Overview. Provider Enrollment Requirements Member Eligibility Hearing Services Authorization and Billing Additional Information
|
|
|
- Rhoda Preston
- 5 years ago
- Views:
Transcription
1 Audiology Services
2 Overview Provider Enrollment Requirements Member Eligibility Hearing Services Authorization and Billing Additional Information 2
3 Provider Enrollment 3
4 Alaska Medicaid Provider Enrollment Providers must be enrolled in Alaska Medicaid to bill for reimbursement of covered health care services rendered to eligible Medicaid members Enrollment starts at the Enrollment portal. Go to under Providers, then Enrollment Audiologist Licensing: Active license under AS to practice audiology individually or as a group Out-of-state providers must also have active license as an audiologist and be enrolled in the Medicaid program in state where services are provided Hearing Aid Dealer Licensing Active license under AS as a provider of hearing services and items Out-of-state providers must also have active license as a provider of hearing services and items and be enrolled in the Medicaid program in state where services are provided 4
5 Recordkeeping Recordkeeping requirements are documented in the Individual Provider Agreement and Tax Certification and Group Provider Agreement and Tax Certification Although most recordkeeping requirements are consistent for all providers, some requirements are provider-type specific Providers must maintain complete and accurate clinical, financial, and other relevant records to support the care and services for which they bill Alaska Medical Assistance for a minimum of 7 years from the date of service Providers are subject to audits, reviews and investigations Providers must ensure their staff, billing agents, and any other entities responsible for any aspect of records maintenance meet the same requirements. 5
6 Member Eligibility 6
7 Member Eligibility Always verify member eligibility by using one of the following options: Request to see the member's eligibility coupon or card that shows the current month of eligibility; photocopy for your records Call Automated Voice Response System (AVR): (toll-free) Verify via Alaska Medicaid Health Enterprise website Fax complete Recipient Eligibility Inquiry Form - General Submit a HIPAA compliant 270/271 electronic Eligibility Inquiry transaction Call Provider Inquiry , option 1 or , option 1, 1 (toll-free) 7
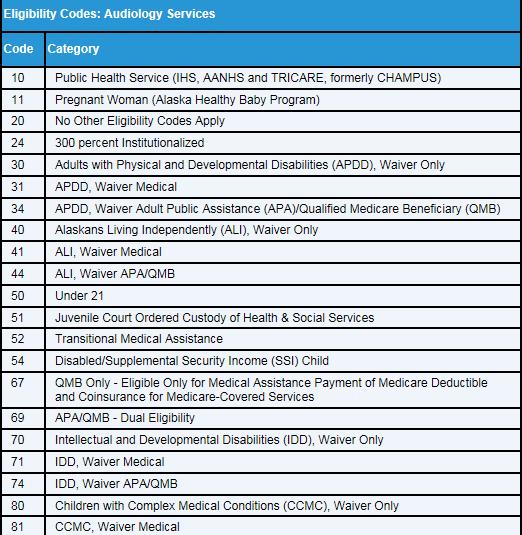
8 Member Eligibility 8
9 Audiology Services 9
10 Audiologist Services Audiologist covered hearing services and hearing items: Identified in 7 AAC Rendered within scope of the audiologist s license Include audiometric evaluation, diagnostic testing, audiometric screening, rehabilitative therapy, preventive services, corrective services, hearing items, and hearing item repairs Cochlear implantation-related services Cochlear implantation-related services include: a preliminary assessment, programming of the device, adjustments, member education, auditory rehabilitation and treatment sessions Cochlear implantation replacement parts are covered if they are prescribed by an appropriate, enrolled provider Covered parts include a microphone, speech processor, and transmitter 10
11 Hearing Aid Dealer Services Hearing Aid Dealer covered hearing services and hearing items: Identified in 7 AAC Rendered within scope of the hearing aid dealer s license Includes hearing devices, accessories, supplies, repairs, and covered services when prescribed by a licensed provider within the scope of their license The department will not pay a hearing aid dealer For services rendered after the member waived the hearing evaluation For a hearing test or diagnostic procedure designed to determine the cause of hearing impairment 11
12 Covered Services and Items Providers must be enrolled and services or items covered Hearing services and items must be identified by the prescriber as medically necessary to alleviate a disability due to hearing impairment Services or items must be least costly service that meets member s medical need Providers must include a manufacturer s warranty of no less than one year from the original purchase date for hearing items Delivery and dispensing costs of new item or delivery of repaired item covered if item or repair capabilities are unavailable in member s municipality Trial use if supported by medical documentation and proper service authorization obtained to be covered 12
13 Non-covered Services and Items Administrative Expenses Included in payment for covered services and items Administrative expenses include telephone responses to questions, mileage, travel expenses, travel time, equipment setup, installation, office inventory supply, and orientation and training regarding the proper use of equipment Assistive Listening Devices Identified in HCPCS codes Assistive listening devices include telephone amplifiers, alerters, television amplifiers, television caption decoders, telecommunication devices for the deaf, and devices for use with a cochlear implant Charges submitted for adjustments, labor, repairs or replacement parts for a previously purchased hearing item when the department has purchased a newer like item 13
14 Labor, Repair or Replacement When a damaged hearing item is no longer under warranty, labor will be paid to assess and repair the item Labor and repair will be covered if necessary for the hearing item to function as intended Repairs will not be covered if replacement of item would be more cost effective Claims must include: Statement describing the cause for and nature of repair Description of item and its serial number if available Documentation of labor charges Labor, repair or replacement will not be covered if: Item is covered under manufacturer s warranty Item needs repair because of manufacturer s defect Item is a previously purchased hearing item and the department has since purchased a newer like item for the member 14
15 Rental Rental or rent-to-purchase will not be covered if purchase is less expensive Rental or rent-to-purchase will be paid as follows: Rental period thirty days or longer, monthly rental fee will be ten percent of allowed purchase price Rental period less than thirty days, amount paid = rental fee (as calculated above) / number of days in the month x number of days item was rented Rental periods over twelve months of continuous use will not be paid Labor, repair and maintenance will not be paid before total rental fee payments equal the allowed purchase price; these costs must be included in the rental fee When total rental payments reach allowed purchase price, labor, repair or maintenance will be paid after sixty days or when warranty expires, whichever is later 15
16 Hearing Aids - Covered No more than one hearing aid per ear, per member, per three calendar years One fitting fee per ear, per purchase or rental of hearing aid One dispensing fee per ear, per purchase or rental of hearing aid Any type of monaural or binaural hearing aid that is worn in or behind the ear If replacement is covered and manufacturer s warranty is in effect, only difference between deductible and maximum allowable will be paid 16
17 Hearing Aids Hearing aid supplies included with hearing aid: Single cord Y-cord Harness New receiver Bone-conduction receiver with headband 17
18 Hearing Aids Under Twenty One Unlimited ear mold impressions and ear molds Unlimited hearing aid repairs if: Hearing aid warranty is no longer in effect and Provider has not been paid a dispensing fee No more than two replacements of lost hearing aids if: Hearing aid warranty is no longer in effect Hearing aid was lost no more than three years after original purchase date Written explanation of device loss is submitted with claim No more than two replacements of broken hearing aids if: Hearing aid warranty is no longer in effect Hearing aid was broken no more than three years after original purchase date Hearing aid cannot be repaired, or cost of repairs exceeds replacement 18
19 Hearing Aids Over Twenty One No more than two ear mold impressions and ear molds per ear, per three calendar years No more than two hearing aid repairs if: Hearing aid warranty is no longer in effect and Provider has not been paid a dispensing fee No more than one replacement of lost hearing aid if: Hearing aid warranty is no longer in effect Hearing aid was lost no more than three years after original purchase date Written explanation of device loss is submitted with claim No more than one replacement of broken hearing aid if: Hearing aid warranty is no longer in effect Hearing aid was broken no more than three years after original purchase date Hearing aid cannot be repaired, or cost of repairs exceeds replacement 19
20 Hearing Aids - Batteries Twenty hearing aid batteries a month up to one hundred and sixty a year per member Thirty cochlear implant alkaline batteries per month Fifty five cochlear implant zinc air batteries per month If batteries are for hearing aid the department did not purchase, provider must record manufacturer s serial number and purchase date of the hearing aid 20
21 Authorization and Billing 21
22 Service Authorization Required for some services and items Required for payment amounts that exceed the maximum allowable Requests for replacement must show necessity of replacement and lack of warranty coverage Requested on a Certificate of Medical Necessity (CMN) form Requests are reviewed on an individual basis Factors considered include: Degree of member s hearing loss Type of hearing loss suffered Configuration of member s hearing loss Management and treatment plan prepared 22

23 Fee Schedules Fee schedules tell you: What services are covered Maximum allowed reimbursement Additional documentation requirements Other special considerations Fee schedules can be found on in the Documents & Forms section 23

24 Certificate of Medical Necessity 24

25 Certificate of Medical Necessity 25
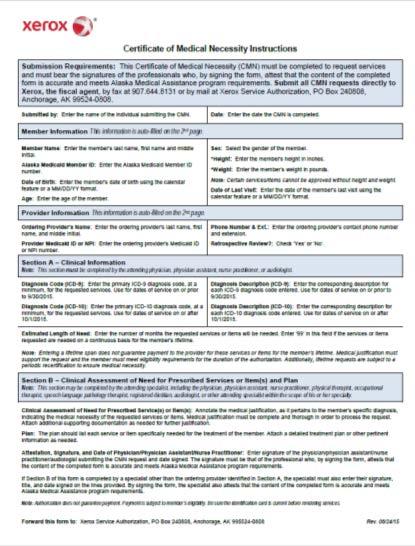
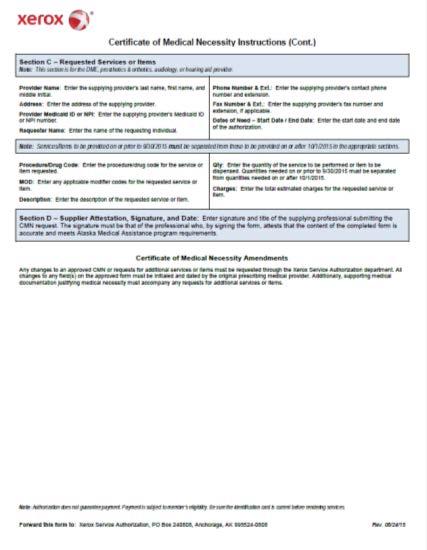
26 Certificate of Medical Necessity 26
27 Service Authorization Tips For relevant services, be sure to use a modifier to indicate the ear to which a service will be rendered Make sure dates are within appropriate timeframes Must attach an audiogram test report to CMN request or complete the clinical assessment section with great detail, including the assessment or audiogram results 27
28 Billing 837P electronic transaction Health Enterprise Payerpath CMS-1500, professional paper claim form 28
29 Additional Information 29
30 Overpayments & Repayment of Payment Errors Providers should closely review each remittance advice (RA) to ensure it reflects accurate payment for all billed services, including correct member details and services provided. In accordance with 7 AAC (e), Alaska Medical Assistance providers have 30 days from the time of payment to notify the department in writing of a payment error. Federal law (42 U.S.C. 1320(d)) requires repayment of overpayments to the department within 60 days of identifying the overpayment. Mail the written overpayment notification and a copy of the RA page detailing the overpayment to the address below: Conduent State Healthcare, LLC P.O. Box Anchorage, Alaska
31 Additional Resources Alaska Medicaid Health Enterprise website at Information necessary for successful billing Includes provider-specific Medicaid billing manuals and fee schedules You may also call: Provider Inquiry Eligibility only , option 1,2 or (toll-free), option 1,1,2 Claim status and other inquiries , option 1,1 or (toll-free), option 1,1,1 31

32 2016 Conduent Business Services, LLC. All rights reserved. Conduent and Conduent Design are trademarks of Conduent Business Services, LLC in the United States and/or other countries.
Changes to Texas Medicaid Hearing Services Benefits to Accompany PACT Transition
 Changes to Texas Medicaid Hearing Services Benefits to Accompany PACT Transition Information posted July 31, 2009 Effective for dates of service on or after September 1, 2009, Texas Medicaid clients who
Changes to Texas Medicaid Hearing Services Benefits to Accompany PACT Transition Information posted July 31, 2009 Effective for dates of service on or after September 1, 2009, Texas Medicaid clients who
Benefit: Hearing Services and Hearing Aid Devices
 CSHCN Services Program Hearing Services Benefits (PACT Transition) Information posted July 31, 2009 Effective for dates of service on or after September 1, 2009, the hearing services benefits for children
CSHCN Services Program Hearing Services Benefits (PACT Transition) Information posted July 31, 2009 Effective for dates of service on or after September 1, 2009, the hearing services benefits for children
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Audiology
 Fee-for-Service Provider Manual Audiology Updated 07.2015 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Audiology Billing Instructions................ 7-1 CMS-1500..................... 7-1
Fee-for-Service Provider Manual Audiology Updated 07.2015 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Audiology Billing Instructions................ 7-1 CMS-1500..................... 7-1
NEW YORK STATE MEDICAID PROGRAM HEARING AID/AUDIOLOGY MANUAL
 NEW YORK STATE MEDICAID PROGRAM HEARING AID/AUDIOLOGY MANUAL POLICY GUIDELINES Table of Contents SECTION I - REQUIREMENTS FOR PARTICIPATION IN MEDICAID...2 SERVICES PROVIDED TO PATIENTS UNDER 21 YEARS
NEW YORK STATE MEDICAID PROGRAM HEARING AID/AUDIOLOGY MANUAL POLICY GUIDELINES Table of Contents SECTION I - REQUIREMENTS FOR PARTICIPATION IN MEDICAID...2 SERVICES PROVIDED TO PATIENTS UNDER 21 YEARS
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Version 2013-1 (04/01/2013) Table of Contents WHAT S NEW FOR THE 2013 MANUAL? ---------------------------------------------------------------------------------
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Version 2013-1 (04/01/2013) Table of Contents WHAT S NEW FOR THE 2013 MANUAL? ---------------------------------------------------------------------------------
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Audiology
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Audiology PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Audiology Billing Instructions................ 7-1 Submission of Claim..................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Audiology PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Audiology Billing Instructions................ 7-1 Submission of Claim..................
TO BE RESCINDED Hearing aids. (A) Definitions. (1) "Audiologist."
 Definitions. (1) Audiologist.") ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-11 Hearing aids. TO BE RESCINDED (A) Definitions. (1) "Audiologist." A person licensed to practice audiology in Ohio under Chapter 4753. of the Revised Code,
ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-11 Hearing aids. TO BE RESCINDED (A) Definitions. (1) "Audiologist." A person licensed to practice audiology in Ohio under Chapter 4753. of the Revised Code,
Michigan Rehab Service Provider Manual
 Michigan Rehab Service Provider Manual (800) 769-0913 www.americanhearingbenefits.com Table of Contents INTRODUCTION... 3 PARTICIPATING PROVIDERS... 3 NEW HEARING INSTRUMENT(S)... 3 Coverage... 3 Authorization...
Michigan Rehab Service Provider Manual (800) 769-0913 www.americanhearingbenefits.com Table of Contents INTRODUCTION... 3 PARTICIPATING PROVIDERS... 3 NEW HEARING INSTRUMENT(S)... 3 Coverage... 3 Authorization...
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Table of Contents WHAT S NEW FOR THE 2014 MANUAL? --------------------------------------------------------------------------------
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Table of Contents WHAT S NEW FOR THE 2014 MANUAL? --------------------------------------------------------------------------------
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Table of Contents WHAT S NEW FOR THE 2018 MANUAL? --------------------------------------------------------------------------------
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES PROCEDURE CODES Table of Contents WHAT S NEW FOR THE 2018 MANUAL? --------------------------------------------------------------------------------
(b) A copy of the hearing test results; and
 A copy of the hearing test results; and") ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-11 DMEPOS: hearing aids. (A) Definition. "Basic hearing test" is an evaluation of an individual's ability to hear that includes the following components:
ACTION: Final DATE: 07/02/2018 10:05 AM 5160-10-11 DMEPOS: hearing aids. (A) Definition. "Basic hearing test" is an evaluation of an individual's ability to hear that includes the following components:
Benefit: Hearing Services and Hearing Aid Devices
 Changes to Texas Medicaid Hearing Services Benefits to Accompany PACT Transition Information posted August 20, 2009 Effective for dates of service on or after September 1, 2009, Texas Medicaid clients
Changes to Texas Medicaid Hearing Services Benefits to Accompany PACT Transition Information posted August 20, 2009 Effective for dates of service on or after September 1, 2009, Texas Medicaid clients
Audiology. Hearing Aids, Cochlear Devices, Audiology Services Overview/Reminders 2017
 Audiology Hearing Aids, Cochlear Devices, Audiology Services Overview/Reminders 2017 General Information Cochlear Devices and Hearing aids are review areas that are authorized per calendar year. A calendar
Audiology Hearing Aids, Cochlear Devices, Audiology Services Overview/Reminders 2017 General Information Cochlear Devices and Hearing aids are review areas that are authorized per calendar year. A calendar
Section. 24Hearing Aid and Audiometric. Evaluations
 Section 24Hearing Aid and Audiometric Evaluations 24 24.1 Enrollment...................................................... 24-2 24.1.1 Medicaid Managed Care Enrollment............................... 24-2
Section 24Hearing Aid and Audiometric Evaluations 24 24.1 Enrollment...................................................... 24-2 24.1.1 Medicaid Managed Care Enrollment............................... 24-2
Bone Anchored Hearing Aids (BAHA) and Partially-Implantable Magnetic Bone Conduction Hearing Aids
 and Partially-Implantable Magnetic Bone Conduction Hearing Aids") Bone Anchored Hearing Aids (BAHA) and Partially-Implantable Magnetic Bone Conduction Hearing Aids Policy Number: 2016M0023A Effective Date: 5/14/2018 Review Date: 4/27/2018 Next Review Date: 5/14/2020
Bone Anchored Hearing Aids (BAHA) and Partially-Implantable Magnetic Bone Conduction Hearing Aids Policy Number: 2016M0023A Effective Date: 5/14/2018 Review Date: 4/27/2018 Next Review Date: 5/14/2020
HEARING SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL
 HEARING SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL AUGUST 2018 CSHCN PROVIDER PROCEDURES MANUAL AUGUST 2018 HEARING SERVICES Table of Contents 20.1 Enrollment......................................................................
HEARING SERVICES CSHCN SERVICES PROGRAM PROVIDER MANUAL AUGUST 2018 CSHCN PROVIDER PROCEDURES MANUAL AUGUST 2018 HEARING SERVICES Table of Contents 20.1 Enrollment......................................................................
VETERANS AFFAIRS CANADA PAGE 1 PRINT DATE: JULY 24, 2018 BENEFIT GRID
 ************************************************************************************************************************************************************************************************* * CUSTOMER...VAC/ACC
************************************************************************************************************************************************************************************************* * CUSTOMER...VAC/ACC
MNPS Hearing Service Plan Employee Booklet 2015 HEAR BETTER LIVE FULLY. epichearing.com
 MNPS Hearing Service Plan Employee Booklet 2015 HEAR BETTER LIVE FULLY epichearing.com Introduction to the EPIC Hearing Service Plan (HSP) The EPIC Hearing Service Plan is the nation s first specialty
MNPS Hearing Service Plan Employee Booklet 2015 HEAR BETTER LIVE FULLY epichearing.com Introduction to the EPIC Hearing Service Plan (HSP) The EPIC Hearing Service Plan is the nation s first specialty
Archived 19.1 CPT CODES PROCEDURE CODES HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14
 SECTION 19 - PROCEDURE CODES 19.1 CPT CODES... 2 19.2 PROCEDURE CODES... 3 19.3 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14 1 SECTION 19-PROCEDURE CODES Procedure codes used by Medicaid
SECTION 19 - PROCEDURE CODES 19.1 CPT CODES... 2 19.2 PROCEDURE CODES... 3 19.3 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14 1 SECTION 19-PROCEDURE CODES Procedure codes used by Medicaid
Audiology Services. Table of Contents. Audiology Services Guidelines : Hearing services
 Audiology Services Table of Contents Audiology Services Guidelines... 2 317:30-3-65.9 Hearing services... 3-4 Audiology Services- General Considerations for Prior Authorization... 5-6 Audiogram and other
Audiology Services Table of Contents Audiology Services Guidelines... 2 317:30-3-65.9 Hearing services... 3-4 Audiology Services- General Considerations for Prior Authorization... 5-6 Audiogram and other
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES POLICY GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES POLICY GUIDELINES Table of Contents Section I - Requirements for Participation in Medicaid... 2 Section II- Hearing Screening and Testing
NEW YORK STATE MEDICAID PROGRAM HEARING AID/ AUDIOLOGY SERVICES POLICY GUIDELINES Table of Contents Section I - Requirements for Participation in Medicaid... 2 Section II- Hearing Screening and Testing
Hearing Services. Chapter
 Hearing Services Chapter.1 Enrollment..................................................................... -2.1.1 Non-Implantable Hearing Aid Devices and Services........................ -2.1.2 Implantable
Hearing Services Chapter.1 Enrollment..................................................................... -2.1.1 Non-Implantable Hearing Aid Devices and Services........................ -2.1.2 Implantable
Hearing Devices Policy and Administration Manual
 Ministry of Health & Long-Term Care Hearing Devices Policy and Administration Manual Assistive Devices Program Ministry of Health & Long-Term Care www.health.gov.on.ca/adp Table of Amendments This page
Ministry of Health & Long-Term Care Hearing Devices Policy and Administration Manual Assistive Devices Program Ministry of Health & Long-Term Care www.health.gov.on.ca/adp Table of Amendments This page
Section. CPT only copyright 2008 American Medical Association. All rights reserved. 23Hearing Aid and Audiological Services
 Section 23Hearing Aid and Audiological Services 23 23.1 Enrollment...................................................... 23-2 23.2 Reimbursement.................................................. 23-2 23.3
Section 23Hearing Aid and Audiological Services 23 23.1 Enrollment...................................................... 23-2 23.2 Reimbursement.................................................. 23-2 23.3
The purchaser has read and acknowledged Factory Direct Hearing s Terms of Service as outlined on our website:
 FACTORY DIRECT HEARING BILL OF SALE 1. Terms of Service The purchaser has read and acknowledged Factory Direct Hearing s Terms of Service as outlined on our website: www.factorydirecthearing.com 2. Warranties
FACTORY DIRECT HEARING BILL OF SALE 1. Terms of Service The purchaser has read and acknowledged Factory Direct Hearing s Terms of Service as outlined on our website: www.factorydirecthearing.com 2. Warranties
BlueCHiP for Medicare Not applicable
 Medical Coverage Policy Hearing Aid Mandate EFFECTIVE DATE: 01 14 2014 POLICY LAST UPDATED: 09 04 2018 OVERVIEW As defined by the Mandate, "hearing aid is any nonexperimental, wearable instrument or device
Medical Coverage Policy Hearing Aid Mandate EFFECTIVE DATE: 01 14 2014 POLICY LAST UPDATED: 09 04 2018 OVERVIEW As defined by the Mandate, "hearing aid is any nonexperimental, wearable instrument or device
Archived SECTION 19 - PROCEDURE CODES. Section 19 - Procedure Codes
 SECTION 19 - PROCEDURE CODES 19.1 CPT CODES (TEXT DELETED 9/08)... 2 19.2 PARTICIPANT COPAY (TEXT DELETED 12/10)... 2 19.3 PROCEDURE CODES... 2 19.4 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND
SECTION 19 - PROCEDURE CODES 19.1 CPT CODES (TEXT DELETED 9/08)... 2 19.2 PARTICIPANT COPAY (TEXT DELETED 12/10)... 2 19.3 PROCEDURE CODES... 2 19.4 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND
NEW YORK STATE MEDICAID PROGRAM HEARING AID PRIOR APPROVAL GUIDELINES
 NEW YORK STATE MEDICAID PROGRAM HEARING AID PRIOR APPROVAL GUIDELINES Version 2015 1 (10/1/2015) Page 1 of 12 TABLE OF CONTENTS Section I - Purpose Statement... 3 Section II - Instructions for Obtaining
NEW YORK STATE MEDICAID PROGRAM HEARING AID PRIOR APPROVAL GUIDELINES Version 2015 1 (10/1/2015) Page 1 of 12 TABLE OF CONTENTS Section I - Purpose Statement... 3 Section II - Instructions for Obtaining
Head & Neck Institute. Hearing Aid Guide. Achieve a world of better hearing.
 Head & Neck Institute Hearing Aid Guide Achieve a world of better hearing. Good hearing is part of a full and active life. Let us help you achieve a world of better hearing. The Right Choice. Cleveland
Head & Neck Institute Hearing Aid Guide Achieve a world of better hearing. Good hearing is part of a full and active life. Let us help you achieve a world of better hearing. The Right Choice. Cleveland
Choice, Service, Savings. To help you enroll, the following pages outline your company's dental plan and address any questions you may have.
 Dental Plan Design for: San Jose Convention & Visitors Bureau Effective Date: March 1, 2000 Amendment Effective Date ± : November 1, 2017 Date Prepared: January 4, 2018 Choice, Service, Savings. To help
Dental Plan Design for: San Jose Convention & Visitors Bureau Effective Date: March 1, 2000 Amendment Effective Date ± : November 1, 2017 Date Prepared: January 4, 2018 Choice, Service, Savings. To help
MEDICAID PRIOR AUTHORIZATION TRANSITION
 MEDICAID PRIOR AUTHORIZATION TRANSITION Prepared for: Mississippi Medicaid Hearing Providers November 2013 December 1, 2013 The Road Ahead 12/8/2013 HEARING PROVIDER PRESENTATION 2 Today s Goals and Objectives
MEDICAID PRIOR AUTHORIZATION TRANSITION Prepared for: Mississippi Medicaid Hearing Providers November 2013 December 1, 2013 The Road Ahead 12/8/2013 HEARING PROVIDER PRESENTATION 2 Today s Goals and Objectives
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: PA.010.MH Last Review Date: 05/11/2017 Effective Date: 07/01/2017
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Last Review Date: 05/11/2017 Effective Date: 07/01/2017 PA.010.MH Durable Medical Equipment, Corrective Appliances and This policy applies to the following
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Last Review Date: 05/11/2017 Effective Date: 07/01/2017 PA.010.MH Durable Medical Equipment, Corrective Appliances and This policy applies to the following
Archived 19.1 CPT CODES PROCEDURE CODES HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 12
 SECTION 19 - PROCEDURE CODES 19.1 CPT CODES... 2 19.2 PROCEDURE CODES... 2 19.3 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 12 Hing Aid Manual 1-01##2009 SECTION 19-PROCEDURE CODES Procedure
SECTION 19 - PROCEDURE CODES 19.1 CPT CODES... 2 19.2 PROCEDURE CODES... 2 19.3 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 12 Hing Aid Manual 1-01##2009 SECTION 19-PROCEDURE CODES Procedure
Appendix C NEWBORN HEARING SCREENING PROJECT
 Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Section Prosthetic and Assistive Devices
 The WSIB may pay for the provision, replacement, or repair of hearing aids and related accessories, and hearing assistive technologies where entitlement has been established for work-related traumatic
The WSIB may pay for the provision, replacement, or repair of hearing aids and related accessories, and hearing assistive technologies where entitlement has been established for work-related traumatic
CAA and SAC 2017 Fall Meeting with the Federal Healthcare Partnership
 CAA and SAC 2017 Fall Meeting with the Federal Healthcare Partnership NIHB/CAF/VAC 1. I would like clarification on entry level 1 vs entry level 2. My understanding is that NIHB always gets entry level
CAA and SAC 2017 Fall Meeting with the Federal Healthcare Partnership NIHB/CAF/VAC 1. I would like clarification on entry level 1 vs entry level 2. My understanding is that NIHB always gets entry level
APPLICATION INSTRUCTIONS
 APPLICATION INSTRUCTIONS This application is a six (6) page document dated 8/2015 1. Pages 1 and 2 of the application is the INFORMATION FOR PARENT/GUARDIAN to read and keep... 2. Pages 5 and 6 of the
APPLICATION INSTRUCTIONS This application is a six (6) page document dated 8/2015 1. Pages 1 and 2 of the application is the INFORMATION FOR PARENT/GUARDIAN to read and keep... 2. Pages 5 and 6 of the
Deductible 3 Individual $50 $50. Annual Maximum Benefit: Per Individual $2,000 $2,000
 Dental Plan Design for: Ector County Independent School District Original Plan Effective Date: January 1, 2018 Network: PDP Plus The Preferred Dentist Program was designed to help you get the dental care
Dental Plan Design for: Ector County Independent School District Original Plan Effective Date: January 1, 2018 Network: PDP Plus The Preferred Dentist Program was designed to help you get the dental care
Section. 23Hearing Aid and Audiometric. Evaluations
 Section 23Hearing Aid and Audiometric Evaluations 23 23.1 Enrollment...................................................... 23-2 23.1.1 Medicaid Managed Care Enrollment............................... 23-2
Section 23Hearing Aid and Audiometric Evaluations 23 23.1 Enrollment...................................................... 23-2 23.1.1 Medicaid Managed Care Enrollment............................... 23-2
Clinical Policy: Cochlear Implant Replacements
 Clinical Policy: Reference Number: CP.MP.14 Last Review Date: 07/18 Revision Log Coding Implications See Important Reminder at the end of this policy for important regulatory and legal information. Description
Clinical Policy: Reference Number: CP.MP.14 Last Review Date: 07/18 Revision Log Coding Implications See Important Reminder at the end of this policy for important regulatory and legal information. Description
PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS. LCB File No. R July 6, 2001
 PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS LCB File No. R062-01 July 6, 2001 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted. AUTHORITY:
PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS LCB File No. R062-01 July 6, 2001 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted. AUTHORITY:
Purpose of Session. Discuss. Review. Medicare audiology coverage policy. Issues raised by transmittals Possible outcomes 11/24/2008
 Purpose of Session Review Medicare audiology coverage policy 2008 Medicare audiologytransmittals Discuss Issues raised by transmittals Possible outcomes 1 Three Audiology Update Transmittals Transmittal
Purpose of Session Review Medicare audiology coverage policy 2008 Medicare audiologytransmittals Discuss Issues raised by transmittals Possible outcomes 1 Three Audiology Update Transmittals Transmittal
hi HealthInnovations TM Bill of Sale
 hi HealthInnovations TM Bill of Sale EAR MOLDS AND ACCESSORIES 1. EARMOLDS. The hi BTE power and hi BTE power plus models require ear molds. Ear molds are prepared and provided separately from the hi BTE
hi HealthInnovations TM Bill of Sale EAR MOLDS AND ACCESSORIES 1. EARMOLDS. The hi BTE power and hi BTE power plus models require ear molds. Ear molds are prepared and provided separately from the hi BTE
Clinical Policy: Cochlear Implant Replacements Reference Number: CP.MP.14
 Clinical Policy: Reference Number: CP.MP.14 Effective Date: 02/09 Last Review Date: 09/17 Revision Log Coding Implications See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CP.MP.14 Effective Date: 02/09 Last Review Date: 09/17 Revision Log Coding Implications See Important Reminder at the end of this policy for important regulatory and
New patients approved for the Novo Nordisk PAP may only be eligible for insulin vials. For a full list of available products, please visit:
 The Novo Nordisk Diabetes Patient Assistance Program (PAP) provides medication to qualifying applicants at no charge. If the applicant qualifies under the Novo Nordisk Diabetes PAP guidelines, a 120-day
The Novo Nordisk Diabetes Patient Assistance Program (PAP) provides medication to qualifying applicants at no charge. If the applicant qualifies under the Novo Nordisk Diabetes PAP guidelines, a 120-day
Cochlear Implant Corporate Medical Policy
 Cochlear Implant Corporate Medical Policy File Name: Cochlear Implant & Aural Rehabilitation File Code: UM.REHAB.06 Origination: 03/2015 Last Review: 01/2019 Next Review: 01/2020 Effective Date: 04/01/2019
Cochlear Implant Corporate Medical Policy File Name: Cochlear Implant & Aural Rehabilitation File Code: UM.REHAB.06 Origination: 03/2015 Last Review: 01/2019 Next Review: 01/2020 Effective Date: 04/01/2019
Archived 19.1 PROCEDURE CODES HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14
 SECTION 19 - PROCEDURE CODES 19.1 PROCEDURE CODES... 2 19.2 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14 1 SECTION 19-PROCEDURE CODES Procedure codes used by MO HealthNet are identified
SECTION 19 - PROCEDURE CODES 19.1 PROCEDURE CODES... 2 19.2 HCY PROCEDURE CODES FOR PARTICIPANTS 20 YEARS OLD AND UNDER... 14 1 SECTION 19-PROCEDURE CODES Procedure codes used by MO HealthNet are identified
Hearing Aid Loaner Program
 Leadership Project Committee Members: Teresa Garcia Sachin Pavithran Robert Robinson Andrew Cobabe Hearing Aid Loaner Program According to the Joint Committee on Infant Hearing, all infants with confirmed
Leadership Project Committee Members: Teresa Garcia Sachin Pavithran Robert Robinson Andrew Cobabe Hearing Aid Loaner Program According to the Joint Committee on Infant Hearing, all infants with confirmed
about your benefits and how to find a network provider for all of your
 GM Benefits & Services Center gmbenefits.com 1-800-489-4646 nternational Access Dial AT&T Direct" Access Code then 877-833-9900 TTY Service for Hearing or Speech mpaired 1-877 -34 7-5225 June 18 2012 Dear
GM Benefits & Services Center gmbenefits.com 1-800-489-4646 nternational Access Dial AT&T Direct" Access Code then 877-833-9900 TTY Service for Hearing or Speech mpaired 1-877 -34 7-5225 June 18 2012 Dear
RESIDENTIAL SERVICE PROTECTION FUND
 RESIDENTIAL SERVICE PROTECTION FUND 759.685 Surcharge assessed on retail telecommunications subscribers; rules. (1)(a) In order to fund the programs provided in sections 2 to 6, chapter 290, Oregon Laws
RESIDENTIAL SERVICE PROTECTION FUND 759.685 Surcharge assessed on retail telecommunications subscribers; rules. (1)(a) In order to fund the programs provided in sections 2 to 6, chapter 290, Oregon Laws
In-Network % of Negotiated Fee * % of Negotiated Fee * 100% 80% 50%
 Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major Restorative (bridges,
Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major Restorative (bridges,
UARTERLY ENTAL. Welcome to the New Dental Newsletter ACS FIELD REPRESENTATIVE VISITS
 Volume 1, Issue 1 April 200 ENTAL UARTERLY Welcome to the New Dental Newsletter Inside This Issue Introduction and Welcome ACS Field Representative Support and Visits Online Remittance Advices Medifax
Volume 1, Issue 1 April 200 ENTAL UARTERLY Welcome to the New Dental Newsletter Inside This Issue Introduction and Welcome ACS Field Representative Support and Visits Online Remittance Advices Medifax
TELEPHONIC COMMUNICATION DEVICE LOAN APPLICATION. Personal Information. Date of Application. City County State Zip Code
 West Virginia Commission for the Deaf and Hard-of-Hearing 405 Capitol Street, Suite 800 Charleston, West Virginia 25301 (304) 558-1675 or (866) 461-3578 TELEPHONIC COMMUNICATION DEVICE LOAN APPLICATION
West Virginia Commission for the Deaf and Hard-of-Hearing 405 Capitol Street, Suite 800 Charleston, West Virginia 25301 (304) 558-1675 or (866) 461-3578 TELEPHONIC COMMUNICATION DEVICE LOAN APPLICATION
Assistive Technology for Early Intervention
 AT Assistive Technology for Early Intervention Designated Service Coordinator Training Supporting Families who have children who are deaf, hard of hearing, visually impaired, blind or deaf-blind AT Authorizations
AT Assistive Technology for Early Intervention Designated Service Coordinator Training Supporting Families who have children who are deaf, hard of hearing, visually impaired, blind or deaf-blind AT Authorizations
PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL
 PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 PHYSICAL MEDICINE AND REHABILITATION Table of Contents 30.1 Enrollment......................................................................
PHYSICAL MEDICINE AND REHABILITATION CSHCN SERVICES PROGRAM PROVIDER MANUAL NOVEMBER 2017 CSHCN PROVIDER PROCEDURES MANUAL NOVEMBER 2017 PHYSICAL MEDICINE AND REHABILITATION Table of Contents 30.1 Enrollment......................................................................
IC ARTICLE 20. HEARING AID DEALERS. IC Chapter 1. Regulation of Hearing Aid Dealers; Creation of Advisory Committee; Certificates
 IC 25-20 ARTICLE 20. HEARING AID DEALERS IC 25-20-1 Chapter 1. Regulation of Hearing Aid Dealers; Creation of Advisory Committee; Certificates IC 25-20-1-1 Definitions Sec. 1. Except as the context requires
IC 25-20 ARTICLE 20. HEARING AID DEALERS IC 25-20-1 Chapter 1. Regulation of Hearing Aid Dealers; Creation of Advisory Committee; Certificates IC 25-20-1-1 Definitions Sec. 1. Except as the context requires
Keeping Track Section 1 1
 Keeping Track Section 1 1 Keeping Track Alberta Hands & Voices Parent Toolkit Keeping Track The Keeping Track section is intended to help you organize all of the information you are gathering. Whether
Keeping Track Section 1 1 Keeping Track Alberta Hands & Voices Parent Toolkit Keeping Track The Keeping Track section is intended to help you organize all of the information you are gathering. Whether
School Based Services Date: April 1, 2018 Page 20
 2.4 SPEECH, LANGUAGE AND HEARING THERAPY (INCLUDES ASSISTIVE TECHNOLOGY DEVICE SERVICES) 2.4.A. SPEECH, LANGUAGE AND HEARING THERAPY Speech, language and hearing therapy must be a diagnostic or corrective
2.4 SPEECH, LANGUAGE AND HEARING THERAPY (INCLUDES ASSISTIVE TECHNOLOGY DEVICE SERVICES) 2.4.A. SPEECH, LANGUAGE AND HEARING THERAPY Speech, language and hearing therapy must be a diagnostic or corrective
Lions Sight & Hearing Foundation Phone: Fax: Hearing Aid: Request for assistance
 Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
Lions Sight & Hearing Foundation Phone: 602-954-1723 Fax: 602-954-1768 Hearing Aid: Request for assistance 3427 N 32 nd Street office use only Date received Case number Applicant: (Name; please print clearly)
PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS. LCB File No. R February 29, 2000
 PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS LCB File No. R020-00 February 29, 2000 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted.
PROPOSED REGULATION OF THE BOARD OF HEARING AID SPECIALISTS LCB File No. R020-00 February 29, 2000 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted.
MetLife Dental Insurance Plan Summary. In-Network % of Negotiated Fee * % of R&C Fee 100% 100% 80% 80% 50% 50%
 TriNet IV, Inc. Classic Option LA, MS, MT& TX Employees Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major Restorative
TriNet IV, Inc. Classic Option LA, MS, MT& TX Employees Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major Restorative
Amplifon Hearing Health Care. Process & FAQ Guide. Miracle-Ear
 Amplifon Hearing Health Care Process & FAQ Guide Miracle-Ear Discount & Funded February 15, 2018 Table of Contents About Amplifon and Processes....... 2 Discount Plan.. 2 Funded Plan.... 3 Referrals......
Amplifon Hearing Health Care Process & FAQ Guide Miracle-Ear Discount & Funded February 15, 2018 Table of Contents About Amplifon and Processes....... 2 Discount Plan.. 2 Funded Plan.... 3 Referrals......
PLAN OPTION 1. Network Select Plan. Out-of-Network % of R&C Fee **
 Harvest Management Sub LLC. dba Holiday Retirement Dental Metropolitan Life Insurance Company Network: PDP Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic (fillings, extractions)
Harvest Management Sub LLC. dba Holiday Retirement Dental Metropolitan Life Insurance Company Network: PDP Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic (fillings, extractions)
Application for Wireless Equipment
 Colorado Telecommunications Equipment Distribution Program (TEDP) Application for Wireless Equipment This is an application for qualified citizens to receive wireless telecommunications equipment. If you
Colorado Telecommunications Equipment Distribution Program (TEDP) Application for Wireless Equipment This is an application for qualified citizens to receive wireless telecommunications equipment. If you
Chapter 87 *** SPEECH-LANGUAGE PATHOLOGISTS AND AUDIOLOGISTS *** (1) "Audiologist" means a person licensed to practice audiology under this chapter.
 Audiologist means a person licensed to practice audiology under this chapter.") Chapter 87 *** SPEECH-LANGUAGE PATHOLOGISTS AND AUDIOLOGISTS *** Sec. X 26 V.S.A. 4451 is amended to read: Definitions As used in this chapter: (1) "Audiologist" means a person licensed to practice audiology
Chapter 87 *** SPEECH-LANGUAGE PATHOLOGISTS AND AUDIOLOGISTS *** Sec. X 26 V.S.A. 4451 is amended to read: Definitions As used in this chapter: (1) "Audiologist" means a person licensed to practice audiology
Amplifon Hearing Health Care
 Amplifon Hearing Health Care Myamplifonusa.com Quick Guide Miracle-Ear July, 2016 Myamplifonusa.com User Guide The Myamplifonusa.com system was created to give you easy access to view Amplifon referrals,
Amplifon Hearing Health Care Myamplifonusa.com Quick Guide Miracle-Ear July, 2016 Myamplifonusa.com User Guide The Myamplifonusa.com system was created to give you easy access to view Amplifon referrals,
FOR QUESTIONS PLEASE CONTACT US AT
 MAGNETIC BONE- ANCHORED HEARING SYSTEM (BAHS) EFFECTIVE JANUARY 2018 Medtronic provides this information for your convenience only. It does not constitute legal advice or a recommendation regarding clinical
MAGNETIC BONE- ANCHORED HEARING SYSTEM (BAHS) EFFECTIVE JANUARY 2018 Medtronic provides this information for your convenience only. It does not constitute legal advice or a recommendation regarding clinical
UNOFFICIAL COPY OF HOUSE BILL 1329 A BILL ENTITLED
 UNOFFICIAL COPY OF HOUSE BILL 1329 J2 6lr1558 CF 6lr1733 By: Delegate Hubbard Introduced and read first time: February 10, 2006 Assigned to: Health and Government Operations 1 AN ACT concerning A BILL
UNOFFICIAL COPY OF HOUSE BILL 1329 J2 6lr1558 CF 6lr1733 By: Delegate Hubbard Introduced and read first time: February 10, 2006 Assigned to: Health and Government Operations 1 AN ACT concerning A BILL
PLAN OPTION 1 Low Plan Employees (30 hours) Out-of-Network % of Negotiated Fee*
 Out-of-Network % of Negotiated Fee*") Green Dot Public Schools MetLife Dental Insurance Plan Summary Network: PDP PLAN OPTION 1 Low Plan Employees (30 hours) PLAN OPTION 2 High Plan Employees (30 hours) Coverage Type In-Network Fee * Out-of-Network
Green Dot Public Schools MetLife Dental Insurance Plan Summary Network: PDP PLAN OPTION 1 Low Plan Employees (30 hours) PLAN OPTION 2 High Plan Employees (30 hours) Coverage Type In-Network Fee * Out-of-Network
MENTORPROMISE AND MENTORPROMISE ENHANCED PROTECTION PLAN
 MENTORPROMISE AND MENTORPROMISE ENHANCED PROTECTION PLAN FOR MEMORYGEL BREAST IMPLANTS AND MEMORYSHAPE BREAST IMPLANTS This document describes the Mentor Worldwide LLC ( Mentor ) Product Replacement Policy
MENTORPROMISE AND MENTORPROMISE ENHANCED PROTECTION PLAN FOR MEMORYGEL BREAST IMPLANTS AND MEMORYSHAPE BREAST IMPLANTS This document describes the Mentor Worldwide LLC ( Mentor ) Product Replacement Policy
ROYAL CANADIAN MOUNTED POLICE PAGE 1 PRINT DATE: JULY 03, 2018 BENEFIT GRID
 ************************************************************************************************************************************************************************************************* * CUSTOMER...RCMP/GRC
************************************************************************************************************************************************************************************************* * CUSTOMER...RCMP/GRC
Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP Your Network: California Care HMO
 Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Anthem Blue Cross Your Plan: Premier HMO 20/200 admit/100 OP Your Network: California Care HMO This summary of benefits is a brief outline of coverage, designed to help you with the selection process.
Application for Wireless Equipment
 Colorado Communications Technology Program (CTP) Application for Wireless Equipment This is an application for qualified citizens to receive wireless telecommunications equipment. If you are eligible,
Colorado Communications Technology Program (CTP) Application for Wireless Equipment This is an application for qualified citizens to receive wireless telecommunications equipment. If you are eligible,
MENTOR PROMISE AND MENTOR PROMISE ENHANCED PROTECTION PLAN
 MENTOR PROMISE AND MENTOR PROMISE ENHANCED PROTECTION PLAN FOR MEMORYGEL BREAST IMPLANTS, MEMORYGEL XTRA BREAST IMPLANTS AND MEMORYSHAPE BREAST IMPLANTS This document describes the Mentor Worldwide LLC
MENTOR PROMISE AND MENTOR PROMISE ENHANCED PROTECTION PLAN FOR MEMORYGEL BREAST IMPLANTS, MEMORYGEL XTRA BREAST IMPLANTS AND MEMORYSHAPE BREAST IMPLANTS This document describes the Mentor Worldwide LLC
APPLICATION FOR NORTH DAKOTA TELECOMMUNICATIONS EQUIPMENT DISTRIBUTION SERVICE
 APPLICATION FOR NORTH DAKOTA TELECOMMUNICATIONS EQUIPMENT DISTRIBUTION SERVICE Personal Information Name: Date: Mailing Address: Street Address, if different (must include): City: State: ND Zip: County:
APPLICATION FOR NORTH DAKOTA TELECOMMUNICATIONS EQUIPMENT DISTRIBUTION SERVICE Personal Information Name: Date: Mailing Address: Street Address, if different (must include): City: State: ND Zip: County:
MODEL SUPERBILL for AUDIOLOGY
 MODEL SUPERBILL for AUDIOLOGY The following is a model of a superbill which could be used by an audiology practice when billing private health plans. This sample is not meant to dictate which services
MODEL SUPERBILL for AUDIOLOGY The following is a model of a superbill which could be used by an audiology practice when billing private health plans. This sample is not meant to dictate which services
tation DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE EFFECTIVE DATE: April 8, 2014 BY:
 tation DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE DATE OF ISSUE: April 8, 2014 EFFECTIVE DATE: April 8, 2014 NUMBER 00-14-04 SUBJECT: Accessibility of Intellectual
tation DEVELOPMENTAL PROGRAMS BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE DATE OF ISSUE: April 8, 2014 EFFECTIVE DATE: April 8, 2014 NUMBER 00-14-04 SUBJECT: Accessibility of Intellectual
Dental. Lower Colorado River Authority. Network: PDP Plus. L i s t o f P r i m a r y C o v e r e d S e r v i c e s & L i m i t a t i o n s.
 Lower Colorado River Authority Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions)
Lower Colorado River Authority Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions)
In-Network 70% Deductible Individual $25 $50 Annual Maximum Benefit Per Person $2,000 $2,000
 UC Berkeley Student Health Insurance Plan (SHIP) Group Number: 151675 MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative
UC Berkeley Student Health Insurance Plan (SHIP) Group Number: 151675 MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative
Therapy Services INDIANA HEALTH COVERAGE PROGRAMS. Copyright 2017 DXC Technology Company. All rights reserved.
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Therapy Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 9 P U B L I S H E D : A U G U S T 1, 2 0 1 7 P O L I C I E
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Therapy Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 4 9 P U B L I S H E D : A U G U S T 1, 2 0 1 7 P O L I C I E
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Rehabilitative Therapy Services
 Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Fee-for-Service Provider Manual Rehabilitative Therapy Services Updated 12.2015 PART II (PHYSICAL THERAPY, OCCUPATIONAL THERAPY, SPEECH/LANGUAGE PATHOLOGY) Introduction Section BILLING INSTRUCTIONS Page
Dental. Ingredion Corporation. Network: PDP. In-Network. Out-of-Network. Coverage Type. Metropolitan Life Insurance Company
 Ingredion Corporation Dental Metropolitan Life Insurance Company Network: PDP Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major
Ingredion Corporation Dental Metropolitan Life Insurance Company Network: PDP Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings, extractions) Type C: Major
MetLife Dental Insurance Plan Summary
 Northshore School District MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Level 1 % of Negotiated 99% of R&C * % of Negotiated Level 2 99% of R&C * Type A: Preventive (cleanings,
Northshore School District MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Level 1 % of Negotiated 99% of R&C * % of Negotiated Level 2 99% of R&C * Type A: Preventive (cleanings,
Cochlear Implant Candidacy Programming Protocol, Adult Ear & Hearing Center for Neurosciences
 Cochlear Implant Candidacy Programming Protocol, Adult Ear & Hearing Center for Neurosciences Activation of the Cochlear Implant (CI) is performed by the Audiologist 2-6 weeks following surgery. While
Cochlear Implant Candidacy Programming Protocol, Adult Ear & Hearing Center for Neurosciences Activation of the Cochlear Implant (CI) is performed by the Audiologist 2-6 weeks following surgery. While
The Savvy Hearing Aid Consumer. Gloria Garner, Au.D. Doctor of Audiology University Hospital Speech & Hearing Center
 The Savvy Hearing Aid Consumer Gloria Garner, Au.D. Doctor of Audiology University Hospital Speech & Hearing Center Agenda Prevalence, Symptoms and Causes of Hearing Loss Impact of Hearing Loss Ten Tips
The Savvy Hearing Aid Consumer Gloria Garner, Au.D. Doctor of Audiology University Hospital Speech & Hearing Center Agenda Prevalence, Symptoms and Causes of Hearing Loss Impact of Hearing Loss Ten Tips
Physician Injectable Drug List (PIDL) Department for Medicaid Services, HP, and Magellan Rx Management June 1, 2010
 Department for Medicaid Services, HP, and Magellan Rx Management June 1, 2010") Physician Injectable Drug List (PIDL) Department for Medicaid Services, HP, and Magellan Rx Management June 1, 2010 Physician-Administered Drugs Physician-administered drugs are drugs, other than vaccines,
Physician Injectable Drug List (PIDL) Department for Medicaid Services, HP, and Magellan Rx Management June 1, 2010 Physician-Administered Drugs Physician-administered drugs are drugs, other than vaccines,
Hearing Aids and Assistive Listening Devices
 Hearing Aids and Assistive Listening Devices Audiological Rehabilitation Three Goals of Hearing Aid Fitting Increase strength of to make it audible Shape the signal to match the Protect the ear from loudness
Hearing Aids and Assistive Listening Devices Audiological Rehabilitation Three Goals of Hearing Aid Fitting Increase strength of to make it audible Shape the signal to match the Protect the ear from loudness
3. How does your state collect these results? (Check all that apply.) collecting this information.
 collecting this information.") NEWBORN HEARING SCREENING SURVEY Please send completed survey to: Janet Farrell Massachusetts Department of Public Health Bureau of Family and Community Health 250 Washington Street, 4 th Floor Boston,
NEWBORN HEARING SCREENING SURVEY Please send completed survey to: Janet Farrell Massachusetts Department of Public Health Bureau of Family and Community Health 250 Washington Street, 4 th Floor Boston,
Group Hospitalization and Medical Services, Inc., doing business as CareFirst BlueCross BlueShield
 Group Hospitalization and Medical Services, Inc. doing business as CareFirst BlueCross BlueShield 840 First Street, NE Washington, DC 20065 202-479-8000 An independent licensee of the Blue Cross and Blue
Group Hospitalization and Medical Services, Inc. doing business as CareFirst BlueCross BlueShield 840 First Street, NE Washington, DC 20065 202-479-8000 An independent licensee of the Blue Cross and Blue
PLAN OPTION 1 High Plan. Out-of-Network % of R&C Fee ** % of Negotiated
 Clearway Energy Group LLC Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type In-Network % of Negotiated Fee * PLAN OPTION 1 High Plan In-Network Out-of-Network % of R&C Fee ** %
Clearway Energy Group LLC Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type In-Network % of Negotiated Fee * PLAN OPTION 1 High Plan In-Network Out-of-Network % of R&C Fee ** %
In-Network 100% 80% 50% 40%
 DriveTime Automotive Group, Inc. Dental Network: PDP Plus Standard Plan Coverage Type Type A: Preventive (cleanings, exams, X-rays, composite fillings ) Type B: Basic Restorative (extractions, endodontics,
DriveTime Automotive Group, Inc. Dental Network: PDP Plus Standard Plan Coverage Type Type A: Preventive (cleanings, exams, X-rays, composite fillings ) Type B: Basic Restorative (extractions, endodontics,
Medicaid Provider Manual
 2.4 SPEECH, LANGUAGE AND HEARING THERAPY (INCLUDES ASSISTIVE TECHNOLOGY DEVICE SERVICES) 2.4.A. SPEECH, LANGUAGE AND HEARING THERAPY Definition Prescription Provider Qualifications Evaluations for Speech
2.4 SPEECH, LANGUAGE AND HEARING THERAPY (INCLUDES ASSISTIVE TECHNOLOGY DEVICE SERVICES) 2.4.A. SPEECH, LANGUAGE AND HEARING THERAPY Definition Prescription Provider Qualifications Evaluations for Speech
SCHOOL AUDIOLOGIST STATE STANDARDS CHECKLIST Aurora Public Schools Induction Program
 The Aurora Public Schools (APS) Induction Program is designed to assist School Audiologists in meeting the Colorado Department of Education Colorado Licensing Act of 1991. This checklist serves as documentation
The Aurora Public Schools (APS) Induction Program is designed to assist School Audiologists in meeting the Colorado Department of Education Colorado Licensing Act of 1991. This checklist serves as documentation
HIGH OPTION PLAN for Eligible Part and Full-Time Employees Excluding Employees Residing in Mississippi or Texas. Out-of-Network.
 Dental Insurance Plan Summary Excluding Employees Residing in Mississippi or Texas Network: PDP Plus HIGH OPTION PLAN for Eligible Part and Full-Time Employees Excluding Employees Residing in Mississippi
Dental Insurance Plan Summary Excluding Employees Residing in Mississippi or Texas Network: PDP Plus HIGH OPTION PLAN for Eligible Part and Full-Time Employees Excluding Employees Residing in Mississippi
MetLife Dental Insurance Plan Summary
 Public School Retirement System of the City of St Louis For MS and TX residents MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams) Type B: Basic
Public School Retirement System of the City of St Louis For MS and TX residents MetLife Dental Insurance Plan Summary Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams) Type B: Basic
IMPLANTABLE MAGNETIC TRANSCUTANEOUS BONE CONDUCTION HEARING SYSTEM REIMBURSEMENT CODING GUIDE
 IMPLANTABLE MAGNETIC TRANSCUTANEOUS BONE CONDUCTION HEARING SYSTEM REIMBURSEMENT CODING GUIDE This document provides general reimbursement information to assist in obtaining coverage and reimbursement
IMPLANTABLE MAGNETIC TRANSCUTANEOUS BONE CONDUCTION HEARING SYSTEM REIMBURSEMENT CODING GUIDE This document provides general reimbursement information to assist in obtaining coverage and reimbursement
Dental. EAG, Inc. - All locations except Easton & Columbia. Network: PDP Plus. In-Network. Out-of-Network. Coverage Type
 EAG, Inc. - All locations except Easton & Columbia Dental Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) In-Network Out-of-Network % of Negotiated Fee * % of R&C Fee ** 100%
EAG, Inc. - All locations except Easton & Columbia Dental Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) In-Network Out-of-Network % of Negotiated Fee * % of R&C Fee ** 100%
Title 32: PROFESSIONS AND OCCUPATIONS
 Title 32: PROFESSIONS AND OCCUPATIONS Chapter 137: BOARD OF SPEECH, AUDIOLOGY AND HEARING Table of Contents Subchapter 1. GENERAL PROVISIONS... 3 Section 17101. DEFINITIONS... 3 Section 17102. INDIVIDUAL
Title 32: PROFESSIONS AND OCCUPATIONS Chapter 137: BOARD OF SPEECH, AUDIOLOGY AND HEARING Table of Contents Subchapter 1. GENERAL PROVISIONS... 3 Section 17101. DEFINITIONS... 3 Section 17102. INDIVIDUAL
In-Network 100% 100% 50% 50% Deductible Individual $50 $50 Family $150 $150 Annual Maximum Benefit Per Person $1,250 $1,250
 Douglas County School System Low Dental Plan Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings,
Douglas County School System Low Dental Plan Dental Metropolitan Life Insurance Company Network: PDP Plus Coverage Type Type A: Preventive (cleanings, exams, X-rays) Type B: Basic Restorative (fillings,