Clostridium difficile Infection (CDI)
|
|
|
- Bertina Wood
- 5 years ago
- Views:
Transcription
1 월요집담회 Clostridium difficile Infection (CDI) R4 송주혜
2
-producing bacillus Transmitted among humans through the")

 Recurrent N")
3 Clostridium difficile infection (CDI) Anaerobic gram (+), spore-forming, toxin(tcda&tcdb)-producing bacillus Transmitted among humans through the fecal oral route In the US, most frequently reported nosocomial pathogen Asymptomatic carrier Diarrhea, medicated by TcdA and TcdB, mild to severe : leading to colonocyte death, loss of intestinal barrier function, and neutrophilic colitis Colitis or pseudomembranous colitis(pmc) Recurrent N ENGL J Med 2015;372:
4 Clostridium difficile infection (CDI) Associated with severe illness, infection-related mortality of 5% and all-cause mortality of 15 to 20 % Mild : afebrile, no notable laboratory abnormalities Moderate : WBC >15000/mm3, BUN or Cr levels above baseline Severe : bloody diarrhea, PMC, ileus, BT>38.9 C, WBC >20000/mm3, albumin <2.5mg/dl, AKI Complicated : toxic megacolon, peritonitis, respiratory distress, hemodynamic instability N ENGL J Med 2015;372:
5 Clostridium difficile infection (CDI) Community-acquired C.difficile : in a person who had no overnight stay in a health care facility within 12 weeks before infection Nosocomial infection : events collected >3 days after admission to the facility N ENGL J Med 2015;372:
6 Incidence of nosocomial CDI N ENGL J Med 2015;372:
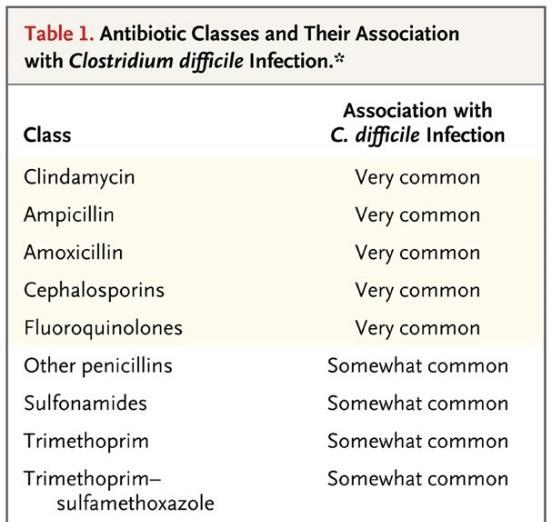
7 Risk factors of CDI Antibiotic use : most important Advanced age : severity increase as age increase Inflammatory bowel disease Chemotherapy Chronic kidney disease Immunodeficiency Organ transplantation Acid suppression (PPI use) : uncertain Risk factors of recurrent CDI Advanced age Severe initial episode of CDI Ongoing use of antibiotics N ENGL J Med 2015;372:
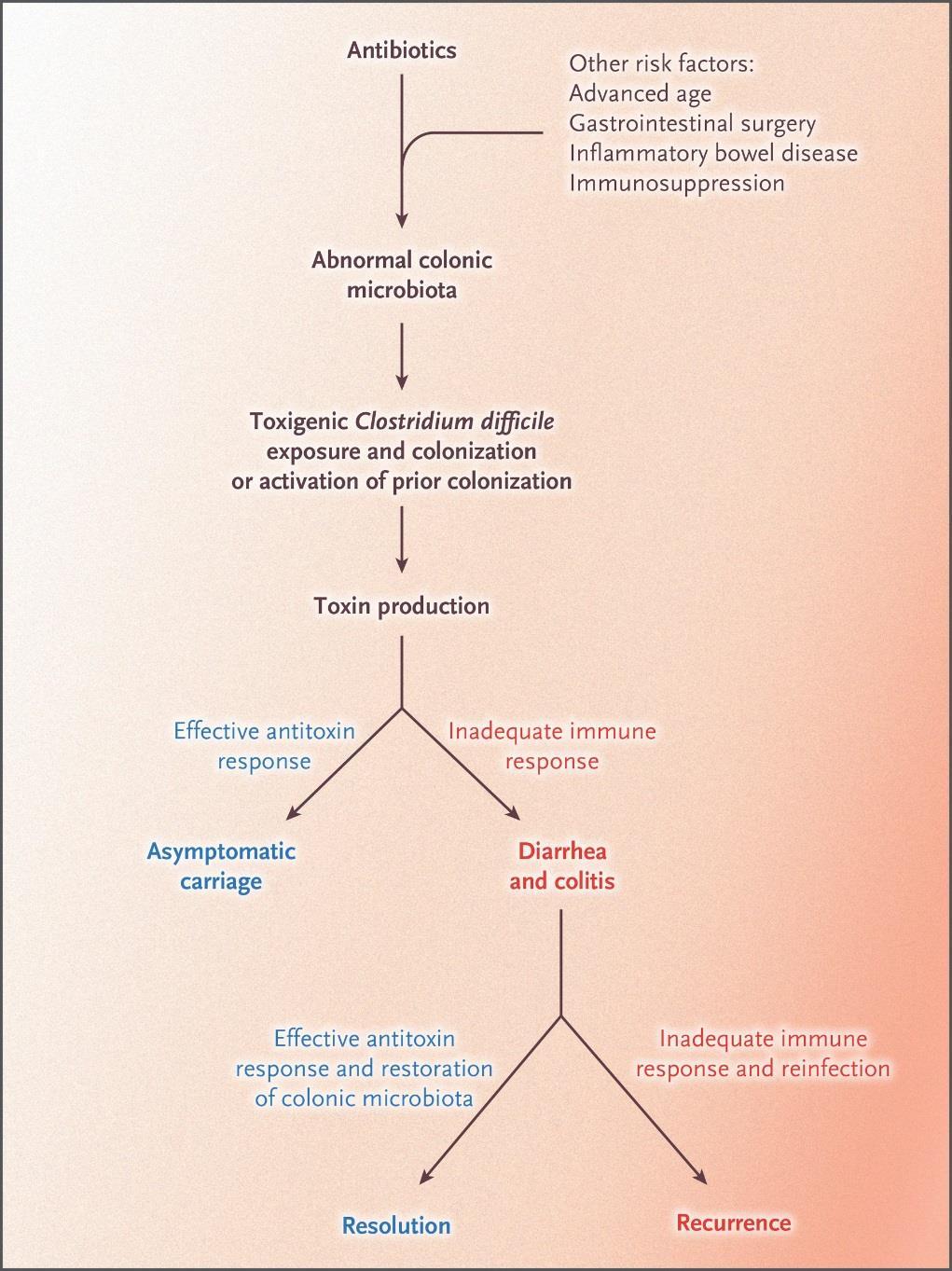
8 Pathogenesis of CDI N ENGL J Med 2015;372:
9 B1/NAP1/027 strain High-level fluoroquinolone resistance Efficient sporulation Markedly high toxin production Mortality rate 3 times higher than less virulent strains N ENGL J Med 2015;372:
10 Diagnosis of CDI Enzyme immunoassay for toxins in stool : rapid, easily performed DNA-based test that identify microbial toxin genes in unformed stool : higher sensitivity, specificity, and can detect BI/NAP1/027 strain Stool culture : not widely available Sequential testing with PCR & enzyme immunoassay But, in clinical practice, in patient with diarrhea either enzyme immunoassay or PCR (+) -> should prompt treatment N ENGL J Med 2015;372:
11 Diagnosis of CDI Stool testing for C.difficile toxins should be confined to patients with diarrhea Posttreatment testing has no role in confirming eradication After resolution of symptoms, many successfully treated patients will continue to test (+) for weeks or months Ongoing or recurrent diarrhea, after initial treatment, stool testing can be helpful in differentiating recurrent CDI from postinfectious IBS or IBD N ENGL J Med 2015;372:
12 Severity of CDI Old age Comorbidity Immunocompromised state Organ failure(respiratory failure, Hypotension) Severe leukocytosis(>15,000/mm3), Renal dysfunction(cr >2.3 mg/dl or X1.5 of base line ) Hypoalbuminemia(<2.5 mg/dl) Pancolitis Toxic megacolon Bowel perforation N Engl J Med 2005;353: CMAJ 2004;171: Clin Infect Dis 2010;50: World J Gastroenterol 2009;15: Infect Control Hosp Epidemiol 2010;31:
13 Treatment of CDI Metronidazole(MTZ) 500mg q8hr Oral vancomycin(van) 125mg-500mg q6hr Mild to moderate infection : MTZ = VAN Severe infection : MTZ < VAN Recent data : overall superiority of VAN More frequent side effects of MTZ Decreasing cost of generic VAN Increasing use of VAN 2017 update by IDSA and SHEA Initial CDI: oral VAN or FDX > MTZ N ENGL J Med 2015;372:
 bacteria : Cure")

14 Treatment of CDI Fidaxomicin(FDX) 200mg q12hr : Poorly absorbed, bactericidal, macrocyclic antibiotic with activity against specific anaerobic gram (+) bacteria : Cure rate for acute infection was nearly equivalent to VAN : Reducing the risk of recurrence : Less disruption of the normal colonic anaerobic microflora : Higher cost N ENGL J Med 2015;372:

15 Fidaxomicin VS. vancomycin for CDI in Europe, Canada, and the USA: a double-blind, non-inferiority, RCT Lancet infect Dis. 2012; 12:

16 Fidaxomicin preserves the intestinal microbiome during and after treatment of CDI Clin Infect Dis. 2012;55 Suppl 2:S132-42

17 Treatment of CDI v v N ENGL J Med 2015;372:

18 Treatment of CDI v v N ENGL J Med 2015;372:
19 Recurrent CDI Risk of CDI recurrence : ranges from 20 % after initial episode to 60% after multiple prior recurrences Re-exposure to or reactivation of spores in patients, who have impaired immune response to infection and weakened barrier function of the colonic microbiota N ENGL J Med 2015;372:
20 Treatment of recurrent CDI First recurrence : VAN for days Second recurrence : FDX or VAN tapered and pulsed regimen : Fecal microbial transplantation (FMT) N ENGL J Med 2015;372:

21
22 Fecal microbial transplantation (FMT) Human colonic microbiota provides colonization resistance against bacterial pathogen Exposure to antibiotics -> rapid decline in fecal microbial diversity Stopping administration of antibiotics -> eliminate C.difficile from colon and allow microbiota to recover (12wks or longer) Oral or rectal transplantation of feces from healthy, pretested donor Phyla Bacteroidetes and Firmicutes are critical components but, precise components of fecal microbiome are not known N ENGL J Med 2015;372:
23 FMT N ENGL J Med 2015;372:


24 FMT Clin Endosc 2016 March 9



25 69/F PMC by colonoscopy Metronidazole 10 days and vancomycin 4 weeks FMT in refractory PMC Initial colonoscopic and pathologic findings Colonoscopic findings on the day of the procedure and fecal microbial transplantation Colonoscopic findings one month after FMT Intest Res. 2016; 14: 83-88

26 Treatment of recurrent CDI v v N ENGL J Med 2015;372:
27 Prevention Absence of an effective vaccine Infection control : Antibiotic stewardship : Prevention of spread in health care facilities : Probiotics (?) N ENGL J Med 2015;372:
28 Prevention Minimizing antibiotic use Washing with soap and water, reduce number of viable C.difficile spores (not alcohol-based hand sanitizer) Patients with known or suspected C.difficile should be isolated Wear gloves and gowns, postdischarge disinfection Probiotics : uncertain effect on the prevention of CDI N ENGL J Med 2015;372:
29
30 EPIDEMIOLOGY I. How are CDI cases best defined? Recommendation 1. To increase comparability between clinical settings, use available standardized case definitions for surveillance of (1) healthcare facility-onset (HO) CDI; (2) community-onset, healthcare facility associated (CO-HCFA) CDI; and (3) community-associated (CA) CDI (good practice recommendation)
31 II. What is the minimal surveillance recommendation for institutions with limited resources? Recommendation 1. At a minimum, conduct surveillance for HO-CDI in all inpatient healthcare facilities to detect elevated rates or outbreaks of CDI within the facility EPIDEMIOLOGY (weak recommendation, low quality of evidence)
32 EPIDEMIOLOGY II. What is the best way to express CDI incidence and rates? Recommendation 1. Express the rate of HO-CDI as the number of cases per patient-days. Express the CO-HCFA prevalence rate as the number of cases per 1000 patient admissions (good practice recommendation)
33 IV. How should CDI surveillance be approached in settings of high endemic rates or outbreaks? Recommendation EPIDEMIOLOGY 1. Stratify data by patient location to target control measures when CDI incidence is above national and/or facility reduction goals or if an outbreak is noted (weak recommendation, low quality of evidence)
34 DIAGNOSIS VI. What is the preferred population for C. difficile testing, and should efforts be made to achieve this target? Recommendation 1. Patients with unexplained and new-onset 3 unformed stools in 24 hours are the preferred target population for testing for CDI (weak recommendation, very low quality of evidence)

35 Diagnosis of CDI
36 DIAGNOSIS VII. What is the best-performing method (ie, in use positive and negative predictive value) for detecting patients at increased risk for clinically significant C. difficile infection in commonly submitted stool specimens? Recommendation 1. Use a stool toxin test as part of a multistep algorithm (ie, glutamate dehydrogenase [GDH] plus toxin; GDH plus toxin, arbitrated by nucleic acid amplification test [NAAT]; or NAAT plus toxin) rather than a NAAT alone for all specimens received in the clinical laboratory when there are no preagreed institutional criteria for patient stool submission
37 DIAGNOSIS VIII. What is the most sensitive method of diagnosis of CDI in stool specimens from patients likely to have CDI based on clinical symptoms? Recommendation 1. Use a NAAT alone or a multistep algorithm for testing (ie, GDH plus toxin; GDH plus toxin, arbitrated by NAAT; or NAAT plus toxin) rather than a toxin test alone when there are preagreed institutional criteria for patient stool submission (weak recommendation, low quality of evidence)
38 IX. What is the role of repeat testing, if any? Are there asymptomatic patients in whom repeat testing should be allowed, including test of cure? Recommendation 1. Do not perform repeat testing (within 7 days) during the same episode of diarrhea and do not test stool from asymptomatic patients, except for epidemiological studies DIAGNOSIS (strong recommendation, moderate quality of evidence)
39 DIAGNOSIS X. Does detection of fecal lactoferrin or another biologic marker improve the diagnosis of CDI over and above the detection of toxigenic C. difficile Can such a subset predict a more ill cohort? Recommendation 1. There are insufficient data to recommend use of biologic markers as an adjunct to diagnosis (no recommendation)
40 XIII. Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI? Recommendations INFECTION PREVENTION AND CONTROL 1. Accommodate patients with CDI in a private room with a dedicated toilet to decrease transmission to other patients. If there is a limited number of private single rooms, prioritize patients with stool incontinence for placement in private rooms (strong recommendation, moderate quality of evidence)
41 INFECTION PREVENTION AND CONTROL XIII. Should private rooms and/or dedicated toilet facilities be used for isolated patients with CDI? Recommendations 2. If cohorting is required, it is recommended to cohort patients infected or colonized with the same organism(s) that is, do not cohort patients with CDI who are discordant for other multidrugresistant organisms such as methicillin-resistant Staphylococcus aureus or vancomycin-resistant Enterococcus (strong recommendation, moderate quality of evidence)
42 INFECTION PREVENTION AND CONTROL XIV. Should gloves and gowns be worn while caring for isolated CDI patients? Recommendation 1. Healthcare personnel must use gloves (strong recommendation, high quality of evidence) and gowns on entry to a room of a patient with CDI and while caring for patients with CDI (strong recommendation, moderate quality of evidence)
43 INFECTION PREVENTION AND CONTROL XV. When should isolation be implemented? Recommendation 1. Patients with suspected CDI should be placed on preemptive contact precautions pending the C. difficile test results if test results cannot be obtained on the same day (strong recommendation, moderate quality of evidence).
44 INFECTION PREVENTION AND CONTROL XVI. How long should isolation be continued? Recommendations 1. Continue contact precautions for at least 48 hours after diarrhea has resolved (weak recommendation, low quality of evidence) 2. Prolong contact precautions until discharge if CDI rates remain high despite implementation of standard infection control measures against CDI (weak recommendation, low quality of evidence)
45 INFECTION PREVENTION AND CONTROL XVII. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI? Recommendations 1. In routine or endemic settings, perform hand hygiene before and after contact of a patient with CDI and after removing gloves with either soap and water or an alcoholbased hand hygiene product (strong recommendation, moderate quality of evidence)
46 INFECTION PREVENTION AND CONTROL XVII. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI? Recommendations 2. In CDI outbreaks or hyperendemic (sustained high rates) settings, perform hand hygiene with soap and water preferentially instead of alcohol-based hand hygiene products before and after caring for a patient with CDI given the increased efficacy of spore removal with soap and water (weak recommendation, low quality of evidence)
47 INFECTION PREVENTION AND CONTROL XVII. What is the recommended hand hygiene method (assuming glove use) when caring for patients in isolation for CDI? Recommendations 3. Handwashing with soap and water is preferred if there is direct contact with feces or an area where fecal contamination is likely (eg, the perineal region) (good practice recommendation)
48 INFECTION PREVENTION AND CONTROL XVIII. Should patient bathing interventions be implemented to prevent CDI? Recommendation 1. Encourage patients to wash hands and shower to reduce the burden of spores on the skin (good practice recommendation)
49 INFECTION PREVENTION AND CONTROL XIX. Should noncritical devices or equipment be dedicated to or specially cleaned after being used on the isolated patient with CDI? Recommendation 1. Use disposable patient equipment when possible and ensure that reusable equipment is thoroughly cleaned and disinfected, preferentially with a sporicidal disinfectant that is equipment compatible (strong recommendation, moderate quality of evidence)
50 INFECTION PREVENTION AND CONTROL XX. What is the role of manual, terminal disinfection using a C. difficile sporicidal agent for patients in isolation for CDI? Recommendation 1. Terminal room cleaning with a sporicidal agent should be considered in conjunction with other measures to prevent CDI during endemic high rates or outbreaks, or if there is evidence of repeated cases of CDI in the same room (weak recommendation, low quality of evidence)
51 INFECTION PREVENTION AND CONTROL XXI. Should cleaning adequacy be evaluated? Recommendation 1. Incorporate measures of cleaning effectiveness to ensure quality of environmental cleaning (good practice recommendation)
52 INFECTION PREVENTION AND CONTROL XXII. What is the role of automated terminal disinfection using a method that is sporicidal against C. difficile? 1. There are limited data at this time to recommend use of automated, terminal disinfection using a sporicidal method for CDI prevention (no recommendation)
53 INFECTION PREVENTION AND CONTROL XXIII. What is the role of daily sporicidal disinfection? Recommendation 1. Daily cleaning with a sporicidal agent should be considered in conjunction with other measures to prevent CDI during outbreaks or in hyperendemic (sustained high rates) settings, or if there is evidence of repeated cases of CDI in the same room (weak recommendation, low quality of evidence)
54 INFECTION PREVENTION AND CONTROL XXIV. Should asymptomatic carriers of C. difficile be identified and isolated if positive? Recommendation 1. There are insufficient data to recommend screening for asymptomatic carriage and placing asymptomatic carriers on contact precautions (no recommendation)
55 INFECTION PREVENTION AND CONTROL XXV. What is the role of antibiotic stewardship in controlling CDI rates? Recommendations 1. Minimize the frequency and duration of high-risk antibiotic therapy and the number of antibiotic agents prescribed, to reduce CDI risk (strong recommendation, moderate quality of evidence) 2. Implement an antibiotic stewardship program (good practice recommendation)
56 INFECTION PREVENTION AND CONTROL XXV. What is the role of antibiotic stewardship in controlling CDI rates? Recommendations 3. Antibiotics to be targeted should be based on the local epidemiology and the C. difficile strains present. Restriction of fluoroquinolones, clindamycin, and cephalosporins (except for surgical antibiotic prophylaxis) should be considered (strong recommendation, moderate quality of evidence)
57 INFECTION PREVENTION AND CONTROL XXVI. What is the role of proton pump inhibitor restriction in controlling CDI rates? Recommendation 1. Although there is an epidemiologic association between proton pump inhibitor (PPI) use and CDI, and unnecessary PPIs should always be discontinued, there is insufficient evidence for discontinuation of PPIs as a measure for preventing CDI (no recommendation)
58 INFECTION PREVENTION AND CONTROL XXVII. What is the role of probiotics in primary prevention of CDI? Recommendation 1. There are insufficient data at this time to recommend administration of probiotics for primary prevention of CDI outside of clinical trials (no recommendation)
59 TREATMENT XXVIII. What are important ancillary treatment strategies for CDI? Recommendations 1. Discontinue therapy with the inciting antibiotic agent(s) as soon as possible, as this may influence the risk of CDI recurrence (strong recommendation, moderate quality of evidence)
60 TREATMENT XXVIII. What are important ancillary treatment strategies for CDI? Recommendations 2. Antibiotic therapy for CDI should be started empirically for situations where a substantial delay in laboratory confirmation is expected, or for fulminant CDI (weak recommendation, low quality of evidence)
61 TREATMENT XXIX. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment? Recommendations 1. Either vancomycin or fidaxomicin is recommended over metronidazole for an initial episode of CDI. The dosage is vancomycin 125 mg orally 4 times per day or fidaxomicin 200 mg twice daily for 10 days (strong recommendation, high quality of evidence)
62 XXIX. What are the best treatments of an initial CDI episode to ensure resolution of symptoms and sustained resolution 1 month after treatment? Recommendations 2. In settings where access to vancomycin or fidaxomicin is limited, we suggest using metronidazole for an initial episode of nonsevere CDI only (weak recommendation, high quality of evidence) TREATMENT The suggested dosage is metronidazole 500 mg orally 3 times per day for 10 days. Avoid repeated or prolonged courses due to risk of cumulative and potentially irreversible neurotoxicity (strong recommendation, moderate quality of evidence)
63 TREATMENT XXX. What are the best treatments of fulminant CDI? Recommendations 1. For fulminant CDI*, vancomycin administered orally is the regimen of choice (strong recommendation, moderate quality of evidence) If ileus is present, vancomycin can also be administered per rectum (weak recommendation, low quality of evidence) *Fulminant CDI, previously referred to as severe, complicated CDI, may be characterized by hypotension or shock, ileus, or megacolon.
64 TREATMENT XXX. What are the best treatments of fulminant CDI? Recommendations The vancomycin dosage is 500 mg orally 4 times per day and 500 mg in approximately 100 ml normal saline per rectum every 6 hours as a retention enema. Intravenously administered metronidazole should be administered together with oral or rectal vancomycin, particularly if ileus is present (strong recommendation, moderate quality of evidence) The metronidazole dosage is 500 mg intravenously every 8 hours.*
65 TREATMENT XXX. What are the best treatments of fulminant CDI? Recommendations 2. If surgical management is necessary for severely ill patients, perform subtotal colectomy with preservation of the rectum (strong recommendation, moderate quality of evidence). Diverting loop ileostomy with colonic lavage followed by antegrade vancomycin flushes is an alternative approach that may lead to improved outcomes (weak recommendation, low quality of evidence).
66 TREATMENT XXXI. What are the best treatments for recurrent CDI? Recommendations 1. Treat a first recurrence of CDI with oral vancomycin as a tapered and pulsed regimen rather than a second standard 10-day course of vancomycin (weak recommendation, low quality of evidence), OR 2. Treat a first recurrence of CDI with a 10-day course of fidaxomicin rather than a standard 10-day course of vancomycin (weak recommendation, moderate quality of evidence), OR
67 TREATMENT XXXI. What are the best treatments for recurrent CDI? Recommendations 3. Treat a first recurrence of CDI with a standard 10-day course of vancomycin rather than a second course of metronidazole if metronidazole was used for the primary episode (weak recommendation, low quality of evidence)
68 TREATMENT XXXI. What are the best treatments for recurrent CDI? Recommendations 4. Antibiotic treatment options for patients with >1 recurrence of CDI include oral vancomycin therapy using a tapered and pulsed regimen, (weak recommendation, low quality of evidence) a standard course of oral vancomycin followed by rifaximin (weak recommendation, low quality of evidence), or fidaxomicin (weak recommendation, low quality of evidence).
69 XXXI. What are the best treatments for recurrent CDI? TREATMENT 5. Fecal microbiota transplantation is recommended for patients with multiple recurrences of CDI who have failed appropriate antibiotic treatments (strong recommendation, moderate quality of evidence)
70 TREATMENT XXXI. What are the best treatments for recurrent CDI? 6. There are insufficient data at this time to recommend extending the length of anti C. difficile treatment beyond the recommended treatment course or restarting an anti C. difficile agent empirically for patients who require continued antibiotic therapy directed against the underlying infection or who require retreatment with antibiotics shortly after completion of CDI treatment, respectively (no recommendation)

71 Treatment of CDI Initial episode

72 Treatment of CDI Recurrent episode
73 References L. Clifford MacDonald at el. in adults and children:2017 update by IDSA and SHEA, CID 2018: 66 (1 April), Daniel A. at el. Clostridium difficile infection, N ENGL J Med 2015;372: Comely OA at el. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomized controlled trial, Lancet infect Dis. 2012; 12: Thomas J. Louie at el. Fidaxomicin preserves the intestinal microbiome during and after treatment of Clostridium difficile infection(cdi) and reduces both toxin reexpression and recurrence of CDI, Clin Infect Dis. 2012;55 Suppl 2:S Hyun Ho Choi at el. Fecal microbiota transplantation: current applications, effectiveness, and future perspectives, Clinical endoscopy, March 9,2016 Jun Young Shin at el. Refractory pseudomembranous colitis that was treated successfully with colonoscopic fecal microbial transplantation, Intest Res. 2016; 14: 83-88
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
VIII Congresso Nazionale Maggio 2018
 VIII Congresso Nazionale Attualità e prospettive nella prevenzione e controllo delle infezioni nelle organizzazioni sanitarie 21-23 Maggio 2018 Bergamo, Ospedale Papa Giovanni XXIII Clostridium difficile
VIII Congresso Nazionale Attualità e prospettive nella prevenzione e controllo delle infezioni nelle organizzazioni sanitarie 21-23 Maggio 2018 Bergamo, Ospedale Papa Giovanni XXIII Clostridium difficile
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review
 Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
C. DIFFICILE UPDATE. Heather Bell, DO Infectious Diseases Physician
 C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Questions Testing recommendations Treatment recommendations
C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Questions Testing recommendations Treatment recommendations
7/30/2018 C. DIFFICILE UPDATE DISCLOSURE OUTLINE. Heather Bell, DO Infectious Diseases Physician. None to report
 C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Testing recommendations Treatment recommendations Isolation
C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Testing recommendations Treatment recommendations Isolation
Clinical Infectious Diseases IDSA GUIDELINE
 Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and
Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH
 The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections
 ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
CDI The Impact. Disclosures. Acknowledgments. Objectives and Agenda. What s in the Name? 11/14/2012. Lets Talk Numbers
 Disclosures No conflict of interest to declare Acknowledgments Objectives and Agenda Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Guidelines
Disclosures No conflict of interest to declare Acknowledgments Objectives and Agenda Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Guidelines
ABSTRACT PURPOSE METHODS
 ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate
 Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Clostridium difficile Essential information
 Clostridium difficile Essential information Clostridium difficile Origins Clostridium difficile (C. diff) is a Gram positive, spore forming, anaerobic bacterium with a rod structure. It was first identified
Clostridium difficile Essential information Clostridium difficile Origins Clostridium difficile (C. diff) is a Gram positive, spore forming, anaerobic bacterium with a rod structure. It was first identified
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018
 Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile: An Overview
 Clostridium difficile: An Overview CDI Webinar July 11, 2017 PUBLIC HEALTH DIVISION Acute and Communicable Disease Prevention Section Outline Background Microbiology Burden Pathogenesis Diagnostic testing
Clostridium difficile: An Overview CDI Webinar July 11, 2017 PUBLIC HEALTH DIVISION Acute and Communicable Disease Prevention Section Outline Background Microbiology Burden Pathogenesis Diagnostic testing
Clostridium Difficile Associated Disease. Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011
 Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Update on Clostridium difficile infection.
 Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest wit
 Potential for conflicts of interest wit") GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Clostridium Difficile Infection in Adults Treatment and Prevention
 Clostridium Difficile Infection in Adults Treatment and Prevention Definition: Clostridium Difficile colonizes the human intestinal tract after the normal gut flora has been altered by antibiotic therapy
Clostridium Difficile Infection in Adults Treatment and Prevention Definition: Clostridium Difficile colonizes the human intestinal tract after the normal gut flora has been altered by antibiotic therapy
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017)
 Week 52 (Ending 30/12/2017)") Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Los Angeles County Department of Public Health: Your Partner in CDI Prevention
 Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
Modern approach to Clostridium Difficile Infection
 Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Clostridium difficile: Can you smell the new updates?
 Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
March 3, To: Hospitals, Long Term Care Facilities, and Local Health Departments
 March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
What s New for Clostridium difficile John Lynch MD MPH Harborview Medical Center University of Washington
 What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
Clostridium difficile Infection (CDI) Guideline Update:
 Guideline Update:") Clostridium difficile Infection (CDI) Guideline Update: Understanding the Data Behind the Recommendations Erik R. Dubberke, MD, MSPH A Webinar for HealthTrust Members Professor of Medicine September 24,
Clostridium difficile Infection (CDI) Guideline Update: Understanding the Data Behind the Recommendations Erik R. Dubberke, MD, MSPH A Webinar for HealthTrust Members Professor of Medicine September 24,
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
A Pharmacist Perspective
 Leveraging Technology to Reduce CDI A Pharmacist Perspective Ed Eiland, Pharm.D., MBA, BCPS (AQ-ID) Clinical Practice and Business Supervisor Huntsville Hospital System Huntsville Hospital 881 licensed
Leveraging Technology to Reduce CDI A Pharmacist Perspective Ed Eiland, Pharm.D., MBA, BCPS (AQ-ID) Clinical Practice and Business Supervisor Huntsville Hospital System Huntsville Hospital 881 licensed
Annex C: - CDI What s the diff? 4 th Annual Outbreak Management Workshop September 19, 2013 Naideen Bailey & Grace Volkening
 Annex C: - CDI What s the diff? 4 th Annual Outbreak Management Workshop September 19, 2013 Naideen Bailey & Grace Volkening There s an updated Annex C Annex C is an extension to the PIDAC Infection Prevention
Annex C: - CDI What s the diff? 4 th Annual Outbreak Management Workshop September 19, 2013 Naideen Bailey & Grace Volkening There s an updated Annex C Annex C is an extension to the PIDAC Infection Prevention
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure
 Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
The incubation period is unknown. However; the onset of clinical disease is typically 5-10 days after initiation of antimicrobial treatment.
 C. DIFFICILE Case definition CONFIRMED CASE A patient is defined as a case if they are one year of age or older AND have one of the following requirements: A laboratory confirmation of a positive toxin
C. DIFFICILE Case definition CONFIRMED CASE A patient is defined as a case if they are one year of age or older AND have one of the following requirements: A laboratory confirmation of a positive toxin
! MQ is a 44 year old woman that I first saw in Sept ! In MVA in Jan 2003 requiring spinal surgery
 Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Patient Safety Summit 2014
 Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
6/14/2012. Welcome! PRESENTATION OUTLINE CLOSTRIDIUM DIFFICILE PREVENTION. Teaming Up to Prevent Infections! 1) Impact. 2) Testing Recommendations
 Impact. 2) Testing Recommendations") CLOSTRIDIUM DIFFICILE PREVENTION Beth Goodall, RN, BSN Board Certified in Infection Prevention and Control DCH Health System Epidemiology Director Welcome! Teaming Up to Prevent Infections! CLOSTRIDIUM
CLOSTRIDIUM DIFFICILE PREVENTION Beth Goodall, RN, BSN Board Certified in Infection Prevention and Control DCH Health System Epidemiology Director Welcome! Teaming Up to Prevent Infections! CLOSTRIDIUM
Journey to Decreasing Clostridium Difficile and the Unexpected Twist. Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer
 Journey to Decreasing Clostridium Difficile and the Unexpected Twist Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer 4/13/2018 Objectives Discuss the organism and clinical
Journey to Decreasing Clostridium Difficile and the Unexpected Twist Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer 4/13/2018 Objectives Discuss the organism and clinical
CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT. Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates
 CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates Learning Objectives Recognize patients who are highest risk for C. diff infections
CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates Learning Objectives Recognize patients who are highest risk for C. diff infections
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital
 as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital") Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
Patient presentation
 Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Clostridium difficile
 Clostridium difficile Care Homes IPC Study Day Sue Barber Infection Prevention & Control Lead AV & Chiltern CCG s Clostridium difficile A spore forming Bacterium. Difficult to grow in the laboratory hence
Clostridium difficile Care Homes IPC Study Day Sue Barber Infection Prevention & Control Lead AV & Chiltern CCG s Clostridium difficile A spore forming Bacterium. Difficult to grow in the laboratory hence
Clostridioides difficile Infection: What s the BIG Stink?
 Clostridioides difficile Infection: What s the BIG Stink? GLORIA MATHIS, RN, BSN, CIC 29 TH ANNUAL MEDICAL SURGICAL CONFERENCE APRIL 4, 2019 SAN FRANCISCO, CA I am sre my patient has C. diff. I cold smell
Clostridioides difficile Infection: What s the BIG Stink? GLORIA MATHIS, RN, BSN, CIC 29 TH ANNUAL MEDICAL SURGICAL CONFERENCE APRIL 4, 2019 SAN FRANCISCO, CA I am sre my patient has C. diff. I cold smell
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Clostridium difficile Infection in the Department of Defense (DOD):
:") 1 1 Clostridium difficile Infection in the Department of Defense (DOD): 2007-2013 NMCPHC-EDC- TR-271-2015 By Charlotte Neumann and Uzo Chukwuma February 2015 Approved for public release. Distribution is
1 1 Clostridium difficile Infection in the Department of Defense (DOD): 2007-2013 NMCPHC-EDC- TR-271-2015 By Charlotte Neumann and Uzo Chukwuma February 2015 Approved for public release. Distribution is
Nursing Infectious Diseases Topics. David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle
 Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection
 Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
C. difficile: The Changing Epidemiology Evaluations Clostridium difficile Thank You to our Sponsors
 C. difficile: The Changing Epidemiology Ghinwa Dumyati, MD University of Rochester Monroe County Department of Public Health Thank You to our Sponsors Evaluations School of Public Health, University at
C. difficile: The Changing Epidemiology Ghinwa Dumyati, MD University of Rochester Monroe County Department of Public Health Thank You to our Sponsors Evaluations School of Public Health, University at
Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo
 Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo Istituto Nazionale per le Malattie Infettive «lazzaro Spallanzani», IRCCS-Roma The infectious cycle of transmission
Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo Istituto Nazionale per le Malattie Infettive «lazzaro Spallanzani», IRCCS-Roma The infectious cycle of transmission
Clostridium difficile
 Clostridium difficile Alex Aspinall MD, PhD, FRCPC Clinical Assistant Professor, University of Calgary Division of Gastroenterology and Hepatology, South Health Campus www.seacourses.com 1 Learning Points
Clostridium difficile Alex Aspinall MD, PhD, FRCPC Clinical Assistant Professor, University of Calgary Division of Gastroenterology and Hepatology, South Health Campus www.seacourses.com 1 Learning Points
DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE
 CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE Policy Number: PDS 021 Effective Date:
CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE Policy Number: PDS 021 Effective Date:
Managing Clostridium Difficile: An Old Bug With
 932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile
 OBJECTIVES HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile Identify and describe the pathophysiology of C. diff. Identify and describe current therapies in treatment of C. diff Identify
OBJECTIVES HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile Identify and describe the pathophysiology of C. diff. Identify and describe current therapies in treatment of C. diff Identify
Note: Active Table of Contents Click to follow link
 Clostridium difficile Infection: Prevention, Diagnosis and Treatment Adult/Pediatric Inpatient/Ambulatory/Emergency Department Clinical Practice Guideline Note: Active Table of Contents Click to follow
Clostridium difficile Infection: Prevention, Diagnosis and Treatment Adult/Pediatric Inpatient/Ambulatory/Emergency Department Clinical Practice Guideline Note: Active Table of Contents Click to follow
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Clostridium difficile in Adults
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in April 2018 ~ Resource #340405 Clostridium difficile in Adults Clostridium difficile (C. difficile)
This Clinical Resource gives subscribers additional insight related to the Recommendations published in April 2018 ~ Resource #340405 Clostridium difficile in Adults Clostridium difficile (C. difficile)
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Literature Scan: Antibiotics for Clostridium difficile Infection. Month/Year of Review: May 2015 Date of Last Review: April 2012
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Clostridium difficile infections Crappy Options
 Clostridium difficile infections Crappy Options Alexandru Petre David MD Infectious Diseases April 21, 2015 Objectives Microbiology Epidemiology Who is at risk? Pathogenesis Diagnosis Treatment Historical
Clostridium difficile infections Crappy Options Alexandru Petre David MD Infectious Diseases April 21, 2015 Objectives Microbiology Epidemiology Who is at risk? Pathogenesis Diagnosis Treatment Historical
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond
: Current Concepts in Clostridium difficile and beyond") Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
JMSCR Vol 05 Issue 07 Page July 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.15 Rapid Diagnosis of Toxigenic Clostridium
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.15 Rapid Diagnosis of Toxigenic Clostridium
Terapia dell infezione da Clostridium difficile. Massimo Coen I Div Mal Inf AO L Sacco
 Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery
 Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
All POOPed out: fecal microbiota transplant in C. difficile
 All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
C. difficile: When to Do Fecal Microbiota Transplant (FMT)
") C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
Clostridium Difficile colitismore
 Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
New approaches to treating Clostridium difficile Infection
 7:45 8:45 am New Approaches to Treating C. difficile Infection SPEAKER Fred A. Lopez, MD, MACP Presenter Disclosure Information The following relationships exist related to this presentation: Fred A. Lopez,
7:45 8:45 am New Approaches to Treating C. difficile Infection SPEAKER Fred A. Lopez, MD, MACP Presenter Disclosure Information The following relationships exist related to this presentation: Fred A. Lopez,
Clostridium difficile Infection (CDI) What is it? Modes of transmission? Environmental Sources? Control Measures?
 What is it? Modes of transmission? Environmental Sources? Control Measures?") Clostridium difficile Infection (CDI) What is it? Modes of transmission? Environmental Sources? Control Measures? Clostridium difficile Clostridium difficile - first described in 1935 when it was isolated
Clostridium difficile Infection (CDI) What is it? Modes of transmission? Environmental Sources? Control Measures? Clostridium difficile Clostridium difficile - first described in 1935 when it was isolated
Long-Term Care Updates
 Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printed page of such transmission.
 Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA)
Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA)
Clostridium difficile Diagnostic and Clinical Challenges
 Papers in Press. Published December 11, 2015 as doi:10.1373/clinchem.2015.243717 The latest version is at http://hwmaint.clinchem.org/cgi/doi/10.1373/clinchem.2015.243717 Clinical Chemistry 62:2 000 000
Papers in Press. Published December 11, 2015 as doi:10.1373/clinchem.2015.243717 The latest version is at http://hwmaint.clinchem.org/cgi/doi/10.1373/clinchem.2015.243717 Clinical Chemistry 62:2 000 000
Corporate Medical Policy Fecal Microbiota Transplantation
 Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Rapid-VIDITEST C. difficile Ag (GDH) Card/Blister
 Card/Blister") Li StarFish S.r.l. Via Cavour, 35-20063 Cernusco S/N (MI), Italy Tel. +39-02-92150794 - Fax. +39-02-92157285 info@listarfish.it -www.listarfish.it Rapid-VIDITEST C. difficile Ag (GDH) Card/Blister One
Li StarFish S.r.l. Via Cavour, 35-20063 Cernusco S/N (MI), Italy Tel. +39-02-92150794 - Fax. +39-02-92157285 info@listarfish.it -www.listarfish.it Rapid-VIDITEST C. difficile Ag (GDH) Card/Blister One
EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI)
") EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI) David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics & Epidemiology Associate Chief Medical Offer, UNC Health Care Medical
EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI) David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics & Epidemiology Associate Chief Medical Offer, UNC Health Care Medical
The Potential For Microbiome Modification In Critical Illness. Deborah Cook
 The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
A Comparison of Current Guidelines of Five International Societies on Clostridium difficile Infection Management
 Infect Dis Ther (2016) 5:207 230 DOI 10.1007/s40121-016-0122-1 REVIEW A Comparison of Current Guidelines of Five International Societies on Clostridium difficile Infection Management Csaba Fehér. Josep
Infect Dis Ther (2016) 5:207 230 DOI 10.1007/s40121-016-0122-1 REVIEW A Comparison of Current Guidelines of Five International Societies on Clostridium difficile Infection Management Csaba Fehér. Josep
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Carbapenem-resistant Enterobacteriaceae
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 47: Carbapenem-resistant Enterobacteriaceae Authors E-B Kruse, MD H. Wisplinghoff, MD Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key Issue Known
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 47: Carbapenem-resistant Enterobacteriaceae Authors E-B Kruse, MD H. Wisplinghoff, MD Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key Issue Known
Disclosure. Objectives. Assessment Questions. History. Clinical Case 2/27/2015. Clostridium difficile update and new therapies
 Disclosure Clostridium difficile update and new therapies Corey Frederick, PharmD PGY-2 Pharmacy Resident, Infectious Diseases Jackson Memorial Hospital Miami, Florida I do not have a vested interest in
Disclosure Clostridium difficile update and new therapies Corey Frederick, PharmD PGY-2 Pharmacy Resident, Infectious Diseases Jackson Memorial Hospital Miami, Florida I do not have a vested interest in
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection
 Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS
 GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS Version 3.0 Date ratified May 2008 Review date May 2010 Ratified by NUH Antibiotic Guidelines Committee NUH Drugs and Therapeutics
GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS Version 3.0 Date ratified May 2008 Review date May 2010 Ratified by NUH Antibiotic Guidelines Committee NUH Drugs and Therapeutics
Treatment Update on Fecal Microbiota Transplantation. Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department
 Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Clostridiodes Difficile Colitis: Update on Guidelines. Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018
 Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Presenter Disclosure Information
 10:45 11:45am New Approaches to Treating C. Difficile Infection SPEAKER Kalpana Gupta, MD, MPH Presenter Disclosure Information The following relationships exist related to this presentation: Kalpana Gupta,
10:45 11:45am New Approaches to Treating C. Difficile Infection SPEAKER Kalpana Gupta, MD, MPH Presenter Disclosure Information The following relationships exist related to this presentation: Kalpana Gupta,
New approaches to treating
 9:45 10:45am New Approaches to Treating C Difficile Infection SPEAKER Kalpana Gupta, MD, MPH Presenter Disclosure Information The following relationships exist related to this presentation: Kalpana Gupta,
9:45 10:45am New Approaches to Treating C Difficile Infection SPEAKER Kalpana Gupta, MD, MPH Presenter Disclosure Information The following relationships exist related to this presentation: Kalpana Gupta,
Historical Perspective
 The Diagnosis of C. difficile Infections: Does Molecular Make it More or Less difficile? Stephen M. Brecher Ph.D. VA Boston Health Care System BU School of Medicine The opinions expressed in this presentation
The Diagnosis of C. difficile Infections: Does Molecular Make it More or Less difficile? Stephen M. Brecher Ph.D. VA Boston Health Care System BU School of Medicine The opinions expressed in this presentation
Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience
 Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience Benoit Guery Unité des Maladies Infectieuses CHRU - Faculté de Médecine Lille Conflicts of interest Conferences,
Duodenal infusion of donor feces for recurrent Clostridium difficile infection A French experience Benoit Guery Unité des Maladies Infectieuses CHRU - Faculté de Médecine Lille Conflicts of interest Conferences,
Star Articles in Review
 Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News. Volume 3, Number 6, June 2015
 Antimicrobial Stewardship News. Volume 3, Number 6, June 2015") DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News Volume 3, Number 6, June 2015 Diagnostic Testing for Clostridium difficile Infection Background Clostridium difficile
DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News Volume 3, Number 6, June 2015 Diagnostic Testing for Clostridium difficile Infection Background Clostridium difficile
Understanding C. diff. atomalliance.org/cdifftraining
 Understanding C. diff atomalliance.org/cdifftraining This booklet is a printed guide of the online educational resource atomalliance.org/cdifftraining Target Audience Understanding C. diff This educational
Understanding C. diff atomalliance.org/cdifftraining This booklet is a printed guide of the online educational resource atomalliance.org/cdifftraining Target Audience Understanding C. diff This educational
Treatment of Clostridium Difficile Infection in Community Teaching Hospital: A Retrospective Study
 International Journal of Infectious Diseases and Therapy 2018; 3(3): 52-61 http://www.sciencepublishinggroup.com/j/ijidt doi: 10.11648/j.ijidt.20180303.12 ISSN: 2578-9651 (Print); ISSN: 2578-966X (Online)
International Journal of Infectious Diseases and Therapy 2018; 3(3): 52-61 http://www.sciencepublishinggroup.com/j/ijidt doi: 10.11648/j.ijidt.20180303.12 ISSN: 2578-9651 (Print); ISSN: 2578-966X (Online)
Antibiotic Associated Diarrhea (AAD) and Clostridium Difficile Infection (CDI)
 and Clostridium Difficile Infection (CDI)") Antibiotic Associated Diarrhea (AAD) and Clostridium Difficile Infection (CDI) Dario Conte, M.D. Gastroenterology and Endoscopy Unit Postgraduate School of Gastroenterology Fondazione IRCCS Ca Granda Ospedale
Antibiotic Associated Diarrhea (AAD) and Clostridium Difficile Infection (CDI) Dario Conte, M.D. Gastroenterology and Endoscopy Unit Postgraduate School of Gastroenterology Fondazione IRCCS Ca Granda Ospedale
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
Sherwood L. Gorbach, MD Professor of Public Health, Medicine, and Microbiology Tufts University School of Medicine
 Sherwood L. Gorbach, MD Professor of Public Health, Medicine, and Microbiology Tufts University School of Medicine Chief Scientific Officer, Optimer Pharmaceuticals, Inc. Conflicts: Chief Scientific Officer,
Sherwood L. Gorbach, MD Professor of Public Health, Medicine, and Microbiology Tufts University School of Medicine Chief Scientific Officer, Optimer Pharmaceuticals, Inc. Conflicts: Chief Scientific Officer,
L. Clifford McDonald, MD. Senior Advisor for Science and Integrity September 16, 2015
 Controversies and Current Issues in Diagnosis, Surveillance, and Treatment of Clostridium difficile infeciton L. Clifford McDonald, MD Senior Advisor for Science and Integrity September 16, 2015 Division
Controversies and Current Issues in Diagnosis, Surveillance, and Treatment of Clostridium difficile infeciton L. Clifford McDonald, MD Senior Advisor for Science and Integrity September 16, 2015 Division