Hearing Status Questionnaire Instructions
|
|
|
- Gillian Henry
- 5 years ago
- Views:
Transcription
1 Hearing Status Questionnaire Instructions TABLE OF CONTENTS Introduction...1 Help Me Grow Hearing Status Questionnaire...2 General Information...3 Part I...5 Part II...6 Diagnosed Medical Conditions...6 Risk Factors for Hearing Loss...7 Blood Relatives with Permanent Hearing Loss...8 Behavioral Observation by Parent/Guardian...10 Parent/Guardian Concerns Regarding Child s Hearing...11 Appendix (Medical Conditions)...12
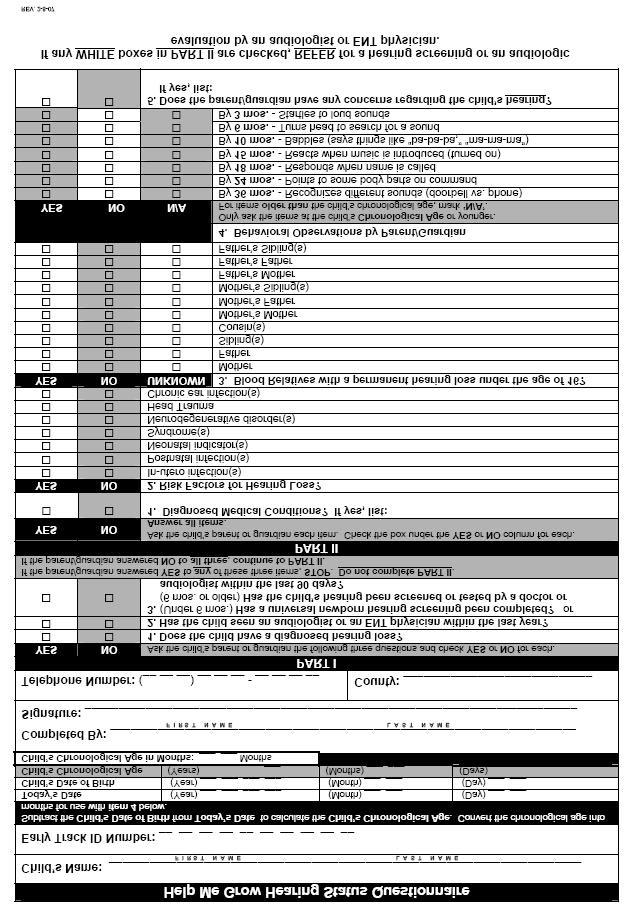
2 Introduction These instructions are to accompany the training DVD for the Help Me Grow Hearing Status Questionnaire. The Help Me Grow Hearing Status Questionnaire meets the federal requirement for a hearing status check. By definition, a hearing screening is a quick physiological hearing test, using calibrated equipment and performed by an audiologist, a trained RN or a physician. There are no valid or accepted paper hearing screenings, so DO NOT refer to the Hearing Status Questionnaire as a screening. Only those who have completed viewing the training DVD may complete the Hearing Status Questionnaire. The Help Me Grow Service Coordinators who have completed viewing the training DVD will be responsible for completing the Hearing Status Questionnaire with the parent/guardian of every child referred for Help Me Grow ongoing services (Part C and at-risk). The Questionnaire must be completed within 45 days of referral to Help Me Grow. This Questionnaire is not to be completed on prenatal referrals or newborn home visits. The Questionnaire is to be completed in person with the child s parent/guardian. DO NOT complete over the telephone. DO NOT send to a parent/guardian for completion. PRINT LEGIBLY IN INK WHEN COMPLETING! It must be emphasized that all information on the Hearing Status Questionnaire must be printed clearly. It is imperative that both letters and numbers are PRINTED LEGIBLY. Nothing should be left blank. There should be no items left blank on the Hearing Status Questionnaire (unless a parent/guardian answers yes to any of the three items in Part I, in which case Part II does not need to be completed). When the Hearing Status Questionnaire has been completed, carefully review what has been answered. If any of the WHITE boxes have been checked (YES for everything except Behavioral Observations; NO only for Behavioral Observations), the child should be referred to his or her primary care physician/medical home to be referred to an audiologist or an ENT physician for an actual hearing screening or an audiologic evaluation. The completed Questionnaire is to be placed in the child s HMG record (which may be checked as part of the monitoring process), and entered in Early Track 3.0. Questions? Contact Sharon Marcum at by at sharon.marcum@odh.ohio.gov. or by telephone at
3 2
4 General Information This section is very important. It is critical that this section is completed neatly and accurately in its entirety. Double-check before ending the session with the parent/caregiver to make sure that there is no missing information. PRINT NEATLY! A. Child s Name: Print the child s first and last name in the following format: First Last Example: The child referred is named Johnny Brown; print Johnny Brown B. Early Track Identification Number (ET ID#): Print the child s Early Track Identification Number in its entirety. Enter one number per space to make sure that the entire ET ID# (all ten digits) has been included. Ex: Johnny s ET ID# is ; print NOTE: If the Service Coordinator does not have the child s ET ID# at the time that the Help Me Grow Hearing Status Questionnaire is completed, the ET ID# MUST be entered. C. Today s Date: Print the date on which you and the parent/guardian completed the Hearing Status Questionnaire in the spaces provided. The date will be entered in following format: YYYY/MM/DD Ex: This Questionnaire was completed with Johnny s mother on September 27, 2006; print D. Child s Date of Birth: Print the date that the child was born in the spaces provided. The date will be entered in following format: YYYY/MM/DD Ex: Johnny was born on October 26, 2004; print E. Child s Chronological Age: To calculate the child s chronological age, subtract the Child s Date of Birth from Today s Date. Print the results in the spaces provided. Ex1: If the values (year, month, day) for the date of birth are less than the values for today s date, do straight subtraction (Today s Date) (Date of Birth) (Child s Chronological Age) Ex2: If the day under Date of Birth is a larger number than the day under Today s Date, borrow 30 (days) from the month. Always use 30 days. Then do straight subtraction (Today s Date) (Today s Date) (Date of Birth) (Date of Birth) (Child s Chronological Age) 3
5 2004 Ex3: If the month under Date of Birth is a larger number than the month under Today s Date, borrow 12 (months) from the year. Always use 12 months. Then do straight subtraction (Today s Date) (Today s Date) (Date of Birth) (Date of Birth) (Child s Chronological Age) F. Child s Chronological Age in Months: Once you ve calculated the child s chronological age, convert that age into months (this will be used in Question 4). To convert to months, multiply the years value by 12, then add the months value. If the days value is 15 or more, round up one month. If the days value is 14 or less, do not round. Ex1: The Chronological Ages from above would convert as follows: = 26 months (2 x 12 = 24; = 26; days = 2, so do not round) = 25 months (2 x 12 = 24; = 25; days = 3, so do not round) = 27 months (2 x 12 = 24; = 27; days = 2, so do not round). Ex2: If a Chronological Age was calculated to be 2 years, 11 months, 16 days: = 36 months (2 x 12 = 24; = 35; days = 16, so round up). G. Completed by: PRINT your first name and last name. DO NOT sign or write in cursive! Your name must be legible. Ex: Your name is Jenny Peters; neatly print Jenny Peters H. Signature: This is the ONLY place on the Questionnaire where you are not required to print! Sign your name as you normally would when a signature is required. I. County: PRINT the county in which your Help Me Grow program is located. Ex: Your Help Me Grow program serves Guernsey County, neatly print Guernsey J. Telephone Number: Print the telephone number where you can be reached at work in the spaces provided. Be sure to include your area code. Ex: Your personal line at HMG is (937) ; neatly print (937)
6 PART I This section is to be completed on every referral for Help Me Grow ongoing services (Part C and at-risk). Do not use with prenatal referrals or newborn home visits. Ask the child s parent/guardian each of the three questions. After the parent/guardian answers each question, place an X in the box under YES or NO according to their answer. ASK EVERY PARENT/GUARDIAN ALL THREE QUESTIONS. 1. Does the child have a diagnosed hearing loss? 2. Has the child seen an audiologist or ENT physician within the last year? 3. The question you ask will depend on the child s chronological age in months. If the child is under six (6) months old, ask: Has a universal newborn hearing screening been completed? If the child is six (6) months old or older, ask: Has the child s hearing been screened or tested by a doctor or audiologist within the last 90 days? For each of the three questions: If the parent/guardian answers YES, place an X in the box under YES. Continue to the next question. If the parent/guardian answers NO, place an X in the box under NO. Continue to the next question. NOTES: If any of these three questions is answered YES, the Hearing Status Questionnaire is complete. Do not continue to Part II. Request a copy of any results to provide documentation in the child s HMG record. If the parent/guardian reports that the child has a diagnosed hearing loss, provide the parent/guardian information about the Regional Infant Hearing Program (RIHP), and refer the child to the RIHP for services. If the parent/guardian answers NO to ALL THREE questions, continue to PART II. Ex1: The mother answers that her child does not have a diagnosed hearing loss, place an X in the box under NO and continue to the next question. Ex2: The mother answers that her child has seen an audiologist in the past 180 days, place an X in the box under YES and continue to the next question. DO NOT continue to Part II. Request a copy of any results to provide documentation in the child s HMG record. 5
7 PART II For this section, remember that you are not a medical provider. DO NOT make diagnostic assumptions. DO NOT request the medical chart for review. Mark ALL QUESTIONS based on parent/guardian answers. If a parent/guardian does not understand, or has questions, use the examples below for clarification. DO NOT answer for any parent/guardian! 1. Diagnosed Medical Conditions Ask the parent/guardian if the child has any diagnosed medical conditions that could affect his/her hearing (see Appendix for a list of medical conditions that may include hearing loss). NOTE: Medical conditions not listed in the Appendix are not closely associated with hearing loss. These should not be listed, and should not generate a referral at the end of the Questionnaire. Examples of medical conditions not associated with hearing loss include asthma, allergies, club foot, or apnea. Does (child s name) have any diagnosed medical conditions? If the parent/guardian answers YES, and it is a medical condition listed in the Appendix, place an X in the box under YES. Neatly PRINT the condition(s) that the parent/guardian named in the space provided. Continue to item #2. If the parent/guardian answers NO, or names a diagnosed condition that is not listed in the Appendix, place an X in the box under NO. Continue to item #2. Ex1: If the parent answers that Johnny has been diagnosed with Down s Syndrome, check the Appendix. Since Down s Syndrome is listed in the Appendix, place an X in the box under YES and neatly print Down s Syndrome in the space provided. Ex2: If the parent says that Johnny has been diagnosed with asthma, check the Appendix. Since asthma is not listed in the Appendix, place an X in the box under NO. 6
8 2. Risk Factors for Hearing Loss The presence of a risk factor or factors does not indicate an actual hearing loss. Risk factors simply indicate an increased possibility of hearing loss. In the 2000 position statement, the Joint Committee on Infant Hearing (JCIH) recommended using the following risk factors for hearing loss for infants 29 days through two years of age: In-utero infection(s) - An infection in the mother/child before birth (i.e, Cytomegalovirus, herpes, rubella, syphilis, toxoplasmosis). Postnatal Infection(s) - An infection in the child after birth that is associated with sensorineural hearing loss (i.e., bacterial meningitis). Neonatal Indicator(s) - Condition(s) in the newborn, specifically hyperbilirubinemia requiring an exchange transfusion, persistent pulmonary hypertension requiring mechanical ventilation, and conditions requiring the use of extracorporeal membrane oxygenation (ECMO). Syndrome(s) - A diagnosed syndrome or syndromes associated with progressive hearing loss (hearing loss that develops and increases over time), including Neurofibromatosis, osteopetrosis, Usher s Syndrome. See the Appendix for a list of medical conditions and syndromes that may include hearing loss. Neurodegenerative Disorder(s) - Disorders that can affect hearing (including Hunter syndrome), or sensory motor neuropathies such as Friedreich s ataxia and Charcot- Marie-Tooth syndrome. See the Appendix for a list of medical conditions and syndromes that may include hearing loss. Head Trauma - Any sharp blow to the head (i.e., falling down, being hit by a baseball, physical abuse). Chronic Ear Infections - Ear infection including middle ear fluid lasting three months or longer. A mild or short-term (under three months) ear infection does not count. Ask the parent/guardian if the child has had each of the listed risk factors. If the parent/guardian answers YES to any of the seven risk factors, place an X in the box under YES next to that risk factor. Continue until all seven risk factors have been addressed. If the parent/guardian answers NO to any of the seven risk factors, place an X in the box under NO next to that risk factor. Continue until all seven risk factors have been addressed. 7
9 3. Blood Relatives with Permanent Hearing Loss The term blood relatives means family members who are biologically related to the child. This excludes any step- or foster- parents, siblings, grandparents, etc. This question only refers to the child s actual blood relatives. You will be asking the parent/guardian if any of the child s blood relatives have a permanent hearing loss that started before the age of sixteen and was not caused by an illness, accident or injury. For a parent/guardian to answer YES for any of the blood relatives listed, the hearing loss must meet the following criteria: a. The hearing loss is permanent (i.e., not correctible). Any temporary hearing loss does not count. Ex: A seven year-old sister suffering from repeated ear infections does not count. b. The hearing loss must have begun prior to the relative s sixteenth (16 th ) birthday. Ex: Any relative who developed a hearing loss later in life does not count. c. The hearing loss must not have been caused by an illness (i.e., measles). Ex: The child s mother has had a permanent hearing loss since age eight (8), due to measles; this does not count. Hearing loss due to repeated ear infections or middle ear fluid do not count. d. The hearing loss was not caused by an accident or injury. Ex: A brother with a hearing loss since age 14 due to a football injury does not count. Hearing loss due to head trauma, concussion, torn eardrum, or objects in the ear does not count. Ask about each of the following blood relatives: a. Mother - The child s biological mother only. This does not include a stepmother, adoptive mother, foster mother, guardian, caregiver, or father s partner. b. Father - The child s biological father only. This does not include a stepfather, adoptive father, foster father, guardian, caregiver, or mother s partner. c. Sibling(s) - The child s brother(s) and/or sister(s) that share at least one biological parent. This does include half-brothers and/or half-sisters, but does not include stepbrothers and/or stepsisters. d. Cousin(s) - The child s first cousins only; the biological children of the mother s and father s biological sibling(s). This does not include second/third/fourth cousins, stepcousins or adopted cousins. e. Mother s Mother - The child s maternal grandmother, only if she is the mother s biological mother. This does not include the mother s stepmother or adoptive mother. f. Mother s Father - The child s maternal grandfather, only if he is the mother s biological father. This does not include the mother s stepfather or adoptive father. 8
10 g. Mother s Sibling(s) - The mother s brother(s) and/or sister(s) that share at least one biological parent. This does include half-brothers and/or half-sisters, but does not include stepbrothers and/or stepsisters. h. Father s Mother - The child s paternal grandmother, only if she is the father s biological mother. This does not include the father s stepmother or adoptive mother. i. Father s Father - The child s paternal grandfather, only if he is the father s biological father. This does not include the father s stepfather or adoptive father. j. Father s Sibling(s) - The child s aunt(s) and/or uncle(s) that are brother(s) and/or sister(s) that share at least one biological parent with the child s father. This does include half-brothers and/or half-sisters, but does not include stepbrothers and/or stepsisters. Do you know if (child s name) s had a permanent hearing loss before they were sixteen that was not due to an illness, accident or injury? If the parent/guardian answers YES, verify that the hearing loss meets the four criteria listed above (a-d). If it meets all four criteria, place an X in the box under YES next to that relative. Continue to the next listed blood relative until all ten have been addressed. If the parent/guardian answers NO or doubts that the relative has/had a hearing loss (i.e., I don t think so ), place an X in the box under NO. Continue to the next listed blood relative until all ten have been addressed. If the parent/guardian does not know the hearing status of a particular blood relative (i.e., unknown father; adopted or foster child), place an X in the box under UNKNOWN. Continue to the next listed blood relative until all ten have been addressed. 9
11 4. Behavioral Observations by Parent/Guardian Remember that you are not a medical provider. DO NOT enter information based on your observations; it is the parent/guardian whose observations that are being recorded. The list presented contains hearing milestones, behaviors that are usually observed by a certain age in normally-hearing and normally-developing children. Each behavior is labeled By months. By the stated age, each behavior should be observed in normally-hearing and normally-developing children. Review the child s chronological age in months that was calculated at the top of the Hearing Status Questionnaire. Determine which category the child is in. Do not place a child in the category that is older than their chronological age. Ex1: Johnny is 13 mos. old, so he is in the category labeled By 10 months. DO NOT place him in the By 15 months category. Place an X in the box under N/A (Not Applicable) for all categories older than the child. Do not leave anything blank. Ex2: Johnny is 13 months old. Place an X under N/A for the 36, 24, 18 and 15-month-old categories. Ask the parent/guardian if they have observed the behaviors listed in the 10, 6 and 3-month-old categories and place an X under YES or NO for each behavior based on the parent s/guardian s response. Ask the parent/guardian if the child has been observed doing the behaviors listed for the child's category and all categories younger than the child s chronological age. Phrase each question with Does (child s name)? and fill in the blank with the behavior as listed. Ex4: By 3 mos. - Startles to loud sounds; Ask the parent/guardian Does Johnny startle to loud sounds? Review the child s chronological age in months. Place an X in the box under N/A (Not Applicable) for all categories older than the child. Ask the parent/guardian if they have observed the child doing the behaviors listed for the child's category and all categories younger than the child s chronological age. If the parent/guardian answers YES, place an X in the box under YES next to that behavior. If the parent/guardian answers NO, place an X in the box under NO. Continue until the child s category and all categories younger than the child s chronological age have been addressed. 10
12 5. Parent/Guardian Concerns Regarding Child s Hearing Ask the parent/guardian if they have any concerns about the child s hearing. Do you have any concerns about (child s name) s hearing? If the parent/guardian answers YES, place an X in the box under YES. List any concerns in the space provided. PRINT NEATLY. If the parent/guardian answers NO, place an X in the box under NO. NOTE: This Questionnaire is solely focused on hearing. A parent may state that they do not have concerns about their child s hearing, but that they do have some concerns about speech and/or language development. DO NOT indicate these concerns on this form, but note them in the child s chart and follow-up in an appropriate manner. 11
13 APPENDIX The following is a list of medical conditions that may include hearing loss (from Hearing in Children, Fourth Edition by Jerry L. Northern, Ph.D. and Marion P. Downs, Dr.H.S.). Absence of the Tibia (Robert s Syndrome) Achondroplasia (Chondrodystrophia Fetalis) Acoustic Neuroma Acrocephalosyndactyly Alber-Schönberg Disease of Osteopetrosis (Chalk Bone Disease; Ivory Bone Disease; Marble Bone Disease) Albinism with Blue Irides (Oculocutaneous Albinism) Alport s Syndrome (Hereditary Nephritis with Nerve Deafness) Amyloidosis, Nephritis and Urticaria (Muckle-Wells Syndrome) Apert s Syndrome (Acrocephalosyndactyly) Atopic Dermatitis Brevicollis Cardioauditory Syndrome Cerebral Palsy Cervico-oculoacoustic Dysplasia Cleft Palate and/or Lip Cleidocranial Dysostosis (Cleidocranial Dysplasia; Osteodental Dysplasia) Cockayne s Syndrome Cornelia de Lange Syndrome Craniofacial Dystosis Crouzon s Syndrome Cryptophthalmus Cytomegalovirus Disease Diastrophic Dwarfism Down s Syndrome (Trisomy 21 Syndrome; Mongolism) Duane s Syndrome (Cervico-oculoacoustic Dysplasia) Dyschondrosteosis Ectodermal Dysplasia (Ectrosyndactyly, Ectodermal Dysplasia and Cleft Palate Syndrome; Lobster- Claw Syndrome) Engelmann s Syndrome (Craniodiaphyseal Dysplasia; Diaphyseal Dysplasia) Franconi s Anemia Syndrome (infantile and/or Adolesceny Renal Tubular Acidosis) Fetal Alcohol Syndrome Fragile X Syndrome Friedrich s Ataxia Goiter, Stippled Epiphysis and High Protein-Bound Iodine Goldenhar s Syndrome (Oculoauriculovertebral Dysplasia) Hallgren s Syndrome Hand-Hearing Syndrome (Hand Muscle Wasting and Sensorineural Deafness) Hemifacial Microsomia Hereditary Hyperphosphatasia Herrmann s Syndrome (Photomyelonus, Diabetes Mellitus, Nephropathy and Sensorineural Deafness) Hurler s Syndrome-Hunter s Syndrome (Mucopolysaccharidosis I and II) Hydrocephalus Hyperprolinemia I and II Hyperuricemia Jervell and Lange-Nielsen Syndrome (Cardioauditory Syndrome; Surdocardiac Syndrome) Keratopachyderma and Digital Constrictions Klippel-Feil Syndrome (Brevicollis; Cervico-oculoacoustic Dysplasia; Wildervanck s Syndrome) 12
14 Knuckle Pads and Leukonychia Laurence-Moon-Biedl-Bardet Syndromes Leri-Weill Disease Lobster-Claw Syndrome Long Arm 18 Deletion Syndrome Madelung s Deformity (Dyschondrosteosis; Leri-Weill Disease) Malformed Low-Set Ears Syndrome Marfan s Syndrome Measles Meningitis Möbius Syndrome (Facial Dysplagia) Mohr s Syndrome (Oral-Facial-Digital II; OFD II) Mumps Muscular Dystrophy Myoclonic Epilepsy Myopia and Congenital Deafness Nephrosis, Urinary Tract Malformations Neurofibromatosis Norrie s Syndrome (Oculoacousticicereberal Degeneration) Oculoacousticicereberal Degeneration Onychodystrophy Optic Atrophy and Diabetes Mellitus Optic Atrophy and Polyneuropathy Opticocochleodentate Degenration Osteogenesis Imperfecta (Van Der Hoeve s Syndrome) Osteopetrosis Otopalatodigital Syndrome Paget s Disease (Juvenile) (Hereditary Hyperphosphatasia) Pendred s Syndrome (Goiter and Profound Deafness) Piebaldness Pierre Robin Sequence (Cleft Palate, Micrognatha, and Glossoptosis) Pili Torti Preauricular Abnormalities Pyle s Disease (Craniometaphysial Dysplasia) Refsum s Syndrome Renal-Genital Syndrome Renal Tubular Acidosis (Fanconi s Anemia Syndrome) Richards-Rundle Syndrome (Ataxia-Hypogonadism Syndrome) Rubella, Congenital Saddle Nose and Myopia (Marshall Syndrome) Sensory Radicular Neuropathy Symphalangism Syphilis, Congenital Treacher Collins Syndrome (Mandibular Dysostosis, First Arch Syndrome) Trisomy Syndrome Trisomy 18 Syndrome Trisomy 21 Syndrome Turner s Syndrome (Gonadal Dysgenesis) Usher s Syndrome Van Buchem s Syndrome (Hyperostosis Corticalis Generalisata) Van Der Hoeve s Syndrome (Osteogenesis Imperfecta) Von Recklinghausen s Neurofibromatosis Waardenberg s Syndrome Wildervanck s Syndrome (Otofaciocervical Dysmorphia; Cervico-oculoacoustic Dysplasia) 13
JCIH Recommendations for Following Children At Risk for Hearing Loss
 JCIH Recommendations for Following Children At Risk for Hearing Loss With newborn hearing screening, the Joint Commission on Infant Hearing (JCIH) has recommendations for following children who may be
JCIH Recommendations for Following Children At Risk for Hearing Loss With newborn hearing screening, the Joint Commission on Infant Hearing (JCIH) has recommendations for following children who may be
Iowa Deafblind Registry New Referral
 Iowa Deafblind Registry New Referral Today s Date: Child s Name First: Address: Is there an IFSP or IEP in place for this child? Yes. Although written parental consent is not necessary for adding this
Iowa Deafblind Registry New Referral Today s Date: Child s Name First: Address: Is there an IFSP or IEP in place for this child? Yes. Although written parental consent is not necessary for adding this
Parent 1/Guardian Information. Parent 1/Guardian Information (If Different from Above)
") New Jersey Center on Deafblindness CENSUS REPORTING FORM (Please Print) Today s Date: Name of the Reporter: CHILD/STUDENT INFORMATION Last Name: First Name: MI: Age: Gender: M F Date of Birth: / / MM DD
New Jersey Center on Deafblindness CENSUS REPORTING FORM (Please Print) Today s Date: Name of the Reporter: CHILD/STUDENT INFORMATION Last Name: First Name: MI: Age: Gender: M F Date of Birth: / / MM DD
Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014)
") Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014) Being deaf is a worse handicap than being blind because deafness separates people from people. -Helen Keller Goals of the Newborn
Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014) Being deaf is a worse handicap than being blind because deafness separates people from people. -Helen Keller Goals of the Newborn
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT
 KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
COLORADO STATEWIDE CHILD COUNT FOR CHILDREN AND YOUTH WITH COMBINED VISION AND HEARING LOSS (DEAF-BLINDNESS)
") COLORADO STATEWIDE CHILD COUNT FOR CHILDREN AND YOUTH WITH COMBINED VISION AND HEARING LOSS (DEAF-BLINDNESS) Colorado Department of Education / Exceptional Student Services Unit 1560 Broadway, Suite 1100,
COLORADO STATEWIDE CHILD COUNT FOR CHILDREN AND YOUTH WITH COMBINED VISION AND HEARING LOSS (DEAF-BLINDNESS) Colorado Department of Education / Exceptional Student Services Unit 1560 Broadway, Suite 1100,
New York Deaf-Blind Collaborative Referring a Child
 New York Deaf-Blind Collaborative Referring a Child NYDBC Overview The New York Deaf-Blind Collaborative (NYDBC) is statewide grant that provides technical assistance to improve services for children and
New York Deaf-Blind Collaborative Referring a Child NYDBC Overview The New York Deaf-Blind Collaborative (NYDBC) is statewide grant that provides technical assistance to improve services for children and
Early Identification of Young Children with Deaf-Blindness
 Early Identification of Young Children with Deaf-Blindness Jerry G. Petroff & Madeline Appell Based on the work of.. Dr. Sarah Cawthon, M.D. What is Deaf-Blindness? the term deaf-blind, with respect to
Early Identification of Young Children with Deaf-Blindness Jerry G. Petroff & Madeline Appell Based on the work of.. Dr. Sarah Cawthon, M.D. What is Deaf-Blindness? the term deaf-blind, with respect to
IN-VITRO FERTILIZATION WITH DONATED OOCYTES COMPREHENSIVE HISTORY OF RECIPIENT COUPLE (HUSBAND)
") Personal History Name Date of Birth Home Address Home Phone Work Phone Type of Employment Social Security # Medical Insurance Marital Status Religion Highest education degree (high school, college, graduate
Personal History Name Date of Birth Home Address Home Phone Work Phone Type of Employment Social Security # Medical Insurance Marital Status Religion Highest education degree (high school, college, graduate
Screening Training Manual. Section 4: The Auditory System
 Screening Training Manual Section 4: The Auditory System 4.1 Anatomy and Physiology of the Ear 4.2 Types, Degrees and Implications of Hearing Loss 4.3 Risk Factors for Late onset Hearing Loss Page 1 of
Screening Training Manual Section 4: The Auditory System 4.1 Anatomy and Physiology of the Ear 4.2 Types, Degrees and Implications of Hearing Loss 4.3 Risk Factors for Late onset Hearing Loss Page 1 of
Quick Reference Guide
 This index may help determine a clinical diagnosis. Fairly common dysmorphic features are listed with corresponding syndromes in which the characteristic is a frequent finding. The syndrome features are
This index may help determine a clinical diagnosis. Fairly common dysmorphic features are listed with corresponding syndromes in which the characteristic is a frequent finding. The syndrome features are
Original signed by: Colleagues:
 Dr. Michael Routledge, Chief Provincial Public Health Officer, MHSAL Dr. Darren Leitao, Clinical Director, Pediatric Cochlear Implant Program; Section Head, Pediatric Otolaryngology, W Diana Dinon, Clinical
Dr. Michael Routledge, Chief Provincial Public Health Officer, MHSAL Dr. Darren Leitao, Clinical Director, Pediatric Cochlear Implant Program; Section Head, Pediatric Otolaryngology, W Diana Dinon, Clinical
Rory Attwood MBChB,FRCS
 Hearing loss Overview Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Not deafness Deaf is a total lack of hearing Deafness
Hearing loss Overview Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Not deafness Deaf is a total lack of hearing Deafness
History Form for Adult Client
 History Form for Adult Client Referral Date: Who referred you to our office (please circle one)? Self Other, please specify: Reason for Referral: Require a Diagnostic Evaluation for Autism Spectrum Disorder
History Form for Adult Client Referral Date: Who referred you to our office (please circle one)? Self Other, please specify: Reason for Referral: Require a Diagnostic Evaluation for Autism Spectrum Disorder
3. If the presence of middle ear pathology is suspected based on immittance test results, case history, or otoscopic exam, perform Wave V threshold se
 GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags
 A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags 1 The Ear Video of how the ear works (http://www.entnet.org/content/how-ear-works)
A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags 1 The Ear Video of how the ear works (http://www.entnet.org/content/how-ear-works)
Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations
 Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations Dr Karen Liddle - 20th May 2017 9th Australasian Newborn Screening Conference Childhood Hearing Clinic Multidisciplinary
Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations Dr Karen Liddle - 20th May 2017 9th Australasian Newborn Screening Conference Childhood Hearing Clinic Multidisciplinary
COCHLEAR IMPLANT SERVICE PATIENT QUESTIONNAIRE. Address: Gender: Male Female. Has your child been a patient at B.C. Children s Hospital?
 - 1 - COCHLEAR IMPLANT SERVICE PATIENT QUESTIONNAIRE Patient s Name: Date of birth: / / d m y B.C. Children s Unit #: Provincial Health #: Address: Gender: Male Female Date Questionnaire completed: Primary
- 1 - COCHLEAR IMPLANT SERVICE PATIENT QUESTIONNAIRE Patient s Name: Date of birth: / / d m y B.C. Children s Unit #: Provincial Health #: Address: Gender: Male Female Date Questionnaire completed: Primary
City: Person Completing this Form (if not patient): Relation to patient: Reason for Appointment:
: Relation to patient: Reason for Appointment:") Ball State University Speech and Audiology Clinic Family Medical History Form : Date: Birthdate: Sex: Address: City: State: ZIP: Home Phone: ( ) Other Phone: ( ) Email: Primary Care Physician: Maternal
Ball State University Speech and Audiology Clinic Family Medical History Form : Date: Birthdate: Sex: Address: City: State: ZIP: Home Phone: ( ) Other Phone: ( ) Email: Primary Care Physician: Maternal
6 AAMD Classifications
 6 AAMD Classifications This section contains the American Association on Mental Deficiency (1977 AAMD version) codes and decode values used in CARE. The codes are listed in numerical order. CARE System
6 AAMD Classifications This section contains the American Association on Mental Deficiency (1977 AAMD version) codes and decode values used in CARE. The codes are listed in numerical order. CARE System
Guidelines for Primary Care and Medical Home Providers
 EARLY HEARING DETECTION AND INTERVENTION Guidelines for Primary Care and Medical Home Providers Original Publication: April 2009 Last Revision Approved: February 2017 INTRODUCTION This document is intended
EARLY HEARING DETECTION AND INTERVENTION Guidelines for Primary Care and Medical Home Providers Original Publication: April 2009 Last Revision Approved: February 2017 INTRODUCTION This document is intended
Has your child ever received a speech and language evaluation? if so, when? Has he/she attended therapy?
 Today s Date: Cleft Palate and Craniofacial Speech Disorders - Intake Form Welcome to Momentum Therapy Center. The information you provide on this form will help us prepare your child s upcoming speech-language
Today s Date: Cleft Palate and Craniofacial Speech Disorders - Intake Form Welcome to Momentum Therapy Center. The information you provide on this form will help us prepare your child s upcoming speech-language
NEW PATIENT INFORMATION *All information provided is kept in strict confidence
 NEW PATIENT INFORMATION *All information provided is kept in strict confidence Name: Date: Address: Telephone: (home) (cell) (work) E-mail: Emergency contact: (name) (relationship) telephone: (home) (cell)
NEW PATIENT INFORMATION *All information provided is kept in strict confidence Name: Date: Address: Telephone: (home) (cell) (work) E-mail: Emergency contact: (name) (relationship) telephone: (home) (cell)
Date of Birth: Age: Sex: male female. Weight: Height: Address: Parents: Mother s Phone: (home) (cell) (work) Mother s
 (cell) (work) Mother s") *All information provided is kept in strict confidence Child s Name: Date: Date of Birth: Age: Sex: male female Weight: Height: Girls: Age at first period: Address: Parents: Mother s Phone: (home) (cell)
*All information provided is kept in strict confidence Child s Name: Date: Date of Birth: Age: Sex: male female Weight: Height: Girls: Age at first period: Address: Parents: Mother s Phone: (home) (cell)
Babies First and CaCoon Risk Factors (A Codes and B Codes)
") Babies First and Risk Factors (A Codes and B Codes) (Birth through 4 years of age) Medical Risk Factors A1. Drug exposed infant (See A29) A2. Infant HIV positive A3. Maternal PKU or HIV positive A4. Intracranial
Babies First and Risk Factors (A Codes and B Codes) (Birth through 4 years of age) Medical Risk Factors A1. Drug exposed infant (See A29) A2. Infant HIV positive A3. Maternal PKU or HIV positive A4. Intracranial
Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners
 Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners The Portable OAE Hearing Screener of Choice... Ear canal Middle ear Eardrum The AuDX device
Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners The Portable OAE Hearing Screener of Choice... Ear canal Middle ear Eardrum The AuDX device
The hearing-impaired child. D J H Wagenfeld. (CME, Nov/Dec 2003, Vol 21, No 11.)
") The hearing-impaired child D J H Wagenfeld (CME, Nov/Dec 2003, Vol 21, No 11.) It has become universally accepted that early identification and intervention in children with hearing loss is the key to
The hearing-impaired child D J H Wagenfeld (CME, Nov/Dec 2003, Vol 21, No 11.) It has become universally accepted that early identification and intervention in children with hearing loss is the key to
Unifactorial or Single Gene Disorders. Hanan Hamamy Department of Genetic Medicine and Development Geneva University Hospital
 Unifactorial or Single Gene Disorders Hanan Hamamy Department of Genetic Medicine and Development Geneva University Hospital Training Course in Sexual and Reproductive Health Research Geneva 2011 Single
Unifactorial or Single Gene Disorders Hanan Hamamy Department of Genetic Medicine and Development Geneva University Hospital Training Course in Sexual and Reproductive Health Research Geneva 2011 Single
Medical Conditions Resulting in High Probability of Developmental Delay and DSCC Screening Information
 Jame5. L.Jma5, ~reuiry Medical Conditions Medical Conditions Resulting in High Probability of Developmental Delay and DSCC Screening Information I Not Listed later Children with medical conditions which
Jame5. L.Jma5, ~reuiry Medical Conditions Medical Conditions Resulting in High Probability of Developmental Delay and DSCC Screening Information I Not Listed later Children with medical conditions which
Georgia Department of Human Services BIRTH FAMILY BACKGROUND INFORMATION FOR CHILD. Name of Child Date of Birth Sex Race Hispanic Ethnicity Yes No
 Georgia Department of Human Services BIRTH FAMILY BACKGROUND INFORMATION FOR CHILD Name of Child Date of Birth Sex Race Hispanic Ethnicity Yes No Legal County (DHS Child) Resident County (Non-DHS Child)
Georgia Department of Human Services BIRTH FAMILY BACKGROUND INFORMATION FOR CHILD Name of Child Date of Birth Sex Race Hispanic Ethnicity Yes No Legal County (DHS Child) Resident County (Non-DHS Child)
Child Intake Form (To be completed by the parent or guardian and returned to the clinic) Phone: Select.
 Phone: Select.") NORTHEASTERN UNIVERSITY Speech, Language, and Hearing Center 30 Leon Street 503 Behrakis Health Science Center Boston, MA 02115 Ph: (617) 373-2492 Fx: (617) 373-8756 1 TODAY S DATE: Child Intake Form (To
NORTHEASTERN UNIVERSITY Speech, Language, and Hearing Center 30 Leon Street 503 Behrakis Health Science Center Boston, MA 02115 Ph: (617) 373-2492 Fx: (617) 373-8756 1 TODAY S DATE: Child Intake Form (To
Dizziness/Balance Questionnaire
 Dizziness/Balance Questionnaire Name: Date: 1. Which of these best describes your dizziness? Please mark only one. A sensation of movement of yourself or the room (spinning, tilting, or wave-like movement)
Dizziness/Balance Questionnaire Name: Date: 1. Which of these best describes your dizziness? Please mark only one. A sensation of movement of yourself or the room (spinning, tilting, or wave-like movement)
PEDIATRIC MEDICAL HISTORY QUESTIONNAIRE
 Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,
Division of Otolaryngology Main Phone: 847 504-3300 Main Fax: 847 504-3305 Mihir Bhayani, MD Judy L. Chen, MD Mark E. Gerber, MD, FACS, FAAP Joseph Raviv, MD Ilana Seligman, MD, FACS, FAAP Michael J. Shinners,
Pediatric Case History Form
 Pediatric Case History Form Patient s full name: Date of completion: Date of birth: Gender (circle one): Male Female Mother s full name: Father s full name: Legal guardian s full name(s): Person completing
Pediatric Case History Form Patient s full name: Date of completion: Date of birth: Gender (circle one): Male Female Mother s full name: Father s full name: Legal guardian s full name(s): Person completing
Executive Summary. JCIH Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs
 Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT
 NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT -Department of ENT and Audiology HOSPITAL MANKHOOL ASTERHOSPITAL.COM 04-4400500 RELIABLE EASY FAST SAFE (WHO) states that 0.5-5 newborns in every 1000 births
NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT -Department of ENT and Audiology HOSPITAL MANKHOOL ASTERHOSPITAL.COM 04-4400500 RELIABLE EASY FAST SAFE (WHO) states that 0.5-5 newborns in every 1000 births
Child s Information (Please print) Name Birth Date Age Home Address City State Zip Code
 Name Birth Date Age Home Address City State Zip Code") The following questions are asked so that we can best understand your child. Please fill out this questionnaire before the child is evaluated. Please read the questions carefully and answer them as fully
The following questions are asked so that we can best understand your child. Please fill out this questionnaire before the child is evaluated. Please read the questions carefully and answer them as fully
Early Hearing Detection and Intervention How You Matter! Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD
 Early Hearing Detection and Intervention How You Matter! Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD Jessica J Messersmith, PhD, CCC-A, FAAA Associate Professor of Audiology,
Early Hearing Detection and Intervention How You Matter! Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD Jessica J Messersmith, PhD, CCC-A, FAAA Associate Professor of Audiology,
Effective factors on Auditory Brainstem Response test in Newborns
 BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
Recommendations for monitoring hearing in children using a risk factor registry
 Recommendations for monitoring hearing in children using a risk factor registry Rachael Beswick Carlie Driscoll Joseph Kei Shirley Glennon 7th Australasian Newborn Hearing Screening Conference 2012 Background
Recommendations for monitoring hearing in children using a risk factor registry Rachael Beswick Carlie Driscoll Joseph Kei Shirley Glennon 7th Australasian Newborn Hearing Screening Conference 2012 Background
Risk Factors for Late-Onset Hearing Loss in Children
 Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
Congenital permanent hearing loss occurs in about 3
 Online Exclusive Problem with baby s hearing? An intervention checklist It s time to make sure infants with positive screens for hearing loss get the follow-up treatment they need and deserve. This tool
Online Exclusive Problem with baby s hearing? An intervention checklist It s time to make sure infants with positive screens for hearing loss get the follow-up treatment they need and deserve. This tool
Asking questions Misunderstood questions or inappropriate responses Presence of a aid Sign language or
 1 Chapter 45 The Challenged Patient 2 Hearing Impairments 3 Types of Hearing Impairments Deafness: a blockage of the transmission of sound waves through the external ear canal to the middle or inner ear.
1 Chapter 45 The Challenged Patient 2 Hearing Impairments 3 Types of Hearing Impairments Deafness: a blockage of the transmission of sound waves through the external ear canal to the middle or inner ear.
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print
 - AUDIOLOGY Please Print") JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
JACKSONVILLE SPEECH & HEARING CENTER PATIENT INFORMATION FORM PEDIATRIC (CHILD) - AUDIOLOGY Please Print Referring Physician: Child s (Patient) Name: LAST FIRST MIDDLE Gender: Male Female Date of Birth:
AAC Child Case History Form
 Client Name: Date-of-Birth: School: Native Language: Mother s Name: Address: Phone: AAC Child Case History Form Date: Age: Grade: Primary Language: Father s Name: Address (if different): Phone: Home Work
Client Name: Date-of-Birth: School: Native Language: Mother s Name: Address: Phone: AAC Child Case History Form Date: Age: Grade: Primary Language: Father s Name: Address (if different): Phone: Home Work
AAC Child Case History Form
 AAC Child Case History Form Name Date Date-of-Birth School Age Grade Native Language Primary Language Mother s Name Alernate Email Home Work Cell (CIRCLE ONE) Home Work Cell (CIRCLE ONE) Father s Name
AAC Child Case History Form Name Date Date-of-Birth School Age Grade Native Language Primary Language Mother s Name Alernate Email Home Work Cell (CIRCLE ONE) Home Work Cell (CIRCLE ONE) Father s Name
Craniofacial Microsomia
 Patient and Family Education Craniofacial Microsomia Children with craniofacial microsomia (CFM) have a small or underdeveloped part of the face, usually the ear and jaw. The eye, cheek and neck may also
Patient and Family Education Craniofacial Microsomia Children with craniofacial microsomia (CFM) have a small or underdeveloped part of the face, usually the ear and jaw. The eye, cheek and neck may also
QUESTION. Personal Behavior History. Donor Genetic History. Donor Medical History. Family Medical History PERSONAL BEHAVIOR HISTORY. Never N/A.
 Donor 4576 Medical Profile S Personal Behavior History Donor Genetic History Donor Medical History Family Medical History PERSONAL BEHAVIOR HISTORY Current alcohol use: If yes, oz./week and type of alcohol:
Donor 4576 Medical Profile S Personal Behavior History Donor Genetic History Donor Medical History Family Medical History PERSONAL BEHAVIOR HISTORY Current alcohol use: If yes, oz./week and type of alcohol:
NEW PATIENT FORM. Please print in ink and fill in all blanks Please fill out front and back. Patient s Full Name
 NEW PATIENT FORM Please print in ink and fill in all blanks Please fill out front and back Patient s Full Name Date of Birth Age Sex Social Security Number Referring Doctor or Family Physician Phone #
NEW PATIENT FORM Please print in ink and fill in all blanks Please fill out front and back Patient s Full Name Date of Birth Age Sex Social Security Number Referring Doctor or Family Physician Phone #
K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 9: Congenital Deafness. General Information
 Chapter 9: Congenital Deafness. General Information") K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 9: Congenital Deafness General Information 1. One person in eight carries a recessive gene for deafness; 1:4000 live births
K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 9: Congenital Deafness General Information 1. One person in eight carries a recessive gene for deafness; 1:4000 live births
COCHLEAR IMPLANT PROGRAM PATIENT QUESTIONNAIRE
 COCHLEAR IMPLANT PROGRAM PATIENT QUESTIONNAIRE Patient s Name Address... Postal code.. Date of birth /.../.../.../ Sex.. OHIP #..... d m y Version Hospital for Sick Children number (if available) HSC#.
COCHLEAR IMPLANT PROGRAM PATIENT QUESTIONNAIRE Patient s Name Address... Postal code.. Date of birth /.../.../.../ Sex.. OHIP #..... d m y Version Hospital for Sick Children number (if available) HSC#.
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS
 HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE
Disclosures. Objectives 2/29/2016. Bradley Golner M.D. FAAP. AzEHDI chapter champion AAP EHDI leadership team
 Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
UNIVERSITY OF WASHINGTON
 UNIVERSITY OF WASHINGTON THE FETAL ALCOHOL SYNDROME DIAGNOSTIC AND PREVENTION NETWORK (FAS DPN) Center for Human Development and Disability Dear Sir or Madam, Thank you very much for your request for an
UNIVERSITY OF WASHINGTON THE FETAL ALCOHOL SYNDROME DIAGNOSTIC AND PREVENTION NETWORK (FAS DPN) Center for Human Development and Disability Dear Sir or Madam, Thank you very much for your request for an
NYEIS Version 4.3 (ICD) ICD - 10 Codes Available in NYEIS at time of version launch (9/23/2015)
 ICD - 10 Codes Available in NYEIS at time of version launch (9/23/2015)") D82.1 Di George's syndrome E63.9 Nutritional deficiency, unspecified E70.21 Tyrosinemia E70.29 Other disorders of tyrosine metabolism E70.30 Albinism, unspecified E70.5 Disorders of tryptophan metabolism
D82.1 Di George's syndrome E63.9 Nutritional deficiency, unspecified E70.21 Tyrosinemia E70.29 Other disorders of tyrosine metabolism E70.30 Albinism, unspecified E70.5 Disorders of tryptophan metabolism
Genetics Questions: There are 15 questions in total. The answers can be found on the accompanying document
 Page 1 Genetics Questions: These questions are aimed at medical and allied health professionals and they are designed to show where genetics has a role in clinical practice. There are 15 questions in total
Page 1 Genetics Questions: These questions are aimed at medical and allied health professionals and they are designed to show where genetics has a role in clinical practice. There are 15 questions in total
Newborn hearing screening - well baby protocol Paediatrics > Screening > Newborn hearing screening
 Map of Medicine National Library for Health Newborn hearing screening well baby protocol Automated oto-acoustic emission (AOAE) screening test Missed or incomplete AOAE screening test AOAE no clear response
Map of Medicine National Library for Health Newborn hearing screening well baby protocol Automated oto-acoustic emission (AOAE) screening test Missed or incomplete AOAE screening test AOAE no clear response
Newborn hearing screening - NICU or SCBU protocol Paediatrics > Screening > Newborn hearing screening
 Map of Medicine National Library for Health Newborn hearing screening NICU/SCBU protocol Automated oto-acoustic emission (AOAE) screening test Automated auditory brainstem response (AABR) screening test
Map of Medicine National Library for Health Newborn hearing screening NICU/SCBU protocol Automated oto-acoustic emission (AOAE) screening test Automated auditory brainstem response (AABR) screening test
REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY GROUP
 REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY GROUP NEW PATIENT EVALUATION FORM Name: Age: Partner: Age: Reason for Referral: Date of Appt: Have you ever seen any other physician(s) for this problem? Name:
REPRODUCTIVE ENDOCRINOLOGY AND INFERTILITY GROUP NEW PATIENT EVALUATION FORM Name: Age: Partner: Age: Reason for Referral: Date of Appt: Have you ever seen any other physician(s) for this problem? Name:
Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease.
 Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease. Listen Observe Evaluate Test Refer Guide for primary care providers includes: Surveillance Aid: Assessing Weakness
Learn the steps to identify pediatric muscle weakness and signs of neuromuscular disease. Listen Observe Evaluate Test Refer Guide for primary care providers includes: Surveillance Aid: Assessing Weakness
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS
 HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE.
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE.
PATIENT INFORMATION FORM (WOMEN ONLY)
") PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
PATIENT INFORMATION FORM (WOMEN ONLY) Name: Age: Sex: Birthdate: / / SS # A. Describe briefly your present symptom(s) or the reason(s) for seeing the doctor today: B. Name all illnesses or conditions for
Preconception/prenatal family history questionnaire
 1 of 5 Today s date: Person completing questionnaire: Patient Partner/spouse Name Date of birth Occupation Marital status (married, divorced, widowed, single) Last grade completed Height Weight Adopted
1 of 5 Today s date: Person completing questionnaire: Patient Partner/spouse Name Date of birth Occupation Marital status (married, divorced, widowed, single) Last grade completed Height Weight Adopted
Physical Characteristics
 Donor ID# (to be assigned by staff) Please answer the following questions with as much detail and thoroughness as possible. Please mail the finished questionnaire back to the clinic. Please call us if
Donor ID# (to be assigned by staff) Please answer the following questions with as much detail and thoroughness as possible. Please mail the finished questionnaire back to the clinic. Please call us if
REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY. Better Hearing Philippines Inc.
 REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY Better Hearing Philippines Inc. How To Get Started? 1. Testing must be done in an acoustically treated environment far from all the environmental noises
REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY Better Hearing Philippines Inc. How To Get Started? 1. Testing must be done in an acoustically treated environment far from all the environmental noises
Section F: Discussing the diagnosis and developing a management plan
 Section E: Formulating a diagnosis Information collected during the diagnostic assessment should be reviewed, ideally in a multi-disciplinary team context, to evaluate the strength of evidence to: Support
Section E: Formulating a diagnosis Information collected during the diagnostic assessment should be reviewed, ideally in a multi-disciplinary team context, to evaluate the strength of evidence to: Support
(OAEs) for. Steven D. Smith, Au.D.
 for. Steven D. Smith, Au.D.") A Guide to Otoacoustic Emissions (OAEs) for School Nurses Steven D. Smith, Au.D. Director of Audiology, Director of Physicians Hearing & Balance Center Drs. Kitchens, Chapman, & Anderson, PA, Montgomery,
A Guide to Otoacoustic Emissions (OAEs) for School Nurses Steven D. Smith, Au.D. Director of Audiology, Director of Physicians Hearing & Balance Center Drs. Kitchens, Chapman, & Anderson, PA, Montgomery,
INTAKE INFORMATION BASIC INFORMATION. Gender: (circle) Male Female Race: (circle) White Black Other. Special Education Placement/Services (if any):
 Male Female Race: (circle) White Black Other. Special Education Placement/Services (if any):") INTAKE INFORMATION BASIC INFORMATION Child s Name: Today s Date: Gender: (circle) Male Female Race: (circle) White Black Other Birth Date: Parent/Guardian: Home Address: City: State: ZIP School/Daycare:
INTAKE INFORMATION BASIC INFORMATION Child s Name: Today s Date: Gender: (circle) Male Female Race: (circle) White Black Other Birth Date: Parent/Guardian: Home Address: City: State: ZIP School/Daycare:
Feil & Oppenheimer Psychological Services
 Feil & Oppenheimer Psychological Services 260 Waseca Ave. Barrington, RI 02806 401-245-4040 Fax: 401-245-1240 feiloppenheimer@gmail.com Adult Patient Questionnaire Name: Today's Date: Address: Home Phone:
Feil & Oppenheimer Psychological Services 260 Waseca Ave. Barrington, RI 02806 401-245-4040 Fax: 401-245-1240 feiloppenheimer@gmail.com Adult Patient Questionnaire Name: Today's Date: Address: Home Phone:
Tell Us About Your Child. Who is Accompanying Your Child Today? Parent Information. Primary Dental Insurance
 1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
1 Today s Date: 2 (225) 664-2646 (225) 664-2640 (fax) 245 VETERANS BLVD. DENHAM SPRINGS, LA 70726 Who is Accompanying Your Child Today? Name: Relation: Do you have legal custody of this child? Yes No Tell
Birth mother Foster carer Other
 PATIENT DETAILS NAME Sex Female Male Other Date of birth (DD/MM/YYYY) / / Age at assessment: Racial/ ethnic background Preferred language Hospital number (if applicable) Referral source, date, provider
PATIENT DETAILS NAME Sex Female Male Other Date of birth (DD/MM/YYYY) / / Age at assessment: Racial/ ethnic background Preferred language Hospital number (if applicable) Referral source, date, provider
Evergreen Speech & Hearing Clinic, Inc. Transforming Lives Through Improved Communication Since 1979
 Audiology Hearing Testing VRA VNG/VEMP OAE BAER/ECochG Hearing Aids Cochlear/Bone Implants Tinnitus CAPD EHDDI Speech-Language Pathology Language Voice Accent Modification Autism Evaluation & Treatment
Audiology Hearing Testing VRA VNG/VEMP OAE BAER/ECochG Hearing Aids Cochlear/Bone Implants Tinnitus CAPD EHDDI Speech-Language Pathology Language Voice Accent Modification Autism Evaluation & Treatment
Medical Professionals Guide. children with deafblindness. for the identification of. Systems Development & Improvement Center
 Medical Professionals Guide for the identification of children with deafblindness Systems Development & Improvement Center Medical Professionals Guide for the Identification of Children with Deafblindness*
Medical Professionals Guide for the identification of children with deafblindness Systems Development & Improvement Center Medical Professionals Guide for the Identification of Children with Deafblindness*
Treatments that require prior authorization by NHS
 Treatments that require prior authorization by NHS If you want to apply for the cost reimbursement covering your treatment in Poland please check if you need to apply before your medical travel. Please
Treatments that require prior authorization by NHS If you want to apply for the cost reimbursement covering your treatment in Poland please check if you need to apply before your medical travel. Please
Date: Patient Name: DOB: Name of Person Completing Form: Relationship to Patient: Primary Care Physician: Referring Physician: Preferred Pharmacy:
 Date: Patient Name: DOB: Name of Person Completing Form: Relationship to Patient: Primary Care Physician: Referring Physician: Preferred Pharmacy: Reason For Today s Visit Please list the reason for your
Date: Patient Name: DOB: Name of Person Completing Form: Relationship to Patient: Primary Care Physician: Referring Physician: Preferred Pharmacy: Reason For Today s Visit Please list the reason for your
DENTISTRY IN PROFOUND CHILDHOOD DEAFNESS
 DENTISTRY IN PROFOUND CHILDHOOD DEAFNESS IN SOUTH AFRICA LAWRENCE STEPHEN 1, SEAN SELLARS 2, PETER BEIGHTON 3 Abstract The dental care of children with profound childhood deafness is influenced by difficulties
DENTISTRY IN PROFOUND CHILDHOOD DEAFNESS IN SOUTH AFRICA LAWRENCE STEPHEN 1, SEAN SELLARS 2, PETER BEIGHTON 3 Abstract The dental care of children with profound childhood deafness is influenced by difficulties
Referral Packet. COLLEGE OF EDUCATION Revised December Table of Contents
 2015 Referral Packet Table of Contents Who are the children with dual sensory impairments? 1 What is the Nevada Dual Sensory Impairment Project?. 1 Who can refer children to the project?... 1 What is next?.
2015 Referral Packet Table of Contents Who are the children with dual sensory impairments? 1 What is the Nevada Dual Sensory Impairment Project?. 1 Who can refer children to the project?... 1 What is next?.
PEDIATRIC PRE-EXAM INFORMATION
 PEDIATRIC PRE-EXAM INFORMATION Name: Date of Birth dd /mm /YY Sex: M F Age Address Postal Code Mother s Name Home Phone: Occupation : Work Phone: Father s name Home Phone: Occupation: Work Phone: Siblings
PEDIATRIC PRE-EXAM INFORMATION Name: Date of Birth dd /mm /YY Sex: M F Age Address Postal Code Mother s Name Home Phone: Occupation : Work Phone: Father s name Home Phone: Occupation: Work Phone: Siblings
Why Pediatric Hearing Clinic
 Why Pediatric Hearing Clinic RICHARD KANG, M.D., ASHLEY KAUFMAN, AU.D. AND MALLORY AUCH, RN Our Staff: Mallory Auch, RN Nurse Coordinator Kristen Janky, PhD, AuD, CCC-A Vestibular Audiologist Richard Kang,
Why Pediatric Hearing Clinic RICHARD KANG, M.D., ASHLEY KAUFMAN, AU.D. AND MALLORY AUCH, RN Our Staff: Mallory Auch, RN Nurse Coordinator Kristen Janky, PhD, AuD, CCC-A Vestibular Audiologist Richard Kang,
What else would you like to see changed in his/her health?
 Simmonds McMurrer Naturopathic Medicine Dr.Kali Simmonds,N.D. Dr.Lana McMurrer,N.D. Dr.Nara Simmonds,N.D. 34 Queen Street, 2nd Floor Charlottetown, PE C1A 4A3 Tel.902.894.3868 Fax.902.894.4054 www.simmondsmcmurre.com
Simmonds McMurrer Naturopathic Medicine Dr.Kali Simmonds,N.D. Dr.Lana McMurrer,N.D. Dr.Nara Simmonds,N.D. 34 Queen Street, 2nd Floor Charlottetown, PE C1A 4A3 Tel.902.894.3868 Fax.902.894.4054 www.simmondsmcmurre.com
School Nurses Guide to Otoacoustic Emissions (OAEs)
") School Nurses Guide to Otoacoustic Emissions (OAEs) www.maico-diagnostics.com Rationale for hearing screening with OAEs Hearing loss is not uncommon in children. Approximately 6 out of every thousand children
School Nurses Guide to Otoacoustic Emissions (OAEs) www.maico-diagnostics.com Rationale for hearing screening with OAEs Hearing loss is not uncommon in children. Approximately 6 out of every thousand children
AFL NSW/ACT Exemption & Dispensation Policy
 AFL NSW/ACT Exemption & Dispensation Policy Last reviewed 14 May 2012. AFL NSW/ACT s policy is that age exceptions and/or dispensations will only exist in cases of disability These exemptions require approval
AFL NSW/ACT Exemption & Dispensation Policy Last reviewed 14 May 2012. AFL NSW/ACT s policy is that age exceptions and/or dispensations will only exist in cases of disability These exemptions require approval
The First Meeting of the Joint Committee
 The First Meeting of the Joint Committee First Report of the Joint Committee---1970 The Committee found that the reported results of mass behavioral screening programs are inconsistent and misleading,
The First Meeting of the Joint Committee First Report of the Joint Committee---1970 The Committee found that the reported results of mass behavioral screening programs are inconsistent and misleading,
Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module. Inside this issue:
 Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS
 HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE.
HEALTH EXAMINATION GUIDELINES FOR ENTRY INTO MALAYSIAN HIGHER EDUCATIONAL INSTITUTIONS 1. PLEASE READ THE INSTRUCTIONS CAREFULLY BEFORE FILLING IN THE FORM. 2. PLEASE FILL IN THE FORM IN ENGLISH LANGUAGE.
Hereditary Cancer Risk Testing: What to Expect
 Hereditary Cancer Risk Testing: What to Expect PHONE APPOINTMENT The first appointment with the Vanderbilt Hereditary Cancer Clinic is by phone. We will record your family history information and create
Hereditary Cancer Risk Testing: What to Expect PHONE APPOINTMENT The first appointment with the Vanderbilt Hereditary Cancer Clinic is by phone. We will record your family history information and create
3/20/2017. D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital
 D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
History Form for Parent/Guardian of Children and Adolescents (through age 17) Center: Case #: First Name: Preferred Name: Middle Name:
 Center: Case #: First Name: Preferred Name: Middle Name:") 1 of 11 (through age 17) To be completed by TEACCH Center Center: Case #: UNC Hospital Unit# (if available): Referral Date: Who referred you to TEACCH? Self Other, please specify: Reason for Referral:
1 of 11 (through age 17) To be completed by TEACCH Center Center: Case #: UNC Hospital Unit# (if available): Referral Date: Who referred you to TEACCH? Self Other, please specify: Reason for Referral:
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018
 The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
INTAKE CASE HISTORY FORM
 INTAKE CASE HISTORY FORM I. Identifying Information Today s Date: Student s Name: Last First Middle Date of Birth: / / Gender: Male / Female Has there been a change in address, since the student s application
INTAKE CASE HISTORY FORM I. Identifying Information Today s Date: Student s Name: Last First Middle Date of Birth: / / Gender: Male / Female Has there been a change in address, since the student s application
BEHAVIOR & ADHD SCREENING INTAKE FORM
 3171 N.E. Carnegie Drive, Suite A Lee s Summit, MO 64064 P: (816) 525-2800 F: (816) 525-4077 www.summitdoctors.com BEHAVIOR & ADHD SCREENING INTAKE FORM PATIENT NAME: TODAYS DATE / / LAST FIRST MI DATE
3171 N.E. Carnegie Drive, Suite A Lee s Summit, MO 64064 P: (816) 525-2800 F: (816) 525-4077 www.summitdoctors.com BEHAVIOR & ADHD SCREENING INTAKE FORM PATIENT NAME: TODAYS DATE / / LAST FIRST MI DATE
Gishela Satarino, MA, LPC-S 6750 Hillcrest Plaza Drive, #203 Dallas, TX History Form for Counseling Services
 Gishela Satarino, MA, LPC-S 6750 Hillcrest Plaza Drive, #203 Dallas, TX 75230 214-280-3664 History Form for Counseling Services Client s Name: Age: Today s Date: / / Client s Sex: Client s Birthplace:
Gishela Satarino, MA, LPC-S 6750 Hillcrest Plaza Drive, #203 Dallas, TX 75230 214-280-3664 History Form for Counseling Services Client s Name: Age: Today s Date: / / Client s Sex: Client s Birthplace:
DR. CESTNICK ADULT BACKGROUND QUESTIONNAIRE. Birth date: Age: Sex (circle one): Male Female. Home address: City: Zip Code:
: Male Female. Home address: City: Zip Code:") DR. CESTNICK ADULT BACKGROUND QUESTIONNAIRE Your name: Today s date: Birth date: Age: Sex (circle one): Male Female Home address: City: Zip Code: Phone: Home # Cell # Other # Email: School (if student):
DR. CESTNICK ADULT BACKGROUND QUESTIONNAIRE Your name: Today s date: Birth date: Age: Sex (circle one): Male Female Home address: City: Zip Code: Phone: Home # Cell # Other # Email: School (if student):
Children s hearing. A guide for parents
 Children s hearing A guide for parents Creating the future Children are our future. By giving them access to a world full of sounds, we can help them to develop the hearing skills they need to build their
Children s hearing A guide for parents Creating the future Children are our future. By giving them access to a world full of sounds, we can help them to develop the hearing skills they need to build their
Department of Psychiatry\Behavioral Health 200 Mercy Drive, Suite 201 Dubuque, IA or
 Department of Psychiatry\Behavioral Health 200 Mercy Drive, Suite 201 Dubuque, IA 52001 563 584 3500 or 800 648 6868 C H I L D H I S T O R Y F O R M Today s Date: Child s Name: Date of Birth: Age: Grade:
Department of Psychiatry\Behavioral Health 200 Mercy Drive, Suite 201 Dubuque, IA 52001 563 584 3500 or 800 648 6868 C H I L D H I S T O R Y F O R M Today s Date: Child s Name: Date of Birth: Age: Grade:
HEALTH VISITOR INFORMATION PACK
 HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods
HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods
Beauregard Memorial Hospital Rehabilitation Services Pediatric Speech Pathology Intake Form. Today's Date: M/D/Yr (e.g.
 Today's Date: M/D/Yr (e.g., 03/28/2012) Patient's Name: Date of Birth: M/D/Yr (e.g., 03/28/2012) Age: Gender: Male Female Address: Apt. CITY: STATE: ZIP CODE: Home Phone: Cell Phone: Business Phone: Other
Today's Date: M/D/Yr (e.g., 03/28/2012) Patient's Name: Date of Birth: M/D/Yr (e.g., 03/28/2012) Age: Gender: Male Female Address: Apt. CITY: STATE: ZIP CODE: Home Phone: Cell Phone: Business Phone: Other
Single Gene (Monogenic) Disorders. Mendelian Inheritance: Definitions. Mendelian Inheritance: Definitions
 Disorders. Mendelian Inheritance: Definitions. Mendelian Inheritance: Definitions") Single Gene (Monogenic) Disorders Mendelian Inheritance: Definitions A genetic locus is a specific position or location on a chromosome. Frequently, locus is used to refer to a specific gene. Alleles are
Single Gene (Monogenic) Disorders Mendelian Inheritance: Definitions A genetic locus is a specific position or location on a chromosome. Frequently, locus is used to refer to a specific gene. Alleles are