Kerry Callahan Mandulak, PhD, CCC-SLP Department of Speech and Hearing Sciences Portland State University, Portland, OR
|
|
|
- Clare Farmer
- 5 years ago
- Views:
Transcription
1 Kerry Callahan Mandulak, PhD, CCC-SLP Department of Speech and Hearing Sciences Portland State University, Portland, OR Adriane Baylis, PhD, CCC-SLP Nationwide Children s Hospital, Columbus, OH Anna Thurmes, PhD, CCC-SLP University of Minnesota, Minneapolis, MN Special Interest Group 5 Short Course November 19, 2011
2

3 Orofacial Clefting (cleft lip and palate) are the most PREVALENT birth defects in the United States 1 in 600 Caucasian births Higher in American Indian / Asian populations Lower in African American population Affects approximately 6800 babies / year
4 Percentage requiring speech-language treatment 50%-75%, from various sources Percentage requiring treatment for resonance disorder 25%-38%, from various sources Percentage with middle ear disease/conductive hearing loss in infancy 95%-97%, from various sources
5 Multifactorial Inheritance Combination of genetic and environmental factors Specific genetic regions have been investigated Isolated or associated with no recognized syndrome Over 350 recognized cleft syndromes Only 2 4% of total cases Specific cleft syndromes (Pierre) Robin Sequence Apert Syndrome Crouzon Syndrome Treacher Collins Syndrome Hemifacial Microsomia Stickler Syndrome 22q11.2 deletion syndrome (Velocardiofacial Syndrome)

")

6 Number of SLPs who are members of ACPA: 387 (2006) Number of SLPs who are members of ASHA Division 5, Speech Science and Orofacial Disorders: 615 (2007) Number of SLPs who are ASHA members: 122,762 (2006) Percentage of SLPs reporting they feel "not competent" to treat children with cleft lip/palate (Bedwinek et. al, 2010): 44.1%

7 Cleft team SLP / Community SLP Evaluation vs. treatment Scope of practice for SLP = Decreased preparation of SLPs to provide services for children with repaired cleft palate


8 Fewer programs offering courses Less courses offered Small number of training programs Less academics trained to teach courses Less preparation for student clinicians Fewer places for doctoral students
9
 to a complete cleft extending back to the incisive")
 May be")

10 Cleft Lip Only (CL) Varies from a unilateral or bilateral notch of the lip (incomplete cleft) to a complete cleft extending back to the incisive foramen Cleft Palate Only (CPO) varies from a unilateral or bilateral cleft of the hard and/or soft palate Cleft Lip & Palate (CLP) May be unilateral or bilateral Complete bilateral clefts of the lip result in a free-floating premaxilla which is not attached to anything except the columella (Bzoch, 1997)
11 Combination of CLP is more common than CL only or CP only CL +/- CP CP only (isolated CP) Clefts of PRIMARY PALATE Anterior to incisive foramen (lip, alveolar ridge) Clefts of SECONDARY PALATE Posterior to incisive foramen (hard palate, soft palate, uvula) Complete vs. Incomplete

12

13

14

15
16 Bifid Uvula Zona Pellucida (midline tissue of the soft palate has a thin and/or bluish appearance) Bony notch of the posterior hard palate (need to palpate to feel, cannot be seen) Tenting of palate on production of ah May or may not have accompanying hypernasal speech or nasal air emission (Peterson-Falzone et al., 2001)

17

18

19
20 Patients with should be their palates repaired evidence of and if there is or (ACPA, 2000)
21

22

23

24

25

26
27

28

29


30 The VP mechanism does not merely close for oral speech and then fall open for nasal consonants or silence. It closes to different degrees, depending on such variables as vowel height, voicing, and proximity to nasal consonants. Variables: age, gender, phonemic context

31
32

33

34
35
36
37
38

39
40 Children who have craniofacial anomalies are at for speech-language disorders. Evaluation of speech and language development provides information that is needed by the team in, particularly surgical and dental management. Further, information about the patient s speech and language is important in the.
41 Children with an isolated cleft lip are unlikely to develop abnormal speech patterns related to the cleft Approximately 20% of children with repaired cleft palate will develop speech deficits that require additional intervention (Witt & D Antonio, 1993)
42 Communication development begins at birth. Controversy over time of palate surgery In a child with a cleft beginning with an impaired mechanism 9 months vs. 12 months vs. 18 months Speech vs. growth Heterogeneous population? Errors cleft related? Or not?
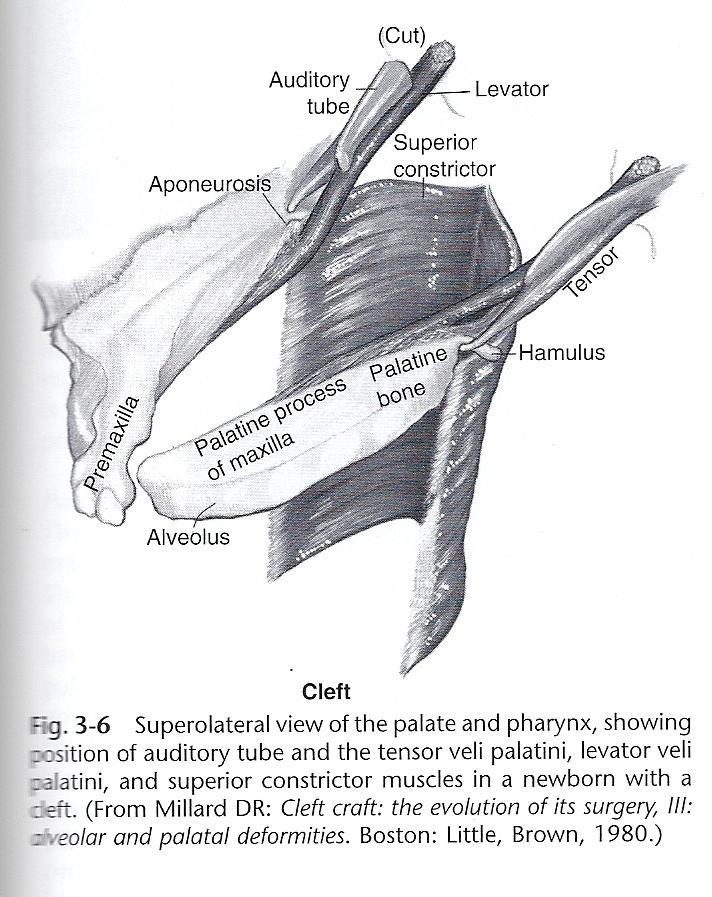
43 Problem Oral and nasal cavities open to each other Lack of place of articulation Fluctuating hearing secondary to chronic otitis media / eustachian tube dysfunction due to faulty insertion of palatal muscles (Hardin- Jones, 2007)


44 Cannot create intra-oral air pressure for sounds like / p b t d k g/ Phonemic repertoire limited to /m/, /n/, ng and vowels Faulty learning for oral air flow sounds Affects manner of articulation
45 Major place of articulation missing 67% of English consonants use alveolar / palatal structures Selective avoidance of consonants that require hard palate contact Research has shown that children with clefts prefer to make sounds in the extremes of the vocal tract (O Gara & Logemann, 1988)




46 VP Dysfunction Palate and pharynx not working together properly for speech production VP Inadequacy VP Insufficiency VP Incompetency Inability of the velum to close off the nasopharynx for the production of oral consonants Structural deficiency: Submucous cleft, short palate/deep pharynx, atrophied adenoids, postadenoidectomy, etc. Neurogenic etiology such as cerebral palsy, TBI, apraxia, etc. (Peterson-Falzone, 2001)
47 Types of resonance disorders Hypernasality Hyponasality Cul-de-sac Resonance Mixed resonance disorder Nasal Air Emission Resonance Disorder Voice Disorder
48 Excessive nasal resonance during speech production Perceptual descriptor (wide range of normal ) Primarily affects vowels and voiced consonants Related to inability to maintain separation of oral and nasal cavities during speech (VPI, fistula, unrepaired cleft) Transpalatal nasalance
49 Reduction in normal nasal resonance Insufficient nasal airflow Primarily affects nasal phonemes (/m/, /n/, ng ) Indicative of obstruction in nasopharynx or nasal cavity
50 Considered disorder Often co-exists w/ hypernasality Can be, not resonance Turbulence / patterns of airflow / size of gap Can be Learned pattern (not due to structural deficit) Normal resonance Treated w/ traditional articulation therapy techniques (Peterson Falzone et al., 2006; Peterson-Falzone & Graham, 1990)
51 Type of hyponasality Caused by an anterior nasal obstruction sound gets trapped in nasopharynx Muffled speech quality
52 Defining resonance is not always clear-cut! The same child can display both hypernasal and hyponasal resonance depending on context Fairly common in cleft population, especially post-pharyngeal flap

53 Hypernasality Hyponasality Mixed Nasality Cul-de-sac Resonance Nasal Air Emission Resonance alteration of vowels and vocalic consonants that occurs when the oral and nasal cavities are abnormally coupled Reduction in nasal resonance that is heard when the nasal airway itself is partially blocked or the entrance to the nasal passages is partially occluded (Peterson Falzone et. al 2001) Elements of both hypo- and hypernasality which cooccur in patients with VPI For example, nasal emission heard on high pressure consonants (s/z), but nasal sounds are hyponasal due to some type of nasal obstruction or septal deviation Muffled characteristic Tight anterior nasal constriction Articulation distortion that affects high pressure consonants (Peterson Falzone et. al 2001)
54 Undiagnosed submucous cleft Palatopharyngeal disproportion (congenitally short palate and/or deep pharynx; ablative surgery to palate and/or pharynx; excessive tissue removal during T & A) Anatomical irregularities involving tonsils, adenoids and/or faucial pillars Limited movement patterns due to neurologic involvement (Peterson-Falzone, 2001)
55
 Posterior Nasal Fricatives Anterior Nasal Fricatives (grimacing) (Riski,")
56 Glottal Stops Pharyngeal Stops Pharyngeal Fricatives Pharyngeal Affricates Mid-Dorsum Palatal Stops Velar Fricatives (backed oral productions) Posterior Nasal Fricatives Anterior Nasal Fricatives (grimacing) (Riski, 1994)

57
58 Also considered obligatory (equipment) Errors Due to Malocclusion Class III ( Underbite or anterior crossbite) May affect tongue placement for /t/, /d/, /s/, /z/ and labiodental placement for /f/, /v/ Class II ( Overbite ) May affect lip closure for bilabials Sibilants may be distorted
59 Crossbite Can contribute to lateralization of sibilants Lowered palatal vault Restricts tongue s articulatory space Dental Deviations Missing teeth may result in lateralization of sibilants Rotated teeth may result in distorted sibilants
")
60 Kummer, 2001)
")
61 Kummer, 2001)
")
62 Kummer, 2001)
63 Hypernasality, nasal air emission, weakened oral pressure consonants and/or structural errors Obligatory or unavoidable errors (probably require physical management) Secondary surgery / Orthodontic / Orthognathic management Compensatory articulation errors Learned errors (can remain after physical management; require speech therapy)
64
65 Classification and description of communication disorders (Metz, Schiavetti, & Sacco, 1990; Southwood & Weismer, 1993; Eadie and Doyle, 2002) Gold standard for clinical speech assessment of persons with cleft palate (Kuehn and Moller, 2000) Provide standards against which instrumental measures are evaluated (Kent, 1996) Treatment should only be indicated when a problem is perceived by a listener (Moller, 1991; Conley et al., 1997)
66 Types of Rating Tasks Categorical Mild-moderate-severe Equal-Appearing Interval Scaling 0-6 rating scale Direct Magnitude Estimation Rate the magnitude or ratio of difference between stimuli Other: Visual Analog Scaling, Binary, etc.
67 Intelligibility Articulation Nasal air emission Resonance Voice Acceptability
68 Methods of assessment Categorical Rating scales Percentages Comparison to peers Listener: familiar vs unfamiliar Context: conversation vs predictable tasks

69 Listen for: compensatory articulation errors audible nasal emission weak oral pressure consonants other articulation and phonological errors
70 Listen and watch for: Anterior Crossbite (Class III malocclusion) Distortions: fricatives, affricates, sibilants Labiodentals: reversed labiodental placement Overjet (Class II malocclusion) Bilabials: labiodental placement Missing / malopositioned teeth Distortions of sibilants
71 Listen for: Reduction or elimination the plosive quality of oral stop consonants or fricatives (high pressure consonants p, b, t, d, k, g, f, s, sh, z, ch, dg, th) Pressure improves when you plug the nose Often co-occur with audible nasal emission When severe, oral stop consonants can be perceived as nasal consonants (b m)
72 Listen for: (includes nasal turbulence, nasal snort, and nasal rustle) Obligatory: consistent nasal emission on virtually all pressure consonants usually accompanied by hypernasality Usually present on all pressure consonants except VELARS if due to a fistula only VS. Learned: only heard on specific sounds such as /s/, /z/, /ʃ/, /ʧ/, and/ or /f/ Watch for nasal/facial grimacing
73 Typically used as substitutions for /s/, /z/, /ʃ/, /ʧ/, /f/ Phoneme-specific nasal emission Diagnostic approaches to differentiate nasal fricatives vs. obligatory audible nasal emission Nasal occlusion
74 VPD usually associated with PERCEPTION of excessive nasality (too much nasal resonance) during production of vowels (esp. /i/, /u/), glides (/w/, /j/), and liquids (/l/, /r/) Often co-occurs with audible nasal emission (although inverse relationship with gap size and turbulence of nasal emission) Often co-occurs with weak pressure consonants and/or nasalized oral consonants
75 usually associated with nasal obstruction, obstructive pharyngeal flap, midface hypoplasia, septal deviation, choanal atresia, adenoid hypertrophy PERCEPTION of denasality/too little nasal resonance during production of vowels and nasal consonants /n, m/ and ng Denasalized nasal consonants, makes them perceptually similar to their oral counterpart (/m/ /b/, /n/ /d/)
76 Resonance distortions can vary in or Hypernasality may be inconsistent in presence or severity Hyponasality tends to be consistent in both respects Mixed distortions tend to be the most variable If articulation skills are severely impaired, may make it very difficult to judge resonance E.g., child with pervasive glottal stops
77 Listen for: often associated with VPD or pervasive glottal stop errors Characteristics: rough, breathy, strained, decreased loudness Possible vocal nodules Volume/intensity Is reduced loudness or dysphonia masking the severity of hypernasality? VPD may result in the perception of reduced loudness Is increased loudness/effort being utilized to increase pressure to compensate for VPD?
78 To the patient? Family? Clinician? Surgeon? Based on input of one or all? Impact on future vocational choices?
79 Obtain an adequate speech sample Perceptually analyze each speech parameter Correlate perceptual speech data with any orofacial examination findings Interpret your observations Make impressions/diagnosis Recommend instrumental assessment and imaging if concerns with VPD
80 Target your listening to different portions of the speech sample and RECORD the speech sample so you can listen again later Intelligibility: conversational sample (include some low-predictability questions) Articulation: use standard sentences and standardized testing (e.g., GFTA-2) Voice, resonance, nasal emission: use standard sentences, reading passage, conversational speech
81 Depends on age of patient, cognitive ability, reading ability, attention span Conversational sample Reading passages Picture description task, counting, recite words to a nursery rhyme, etc.
82 Repetition of a standard list of phrases and sentences (Henningsson et al., 2008; Trost Cardamone et al., 2011) Oral-only (no nasal phonemes, usually loaded with high pressure phonemes) Buy baby a bib. Pet the puppy. Take it to Ted. Daddy did it. Go get a bigger egg. I like cookies. I have six sisters. Shelly wears shoes. Zebras live at the zoo. Chuck goes to church. Judges like to jump. Fifty five fish. Nasal-loaded Mama made lemonade. Ten men came in when Jane rang. Mixed (oral and nasal phonemes)
83 Listen during: Oral-only stimuli (test for VPD symptoms) Nasal-loaded stimuli (test for hyponasality) Vowels or sustained SSS, FFF If a patient has listen for increase in pressure, improved resonance, and elimination of nasal emission when nose is closed. If patient is : listen for lack of change in nasal consonants when nose is closed.
84 Nasal emission may or may not be audible Listen for presence, consistency, and quality (turbulence) of nasal emission Determine if phoneme-specific or not Determine if only related to a fistula or not Confirm what you hear look for fogging during oral consonants; Fogging immediately prior to and after sentence production is NORMAL Can also use See-Scape, listening tubes, straw
85 Various standardized articulation tests are acceptable for use with patients with cleft palate/vpd (e.g., GFTA-2) Compare to norms Older Cleft Palate Tests are not widely used anymore Iowa Pressure Articulation Test Bzoch Test Fisher Logemann
86 What CAN the speaker do? Stimulability testing with the nose plugged for oral consonants Consider dental-occlusal hazards too
87 Are any related to the articulation errors? Dentition: missing/malposed teeth Occlusion Orthodontic appliances present (e.g., expander, W-arch wire) Maxillary arch width
88 Lips: closure at rest/breathing and speech Open mouth posture? Difficulty with lip closure due to overjet? Don t overanalyze tension of upper lip after cleft lip repair Fistula in hard or soft palate Soft palate: Length: short? Can you see the adenoid pad? Elevation during /a/ phonation: hints Symmetrical? Degree of elevation? Uvula (for noncleft patients): single and at midline? bifid? Other signs of SMCP? Tonsils: size
89 Consider: Is the child s speech appropriate for their age? Is intelligibility and/or acceptability significantly impacted by the child s speech disorder? Is the speech profile suggestive of underlying VPD? Are there articulation distortions due to dental-occlusal hazards? Is the child stimulable for improved articulation? What other factors are contributing to the speech disorder (e.g., hearing loss, fistula, nasal congestion, learning difficulties, etc.)?
90 Is additional diagnostic information necessary? of VP closure for speech (e.g., imaging)? Acoustic assessment of nasality (e.g., Nasometry)? Other medical testing (e.g., audiometry, genetics)? Is a necessary BEFORE performing imaging studies or making recommendations for physical management of VP closure for speech?
91
92 Does the instrumental assessment support the need for behavioral treatment (therapy) or physical management (surgery or a prosthesis)? What can the instrumental assessment tell us about the type of intervention that should be recommended?
93 Perceptual speech assessment Acoustic (e.g., Nasometry) Aerodynamic (e.g., Pressure-flow) Visualization of the VP mechanism Nasopharyngoscopy Multiview Videofluoroscopy
94 Acoustic correlate of nasality Nasalance = nasal sound energy / nasal + oral sound energy Higher nasalance correlates with perception of hypernasality Not a 1:1 relationship to listener perceptual judgments of resonance, but should confirm what you hear Good tool for comparison pre/post treatment Different products on the market can measure nasalance Nasometer II (KayPentax), Glottal Enterprises

95
96 Expressed as a percentage (or ratio), ranges from 1-100% (you can t have 0% nasalance) Norms available for a variety of stimuli, languages, dialects
97 Various stimuli options Standard reading passages Zoo Passage Rainbow Passage Nasal Sentences SNAP test-r (Simplified Nasometric Assessment Protocol, McKay-Kummer) Patient repeats syllables and prolonged sounds or produces sentences using read or picturecued stimuli
98 Treatment applications Biofeedback therapy Different treatment targets Ideal candidate: age 8 years+, good attention span, cooperative, can read sentences/passages, stimulable to modify nasal emission or resonance, good articulation, motivated
99 The Nasometer does not measure hypernasality The Nasometer does not measure nasal airflow Multiple score confounds lead to risk for underestimation or overestimation of nasalance score: Articulation errors, nasal congestion, nasal turbulence, voice disorders, mixed resonance, dialect/accent Surgical decisions should not be based only on nasalance scores
100 Often called multiview videofluoroscopy Lateral view, frontal view, base view, Towne s view Exposure to radiation Usually involves administration of barium via the nasal cavity Assess VP closure for speech, palatal length and elevation, size of adenoids and tonsils Patient repeats words and phrases

101
102 Provides direct view of VP (and laryngeal) structures and the VP port during speech Flexible fiberoptic or CHIP TIP technology combined with a nasopharyngoscope (adult or pediatric sizes) Topical anesthetic and nasal decongestant typically used Higher cooperation required Patient repeats standard words and phrases (primarily oral-only sample used to assess VP closure)
103 Determine presence and extent of VPD during speech Size of gap, shape Consistency of VP closure Movement of individual structures (velum, LPW, PPW) Size of adenoids, tonsils, and potential role in VPC Signs of occult SMCP
104 Limitations of Nasopharyngoscopy Subjective cannot obtain absolute measurements of gap size Differences in viewing perspectives, position of scope Possible tongue backing contribution to VPC Minimally invasive Discomfort Cooperation best if age 4 yrs+
105 Biofeedback therapy with Nasopharyngoscopy Option for treatment of compensatory errors (e.g., glottal stops, nasal fricatives) Provide visual cues for closure on specific sounds Compare and contrast open/closed port Requires highly cooperative patient, typically older schoolage, teen, or adult
106
107 Readily intelligible speech Socially acceptable speech Age-appropriate articulation skills Age-appropriate language skills
108 Improve velopharyngeal closure as soon as it is clear that the potential for adequacy is not present Most surgery for VPD is between 3-6 years
109 1. Improve VPC (physical management) but no speech therapy needed 2. Improve VPC and speech therapy needed 3. Speech therapy only- defer decision on VP management until additional therapy completed 4. Speech therapy needed and VPC is adequate 5. No treatment needed (continue to monitor)
 on an especially when compensatory articulation errors are")
110 Start therapy as soon as possible- for surgery or the cleft team to tell you to start therapy Need to establish at least some correct articulation placement prior to VP imaging or surgical decision Utilize a hierarchical- traditional articulation approach that (minimum 2x/week) on an especially when compensatory articulation errors are present

111 Only one sound is targeted and stabilized at a time in a hierarchical progression of speech contexts Start with isolation, syllable level, words, multisyllabic words, phrases, sentences, then connected speech Make sure that the child can produce the sound in spontaneous/connected speech before moving to the next goal. Give the child sufficient practice to solidify the new sound aim for high accuracy (90%+)
112 Where do I start? Options: Start with the sounds causing the most negative impact on intelligibility or VPC ( the compensatory errors) Target sounds for which the child is stimulable Keep developmental progression in mind, but don t be afraid to deviate from it Start with the sounds that are most visible (anterior) Usually, it is easier to start with voiceless sounds before voiced ones (especially if glottal stops are present)
113 Articulation errors compensatory articulation errors placement errors (substitutions, distortions) omissions backing of phonemes and other phonological errors In carefully selected cases, inconsistent mild hypernasality or inconsistent audible nasal emission MAY be improved with behavioral therapy Usually with biofeedback refer to a cleft SLP expert for this treatment
114 Traditional Articulation Therapy is the preferred method of treatment In most cases, this is NOT phonological therapy, at least not initially NOT oral-motor therapy This is therapy focused on phonetic-based approaches, with perceptual training using auditory, tactile, and visual cueing, and self-monitoring techniques Also utilizes motor-learning principles Drill practice as soon as child is mature enough

115 Teach identity, location, and actions of oral structures Teeth, lips, tongue Use a picture, mirror, Mr. Potato, Mighty-Mouth Teach sounds and their corresponding structures /p/: lip sound, popping sound, poof sound /t/: tongue sound or teeth sound /s/: snake sound /ʃ/: quiet/windy sound
116
117
118
119 Get the target sounds into the inventory Use easier sounds to elicit new sounds (shaping) /w/ or /m/ /p/, /b/ /l/ or /n/ /d/ /j/ /ʃ/ Provide auditory, visual, and tactile cues Use nasal occlusion as needed Teach correct oral target vs error sound contrasts auditory discrimination & negative practice: old sound vs new sound Establish reliable self-monitoring
120
121 Teach them to discriminate and identify throat sounds vs mouth sounds (or nose vs mouth ) Start teaching most visible or anterior sounds (e.g., /w/, /h/, /p/, /t/) and shape into target sounds Try voiceless sounds first (e.g., /p/, /t/ before /b/, /d/) Plug nose as needed to provide sensation of oral pressure Try /h/ words with the final consonants as targets (e.g., hoop, hop) Use overaspiration of air and whispering as needed Avoid words with nasal sounds or vowel initial words
122
123 horn-therapy program straw blowing/lip strengthening program palate massage/stimulation program yawning/sighing exercises whistle blowing exercises tongue movement exercises cookbooks to improve resonance
124 See-Scape Sometimes useful for treating learned nasal emission (nasal fricative substitutions) only if Phoneme Specific Auditory Biofeedback: listening tube, straw, oral-nasal listener Nasopharyngoscopy Nasometry? CPaP (Kuehn 1991, Kuehn et al., 2002)
125 Surgical Palatal lengthening and muscle repair (Furlow Z-plasty) Superiorly-based pharyngeal flap Sphincter pharyngoplasty Posterior wall augmentation / Fat injections Prosthetic Palatal lift Speech bulb
126 Indicated for short soft palate (or minimal elevation) when at least some degree of LPW movement is present

127 Pharyngeal Flap

128
129 Indicated when soft palate length and elevation are adequate but there is minimal LPW movement
130 Furlow z-plasty Muscle reorientation/repair and lengthening Often used for SMCP repair Option for very small VP gaps, nonsyndromic cases Pharyngeal wall augmentation (rarely used) Fat injection: results may only be temporary
131 When most commonly considered: Multiple surgical failures Surgical risk Airway concerns Neuromuscular etiology of VPD Borderline cases Diagnostic treatment


132 Palatal Lift Speech Bulb Obturator KNC/AT/LG/KM '10


133 Palatal Lift Palatal Bulb KNC/AT/LG/KM '10
134
135 5 year old female, adopted from China Repaired bilateral cleft lip and palate (lip-china, palate-age 2 years in US) Chronic OME, unilateral conductive hearing loss at last visit with right ear perforation In therapy at a local private practice, 1x per week, targets include /p/, /t/, and blowing exercises Unable to enroll in school-based therapy Held back from kindergarten this year due to concerns with intelligibility
136 Perceptual Speech Evaluation Standardized Articulation Testing (Language Testing) Oral Exam

137
138
139 Articulation errors: Pharyngeal fricatives for S, F, SH, Z, CH, TH, J Glottal stops for T, P, K, SH, Z, G, and inconsistent glottal coarticulation Nasal substitutions for K, G, Z, F, TH, CH, B, V inconsistently W/R substitutions D/G substitutions inconsistently B/V substitutions H substitutions for S, Z inconsistently Consistent weak pressure consonants Standard Score: <40, Percentile Rank <1st
140 Intelligibility : Child's connected speech is usually intelligible to familiar listeners but only occasionally intelligible to unfamiliar listeners Hypernasality: severe Hyponasality: none Audible Nasal Emission: present Voice Quality: rough, breathy Articulation: compensatory errors present
141 Dentition: Anterior crossbite (underbite) Fistula: Anterior hard palate fistula Palate: Soft palate is judged to be short in length Passavant's ridge activity is visible intraorally
142 Is there a role for continued or increased speech therapy? What suggestions would you make to her current therapy programming? Would instrumental assessment of nasality be helpful (i.e., Nasometry)? Is VP imaging indicated now? If yes, what stimuli would you use? What is your tentative hypothesis for the etiology of her speech disorder?
143 Increase frequency/intensity of current speechlanguage services to at least 2-3x per week with primary focus on articulation placement skills Therapy should target remediation of glottal stops, nasal substitutions, and pharyngeal fricatives first, before moving to other goals. Provide extensive placement cues for target sounds. Discontinue use of blowing exercises.
144 Carryover of accuracy at the word, phrase, sentence, and spontaneous speech levels at 90% accuracy for each target, prior to adding new goals to ensure mastery of skills. Nasal occlusion may be helpful (nose plugging) if tolerated intermittently during therapy. Avoid excessive loudness/effort during therapy sessions to minimize vocal hyperfunction.
145 Nasometry was not completed due to frequency and type of articulation errors and dysphonia, as well as some cooperation challenges
146 Cooperation was poor Level of speech sample: Single syllables and words only (sample focused on accurate phonemes only) Consistent velopharyngeal gap present during an oral-only speech sample. VP Gap Size: 4-Large Location of VP gap: Central VP Closure Pattern: Coronal Degree of Palatal Elevation: Minimal Medial Movement of the Lateral Pharyngeal Walls: Minimal
147 Would you proceed with recommending physical management? If yes, surgical or prosthetic?
148 Pharyngeal flap Increased speech therapy Future fistula closure/obturation Management of hearing loss Reassess speech at Team visit 6 months post-surgery
149 12 year old male 22q11.2 deletion syndrome (velocardiofacial syndrome) Congenital velopharyngeal dysfunction S/P pharyngeal flap, flap revision, previous tonsillectomy and adenoidectomy Seasonal allergies, learning disabilities, social skills deficits Home schooled, receiving teletherapy for articulation and language Parent voices concerns with resonance and intelligibility
150 Perceptual Speech Evaluation Standardized Articulation Testing (Language Testing) Oral Exam Nasopharyngoscopy and Nasometry
151
152 Intelligibility: intelligible to familiar listeners consistently, occasionally not understood by unfamiliar listeners Hypernasality: moderate Hyponasality: none Audible Nasal Emission: Consistently inaudible, inconsistently audible Voice Quality: rough Articulation: compensatory errors present, weak pressure for consonants? Dysarthric features
153 Standard score: 40, Percentile Rank: <1 st Errors: glottal stop substitutions for K and G, nasal fricatives for F and V, N for NG, N for L inconsistently, nasal fricative inconsistently for "J", nasal fricatives for TH, H/K substitutions only in blends. W/R substitutions distortions of CH S/SH substitutions Articulation errors were noted to increase with an increase in utterance length and complexity. This includes a significant increase in frequency of glottal stop errors in conversation as compared to structured tasks.
154 Facial and lip asymmetry at rest and in motion The left side of his face/lips has reduced movement Facial/lip motion for smiling is reduced. Significant overjet which interferes with lip closure Soft palate demonstrates asymmetrical elevation toward the right side Suggests left palatal weakness. Sensitive gag reflex observed Unlikely to tolerate palatal prosthesis
155 Zoo passage: 46% (mean 15%, +/- 5%) SNAP stimuli (picture-cued subtest): Bilabials: 20% (mean 11%, S.D. +/- 5%) Alveolars 27% (mean 11%, S.D., +/- 5%)
156
157 Very cooperative for the procedure. Slightly narrow and asymmetrical pharyngeal flap is present. The left port is larger than the right at rest. The right port demonstrates virtually complete (.90) closure during most speech tasks, with some mucous/bubbling. The left port demonstrates an inconsistent degree of closure, based on the speech stimuli and accuracy.

158 For accurate oral phonemes, closure is estimated at , but during inaccurate speech, closure is approximately.20 on the left Demonstrated the ability to modify and increase the closure of the left port during speech with endoscopic biofeedback L lateral pharyngeal wall demonstrates reduced degree of closure and slower motion than R side Consistent with suspected left pharyngeal weakness Atypical posterior pharyngeal wall motion emanating near midline with extension toward the left side of the pharynx is noted during speech Likely a compensatory behavior to assist with VP closure.
159 COMBINATION of traditional and biofeedback 2x per week TREATMENT GOALS: Increased VP closure for speech (left VP port) Accurate articulation placement Additional formal language testing. Candidate for flap revision in future Depends on results of therapy Re-eval with Cleft/Cranio team in 6 months Orthodontic treatment to correct his overjet to facilitate lip closure.
160 TRADITIONAL: Placement for velars Placement / oral airflow for /ʃ/, /ʧ/, /ɵ/, /f/, /j/ NASOPHARYNGOSCOPY: 100% closure in 80% of words and phrases targeted. NASOMETRY: Nasalance scores within normal limits at phrase level for SNAP stimuli 80% accuracy (below target reference line) for specific target words and phrases Consistent home practice
161 Achieved stimulability for velars with slight distortion, with higher accuracy for /k/ than /g/ CURRENT STATUS: /k/ in all positions of words (with slight distortion) with a model and intermittent auditory cues in 90% of opportunities /g/ in isolation with 75% accuracy (inconsistent uvularized placement or glottals) /ʃ/, /ʧ/, /f/ and /ɵ/ in words and phrases reviewed and 75% accuracy noted with frequent placement and auditory cues needed
162 Can produce all vowels except /i/ at or below a 40% nasalance reference line with and without a model; CV syllables for /p/, /t/, /k/, /s/, /ʃ/ with a model for all vowels except /i/ with 90% accuracy Can produce these CV syllables in oral-nasal contrasts with 90% accuracy Can produce CVC words for this set of sounds below the 40% reference line for all vowels except /i/ with 75% accuracy
163 Articulation placement for /k/ at the word and short phrase level. Achieved 90% accuracy in words and 80% in phrases (in all word positions) with a model, with slight distortion persisting inconsistently. /g/ is produced with uvular placement or as a /k/ substitution Fricatives and affricates: 90% accurate for oral airflow (with S/SH placement issues) at the phrase level Decreased accuracy noted in spontaneous speech--but good self correction with minimal cues
164 No change in resonance in spontaneous speech. Ccontinued difficulties with /i/ and /u/ Anticipatory nasal emission noted for /t/ and /d/ but generally oral and accurate /p/, /b/, /k/ and fricatives accurate at the syllable and selected word level Goals sustained at 30% reference line in 80% of cases at the syllable level only for constrained stimuli (without /i/, /g/, /u/ and diphthongs)
165


166
167 5:10 year old male Adopted from China Lip repair: China (age 7 months) Palate Repair: Age 15 months Fistula Repair: Age 2 years Secondary Surgery: Palatal lengthening at 4:9 Highly compliant for nasopharyngoscopy
168 Received speech therapy through EI and privately (outpatient) Had attended speech therapy at PSU, 2x weekly, in Spring 2011 term Enrolled in 2011 Summer Clinic program at PSU CONCERN: speech intelligibility
169 Receptive / Expressive Language: Not formally assessed, but believed to be well aboveaverage Reads at 2 nd grade level (at age 5) Speech: Distorted /s/ and /ʃ/ Gliding errors on /r/ and /l/ Final consonant deletion of plosives and /s/ Speech intelligibility improved with slower rate and focus on precision Nasal air emission on labial and alveolar sounds Resonance: WNL
170
171

172
173 Large anterior oral-nasal fistula Advanced cognitive skills Maintenance of speech skills Financial / Insurance constraints Adequate velopharyngeal closure
174 Accurate placement of /s/, /ʃ/, /l/ ISSUES: Loss of airflow, especially at the end of a sentence is, was, his Equipment issues! PROGRESS: Accurate production of /l/ as singleton (not yet in blends) Implementation of self-monitoring skills for rate Slower rate / over articulation Visual and verbal cues Reading aloud
175
176

177
178 Work within constraints Promote effective / efficient communication Preserve self-image / self-esteem Communicate with parents regarding expectations
179
Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563. Key Components of Cleft Palate Speech.
 Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563 Key Components of Cleft Palate Speech Disorder Type of Disorder/ Causes Hypernasality Resonance Disorder insufficiency
Cleft Palate Speech-Components and Assessment Voice and Resonance Disorders-ASLS-563 Key Components of Cleft Palate Speech Disorder Type of Disorder/ Causes Hypernasality Resonance Disorder insufficiency
Financial Disclosures
 Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Employment: Financial Disclosures Cincinnati Children
Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Employment: Financial Disclosures Cincinnati Children
Cleft Lip and Palate: The Effects on Speech and Resonance
 Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Cleft lip and/or palate can have a negative impact on both speech and resonance. The following is a summary of normal anatomy, the types and causes of
Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Cleft lip and/or palate can have a negative impact on both speech and resonance. The following is a summary of normal anatomy, the types and causes of
Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment
 Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Resonance Disorders and Velopharyngeal Dysfunction
Resonance Disorders and Velopharyngeal Dysfunction: Evaluation and Treatment Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Resonance Disorders and Velopharyngeal Dysfunction
Resonance Disorders & Velopharyngeal Dysfunction
 Resonance Disorders & Velopharyngeal Dysfunction Cincinnati Children s Normal Velopharyngeal Function Structures Active in Velopharyngeal Closure Velum (soft palate) - The velum moves in a superior and
Resonance Disorders & Velopharyngeal Dysfunction Cincinnati Children s Normal Velopharyngeal Function Structures Active in Velopharyngeal Closure Velum (soft palate) - The velum moves in a superior and
Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies
 Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Royalties: Financial Disclosures Book: Kummer, AW. Cleft Palate
Speech/Resonance Disorders due to Clefts and Craniofacial Anomalies Ann W. Kummer, PhD, CCC-SLP Cincinnati Children s Hospital Medical Center Royalties: Financial Disclosures Book: Kummer, AW. Cleft Palate
Evaluation and Treatment: using low-tech and no tech procedures
 Evaluation and Treatment: using low-tech and no tech procedures 6. Perceptual Evaluation When, What, How, and Why When the evaluation should be done for the most reliable results and maximum benefit for
Evaluation and Treatment: using low-tech and no tech procedures 6. Perceptual Evaluation When, What, How, and Why When the evaluation should be done for the most reliable results and maximum benefit for
Def. - the process of exchanging information and ideas
 What is communication Def. - the process of exchanging information and ideas All living things communicate. Acquiring Human Communication Humans communicate in many ways What is a communication disorder?
What is communication Def. - the process of exchanging information and ideas All living things communicate. Acquiring Human Communication Humans communicate in many ways What is a communication disorder?
Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash
 Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash Judith Trost-Cardamone, PhD CCC/SLP California State University at Northridge Ventura Cleft Lip & Palate Clinic and Lynn
Speech Sound Disorders Alert: Identifying and Fixing Nasal Fricatives in a Flash Judith Trost-Cardamone, PhD CCC/SLP California State University at Northridge Ventura Cleft Lip & Palate Clinic and Lynn
CLEFT PALATE & MISARTICULATION
 CLEFT PALATE & MISARTICULATION INTRODUCTION o Between the 6th and 12th weeks of fetal gestation,the left and right sides of the face and facial skeleton fuse in the midddle. When they do fail to do so,
CLEFT PALATE & MISARTICULATION INTRODUCTION o Between the 6th and 12th weeks of fetal gestation,the left and right sides of the face and facial skeleton fuse in the midddle. When they do fail to do so,
VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more!
 VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more! Brenda Sitzmann, MA, CCC-SLP Speech Language Pathologist Jill Arganbright, MD Assistant Professor, Pediatric
VPD Clinic: Using Nasopharyngoscopy to Evaluate Velopharyngeal Dysfunction and so much more! Brenda Sitzmann, MA, CCC-SLP Speech Language Pathologist Jill Arganbright, MD Assistant Professor, Pediatric
Let s start by tuning our ears!
 Craniofacial Speech Disorders: How to Identify, Transcribe & Plan Treatment Let s start by tuning our ears! Judith Trost-Cardamone, PhD - CCC/SLP, FASHA Professor, California State University-Northridge
Craniofacial Speech Disorders: How to Identify, Transcribe & Plan Treatment Let s start by tuning our ears! Judith Trost-Cardamone, PhD - CCC/SLP, FASHA Professor, California State University-Northridge
Developmental communication disorders
 Part I Developmental communication disorders 1 Cleft lip and palate and other craniofacial anomalies John E. Riski 1.1 Introduction Despite reports from the Centers for Disease Control and Prevention
Part I Developmental communication disorders 1 Cleft lip and palate and other craniofacial anomalies John E. Riski 1.1 Introduction Despite reports from the Centers for Disease Control and Prevention
LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology THE BASIC SOUNDS OF ENGLISH
 LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology 1. STOPS THE BASIC SOUNDS OF ENGLISH A stop consonant is produced with a complete closure of airflow in the vocal tract; the air pressure
LINGUISTICS 221 LECTURE #3 Introduction to Phonetics and Phonology 1. STOPS THE BASIC SOUNDS OF ENGLISH A stop consonant is produced with a complete closure of airflow in the vocal tract; the air pressure
It is important to understand as to how do we hear sounds. There is air all around us. The air carries the sound waves but it is below 20Hz that our
 Phonetics. Phonetics: it is a branch of linguistics that deals with explaining the articulatory, auditory and acoustic properties of linguistic sounds of human languages. It is important to understand
Phonetics. Phonetics: it is a branch of linguistics that deals with explaining the articulatory, auditory and acoustic properties of linguistic sounds of human languages. It is important to understand
TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION.
 TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION Meredith Gaylord A thesis submitted to the faculty of the University of North
TEMPORAL CHARACTERISTICS OF ALVEOLAR STOP CONSONANTS PRODUCED BY CHILDREN WITH VARYING LEVELS OF VELOPHARYNGEAL DYSFUNCTION Meredith Gaylord A thesis submitted to the faculty of the University of North
Communication disorders in individuals with cleft lip and palate: An overview
 Review Article Free full text on www.ijps.org DOI: 10.4103/0970-0358.57199 Communication disorders in individuals with cleft lip and palate: An overview Roopa Nagarajan, V. H. Savitha, B. Subramaniyan
Review Article Free full text on www.ijps.org DOI: 10.4103/0970-0358.57199 Communication disorders in individuals with cleft lip and palate: An overview Roopa Nagarajan, V. H. Savitha, B. Subramaniyan
Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP. November 20, 2009
 Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP November 20, 2009 Inadequate tissue with good innervation Classically associated with cleft palate Inadequate tissue
Mark Hakel, Ph.D., CCC-SLP, Julie Marshall, D.D.S., M.S. Monica McHenry, Ph.D. CCC-SLP November 20, 2009 Inadequate tissue with good innervation Classically associated with cleft palate Inadequate tissue
Cleft Lip and Palate. February 21, February 28, /17/2015
 Cleft Lip and Palate Dianne M. Altuna, M.S./CCC-SLP Region X ESC November 20, 2015 paltuna@aol.com 214.763.7388 February 21, 2014 Diagnosis/Types Common craniofacial syndromes associated with cleft lip
Cleft Lip and Palate Dianne M. Altuna, M.S./CCC-SLP Region X ESC November 20, 2015 paltuna@aol.com 214.763.7388 February 21, 2014 Diagnosis/Types Common craniofacial syndromes associated with cleft lip
Longitudinal Evaluation of Articulation and Velopharyngeal
 _ Longitudinal Evaluation of Articulation and Velopharyngeal Competence of Patients with Pharyngeal Flaps D. R. Van Demark, PH.D. M. A. Harpin, PH.D. In this study, 129 patients with cleft palate who had
_ Longitudinal Evaluation of Articulation and Velopharyngeal Competence of Patients with Pharyngeal Flaps D. R. Van Demark, PH.D. M. A. Harpin, PH.D. In this study, 129 patients with cleft palate who had
UNIVERSITY OF CINCINNATI
 UNIVERSITY OF CINCINNATI Date: I,, hereby submit this work as part of the requirements for the degree of: in: It is entitled: This work and its defense approved by: Chair: Speech Outcomes following Surgical
UNIVERSITY OF CINCINNATI Date: I,, hereby submit this work as part of the requirements for the degree of: in: It is entitled: This work and its defense approved by: Chair: Speech Outcomes following Surgical
Asia Pacific Journal of Research ISSN (Print) : ISSN (Online) :
 : ISSN (Online) :") CLEFT SPEECH A TELLTALE SIGN OF OCCULT SUBMUCOUS CLEFT: A CASE STUDY MS. ARPITA CHATTERJEE SHAHI AUDIOLOGIST AND SPEECH LANGUAGE PATHOLOGIST ALI YAVAR JUNG NATIONAL INSTITUTE FOR THE HEARING HANDICAPPED
CLEFT SPEECH A TELLTALE SIGN OF OCCULT SUBMUCOUS CLEFT: A CASE STUDY MS. ARPITA CHATTERJEE SHAHI AUDIOLOGIST AND SPEECH LANGUAGE PATHOLOGIST ALI YAVAR JUNG NATIONAL INSTITUTE FOR THE HEARING HANDICAPPED
 - speech-~echanism Assessment tion, a small dental mirror and gauze pads may be necessary. Before putting the gloves on, clean the table with disinfectant and wash your hands thoroughly with antibacterial
- speech-~echanism Assessment tion, a small dental mirror and gauze pads may be necessary. Before putting the gloves on, clean the table with disinfectant and wash your hands thoroughly with antibacterial
EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE
 EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE DEFINING TERMS PRIMARY PALATE- Structures anterior to the incisive foramen Includes the nose, lip alveolus, and hard palate back to the incisive
EVALUATION AND MANAGEMENT OF PATIENTS WITH CLEFT LIP AND PALATE DEFINING TERMS PRIMARY PALATE- Structures anterior to the incisive foramen Includes the nose, lip alveolus, and hard palate back to the incisive
Place and Manner of Articulation Sounds in English. Dr. Bushra Ni ma
 Place and Manner of Articulation Sounds in English Dr. Bushra Ni ma Organs of Speech Respiratory System Phonatory System Articulatory System Lungs Muscles of the chest Trachea Larynx Pharynx Lips Teeth
Place and Manner of Articulation Sounds in English Dr. Bushra Ni ma Organs of Speech Respiratory System Phonatory System Articulatory System Lungs Muscles of the chest Trachea Larynx Pharynx Lips Teeth
Speech: Something We Can Really Fix
 CHAPTER 2 Speech: Something We Can Really Fix As we have just seen, speech impairment is one of the most common findings in VCFS, occurring in at least 70% of cases (Shprintzen & Golding-Kushner, 2009).
CHAPTER 2 Speech: Something We Can Really Fix As we have just seen, speech impairment is one of the most common findings in VCFS, occurring in at least 70% of cases (Shprintzen & Golding-Kushner, 2009).
G l o s s a r y. The lack of closure of a normal body orifice or. passage
 A P P E N D I XE G l o s s a r y Allergic rhinitis Swelling of the membrane in the nasal chamber due to allergic reactions; the condition may obstruct breathing Alveolar ridge The bony arches of the maxilla
A P P E N D I XE G l o s s a r y Allergic rhinitis Swelling of the membrane in the nasal chamber due to allergic reactions; the condition may obstruct breathing Alveolar ridge The bony arches of the maxilla
LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY
 LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY LIPS (Latin labia ) labial sounds bilabial labiodental e.g. bee, my e.g. fly, veal TEETH (Latin dentes) dental sounds e.g. think, they ALVEOLAR
LINGUISTICS 130 LECTURE #4 ARTICULATORS IN THE ORAL CAVITY LIPS (Latin labia ) labial sounds bilabial labiodental e.g. bee, my e.g. fly, veal TEETH (Latin dentes) dental sounds e.g. think, they ALVEOLAR
Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate?
 Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate? Brenna Singer M.Cl.Sc (SLP) Candidate University of Western Ontario:
Critical Review: Is videonasopharyngoscopy biofeedback therapy effective in improving velopharyngeal closure in patients with cleft palate? Brenna Singer M.Cl.Sc (SLP) Candidate University of Western Ontario:
THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL
 V P I A CHALLENGE 40 YEARS A PHYSICIAN 37 YEARS TREATING PATIENTS WITH V P I THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL NO CP CENTER IN THE WORLD CAN CLAIM 0% PREVALENCE OF V P I AFTER
V P I A CHALLENGE 40 YEARS A PHYSICIAN 37 YEARS TREATING PATIENTS WITH V P I THE DEVIL KNOWS MORE FOR BEING OLD THAN FOR BEING THE DEVIL NO CP CENTER IN THE WORLD CAN CLAIM 0% PREVALENCE OF V P I AFTER
Figure 1. Basic anatomy of the palate
 CHAPTER 10 CLEFT LIP AND PALATE Chen Yan, MD and Sanjay Naran, MD I. ANATOMY AND DEFINITIONS A. Cleft Lip (CL) alone, Cleft Lip with Cleft Palate (CLP), and Cleft Palate (CP) alone 1. CL alone and CLP
CHAPTER 10 CLEFT LIP AND PALATE Chen Yan, MD and Sanjay Naran, MD I. ANATOMY AND DEFINITIONS A. Cleft Lip (CL) alone, Cleft Lip with Cleft Palate (CLP), and Cleft Palate (CP) alone 1. CL alone and CLP
Longitudinal outcome of pharyngoplasty
 Archives of Orofacial Sciences (2009), 4(1): 17-21 CASE REPORT Longitudinal outcome of pharyngoplasty Peter J. Anderson*, Roslynn K. Sells, David. J. David Australian Craniofacial Unit, Women s and Children
Archives of Orofacial Sciences (2009), 4(1): 17-21 CASE REPORT Longitudinal outcome of pharyngoplasty Peter J. Anderson*, Roslynn K. Sells, David. J. David Australian Craniofacial Unit, Women s and Children
Speech (Sound) Processing
 Processing") 7 Speech (Sound) Processing Acoustic Human communication is achieved when thought is transformed through language into speech. The sounds of speech are initiated by activity in the central nervous system,
7 Speech (Sound) Processing Acoustic Human communication is achieved when thought is transformed through language into speech. The sounds of speech are initiated by activity in the central nervous system,
Associations between speech features and phenotypic severity in Treacher Collins syndrome
 Åsten et al. BMC Medical Genetics 2014, 15:47 RESEARCH ARTICLE Open Access Associations between speech features and phenotypic severity in Treacher Collins syndrome Pamela Åsten 1*, Harriet Akre 2,3 and
Åsten et al. BMC Medical Genetics 2014, 15:47 RESEARCH ARTICLE Open Access Associations between speech features and phenotypic severity in Treacher Collins syndrome Pamela Åsten 1*, Harriet Akre 2,3 and
Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults
 Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults Objectives: The primary purpose of this study was to determine the temporal characteristics of aerodynamic segments
Temporal Characteristics of Aerodynamic Segments in the Speech of Children and Adults Objectives: The primary purpose of this study was to determine the temporal characteristics of aerodynamic segments
Overview. Acoustics of Speech and Hearing. Source-Filter Model. Source-Filter Model. Turbulence Take 2. Turbulence
 Overview Acoustics of Speech and Hearing Lecture 2-4 Fricatives Source-filter model reminder Sources of turbulence Shaping of source spectrum by vocal tract Acoustic-phonetic characteristics of English
Overview Acoustics of Speech and Hearing Lecture 2-4 Fricatives Source-filter model reminder Sources of turbulence Shaping of source spectrum by vocal tract Acoustic-phonetic characteristics of English
Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE
 Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE Cleft lip (cheiloschisis) and cleft palate (palatoschisis), which can also occur together as cleft lip and palate, are variations of a type of clefting
Dr.ALI AL BAZZAZ PLASTIC SURGON CLEFT LIP AND PALATE Cleft lip (cheiloschisis) and cleft palate (palatoschisis), which can also occur together as cleft lip and palate, are variations of a type of clefting
Slide 1. Slide 2. Slide 3. Introduction to the Electrolarynx. I have nothing to disclose and I have no proprietary interest in any product discussed.
 Slide 1 Introduction to the Electrolarynx CANDY MOLTZ, MS, CCC -SLP TLA SAN ANTONIO 2019 Slide 2 I have nothing to disclose and I have no proprietary interest in any product discussed. Slide 3 Electrolarynxes
Slide 1 Introduction to the Electrolarynx CANDY MOLTZ, MS, CCC -SLP TLA SAN ANTONIO 2019 Slide 2 I have nothing to disclose and I have no proprietary interest in any product discussed. Slide 3 Electrolarynxes
Speech production: disordered EPG data
 Speech production: disordered EPG data F.E. Gibbon QMUC, Edinburgh VISPP Summer School - Palmse, Estonia August 10-15 2005 aims of lecture 2 recognise EPG patterns produced by those with speech disorders
Speech production: disordered EPG data F.E. Gibbon QMUC, Edinburgh VISPP Summer School - Palmse, Estonia August 10-15 2005 aims of lecture 2 recognise EPG patterns produced by those with speech disorders
o Spectrogram: Laterals have weak formants around 250, 1200, and 2400 Hz.
 Ch. 10 Places of articulation 1) Primary places of articulation a) Labials: made with one or both lips i) Bilabial: two lips. Bilabial stops and nasals are common, while fricatives are uncommon. ii) Labiodental:
Ch. 10 Places of articulation 1) Primary places of articulation a) Labials: made with one or both lips i) Bilabial: two lips. Bilabial stops and nasals are common, while fricatives are uncommon. ii) Labiodental:
Speech Generation and Perception
 Speech Generation and Perception 1 Speech Generation and Perception : The study of the anatomy of the organs of speech is required as a background for articulatory and acoustic phonetics. An understanding
Speech Generation and Perception 1 Speech Generation and Perception : The study of the anatomy of the organs of speech is required as a background for articulatory and acoustic phonetics. An understanding
Spoken language phonetics: Consonant articulation and transcription. LING 200 Spring 2006
 Spoken language phonetics: Consonant articulation and transcription LING 200 Spring 2006 Announcements, reminders Quiz re Ch. 1-2: question 9 dropped, results have been recalculated Homework #1 (transcription
Spoken language phonetics: Consonant articulation and transcription LING 200 Spring 2006 Announcements, reminders Quiz re Ch. 1-2: question 9 dropped, results have been recalculated Homework #1 (transcription
CLEFT LIP and PALATE. Sahlgrenska University Hospital Göteborg, Sweden. Information about Cleft Lip and Palate. English version
 CLEFT LIP and PALATE Sahlgrenska University Hospital Göteborg, Sweden Information about Cleft Lip and Palate English version 1 TABLE OF CONTENTS page What are cleft lip and palate? 3 Which children can
CLEFT LIP and PALATE Sahlgrenska University Hospital Göteborg, Sweden Information about Cleft Lip and Palate English version 1 TABLE OF CONTENTS page What are cleft lip and palate? 3 Which children can
Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after Cleft Palate Repair
 Egypt, J. Plast. Reconstr. Surg., Vol. 29, No. 2, July: 149-156, 2005 Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after
Egypt, J. Plast. Reconstr. Surg., Vol. 29, No. 2, July: 149-156, 2005 Comparative Study between Superiorly Based Pharyngeal Flap and Sphincteroplasty in Treatment of Velopharyngeal Insufficiency after
Introduction to Standard Esophageal Speech. Texas Laryngectomy Association 2018
 Introduction to Standard Esophageal Speech Texas Laryngectomy Association 2018 Disclosure Objectives At the end of this presentation the participant will be able to: Describe the production of standard
Introduction to Standard Esophageal Speech Texas Laryngectomy Association 2018 Disclosure Objectives At the end of this presentation the participant will be able to: Describe the production of standard
Page 2 of 5 9th weeks of gestation, as the palatal shelves change from a vertical to horizontal position and fuse. The tongue must migrate away from t
 Page 1 of 5 TITLE: Cleft Lip and Palate SOURCE: UTMB Dept. of Otolaryngology Grand Rounds DATE: January 28, 1998 RESIDENT PHYSICIAN: Greg Young, M.D. FACULTY: Ronald Deskin, M.D. SERIES EDITOR: Francis
Page 1 of 5 TITLE: Cleft Lip and Palate SOURCE: UTMB Dept. of Otolaryngology Grand Rounds DATE: January 28, 1998 RESIDENT PHYSICIAN: Greg Young, M.D. FACULTY: Ronald Deskin, M.D. SERIES EDITOR: Francis
Speech and Intelligibility Characteristics in Fragile X and Down Syndromes
 Speech and Intelligibility Characteristics in Fragile X and Down Syndromes David J. Zajac, Ph.D. 1 Gary E. Martin, Ph.D. 1 Elena Lamarche, B.A. 1 Molly Losh, Ph.D. 2 1 Frank Porter Graham Child Development
Speech and Intelligibility Characteristics in Fragile X and Down Syndromes David J. Zajac, Ph.D. 1 Gary E. Martin, Ph.D. 1 Elena Lamarche, B.A. 1 Molly Losh, Ph.D. 2 1 Frank Porter Graham Child Development
Has your child ever received a speech and language evaluation? if so, when? Has he/she attended therapy?
 Today s Date: Cleft Palate and Craniofacial Speech Disorders - Intake Form Welcome to Momentum Therapy Center. The information you provide on this form will help us prepare your child s upcoming speech-language
Today s Date: Cleft Palate and Craniofacial Speech Disorders - Intake Form Welcome to Momentum Therapy Center. The information you provide on this form will help us prepare your child s upcoming speech-language
Objectives. Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP
 Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP 503-808-9919 linda@donofrioslp.com My clinical experience & scope of practice n Be able to conduct an oromyofunctional
Oromyofunction & Oral Health Gum Gardeners April 28, 2014 Linda D Onofrio, MS, CCC-SLP 503-808-9919 linda@donofrioslp.com My clinical experience & scope of practice n Be able to conduct an oromyofunctional
Clinical Study Clinical Outcomes of Primary Palatal Surgery in Children with Nonsyndromic Cleft Palate with and without Lip
 Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 185459, 5 pages http://dx.doi.org/10.1155/2015/185459 Clinical Study Clinical Outcomes of Primary Palatal Surgery in
Hindawi Publishing Corporation BioMed Research International Volume 2015, Article ID 185459, 5 pages http://dx.doi.org/10.1155/2015/185459 Clinical Study Clinical Outcomes of Primary Palatal Surgery in
Downloaded on T04:25:43Z. Title. Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate
 Title Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate Author(s) Gibbon, Fiona E. Publication date 2004-08 Original citation Type of publication Link to publisher's
Title Abnormal patterns of tongue-palate contact in the speech of individuals with cleft palate Author(s) Gibbon, Fiona E. Publication date 2004-08 Original citation Type of publication Link to publisher's
Clinical experience from primary palatoplasty and studies of velopharyngeal
 The Effect of Intravelar Veloplasty on Velopharyngeal Competence Following Pharyngeal Flap Surgery Bennie L. Jarvis, M.D. Wicuiam C. Trier, M.D. Clinical experience from primary palatoplasty and studies
The Effect of Intravelar Veloplasty on Velopharyngeal Competence Following Pharyngeal Flap Surgery Bennie L. Jarvis, M.D. Wicuiam C. Trier, M.D. Clinical experience from primary palatoplasty and studies
Assignment #4: Speech Target /p/ By: Robyn Black STAGE MODALITY STRATEGIES/TECHNIQUES MATERIALS
 Assignment #4: Speech Target /p/ By: Robyn Black Target phoneme: /p/ Manner: Plosive Description: A plosive is a speech sound produced by the closure of the oral passage followed by a release accompanied
Assignment #4: Speech Target /p/ By: Robyn Black Target phoneme: /p/ Manner: Plosive Description: A plosive is a speech sound produced by the closure of the oral passage followed by a release accompanied
Phonetics is the study of vocal sounds. Phonetics and flight safety - An orodental view point. Gp Capt K Ravishankar *, Air Cmde GP Singh VSM +
 Phonetics Methods and in flight Aerospace safety - Medicineethods An orodental view point: Aerospace Ravishankar Medicine K ABSTRACT Phonetics and flight safety - An orodental view point Gp Capt K Ravishankar
Phonetics Methods and in flight Aerospace safety - Medicineethods An orodental view point: Aerospace Ravishankar Medicine K ABSTRACT Phonetics and flight safety - An orodental view point Gp Capt K Ravishankar
Communication and Swallowing with PSP/CBD. Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist
 Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Communication and Swallowing with PSP/CBD Megan DePuy, MBA, MS, CCC-SLP Private Speech Pathologist A Speech Therapist? Why? Swallowing (Dysphagia) Speech (Dysarthria, Dysphonia) Language (Aphasia) An Experienced
Historical study of a program of systematic obturator reduction for palatal incompetence
 University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1980 Historical study of a program of systematic obturator reduction
University of Montana ScholarWorks at University of Montana Graduate Student Theses, Dissertations, & Professional Papers Graduate School 1980 Historical study of a program of systematic obturator reduction
Sylvia Rotfleisch, M.Sc.(A.) hear2talk.com HEAR2TALK.COM
 hear2talk.com HEAR2TALK.COM") Sylvia Rotfleisch, M.Sc.(A.) hear2talk.com 1 Teaching speech acoustics to parents has become an important and exciting part of my auditory-verbal work with families. Creating a way to make this understandable
Sylvia Rotfleisch, M.Sc.(A.) hear2talk.com 1 Teaching speech acoustics to parents has become an important and exciting part of my auditory-verbal work with families. Creating a way to make this understandable
UCL Repair: Emphasis on Muscle Dissection and Reconstruction
 UCL Repair: Emphasis on Muscle Dissection and Reconstruction Unilateral cleft lip repair is performed using rotation-advancement technique. Markings are made on columella base, redlines, Cupid s bow on
UCL Repair: Emphasis on Muscle Dissection and Reconstruction Unilateral cleft lip repair is performed using rotation-advancement technique. Markings are made on columella base, redlines, Cupid s bow on
Acoustic Analysis of Nasal and Oral Speech of Normal versus Cleft Lip and Palate Asharani Neelakanth 1 Mrs. Umarani K. 2
 IJSRD - International Journal for Scientific Research & Development Vol. 3, Issue 05, 2015 ISSN (online): 2321-0613 Acoustic Analysis of Nasal and Oral Speech of Normal versus Cleft Lip and Palate Asharani
IJSRD - International Journal for Scientific Research & Development Vol. 3, Issue 05, 2015 ISSN (online): 2321-0613 Acoustic Analysis of Nasal and Oral Speech of Normal versus Cleft Lip and Palate Asharani
Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings
 Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings Objective: The purpose of this study was to describe the pressure-flow characteristics of
Pressure-Flow Characteristics of /m/ and /p/ Production in Speakers Without Cleft Palate: Developmental Findings Objective: The purpose of this study was to describe the pressure-flow characteristics of
Carolinas Center for Cleft Lip & Palate Surgery
 Carolinas Center for Cleft Lip & Palate Surgery Carolinas Center for Oral & Facial Surgery 8840 Blakeney Professional Drive Suite 300 Charlotte NC 28277 P: 704.716.9840 F: 704.716.9841 Clinical Coordinator
Carolinas Center for Cleft Lip & Palate Surgery Carolinas Center for Oral & Facial Surgery 8840 Blakeney Professional Drive Suite 300 Charlotte NC 28277 P: 704.716.9840 F: 704.716.9841 Clinical Coordinator
ASU Speech and Hearing Clinic Spring Testing. Adult Speech and Language Evaluation
 Adult Speech and Language Evaluation ASU Speech and Hearing Clinic Spring Testing Name: DOB:_ Gender: Examiner:_ Date: Instructions: Administer the following screening tools and standardized tests/batteries.
Adult Speech and Language Evaluation ASU Speech and Hearing Clinic Spring Testing Name: DOB:_ Gender: Examiner:_ Date: Instructions: Administer the following screening tools and standardized tests/batteries.
Jan 24: Cleft Lip/Cleft Palate (updated 08/06) Jan 24: Cleft Lip/Cleft Palate (updated 08/06) Preceptor: ; Vacation Scott
 Jan 24: Cleft Lip/Cleft Palate (updated 08/06) Preceptor: ; Vacation Scott") Jan 24: Cleft Lip/Cleft Palate (updated 08/06) Preceptor: ; Vacation Scott 1. (Amy) Discuss the incidence, causes and genetic aspects of cleft lips and palates (CL and CP). Cleft lip/palate deformities
Jan 24: Cleft Lip/Cleft Palate (updated 08/06) Preceptor: ; Vacation Scott 1. (Amy) Discuss the incidence, causes and genetic aspects of cleft lips and palates (CL and CP). Cleft lip/palate deformities
International Confederation for Cleft Lip and Palate and Related Craniofacial Anomalies Task Force Report: Speech Assessment
 The Cleft Palate Craniofacial Journal 51(6) pp. e138 e145 November 2014 Ó Copyright 2014 American Cleft Palate Craniofacial Association BRIEF COMMUNICATION International Confederation for Cleft Lip and
The Cleft Palate Craniofacial Journal 51(6) pp. e138 e145 November 2014 Ó Copyright 2014 American Cleft Palate Craniofacial Association BRIEF COMMUNICATION International Confederation for Cleft Lip and
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page
 Vol. 73 (9), Page") The Egyptian Journal of Hospital Medicine (October 18) Vol. 73 (9), Page 7604-7609 Role of MRI in Detection of Repaired Cleft Palate Muscles and Correlation to Speech Amro Mahmoud Abdelrahman Ali, Mahmoud
The Egyptian Journal of Hospital Medicine (October 18) Vol. 73 (9), Page 7604-7609 Role of MRI in Detection of Repaired Cleft Palate Muscles and Correlation to Speech Amro Mahmoud Abdelrahman Ali, Mahmoud
We Can Predict Postpalatoplasty Velopharyngeal Insufficiency in Cleft Palate Patients
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. We Can Predict Postpalatoplasty Velopharyngeal Insufficiency in Cleft Palate Patients Jacques E. Leclerc,
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. We Can Predict Postpalatoplasty Velopharyngeal Insufficiency in Cleft Palate Patients Jacques E. Leclerc,
LINGUISTICS 221 LECTURE #6 Introduction to Phonetics and Phonology. Consonants (continued)
") LINGUISTICS 221 LECTURE #6 Introduction to Phonetics and Phonology FRICATIVES 1. Bilabial fricatives: Consonants (continued) The constriction is between the upper and lower lips. The lips are brought together
LINGUISTICS 221 LECTURE #6 Introduction to Phonetics and Phonology FRICATIVES 1. Bilabial fricatives: Consonants (continued) The constriction is between the upper and lower lips. The lips are brought together
CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1
 CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1 By JOHN E. HOOPES, M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D.,
CINERADIOGRAPHIC ASSESSMENT OF COMBINED ISLAND FLAP PUSHBACK AND PHARYNGEAL FLAP IN THE SURGICAL MANAGEMENT OF SUBMUCOUS CLEFT PALATE 1 By JOHN E. HOOPES, M.D., z A. LEE DELLON, 3 JACOB I. FABRIKANT, M.D.,
IN THE UNITED STATES PATENT AND TRADEMARK OFFICE. For PROVISIONAL APPLICATION FOR LETTERS PATENT. Inventor: David Rexford. Logical Phonetic Alphabet
 IN THE UNITED STATES PATENT AND TRADEMARK OFFICE PROVISIONAL APPLICATION FOR LETTERS PATENT For Logical Phonetic Alphabet Inventor: David Rexford Logical Phonetic Alphabet Inventor: David Rexford FIELD
IN THE UNITED STATES PATENT AND TRADEMARK OFFICE PROVISIONAL APPLICATION FOR LETTERS PATENT For Logical Phonetic Alphabet Inventor: David Rexford Logical Phonetic Alphabet Inventor: David Rexford FIELD
VOICE LESSON #6. Resonance: Creating Good Vocal Vibes. The Soft Palate
 VOICE LESSON #6 Resonance: Creating Good Vocal Vibes Voice Lesson #6 - Resonance Page 1 of 7 RESONANCE is the amplification and enrichment of tones produced by the voice. When we talk about resonance,
VOICE LESSON #6 Resonance: Creating Good Vocal Vibes Voice Lesson #6 - Resonance Page 1 of 7 RESONANCE is the amplification and enrichment of tones produced by the voice. When we talk about resonance,
Velopharyngeal dysfunction (VPD) occurs
 occurs") Clinical Experience The Effect of Timing of Surgery for Velopharyngeal Dysfunction on Speech Devra B. Becker, MD,* Lynn M. Grames, SLP-CCC,* Thomas Pilgram, PhD,* Alex A. Kane, MD,* Jeffrey L. Marsh, MD
Clinical Experience The Effect of Timing of Surgery for Velopharyngeal Dysfunction on Speech Devra B. Becker, MD,* Lynn M. Grames, SLP-CCC,* Thomas Pilgram, PhD,* Alex A. Kane, MD,* Jeffrey L. Marsh, MD
The Ear, Nose and Throat in MPS
 The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
The Ear, Nose and Throat in MPS Annerose Keilmann Voice Care Center Bad Rappenau, Germany Preciptorship program on MPS Wiesbaden, November 2 nd 2015 Alterations of the outer and middle ear in MPS I narrowing
Sibilants Have Similar Sound Production
 The Entire World of Sibilants Christine Ristuccia, M.S. CCC-SLP Sibilants Have Similar Sound Production Related sounds. They are produced at or just behind alveolar ridge (bumpy gum area behind front teeth).
The Entire World of Sibilants Christine Ristuccia, M.S. CCC-SLP Sibilants Have Similar Sound Production Related sounds. They are produced at or just behind alveolar ridge (bumpy gum area behind front teeth).
rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center
 Treatment of Gom pensatory Articulation Errors rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center chans "+##ffilhospitar =X}H 6JhEFSHIM+,L. Com pensatory m isarticulations are substitution errors
Treatment of Gom pensatory Articulation Errors rcgftffi$ehffih!htr Claudia Yun,tA Grainiofacial Center chans "+##ffilhospitar =X}H 6JhEFSHIM+,L. Com pensatory m isarticulations are substitution errors
how stopped air is released when released with puff of air = aspirated when release is unaspirated, captured air is released into vowel (i.e.
 1 STOP CONSONANTS also referred to as plosives labeled to describe manner of production a speech sound with closure or stopping of airstream within the oral cavity interruption of airflow has two phases:
1 STOP CONSONANTS also referred to as plosives labeled to describe manner of production a speech sound with closure or stopping of airstream within the oral cavity interruption of airflow has two phases:
Evaluating the Clinical Effectiveness of EPG. in the Assessment and Diagnosis of Children with Intractable Speech Disorders
 Evaluating the Clinical Effectiveness of EPG in the Assessment and Diagnosis of Children with Intractable Speech Disorders Sara E. Wood*, James M. Scobbie * Forth Valley Primary Care NHS Trust, Scotland,
Evaluating the Clinical Effectiveness of EPG in the Assessment and Diagnosis of Children with Intractable Speech Disorders Sara E. Wood*, James M. Scobbie * Forth Valley Primary Care NHS Trust, Scotland,
Speech Spectra and Spectrograms
 ACOUSTICS TOPICS ACOUSTICS SOFTWARE SPH301 SLP801 RESOURCE INDEX HELP PAGES Back to Main "Speech Spectra and Spectrograms" Page Speech Spectra and Spectrograms Robert Mannell 6. Some consonant spectra
ACOUSTICS TOPICS ACOUSTICS SOFTWARE SPH301 SLP801 RESOURCE INDEX HELP PAGES Back to Main "Speech Spectra and Spectrograms" Page Speech Spectra and Spectrograms Robert Mannell 6. Some consonant spectra
A Simple Technique for Determining Velopharyngeal Status during Speech Production
 A Simple Technique for Determining Velopharyngeal Status during Speech Production Kate Bunton, Ph.D., CCC-SLP, 1 Jeannette D. Hoit, Ph.D., CCC-SLP, 1 and Keegan Gallagher 1 ABSTRACT Clinical evaluation
A Simple Technique for Determining Velopharyngeal Status during Speech Production Kate Bunton, Ph.D., CCC-SLP, 1 Jeannette D. Hoit, Ph.D., CCC-SLP, 1 and Keegan Gallagher 1 ABSTRACT Clinical evaluation
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
C ritical Review: How is Quality of Life Affected in Children with Velo-pharyngeal Insufficiency?
 C ritical Review: How is Quality of Life Affected in Children with Velo-pharyngeal Insufficiency? Shannon Serdar M.Cl.Sc (SLP) Candidate University of Western Ontario: School of Communication Sciences
C ritical Review: How is Quality of Life Affected in Children with Velo-pharyngeal Insufficiency? Shannon Serdar M.Cl.Sc (SLP) Candidate University of Western Ontario: School of Communication Sciences
DENTAL MANAGEMENT OF CLEFT LIP AND PALATE. J Harewood DDS MA MS
 DENTAL MANAGEMENT OF CLEFT LIP AND PALATE J Harewood DDS MA MS CLEFT LIP/PALATE: INCIDENCE Cleft lip and/or palate 1:1000 Varies with race Japan: 20: 10 000 Western Europe: 12: 10 000 USA: 10.2:10 000
DENTAL MANAGEMENT OF CLEFT LIP AND PALATE J Harewood DDS MA MS CLEFT LIP/PALATE: INCIDENCE Cleft lip and/or palate 1:1000 Varies with race Japan: 20: 10 000 Western Europe: 12: 10 000 USA: 10.2:10 000
Understanding 22q11.2 Deletion Syndrome
 Understanding 22q11.2 Deletion Syndrome 22q11.2 Deletion Syndrome ( 22q11.2 ) is a genetic disorder that is also referred to as Velo- Cardio-Facial Syndrome ( VCFS ), Shprintzen Syndrome, and/or DiGeorge
Understanding 22q11.2 Deletion Syndrome 22q11.2 Deletion Syndrome ( 22q11.2 ) is a genetic disorder that is also referred to as Velo- Cardio-Facial Syndrome ( VCFS ), Shprintzen Syndrome, and/or DiGeorge
Surgery for Pediatric Velopharyngeal Insufficiency
 oks ==> freeinebo Advances Oto-Rhino-Laryngology Editor: G. Randolph Vol. 76 Surgery for Pediatric Velopharyngeal Insufficiency Editors N. Raol C.J. Hartnick Surgery for Pediatric Velopharyngeal Insufficiency
oks ==> freeinebo Advances Oto-Rhino-Laryngology Editor: G. Randolph Vol. 76 Surgery for Pediatric Velopharyngeal Insufficiency Editors N. Raol C.J. Hartnick Surgery for Pediatric Velopharyngeal Insufficiency
The patient, a white male, was born with a submucous cleft palate, bifid uvula, and a notch of the posterior hard palate. He received speechlanguage
 CASE REPORTS Maxillary protraction to intentionally ankylosed deciduous canines in a patient with cleft palate M. Lena Omnell, DDS, MSD,' and Barbara Sheller, DDS, MSD b Seattle, Wash. The patient, a white
CASE REPORTS Maxillary protraction to intentionally ankylosed deciduous canines in a patient with cleft palate M. Lena Omnell, DDS, MSD,' and Barbara Sheller, DDS, MSD b Seattle, Wash. The patient, a white
Critical Review: Effectiveness of EMA in improving articulatory accuracy in adults with AOS
 Critical Review: Effectiveness of EMA in improving articulatory accuracy in adults with AOS Lana Goldberg M.Cl.Sc SLP Candidate The University of Western Ontario: School of Communication Sciences and Disorders
Critical Review: Effectiveness of EMA in improving articulatory accuracy in adults with AOS Lana Goldberg M.Cl.Sc SLP Candidate The University of Western Ontario: School of Communication Sciences and Disorders
Plastic and Jaw Department, United Sheffield Hospitals
 THE EXAMINATION OF IMPERFECT SPEECH FOLLOWING CLEFT-PALATE OPERATIONS By WILFRED HYNES, F.R.C.S Plastic and Jaw Department, United Sheffield Hospitals THE results of cleft-palate operations can be difficult
THE EXAMINATION OF IMPERFECT SPEECH FOLLOWING CLEFT-PALATE OPERATIONS By WILFRED HYNES, F.R.C.S Plastic and Jaw Department, United Sheffield Hospitals THE results of cleft-palate operations can be difficult
PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE. Robert M. Mason, DMD, PhD
 PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE Robert M. Mason, DMD, PhD ABSTRACT: A parent s questions about a 3 year old with tongue thrusting and an anterior open bite are
PARENT CONCERNS A 3 YEAR OLD CHILD WITH TONGUE THRUSTING AND AN OPEN BITE Robert M. Mason, DMD, PhD ABSTRACT: A parent s questions about a 3 year old with tongue thrusting and an anterior open bite are
Made available courtesy of the Acoustical Society of America:
 Controlling changes in vocal tract resistance By: Donald W. Warren, Anne Putnam Rochet, Rodger M. Dalston, and Robert Mayo Warren, D.W., Roceht, A.P., Dalston, R.M., and Mayo, R. (1992). Controlling changes
Controlling changes in vocal tract resistance By: Donald W. Warren, Anne Putnam Rochet, Rodger M. Dalston, and Robert Mayo Warren, D.W., Roceht, A.P., Dalston, R.M., and Mayo, R. (1992). Controlling changes
ARTICULATION THERAPY FOR CHILDREN WITH CLEFT PALATE USING VISUAL ARTICULATORY MODELS AND ULTRASOUND BIOFEEDBACK
 Roxburgh, Z. and Scobbie, J. M. and Cleland, J. (2015) Articulation therapy for children with cleft palate using visual articulatory models and ultrasound biofeedback. In: Proceedings of the 18th International
Roxburgh, Z. and Scobbie, J. M. and Cleland, J. (2015) Articulation therapy for children with cleft palate using visual articulatory models and ultrasound biofeedback. In: Proceedings of the 18th International
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Kristina M. Blaiser, PhD, CCC-SLP Assistant Professor, Utah State University Director, Sound Beginnings
 Kristina M. Blaiser, PhD, CCC-SLP Assistant Professor, Utah State University Director, Sound Beginnings Objectives Discuss changes in population of children with hearing loss: Impacts on speech production
Kristina M. Blaiser, PhD, CCC-SLP Assistant Professor, Utah State University Director, Sound Beginnings Objectives Discuss changes in population of children with hearing loss: Impacts on speech production
Effect of temporary prosthetic mandibular advancement on velopharyngeal closure for speech
 University of Iowa Iowa Research Online Theses and Dissertations Summer 2015 Effect of temporary prosthetic mandibular advancement on velopharyngeal closure for speech Kyungsup Shin University of Iowa
University of Iowa Iowa Research Online Theses and Dissertations Summer 2015 Effect of temporary prosthetic mandibular advancement on velopharyngeal closure for speech Kyungsup Shin University of Iowa
SPEECH PERCEPTION IN A 3-D WORLD
 SPEECH PERCEPTION IN A 3-D WORLD A line on an audiogram is far from answering the question How well can this child hear speech? In this section a variety of ways will be presented to further the teacher/therapist
SPEECH PERCEPTION IN A 3-D WORLD A line on an audiogram is far from answering the question How well can this child hear speech? In this section a variety of ways will be presented to further the teacher/therapist
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
Title of Mucoperiosteal Flap on the Cleft. Citation 音声科学研究 = Studia phonologica (1991),
,") Title Velopharyngeal Function after Palat of Mucoperiosteal Flap on the Cleft Matsumoto, K Akiko; Isshiki, Nobuhi Author(s) Kimura, Tadashi; Nose, Kensuke; Kaw Tomoko Citation 音声科学研究 = Studia phonologica
Title Velopharyngeal Function after Palat of Mucoperiosteal Flap on the Cleft Matsumoto, K Akiko; Isshiki, Nobuhi Author(s) Kimura, Tadashi; Nose, Kensuke; Kaw Tomoko Citation 音声科学研究 = Studia phonologica
APPENDIX A. MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge)
 You will need this scoresheet and a disposable ruler (or a Boley Gauge)") APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
Prosthetic Rehabilitation of a Velopharyngeal Defect: A Case Report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 4 Ver. X (Apr. 2015), PP 01-05 www.iosrjournals.org Prosthetic Rehabilitation of a Velopharyngeal
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 4 Ver. X (Apr. 2015), PP 01-05 www.iosrjournals.org Prosthetic Rehabilitation of a Velopharyngeal
Disclosures. Overview. Goals I. Goals II. Clefts, Syndromes, and Care from Prenatal to Adulthood
 Age 11 Cleft lip and palate playing a game Clefts, Syndromes, and Care from Prenatal to Adulthood Robert Byrd, MD, MPH Associate Professor of Clinical Pediatrics Pediatrician, UCDMC Cleft and Craniofacial
Age 11 Cleft lip and palate playing a game Clefts, Syndromes, and Care from Prenatal to Adulthood Robert Byrd, MD, MPH Associate Professor of Clinical Pediatrics Pediatrician, UCDMC Cleft and Craniofacial