22 Linenhall Street Belfast BT2 8BS Tel : 028 90553782 Fax : 028 90553622 Web Site: www.hscboard.hscni.net 7 th November 2013 Dear colleague
Directorate of Integrated Care Health and Social Care Board 12-22 Linenhall Street Belfast BT2 8BS Tel : 028 90553782 Fax : 028 90553622 Web Site: www.hscboard.hscni.net 7 th November 2013 Dear colleague
Scottish Medicines Consortium
 Scottish Medicines Consortium duloxetine 30mg and 60mg capsules (Cymbalta ) No. (285/06) Eli Lilly and Company Limited/Boehringer Ingelheim 4 August 2006 The Scottish Medicines Consortium has completed
Scottish Medicines Consortium duloxetine 30mg and 60mg capsules (Cymbalta ) No. (285/06) Eli Lilly and Company Limited/Boehringer Ingelheim 4 August 2006 The Scottish Medicines Consortium has completed
Practice Name. Audit Undertaken By and Job Title. Date of Audit
 Pregabalin Audit Template This template can be used to document the Pregabalin audit undertaken by practices as part of the Incentive Scheme. It has been produced to provide practices with a guide but
Pregabalin Audit Template This template can be used to document the Pregabalin audit undertaken by practices as part of the Incentive Scheme. It has been produced to provide practices with a guide but
Advice following an Independent Review Panel (IRP)
") Scottish Medicines Consortium Advice following an Independent Review Panel (IRP) Pregabalin 25, 50, 75, 100, 150, 200 and 300mg capsules (Lyrica ) Pfizer No. 157/05 7 July 2006 The Scottish Medicines Consortium
Scottish Medicines Consortium Advice following an Independent Review Panel (IRP) Pregabalin 25, 50, 75, 100, 150, 200 and 300mg capsules (Lyrica ) Pfizer No. 157/05 7 July 2006 The Scottish Medicines Consortium
Primary care review of Tramadol Prescribing
 Primary care review of Tramadol Prescribing Aim of the Audit To ensure the prescribing of tramadol is safe, appropriate and regularly reviewed, in line with local chronic pain guidelines 1 Background Tramadol
Primary care review of Tramadol Prescribing Aim of the Audit To ensure the prescribing of tramadol is safe, appropriate and regularly reviewed, in line with local chronic pain guidelines 1 Background Tramadol
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP
 GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
GREATER MANCHESTER INTERFACE PRESCRIBING GROUP On behalf of the GREATER MANCHESTER MEDICINES MANAGEMENT GROUP SHARED CARE GUIDELINE FOR THE PRESCRIBING OF SELECTIVE SEROTONIN REUPTAKE INHIBITORS (SSRIs)
Volume 4; Number 5 May 2010
 Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Volume 4; Number 5 May 2010 CLINICAL GUIDELINES FOR ANTIDEPRESSANT USE IN PRIMARY AND SECONDARY CARE Lincolnshire Partnership Foundation Trust in conjunction with Lincolnshire PACEF have recently updated
Gateshead Pain Guidelines for Chronic Conditions
 Gateshead Pain Guidelines for Chronic Conditions Effective Date: 13.2.2013 Review Date: 13.2.2015 Gateshead Pain Guidelines: Contents PAIN GUIDELINES Chronic Non-Malignant Pain 5 Musculoskeletal Pain 6
Gateshead Pain Guidelines for Chronic Conditions Effective Date: 13.2.2013 Review Date: 13.2.2015 Gateshead Pain Guidelines: Contents PAIN GUIDELINES Chronic Non-Malignant Pain 5 Musculoskeletal Pain 6
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update 1 Guideline title Anxiety: management of generalised anxiety disorder in adults in primary, secondary and community care (update)
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Scope for Partial Update 1 Guideline title Anxiety: management of generalised anxiety disorder in adults in primary, secondary and community care (update)
Scottish Medicines Consortium
 Scottish Medicines Consortium escitalopram, 5mg, 10mg, and 20mg tablets and 10mg/ml oral drops (Cipralex) No. (406/07) Lundbeck Ltd 7 September 2007 The Scottish Medicines Consortium has completed its
Scottish Medicines Consortium escitalopram, 5mg, 10mg, and 20mg tablets and 10mg/ml oral drops (Cipralex) No. (406/07) Lundbeck Ltd 7 September 2007 The Scottish Medicines Consortium has completed its
Pain CONCERN. Medicines for long-term pain. Antidepressants
 Pain CONCERN Medicines for long-term pain Antidepressants Many people living with long-term pain (also known as chronic or persistent pain) are worried about using medicines like antidepressants. They
Pain CONCERN Medicines for long-term pain Antidepressants Many people living with long-term pain (also known as chronic or persistent pain) are worried about using medicines like antidepressants. They
Benzodiazepines and Hypnotics
 Benzodiazepines and Hypnotics Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date):
Benzodiazepines and Hypnotics Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out of date):
Appendix C - Summary form
 National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
National Institute for Health and Clinical Excellence Appendix C - Summary form Single Techn Appraisal (STA) Agomelatine for the treatment of major depressive episodes Response to consultee and commentator
Switching Tramacet to paracetamol alone or paracetamol and codeine
 Bulletin 62 February 2014 Community Interest Company Switching Tramacet to paracetamol alone or paracetamol and codeine This is one of a number of bulletins providing further information on medicines contained
Bulletin 62 February 2014 Community Interest Company Switching Tramacet to paracetamol alone or paracetamol and codeine This is one of a number of bulletins providing further information on medicines contained
A new model for prescribing varenicline
 Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Persistent Pain in Secure Environments Health and Justice Pharmacy Network Meeting Tuesday 18 March 2014
 Persistent Pain in Secure Environments Health and Justice Pharmacy Network Meeting Tuesday 18 March 2014 Dr Iain Brew Vice Chair RCGP SEG Health & Justice CRG Member Special Considerations General reluctance
Persistent Pain in Secure Environments Health and Justice Pharmacy Network Meeting Tuesday 18 March 2014 Dr Iain Brew Vice Chair RCGP SEG Health & Justice CRG Member Special Considerations General reluctance
Pregnancy. General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition)
") Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Pregnancy General Principles of Prescribing in Pregnancy (The Maudsley, 12 th Edition) In all women of child bearing potential Always discuss the possibility of pregnancy; half of all pregnancies are unplanned
Persistent Pain Resources. Ten Key Messages
 Persistent Pain Resources Ten Key Messages October 2016 This document has been prepared by a multiprofessional collaborative group, with support from the All Wales Prescribing Advisory Group (AWPAG) and
Persistent Pain Resources Ten Key Messages October 2016 This document has been prepared by a multiprofessional collaborative group, with support from the All Wales Prescribing Advisory Group (AWPAG) and
Management of neuropathic pain (non-malignant) Medicines Initiation Protocol
 Medicines Initiation Protocol") Introduction Management of neuropathic pain (non-malignant) Medicines Initiation Protocol Pain is one of the most common reasons that patients present to Primary Care It is known that there are widespread
Introduction Management of neuropathic pain (non-malignant) Medicines Initiation Protocol Pain is one of the most common reasons that patients present to Primary Care It is known that there are widespread
MMG004 GUIDELINES FOR THE USE OF HIGH DOSE VENLAFAXINE AND THE COMBINATION OF VENLAFAXINE AND MIRTAZAPINE IN THE TREATMENT OF DEPRESSION
 MMG004 GUIDELINES FOR THE USE OF HIGH DOSE VENLAFAXINE AND THE COMBINATION OF VENLAFAXINE AND MIRTAZAPINE IN THE TREATMENT OF DEPRESSION Page 1 of 13 Table of Contents Why we need this Guideline... 3 What
MMG004 GUIDELINES FOR THE USE OF HIGH DOSE VENLAFAXINE AND THE COMBINATION OF VENLAFAXINE AND MIRTAZAPINE IN THE TREATMENT OF DEPRESSION Page 1 of 13 Table of Contents Why we need this Guideline... 3 What
Pain Management Documents
 Pain Management Documents Prescriber and Patient Resources Non-cancer Pain Guidance Neuropathic Pain Guidance Stopping or Switching low strength Buprenorphine Patches Red and Yellow Flags Medicines Management
Pain Management Documents Prescriber and Patient Resources Non-cancer Pain Guidance Neuropathic Pain Guidance Stopping or Switching low strength Buprenorphine Patches Red and Yellow Flags Medicines Management
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over)
") Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
Appendix 4B - Guidance for the use of Pharmacological Agents for the Treatment of Depression in Adults (18 years and over) Introduction / Background Treatment comes after diagnosis Diagnosis is based on
requesting information regarding prescribing incentive schemes in Canterbury and Coastal Clinical Commissioning Group
 requesting information regarding prescribing incentive schemes in Canterbury and Coastal Clinical Commissioning Group Canterbury and Coastal Clinical Consortium Group Medicine Management plans 2013/14
requesting information regarding prescribing incentive schemes in Canterbury and Coastal Clinical Commissioning Group Canterbury and Coastal Clinical Consortium Group Medicine Management plans 2013/14
Other classical forms of neuropathic pain include diabetic peripheral neuropathy, trigeminal neuralgia and postherpetic
 Guideline Name: Neuropathic Pain Neuropathic pain is defined by the International Association for the Study of Pain, Neuropathic Special Interest group as pain arising as a direct consequence of a lesion
Guideline Name: Neuropathic Pain Neuropathic pain is defined by the International Association for the Study of Pain, Neuropathic Special Interest group as pain arising as a direct consequence of a lesion
Job Title Name Signature Date. Director of Nursing Angela Wallace Signed Angela Wallace 30/6/2014
 PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE (CHAMPIX ) BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN FORTH VALLEY Protocol Number 445 Version 1 Date protocol prepared: June 2014 Date protocol due
PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE (CHAMPIX ) BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN FORTH VALLEY Protocol Number 445 Version 1 Date protocol prepared: June 2014 Date protocol due
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]
![SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]](/thumbs/80/80440271.jpg "SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA. [compatible with NICE guidance]") SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
SiGMA/ MMHSCT GUIDELINES FOR ANTIPSYCHOTIC DRUG TREATMENT OF SCHIZOPHRENIA [compatible with NICE guidance] Medicines Management Committee August 2002 For review August 2003 Rationale The SiGMA algorithm
Scottish Medicines Consortium
 Scottish Medicines Consortium pregabalin, 25mg, 50mg, 75mg, 100mg, 150mg, 200mg, 225mg, 300mg capsules (Lyrica ) No. (389/07) Pfizer Limited 6 July 2007 The Scottish Medicines Consortium has completed
Scottish Medicines Consortium pregabalin, 25mg, 50mg, 75mg, 100mg, 150mg, 200mg, 225mg, 300mg capsules (Lyrica ) No. (389/07) Pfizer Limited 6 July 2007 The Scottish Medicines Consortium has completed
Costing statement. Implementing NICE guidance. January NICE clinical guideline 137
 The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care (partial update of NICE clinical guideline 20) Costing statement Implementing NICE guidance
The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care (partial update of NICE clinical guideline 20) Costing statement Implementing NICE guidance
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE. Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust
 Mersey Care NHS Trust") PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
PSYCHIATRIC MANAGEMENT IN PRIMARY CARE Dr Fayyaz Khan MBBS, MRCPsych, MSc Consultant Psychiatrist (Locum) Mersey Care NHS Trust Areas to cover Mood Disorders Anxiety Disorders Miscellaneous Conditions
Depression: selective serotonin reuptake inhibitors
 Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Depression: selective serotonin reuptake inhibitors Selective serotonin reuptake inhibitors (SSRIs) are considered first-line treatment for the majority of patients with depression. citalopram and fluoxetine
Anxiety Disorders: First aid and when to refer on
 Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Anxiety Disorders: First aid and when to refer on Presenter: Dr Roger Singh, Consultant Psychiatrist, ABT service, Hillingdon Educational resources from NICE, 2011 NICE clinical guideline 113 What is anxiety?
Neuropathic pain (pain due to nerve damage)
") Neuropathic pain (pain due to nerve damage) Clinical Guideline Pain can be nociceptive, neuropathic or mixed. The neuropathic component of pain generally responds poorly to conventional analgesics. Consider
Neuropathic pain (pain due to nerve damage) Clinical Guideline Pain can be nociceptive, neuropathic or mixed. The neuropathic component of pain generally responds poorly to conventional analgesics. Consider
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine
 -Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
-Guidelines for the discontinuation of oral antipsychotics in patients with BPSD within the primary care setting Summary- Quetiapine An independent report Time for action 1 by Professor Sube Banerjee looked
PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE (CHAMPIX ) BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN TAYSIDE
 BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN TAYSIDE") PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE (CHAMPIX ) BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN TAYSIDE GENERAL POLICY 2 PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE 4 STANDING ORDER
PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE (CHAMPIX ) BY AUTHORISED COMMUNITY PHARMACISTS WORKING IN TAYSIDE GENERAL POLICY 2 PATIENT GROUP DIRECTIONS FOR SUPPLY OF VARENICLINE 4 STANDING ORDER
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Guideline scope Persistent pain: assessment and management
 National Institute for Health and Clinical Excellence [document type for example, IFP, QRG] on [topic] Document cover sheet Date Version number Editor 30/08/2017 1 NGC Action 1 2 3 4 5 6 7 8 9 10 11 12
National Institute for Health and Clinical Excellence [document type for example, IFP, QRG] on [topic] Document cover sheet Date Version number Editor 30/08/2017 1 NGC Action 1 2 3 4 5 6 7 8 9 10 11 12
Product Cost per Pack Cost per 28 days (assuming 2 sprays od) Flixonase years 50mcg in both nostrils od (increasing to max bd prn)
 Flixonase years 50mcg in both nostrils od (increasing to max bd prn)") Protocol for Flixonase to Avamys Nasal Spray Switch May 2010 1. Reason Avamys contains the corticosteroid fluticasone furoate (27.5mcg/spray) and Flixonase nasal spray contains fluticasone propionate (50mcg/spray).
Protocol for Flixonase to Avamys Nasal Spray Switch May 2010 1. Reason Avamys contains the corticosteroid fluticasone furoate (27.5mcg/spray) and Flixonase nasal spray contains fluticasone propionate (50mcg/spray).
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014)
") Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 3 October 2014) Date of Preparation: September 2014 Date for next full
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
PRIMARY MANAGEMENT OF DRUG PRESCRIBING IN NON-MALIGNANT PAIN
 NORTH OF TYNE GUIDELINES FOR: PRIMARY MANAGEMENT OF DRUG PRESCRIBING IN NON-MALIGNANT PAIN (EXCLUDING DETAILED RECOMMENDATIONS FOR LONG TERM STRONG OPIATES) February 2015 (minor update April 2017) 1 CONTENTS
NORTH OF TYNE GUIDELINES FOR: PRIMARY MANAGEMENT OF DRUG PRESCRIBING IN NON-MALIGNANT PAIN (EXCLUDING DETAILED RECOMMENDATIONS FOR LONG TERM STRONG OPIATES) February 2015 (minor update April 2017) 1 CONTENTS
Antidepressant Selection in Primary Care
 Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Antidepressant Selection in Primary Care R E B E C C A D. L E W I S, D O O O A S U M M E R C M E B R A N S O N, M O 1 5 A U G U S T 2 0 1 5 Objectives Understand the epidemiology of depression. Recognize
Elements for a Public Summary
 VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Generalised anxiety disorder Generalised anxiety disorder (GAD) is an umbrella term that covers a wide range of anxiety disorders
VI.2 Elements for a Public Summary VI.2.1 Overview of disease epidemiology Generalised anxiety disorder Generalised anxiety disorder (GAD) is an umbrella term that covers a wide range of anxiety disorders
Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults
 Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults Ref: PHARM-0025-v3 Status: FINAL Document type: Guidelines Guidance on Safe Prescribing of Melatonin Page
Guidance on Safe Prescribing of Melatonin for Sleep Disorders in Children, Young People and Adults Ref: PHARM-0025-v3 Status: FINAL Document type: Guidelines Guidance on Safe Prescribing of Melatonin Page
for adults engaged with the Family Wellbeing Service Isle of Wight In Community Pharmacy for Isle of Wight Public Health Commissioned Services
 The supply of Champix (Varenicline) Tablets 500mcg and 1mg by registered community pharmacists for smoking cessation / management of nicotine withdrawal for adults engaged with the Family Wellbeing Service
The supply of Champix (Varenicline) Tablets 500mcg and 1mg by registered community pharmacists for smoking cessation / management of nicotine withdrawal for adults engaged with the Family Wellbeing Service
Patient Profile. Patient s details Initials: IF Age: 40 Gender: Male. Weight: 139.7kg Height: 510 metres BMI: >47
 Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Lidocaine 5% Medicated Plaster (Versatis )
") Medicines Management Programme Lidocaine 5% Medicated Plaster (Versatis ) Prescribing and Cost Guidance Table of Contents 1. Background... 2 2. Purpose... 2 3. Definitions... 3 4. Mode of action... 3 5.
Medicines Management Programme Lidocaine 5% Medicated Plaster (Versatis ) Prescribing and Cost Guidance Table of Contents 1. Background... 2 2. Purpose... 2 3. Definitions... 3 4. Mode of action... 3 5.
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
BOTULINUM TOXIN POLICY TO INCLUDE:
 BOTULINUM TOXIN POLICY TO INCLUDE: Blepharospasm in adults, Hemi facial spasm in adults, spasmodic torticollis (cervical dystonia), focal spasticity treatment of dynamic equinus foot deformity, focal spasticity
BOTULINUM TOXIN POLICY TO INCLUDE: Blepharospasm in adults, Hemi facial spasm in adults, spasmodic torticollis (cervical dystonia), focal spasticity treatment of dynamic equinus foot deformity, focal spasticity
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.
 Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Guidance on the use of Antidepressants for the Treatment of Unipolar Depression and Anxiety Spectrum Disorders in adults (Version 4.1 December 2018) Date of Preparation: January 2018 (with addition of
Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181)
") Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
Putting NICE guidance into practice Costing report: Lipid modification Implementing the NICE guideline on lipid modification (CG181) Published: July 2014 This costing report accompanies Lipid modification:
London Medicines Information Service
 London Medicines Information Service Extended-release methylphenidate a review of the pharmacokinetic profiles available March 2018 First authored by Martin Bradley (martin.bradley@gstt.nhs.uk) May 2016
London Medicines Information Service Extended-release methylphenidate a review of the pharmacokinetic profiles available March 2018 First authored by Martin Bradley (martin.bradley@gstt.nhs.uk) May 2016
FORMULARY UPDATES ABUHB s Drug Formulary is at:
 Aneurin Bevan University Health Board Medicines & Therapeutics Committee PRESCRIBING enewsletter archive at: http://www.wales.nhs.uk/sites3/page.cfm?orgid=814&pid=48407 Dear Gwent Prescriber At its last
Aneurin Bevan University Health Board Medicines & Therapeutics Committee PRESCRIBING enewsletter archive at: http://www.wales.nhs.uk/sites3/page.cfm?orgid=814&pid=48407 Dear Gwent Prescriber At its last
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90
 Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Depression in adults: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg90 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
CONCORD INTERNAL MEDICINE. Peripheral Neuropathy. April 22, 2012
 CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
CONCORD INTERNAL MEDICINE Peripheral Neuropathy Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD April 22, 2012 The information contained in this protocol should never
The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs
 The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs Author Version Date Consultation Date of Ratification By JPG Shaista Hussain Joint Formulary Pharmacist V2 16.09.2014 Homerton University
The Management of Overactive Bladder Syndrome with Antimuscarinic Drugs Author Version Date Consultation Date of Ratification By JPG Shaista Hussain Joint Formulary Pharmacist V2 16.09.2014 Homerton University
Managing Behavioural Problems in Patients with Learning Disabilities
 Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
Managing Behavioural Problems in Patients with Learning Disabilities Some people with a learning disability display behaviour that challenges. Although such behaviour is a challenge to services, family
Depression: management of depression in primary and secondary care
 Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
Issue date: December 2004, with amendments April 2007 Quick reference guide (amended) Depression: management of depression in primary and secondary care Amendment of recommendations concerning venlafaxine:
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017
 PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
PROCEDURE REF NO SABP/EXECUTIVE BOARD/0017 NAME OF GUIDELINE REASON FOR GUIDELINE WHAT THE GUIDELINE WILL ACHIEVE? WHO NEEDS TO KNOW ABOUT IT? Medicines Guideline: Hypnotic Medication Compliance with NICE
Common mental health disorders
 Common mental health disorders Identification and pathways to care Issued: May 2011 NICE clinical guideline 123 guidance.nice.org.uk/cg123 NICE has accredited the process used by the Centre for Clinical
Common mental health disorders Identification and pathways to care Issued: May 2011 NICE clinical guideline 123 guidance.nice.org.uk/cg123 NICE has accredited the process used by the Centre for Clinical
Initiation of Clozapine Treatment Community Patients
 Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
Initiation of Clozapine Treatment Community Patients Who Should Read This Policy Target Audience All clinical staff working in the community N/A N/A Initiation of Clozapine Treatment for Patients in the
DRAFT. Consultees are asked to consider and comment on the CEPP National Audit: Antipsychotics in Dementia document.
 Enclosure No: Agenda item No: Author: Contact: xx/xxxxx/xxxx0918 xx CEPP National Audit: Antipsychotics in Dementia All Wales Therapeutics and Toxicology Centre Tel: 02920 71 6900 awttc@wales.nhs.uk 1.0
Enclosure No: Agenda item No: Author: Contact: xx/xxxxx/xxxx0918 xx CEPP National Audit: Antipsychotics in Dementia All Wales Therapeutics and Toxicology Centre Tel: 02920 71 6900 awttc@wales.nhs.uk 1.0
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services
 Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services ANXIETY DISORDERS This guideline covers a range of anxiety disorders, including generalised anxiety disorder, social
Pharmacological treatment of anxiety disorders where is
 Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
Pharmacological treatment of anxiety disorders where is the room for improvement? David S Baldwin, Professor of Psychiatry BAP Masterclass, 15 th April 2011 dsb1@soton.ac.uk Declaration of interests (last
Guidelines on Choice and Selection of Antidepressants for the Management of Depression
 Guidelines on Choice and Selection of Antidepressants for the Management of Depression 1. Introduction This guidance should be considered as part of a stepped care approach in the management of depressive
Guidelines on Choice and Selection of Antidepressants for the Management of Depression 1. Introduction This guidance should be considered as part of a stepped care approach in the management of depressive
Capsaicin cutaneous patch
 New Medicines Profile August 2010 Issue. 10/03 cutaneous patch Concise evaluated information to support the managed entry of new medicines in the NHS Summary cutaneous patch (Qutenza ) is licensed for
New Medicines Profile August 2010 Issue. 10/03 cutaneous patch Concise evaluated information to support the managed entry of new medicines in the NHS Summary cutaneous patch (Qutenza ) is licensed for
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA)
 RISPERIDONE Effective Shared Care Agreement (ESCA)") E102 Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA) Patient details Name: Date of birth: NHS number: Contact details Specialist:
E102 Conduct Disorder in Children and Young People (CYP 5-18 years of age) RISPERIDONE Effective Shared Care Agreement (ESCA) Patient details Name: Date of birth: NHS number: Contact details Specialist:
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES. MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) KEY ISSUES
 KEY ISSUES") MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
MERSEY CARE NHS TRUST HOW WE MANAGE MEDICINES MM11 - High-Dose Antipsychotic Use Guidelines (local guideline) Medicines Management Services aim to ensure that (i) Service users receive their medicines
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am
 Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
Treatment of Neuropathic Pain: What Does the Evidence Say? or Just the Facts Ma am Tim R Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy Cleveland Clinic Akron General Center for Family
Reimbursement of Lidocaine 5% Plasters (Versatis ) effective 1 st September 2017
 effective 1 st September 2017") Feidhmeannacht na Seirbhíse Sláinte, Seirbhís Aisíocaíochta Cúraim Phríomhúil Bealach amach 5 an M50, An Bóthar Thuaidh, Fionnghlas Baile Átha Cliath 11, D11 XKF3 Guthán: (01) 864 7100 Facs: (01) 834 3589
Feidhmeannacht na Seirbhíse Sláinte, Seirbhís Aisíocaíochta Cúraim Phríomhúil Bealach amach 5 an M50, An Bóthar Thuaidh, Fionnghlas Baile Átha Cliath 11, D11 XKF3 Guthán: (01) 864 7100 Facs: (01) 834 3589
NHS Dumfries & Galloway Ferrous Salt Review Protocol November 09
 Title of Project: NHS Dumfries & Galloway Ferrous Salt Review Protocol November 09 1 Reason for the review Choice of iron preparation is based on cost and incidence of side effects (BNF). There is little
Title of Project: NHS Dumfries & Galloway Ferrous Salt Review Protocol November 09 1 Reason for the review Choice of iron preparation is based on cost and incidence of side effects (BNF). There is little
Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91
 Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
Depression in adults with a chronic physical health problem: recognition and management Clinical guideline Published: 28 October 2009 nice.org.uk/guidance/cg91 NICE 2018. All rights reserved. Subject to
VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules
 VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules VI.2.1 Overview of disease epidemiology Depression
VI.2 Elements for a Public Summary DULOXETINE Pharmalex 30 mg hard gastro-resistant capsules DULOXETINE Pharmalex 60 mg hard gastro-resistant capsules VI.2.1 Overview of disease epidemiology Depression
Neuropathic Pain. Scott Magnuson, MD Pain Management of North Idaho, PLLC
 Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
Gabapentin and pregabalin
 Pain CONCERN Medicines for long-term pain Gabapentin and pregabalin This leaflet is about gabapentin and pregabalin, two drugs which are part of a group sometimes called gabapentinoids. The leaflet will
Pain CONCERN Medicines for long-term pain Gabapentin and pregabalin This leaflet is about gabapentin and pregabalin, two drugs which are part of a group sometimes called gabapentinoids. The leaflet will
The legally binding text is the original French version TRANSPARENCY COMMITTEE. Opinion. 1 October 2008
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 1 October 2008 EFFEXOR SR 37.5 mg prolonged-release capsule B/30 (CIP: 346 563-3) EFFEXOR SR 75 mg prolonged-release
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 1 October 2008 EFFEXOR SR 37.5 mg prolonged-release capsule B/30 (CIP: 346 563-3) EFFEXOR SR 75 mg prolonged-release
National Horizon Scanning Centre. Pregabalin (Lyrica) for fibromyalgia. September 2007
 for fibromyalgia. September 2007") Pregabalin (Lyrica) for fibromyalgia September 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Pregabalin (Lyrica) for fibromyalgia September 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive
Amendments to recommendations concerning venlafaxine
 Amendments to recommendations concerning venlafaxine On 31 May 2006 the MHRA issued revised prescribing advice for venlafaxine*. This amendment brings the guideline into line with the new advice but does
Amendments to recommendations concerning venlafaxine On 31 May 2006 the MHRA issued revised prescribing advice for venlafaxine*. This amendment brings the guideline into line with the new advice but does
BRIEF SUMMARY CONTENT
 Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
Page 1 of 17 Brief Summary GUIDELINE TITLE Depression. The treatment and management of depression in adults. BIBLIOGRAPHIC SOURCE(S) National Collaborating Centre for Mental Health. Depression. The treatment
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
SHARED CARE GUIDELINE
 SHARED CARE GUIDELINE Methylphenidate in the treatment of Attention Deficit Hyperactivity Disorder in Children, Young People and Adults Implementation Date: June 2015 Review Date: June 2017 This guidance
SHARED CARE GUIDELINE Methylphenidate in the treatment of Attention Deficit Hyperactivity Disorder in Children, Young People and Adults Implementation Date: June 2015 Review Date: June 2017 This guidance
Guidelines on Choice and Selection of Antidepressants for the Management of Depression
 Working in partnership: Hertfordshire Partnership University NHS Foundation Trust East and North Hertfordshire Clinical Commissioning Group Herts Valleys Clinical Commissioning Group Guidelines on Choice
Working in partnership: Hertfordshire Partnership University NHS Foundation Trust East and North Hertfordshire Clinical Commissioning Group Herts Valleys Clinical Commissioning Group Guidelines on Choice