Factors That Influence Parental Follow-Up After Newborn Hearing Screening in Colorado
|
|
|
- Audrey Jennings
- 6 years ago
- Views:
Transcription
1 University of Northern Colorado Scholarship & Creative Digital UNC Capstones Student Research Factors That Influence Parental Follow-Up After Newborn Hearing Screening in Colorado Jamie Mae Walter Follow this and additional works at: Recommended Citation Walter, Jamie Mae, "Factors That Influence Parental Follow-Up After Newborn Hearing Screening in Colorado" (2017). Capstones This Text is brought to you for free and open access by the Student Research at Scholarship & Creative Digital UNC. It has been accepted for inclusion in Capstones by an authorized administrator of Scholarship & Creative Digital UNC. For more information, please contact Jane.Monson@unco.edu.
2 2017 JAMIE MAE WALTER ALL RIGHTS RESERVED
3 UNIVERSITY OF NORTHERN COLORADO Greeley, Colorado The Graduate School FACTORS THAT INFLUENCE PARENTAL FOLLOW-UP AFTER NEWBORN HEARING SCREENING IN COLORADO A Capstone Research Project Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Audiology Jamie Mae Walter College of Natural and Health Sciences School of Human Sciences Audiology & Speech-Language Sciences May 2017
4 This Capstone Project by: Jamie Mae Walter Entitled: Factors That Influence Parental Follow-Up After Newborn Hearing Screening in Colorado has been approved as meeting the requirement for the Degree of Doctor of Audiology in the College of Natural and Health Sciences in the School of Human Sciences, Program of Audiology and Speech-Language Sciences. Accepted by the Capstone Research Committee Deanna K. Meinke, Ph.D., Research Advisor Jennifer E. Weber, Au.D., Co-Research Advisor Vickie Thomson, Ph.D., Committee Member Accepted by the Graduate School Linda L. Black, Ed.D. Associate Provost and Dean Graduate School and International Admissions
5 ABSTRACT Walter, Jamie Mae. Factors That Influence Parental Follow-Up After Newborn Hearing Screening in Colorado. Unpublished Doctor of Audiology Capstone Project, University of Northern Colorado, One of the current national early hearing detection and intervention goals is to ensure that infants who do not pass their newborn hearing screening process will have a diagnostic evaluation completed before three months of age. However, data collected by the Centers for Disease Control and Prevention (2013b) in 2011 indicated states could not document that diagnostic evaluations were completed within this time frame for 43.1% of infants who needed them. The purpose of this study was to identify factors that affected the ability of parents in Colorado to obtain a rescreening after their infant s initial newborn hearing screening was not passed. Further, this study sought to identify specific factors that affected the ability of parents to obtain an audiologic diagnostic evaluation after a subsequent hearing rescreening was not passed in Colorado. A survey was developed as a factor analysis instrument for parents in Colorado whose infant did not pass the initial newborn hearing screening and/or rescreening in The surveys consisted of demographic questions as well as a series of questions prompting parents to respond regarding their experience with their infant's newborn hearing screening and follow-up. After a trial administration was completed, the survey was mailed by the Colorado Department of Public Health and Environment to 445 parents. Fifteen percent (n = 67) of the surveys were returned as undeliverable. Of the iii
6 23 completed and returned surveys, 43% (n = 10) represented families who had already obtained an appropriate follow-up. Therefore, only 57% (n = 13) of the returned surveys were included in the data analysis. Since approximately 50% of responding parents had already obtained appropriate follow-up services, it was assumed follow-up rates in Colorado might be underestimated. Therefore, simple improvements in accurate record keeping were described, which might also improve the rate of follow-up represented by data at the Colorado Department of Public Health and Environment (2004). The planned factor analysis could not be implemented due to the poor response rate and small number of actual respondents. A summary of survey responses and parent comments highlighting case examples were provided. No one factor was determined to affect parental follow-up for all families. However, five factors did affect follow-up for each family: scheduling, communication, financial, personal and emotional, and cooccurring medical barriers. Of the five factors explored through this study, scheduling barriers were the most frequently reported, influencing follow-up for parents. The second most common barrier related to communication. Given these results, simple improvements in scheduling and parent communication were recommended to improve the follow-up rate after newborn hearing screenings. iv
7 TABLE OF CONTENTS CHAPTER I. STATEMENT OF THE PROBLEM... 1 CHAPTER II. REVIEW OF THE LITERATURE... 4 Importance of Auditory Stimulation... 4 Incidence of Hearing Loss in Children... 5 Importance of Early Identification of Hearing Loss... 5 Newborn Screenings... 7 History of Newborn Hearing Screening... 7 Early Hearing Detection and Intervention Guidelines and Recommendations... 8 Early Hearing Detection and Intervention in Colorado Current Legislation and Guidelines in Colorado Gaps in Early Hearing Detection and Intervention Access Factors Contributing to Lack of Follow Up Role of Parents in the Early Hearing Detection and Intervention Process Previous Parental Studies Factor Identification CHAPTER III. METHODOLOGY Participants Survey Instrumentation Survey Procedure Data Handling and Analysis CHAPTER IV. RESULTS Survey Trial Administration and Revision Survey Response Rate and Completion Experimental Grouping Survey Analysis Summary CHAPTER V. DISCUSSION Parental Presence at Hearing Screening/Testing Parent Utilization of Resources Factors That Influence Parental Follow Up in Colorado v
8 Colorado State Reporting and Recordkeeping System Study Limitations Future Research Recommendations Summary REFERENCES APPENDIX A. INSTITUTIONAL REVIEW BOARD APPROVAL LETTERS APPENDIX B. PARENT CONSENT LETTER AND SURVEY APPENDIX C. RAW SURVEY DATA vi
9 LIST OF TABLES 1. Parental Responses from Trial Administration of Draft Survey Instrument Newborn Hearing Screening Personnel Personnel Who Provided Information Mean Responses for Communication Barriers Mean Responses for Scheduling Barriers Mean Responses for Personal and Emotional Barriers Mean Responses for Financial Barriers Mean Responses for Co-Occurring Medical Barriers Categorization of Parent Comments vii
10 LIST OF FIGURES 1. Relative percentages of barriers indicated by factor viii
11 1 CHAPTER I STATEMENT OF THE PROBLEM Early identification of hearing loss through newborn hearing screenings followed by immediate intervention has made it possible for children born with hearing deficits to achieve higher levels of spoken language and increased reading abilities and academic achievements that otherwise would not have been attainable without access to important auditory information (Flexer, 2012). To provide appropriate interventions for children with hearing loss, they must be identified as quickly as possible after birth, which can be facilitated through a newborn hearing screening. Colorado Revised Statute written in 1997 created an advisory committee on hearing--the Colorado Infant Hearing Advisory Committee (Colorado Department of Public Health and Environment [CDPHE], 2004). The purpose of the committee was to facilitate a way to collect data and provide recommendations to hospitals and healthcare institutions regarding infant hearing. The statute mandated that hearing screenings be conducted on 85% of infants born in hospitals. According to Colorado Infant Hearing Advisory Committee (CDPHE, 2004) benchmarks, 95% of all infants born in Colorado should have a newborn hearing screening before being discharged. This process begins with an initial hearing screening in the form of an automated auditory brainstem response (AABR) or otoacoustic emissions (OAE). It is recommended that infants who do not pass this screening be
12 2 brought back to the hospital for an outpatient hearing screening. At the time of rescreening, the results are interpreted as a refer (did not pass) or a pass. Infants who refer on the re-screening should have a complete audiologic diagnostic evaluation performed by an audiologist. It is important to have this evaluation completed before the infant is three months. This is necessary for the infant to receive appropriate early intervention services as well as appropriate developmental outcomes (CDPHE, 2004). The national Early Hearing Detection and Intervention (EHDI) program was established in 1999 (American Academy of Pediatrics, 2013). One of the goals of EHDI programs was to ensure infants who did not pass the hearing screening process would have a diagnostic evaluation before three months of age. However, data collected by the Centers for Disease Control and Prevention (CDC; 2013b) in 2011 indicated states could not document that diagnostic evaluations were completed within this time frame for 43.1% of infants who needed them. Parents play a large role in EHDI (American Academy of Pediatrics, 2013) process as they serve as the decision-makers for their children. Research revealed the importance of auditory stimulation for typical development and the vital need for early identification to provide this critical auditory information to children with hearing loss. Given this evidence, it was apparent that every infant who does not pass the final hearing screening should obtain an audiologic diagnostic evaluation. Furthermore, it was necessary to evaluate factors that influenced a parent s decision and ability to pursue follow up for a hearing rescreening and/or diagnostic hearing evaluation. Identification of these factors would allow for important quality improvements (QI) to be made, if necessary, to the Colorado Infant Hearing Advisory Committee guidelines for infant
13 3 hearing screening, audiologic assessment, and early intervention (CDPHE, 2004) and potentially the national EHDI process. Therefore, the following research questions guided this study: Q1 Q2 What factors influence a parent s ability to obtain a hearing rescreening for their infant once the initial newborn hearing screening is not passed? What factors influence a parent s ability to obtain a complete diagnostic audiologic evaluation for their infant once the initial newborn hearing screening and rescreening are not passed?
14 4 CHAPTER II REVIEW OF THE LITERATURE Importance of Auditory Stimulation Access to auditory information is a critical element required for the acquisition and development of language, speech, and other developmental milestones in young children. Hearing provides the foundation for social, emotional, and cognitive development as well as academic achievement for children (American Speech-Language- Hearing Association, 2004). According to Cole and Flexer (2011), acoustic stimulation is necessary for auditory pathways to mature. The maturation of these auditory pathways is a vital component for typical speech and language development. As such, normal speech and language development is not possible without adequate access to auditory information. Infants use phonetic categories obtained through consistent listening experiences to form a foundation for new words. This base of vocabulary is directly related to lexicalsemantic use as well as eventual reading and higher order language use (Cole & Flexer, 2011). Infants learn 90% of what they know about the world through consistent listening experiences known as incidental learning. Without frequent auditory stimulation and incidental learning, imperative speech and language development is delayed (Moog & Geers, 2003).
15 5 Incidence of Hearing Loss in Children According to the CDC (2013a), 1.4 per every 1,000 babies screened at birth has a hearing loss. These data were obtained through the CDC s Hearing Screening and Follow-up survey in Infants included in this statistic consisted of those who were documented as being screened at birth for a hearing loss. The type or degree of hearing loss was not indicated. The National Institute on Deafness and Other Communication Disorders (NIDCD; 2010) estimated approximately two to three of every 1,000 children born in the United States are born deaf or hard of hearing. Data currently indicate one to two of every 1,000 newborns has a bilateral severe to profound hearing loss and as many as four per every 1,000 are indicated if mild to moderate and unilateral losses are included in the data (Northern & Downs, 2014). Additionally, White (1997) reported hearing loss affects 12,000 children born in the United States each year, making it one of the most common birth defects in America. Importance of Early Identification of Hearing Loss Research by Yoshinago-Itano, Sedey, Coulter, and Mehl (1998) further confirmed the critical importance of early identification of hearing loss in children for normal speech and language development to occur. Receptive and expressive language abilities were compared for children identified with a hearing loss at or before six months of age and those who were identified after six months of age. It was determined there was a consistent advantage in language skills for the group of children who were identified before six months of age. This advantage became even more evident as the children aged (Yoshinago-Itano et al., 1998).
16 6 In addition to a notable increase in language use found in children who were identified early with a hearing loss (Yoshinago-Itano et al., 1998), children who were identified with a hearing loss late eventually fell behind their peers in language, cognition, and social-emotional development. These delays might result in fewer educational and employment opportunities in adulthood (Gallaudet University Center for Assessment and Demographic Study, 1998). Holt and Svirsky (2008) evaluated the progress of children identified with bilateral congenital profound sensorineural hearing loss and implanted with cochlear implants at various ages. Spoken language development was evaluated as a function of age at implantation. The developmental outcomes of the children identified with a hearing loss earlier were better than those children identified later. The results indicated the presence of a sensitive period for spoken language. Children who received access to important auditory information after the critical period of language development showed deficits in language usage. Sharma, Dorman, and Spahr (2002) reported the critical language learning window occurs from birth to approximately three years of age. After this time, the plasticity of the brain is reduced and children who have not acquired language during this period will experience delays. Similarly, a vital window exists for auditory neural development during the first few years of a child s life. If a hearing loss is not detected early, the lack of auditory stimulation experienced by the child might heavily affect the permanent organization of auditory brain pathways. Therefore, it is imperative for auditory neural development (Cole & Flexer, 2007) and normal language development
17 7 (Yoshinago Itano et al., 1998) that children with hearing loss are identified as early possible. Newborn Screenings Shortly after birth, newborn screenings are conducted to identify the presence of any genetic disorders that can be treated early in a child s life. Genetic testing is utilized in most newborn screenings. One common screening conducted on newborns is the blood spot test for phenylketonuria and hypothyroidism. Additional genetic screening is conducted for those identified with permanent hearing loss and for mutations of the BGJ2 Connexin 26 gene associated with sensorineural hearing loss. Newborn hearing screenings are also conducted on babies shortly after birth (Northern & Downs, 2014). The concept of screening newborns at birth to identify certain disorders or birth defects began with the implementation of the blood spot test. This test was established so doctors could detect the presence of the metabolic disorder phenylketonuria (PKU) in infants. This test is conducted within 24 to 48 hours after a child is born, through the collection of a blood spot from an infant by way of a heel stick. A laboratory analyzes the blood spot to test for biochemical and genetic markers that might indicate hidden congenital disorders. Immediate follow-up programs are provided for families and infant to perform additional diagnostic testing and deliver adequate treatment (Northern & Downs, 2014). History of Newborn Hearing Screening Currently, 97% of newborns born in the United States are screened for hearing loss before they leave the birthing hospital (CDC, 2013a). This has not always been the case, however. Years of applying various models for identification and management of
18 8 infant hearing loss led to the current prevalence of newborn hearing screenings being conducted in the United States. The current state of universal newborn hearing screenings has been carefully developed over many years for cost efficiency, time efficiency, test accuracy, and easy application (Northern & Downs, 2014). The first effort made in the direction of universal newborn hearing screening was spear-headed in 1964 by Marion Downs and a psychologist by the name of Graham Sterritt (Northern & Downs, 2014). During their project, Downs and Sterritt sought to test every baby born during a 12-month period in Denver, Colorado. The project utilized volunteers and their observation of behavioral responses of infants after the presentation of a sound stimulus. Their efforts successfully identified nine profoundly deaf infants in Denver. A few years later, the Joint Committee on Infant Hearing (JCIH) was developed and was chaired by Downs (Northern & Downs, 2014). In 1969, Downs and a national multidisciplinary committee of various representatives met to evaluate the possibility of early hearing screening for newborns. They are now known as the Joint Committee on Infant Hearing (JCIH). The JCIH met regularly after this initial meeting and proceeded to write and publish statements regarding infant hearing. Early Hearing Detection and Intervention Guidelines and Recommendations The Joint Committee on Infant Hearing published numerous documents containing recommendations for newborn hearing screening programs in America. In 1973, they published the first high-risk register for deafness (JCIH, 1973). The Rhode Island Project became the first effort by a state to meet the goals of universal newborn hearing screening in 1993 (JCIH, 1994). Within Rhode Island, eight maternity hospitals
19 9 adopted a two-tiered screening protocol that included transient evoked otoacoustic emissions (TEOAEs) as an initial screening and the auditory brainstem response (ABR) evaluation for those infants who did not pass the initial screening. As a result of these efforts in Rhode Island, the overall age of identification and age of intervention decreased across the state (Vohr, Carty, Moore, & Letourneau, 1998). The National Institutes of Health sponsored a Consensus Development Conference following the success of the newborn hearing screening project in Rhode Island (NIDCD, 2007). At the conference, it was discussed that nearly 50% of infants were being missed for hearing loss diagnosis because they did not fall in the high risk registry. It was decided newborn hearing screening protocols should be improved to ensure more infants were screened at birth. Therefore, the NIDCD (2007) released a Consensus Statement on Early Identification of Hearing Impairment in Infants and Young Children in The statement recommended universal newborn hearing screenings be implemented for all infants within the first three months of life. Additionally, it was recommended the screenings utilize the same two-stage physiologic test approach used in Rhode Island to include TEOAs initially and an ABR test if the initial screen was not passed. In 1994, following the release of the consensus statement, the JCIH (1994) released the first of three position statements endorsing the goal of universal detection of infants with hearing loss as early as possible. Additionally, they encouraged all infants be identified with hearing loss by three months of age and attain early intervention by six months. The JCIH also endorsed physiologic testing techniques established in the consensus statement and recommended continued research be conducted to evaluate
20 10 screening techniques and develop new and improved protocols. Finally, they recommended the role of deafness indicators associated with sensorineural and conductive hearing loss be expanded (JCIH, 1994). In 1999, the Newborn Hearing Screening and Intervention Act was passed, making federal grants available for the newborn hearing screening efforts in the United States. The EHDI department was established following this act. The first three goals of this department were as follows: (a) All newborns will be screened for hearing loss before one month of age, (b) All infants who screen positive will have a diagnostic audiologic evaluation before three months of age, and (c) All infants identified with a hearing loss will receive appropriate early intervention services before six months of age (National Center for Hearing Assessment and Management [NCHAM], 2015). The JCIH published a position statement in 2007 that endorsed early detection and intervention for infants with hearing loss through integrated, interdisciplinary state and national systems of universal newborn hearing screening, evaluation, and familycentered intervention (Background, para. 2). The statement endorsed the first three goals of the EHDI department and recommended that timing and number of hearing reevaluations for children with high risk factors should be customized (JCIH, 2007). Another statement was published in 2013, which stated that the ultimate goal of EHDI is to optimize language, social and literacy development of children who are deaf and hard of hearing (JCIH, 2013, Introduction, para. 1). Additionally, the statement noted most states and territories, while documenting thorough screening efforts, were unable to provide adequate documentation of outcomes that resulted from early intervention. It was estimated ¼ of children who are deaf and
21 11 hard of hearing were successfully tracked through an early intervention system. Loss to documentation and loss to follow up were crucial elements threatening the effectiveness of EHDI programs across the country (JCIH, 2013). Similarly, the American Academy of Pediatrics (2013) reported almost half of children who do not pass their newborn hearing screening lack a documented diagnosis. Early Hearing Detection and Intervention in Colorado A state-wide universal newborn hearing screening program was inaugurated in Colorado in 1992 (Northern & Downs, 2014). The program was comprised of a five-year plan that strove to implement universal newborn hearing screening in every hospital in Colorado. The program took advantage of volunteers who completed screenings under the supervision of a certified audiologist. As such, the initial expense for one screening was close to $ The success of the Colorado newborn hearing screening program demonstrated the implementation of universal newborn hearing screening could be both feasible and cost effective (Northern & Downs, 2014). At the time of the inauguration of the Colorado Newborn Hearing Screening Program (Mehl & Thomson, 2002), four Colorado hospitals voluntarily began to perform newborn hearing screenings on every infant born before they were discharged. Four years later, 26 Colorado hospitals had begun to participate in the screening program. As more hospitals began to enact mandatory newborn hearing screening protocols, data were collected, which served as a driving factor in establishing legislation to require all birthing hospitals to adopt a newborn hearing screening program. By 1999, many Colorado hospitals had initiated mandatory newborn hearing screening programs; as a result, congenital hearing loss was diagnosed in 86 newborns (Mehl & Thomson, 2002).
22 12 Mehl and Thomson (2002) evaluated the effectiveness of the Colorado Newborn Hearing Screening Project. They sought to explore the level of hospital participation as well as the general success of screening efforts. Additionally, they tracked improvements in establishing programs across Colorado and follow up for outpatients over time. They reported that between the years of 1992 and 1999, 148,240 infants were screened in Colorado. Of those newborns, 291 were diagnosed with a congenital hearing loss. Given these results, it was concluded universal newborn hearing screening was possible when efforts were made on a regional level and with legislatively mandated participations. In 2008, Christensen, Thomson, and Letson published data to indicate that between January of 2002 and December of 2004, 98% of infants born in Colorado hospitals were screened for hearing loss. Current Legislation and Guidelines in Colorado Colorado Revised Statute written in 1997 created an advisory committee on hearing--the Colorado Infant Hearing Advisory Committee (CDPHE, 2004). The purpose of the committee was to facilitate a way to collect data and provide recommendations to hospitals and health care institutions regarding infant hearing. The statute mandated that hearing screenings be conducted on 85% of infants born in hospitals. Current benchmarks outlined by the Colorado Infant Hearing Advisory Committee (CDPHE, 2004) stated that 95% of all infants born in Colorado should be screened for hearing loss prior to hospital discharge. The first step in this assessment should be a hearing screening to include an auditory brainstem response (ABR) or an evoked otoacoustic emission--either transient evoked otoacoustic emission (TEOAE) or
23 13 distortion product otoacoustic emission (DPOAE). Once the initial screening is performed, the results should be discussed with parents. If an infant does not pass the initial screening, a rescreening should be provided before discharge. If the rescreening is missed or not passed, the infant should be rescreened within two weeks of discharge. If this screening is not passed, a complete audiologic diagnostic evaluation should be completed with an audiologist. It is necessary to obtain this evaluation prior to three months of age (CDPHE, 2004). The audiologic diagnostic evaluation should include an auditory brainstem response (ABR) evaluation to a click and tone burst stimulus or an auditory steady state response (ASSR) evaluation. Further, the evaluation should include otoacoustic emission (OAE) testing and high frequency tympanometry. The results of these tests should be discussed with the parents and a report should be generated to include an interpretation of all test results. Upon a confirmed hearing loss, a referral should be made to an otolaryngologist and to the Colorado Hearing Resource (CO-Hearing) Coordinator. The CO-Hearing Coordinator contacts the family immediately after diagnosis to begin the early intervention process. Finally, an audiologic assessment reporting form must be filled out by the audiologist and submitted to the Colorado Department of Public Health and Environment to document the confirmed hearing loss with the state (CDPHE, 2004). Following a diagnosis of hearing loss, infants should be followed audiologicly every three months until they are two years old. After this, they should be followed every six months until age five (CDPHE, 2004).
24 14 Gaps in Early Hearing Detection and Intervention Access Challenges remain in terms of the EHDI process including the confirmation of a timely diagnostic evaluation for infants who do not pass the final newborn hearing screening. Although one of EHDI s goals is infants will have a diagnostic audiologic evaluation completed before three months of age, data collected by the CDC indicated in 2011 states could not document that diagnostic evaluations were completed for 43.1% of infants who needed them (CDC, 2013b). While 97.9% of all U.S. infants are documented as receiving a hearing screening before one month of age (CDC, 2013b), there is still work to be done to ensure all infants also have access to a timely diagnostic evaluation after the failing of an initial hearing screening (Northern & Downs, 2014). Factors Contributing to Lack of Follow Up The effectiveness of universal newborn hearing screening programs is dependent upon the effectiveness of a subsequent follow-up program (Northern & Downs, 2014). Many factors might account for the documented gap occurring between the newborn hearing screening and completion of a rescreening or diagnostic evaluation. Hyde (2005) reported a positive explanation of infant hearing screening results from screening personnel as well as use of informal and invalid tests of hearing by family might affect a parent s decision to pursue further testing. Shulman, Katz, Ireys, and Besculides (2006) additionally noted screening personnel often indicate a lack of urgency when reporting information about screening results to a family, which might persuade them not to obtain an immediate evaluation. Lack of appropriate equipment was also reported, which might have contributed to the absence of documented diagnostic appointments. White and
25 15 Blaiser (2011) stated a lack of thorough documentation throughout the EHDI process as well as a shortage of pediatric audiologists might contribute to the gap in this area. Russ, Hanna, DesGeorges, and Forsman (2010) pointed to the burden of traveling long distances for audiologic services, particularly from rural areas, as a possible cause for a lack of diagnostic evaluations. Young and Tattersall (2007) evaluated the responses of parents of children with hearing loss and found parents were often given inconclusive messages from screening deliverers. The possibility of deafness was not always presented to these parents, which could be another deterrent for parents who are given the decision to pursue a timely diagnostic evaluation or not. Additional factors that contributed to the lack of attendance at timely diagnostic appointments were identified by Munoz, Nelson, Goldgewicht, and Odell (2011): noncompliance on the part of the parents with regard to scheduling, the presence of middle ear fluid, additional medical conditions that require attention, and distance from the testing facility. Chapman et al. (2011) added that co-occurring birth defects might contribute to lack of diagnostic appointments. Finally, Munoz et al. (2011) noted that variability in wait times for scheduling diagnostic appointments with audiologists might present an additional challenge for parents. The National Institute on Deafness and Other Communication Disorders (n.d.) reported three methods that could be beneficial in improving the rate of diagnostic evaluations obtained by parents of children who do not pass their newborn screening. They concluded if parents fully understood their child s screening results and the importance of the diagnostic evaluation and if they were provided with necessary contact and resource information, follow-up results would increase.
26 16 Role of Parents in the Early Hearing Detection and Intervention Process Ninety percent of children who are born with a permanent hearing loss are born to hearing parents, which makes the parental experience with the EHDI process a unique one (Harlor & Bower, 2009). The period of time that lapses between the suspicion and the confirmation of a hearing loss is critically important. Decisions parents make during this time will form the foundation for later decisions made with regard to their child. Parents serve as the primary decision makers for their children and are often presented with information that can vary in nature (Matthijs et al., 2012). Additionally, even with the provision of accurate and complete information, parents often filter and accept only what they want to hear depending upon their current emotions and feelings regarding their child s hearing loss (Kurtzer-White & Luterman, 2003). Young and Tattersall (2007) reported that circumstances involving newborn hearing screenings and diagnosis have evolved with regard to early family experiences. Three primary factors were identified as causes of this change. First was the fact that discovery is now routine and driven by medical personnel instead of through parental interaction and observation (Luterman, 2001). Additionally, there is a compressed timeline parents face between birth and identification of deafness. Finally, the age of identification of hearing loss in infants occurs at a much earlier stage of the formation of a relationship than previously experienced. These factors make the present-day parental experience with the EHDI process a unique one that requires further evaluation. Given the importance of early identification of hearing loss for language, cognitive, and socio-emotional development, in addition to the reduction of the risk of lower educational and employment levels later in adulthood (Gallaudet University
27 17 Center, 1998), it is crucial that steps be made to identify factors that affect a family s access to rescreening and/or diagnostic services once an initial hearing screening is not passed. With regard to the current study, parents of children with hearing loss provided information regarding their experiences with their child s newborn hearing screening process. Factors found to be significant with regard to the parental experience with the newborn hearing screening process were extracted from the collected data. Once these factors were identified, additional steps were made to improve the EHDI process by bridging the success of universal newborn hearing screening programs and appropriate interventions with timely diagnosis. Previous Parental Studies In addition to hearing, other newborn screenings are routinely conducted shortly after a baby is born. Specifically, the majority of screenings conducted in the United States are for treatable conditions such as phenylketonuria (PKU). Phenylketonuria is a disorder relating to metabolism, which can be detected through a blood spot test. Parents were asked about their attitudes regarding newborn screenings in a study by Campbell and Ross (2003). Overall, the parents supported the idea of newborn screenings. Particularly, they reported mandatory screenings, such as hearing and the blood spot test, were important. They felt mandatory screenings were necessary because younger or less educated parents might not understand the importance of some testing. Results were obtained for this study through a focus group conducted in Chicago, Illinois. In a study conducted by Waisbren et al. (2003), researchers evaluated the impact the identification of biochemical genetic disorders had on a family. They wanted to compare how a family was affected when a false-positive result was obtained from the
28 18 screening compared to a normal result. To contact parents, the directors of metabolic centers in New England or Pennsylvania sent recruitment letters to parents of children identified with a metabolic disorder through a newborn screening. The parents were asked to complete an interview as well as the Parenting Stress Index (PSI) questionnaire. Results of the study indicated parents who had children who received a false-positive finding in a newborn screening felt anxiety when compared to those who were clinically identified with a biochemical genetic disorder (Waisbren et al., 2003). Factor Identification This study identified and illustrated the relationship between specific factors and parental ability to obtain a newborn hearing rescreen or diagnostic evaluation. Five factors were extracted from research relating directly to parents ability to obtain followup services for their infant: communication barriers, financial barriers, scheduling barriers, personal and emotional barriers, and co-occurring medical condition barriers. Survey questions were derived from these factors. Communication Barriers Young and Tattersall (2007) indicated inconclusive messages are often given to parents after their child s hearing is screened. Given this message, the possibility of deafness and the urgency of obtaining follow-up services is not always acknowledged. Hyde (2005) further illustrated screening personnel often express a sense of positivity, which does not urge parents to obtain timely services after the screening. In an overview of newborn hearing screening recommendations, the American Speech-Language-Hearing Association (ASHA; n.d.) recommended a parent/caregiver should be provided with written education materials regarding the importance of early
29 19 hearing detection and intervention, an overview of the screening process, and information about the screening and risk factors relating to late-onset hearing loss. Also, communication regarding the results should be made in a family-friendly manner and include explicit explanations about how to obtain follow-up services (JCIH, 2007). Finally, it was urged that parental and pediatrician contact information be obtained from families of newborns who did not pass the initial screening in order to prevent a loss of follow up (ASHA, n.d.) Financial Barriers Russ et al. (2010) explained experienced pediatric audiologists, of whom there is a shortage, must conduct diagnostic evaluations on newborns. Thus, families commonly have to travel extensive distances to obtain follow-up services. Several sessions are sometimes needed, which could cause a financial burden on the family. Beyond the financial burden of travel, parents of children with medical needs experience additional financial barriers. Thyen, Kuhlthau, and Perrin (1999) evaluated financial situations of parents who had children with chronic conditions. The authors concluded the care needed for the children increased the financial burden on the parents. Additionally, barriers were created for employment. This further harmed financial stability while financial needs continued to increase. This factor was evaluated to determine if financial stability or medical costs were related to access of follow-up services. Scheduling Barriers Research conducted on EHDI programs across the country concluded parents frequently experienced difficulty in identifying pediatric audiology facilities in their area
30 20 that provided the appropriate services for their infant. Further, parental compliance in scheduling was identified as the main challenge in completing timely diagnostic testing (Munoz et al., 2011). Russ et al. (2010) further explained scheduling becomes complicated for parents because longer appointments are needed to complete a sedated ABR evaluation. To decrease loss to follow up for infants who do not pass their initial hearing screening, Russ et al. (2010) recommended an appointment for a rescreening or diagnostic appointment should be made before the family leaves the hospital. Additionally, the family should be contacted by phone to verify the appointment. Personal and Emotional Barriers Parents whose children were identified early with hearing loss were asked to describe emotions experienced when they first found out their child had a hearing loss. While the majority of the parents interviewed by Young and Tattersall (2007) reflected they were glad the discovery was made early, they also expressed this knowledge came with a sense of shock, grief, and loss. One parent who was included in the study commented these emotions were especially difficult to handle because they were at a particularly vulnerable time after the birth of their child and were tired. Additionally, a mother included in the study commented on the extreme worry experienced after her child s newborn hearing screening, noting, Then we came home and rather than having the joy of bringing a new baby home, all we had in our head was worry. As such, Hyde (2005) expressed that many parents will utilize informal and invalid tests of hearing to assure themselves their child can in fact hear.
31 21 In some cases, specific religious or spiritual traditions or beliefs can affect the decisions of parents. Because prayer and alternative healing methods are often called upon before medical practices, these religious choices might affect clinical interactions. This has been recognized in other medical fields beyond audiology. For example, patients and parents frequently request for a referral to a rabbi, minister, priest, imam, shaman, or other spiritual care provider before accepting medical care from doctors (Barnes, Plotnikoff, Fox, & Pendleton, 2000). This factor was evaluated to determine if parents might have delayed an audiologic follow up due to religious or spiritual beliefs. Co-Occurring Medical Condition Barriers Nearly 40% of children born with a hearing loss have an additional disability (Gallaudet Research Institute, 2003). According to Chapman et al. (2011), the presence of additional medical conditions can exacerbate barriers in accessing timely follow-up services for children who do not pass their initial newborn hearing screening. In fact, a correlation was drawn by Chapman et al. between the delay in obtaining follow-up services and complexity of medical needs. Particularly, infants who spent time in the neonatal intensive care unit after birth were estimated to experience common delays in rescreening and diagnostic services. Further, Chapman et al. (2011) discovered infants with ear anomalies experienced significant delays in hearing loss diagnoses. In the group evaluated, only half had their hearing loss diagnosed by three months of age. Munoz et al. (2011) discovered the presence of middle ear fluid was the second most common challenge expressed by EHDI personnel in obtaining follow-up services for infants across the country. The third most
32 22 commonly expressed challenge was the presence of other medical and health complications.
33 23 CHAPTER III METHODOLOGY The purpose of this study was to identify factors that affected the ability of parents in Colorado to obtain a rescreening after their child s initial newborn hearing screening was not passed. Additionally, the aim was to identify specific factors that affected the ability of parents to obtain an audiologic diagnostic evaluation after the initial screening and/or rescreening was not passed. This chapter describes the survey methods and analysis. The research was conducted under an approved University of Northern Colorado Institutional Review Board protocol (see Appendix A). Participants Trial Administration A trial administration of the developed parental survey was conducted with three parents of children with hearing loss between the ages of three and five in northern Colorado. All three parents attended a resource group for families of children with hearing loss and their children all received newborn hearing screenings. The aim of the trial administration was to assess the length of time it took for each parent to complete the survey. Additionally, parents were asked to report their general understanding of the survey questions and provide any suggestions or clarifications if needed. The survey was modified to reflect the feedback given from the parents included in the trial administration.
34 24 Final Survey Dissemination Participants for final survey dissemination were identified through collaboration with staff at the Colorado Department of Public Health and Environment (2004). All participants were parents of children born in 2014 who did not receive appropriate audiologic services (either a hearing rescreen or diagnostic hearing testing) after an initial newborn hearing screening and/or the hearing rescreen was not passed. The CDPHE assisted the researcher in disseminating the final survey and cover letter (see Appendix B) to participants by mail. All survey participants had to be able to read and write in standard American English or Spanish as the surveys were mailed in both of these languages. In addition to the survey, a cover letter was included in the packet mailed to each participant. The cover letter asked that the survey be completed by the infant s biological parent, grandparent, or another family member/legal guardian. The mailing addresses utilized were those listed on the infant s birth certificate. Participants were informed that through the completion and submission of the survey, they acknowledged and consented to participate in the study. Therefore, a separate informed consent form was not necessary. Survey Instrumentation Survey Development The survey utilized for this study was created as a factor analysis instrument, which began with the establishment of empirical referents from previous research studies conducted in the area (Barnes et al., 2000; Chapman et al., 2011; Hyde, 2005; Munoz et al., 2011; Russ et al., 2010; Shulman et al., 2010; Thyen et al., 1999; White & Blaiser, 2011; Young & Tattersall, 2007). A set of five possible factors contributing to a lack of
35 25 parental follow up to either a hearing re-screen or an audiologic diagnostic evaluation were identified and extracted from previous studies. These factors served as the foundation for the development of the survey instrument and included scheduling barriers, communication barriers, financial barriers, personal and emotional barriers, and co-occurring medical barriers. Questions used in previous parental surveys were utilized as a reference for the development of the survey (Park, Warner, Sturgill, & Alder, 2006). All parents were asked to respond to questions about their relationship to the infant born in 2014 as well as questions about their newborn hearing screening experience. Next, the parents were provided with questions and Likert scale responses relating to the first newborn hearing screening. Those who did not obtain a hearing rescreening for their infant were asked to complete a set of Likert scale questions on the next page entitled, Hearing Rescreening. Parents who did not obtain a hearing evaluation for their infant were asked to complete a set of Likert scale questions labeled Hearing Evaluation. Respondents who obtained either a rescreening or a hearing evaluation for their infant were instructed to skip the set of questions relating to that particular event. The Likert scale was developed as a principle of measuring attitudes by requesting individuals respond to a number of statements regarding a certain topic. Each statement was accompanied by a closed set of possible responses relating to the extent to which the individual agreed with the statement. A neutral point was included to indicate the respondent neither agreed nor disagreed with the statement (McLeod, 2008). For the purpose of this study, five possible responses were provided for each statement regarding the parent s experience and access to follow-up care. For example, some questions asked
36 26 parents to rate the extent to which they agreed or disagreed with statements relating to communication with screening personnel. Finally, all participants were asked to indicate whether or not they received specific family resources after their infant did not pass their initial newborn hearing screening. Specifically, one question inquired whether or not the parent received the Roadmap for Families (Colorado Families for Hands and Voices, 2010) and another question inquired whether or not they viewed the Loss and Found (Colorado Families for Hands and Voices, 2010) video either before or after leaving the hospital. At the conclusion of the survey, all participants had the opportunity to free-write one or two additional barriers that might have prevented them from obtaining a hearing rescreening or a hearing evaluation for their infant. Survey Translation The written survey and cover letter were translated into Spanish before final dissemination. As such, the survey was administered to both English and Spanish speakers in Colorado. Survey Procedure After the survey was updated to reflect feedback provided by parents during the trial administration, the CDPHE (2004) facilitated distribution of surveys to parents in Colorado who met inclusion criteria for this study. The total number of distributed surveys was 445. Parents were asked to return their completed survey to the CDPHE within two weeks of receiving it in the mail. The researcher obtained the surveys in person from the CDPHE. A full copy of the survey and cover letter can be found in Appendix B.
37 27 Data Handling and Analysis Survey Coding and Data Analysis To protect the identity of the participants, a numerical code was assigned to each survey before dissemination. After the surveys were returned, responses were coded and entered into an Excel (Version 14.0) spreadsheet to facilitate analysis. Raw survey data are provided in Appendix C. Small Group Case Study Of the 445 surveys distributed to parents in Colorado, only 13 were returned that qualified for analysis. Because a limited number of surveys were returned, the proposed factor analysis could not be completed. Therefore, a small group case study was conducted to analyze and best reflect parental responses. Two experimental groups were utilized as case studies--the parents who were lost at the rescreen step and those who were lost at the hearing evaluation step. According to Yin (2014), case study research is utilized to contribute to knowledge about individual or group phenomena. This research design allows for analysis of one or more cases. One use of this analysis could be to study small group behavior (Yin, 2014). In the case of this study, the researcher analyzed results provided by parents to determine which pre-determined factors most significantly affected their access to follow up after a newborn hearing screening was not passed. The researcher sought to discover how these factors were different with regard to the two experimental groups. Likert scale question responses were evaluated by factor to determine the percentage of respondents from each experimental group who agreed, disagreed, or felt neutral with regard to each question. These collapsed responses were compared between
38 28 both experimental groups. To obtain the percentage of respondents who agreed to questions stating a barrier was present, the researcher altered responses for positively worded questions. Answers to positively phrased questions were evaluated as though inverse responses had been given. This indicated if the respondent agreed to a positive experience (e.g., I was provided with contact information for an audiologist) or they also disagreed with the inverse statement (e.g., I was not provided with contact information for an audiologist). To determine which factors might have had the greatest effect on follow-up, collapsed responses were assessed to determine which factors had the largest percentage of respondents who agreed barriers were present. Responses relating to the provision of the Roadmap for Families and the Loss and Found video (Colorado Families for Hands and Voices, 2010) were averaged to determine how many respondents from each experimental group received those resources. Written comments were also evaluated to determine common themes. Once two common themes were extracted from the written comments, the exact statements relating to each theme were grouped together to indicate the relative frequency the barriers included in each theme were expressed.
39 29 CHAPTER IV RESULTS The purpose of this study was to evaluate factors that affected parental follow-up after newborn hearing screening in Colorado. Specifically, this study aimed to identify self-reported factors that influenced a group of parents abilities to obtain a hearing rescreening for their infant born in 2014 once an initial newborn hearing screening was not passed. Additionally, the study assessed what factors influenced their ability to obtain a complete diagnostic hearing evaluation once the initial newborn hearing screening and/or rescreening were not passed. Survey Trial Administration and Revision A trial administration of the survey was conducted with three parents of children with hearing loss between the ages of three and five in northern Colorado. All three parents attended a resource group for families of children with hearing loss and their children all received newborn hearing screenings and diagnostic follow-up. These parents were felt to be familiar with the Colorado newborn hearing screening follow-up process. The aim of the trial administration was to assess the length of time it took for each parent to complete the survey. Additionally, parents were asked to report their general understanding of the survey questions and any suggestions or if clarification was needed. The survey was subsequently modified to reflect feedback given by these
40 30 parents. Specific questions asked of the parents are provided in Table 1 along with the answers given from each of the three respondents and a summary of the final modifications made to the survey instrument.
41 31 31 Table 1 Parental Responses from Trial Administration of Draft Survey Instrument Respondent How long did it take you to complete the survey? Were all of the questions easy to understand or were there any that needed clarification? Were there any aspects of your experience with the newborn hearing screening and follow-up process that were not addressed? Modifications to survey minutes I would recommend differentiating the rescreening that occurred at the hospital and the outpatient rescreening, because I was confused about which one you were talking about in the questions. I would include a question about whether or not a parent would have liked to be present for a hearing screening or not. I know I wish I would have been present, and you asked whether or not I was- but maybe ask if parents would like to have been there. Fifth question added to survey, Would you have liked to have been present for the FIRST newborn hearing screening that was completed on your baby? minutes I think the questions you had made sense, I just had suggestions for other questions you could ask. I would also add question for every section about how old the baby was when the testing was conducted. Like on the page for the hearing rescreening and the hearing evaluation, how old were they when they got it done. Added space next to the yes response on question eight for parents to indicate how old their infant was when an evaluation was completed minutes No, they were all worded appropriately I was told that my baby was too young to be seen at an audiology clinic include a question about whether or not they were told any of these things when they tried to access follow-up services. Specific questions not added for this response. The option to include written responses was added at the end of the survey.
42 32 Survey Response Rate and Completion The Colorado Department of Public Health and Environment (2004) mailed a cover letter and survey (see Appendix B) to 445 parents using addresses listed on birth certificates. The letter and survey were sent in both English and Spanish to each parent who had a baby born in Colorado in 2014, who did not pass his/her initial newborn hearing screening, and had no documentation indicating follow up was pursued (either rescreen or diagnostic evaluation). Parents were asked to return completed surveys to the CDPHE within two weeks of receiving the survey in the mail. A total of 15% (n = 67) of the surveys were returned as undeliverable due to invalid addresses. Of the remaining 378 surveys, only 5% (n = 23) of surveys were completed and returned. Of those returned surveys, 43% (n = 10) represented families who had already obtained appropriate follow up after a newborn hearing screening was not passed. This suggested the reporting system to the CDPHE was incomplete or inaccurate for these families. Therefore, only 57% (n = 13) of the completed and returned surveys were included in the data analysis, yielding a total survey completion rate of 2.9%. The overall response rate (2.9%) for this study was lower than those documented in a previous parental survey study conducted by Thomson (2006). In this study, three different surveys were disseminated to families in Colorado. The first survey was sent to 1,500 families who had an infant who did not pass their newborn hearing screening before being discharged from the hospital. This survey resulted in a 17% return rate. A second survey was sent to 1,500 families whose infant did not pass their initial newborn hearing screening before hospital discharge but passed a hearing rescreening as an outpatient. This survey had a 16% response rate. Finally, a third survey was
43 33 administered to 383 families whose infant had been diagnosed with hearing loss in Colorado. The response rate was 21%. Upon evaluation of survey responses, it was determined not all subjects followed instructions correctly or answered all questions regarding their specific experiences. Of the actual survey respondents, 92% (n = 12) completed all of the correct sections of the survey based on their experiences. The respondent who did not fill out the full survey skipped sections of questions relating to factors that might have prevented follow up in the form of a hearing rescreening. To address this issue, each question was evaluated based on the actual number of respondents to each survey question as opposed to the number in the experimental group. Experimental Grouping Two experimental groups were formulated from the 13 completed and returned surveys selected as appropriate for data analysis. The first group (n = 6) was composed of those parents whose infant was born in 2014 did not pass his/her initial newborn hearing screening and responded either no or I don t know when asked if a hearing rescreening was obtained. This group was categorized as Lost at Rescreen as they did not reach this step in the follow-up process. Additionally, any parent who reported he/she did not receive either a hearing rescreening or a hearing evaluation for his/her infant was also placed in the Lost at Rescreen group. The second experimental group, determined to be Lost at Hearing Evaluation, was composed of those parents whose infant born in 2014 did not pass his/her initial newborn hearing screening, received a hearing rescreening, but then responded either no or I don t know when asked if a hearing evaluation was obtained. Parents who did not receive a rescreening for their infant but reported a
44 34 diagnostic evaluation was obtained were not included in either experimental group as they ultimately received appropriate follow up. The majority of survey respondents indicated they were related as mother to the infant born in 2014 while one respondent in the Lost at Rescreen group was the infant s father. All of the responding parents included in data analysis reported English was their primary spoken language. Additionally, all of the parents indicated their infant was born in a hospital. For both groups, more than half of the respondents (57% and 67%, respectively) did not remember the initial newborn hearing screening performed on their infant or whether they were physically present for it. Further, many of the parents in both experimental groups (43% and 83%, respectively) indicated they would like to have been present for this process. Parental report of newborn hearing screening personnel is included in Table 2. Table 2 Newborn Hearing Screening Personnel Screening Program Personnel Percentage Lost at Rescreen (n = 6) Nurse 16.7 Volunteer 0 Audiologist 0 Don t Know 66.6 Other 16.6 Lost at Hearing Evaluation (n = 7) Nurse 42.8 Volunteer 28.6 Audiologist 0 Don t Know 28.6 Other 0
45 35 The majority of parents (66.6%) in the Lost at Rescreen group indicated they did not know who conducted the newborn hearing screening on their baby after birth. Additionally, 28.6% of parents reported the same response to this question in the Lost at Hearing Evaluation group. While around 17% of parents in the Lost at Rescreen group responded either a nurse or another individual conducted the initial newborn hearing screening on their infant, the majority of the parents in the Lost at Hearing Evaluation group expressed either a nurse or volunteer conducted the screening. Table 3 presents the responses regarding who told the parents their infant needed additional testing after the initial newborn hearing screening. Both experimental groups (33.3% and 57.8%, respectively) most commonly reported a nurse communicated to them more testing was necessary after the initial newborn hearing screening. The second most common response for both experimental groups (16.7% and 28.6%, respectively) was a volunteer told them more testing was necessary.
46 36 Table 3 Personnel Who Provided Information Screening Program Personnel Percentage Lost at Rescreen (n = 6) Nurse 33.3 Physician 0 Volunteer 16.7 Audiologist 0 Nobody told me; I received a written notice/card 0 No one 16.7 I don t know 33.3 Other 0 Lost at Hearing Evaluation (n = 7) Nurse 57.1 Physician 14.2 Volunteer 28.6 Audiologist 0 Nobody told me; I received a written notice/card 0 No one 0 I don t know 0 Other 0
47 37 Survey Analysis Small Group Case Study Given the low survey response rate of parents and the minimal number of actual respondents, the proposed factor analysis could not be implemented (Costello & Osborne, 2005). Therefore, a small group descriptive case study was reported (Yin, 2014). The primary purpose of analyzing parental responses was to determine what factors affected their ability to obtain follow-up services after their infant did not pass the initial newborn hearing screening. Questions on the survey encompassed five pre-determined factors thought to contribute to lack of parental follow up based upon a literature review: communication barriers, scheduling barriers, personal and emotional barriers, financial barriers, and co-occurring medical barriers. Responses relating to each factor were analyzed descriptively to describe which factors appeared to affect parental follow up. Results were summarized with regard to each factor for both the Lost at Rescreen and Lost at Hearing Evaluation experimental groups. Communication Barriers Questions encompassing the communication barriers primarily related to the experiences parents had when communicating with newborn hearing screening personnel during and after the initial hearing screening process. To determine the degree to which parents felt communication barriers were prevalent in their experience with the initial newborn hearing screening and follow up, the researcher analyzed all survey questions directly relating to communication barriers. These results are summarized in Table 4.
48 38 38 Table 4 Mean Responses for Communication Barriers Questions Lost at Rescreen (n=6) Lost at Hearing Evaluation (n=7) The people doing the screening told me the process in a language that I could understand. * D N A D N A 83% 0% 17% 85% 14% 0% (n=5) (n=0) (n=1) (n=6) (n=1) (n=0) I was told that it was important that my baby get a rescreening or an evaluation by an audiologist. * 83% (n=5) 0% (n=0) 17% (n=1) 57% (n=4) 29% (n=2) 14% (n=1) The person who told me the results of the screening did not seem worried about my baby s hearing. 33% (n=2) 17% (n=1) 50% (n=3) 0% (n=0) 29% (n=2) 71% (n=5) I felt sure that the person who performed the hearing screening on my baby did a good job of explaining the results to me. * 50% (n=3) 17% (n=1) 33% (n=2) 100% (n=7) 0% (n=0) 0% (n=0) I was told that my baby might have fluid in their ears 50% (n=3) 17% (n=1) 33% (n=2) 71% (n=5) 0% (n=5) 29% (n=2) I was told by a doctor/nurse or hospital worker to not worry about my baby s hearing. 50% (n=3) 33% (n=2) 17% (n=1) 29% (n=2) 29% (n=2) 43% (n=3) Someone at the hospital told me it was important to get a hearing rescreening within the next 1-2 months. * 50% (n=3) 33% (n=3) 17% (n=1) 71% (n=5) 14% (n=1) 14% (n=1) Average Responses 57% 17% 26.3% 59.0% 18.7% 24.4% Note. D represents those that disagreed, N represents those that were neutral and A indicates those that agreed. Those questions marked with an asterisk are those that had the responses re-coded since it was worded positively.
49 39 The majority of parents in both experimental groups (57% and 59%, respectively) did not indicate communication was a barrier to receiving follow-up services. However, a large percentage of both groups (50% and 71%, respectively) reported the person who told them the results of the screening did not seem worried about their baby s hearing. While only one question encompassed the amount of concern expressed by the screener, this could definitely have contributed to a barrier with regard to obtaining follow up for these families. One parent (Subject #247) reported he did not feel sure the person who performed the hearing screening on his infant did a good job of explaining the results to him. He was also told his baby might have fluid in the ears. This father indicated his infant never received a hearing rescreening or a hearing evaluation because the baby showed every sign of hearing everything perfectly. Therefore, the perceived need for a rescreening was possibly minimized in some cases. Scheduling Barriers Scheduling barrier questions were related to the provision of appropriate materials and verbal or written information to facilitate the parent s attainment of further hearing testing after the newborn hearing screening was not passed. The averaged responses are summarized by experimental group in Table 5.
50 40 40 Table 5 Mean Responses for Scheduling Barriers Lost at Rescreen (n=6) Lost at Hearing Evaluation (n=7) Questions D N A D N A I was given the contact information for an audiologist or another person to see about my baby s hearing after the screening was completed.* 66% (n=4) 17% (n=1) 17% (n=1) 29% (n=2) 29% (n=2) 43% (n=3) I was given an appointment for a rescreen before I left the birthing hospital.* 0% (n=0) 17% (n=1) 66% (n=4) NA NA NA I had choices for places to take my baby to for a hearing rescreening.* 17% (n=1) 17% (n=1) 33% (n=3) NA NA NA I was given the contact information for an audiologist or another person to see about my baby s hearing.* NA NA NA 57% (n=4) 29% (n=2) 14% (n=1) I had choices for places to take my baby for a hearing evaluation by an audiologist.* NA NA NA 14% (n=1) 43% (n=3) 43% (n=3) I was given an appointment for a hearing evaluation after my baby s hearing screen or rescreen.* NA NA NA 14% (n=1) 14% (n=1) 71% (n=5) Averaged Responses 27.7% 17% 38.7% 28.5% 28.75% 42.75% Note. D represents those that disagreed, N represents those that were neutral and A indicates those that agreed. Those questions marked with an asterisk are those that had the responses re-coded since it was worded positively.
51 41 As evidenced in Table 5, the majority of parents were not provided with appropriate contact information for an audiologist or another professional after their baby did no pass their initial newborn hearing screening. Additionally, approximately half (39% and 42.8%, respectively) of respondents agreed scheduling barriers might have occurred during their experience with the newborn hearing screening conducted on their infant. One mother (Subject #204) shared a volunteer completed the first newborn hearing screening on her baby while she was present and told her that she needed to pursue additional testing. The mother indicated she was not given contact information for an audiologist or another person to facilitate the attainment of further testing. Personal and Emotional Barriers The frequency of personal and emotional barriers is summarized by experimental group in Table 6.
52 42 42 Table 6 Mean Responses for Personal and Emotional Barriers Lost at Rescreen (n=6) Lost at Hearing Evaluation (n=7) Questions D N A D N A I did not think that the hearing screening results were true. 50% (n=3) 0% (n=0) 50% (n=3) 28.5% (n=2) 42.8% (n=3) 28.5% (n=2) I felt overwhelmed thinking that my baby might possibly have hearing loss after the hearing screening results were given. 83% (n=5) 0% (n=0) 17% (n=0) 86% (n=6) 14% (n=1) 0% (n=0) I was not prepared when they told me the results of my baby s hearing screen. 50% (n=3) 33% (n=2) 17% (n=1) 71% (n=5) 28.5% (n=2) 0% (n=0) I did not think that my baby had a problem hearing at the time of the hearing screening. 0% (n=0) 33% (n=2) 66% (n=4) 0% (n=0) 28.5% (n=2) 71% (n=5) A family member (husband, wife, or parent) told me to not worry about my baby s hearing after the hearing screening. 50% (n=3) 33% (n=2) 17% (n=1) 28.5% (n=2) 28.5% (n=2) 42.8% (n=3) I wanted to talk with a religious or other non-medical advisor before making a choice about getting more care for my baby s hearing. 66% (n=4) 33% (n=2) 0% (n=0) 71% (n=5) 28.5% (n=2) 0% (n=0) Averaged Responses 49.8% 22% 27.8% 47.5% 28.5% 23.7% Note. D represents those that disagreed, N represents those that were neutral and A indicates those that agreed. Those questions marked with an asterisk are those that had the responses re-coded since it was worded positively.
53 43 As indicated in Table 6, the majority of parents in both experimental groups (83% and 86%, respectively) disagreed with the statement that they felt overwhelmed thinking that their baby might possibly have hearing loss. Similarly, a large percentage (66% and 71%, respectively) of both groups denied the need to seek counsel with a religious or other non-medical advisor before making choices relating to their infant s hearing. However, the same percentage of parents also reported they did not think their infant had a problem hearing at the time of the initial newborn hearing screening. This belief was the only personal and emotional factor that appeared to have affected parental follow-up attainment for these families. One mother (Subject #364) reported she was present for her infant s initial newborn hearing screening and a volunteer indicated to her she needed to obtain additional testing. While she obtained a hearing rescreening for her baby, she did not obtain a diagnostic evaluation. She explained, I was not concerned with his hearing and don't feel it was necessary in my case. Financial Barriers Potential financial barriers were determined through questions relating to the financial burden of driving far away for an appointment, paying for services, or losing pay when taking off time from work. The responses are summarized by experimental group in Table 7.
54 44 44 Table 7 Mean Responses for Financial Barriers Lost at Rescreen (n=5) Lost at Hearing Evaluation (n=7) Questions D N A D N A I lived far away from the hospital or clinic where I needed to get a hearing rescreening, and it was too far to travel. 80% (n=4) 0% (n=0) 20% (n=1) NA NA NA When they told me I had to bring my baby back for a hearing rescreen, I was worried about the travel costs. 80% (n=4) 0% (n=0) 20% (n=1) NA NA NA I could not take time off of work and lose pay in order to take my baby to a hearing rescreen. 40% (n=2) I was worried about the costs of a hearing screening for my baby and so I did not make additional 80% appointments. (n=4) 0% (n=0) 20% (n=1) 60% (n=3) 0% (n=0) NA NA NA NA NA NA I had a way to pay, with insurance or on my own, for a hearing evaluation by an audiologist. * NA NA NA 14.3% (n=1) I was worried about the costs of a hearing evaluation for my baby and so I did not make NA NA NA 57.1% additional appointments. (n=4) 57.1% (n=4) 28.6% (n=2) 28.6% (n=2) 14.3% (n=1) I lived far away from the hospital or clinic where I needed to get a hearing evaluation and it was too far to travel. NA NA NA 57.1% (n=4) 28.6% (n=2) 14.3% (n=1) When they told me I had to bring my baby to a hearing evaluation, I was worried about the travel costs. NA NA NA 57.1% (n=4) 42.9% (n=3) 0% (n=0) I could not take time off of work and lose pay in order to take my baby to a hearing rescreen or a hearing evaluation. NA NA NA 57.1% (n=4) 14.3% (n=1) 28.6% (n=2) Averaged Responses 70% 5% 25% 48.5% 34.3% 17.16% Note. D represents those that disagreed, N represents those that were neutral and A indicates those that agreed. Those questions marked with an asterisk are those that had the responses re-coded since it was worded positively.
55 45 As indicated in Table 7, many of the parents in both experimental groups (48% and 70%, respectively) disagreed that finances were a potential burden (e.g., I was worried about the costs of a hearing screening for my baby so I did not make additional appointments ). The majority of parents in the Lost at Rescreen group denied they lived far away from the hospital or clinic where services were provided. Additionally, the majority of this group denied they were worried about the cost of travel or the cost of the hearing screening. The majority of the Lost at Hearing Evaluation group similarly reported the cost of the hearing evaluation or travel to the appointment were not of concern. These results generally indicated financial barriers were not felt to be factor in terms of access to follow-up services. One mother in particular (Subject #46), however, did report finances presented a barrier for her attaining follow-up services. She indicated she did not have choices for places to take her baby for additional testing after the newborn hearing screening was completed and not passed. She also expressed she did not own a car so had no way to get her baby to any additional appointments needed. Hearing tests were not accessible in her town and required driving to another town. She was also not given an appointment for a hearing rescreening before she left the hospital. Her baby has not received a hearing rescreening or a hearing evaluation. Co-occurring Medical Barriers One question was included in the survey regarding co-occurring medical conditions that might have taken precedence over the parent/guardian s ability to obtain further hearing testing for his/her infant: I was worried about the other health problems
56 46 my baby had to deal with after birth more than their hearing ability. The percentages of responses are provided in Table 8. The majority of both experimental groups (66.7% and 71.4%, respectively) disagreed they were worried about other health problems their baby had to deal with after birth than their hearing ability. However, one mother (Subject #273) expressed her baby was flown back to a hospital three times in the first three months of life. She expressed she was more concerned with her being alive than if she could hear or not. This mother did report she had recently made an appointment with an audiologist to have her baby s hearing evaluated. Table 8 Mean Responses for Co-Occurring Medical Barriers Question Lost at Rescreen (n=6) Lost at Hearing Evaluation (n=7) I was worried about the other health problems my baby had to deal with after birth more than their hearing ability. 66.7% (n=4) 16.7% (n=1) 16.7% (n=1) 71.4% (n=5) 28.6% (n=2) 0% (n=0) Note. D represents those that disagreed, N represents those that were neutral and A indicates those that agreed. Those questions marked with an asterisk are those that had the responses re-coded since it was worded positively. Factor Comparison No single factor appeared to clearly dominate the reason for lack of parental follow up in either experimental group. However, the factor most parents commonly reported as being a barrier to follow up was scheduling barriers for both experimental groups (38.7% and 42.75%, respectively). The responses provided from both experimental groups were averaged for each factor to determine the occurrence of each
 Personal and Emotional Barriers (25.8%) Communication Barriers (25.4%) Financial Barriers (21.1%) Co-Occurring Medical Barriers (16.")
57 47 factor. Figure 1 summarizes the relative percentages of respondents who indicated the respective barriers were present for each factor % MEAN RESPONSES BY FACTOR 40.00% 35.00% 30.00% 25.00% 20.00% 15.00% 10.00% 5.00% 0.00% Scheduling Barriers (40.7%) Personal and Emotional Barriers (25.8%) Communication Barriers (25.4%) Financial Barriers (21.1%) Co-Occurring Medical Barriers (16.7%) Figure 1. Relative percentages of barriers indicated by factor. Scheduling is the largest barrier to follow up. Next, personal and emotional barriers and communication barriers were relatively equal in occurrence. Co-occurring medical issues appears to be the least prevalent factor affecting follow up for either experimental group. Family Resources Parents were asked if they received two different family resources--distributed by the Colorado Department of Health and Environment (2004)--after their infant s newborn hearing screening. Responses from both experimental groups reflected these resources were largely inaccessible to parents. When asked about whether or not the Loss and Found video (Colorado Families for Hands and Voices, 2010) was viewed, only one parent in the Lost at Rescreen group reported he/she viewed the video. None of the
58 48 parents in the Lost at Hearing Evaluation group had viewed the video. With regard to both experimental groups, 62.9% of respondents did not receive the Roadmap for Families (Colorado Families for Hands and Voices, 2010), 23% reported they had received this resource, and 7.7% indicated they did not know if they were given the Roadmap for Families. Parent Comments Open response parental/guardian comments appeared to cluster around two main factors. One factor, personal and emotional barriers, was originally determined as a possible factor that might contribute to lack of parental follow up. A second factor was related to the unpleasantness or perceived lack of success of the testing procedures. Written comments relating to these factors are summarized in Table 9. While the perception of inconvenience or ease of testing was not evaluated as one of the factors affecting parental follow up, three parents expressed they were not satisfied with the testing procedure and/or felt bringing their baby back for additional testing was inconvenient so soon after birth. Further, two of the parents expressed they did not worry about their baby s ability to hear and therefore did not pursue any additional testing. These two comments reflected personal and emotional attitudes were factors in the attainment of appropriate follow-up services for these families.
59 49 Table 9 Categorization of Parent Comments Factor Parental Belief That Baby Could Hear (Personal and Emotional Barriers) Parent Comments The first test was less than 24 hours after birth. The baby later showed every sign of hearing everything perfectly. We didn't bother following up. I was not concerned with his hearing. I don't feel it was necessary in my case. The test is not pleasant and we wanted our baby at home in the first weeks after his birth. Testing Procedure Inconvenient or Unsuccessful Attempted the rescreening at the audiologist but was unsuccessful since they required my baby to fall asleep. My baby does not do well in environments he's not familiar with or people. We (audiologist and I) couldn t get him to fall asleep. He'd fuss and cry when putting the testing stuff on. Change the hearing test process. It's bloody ridiculous making an infant fall asleep. Newborns are already a lot of work. Asking parents to do a lot related to their child when they are exhausted and/or trying to heal is very discouraging. The failed test just felt like another task I didn t feel up to doing. I would not go for a second test if the location and times were inconvenient. Summary As stated previously, due to the small response rate and number of actual respondents who were able to be included in the study, the planned factor analysis could not be completed. Therefore, a small group descriptive case study was employed to determine which factors affected parental follow up to either a hearing rescreening or a
60 50 diagnostic hearing evaluation. Parental responses were evaluated and compiled to determine which factors were most commonly expressed as causing a barrier to follow up. The majority of parents reported scheduling inconvenience was a factor that impeded obtaining follow-up services for their infant. All other factors did not appear to have a widespread effect on the parents experiences with the initial newborn hearing screening and follow up. Written open-ended comments were categorized by two descriptive themes: parental belief that baby could hear and testing procedure inconvenient or unsuccessful. Given the nature of the small group case study, each individual story was evaluated; it was concluded the uniqueness of each parent s experience reflected unique or individualized challenges and barriers. While scheduling appeared to affect the largest majority of responding parents, other parents shared they truly did not believe their baby had a problem hearing and, therefore, did not pursue follow up. Further other parents indicated a lack of appropriate transportation impeded their access to care. Finally, one mother shared her baby was flown back to the hospital three times for life-saving measures after she was born. The small number of cases prevented the identification of key barriers that might have driven the lack of follow up for hearing rescreen or diagnostic testing. However, it could be concluded the study design correctly identified factors that affected at least one parent s access to appropriate follow-up services and further identified one additional factor related to parental dissatisfaction with the hearing screen/test procedure for their infant.
61 51 CHAPTER V DISCUSSION The purpose of this study was to examine factors that influenced parental follow up after newborn hearing screening in Colorado through the administration of a parent survey. As previously discussed, early identification of hearing loss through newborn hearing screenings followed by immediate intervention is crucial to the attainment of language, reading abilities, and academic achievements for children with hearing loss (Flexer, 2012). While the majority (97.9%) of children born in the United States currently receive a newborn hearing screening before one month of age, national data collected in 2011 indicated diagnostic evaluations were not documented for 43.1% of infants who needed them (CDC, 2013b). In 2012, the number of parents who did not obtain follow-up services in Colorado after a newborn hearing screening and/or rescreening was not passed was 716 as estimated by the Colorado Health Department (E. McKiever, personal communication, July, 2015). The current study was conducted to identify factors that influenced parental follow up in the form of a hearing rescreening and/or a complete diagnostic hearing evaluation after an initial newborn hearing screening was not passed for infants born in Colorado during Parental Presence at Hearing Screening/Testing Many of the study respondents reported they were not physically present for their infant s newborn hearing screening and would have preferred to have attended. Further,
62 % of the Lost at Rescreen group did not know who conducted the first newborn screening on their infant. From the Lost at Hearing Evaluation group, approximately 28.6% of parents did not know who completed the diagnostic hearing evaluation. Harrell (2009) discussed the role of parents in genetic newborn screening. It was concluded parents are the best individuals to make medical decisions for their children and should be included more routinely in the screening and decision-making process. While this article specifically addressed genetic screening for newborns, the justification for the importance of parental involvement might be relevant to newborn hearing screenings as well. The prevalence of parents being absent from their infant s newborn hearing screening could be explained by a number of possible situations. Newborns are often screened for hearing loss while in the nursery or at night while the parents are asleep. If parents are not informed beforehand that this testing might occur, they might not be able to ensure they are present for the screening. Research by Thomson (2006) indicated 99% of respondents learned their baby was going to be screened for hearing loss either prior to hospital admission or while in the hospital. This data represented most parents should be aware their baby will have his/her hearing screened and should have the opportunity to request to be present for the screening. If parents wish to be present for the screening, the test should be conducted in the parent s hospital room when possible. This might also contribute toward better communication and trust in the test results. Parent Utilization of Resources A written resource called the Roadmap for Families was created by Colorado Hands and Voices (2010) for families of infants who do not pass their initial newborn
63 53 hearing screening. This resource is intended to be distributed to parents while in the hospital after a newborn hearing screening is not passed. Screening personnel should be trained to distribute this resource at all birthing hospitals. However, only one of the respondents in the Lost at Hearing Evaluation group reported receiving this document. None of the respondents in the Lost at Rescreen group reported they had received this document. The Loss and Found video was also developed by Colorado Hands and Voices (2010) to provide information to parents after their newborn did not pass the initial newborn hearing screening. Although this video is intended to be viewed by parents before leaving the hospital, the video was only viewed by one respondent in the Lost at Rescreen group. It was apparent an increased effort is warranted to make sure this resource is being provided to families while they are in the hospital. To improve this problem screening, personnel in all birthing hospitals should ensure this resource is readily available for distribution. Screening personnel should be trained to document the successful viewing of the video by each family with a child who did not pass the newborn hearing screening. If it is not possible to view the video while in the hospital, it should be communicated to families that this resource is also available online on the Colorado Hands and Voices website. Perhaps alternative distribution methods are needed since the time spent in the hospital is short, especially for healthy infants. For instance, for parent with addresses and computer access, a link to the video could be sent out after dismissal. For parents without technology access, perhaps the local health departments could facilitate ways to view the video with the family.
64 54 Factors That Influence Parental Follow Up in Colorado Communication Barriers Potter et al. (2014) addressed parental involvement in PKU newborn screenings and the provision of informational materials to parents in multiple facets. These authors suggested screening personnel and/or health care providers prioritize key messages believed to be relevant to all parents by engaging in conversations at the time of the screening and providing additional details through written or electronic materials. The authors stated parental education about newborn screening should be linked to educational goals. Some possible content messages included the purpose of the screening, the benefit, details about the process, and possible results and their meaning (Potter et al., 2014). Educational goals and messaging for parents might need to be established as they relate to newborn hearing screening. The American Speech-Language-Hearing Association (n.d.) additionally recommended parents/caregivers be provided with written educational materials describing the importance of early hearing detection and intervention, an overview of the screening process, and information about the screening and risk factors related to lateonset hearing loss. When presented with the statement, Someone at the hospital told me it was important to get a hearing rescreening within the next 1-2 months, three parents in the Lost at Rescreen group agreed (50%), while five of the Lost at Hearing Evaluation group respondents (71.4%) agreed with this statement. These findings suggested the recommended timeline for follow-up services was generally communicated appropriately.
65 55 One important communication barrier was spoken/written language. Of the group of parents who were sent surveys, only two of the Spanish surveys were completed and returned. Both of these respondents indicated they had already obtained appropriate follow up and as such were not included in either experimental group. It is possible language barriers obstructed access to follow up if results and recommendations were not communicated in the parent s primary language. Although Spanish surveys were provided in this study, the primary language of the families was unknown; thus, it is possible some of the parents were unable to respond in either English or Spanish. Of the 13 parents included in both experimental groups, only one disagreed the newborn hearing screening process was explained in a language they could understand. Since every parent in the experimental groups reported English as their primary language, it was possible Spanish-speaking parents or those communicating in other languages would report language was a more obtrusive barrier to adequate communication. Young and Tattersall (2007) reported inconclusive messages were frequently given to parents regarding their infant s newborn hearing screening results. Hyde (2005) additionally illustrated screening personnel often expressed positivity regarding an infant s hearing status after the initial screening was not passed, which might not urge parents to obtain timely follow up in the form of a rescreening or diagnostic hearing evaluation. Five parents in the Lost at Hearing Evaluation group agreed with the following statement: The person who told me the results of the screening did not seem worried about my baby s hearing. These results further confirmed the results of previous research that positivity and inconclusive results might affect follow up in the form of a hearing rescreening or a diagnostic hearing evaluation.
66 56 It was apparent the majority of parents in this study were not included in the newborn hearing screening process and did not receive adequate information after the screening. From the Lost at Rescreen group, 33.3% of parents did not know who provided them information about the need for a hearing rescreening after the initial screening. In addition, 16.7% of this group reported no one provided them information. These findings were similar to results indicated by Thomson (2006) in which several surveyed parents commented they only received a card with newborn hearing screening results and would have liked to have had the newborn hearing screening results discussed in person. The lack of direct communication during the newborn hearing screening process might have contributed to the lack of understanding by the parent regarding the importance of follow-up rescreening or diagnostic hearing testing. To improve direct communication screening, personnel should be trained to verbally communicate screening results with parents. It might be challenging to expect all screeners to communicate relevant messages and some screeners might feel unprepared for parent questions. Therefore, it might be worthwhile for the supervising audiologist to make contact with parents when infants do not pass the initial screening. Scheduling Barriers The current study found scheduling barriers might have contributed to some of the experiences described by parents. When asked about potential scheduling barriers, 38.7% of parents in the Lost at Rescreening group and 42.75% of parents in the Lost at Hearing Evaluation group agreed scheduling challenges occurred. Research conducted to evaluate EHDI programs in the United States concluded parents frequently experienced difficulty in identifying pediatric audiology facilities in their area that provided the
67 57 appropriate services for their infant. Further, parental compliance in scheduling was identified as the main challenge in completing timely diagnostic testing (Munoz et al., 2011). Russ et al. (2010) additionally found scheduling was often difficult for parents because longer appointments were needed to complete a sedated ABR evaluation if needed. To address the issue of scheduling barriers observed in previous research, Russ et al. (2010) recommended an appointment for a rescreening or diagnostic appointment be made before the family left the hospital. Additionally, the family should be contacted by phone to verify the appointment. None of the parents in the Lost at Hearing Evaluation group received a specific follow-up appointment when discharged from the hospital. Similarly, only one of the respondents in the Lost at Hearing Evaluation group reported being given an appointment for a hearing evaluation. However, four respondents in this group indicated they did receive contact information for an audiologist. These results concluded that simply providing contact information was not beneficial enough for parents to successfully obtain follow up. Per the recommendations by Russ et al., an appointment should be made for the family before they left the hospital. Personal and Emotional Barriers Young and Tattersall (2007) asked parents to describe emotions experienced when they first found out their child might have a hearing loss. One parent stated her emotions were especially difficult to handle because she was in a particularly vulnerable time after the birth of her child and was tired. Additionally, another mother commented on the extreme worry experienced after her child s newborn hearing screening, noting,
68 58 Then we came home and rather than having the joy of bringing a new baby home all we had in our head was worry. To explore whether personal and emotional barriers affected parental follow up in the present study, questions were asked of parents regarding their thoughts and reactions after their infant s newborn hearing screening. Questions were related to preparedness for having an infant with a hearing loss, feeling overwhelmed, and consultation with religious members or family members to make decisions about follow up. While the majority of parents disagreed personal and emotional factors impacted their experience, written spontaneous responses did indicate some parents did not believe their infant had a problem hearing. Informal and invalid tests of hearing have been documented (Hyde, 2005) as being utilized by parents to confirm their belief that their child could hear. While 50% (n = 3) of the Lost at Rescreen group and 29% (n = 2) of the Lost at Hearing Evaluation group indicated they agreed the hearing results were true, written comments from two parents indicated they observed signs of adequate hearing ability in their baby and therefore did not pursue additional follow up. These comments further confirmed the presence of informal and invalid tests of hearing in at least two of the parental experiences in this study as contributing to the conscious decision not to obtain follow up. Financial Barriers Thyen et al. (1999) evaluated the financial situations of parents who had children with chronic conditions. The authors reported the care needed for the children increased the financial burden on the parents. Barriers were also present with regard to parental
69 59 employment. This further impacted financial stability as financial needs continued to increase as a result of the child s medical needs. The presence of financial barriers was evaluated in this study through a series of questions relating to travel costs, insurance, and the actual costs of the hearing rescreening and/or diagnostic hearing evaluation. Results from the current study were contrary to results indicated by Thyen et al. (1999). The majority of parents in both the Lost at Rescreen group and the Lost at Hearing Evaluation group reported financial barriers did not impact their experience. Only one (14%) of the respondents in the Lost at Hearing Evaluation group agreed with the statement that they were worried about the costs of a hearing evaluation for their baby. Similarly, none of the parents in the Lost at Rescreening group agreed they were worried about the costs of a hearing screening for their baby. One parent in the Lost at Rescreen group agreed they were worried about travel costs while none of the parents in the Lost at Hearing Evaluation group agreed this was a worry for them. Given these results, financial barriers did not appear to have an impact on either of the two experimental groups and their access to either a hearing rescreen or a hearing evaluation. Co-Occurring Medical Barriers Nearly 40% of children who are born with a hearing loss have additional disabilities (Gallaudet Research Institute, 2003). The presence of concomitant medical conditions was found to exacerbate barriers in accessing timely follow-up services for children who did not pass their initial newborn hearing screening. In particular, infants who spent time in the neonatal intensive care unit after birth were estimated to experience delays in obtaining hearing rescreening and diagnostic services (Chapman et al., 2011).
70 60 Despite the prevalence of co-occurring medical conditions in infants with hearing loss, the greatest percentage of both experimental groups indicated co-occurring medical barriers did not impact their access to follow-up services. This might possibly be related to the small number of surveys received and might even have contributed to the reasons why some parents did not return the survey. In terms of returned surveys, one written response expressed their infant experienced many medical complications that took precedence over the hearing rescreening. While this factor was not found to be prevalent in the experiences of all respondents, it is important to acknowledge some families in Colorado do experience co-occurring medical conditions with their infant and they might delay or never receive follow up as a result. Factor Summary In the current study, scheduling barriers were found to be the most prevalent factor that affected parental follow up in the form of both a rescreening and a hearing evaluation. Similarly, parental compliance in scheduling was identified by Munoz et al. (2011) as the main challenge in completing timely diagnostic testing. Communication barriers were the second most prevalent factor expressed by both experimental groups. Specific findings relating to communication barriers found in this study were similar to those found by Thomson (2006) regarding the lack of communicating results in person. Fortunately, solutions to both the communication and scheduling challenges might be addressed by simple procedural changes such as including parents in the screening, providing the opportunity to communicate with the supervising audiologist and providing an appointment, directions, and, if necessary, arranging transportation to the follow-up service provider before discharge.
71 61 The third most prevalent factor related to personal and emotional barriers. This was in the form of parents conducting their own informal tests of hearing, questioning the validity of the hearing screening results, and believing their infant could hear. The prevalence of this factor was similarly reflected by Hyde (2005). Better communication and education provided to parents regarding the importance of having a hearing rescreening or an evaluation completed by a professional would help to address this issue. Financial barriers and co-occurring medical conditions, while expressed in previous literature as affecting access to medical care (Munoz et al., 2011; Thyen et al., 1999), were not determined to be factors that commonly influenced parental follow up in this study. It was felt changes in access to healthcare and state-level healthcare services for children might have addressed this barrier for the majority of parents in the study sample. Responses for both experimental groups were similar with regard to the prevalence of barriers expressed. Therefore, it appeared in this small sample that factors affecting follow up did not differ between the stage of follow up, rescreening, or a diagnostic hearing evaluation. Parental comments revealed the unpleasantness and inconvenience of additional testing after the newborn hearing screening was an additional factor that affected parental follow up. Colorado State Reporting and Recordkeeping System One important finding in this study was the prevalence of poor reporting and recordkeeping as evidenced by the number of respondents who returned surveys indicating they had already received follow-up services. Nearly 50% of respondents had already received appropriate follow-up services; yet, these service outcomes were not
72 62 documented at the Colorado Department of Health and Environment (E. McKiever, personal communication, October 2, 2015). The reporting system utilized for the documentation of follow-up services includes training by the director of the Newborn Hearing Screening Program at the Colorado Department of Public Health and Environment (E. McKiever, personal communication, October 2, 2015). Colorado audiologists are trained to enter diagnostic results directly into the EHDI Integrated Data System. If they have not been trained, audiologists have the option of completing a fillable PDF form online and submitting it through a secure . Ideally, audiologists are trained to submit their findings as soon as the evaluation is complete. They are also asked to refer directly to the Colorado Hearing Resource Coordinator to begin early intervention services. Audiologists should also report findings on infants who pass a screening or diagnostic evaluation in their clinic (E. McKiever, personal communication, October 2, 2015). It is likely that improved training of audiologists regarding the reporting process could improve the prevalence of accurate records of follow up received. Additionally, a system for following up with parents to ask if they have received follow-up services within a few months of the newborn hearing screening and then again a year after could help ensure records are updated appropriately. Study Limitations The purpose of this study was to determine what factors affected parental follow up after newborn hearing screenings in Colorado. Written surveys were mailed to parents in Colorado who were documented as not having received follow-up services for their
73 63 infant born in 2014 once the initial newborn hearing screening was not passed. Limitations involving conducting research on this particular population were numerous. Response Rate The survey completion rate for this study was 2.9%. Compared to previous parental studies such as Thomson (2006), this was an extremely low completion rate. The use of a survey warranted some response bias since the parents who responded were most likely those who felt most strongly (positively or negatively) about their experience. Given this small sample size, the originally planned factor analysis could not be completed and data analysis was limited to a descriptive approach. Because of the high variability of responses expressed by parents, a larger sample size would have contributed to statistical analysis and more generalizable results as to what particular factors most affected parental follow up for either the hearing rescreen or diagnostic hearing test follow up in Colorado. Increased response rates might have been experienced if the surveys were disseminated closer in time to the date of the newborn hearing screening. Given the parents involved in this study had infants born in 2014, the extended timeline of the survey research might have affected the parent s willingness to recall and report about the experience. Family Relocation Of the 445 surveys mailed to families, 15% (n = 67) were returned as undeliverable due to incorrect addresses. Surveys were mailed to the address listed on the birth certificates of the infants born in Therefore, relocation of families limited the number of potential survey responses in this study. Informal information provided by a representative from the vital records department at the Colorado Department of Public
74 64 Health and Environment (E. McKiever, personal communication, October 2, 2015) indicated relocation is common shortly after an infant is born. There is generally a 20% rate of return on CDPHE mail sent to families in the first year after birth and an 80% rate of return three years after their infant is born (E. McKiever, personal communication, October 2, 2015). Surveys for the current study were mailed out approximately one year after birth. Therefore, it could be inferred that the return rate for bad addresses (15%) was slightly less than what would be expected in the first year after birth. Survey Instrument The survey instrument used for this study was eight pages in length. While not every question was required to be answered by all parents, it is possible that receiving a large number of pages in the mail dissuaded parents from wanting to take the time to complete the survey. An electronic survey might have proven more effective as parents were not able to see all of the questions in the beginning and might have been more motivated to take the time to complete the survey. However, it was unknown by this research how accessible the internet/computer or smartphones were to the parent study group. If replicated, the current study could be improved by having a longer timeline for return of the surveys. An extended timeline would allow time for reminder calls or cards to be sent in the mail to ask parents to return the surveys. Additionally, an indicator of how much time the survey was expected to take, utilizing estimations provided during the trial administration, might have helped parents be more motivated to complete the survey. Future Research It is recommended that additional research specifically address the effectiveness of the Colorado hearing screening reporting system. The intent of this research was to
75 65 potentially improve the tracking and reporting process and system for follow-up services after newborn hearing screenings and diagnostic testing. This could be achieved through an additional study evaluating hearing screening personnel to include screeners, hospital staff, and audiologist staff responsible for data entry/reporting of results. Follow up with the parents who reported they did receive appropriate services could determine if there were glitches in the reporting system or software. Following up with these parents could be accompanied by additional follow up with their physicians. In this way, the researcher could determine whether or not reports of follow-up services were actually submitted and possibly not received by the Colorado Department of Health and Environment. Research should be aimed at identifying if more training is warranted, whether it be at the screening stage or the recordkeeping phase. Additional research regarding recordkeeping should evaluate the accuracy of data entered after each stage in the EHDI process to ensure errors were not being made after the initial newborn hearing screening was completed. For example, if an infant passed a newborn hearing screening but was reported as not passing, this could explain the number of infants who did not receive follow-up services. If a baby has a name change, this could also account for errors in recordkeeping. Additionally, research should be conducted to evaluate the knowledge of audiologists who see infant patients regarding the processes and timeline that should be followed to report screening and diagnostic results. To better determine the factors that affected parental follow up for those who did not complete the process, it would also be beneficial to re-examine a similar group of parents through a different research design. Phone interviewing could prove more
76 66 effective with regard to response rate. The personal element of phone contact could result in better participation than paper surveys. Utilizing phone numbers could also allow the researcher to reach out to families more than once without the addition of mailing costs. Additionally, interviewing should take place closer to the actual time the newborn hearing screening was conducted. Recommendations Each parent who responded to this study appeared to have had unique experiences regarding his/her infant s newborn hearing screening and the ability to obtain follow up. However, a few common themes were extracted from their responses and provided feasible improvements that could be considered by the coordinators of the Colorado Early Hearing Detection and Intervention program (National Center for Hearing Assessment and Management, 2015). Improvements in the process could be obtained through increased scheduling assistance and parental involvement in the initial newborn hearing screening process. Including parents in the newborn hearing screening process would be an ideal step toward improving communication; however, the practicalities of this might be challenging in terms of hospital staff efficiency. This would also facilitate parent confidence in the screening results and provide an opportunity to arrange the follow-up services. Russ et al. (2010) recommended that screening personnel should make an appointment for a rescreening or diagnostic hearing evaluation appointment for a family before the family leaves the hospital. This should be implemented and phone numbers provided for the family in the case of rescheduling requests. Certainly reminder phone calls to the parents might also facilitate follow up. Lastly, parents could be provided with
77 67 a hot-line or phone contact with the supervising audiologist to allow for discussion of the importance of the follow-up services and to address parent concerns and potential personal or emotional barriers. The supervising audiologist could also then track that the family had obtained the rescreen or diagnostic testing on a local basis. Summary This study described the barriers to newborn hearing screening follow up as reported by 13 parents of children born in 2014 who were listed as no follow-up received at the CDPHE in the spring of 2015 (E. McKiever, personal communication, June, 2015). Five factors were explored in terms of their contribution to an individual family s decision to obtain follow-up services: (a) scheduling, (b) communication, (c) financial, (d) co-occurring medical conditions, and (e) personal/emotional barriers. Each family had a unique story in terms of their personal challenges or reasons for not receiving follow-up services and could not be generalized to the general population of parents whose children did not receive a hearing rescreen or diagnostic test after referral on the initial screen. Scheduling barriers were the most commonly reported problem followed by communication. Additionally, approximately 50% (n = 10) of the overall study sample had already obtained appropriate follow-up services. This outcome is encouraging and reflects the possibility that the rate of follow up in Colorado might be under-estimated given the lack of accurate recordkeeping. Further study is needed regarding potential systematic changes or screening program design is needed before large-scale changes are considered. In the short-term, simple improvements in scheduling and parent communication might enhance the follow-up rate.
78 68 REFERENCES American Academy of Pediatrics. (2013). Early hearing detection and intervention (EHDI). Retrieved from American Speech-Language-Hearing Association. (2004). Guidelines for the audiologic assessment of children from birth to 5 years of age [Guidelines]. Retrieved from doi: /policy. GL American Speech-Language-Hearing Association. (n.d.) Newborn hearing screening: Overview. Retrieved from Issues/Newborn-Hearing-Screening/ Barnes, L. L., Plotnikoff, G. A., Fox, K., & Pendleton, S. (2000). Spirituality, religion, and pediatrics: Intersecting worlds of healing. Pediatrics, 106, Campbell, E., & Ross, L.R. (2003). Parental attitudes regarding newborn screening of PKU and DMD. American Journal of Medical Genetics, 120A(2), Centers for Disease Control and Prevention. (2013a). Hearing loss in children. Retrieved from Centers for Disease Control and Prevention. (2013b). Summary of 2011 National CDC EHDI data. Retrieved from data/2011_ehdi_hsfs_summary_a.pdf
79 69 Chapman, D., Stampfel, C., Bodurtha, J., Dodson, K., Pandya, A., Lynch, K., & Kirby, R. (2011). Impact of co-occurring birth defects on the timing of newborn hearing screening and diagnosis. American Journal of Audiology, 20, Christensen, M., Thomson, V., & Letson, W. (2008). Evaluating the reach of universal newborn hearing screening in Colorado American Journal of Preventive Medicine, 35(6), Cole, E., & Flexer, C. (2007). Children with hearing loss: Developing listening and talking birth to six. San Diego, CA: Plural Publishing. Cole, E. B., & Flexer, C. (2011). Children with hearing loss: Developing listening and talking birth to six (2nd ed.). San Diego, CA: Plural Publishing. Colorado Department of Public Health and Environment. (2004). Colorado infant hearing advisory committee: Guidelines for infant hearing screening, audiologic assessment, and early intervention. Denver, CO: Author. Costello, A. B., & Osborne, J. W. (2005). Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Practical Assessment, Research & Evaluation, 10, 1-9. Flexer, C. (2012). Auditory brain development: The key to developing listening, language and literacy. Retrieved from /auditory-brain-development Gallaudet University Center for Assessment and Demographic Study. (1998). Thirty years of the annual survey of deaf and hard-of-hearing children and youth: A glance over the decades. American Annals of the Deaf, 142(2),
80 70 Gallaudet Research Institute. (2003). Regional and national summary report of data from the annual survey of deaf and hard of hearing children and you. Washington, DC: Gallaudet University Press. Harlor, A. D., & Bower, C. (2009). Hearing assessment in infants and children: Recommendations beyond neonatal screening. Pediatrics, 124(4), doi: /peds Harrell, H. (2009). Currents in contemporary ethics: The role of parents in expanded newborn screening. The Journal of Law, Medicine & Ethics, 37(1), doi: /j x x Holt, R. E., & Svirsky, M. A. (2008). An exploratory look at pediatric cochlear implantation: Is earliest always best? Ear & Hearing, 29(4), Hyde, M. (2005, August). Newborn hearing screening programs: overview. The Journal of Otolaryngology, 34, Supplement 2. Joint Committee on Infant Hearing. (1973). Statement for infant hearing. Retrieved from Joint Committee on Infant Hearing (1994). Position statement. Retrieved from Joint Committee on Infant Hearing. (2007). Year 2007 position statement: Principles and guidelines for early hearing detection and intervention programs. Retrieved from Joint Committee on Infant Hearing. (2013). Year 2013 position statement: Principles and guidelines for early hearing detection and intervention programs. Retrieved from
81 71 Kurtzer-White, E., & Luterman, D. (2003). Families and children with hearing loss: Grief and coping. Mental Retardation and Developmental Disabilities Research Reviews, 9, Luterman, D. (2001). Closing remarks. In E. K. Kurtzer-White & D. Luterman (Eds.), Early childhood deafness (pp ). Baltimore, MD: York Press. Matthijs, L., Loots, G., Mouvet, K., Herreweghe, M. V., Hardonk, S., Hove, G. V., Leigh, G. (2012). First information parents receive after UNHS detection of their baby's hearing loss. Journal of Deaf Studies and Deaf Education, 17(4), McLeod, S. A. (2008). Likert scale. Retrieved from Mehl, A. L., & Thomson, V. (2002). The Colorado newborn hearing screening project, : On the threshold of effective population-based universal newborn hearing screening. Pediatrics, 109(7), 1-8. Moog, J. S., & Geers, A. E. (2003). Epilogue: Major findings, conclusions and implications for deaf education. Ear & Hearing. 24(1), 121S 125S. Munoz, K., Nelson, L, Goldgewicht, N., & Odell, D. (2011). Early hearing detection and intervention: Diagnostic hearing assessment practices. American Journal of Audiology, 20, National Center for Hearing Assessment and Management. (2015). National goals and program objectives for the EHDI tracking and surveillance system. Retrieved from infanthearing.org
82 72 National Institute on Deafness and Other Communication Disorders. (n.d.). When a newborn doesn't pass the hearing screening: How medical and other health professionals can help increase the number of infants who return for a follow-up evaluation. Retrieved from dotherprofessionals.pdf National Institute on Deafness and Other Communication Disorders. (2007). Statistics about hearing disorders, ear infections, and deafness. Retrieved February 20, 2007, from National Institute on Deafness and Other Communication Disorders. (2010). Quick statistics. Retrieved from Pages/quick.aspx Newborn Hearing Screening and Intervention Act, H.R. 1193, 106 th Congress (1999). Northern, J. L., & Downs, M. P. (2014). Hearing in children (6th ed.). San Diego, CA: Plural Publishing. Park, A. H., Warner, H., Sturgill, N., & Alder, S. C. (2006). A survey of parental views regarding their child s hearing loss: A pilot study. Otolaryngology- Head and Neck Surgery, 134(794). Potter, B. K., Etchegary, H., Nicholls, S. G., Wilson, B. J., Craigie, S. M., & Araia, M. H. (2014). Education and parental involvement in decision-making about newborn screening: understanding goals to clarify content. Journal of Genetic Counseling, 24(3), doi: /s x
83 73 Russ, S., Hanna, D., DesGeorges, J., & Forsman, I. (2010). Improving follow-up to newborn hearing screening: A learning-collaborative experience. Pediatrics, 126, S59-S69. Sharma, A., Dorman, M. F., & Spahr, A. J. (2002). A sensitive period for the development of the central auditory system in children with cochlear implants: Implications for age of implantation. Ear & Hearing, 23(6), Shulman, S., Katz, A., Ireys, H., & Besculides, M. (2006). Evaluation of HRSA s universal newborn hearing screening and intervention program: Final report. Cambridge, MA: Mathematics Policy Research, Inc. Shulman, S., Besculides, M., Saltzman, A., Ireys, H., White, K. R., & Forsman, I. (2010). Evaluation of the universal newborn hearing screening and intervention program. Pediatrics, 126(Suppl. 1), S19 S27. Thomson, V. (2006). A survey of family satisfaction with state early hearing detection and intervention (EHDI). Unpublished dissertation, University of Colorado, Boulder, CO. Thyen, U., Kuhlthau, K., & Perrin, J. M. (1999). Employment, childcare, and mental health of mothers caring for children assisted by technology. Pediatrics, 103(6), Vohr, B., Carty, L., Moore, P., & Letourneau, K. (1998). The Rhode Island hearing assessment program: Experience with statewide hearing screening. Journal of Pediatrics, 133,
84 74 Waisbren, S. E., Albers, S., Amato, S., Ampola, M., Brewster, T. G., Demmer, L., Levy, H. L. (2003). Effect of expanded newborn screening for biochemical genetic disorders on child outcomes and parental stress. JAMA, 290(19), doi: /jama White, K. R. (1997). The scientific basis for newborn hearing screening: Issues and evidence. Invited keynote address to the Early Hearing Detection and Intervention (EHDI) Workshop sponsored by the Centers for Disease Control and Prevention, Atlanta, GA. Retrieved from White, K., & Blaiser, K. (2011). Strategic planning to improve early hearing detection and intervention programs. The Volta Review, 111 (2), Yin, R. K. (2014). Case study research: Design and methods. Los Angeles, CA: Sage Publications. Yoshinago-Itano, C., Sedey, A., Coulter, D., & Mehl, A. (1998). Language of early- and later-identified children with hearing loss. Pediatrics, 102(5), Young, A., & Tattersall, H. (2007). Universal newborn hearing screening and early identification of deafness: Parents responses to knowing early and their expectations of child communication development. Journal of Deaf Studies and Deaf Education, 12,
85 75 APPENDIX A INSTITUTIONAL REVIEW BOARD APPROVAL LETTERS
86 76

87 77
88 78 APPENDIX B PARENT CONSENT LETTER AND SURVEY
89 Dear Parent or Guardian, The Colorado Department of Public Health and Environment is responsible for the newborn hearing screening program in Colorado. We would like to know about your experience of having your baby s hearing screened after they were born, and any other hearing tests that they might have had. This information will be helpful for us as we work to make Colorado s Early Hearing Detection and Intervention program better for all babies and their families. Below is some information about the study: Purpose and Procedures: If you choose to complete this evaluation, we ask you to take a few minutes and fill out the enclosed survey. After you are done with the survey, please place it in the envelope that is in this packet. This envelope already has our address and a stamp on it. If you choose to complete the survey, this is all we ask you to do. Risks There are no medical risks in this survey. However, some of the questions we will ask you might make you feel uncomfortable. If you do not want to answer some of the questions that we ask, you can just leave them blank. Benefits This survey may not directly help you or your baby in any way. But, we may learn important things that will help more families who have their baby s hearing screened. This information may help you and your family if you have another baby. Confidentiality If you choose to be a part of this survey, all information you give us will be kept confidential to the extent allowed by law. To protect your identity, we will keep the information you give us under a code number instead of your name. The information you give us will be used only by staff who are performing this evaluation. We will keep all of your information in locked files. No names will ever be written in reports. Voluntary Participation, Refusal and Withdrawal This survey is voluntary. You can choose whether or not you want to be a part of this evaluation. If you decide that you want to be in this evaluation, please fill out the survey and mail it back to us. We are also working with a student in the clinical doctoral program for audiology at the University of Northern Colorado on this project, Jamie Walter. Jamie is looking forward to learning more about your experience with newborn hearing screening. Her project title is, Factors that Influence Parental Follow-up after Newborn Hearing Screening in Colorado. For more information about her project, you can contact Jamie at walt7654@bears.unco.edu. You can also contact her research advisor, Dr. Jennifer Weber, at jenny.weber@unco.edu. If you have any concerns about your selection or treatment as a research participant, please contact Sherry May, IRB Administrator, Office 79
90 80 of Sponsored Programs, Kepner Hall, University of Northern Colorado, Greeley, CO 80639; If you have questions or need more information about your baby s hearing screening or this survey, please call Erica McKiever at Thank you, Erica McKiever Colorado Department of Public Health and Environment
91 81
92 82
93 83
94 84
95 85
96 86
97 87 APPENDIX C RAW SURVEY DATA
98 88
99 89
100 90
101 91
102 92
103 93
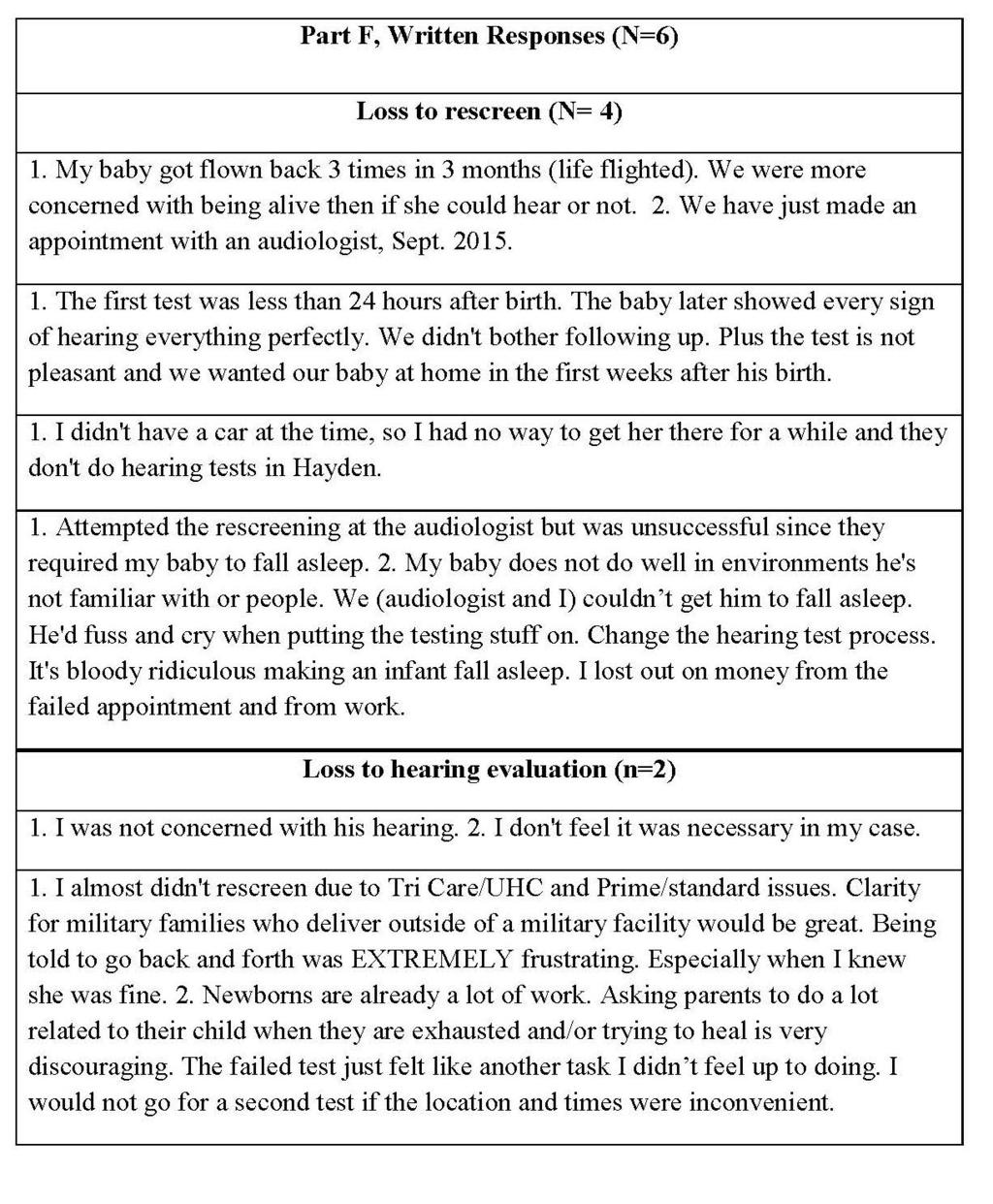
104 94
5. Hospitals will provide the family with a copy of the Michigans Community Program: Information for Parents (MDCH /01). Copies can be ordered,
. Copies can be ordered,") GUIDELINES FOR HEARING SCREENING A goal of newborn hearing screening is to ensure that all newborns receive a hearing screen before discharge from the hospital or before one month of age. All hospitals
GUIDELINES FOR HEARING SCREENING A goal of newborn hearing screening is to ensure that all newborns receive a hearing screen before discharge from the hospital or before one month of age. All hospitals
Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home
: The Role of the Medical Home") Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home A PRESENTATION FROM THE AMERICAN ACADEMY OF PEDIATRICS Hearing Facts Early identification and intervention of a child who is
Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home A PRESENTATION FROM THE AMERICAN ACADEMY OF PEDIATRICS Hearing Facts Early identification and intervention of a child who is
Executive Summary. JCIH Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs
 Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
Appendix C NEWBORN HEARING SCREENING PROJECT
 Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Appendix C NEWBORN HEARING SCREENING PROJECT I. WEST VIRGINIA STATE LAW All newborns born in the State of West Virginia must be screened for hearing impairment as required in WV Code 16-22A and 16-1-7,
Early Hearing Detection and Intervention
 Early Hearing Detection and Intervention ACTION REQUESTED Please co-sponsor and support passage of the Early Hearing Detection and Intervention (EHDI) Act of 2009 (H.R. 1246) that would reauthorize the
Early Hearing Detection and Intervention ACTION REQUESTED Please co-sponsor and support passage of the Early Hearing Detection and Intervention (EHDI) Act of 2009 (H.R. 1246) that would reauthorize the
CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION. Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf
 CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf STRAW POLL ON CMV 100 people surveyed regarding CMV How many knew
CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf STRAW POLL ON CMV 100 people surveyed regarding CMV How many knew
Historical Perspective. JCIH 1973 Position Statement. JCIH Goals. JCIH 1982 Position Statement
 Historical Perspective Effects of Policy Changes on Universal Newborn Hearing Screening Follow up Lata A. Krishnan, PhD, CCC A Shannon Van Hyfte, AuD, CCC A Purdue University The Joint Committee on Infant
Historical Perspective Effects of Policy Changes on Universal Newborn Hearing Screening Follow up Lata A. Krishnan, PhD, CCC A Shannon Van Hyfte, AuD, CCC A Purdue University The Joint Committee on Infant
INPATIENT SCREENING PROTOCOL
 INPATIENT SCREENING PROTOCOL During the maternity stay, a designated hospital staff member will: Inform parents of the hospital s universal newborn hearing screening program. Obtain informed consent for
INPATIENT SCREENING PROTOCOL During the maternity stay, a designated hospital staff member will: Inform parents of the hospital s universal newborn hearing screening program. Obtain informed consent for
Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011
 Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011 2011 National Early Hearing Detection and Intervention Conference Atlanta, Georgia Janet Farrell, Sarah Stone, Rashmi Dayalu MA DPH
Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011 2011 National Early Hearing Detection and Intervention Conference Atlanta, Georgia Janet Farrell, Sarah Stone, Rashmi Dayalu MA DPH
Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan,
 Journal of Educational Audiology 12 (2005) Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan, 1998-2002 Darline K. El Reda, DrPH, MPH, CHES
Journal of Educational Audiology 12 (2005) Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan, 1998-2002 Darline K. El Reda, DrPH, MPH, CHES
EHDI: An Amazing Journey
 EHDI: An Amazing Journey Jackson Roush, PhD Professor & Director Division of Speech and Hearing Sciences Director, North Carolina LEND Program Carolina Institute for Developmental Disabilities UNC School
EHDI: An Amazing Journey Jackson Roush, PhD Professor & Director Division of Speech and Hearing Sciences Director, North Carolina LEND Program Carolina Institute for Developmental Disabilities UNC School
State of Kansas Department of Health and Environment. Permanent Administrative Regulations
 State of Kansas Department of Health and Environment Permanent Administrative Regulations Article 4 MATERNAL AND CHILD HEALTH Newborn Infant Hearing Screening Act 28-4-600. Definitions. (a) AAccepted medical
State of Kansas Department of Health and Environment Permanent Administrative Regulations Article 4 MATERNAL AND CHILD HEALTH Newborn Infant Hearing Screening Act 28-4-600. Definitions. (a) AAccepted medical
CHHA-NL POSITION PAPER. Universal Newborn Hearing Screening Program (UNHSP) in Newfoundland and Labrador
 in Newfoundland and Labrador") CHHA-NL POSITION PAPER Universal Newborn Hearing Screening Program (UNHSP) in Newfoundland and Labrador Introduction: Approximately 4 in 1,000 Canadian babies are born with some degree of hearing loss
CHHA-NL POSITION PAPER Universal Newborn Hearing Screening Program (UNHSP) in Newfoundland and Labrador Introduction: Approximately 4 in 1,000 Canadian babies are born with some degree of hearing loss
How Does Your EHDI Intervention System Measure Up? States Experiences Using the JCIH EHDI System Self-Assessment
 How Does Your EHDI Intervention System Measure Up? States Experiences Using the JCIH EHDI System Self-Assessment March March 2016 2016 National National EHDI EHDI Conference Conference San San Diego, Diego,
How Does Your EHDI Intervention System Measure Up? States Experiences Using the JCIH EHDI System Self-Assessment March March 2016 2016 National National EHDI EHDI Conference Conference San San Diego, Diego,
JFK-HCP Webinar - Partnering to Support Children with Hearing Loss - 2/27/14 1
 1991 Reps from the CO Dept of Public Health, University of Colorado and The Children s Hospital Colorado met to develop a pilot project 1992 Boulder Community Hospital and the University of Colorado Hospital
1991 Reps from the CO Dept of Public Health, University of Colorado and The Children s Hospital Colorado met to develop a pilot project 1992 Boulder Community Hospital and the University of Colorado Hospital
MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM. EHDI Goals, Indicators and Benchmarks
 PROGRAM. EHDI Goals, Indicators and Benchmarks") Protecting, maintaining and improving the health of all Minnesotans MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM EHDI Goals, Indicators and Benchmarks The measures described in this
Protecting, maintaining and improving the health of all Minnesotans MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM EHDI Goals, Indicators and Benchmarks The measures described in this
Risk Factors for Late-Onset Hearing Loss in Children
 Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
Developmental Hearing and Auditory Milestones. Presented by : Amy Packer & Marilyn Nelson
 Developmental Hearing and Auditory Milestones Presented by : Amy Packer & Marilyn Nelson Today s Objectives: 1. The EAR and the Development of Hearing 2. The Developmental Urgency of Hearing 3. The Impact
Developmental Hearing and Auditory Milestones Presented by : Amy Packer & Marilyn Nelson Today s Objectives: 1. The EAR and the Development of Hearing 2. The Developmental Urgency of Hearing 3. The Impact
to the child and the family, based on the child's and family's abilities and needs. The IFSP needs to address the communication needs of the child and
 GUIDELINES FOR EARLY INTERVENTION The goals of newborn hearing screening are to provide a hearing screen to all newborns before one month of age, to ensure that all newborns who do not pass the birth admission
GUIDELINES FOR EARLY INTERVENTION The goals of newborn hearing screening are to provide a hearing screen to all newborns before one month of age, to ensure that all newborns who do not pass the birth admission
Newborn Hearing Screening: Success and Challenges
 Newborn Hearing Screening: Success and Challenges Marcus Gaffney, MPH CDC EHDI Program AAP EHDI Chapter Champion Webinar March 2013 National Center on Birth Defects and Developmental Disabilities Division
Newborn Hearing Screening: Success and Challenges Marcus Gaffney, MPH CDC EHDI Program AAP EHDI Chapter Champion Webinar March 2013 National Center on Birth Defects and Developmental Disabilities Division
Iowa EHDI A Work in Progress. Coordinating Council for Hearing Services November 24, 2008
 Iowa EHDI A Work in Progress Coordinating Council for Hearing Services November 24, 2008 Presenter Lenore Holte, PhD University of Iowa Hospitals and Clinics Center for Disabilities and Development 100
Iowa EHDI A Work in Progress Coordinating Council for Hearing Services November 24, 2008 Presenter Lenore Holte, PhD University of Iowa Hospitals and Clinics Center for Disabilities and Development 100
Trends across the country. Indiana Early Hearing Detection 4/13/2015
 Trends across the country Indiana Early Hearing Detection and Intervention (EHDI) Shortage of pediatric audiologists Shortage of educators and SLPs skilled in working with deaf and hard of hearing children
Trends across the country Indiana Early Hearing Detection and Intervention (EHDI) Shortage of pediatric audiologists Shortage of educators and SLPs skilled in working with deaf and hard of hearing children
Michael Macione, AuD; & Cheryl DeConde Johnson, EdD
 A NATIONAL RESOURCE CENTER GUIDE FOR EARLY HEARING HEARING ASSESSMENT DETECTION && MANAGEMENT INTERVENTION Chapter 21 The Role of Educational Audiologists in the EHDI Process Michael Macione, AuD; & Cheryl
A NATIONAL RESOURCE CENTER GUIDE FOR EARLY HEARING HEARING ASSESSMENT DETECTION && MANAGEMENT INTERVENTION Chapter 21 The Role of Educational Audiologists in the EHDI Process Michael Macione, AuD; & Cheryl
A New Era for the Identification and Treatment of Children with Auditory Disorders
 1 A New Era for the Identification and Treatment of Children with Auditory Disorders ROSS J. ROESER AND MARION P. DOWNS Nothing great was ever achieved without enthusiasm. Ralph Waldo Emerson It is a new
1 A New Era for the Identification and Treatment of Children with Auditory Disorders ROSS J. ROESER AND MARION P. DOWNS Nothing great was ever achieved without enthusiasm. Ralph Waldo Emerson It is a new
The Two I s in EHDI: Intervention and Impact. Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK
 The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK Hearing Loss Facts: Brief Overview The most common birth anomaly: 2 to
The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK Hearing Loss Facts: Brief Overview The most common birth anomaly: 2 to
The Colorado Newborn Hearing Screening Project, : On the Threshold of Effective Population-Based Universal Newborn Hearing Screening
 The Colorado Newborn Hearing Screening Project, 1992 1999: On the Threshold of Effective Population-Based Universal Newborn Hearing Screening Albert L. Mehl, MD*, and Vickie Thomson, MA, CCC-A ABSTRACT.
The Colorado Newborn Hearing Screening Project, 1992 1999: On the Threshold of Effective Population-Based Universal Newborn Hearing Screening Albert L. Mehl, MD*, and Vickie Thomson, MA, CCC-A ABSTRACT.
NEW JERSEY ADMINISTRATIVE CODE Copyright (c) 2011 by the New Jersey Office of Administrative Law
 2011 by the New Jersey Office of Administrative Law") Page 1 Title 8, Chapter 19 -- CHAPTER AUTHORITY: NEW JERSEY ADMINISTRATIVE CODE Copyright (c) 2011 by the New Jersey Office of Administrative Law *** This file includes all Regulations adopted and published
Page 1 Title 8, Chapter 19 -- CHAPTER AUTHORITY: NEW JERSEY ADMINISTRATIVE CODE Copyright (c) 2011 by the New Jersey Office of Administrative Law *** This file includes all Regulations adopted and published
GUAM. Newborn Hearing At-A-Glance. Guam EHDI Progress Report. Håfa Ådai! January - December 2012
 GUAM GUAM EARLY HEARING DETECTION & INTERVENTION Newborn Hearing At-A-Glance Guam EHDI Progress Report January - December 2012 Håfa Ådai! The Guam Early Hearing Detection and Intervention (Guam EHDI) Project
GUAM GUAM EARLY HEARING DETECTION & INTERVENTION Newborn Hearing At-A-Glance Guam EHDI Progress Report January - December 2012 Håfa Ådai! The Guam Early Hearing Detection and Intervention (Guam EHDI) Project
Instructions. 1. About how many babies are born or admitted to this hospital each year?
 Instructions This questionnaire asks for information about hospitals* which use a systematic procedure for identifying newborns with hearing loss. In pilot-tests, respondents required an average of 18
Instructions This questionnaire asks for information about hospitals* which use a systematic procedure for identifying newborns with hearing loss. In pilot-tests, respondents required an average of 18
A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS
 A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS 2017 Developed by the Early Hearing Detection & Intervention Parent to Parent Committee A PARENT S GUIDE TO DEAF AND HARD
A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS 2017 Developed by the Early Hearing Detection & Intervention Parent to Parent Committee A PARENT S GUIDE TO DEAF AND HARD
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT
 KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
Progress in Standardization of Reporting and Analysis of Data from Early Hearing Detection and Intervention (EHDI) Programs
 Programs") 2016; 1(2): 2-7 Progress in Standardization of Reporting and Analysis of Data from Early Hearing Detection and Intervention (EHDI) Programs Suhana Alam,MPH., 1 Ashley Satterfield, MPH., 2 Craig A. Mason,
2016; 1(2): 2-7 Progress in Standardization of Reporting and Analysis of Data from Early Hearing Detection and Intervention (EHDI) Programs Suhana Alam,MPH., 1 Ashley Satterfield, MPH., 2 Craig A. Mason,
the time is now: wisconsin s journey towards improving early intervention services
 Marcy Dicker is the director of Outreach for the Wisconsin Educational Services Program for the Deaf and Hard of Hearing. Her background is in providing services to young children, birth to age 3, who
Marcy Dicker is the director of Outreach for the Wisconsin Educational Services Program for the Deaf and Hard of Hearing. Her background is in providing services to young children, birth to age 3, who
Reducing Lost to Follow Up Percentages In EHDI Programs: The Role of Audiology
 Reducing Lost to Follow Up Percentages In EHDI Programs: The Role of Audiology Michael Dybka, Ph.D., CCC-A, FAAA Director Newborn Hearing Screening Program Department of Otolaryngology Audiology Services
Reducing Lost to Follow Up Percentages In EHDI Programs: The Role of Audiology Michael Dybka, Ph.D., CCC-A, FAAA Director Newborn Hearing Screening Program Department of Otolaryngology Audiology Services
The Two I s in EHDI: Intervention and Impact. Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK
 The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK As the CEO of EI Services Hearing Loss Facts: Brief Overview The most
The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK As the CEO of EI Services Hearing Loss Facts: Brief Overview The most
Hearing Screening, Diagnostics and Intervention
 JCIH Newborn Hearing Screening Guidelines 1-3-6 Model By 1 month Screenhearing Hearing Screening, Diagnostics and Intervention By 3 months: Evaluate hearing and complete diagnosticaudiology and otolaryngology
JCIH Newborn Hearing Screening Guidelines 1-3-6 Model By 1 month Screenhearing Hearing Screening, Diagnostics and Intervention By 3 months: Evaluate hearing and complete diagnosticaudiology and otolaryngology
Disclosures. Objectives 2/29/2016. Bradley Golner M.D. FAAP. AzEHDI chapter champion AAP EHDI leadership team
 Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
The Committee on Genetics of the American
 Newborn Hearing Screening: The Great Omission Albert L. Mehl, MD*, and Vickie Thomson, MA ABSTRACT. Objective. The advent of technologic improvements in assessing the hearing of newborn infants has made
Newborn Hearing Screening: The Great Omission Albert L. Mehl, MD*, and Vickie Thomson, MA ABSTRACT. Objective. The advent of technologic improvements in assessing the hearing of newborn infants has made
A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007
 A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007 REPRODUCED WITH PERMISSION FROM PEDIATRICS, VOL. 120, PAGES 898-921, COPYRIGHT 2007 BY THE AAP. COPIES MADE AVAILABLE THROUGH FINANCIAL SUPPORT FROM
A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007 REPRODUCED WITH PERMISSION FROM PEDIATRICS, VOL. 120, PAGES 898-921, COPYRIGHT 2007 BY THE AAP. COPIES MADE AVAILABLE THROUGH FINANCIAL SUPPORT FROM
Hearing loss is the most frequently occurring congenital
 INVITED COMMENTARY Newborn Hearing Screening: Making a Difference Marcia Fort Newborn hearing screening has become the standard of care in the United States, with over 98% of infants born screened for
INVITED COMMENTARY Newborn Hearing Screening: Making a Difference Marcia Fort Newborn hearing screening has become the standard of care in the United States, with over 98% of infants born screened for
FUNCTIONAL HEARING SCREENING WHO WE ARE: YOU TELL ME OBJECTIVES: SLIGHT HIGH FREQUENCY HEARING LOSS OUTLINE: A PASS IS NOT A PASS FOR LIFE!
 FUNCTIONAL HEARING SCREENING A PASS IS NOT A PASS FOR LIFE! KRISTEN TINA SCHRAML CHILDRES, M.S. S, M.A., SPECIAL CCC-A ED. ILLINOIS SCHOOL FOR FOR THE THE DEAF DEAF OUTREA C HC H CONSULT A NA NT/ RT AI
FUNCTIONAL HEARING SCREENING A PASS IS NOT A PASS FOR LIFE! KRISTEN TINA SCHRAML CHILDRES, M.S. S, M.A., SPECIAL CCC-A ED. ILLINOIS SCHOOL FOR FOR THE THE DEAF DEAF OUTREA C HC H CONSULT A NA NT/ RT AI
Collaboration Between WIC and EHDI to Improve Follow-Up of Newborn Hearing Screening in Greater Cincinnati
 Collaboration Between WIC and EHDI to Improve Follow-Up of Newborn Hearing Screening in Greater Cincinnati Lisa Hunter, Ph.D., Scott Wexelblatt, M.D. Jareen Meinzen-Derr, Ph.D., Susan Wiley, M.D. Laura
Collaboration Between WIC and EHDI to Improve Follow-Up of Newborn Hearing Screening in Greater Cincinnati Lisa Hunter, Ph.D., Scott Wexelblatt, M.D. Jareen Meinzen-Derr, Ph.D., Susan Wiley, M.D. Laura
Michael Macione, AuD, & Cheryl DeConde Johnson, EdD. a critical link within the Early Hearing Detection and Intervention (EHDI) process.
 process.") A NATIONAL RESOURCE CENTER GUIDE FOR EARLY HEARING HEARING ASSESSMENT DETECTION && MANAGEMENT INTERVENTION Chapter 21 The Role of Educational Audiologists in the EHDI Process Michael Macione, AuD, & Cheryl
A NATIONAL RESOURCE CENTER GUIDE FOR EARLY HEARING HEARING ASSESSMENT DETECTION && MANAGEMENT INTERVENTION Chapter 21 The Role of Educational Audiologists in the EHDI Process Michael Macione, AuD, & Cheryl
Minnesota Early Hearing Detection & Intervention Annual Report for 2012 Data
 Minnesota Early Hearing Detection & Intervention Annual Report for 2012 Data Table Of Contents Introduction Minnesota Early Hearing Detection and Intervention Program 1 Minnesota Newborn Hearing Screening
Minnesota Early Hearing Detection & Intervention Annual Report for 2012 Data Table Of Contents Introduction Minnesota Early Hearing Detection and Intervention Program 1 Minnesota Newborn Hearing Screening
EHDI Conference 2009 Addison, TX
 Update on the Joint Committee on Infant Hearing Activities EHDI Conference 2009 Addison, TX Judith Widen - University of Kansas Medical Center - Kansas City, KS Judith Harrison, AG Bell Association Washington,
Update on the Joint Committee on Infant Hearing Activities EHDI Conference 2009 Addison, TX Judith Widen - University of Kansas Medical Center - Kansas City, KS Judith Harrison, AG Bell Association Washington,
Early Hearing Detection and Intervention Tracking Research and Integration with Other Newborn Screening Programs
 CENTERS FOR DISEASE CONTROL AND PREVENTION CENTER ON BIRTH DEFECTS AND DEVELOPMENTAL DISABILLITIES EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM SITE VISIT REPORT U.S. Virgin Islands April 29,
CENTERS FOR DISEASE CONTROL AND PREVENTION CENTER ON BIRTH DEFECTS AND DEVELOPMENTAL DISABILLITIES EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM SITE VISIT REPORT U.S. Virgin Islands April 29,
Teleaudiology: Providing Hearing Assessments to Infants and Children Living in Remote and Rural Communities.
 Teleaudiology: Providing Hearing Assessments to Infants and Children Living in Remote and Rural Communities. Presented by: Alison Collins Date: 19/06/2015 Healthy Hearing Program Queensland Offers newborn
Teleaudiology: Providing Hearing Assessments to Infants and Children Living in Remote and Rural Communities. Presented by: Alison Collins Date: 19/06/2015 Healthy Hearing Program Queensland Offers newborn
COACHingto improve NHS Outcomes: Coalition of Ohio Audiologists and Childrens Hospitals
 COACHingto improve NHS Outcomes: Coalition of Ohio Audiologists and Childrens Hospitals 1 Who we are, how we got here Gina Hounam, Ph.D. -Program Manager of Audiology 2 Lisa Hunter, Ph.D. -Scientific Director,
COACHingto improve NHS Outcomes: Coalition of Ohio Audiologists and Childrens Hospitals 1 Who we are, how we got here Gina Hounam, Ph.D. -Program Manager of Audiology 2 Lisa Hunter, Ph.D. -Scientific Director,
Cochlear Implants: The Role of the Early Intervention Specialist. Carissa Moeggenberg, MA, CCC-A February 25, 2008
 Cochlear Implants: The Role of the Early Intervention Specialist Carissa Moeggenberg, MA, CCC-A February 25, 2008 Case Scenario 3 month old baby with a confirmed severe to profound HL 2 Counseling the
Cochlear Implants: The Role of the Early Intervention Specialist Carissa Moeggenberg, MA, CCC-A February 25, 2008 Case Scenario 3 month old baby with a confirmed severe to profound HL 2 Counseling the
Indiana Early Hearing Detection and Intervention (EHDI)
") Indiana Early Hearing Detection and Intervention (EHDI) Suzanne Foley, M.S., CCC-A Regional Audiology Consultant Indiana State Department of Health www.hearing.in.gov PROGRESS in identification of hearing
Indiana Early Hearing Detection and Intervention (EHDI) Suzanne Foley, M.S., CCC-A Regional Audiology Consultant Indiana State Department of Health www.hearing.in.gov PROGRESS in identification of hearing
SCHOOL AUDIOLOGIST STATE STANDARDS CHECKLIST Aurora Public Schools Induction Program
 The Aurora Public Schools (APS) Induction Program is designed to assist School Audiologists in meeting the Colorado Department of Education Colorado Licensing Act of 1991. This checklist serves as documentation
The Aurora Public Schools (APS) Induction Program is designed to assist School Audiologists in meeting the Colorado Department of Education Colorado Licensing Act of 1991. This checklist serves as documentation
Family-centered early intervention for families and children who are deaf or hard of hearing
 Family-centered early intervention for families and children who are deaf or hard of hearing Christine Yoshinaga-Itano, Ph.D. University of Colorado, Boulder Best Practice Matters Family-centered early
Family-centered early intervention for families and children who are deaf or hard of hearing Christine Yoshinaga-Itano, Ph.D. University of Colorado, Boulder Best Practice Matters Family-centered early
Family Experiences Related to Early Hearing Intervention Guidelines in Washington State
 Western Washington University Western CEDAR WWU Honors Program Senior Projects WWU Graduate and Undergraduate Scholarship 6-2018 Family Experiences Related to Early Hearing Intervention Guidelines in Washington
Western Washington University Western CEDAR WWU Honors Program Senior Projects WWU Graduate and Undergraduate Scholarship 6-2018 Family Experiences Related to Early Hearing Intervention Guidelines in Washington
Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module. Inside this issue:
 Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
Chapter 4 : Newborn Screening
 Chapter 4 : Newborn Screening Almost every child born in the United States undergoes state-mandated newborn screening. For each state, a small blood sample ( heel stick ) is collected from each newborn
Chapter 4 : Newborn Screening Almost every child born in the United States undergoes state-mandated newborn screening. For each state, a small blood sample ( heel stick ) is collected from each newborn
Research findings Current trends in early intervention How can you make a difference?
 Research findings Current trends in early intervention How can you make a difference? First deaf person they met was Discovery of having a deaf child is unexpected Impact of having a deaf child is unknown
Research findings Current trends in early intervention How can you make a difference? First deaf person they met was Discovery of having a deaf child is unexpected Impact of having a deaf child is unknown
for Students Pennsylvania Agenda or Deafblind Who Are Deaf, Hard of Hearing,
 Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind In 1988, the Congressional Commission on the Education
Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind In 1988, the Congressional Commission on the Education
1.2. Please refer to our submission dated 27 February for further background information about NDCS.
 Educational Attainment Gap The role of parents and guardians NDCS response to call for written evidence The National Deaf Children s Society (NDCS) welcomes the opportunity to contribute to this call for
Educational Attainment Gap The role of parents and guardians NDCS response to call for written evidence The National Deaf Children s Society (NDCS) welcomes the opportunity to contribute to this call for
Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh
 Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh Consultant of Otorhinolaryngology Otology & Cochlear implant Jeddah - KSA Screening It is the process of applying to a
Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh Consultant of Otorhinolaryngology Otology & Cochlear implant Jeddah - KSA Screening It is the process of applying to a
These materials are Copyright NCHAM (National Center for Hearing Assessment and Management). All rights reserved. They may be reproduced
. All rights reserved. They may be reproduced") These materials are Copyright 2015-2017 NCHAM (National Center for Hearing Assessment and Management). All rights reserved. They may be reproduced and distributed in print or electronic format at no cost
These materials are Copyright 2015-2017 NCHAM (National Center for Hearing Assessment and Management). All rights reserved. They may be reproduced and distributed in print or electronic format at no cost
Using Virtual Technology to Fully Implement EHDDI (Early Hearing Detection, Diagnosis and Intervention) in Rural Settings
 in Rural Settings") Using Virtual Technology to Fully Implement EHDDI (Early Hearing Detection, Diagnosis and Intervention) in Rural Settings March 27, 2018 Kim Hamren, M.Ed, CED, LSLS Cert. AVT Yoko Ishii, AuD, CCC A Maura
Using Virtual Technology to Fully Implement EHDDI (Early Hearing Detection, Diagnosis and Intervention) in Rural Settings March 27, 2018 Kim Hamren, M.Ed, CED, LSLS Cert. AVT Yoko Ishii, AuD, CCC A Maura
A. Executive Summary:
 Award Number: 5UR3DD000790-02 Report Period: July 1, 2012 through June 30, 2013 Name of Grantee: Indiana State Department of Health Address of Grantee: 2 N. Meridian, Indianapolis, IN 46204 Principal Investigator:
Award Number: 5UR3DD000790-02 Report Period: July 1, 2012 through June 30, 2013 Name of Grantee: Indiana State Department of Health Address of Grantee: 2 N. Meridian, Indianapolis, IN 46204 Principal Investigator:
Contents. Foreword by James W. Hall III, PhD and Virginia Ramachandran, Aud, Series Editors Preface
 Contents Foreword by James W. Hall III, PhD and Virginia Ramachandran, Aud, Series Editors Preface ix xi Rationale for Objective Hearing Assessment 1 A Word about Terminology 1 Important Terms and Concepts
Contents Foreword by James W. Hall III, PhD and Virginia Ramachandran, Aud, Series Editors Preface ix xi Rationale for Objective Hearing Assessment 1 A Word about Terminology 1 Important Terms and Concepts
Factors Associated with Newborn Hearing Screening Follow-up
 Factors Associated with Newborn Hearing Screening Follow-up Vickie Thomson, Ph.D. Director, Newborn Screening Programs Colorado Department of Public Health and Environment Children with Special Health
Factors Associated with Newborn Hearing Screening Follow-up Vickie Thomson, Ph.D. Director, Newborn Screening Programs Colorado Department of Public Health and Environment Children with Special Health
My View On Services. Karen Aguilar, MJ, Coalition Director
 My View On Services Karen Aguilar, MJ, Coalition Director Reasons for the Survey Funders Data instead of anecdotal Use for programming going forward Reduce Lost to Follow-up Thank You Young, A.M., Gascon-Ramos,
My View On Services Karen Aguilar, MJ, Coalition Director Reasons for the Survey Funders Data instead of anecdotal Use for programming going forward Reduce Lost to Follow-up Thank You Young, A.M., Gascon-Ramos,
Jackson Roush, PhD University of North Carolina Chapel Hill
 HEARING SCREENING IN THE NEONATAL INTENSIVE CARE UNIT: CURRENT STATUS AND FUTURE NEEDS Shana Jacobs, AuD University of North Carolina Chapel Hill Jackson Roush, PhD University of North Carolina Chapel
HEARING SCREENING IN THE NEONATAL INTENSIVE CARE UNIT: CURRENT STATUS AND FUTURE NEEDS Shana Jacobs, AuD University of North Carolina Chapel Hill Jackson Roush, PhD University of North Carolina Chapel
Deaf Children and Young People
 Deaf Children and Young People Professor Barry Wright Clinical Lead - National Deaf Children Young People and Family Service, York National Deaf Child and Adolescent Mental Health Service (NDCAMHS) Definitions
Deaf Children and Young People Professor Barry Wright Clinical Lead - National Deaf Children Young People and Family Service, York National Deaf Child and Adolescent Mental Health Service (NDCAMHS) Definitions
Learning to Listen with Hearing Technologies: An interdisciplinary perspective on aural rehabilitation. Do not copy without permission of the author
 Learning to Listen with Hearing Technologies: An interdisciplinary perspective on aural rehabilitation Do not copy without permission of the author Learning to Listen as a Child: Aural (Re)habilitation
Learning to Listen with Hearing Technologies: An interdisciplinary perspective on aural rehabilitation Do not copy without permission of the author Learning to Listen as a Child: Aural (Re)habilitation
3. How does your state collect these results? (Check all that apply.) collecting this information.
 collecting this information.") NEWBORN HEARING SCREENING SURVEY Please send completed survey to: Janet Farrell Massachusetts Department of Public Health Bureau of Family and Community Health 250 Washington Street, 4 th Floor Boston,
NEWBORN HEARING SCREENING SURVEY Please send completed survey to: Janet Farrell Massachusetts Department of Public Health Bureau of Family and Community Health 250 Washington Street, 4 th Floor Boston,
EHDI National EHDI Meeting
 EHDI 101 2015 National EHDI Meeting Presenters Hallie Morrow, MD, MPH, EHDI Systems Any Hunt, M.S Early Intervention Marcus Gaffney, MA, Centers for Disease Control and Prevention (CDC) National Structure
EHDI 101 2015 National EHDI Meeting Presenters Hallie Morrow, MD, MPH, EHDI Systems Any Hunt, M.S Early Intervention Marcus Gaffney, MA, Centers for Disease Control and Prevention (CDC) National Structure
AUDIOLOGICAL TESTING OF COCHLEAR IMPLANTED CHILDREN IN AN EARLY INTERVENTION PROGRAMME IN SOUTH AFRICA
 AUDIOLOGICAL TESTING OF COCHLEAR IMPLANTED CHILDREN IN AN EARLY INTERVENTION PROGRAMME IN SOUTH AFRICA Moodley, S. & Störbeck, C. HI HOPES Early Intervention Programme, University of the Witwatersrand
AUDIOLOGICAL TESTING OF COCHLEAR IMPLANTED CHILDREN IN AN EARLY INTERVENTION PROGRAMME IN SOUTH AFRICA Moodley, S. & Störbeck, C. HI HOPES Early Intervention Programme, University of the Witwatersrand
Developing the Medical Home Approach in EHDI. Albert Mehl, M.D. Vickie Thomson, Ph.D.
 Home, Home on the Range Developing the Medical Home Approach in EHDI Albert Mehl, M.D. Vickie Thomson, Ph.D. Colorado s Medical Home Definition The Colorado Medical Home model is an approach to health
Home, Home on the Range Developing the Medical Home Approach in EHDI Albert Mehl, M.D. Vickie Thomson, Ph.D. Colorado s Medical Home Definition The Colorado Medical Home model is an approach to health
Late Newborn Hearing Screening, Late Follow-up, and Multiple Follow-Ups Increase the Risk of Incomplete Audiologic Diagnosis Evaluation
 2016; 1(2): 4955 Late Newborn Hearing Screening, Late Followup, and Multiple FollowUps Increase the Risk of Incomplete Audiologic Diagnosis Evaluation Tri Tran, MD, MPH, 1,2 Ian Ng, MPH Thira Choojitarom,
2016; 1(2): 4955 Late Newborn Hearing Screening, Late Followup, and Multiple FollowUps Increase the Risk of Incomplete Audiologic Diagnosis Evaluation Tri Tran, MD, MPH, 1,2 Ian Ng, MPH Thira Choojitarom,
C HAPTER SEVEN. The Use of FM Technology for Infants and Young Children. Sandra Abbott Gabbard. Introduction
 C HAPTER SEVEN The Use of FM Technology for Infants and Young Children Sandra Abbott Gabbard Introduction The successful trend of identifying hearing loss in the first few weeks of life has resulted in
C HAPTER SEVEN The Use of FM Technology for Infants and Young Children Sandra Abbott Gabbard Introduction The successful trend of identifying hearing loss in the first few weeks of life has resulted in
A PROGRAMMATIC ANALYSIS OF A NEWBORN HEARING SCREENING PROGRAM FOR EVALUATION AND IMPROVEMENT
 A PROGRAMMATIC ANALYSIS OF A NEWBORN HEARING SCREENING PROGRAM FOR EVALUATION AND IMPROVEMENT by VICKIE RAE THOMSON B.S. University of Northern Colorado, 1977 M.A. University of Northern Colorado, 1979
A PROGRAMMATIC ANALYSIS OF A NEWBORN HEARING SCREENING PROGRAM FOR EVALUATION AND IMPROVEMENT by VICKIE RAE THOMSON B.S. University of Northern Colorado, 1977 M.A. University of Northern Colorado, 1979
H 7978 SUBSTITUTE A ======== LC005519/SUB A ======== S T A T E O F R H O D E I S L A N D
 01 -- H SUBSTITUTE A LC001/SUB A S T A T E O F R H O D E I S L A N D IN GENERAL ASSEMBLY JANUARY SESSION, A.D. 01 A N A C T RELATING TO EDUCATION - INSTRUCTION FOR DEAF OR HARD-OF-HEARING STUDENTS Introduced
01 -- H SUBSTITUTE A LC001/SUB A S T A T E O F R H O D E I S L A N D IN GENERAL ASSEMBLY JANUARY SESSION, A.D. 01 A N A C T RELATING TO EDUCATION - INSTRUCTION FOR DEAF OR HARD-OF-HEARING STUDENTS Introduced
Referral Rates and Costs of Our Modified Two-Step Newborn Hearing Screening Program at a Japanese Perinatal Center
 Original Article Elmer Press Referral Rates and Costs of Our Modified Two-Step Newborn Hearing Screening Program at a Japanese Perinatal Center Mieko Sato a, Shunji Suzuki a, b Abstract Background: We
Original Article Elmer Press Referral Rates and Costs of Our Modified Two-Step Newborn Hearing Screening Program at a Japanese Perinatal Center Mieko Sato a, Shunji Suzuki a, b Abstract Background: We
THE UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL
 THE UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL DIVISION OF SPEECH AND HEARING SCIENCES AUDIOLOGY COURSE LISTINGS AND DESCRIPTIONS 706 CLINICAL PRACTICUM IN AUDIOLOGY (1-3). Prerequisite, permission of
THE UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL DIVISION OF SPEECH AND HEARING SCIENCES AUDIOLOGY COURSE LISTINGS AND DESCRIPTIONS 706 CLINICAL PRACTICUM IN AUDIOLOGY (1-3). Prerequisite, permission of
Map of Medicine National Library for Health
 Map of Medicine National Library for Health Newborn hearing screening Check eligibility Eligible for screening Not eligible for screening Consider risk factors for hearing loss Provide information and
Map of Medicine National Library for Health Newborn hearing screening Check eligibility Eligible for screening Not eligible for screening Consider risk factors for hearing loss Provide information and
What is the Role of the Hearing Specialist in Early Steps? Karen Anderson, PhD Coordinator of Early Intervention Services for Hearing and Vision
 What is the Role of the Hearing Specialist in Early Steps? Karen Anderson, PhD Coordinator of Early Intervention Services for Hearing and Vision What is a Hearing Specialist? A person with expertise in
What is the Role of the Hearing Specialist in Early Steps? Karen Anderson, PhD Coordinator of Early Intervention Services for Hearing and Vision What is a Hearing Specialist? A person with expertise in
universal newborn hearing Screening
 الرحمن الرحيم بم بسم الله universal newborn hearing Screening In various Countries Dr.A. Aziz Jifrey د. عبدالعزيز عبدالله الجفري Assistant Prof, Consultant, انف واذن وحنجرة استشاري ا.م. كلية الطب م. جامعة
الرحمن الرحيم بم بسم الله universal newborn hearing Screening In various Countries Dr.A. Aziz Jifrey د. عبدالعزيز عبدالله الجفري Assistant Prof, Consultant, انف واذن وحنجرة استشاري ا.م. كلية الطب م. جامعة
How Do We Support Families in 2010?
 How Do We Support Families in 2010? A look at family support in newborn hearing screening and follow up ` Define Family Support Family support is the provision of respectful collaboration to provide empowerment
How Do We Support Families in 2010? A look at family support in newborn hearing screening and follow up ` Define Family Support Family support is the provision of respectful collaboration to provide empowerment
Audiology Services. Table of Contents. Audiology Services Guidelines : Hearing services
 Audiology Services Table of Contents Audiology Services Guidelines... 2 317:30-3-65.9 Hearing services... 3-4 Audiology Services- General Considerations for Prior Authorization... 5-6 Audiogram and other
Audiology Services Table of Contents Audiology Services Guidelines... 2 317:30-3-65.9 Hearing services... 3-4 Audiology Services- General Considerations for Prior Authorization... 5-6 Audiogram and other
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018
 The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
PACIFIC Pre- EHDI Mee.ng March 3, 2012
 Guam Early Hearing Detec>on and Interven>on Project (Guam EHDI) Tele Audiology PACIFIC Pre- EHDI Mee.ng March 3, 2012 St. Louis, Missouri Will 30 minutes enough to cover the following aspects: 1. 2. 3.
Guam Early Hearing Detec>on and Interven>on Project (Guam EHDI) Tele Audiology PACIFIC Pre- EHDI Mee.ng March 3, 2012 St. Louis, Missouri Will 30 minutes enough to cover the following aspects: 1. 2. 3.
3/20/2017. D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital
 D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
3. If the presence of middle ear pathology is suspected based on immittance test results, case history, or otoscopic exam, perform Wave V threshold se
 GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
Kansas Successful Strategies in Reducing Loss to Follow-Up/Loss to Documentation
 Kansas Successful Strategies in Reducing Loss to Follow-Up/Loss to Documentation 13th Annual EHDI Conference Jacksonville, FL Liz Abbey, M.A., Audiologist/Kansas EHDI Coordinator Kelly Barr, Kansas Data
Kansas Successful Strategies in Reducing Loss to Follow-Up/Loss to Documentation 13th Annual EHDI Conference Jacksonville, FL Liz Abbey, M.A., Audiologist/Kansas EHDI Coordinator Kelly Barr, Kansas Data
I. Project Identifier Information
 I. Project Identifier Information a. Grant Number: H61MC24882 b. Project Title: Universal Newborn Hearing Screening and Intervention c. Organization Name: d. Mailing Address: Commonwealth of Pennsylvania;
I. Project Identifier Information a. Grant Number: H61MC24882 b. Project Title: Universal Newborn Hearing Screening and Intervention c. Organization Name: d. Mailing Address: Commonwealth of Pennsylvania;
Simplifying Reporting of Communication Development Outcomes for Infants and Toddlers with Hearing Loss
 Simplifying Reporting of Communication Development Outcomes for Infants and Toddlers with Hearing Loss Karen Anderson, PhD Florida EHDI Audiology Consultant Coordinator of EI Services for Hearing Impaired
Simplifying Reporting of Communication Development Outcomes for Infants and Toddlers with Hearing Loss Karen Anderson, PhD Florida EHDI Audiology Consultant Coordinator of EI Services for Hearing Impaired
Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind
 Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind In 1988, the Congressional Commission on the Education
Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind Pennsylvania Agenda for Students Who Are Deaf, Hard of Hearing, or Deafblind In 1988, the Congressional Commission on the Education
Effective factors on Auditory Brainstem Response test in Newborns
 BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
BAEA Roles and Competencies. 1. Child and Family Support.
 BAEA Roles and Competencies 1. Child and Family Support. 1.1 The Educational Audiologists Role may involve the following: 1.1.1 Act as a key member of a multi-professional team offering a seamless family
BAEA Roles and Competencies 1. Child and Family Support. 1.1 The Educational Audiologists Role may involve the following: 1.1.1 Act as a key member of a multi-professional team offering a seamless family
OAE Screening in Healthcare Settings: A Pilot Project. Terry E. Foust, AuD William Eiserman, PhD Lenore Shisler, MS
 OAE Screening in Healthcare Settings: A Pilot Project Terry E. Foust, AuD William Eiserman, PhD Lenore Shisler, MS Why screen in healthcare settings? Up to 50% lost to follow up rates Late onset or progressive
OAE Screening in Healthcare Settings: A Pilot Project Terry E. Foust, AuD William Eiserman, PhD Lenore Shisler, MS Why screen in healthcare settings? Up to 50% lost to follow up rates Late onset or progressive
Making Connections: Early Detection Hearing and Intervention through the Medical Home Model Podcast Series
 Making Connections: Early Detection Hearing and Intervention through the Medical Home Model Podcast Series Podcast 2 Utilization of the Teach-Back Methodology in Early Hearing Detection and Intervention
Making Connections: Early Detection Hearing and Intervention through the Medical Home Model Podcast Series Podcast 2 Utilization of the Teach-Back Methodology in Early Hearing Detection and Intervention
Surveying Pennsylvania s Families of Young Children who are Deaf/Hard of Hearing
 Surveying Pennsylvania s Families of Young Children who are Deaf/Hard of Hearing Results of the FY 2016-17 Family Satisfaction Survey & Record Review Your chance to think how to use this information in
Surveying Pennsylvania s Families of Young Children who are Deaf/Hard of Hearing Results of the FY 2016-17 Family Satisfaction Survey & Record Review Your chance to think how to use this information in
Date January 20, Contact Information
 Curriculum Vitae Deborah Golant Badawi, MD Medical Director, Office of Genetics and People with Special Health Care Needs Maryland Department of Health and Mental Hygiene Date January 20, 2016 Contact
Curriculum Vitae Deborah Golant Badawi, MD Medical Director, Office of Genetics and People with Special Health Care Needs Maryland Department of Health and Mental Hygiene Date January 20, 2016 Contact
Until January 2002, the universal screening programme
 78 ORIGINAL ARTICLE Maternal anxiety and satisfaction following infant hearing screening: a comparison of the health visitor distraction test and newborn hearing screening Rachel Crockett, Holly Baker,
78 ORIGINAL ARTICLE Maternal anxiety and satisfaction following infant hearing screening: a comparison of the health visitor distraction test and newborn hearing screening Rachel Crockett, Holly Baker,
The Evolution of Early HearingDetection and Intervention Programs in the United States
 Utah State University From the SelectedWorks of Karen F. Munoz January 1, 2010 The Evolution of Early HearingDetection and Intervention Programs in the United States K. White I. Forsman J. Eichwald Karen
Utah State University From the SelectedWorks of Karen F. Munoz January 1, 2010 The Evolution of Early HearingDetection and Intervention Programs in the United States K. White I. Forsman J. Eichwald Karen
HEALTH VISITOR INFORMATION PACK
 HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods
HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods