An Investigation of Surface Characteristics of Enamel Treated with Infiltrative Resin: A Scanning Electron Microscopy Study
|
|
|
- Delphia Roberts
- 5 years ago
- Views:
Transcription


1 Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2017 An Investigation of Surface Characteristics of Enamel Treated with Infiltrative Resin: A Scanning Electron Microscopy Study Danielle E. Easterly Virginia Commonwealth University Follow this and additional works at: Part of the Dental Materials Commons, Oral Biology and Oral Pathology Commons, Orthodontics and Orthodontology Commons, and the Other Dentistry Commons Danielle E Easterly Downloaded from This Thesis is brought to you for free and open access by the Graduate School at VCU Scholars Compass. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of VCU Scholars Compass. For more information, please contact libcompass@vcu.edu.
2 Danielle Easterly 2017 All Rights Reserved
3 An Investigation of Surface Characteristics of Enamel Treated with Infiltrative Resin: A Scanning Electron Microscopy Study A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Dentistry at Virginia Commonwealth University. By Danielle E. Easterly B.A., Psychology, University of Virginia, 2010 D.D.S., Virginia Commonwealth University, 2015 Director: Dr. Eser Tüfekçi, D.D.S., M.S., Ph.D., M.S.H.A. Professor, VCU Department of Orthodontics Virginia Commonwealth University Richmond, Virginia May 2017
4 ii Acknowledgement The author wishes to express gratitude to many people. First and foremost, thank you to my mother and father, Margo and Jim Easterly, and to my fiancé Andrew Robb, for their constant support and encouragement. I would also like to extend a large thank you to Jennifer Shim for all her help in preparing the samples and for her help in data preparation. Thank you to Dr. Dmitry Pestov for all of his guidance and expertise in the area of nanomicroscopy and materials. Thank you to Judy Williamson for completing the SEM analysis of all the samples in the study. Thank you also to Dr. Robert Seghi of The Ohio State University for his guidance and donation of the toothbrush simulator. Last but very importantly, thank you to my thesis advisor Dr. Eser Tüfekçi for her motivation, guidance, and friendship.
5 iii Table of Contents Acknowledgement... ii Table of Contents... iii List of Figures... iv List of Tables... v Abstract... vi Introduction... 1 Materials and Methods... 6 Results Discussion Conclusions Literature Cited Appendix: SEM Images of Extracted Teeth Vita... 61
6 iv List of Figures Figure 1: Confirmation of WSLs on Pilot Teeth... 7 Figure 2: Mounting of tooth under toothbrush simulator Figure 3: Baseline Image of Sound Enamel. Tooth B. 250X Magnification Figure 4: Baseline Image of Demineralized Enamel. Tooth C. 250X Magnification Figure 5: Tooth 2. Location B. T1. 250X Magnification Figure 6: Tooth 4. Location B. T1. 250X Magnification Figure 7: Tooth 10. Location B. T1. 250X Magnification Figure 8: Changes in Presence of Enamel Rods After Simulated Brushing Figure 9: Changes in Presence of Microcracks After Simulated Brushing Figure 10: Changes in Presence of Fractures After Simulated Brushing Figure 11: Association between Enamel Rods and Microcracks Figure 12: Association between Enamel Rods and Fractures Figure 13: Tooth 2. Location B. T1 (left) and T2 (right). 250X Magnification Figure 14: Comparison between T1 (left) and T2 (right) of Tooth 4. Location C. 250X Magnification Figure 15: Tooth 1. Location B. T1. 250X Magnification Figure 16: Tooth 3. Location B. T2. 250X Magnification Figure 17: Tooth 6. Location B. T1. 250X Magnification... 25
7 v List of Tables Table 1: Distribution of SEM Characterizations between T1 and T
8 vi Abstract AN INVESTIGATION OF SURFACE CHARACTERISTICS OF ENAMEL TREATED WITH INFILTRATIVE RESIN: A SCANNING ELECTRON MICROSCOPY STUDY Danielle E. Easterly, Doctorate of Dental Surgery. A thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in Dentistry at Virginia Commonwealth University. Virginia Commonwealth University Director: Dr. Eser Tüfekçi D.D.S., M.S., Ph.D., M.S.H.A. Objective: To evaluate the microstructural changes of a resin infiltrant (ICON, DMG America LLC, Englewood, NJ) after six months of simulated toothbrushing. Materials and Methods: Ten extracted third molars (n=10) were collected. Artificial white spot lesions were created and resin applied. Environmental SEM images at 250X and 500X were taken after application of Icon (T1), and after six months of simulated toothbrushing (T2). Micrographs were evaluated for changes in surface characteristics. Results: SEM showed some changes in the surface characteristics of the resin after simulated toothbrushing. However, changes in presence of enamel rods, microcracks, or fractures were not
9 statistically significant (p>0.05). The effects of polymerization shrinkage were noted on most samples in the form of clefts and fissures. Conclusions: Icon resin seems to withstand challenge by toothbrush abrasion over a six-month period, with some evidence of microstructural wear. vi i
10 Introduction White spot lesions (WSLs) are one of the most common unesthetic sequelae from fixed appliances, and leave clinicians with a challenge regarding their management. WSLs develop from dissolution of calcium, phosphate and fluoride ions from the enamel due to prolonged plaque retention, which results in microporosities in the remaining tooth structure. 1 Demineralized enamel takes on a white chalky appearance that represents the initial phase of caries formation prior to more extensive enamel breakdown. Previous studies reported a wide variance in prevalence of WSLs, ranging from 0 to 97%, which was thought to result from the differences in the study designs. 2-4 However, a well-designed study from 2013 found that approximately 25% of patients undergoing orthodontic therapy develop a WSL during treatment. 2 In a recent systematic literature review, the incidence and prevalence of WSLs were reported as 45% and 68%, respectively, in orthodontic patients. 5 Therefore, despite the development of new preventive materials and products, demineralization appears to negatively affect a significant portion of orthodontic patients. Although it is generally accepted that patients are responsible for the prevention of WSLs, orthodontists and general dentists should educate patients at risk, and implement the appropriate preventive measures. 6 Minimally invasive dentistry and fluoride delivery systems in the form of mouthwashes and toothpastes should be considered as the first line of defense to prevent incipient caries. In non-compliant patients, fluoride varnishes or other fluoride delivery systems can be used to arrest the caries process by decreasing the susceptibility of enamel to acid attack or even to promote remineralization. 7 For active or arrested WSLs that are more advanced or 1
11 have been present for a longer duration, fluoride treatment is not recommended as only the external layer of demineralized enamel will harden. This will create an enamel surface that is hard and more lustrous than the initial WSL, however the loss of fluorescence at the deeper layer will largely remain, causing the appearance of a white opacity to remain on the tooth Thus, for deeper or longstanding WSLs, different interventions need to be utilized to arrest the caries process and improve the aesthetic outcome. Recently, an unfilled low-viscosity infiltrative resin (Icon, DMG America LLC, Englewood, NJ) has been introduced as a non-invasive agent to diminish the appearance of WSLs and hence to improve esthetics. 11 One major benefit of this resin is the ability to improve the appearance of WSLs without removal of gross tooth structure, which was reflected by findings in a recent systematic literature review. 12 However, it was concluded that due to insufficient high quality studies, more research was needed to determine long-term efficacy of the infiltrative resin. Icon, abbreviated from Infiltration concept, is composed primarily of monomer triethylene glycol dimethacrylate (TEGDMA), with solvent composed of ethanol and photoinitators camphorquinone (CQ), and ethyl-4-dimethylaminobenzoate (DABE). The unfilled property of this infiltrative resin allows for low viscosity and a high penetration coefficient, which is necessary for the resin to penetrate completely into enamel with a small pore volume. 13 After removal of the superficial hardened enamel layer with 15% hydrochloric acid (HCL), the application of resin over the lesion infiltrates the porosities present in the exposed demineralized enamel by capillary action. This process takes place over the course of several minutes. 14 The enamel consequently is sealed off and filled from within, without requiring a protective surface layer of resin thickness, which is the primary mechanism by which other sealant products on the 2
12 market function. 15 Additionally, since the porosities in the enamel are filled, which would normally serve as pathways for bacterial migration into deeper tooth structures, the resin also serves as a barrier to stop the future progression of incipient lesions by physically blocking further mechanical, bacterial, and acid attack. 15 The TEGDMA in infiltrative resin is comprised of a shorter C-O backbone than other similar monomers such a Bis-GMA, which has a higher viscosity. While the shorter backbone imparts the low viscosity necessary for infiltration, it also causes a higher degree of polymerization shrinkage after light curing, especially with only a single application. 16 The polymerization results in cleft-like structures embedded within the resin, which can lead to decreased acid resistance. 16 Evidence shows that a repeated application of the resin can fill in these clefted areas, and also that a double application after a period of continued demineralization increases the enamel micro-hardness of the demineralized area significantly more than a single application. 17,18 Studies have also shown that hardness for infiltrated lesions is lower than for typical glassionomer cements and composite resins, which could indicate an increased susceptibility for wear Since unfilled resins are typically not resistant to mechanical abrasion over time, it is possible that breakdown or wear of the infiltrant could take place. Therefore, there may be a need for repeated applications of the resin. In the literature, numerous studies focused on the long-term color stability of infiltrative resin. These investigations reported that the demineralized enamel treated with the resin infiltrant becomes discolored over time when exposed to substances such as coffee and wine However, the discoloration is reversible, and upon rubber cup polishing the discolored resin treated enamel readily gains back its original color characteristics. Despite several studies on the color stability, there is only limited information available on the long-term mechanical stability 3
13 of the resin infiltrant when subjected to mechanical wear and daily abrasive challenges such as toothbrushing. Yetkiner et al. 25 compared the stability of Icon paired with different enamel adhesives on bovine teeth, challenging the material with cycles of acidic solution and toothbrush abrasion. To measure stability, the amount of calcium dissolution from the teeth over time into aqueous solution was measured. Despite showing initial stability, the amount of calcium leached from the resin treated teeth was found to increase over time. In contrast, untreated control teeth exhibited calcium dissolution at a more constant rate over time. This finding may be indicative of some mechanical breakdown of the resin infiltrant over time when challenged by an acidic environment and mechanical abrasion. In contrast, a 2011 study investigating the toothbrush abrasion resistance of infiltrative resin applied onto demineralized bovine teeth, reported wear as a vertical loss in height compared to adjacent healthy enamel. 26 Despite a trend in the vertical loss in height, there was not a statistically significant change in the vertical height between the resin treated enamel and untreated adjacent tooth surface. These were promising results, which may be indicative of the stability of the resin infiltrant and its resistance to structural breakdown over time when subjected to repetitive mechanical abrasion. Resin infiltration treatment for human teeth, if shown to exhibit resistance to toothbrush wear over time, may offer clinicians a promising tool in the management of post-orthodontic WSLs. Since the success of the resin infiltrant depends on its structural integrity, it is of interest to investigate Icon s resistance to mechanical wear using a model similar to toothbrushing. Therefore, the purpose of the current study was to evaluate, using scanning electron microscopy (SEM), the microstructural changes of resin infiltrant after six months of simulated 4
14 toothbrushing in extracted human teeth. The null hypothesis was that there would be no visually detectable changes in microstructural surface characteristics on the infiltrative resin surface after six months of simulated toothbrushing. 5
15 Materials and Methods In this in vitro study, previously extracted non-carious human third molars (n=10) were retrieved from the oral and maxillofacial surgery department. Teeth with no visible defects or demineralization were cleaned to remove any debris, and stored in 5% chloramine T hydrate solution (Fischer Chemical, Hampton, NH) for disinfection. The teeth were then transferred into vials filled with distilled water, and stored until the demineralization procedures were started. The most flat surface of each tooth was painted with a thin layer of an acid-resistant varnish (Revlon, Cherries in the Snow, New York City, New York) leaving a 3mm diameter circle in the middle of the crown surface exposed to the acidic solution. The acidic solution was prepared according to the protocol outlined by Kumar et al. 27 by mixing 2.2 mm calcium chloride (Fisher Bioreagents, Hampton, NH), 0.05 mm acetic acid (Fisher Bioreagents, Hampton, NH), 2.2 mm monopotassium phosphate (EMD Millipore, Billerica, MA) and titrating the contents to a ph of 4.4 with 1.0 M potassium hydroxide (Fisher Chemical, Hampton, NH). A small hole was drilled near the apex of each tooth so that a nonfluoridated dental floss could be used to suspend teeth in the acidic solution. Samples were kept in the demineralizing medium for 10 days. Each day, the acidity of the solution was checked with a ph meter to ensure the solution was stable at or near 4.4 ph, and the tooth surfaces were examined for the development of white spot lesions (Figure 1). 6

16 Figure 1: Confirmation of WSLs on Pilot Teeth. Following visual confirmation of the artificial WSLs, resin infiltrant was applied by the same operator to the demineralized area created within the 3mm diameter circle according to the manufacturer s instructions using the following steps: 1. 15% HCl acid gel application for 2 minutes while gently rubbing the gel to ensure the fresh etch contacted with the tooth surface. 2. Rinsing for 30 seconds with water followed by drying with oil free air. 3. Application of Icon Dry ethanol solution for 30 seconds, followed by oil free air drying. 4. Application of Icon Infiltrant, allowed to sit for 3 minutes. Removal of the excess resin with a cotton roll followed by light curing for 40 seconds 5. Application of Icon Infiltrant a second time, allowed to sit for 1 minute. Removal of the excess resin with a cotton roll followed by light curing for 40 seconds. 6. Polishing with fine and extra fine aluminum oxide polishing strips (Soflex, 3M ESPE, St Paul, MN) Following the application of the resin infiltrant, four indentations were made at the north, east, west and south aspects of the circle using a number 8-round bur for easy identification of the resin treated surfaces under the microscope. 7
.")
17 For the SEM analyses, tooth surfaces were examined using SEM under variable pressure, with values ranging between Pa (Zeiss EVO-50XVP). The initial SEM analyses included the examination of tooth surfaces to establish the characteristics of the sound and demineralized enamel (n = 2, each). Microscopic images of the representative areas were taken at 250X magnification on each tooth surface. These micrographs provided the microscopic characteristics of sound and demineralized enamel surfaces, and later were used for comparisons between the baseline and follow-up images. The resin treated tooth surfaces were first examined under the SEM at T1 which represented the original resin treated enamel. Images for each tooth were taken at 250X magnification, taken at three randomly selected points within the circular window. Following the initial analyses of the tooth surfaces for roughness, cracks and scratches, all samples were then subjected to the equivalent of 6 months of toothbrushing using a simulator (Figure 2). Figure 2: Mounting of tooth under toothbrush simulator. 8
18 In this study, a total of 2,500 horizontal strokes were applied to tooth surfaces to simulate six months of toothbrushing, assuming teeth were brushed two times per day for two minutes. The number of strokes were calculated based on the knowledge that, over the course of a two-year period and brushing three times per day, 15,000 toothbrush strokes on average are applied to each tooth in the human mouth. 28 Standard soft bristle toothbrushes (GUM 407 model, Sunstar Global, Schaumberg, IL) were mounted within the toothbrush simulator over one of the six wells. The teeth were mounted in separate wells within the simulator with the Icon-coated surface facing perpendicular to the toothbrush head and bristle tufts. The force of the toothbrush simulator was adjusted to apply 225 g of force during toothbrushing. Between measurements and experimental steps, teeth were stored in randomly numbered containers, submerged in roomtemperature distilled water to prevent desiccation. All teeth were brushed using a fresh toothbrush to protect against wear of the bristles. A new toothbrush was also used after the equivalent of three months of toothbrushing. After toothbrushing, all teeth were again examined with variable pressure SEM using the same magnification parameters, defined as T2. Two examiners were blinded to the images and time points and evaluated changes in images before and after toothbrushing for the presence of 1) enamel rods, 2) microcracks, and 3) fractures. For the purpose of grading the images, the presence of these characteristics was defined as present (Y) if more than 75% of the tooth surface imaged showed the presence of these features, partial (P) if between 25 and 75%, and absent (N) if viewed on less than 25% of the imaged tooth surface. A total of 60 SEM images, 30 at each timepoint, were evaluated by two examiners (Appendix I). Inter-rater reliability was tested for using Cohen s Kappa, and changes between T1 and T2 were compared across time using Bowker s test for symmetry for a single rater s evaluations. Additionally, association between presence of enamel rods with both 9
19 microcracks and fissures were tested using a chi-squared test. A significance level of p = 0.05, and program SAS EG v6.1 were used for all statistical analyses. Inter-rater correlation was classified as strong for scored images at 250X magnification for presence (Y), partial (P), or absence (N) of enamel rods ( =0.80), microcracks ( =0.80), and fractures ( =0.81). 10
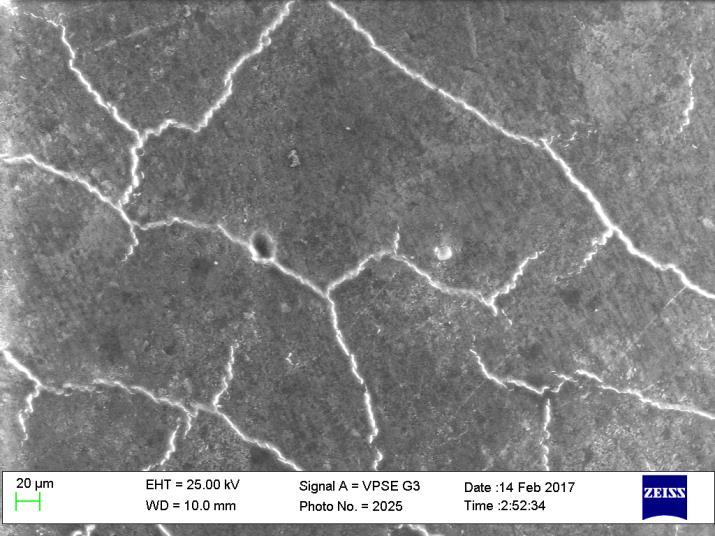
20 Results All of the resin-treated tooth surfaces had, to some degree, microstructural features consisting of enamel rods, microporosity, fissures, and cracks. Enamel rods were generally present both in the sound enamel and enamel treated with infiltrative resin, and in both samples were approximately 4 microns in diameter. This was consistent with measurements found in previous studies which showed the diameter of enamel prisms averaging 4 to 5 microns, with a cylindrical appearance. 29 However, in the demineralized samples, increased porosity was noted at the surface with dissolution of the prism core and thus a larger diameter in width of the rod at the periphery, with many as wide as 6 or 7 microns (Figures 3 and 4). Figure 3: Baseline Image of Sound Enamel. Tooth B. 250X Magnification. 11
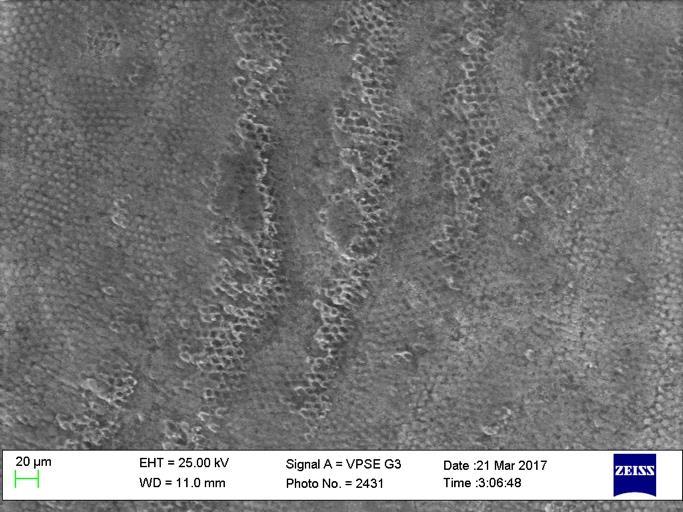
21 Figure 4: Baseline Image of Demineralized Enamel. Tooth C. 250X Magnification. This increased porous enamel was successfully infiltrated in the experimental teeth, which was determined by the absence of hollow prism cores and a restoration of an intact surface. A common presentation of the samples included areas of concentrated enamel rods visible at the level of the tooth surface, with resin either displaying a slight thickness which was visible on the tooth surface in irregular patterns, or interspersed within the typical honey-comb pattern of the enamel rods, filling in areas of porosity between adjacent prisms. While significant heterogeneity existed between teeth, visualization of enamel rods within the resin, as well as microcracks, and fissures, in varying degrees, were common findings. While the porosities in the demineralized tooth structure appeared successfully infiltrated, returning its surface appearance closer to that of sound enamel, the resin coated surfaces did maintain a high degree of visible roughness and surface irregularity. SEM images from T2 appeared generally similar to those in T1, and qualitative differences before and after toothbrushing were mainly noted by direct comparison of paired images. Characteristic images are shown from teeth prior to toothbrushing below (Figures 5-7). 12
22 Figure 5: Tooth 2. Location B. T1. 250X Magnification. Figure 6: Tooth 4. Location B. T1. 250X Magnification. Figure 7: Tooth 10. Location B. T1. 250X Magnification. 13
23 Changes in the presence of enamel rods, microcracks, or fractures between time points are illustrated in Figures While some qualitative changes were noted on paired images over time, none of the overall changes in presence of these microstructural characteristics were found to be statistically significant (p = , p = , and , respectively). Table 1 displays the total number of teeth present within each category before and after toothbrushing, as well as the total percentage of paired images which showed a change in characterization between time points. Table 1: Distribution of SEM Characterizations between T1 and T2. Enamel Rods Fractures Microcracks T1 T2 T1 T2 T1 T2 Y 15, 50% 17, 57% 6, 20% 9, 30% 7, 23% 10, 33% P 9, 30% 5, 17% 8, 27% 4, 13% 12, 40% 13, 43% N 6, 20% 8, 27% 16, 53% 17, 57% 11, 37% 7, 23% Total Changed 10, 33% 14, 47% 11, 37% Figure 8 shows into which specific categories the movement was evident between paired images for presence of enamel rods. At T1, 15 SEM images were found to have enamel rods present (Y), 9 images had enamel rods partially present (P), and 6 showed an absence of enamel rods (N). After toothbrushing, 33% of the images were characterized into different groups than they were at T1 for presence of enamel rods, indicative of some surface changes occurring. Of the images initially showing a presence of enamel rods, a majority (80%) of these teeth were still found to show presence of rods after toothbrushing. None of the images which showed absence of enamel rods were found at T2 to have exposure of enamel rods which would result in movement into either the partial or the present categories. While it was evident that change occurred between time points in the images, the net changes over time of presence of enamel rods was not statistically significant, with most of the changes occurring in the teeth which were described as having partial enamel rod coverage prior toothbrushing (p = ). 14
24 Figure 8: Changes in Presence of Enamel Rods After Simulated Brushing. Microcracks and fissures present on the resin surface were common findings throughout the samples. For this study, fractures were defined as fissures within the resin-enamel interface where a cleft-like gap could be visually detected at 250X magnification. Microcracks displayed a similar appearance to fractures, however the surface of the resin appeared intact, without gap formation. Figure 9 displays the distribution of all samples regarding microcracks at the surface before and after toothbrushing. At T1, 63% of the images displayed microcracks present at some level (either present or partially present), and 37% of the images had a change in classification after toothbrushing. Of images which were found to have presence (Y) of microcracks at T1, 71% of these images were still found to have microcracks after toothbrushing, and no pair of 15

25 images evaluated showed enough of a decrease in microcracks to be defined as absent of this characteristic. Twelve images were found to have partial occurrence of microcracks at baseline. Of these images, 25% of the images were judged to have more microcracks uncovered at T2, and 8% had removal of microcracks from the surface. Similar to the changes in enamel rods, while changes in the distribution of microcracks did occur between groups, these differences were not found at a level of statistical significance to result in a predictable change in any particular direction (p =0.3618). Figure 9: Changes in Presence of Microcracks After Simulated Brushing. Fractures were found to be present on 6 of the tooth images at T1, partially present on 8 16
26 images, and absent on 16 images at T1. In other words, 47% of the tooth images showed gap formation severe enough at the surface of the resin to be able to visualize a cleft-like fissure within the resin. Interestingly, just under half (47%) of these teeth had a change in characterization from before to after toothbrushing, with most of the change evident within the present and partially present groups. For example, of the teeth with fractures present at T1, 50% were still present after toothbrushing, and 33% of images showed fractures only partially present. When fissures were not present at T1, 75% of the teeth continued to show absence of fissures after brushing (Figure 10). Again, despite changes in the characterization of 47% of images regarding fractures, there was not a statistically significant difference for fracture presence to change in either a positive direction (more fractures over time) or negative direction (less fractures over time) (p= ). 17
 and fractures (p =0.0021).")
27 Figure 10: Changes in Presence of Fractures After Simulated Brushing. Of additional interest was the association between presence of enamel rods and both microcracks and fractures. There was a significant positive correlation between absence of enamel rods and presentation of both microcracks (p = ) and fractures (p =0.0021). Specifically, of the images which did not display a presence of enamel rods, 71% of these images also displayed microcracks and 36% displayed fractures. Figures 11 and 12 depict these relationships below. 18
28 Figure 11: Association between Enamel Rods and Microcracks 19
29 Figure 12: Association between Enamel Rods and Fractures 20
30 Discussion While small changes in microstructural characteristics were noted qualitatively in infiltrative resin treated tooth surfaces, none of these differences were large enough in this study s sample to result in statistical significance. Therefore, it may be concluded that there were not significant changes in the microstructural characteristics of resin infiltrant after six months of simulated toothbrushing. However, some qualitative changes were observed which should be taken into consideration for the clinical use of infiltrative resin treatment for WSLs. Infiltrative resin, compared to other resins, sealants, or composites, is uniquely difficult to detect with the naked eye due to its nature as a colorless resin, which takes on the color of the sound enamel which it infiltrates. Thus, changes in fluorescence or differences in color are not reliable methods to detect its presence as it can be with other resin materials. Even microscopically, the resin was found to restore the appearance of demineralized enamel back to that close to the appearance of sound enamel, and at times detection between infiltrated enamel and sound enamel alone was challenging. A high degree of roughness of the infiltrative resin surface was noted throughout samples. This is consistent with previous studies which have shown that after application of infiltrative resin, the roughness of the infiltrated teeth even approximates that of demineralized enamel. 30,31 This finding of significant roughness was also found in the current study. As is visible in the comparison below, small scratches after polishing, despite polishing with fine and very fine aluminum-oxide coated polishing discs, are present at 250X magnification 21
31 (Figure 13). These areas of roughness were noted in many instances to be smoothed by six months of simulated toothbrushing. Comparing T2 at this same location on this tooth, it can be noted that, while resin is still apparent, the number of surface scratches decreased. However, microcracking is seen toward the right side of the image indicating the resin is present at the surface, as well as still interspersed between the enamel rods throughout the image. Figure 13: Tooth 2. Location B. T1 (left) and T2 (right). 250X Magnification. Another feature, which was found in some samples across time, was the opening of fractures at the resin-enamel surface after toothbrushing. A frequent presentation was that microcracks identified before toothbrushing changed appearance to that of a fracture after toothbrushing. While this phenomenon did not occur with high enough frequency to show statistical significance in this study s sample, it should be noted that the manufacturer of Icon recommends a second application of resin to fill in potential gaps that could form due to polymerization shrinkage. 16,17 The change from a microcrack to a fracture is indicative that a small surface layer of infiltrative resin, which may have been occluding these fractures, was removed by toothbrushing, re-exposing the gap within the resin. The comparison between T1 and T2 below on one sample (Figure 14) shows a dramatic representation of this phenomenon. 22
32 Since gap formation at the enamel-resin interface may be susceptible to bacterial, acid, or mechanical attack, repeated application of resin infiltrant six months after initial application could be useful to prevent leakage in these areas of wear. 15 Figure 14: Comparison between T1 (left) and T2 (right) of Tooth 4. Location C. 250X Magnification. It should also be noted that not all teeth with microcracks became fissured after toothbrushing. In some instances, brushing the tooth surface either removed or lessened the quantity of microcracks, and in other cases uncovered new sub-surface microcracks. It is important to note that any movement between categories in the current study was indicative of a surface change. Even if there wasn t a statistically significant pattern to these changes, their overall presence indicates potentially significant clinically changes. Removal or uncovering of additional microcracks and fractures indicates that some qualitative changes in the surface characteristics of the resin took place. This was also true in the case of enamel rod presentation. One of the most striking findings in the current study was the high degree of heterogeneity between the appearances of all the images. Several different explanations for these differences can be hypothesized, including: 1) Embedded debris or contaminants may have 23
33 altered the surface appearance. Specifically, removal of the excess surface layer by cotton rolls could have left small cotton fibers in the surface layer of resin. 2) Differences in natural tooth anatomy may explain why some teeth showed higher prevalence of features such as craze lines. 3) Some teeth may have displayed more fracturing from traumatic extraction procedures. 4) Perhaps some teeth experienced more fracturing from desiccation during the sample preparation for SEM analysis than others. Many of these causes of heterogeneity between samples are also proposed reasons why many of the images show significant surface roughness. An additional important finding of the current study was the significant correlation between absence of enamel rods visible at the tooth surface and an increase in the presence of microcracks and fissures (p = , and p =0.0021, respectively). These were specimens in which a thicker layer of resin appeared to be present at the surface. Previous studies have shown that when resin is present in an increased thickness, the internal pressure from polymerization shrinkage is in turn significantly increased. 16,17,32 As a result, higher gap formation and fracturing is often found within the enamel-resin layer. While removal of the surface layer of resin with a cotton roll prior to polymerization is recommended, it may be tempting for some practitioners to want to leave this excess in place as a potential layer of sealant. The results of this study indicate that this practice could be contraindicated, and lead to decreased structural integrity of the resin. However, this should be weighed against the extra protective benefit previous studies have shown, that leaving an excess of resin on the surface could protect the teeth against acid erosion. 33 Figures show instances of higher resin fracturing when enamel rods are not present, and the surface-resin layer appears thickened. 24
34 Figure 15: Tooth 1. Location B. T1. 250X Magnification. Figure 16: Tooth 3. Location B. T2. 250X Magnification. Figure 17: Tooth 6. Location B. T1. 250X Magnification. 25
35 Studies have also shown an increased tendency for infiltrative resin to stain over time The roughness, microcracks, and fractures found at the surface of the teeth offer possible explanations for why the staining occurs. Rougher surfaces provide more areas for highly staining pigments to leak into and/or become trapped within. 34 Polishing would thus remove the discoloration, as was corroborated by the results of the study by Leland et al., 24 where esthetics was improved when staining from coffee and wine were eliminated by pumice polishing of the tooth surface. In this study, the use of variable pressure SEM as a microscopic technique allowed for evaluation of the infiltrative resin with minimal manipulation or alteration at the tooth surface. SEM with variable pressure enables imaging of non-conductive material such as teeth by lowering the pressure within the gas chamber until artefacts created from electron charging are no longer present, thus eliminating the need for a conductive coating. This technique is particularly useful for biological samples as they can be viewed in their natural state, without the addition of a conductive material coating added to the surface as is typical with conventional SEM. One of the compromises of using a variable pressure SEM, however, is the possibility of artefact creation from contamination of images with material of higher or lower conductive potential than the material of interest. While contamination was generally not found to be present in the samples, there were a few isolated images where this was noted as areas of either excessively light or dark streaks of unknown material. Additionally, while low vacuum imaging is not quite as high in resolution as conventional SEM, it was found to be sufficient for the current study to achieve high quality imaging at 250X. 26
36 An additional unavoidable limitation of variable pressure SEM is the time required outside of liquid. All teeth in the study required mounting on pegs for placement within the imaging chamber, and since variable pressure SEM is a slower microscopy technique, this can result in high degrees of desiccation of samples. While teeth in the samples were stored in distilled water between all other experimental steps, it is possible that changes in the surface structure could have occurred during the time required for imaging. Specifically, enamel has a higher modulus of elasticity than dentin, and thus when dentin desiccation and shrinkage occurs, the fragile enamel prisms are sometimes found to crack at the enamel surface from tensile stresses. 32,35 Because some microcracks were found to be present on the surfaces of baseline teeth A-D (although typically in smaller numbers), this was taken into consideration as a possible etiology of enamel microcracks in all images. A recent study by Arnold et al. 31 investigated the effects of 15% HCl on enamel. Over a course of 2 minutes, this etchant was found to remove an average of 34 microns of enamel. Two rounds of two minutes of etching time, which is the recommended protocol for infiltrative resin, increased enamel removal further microns. In vivo, the double etching is often necessary to remove the hardened outer layer of enamel which is created by salivary remineralization at the enamel surface. 36 However, since in our pilot study the double application of etchant resulted in complete removal of the WSL, in the current study the samples were subjected to only a single two-minute application of 15% HCl. While it could be argued that the etching process recommended for resin infiltration removes a significant layer of enamel in the process, Meyer- Lueckel et al. 36 noted that the procedure still removes far less enamel than other treatments such as veneers or microabrasion, which can remove as much as 360 microns of enamel
37 There were some limitations to note with the design of this study. The in-vitro creation of white spot lesions, storage conditions, and simulated daily challenges have inherent differences compared to teeth in vivo. For example, it is known that WSLs in vivo often tend to be deeper, more longstanding, and may have a hardened surface layer from remineralization in the oral environment, which can be difficult to remove with etching procedures A recently published study by Zhao et al. 37 which investigated both the effect of toothbrush abrasion (600 strokes total) and acidic challenge with orange juice, found material loss via profilometry to average 24.6 microns. Furthermore, in that study the Icon layer was shown to be completely removed with acid and mechanical abrasion. Thus, additional challenges such as acid and bacterial presence could cause differences in how infiltrative resin behaves over time. Prior studies investigating the extent of demineralization have shown a wide range in depth of infiltration by TEGDMA based infiltrative resins, from 15.7 microns to over 400 microns in others in vitro. 37,38 Belli et al. 26 investigated vertical loss of infiltrated enamel in bovine teeth, and found an average loss of 42.6 microns of resin-enamel structure following 20,000 toothbrush abrasion cycles. Evaluating the depth of penetration would not have been feasible in this SEM study, since sectioning of the samples would be required to evaluate depth penetration. In this case, it would not have been possible to evaluate the tooth surfaces at the second time point of the toothbrushing simulation procedures. Ideally, atomic force microscopy to measure microscopic surface roughness and/or a Vicker s hardness test would have been useful additional quantitative information to characterize the behavior of Icon over time. However, both of these methods would require a virtually flat surface to be accurate. It is possible that flat enamel discs could be created for infiltrative resin application; however, this preparation would require removal of the surface layer of enamel, 28
38 which is typically found to be more fluoride-rich than the underneath layers due to presence of fluoride available in the mouth. Therefore, it should be kept in mind that enamel prepared into a slab may behave differently than enamel on the natural tooth surfaces. To date, this is the first study to fully evaluate the microstructural changes of an infiltrative resin applied to WSLs in human teeth over time when challenged with toothbrush abrasion. Future studies with larger sample size, longer duration and conditions more closely approximating that of the natural oral environment are needed to investigate the cause of enamelresin gap formation after resin application and the wear of this material over time. 29
39 Conclusions 1) After six months of simulated toothbrushing on enamel surfaces with WSLs coated with resin infiltrate, there were microstructural changes in enamel rods, microcracks, and fractures, but overall differences were not statistically significant. 2) An increase in incidence of fractures and microcracks was positively correlated with a thicker surface layer of resin infiltrate. 3) Failure to remove the residual surface layer of infiltrative resin prior to light-curing may result in higher fractures and gap formation within the resin due to polymerization shrinkage. 4) Due to the qualitative surface changes after 6 months of simulated toothbrushing, additional application of resin may be indicated over time. 30
40 Literature Cited 31
41 Literature Cited (1) Taher NM, Alkhamis HA, Dowaidi SM. The influence of resin infiltration system on enamel microhardness and surface roughness: An in vitro study. Saudi Dent J. 2012;24(2): (2) Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013;83(4): (3) Tufekci E, Dixon JS, Gunsolley JC, Lindauer SJ. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 2011;81(2): (4) Gorelick L, Geiger AM, Gwinnet AJ. Incidence of white spot formation after bonding and banding. Am J Orthod.1982;81: (5) Sundararaj D, Venkatachalapathy S, Tandon A, Pereira A. Critical evaluation of incidence and prevalence of white spot lesions during fixed orthodontic appliance treatment: A metaanalysis. J of Int Soc of Prev Community Dent.2015;5(6): (6) Maxfield BJ, Hamdan AM, Tüfekçi E, Shroff B, Best AM, Lindauer SJ. Development of white spot lesions during orthodontic treatment: perceptions of patients, parents, orthodontists, and general dentists. Am J Orthod Dentofacial Orthop. 2012;141(3): (7) Griffin SO, Regnier E, Griffin PM, Huntley V. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007;86(5): (8) Ogaard B, Rølla G, Arends J, ten Cate JM. Orthodontic appliances and enamel demineralization. Part 2. Prevention and treatment of lesions. Am J Orth Dentofacial Orthop. 1988;94(2): (9) Ogaard B. The cariostatic mechanism of fluoride. Compend Contin Educ Dent. 1999; 20(1 Suppl):10 7. (10) Zantner C, Martus P, Kielbassa AM. Clinical monitoring of the effect of fluorides on longexisting white spot lesions. Acta Odontol Scandinavica. 2006;64(2): (11) Senestraro SV, Crowe JJ, Wang M, Vo A, Huang G, Ferracane J, Covell DA Jr. Minimally invasive resin infiltration of arrested white-spot lesions: a randomized clinical trial. J Am Dent Assoc. 2013;144(9):
42 (12) Borges AB, Caneppele TMF, Masterson D, Maia LC. Is resin infiltration an effective esthetic treatment for enamel development defects and white spot lesions? A systematic review. J Dent (1): (13) Arnold WH, Gaengler P. Light- and electronmicroscopic study of infiltration of resin into initial caries lesions - a new methodological approach. J Microcs. 2011;245(1): (14) Askar H, Lausch J, Dörfer CE, Meyer-Lueckel H, Paris S. Penetration of micro-filled infiltrant resins into artificial caries lesions. J Dent. 2015;43(7): (15) Paris S, Meyer-Lueckel H. Inhibition of caries progression by resin infiltration in situ. Caries Res. 2010;44(1): (16) Paris S, Meyer-Leuckel H, Colfen H, Kielbassa AM. Resin infiltration of artificial enamel caries lesions with experimental light curing resins. Dent Mater J. 2007;26(4): (17) Robinson C, Brookes SJ, Kirkham J, Wood SR, Shore RC. In vitro studies of the penetration of adhesive resins into artifical caries-like lesions. Caries Res. 2001;35(2): (18) Paris S, Schwendicke F, Seddig S, Müller WD, Dörfer C, Meyer-Lueckel H. Microhardness and mineral loss of enamel lesions after infiltration with various resins: influence of infiltrant composition and application frequency in vitro. J Dent. 2013;41(6): (19) Van Meerbeek B, Willems G, Celis JP, Roos JR, Braem M, Lambrechts P, Vanherle G. Assessment by nano-indentation of the hardness and elasticity of the resin-dentin bonding area. J Dent Res. 1993;72(10): (20) Watts DC, McNaughton V, Grant AA. The development of surface hardness in visible lightcured posterior composites. J Dent. 1986;14(4): (21) Araújo G, Naufel FS, Alonso RC, Lima DA, Puppin-Rontani RM. Influence of Staining Solution and Bleaching on Color Stability of Resin Used for Caries Infiltration. Oper Dent. 2105;40(6):E (22) Borges A, Caneppele T, Luz M, Pucci C, Torres C. Color stability of resin used for caries infiltration after exposure to different staining solutions. Oper Dent. 2014;39(4): (23) Cohen Carneiro F, Pascareli AM, Christino MR, Vale HF, Pontes DG. Color stability of carious incipient lesions located in enamel and treated with resin infiltration or remineralization. Int J Paediatric Dent. 2014;24(4): (24) Leland A, Akyalcin S, English JD, Tufekci E, Paravina R. Evaluation of staining and color changes of a resin infiltration system. Angle Orthod. 2016; 86(6):
43 (25) Yetkiner E, Wegehaupt FJ, Attin R, Wiegand A, Attin T. Stability of two resin combinations used as sealants against toothbrush abrasion and acid challenge in vitro. Acta Odontol Scand. 2014;72(8): (26) Belli R, Rahiotis C, Schubert EW, Baratieri LN, Petschelt A, Lohbauer U. Wear and morphology of infiltrated white spot lesions. J Dent. 2011;39(5): (27) Kumar VL, Itthagarun A, King NM. The effect of casein phosphopeptide-amorphous calcium phosphate on remineralization of artificial caries-like lesions: An in vitro study. Aust Dent J. 2008;53: (28) Hu W, Featherstone JD. Prevention of enamel demineralization: an in-vitro study using light-cured filled sealant. Am J Orthod Dentofacial Orthop. 2005;128(5): (29) Xie ZH, Mahoney EK, Kilpatrick NM, Swain MV, Hoffman M. On the structure-property relationship of sound and hypomineralized enamel. Acta Biomaterial. 2007;3(6): (30) Mueller J, Yang F, Neumann K, Kielbassa AM. Surface tridimensional topography analysis of materials and finishing procedures after resinous infiltration of subsurface bovine enamel lesions. Quintessence Int. 2011;42(2): (31) Arnold WH, Haddad B, Schaper K, Hagemann K, Lippold C, Danesh GH. Enamel surface alterations after repeated conditioning with HCl. Head Face Med. 2015;25(11):32. (32) Yoshikawa T, Morigami M, Sadr A, Tagami J. Environmental SEM and dye penetration observation on resin-tooth interface using different light curing method. Dent Mater J. 2016;35(1): (33) Tereza GP, de Oliveira GC, de Andrade Moreira Machado MA, de Oliveira TM, da Silva TC, Rios D. Influence of removing excess of resin-based materials applied to eroded enamel on the resistance to erosive challenge. J Dent. 2016;47(4): (34) Mair LH. Surface permeability and degradation of dental composites resulting from oral temperature changes. Dent Mater. 1989;5(4): (35) Ikeda T, Uno S, Tanaka T, Kawakami S, Komatsu H, & Sano H. Relation of enamel prism orientation to microtensile bond strength. Am J Orthod Dentofacial Orthop, 2002;15(2), (36) Meyer-Lueckel H, Paris S, Kielbassa AM. Surface layer erosion of natural caries lesions with phosphoric and hydrochloric acid gels in preparation for resin infiltration. Caries Res. 2007;41(3): (37) Zhao, X., Pan, J., Zhang, S. et al. Effectiveness of resin-based materials against erosive and abrasive enamel wear. Clin Oral Investig 2017;21(1):
44 (38) Meyer-Lueckel H, Paris S. Infiltration of Natural Caries Lesions with Experimental Resins Differing in Penetration Coefficients and Ethanol Addition. Caries Res. 2010;44(4):
45 Appendix: SEM Images of Extracted Teeth 36




46 Tooth 1, T1 Location A 250X 500X Location B Location C 37





47 Tooth 1, T2 Location A 250X 500X Location B Location C 38




48 Tooth 2, T1 Location A 250X 500X Location B Location C 39






49 Tooth 2, T2 Location A 250X 500X Location B Location C 40





50 Tooth 3, T1 Location A 250X 500X Location B Location C 41






51 Tooth 3, T2 Location A 250X 500X Location B Location C 42





52 Tooth 4, T1 Location A 250X 500X Location B Location C 43




53 Tooth 4, T2 Location A 250X 500X Location B Location C 44






54 Tooth 5, T1 Location A 250X 500X Location B Location C 45






55 Tooth 5, T2 Location A 250X 500X Location B Location C 46






56 Tooth 6, T1 Location A 250X 500X Location B Location C 47





57 Tooth 6, T2 Location A 250X 500X Location B Location C 48





58 Tooth 7, T1 Location A 250X 500X Location B Location C 49





59 Tooth 7, T2 Location A 250X 500X Location B Location C 50





60 Tooth 8, T1 Location A 250X 500X Location B Location C 51



61 Tooth 8, T2 Location A 250X 500X Location B Location C 52





62 Tooth 9, T1 Location A 250X 500X Location B Location C 53






63 Tooth 9, T2 Location A 250X 500X Location B Location C 54






64 Tooth 10, T1 Location A 250X 500X Location B Location C 55





65 Tooth 10, T2 Location A 250X 500X Location B Location C 56

66 Control A: Sound Enamel 250X 500X 57


67 Control B: Sound Enamel 250X 500X 58


68 Control C: Demineralized Enamel 250X 500X 59


69 Control D: Demineralized Enamel 250X 500X 60
70 Vita Danielle Elizabeth Easterly was born on September 27, 1988 in Fairfax, Virginia. She is currently a citizen of the United States of America. After attending the University of Virginia and receiving a B.A. in Psychology with a minor in Biology in 2010, Dr. Easterly went on to continue her dental education at Virginia Commonwealth University. She earned her Doctorate of Dental Surgery in She is currently enrolled as a resident in the Virginia Commonwealth University Department of Orthodontics. 61
Different Stains, Different Treatment
 Different Stains, Different Treatment Samah Omar DDS, MSD Pediatric Dentistry Department Loma Linda University somar@llu.edu Treatment Options Bleaching Resin Infiltration Microabrasion Tooth colored
Different Stains, Different Treatment Samah Omar DDS, MSD Pediatric Dentistry Department Loma Linda University somar@llu.edu Treatment Options Bleaching Resin Infiltration Microabrasion Tooth colored
EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE
 EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE Monisha Singhal PG STUDENT DEPARTMENT OF PEDODONTICS & PREVENTIVE DENTISTRY CHANDRA DENTAL COLLEGE & HOSPITAL
EVALUATION OF COLOR CHANGE IN WHITE SPOT LESIONS OF ENAMEL FLUOROSIS USING A RESIN INFILTRATE Monisha Singhal PG STUDENT DEPARTMENT OF PEDODONTICS & PREVENTIVE DENTISTRY CHANDRA DENTAL COLLEGE & HOSPITAL
OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH
 ISSN: 1312-773X (Online) Journal of IMAB - Annual Proceeding (Scientific Papers) 2006, vol. 12, issue 2 OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH Snezhanka Topalova-Pirinska,
ISSN: 1312-773X (Online) Journal of IMAB - Annual Proceeding (Scientific Papers) 2006, vol. 12, issue 2 OUR EXPERIENCE WITH GRADIA DIRECT IN THE RESTORATION OF ANTERIOR TEETH Snezhanka Topalova-Pirinska,
MICRO-INVASIVE TREATMENT OF THE NON-CAVITATED CARIOUS LESIONS IN THE SMOOTH SURFACES OF TEETH
 Odontology MICRO-INVASIVE TREATMENT OF THE NON-CAVITATED CARIOUS LESIONS IN THE SMOOTH SURFACES OF TEETH Luiza Ungureanu 1, Albertine Leon 2, Anca Nicolae 3, Ciobanu Gabriela 4 1. Prof. PhD, Dept of Odontology,
Odontology MICRO-INVASIVE TREATMENT OF THE NON-CAVITATED CARIOUS LESIONS IN THE SMOOTH SURFACES OF TEETH Luiza Ungureanu 1, Albertine Leon 2, Anca Nicolae 3, Ciobanu Gabriela 4 1. Prof. PhD, Dept of Odontology,
2 during treatment... how to technique. How to handle white spot lesions associated with orthodontic treatment. Issue
 Issue 17 2013 How to handle white spot lesions associated with orthodontic treatment. 1 background... It is well recognised that the placement of fixed orthodontic appliances increases a patient s risk
Issue 17 2013 How to handle white spot lesions associated with orthodontic treatment. 1 background... It is well recognised that the placement of fixed orthodontic appliances increases a patient s risk
Is there any clinical evidence?
 Current treatment objectives Anticariogenic capacity of restorative materials in paediatric dentistry: in vitro evidence vs. clinical efficiency Prof. Lisa Papagianoulis Restoration with minimal intervention
Current treatment objectives Anticariogenic capacity of restorative materials in paediatric dentistry: in vitro evidence vs. clinical efficiency Prof. Lisa Papagianoulis Restoration with minimal intervention
Adper Easy Bond. Self-Etch Adhesive. Technical Product Profile
 Adper Easy Bond Self-Etch Adhesive Technical Product Profile Table of Contents Table of Contents Introduction... 4 Product Description... 4 Composition...5-8 Background... 5 Mechanism of Adhesion to Enamel
Adper Easy Bond Self-Etch Adhesive Technical Product Profile Table of Contents Table of Contents Introduction... 4 Product Description... 4 Composition...5-8 Background... 5 Mechanism of Adhesion to Enamel
DH220 Dental Materials
 DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
DH220 Dental Materials Lecture #5 Prof. Lamanna RDH, MS Restorative Dentistry: Glass Ionomer Bird & Robinson p.740-741 I. Use Liner Base Luting agent Restorative material: Class III, V, & eroded/abraded
JODE ABSTRACT INTRODUCTION /jp-journals
 A Arvindkumar et al ORIGINAL ARTICLE 10.5005/jp-journals-10047-0025 Caries-preventive Efficacy of Resin Infiltrant, Casein Phosphopeptide-amorphous Calcium Phosphate, and Nanohydroxyapatite using Confocal
A Arvindkumar et al ORIGINAL ARTICLE 10.5005/jp-journals-10047-0025 Caries-preventive Efficacy of Resin Infiltrant, Casein Phosphopeptide-amorphous Calcium Phosphate, and Nanohydroxyapatite using Confocal
MDJ Evaluation the effect of eugenol containing temporary Vol.:9 No.:2 2012
 MDJ Evaluation the effect of eugenol containing temporary fillings on shear bond strength of composite restoration Dr. Farid G. Numan B.D.S., M.Sc Abstract The purpose of this in-vitro study was to evaluate
MDJ Evaluation the effect of eugenol containing temporary fillings on shear bond strength of composite restoration Dr. Farid G. Numan B.D.S., M.Sc Abstract The purpose of this in-vitro study was to evaluate
Linking Research to Clinical Practice
 Prevention of Root Caries Denise M. Bowen, RDH, MS Linking Research to Clinical Practice The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical dental
Prevention of Root Caries Denise M. Bowen, RDH, MS Linking Research to Clinical Practice The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical dental
BioCoat Featuring SmartCap Technology
 new! BioCoat Featuring SmartCap Technology Premier s new bioactive pit and fissure sealant provides relentless protection, outstanding adhesion and extended fluoride release. Bioactive Release - Uptake
new! BioCoat Featuring SmartCap Technology Premier s new bioactive pit and fissure sealant provides relentless protection, outstanding adhesion and extended fluoride release. Bioactive Release - Uptake
Modification of surface pretreatment of white spot lesions to improve the safety and efficacy of resin infiltration
 Original Article THE KOREAN JOURNAL of ORTHODONTICS pissn 2234-7518 eissn 2005-372X http://dx.doi.org/10.4041/kjod.2014.44.4.195 Modification of surface pretreatment of white spot lesions to improve the
Original Article THE KOREAN JOURNAL of ORTHODONTICS pissn 2234-7518 eissn 2005-372X http://dx.doi.org/10.4041/kjod.2014.44.4.195 Modification of surface pretreatment of white spot lesions to improve the
The Effects of the Acid Etch and Direct Bonding Technique in Orthodontics on Enamel Surface Topography
 J. Dent. Ass. S. Afr. Vol. 31, No 10 pp 509-513 The Effects of the Acid Etch and Direct Bonding Technique in Orthodontics on Enamel Surface Topography P L Sadowsky and D H Retief Department of Orthodontics,
J. Dent. Ass. S. Afr. Vol. 31, No 10 pp 509-513 The Effects of the Acid Etch and Direct Bonding Technique in Orthodontics on Enamel Surface Topography P L Sadowsky and D H Retief Department of Orthodontics,
Fuji II LC. A Perfect Choice
 A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
A Perfect Choice is a remarkable restorative material The world s first resin-reinforced glass ionomer has remained the benchmark for light cured glass ionomer cements, delivering more than 15 years of
Scanning electron microscope characterization of abrasion in human teeth
 Dental Journal Mahidol Dental Journal Original Article Scanning electron microscope characterization of abrasion in human teeth B.Sc., D.D.S., Specialty Certificate in Oral Pathology, M.S. Department of
Dental Journal Mahidol Dental Journal Original Article Scanning electron microscope characterization of abrasion in human teeth B.Sc., D.D.S., Specialty Certificate in Oral Pathology, M.S. Department of
stabilisation and surface protection
 Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
Guiding the way to caries stabilisation and surface protection Fissure sealing MI restorations Pulp capping Hypersensitivity Protection Caries stabilisation Fuji Triage from GC. Temporary restorations
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials
 Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
Direct composite restorations for large posterior cavities extended range of applications for high-performance materials A case study by Ann-Christin Meier, Dr. med. dent., Stapelfeld, Germany When large
White lesion eradication using resin infiltration
 Clinical White lesion eradication using resin infiltration Linda Greenwall Introduction White marks and white lesions on anterior teeth can be unsightly. Patients often seek treatment to have these marks
Clinical White lesion eradication using resin infiltration Linda Greenwall Introduction White marks and white lesions on anterior teeth can be unsightly. Patients often seek treatment to have these marks
G-COAT PLUS G-COAT PLUS GET THE BEST OF BOTH WORLDS WITH THE STROKE OF A BRUSH
 G-COAT PLUS BEAUTY BRAWN GET THE BEST OF BOTH WORLDS WITH THE STROKE OF A BRUSH 1 Introducing a Revolutionary new Coating G-COAT PLUS gives your restorations the Best of Both Worlds: A beautiful new finish
G-COAT PLUS BEAUTY BRAWN GET THE BEST OF BOTH WORLDS WITH THE STROKE OF A BRUSH 1 Introducing a Revolutionary new Coating G-COAT PLUS gives your restorations the Best of Both Worlds: A beautiful new finish
BioCoat Featuring SmartCap Technology
 R R Breakthrough! BioCoat Featuring SmartCap Technology The only bioactive pit and fissure sealant that provides relentless protection through daily release of fluoride, calcium and phosphate ions. Bioactive
R R Breakthrough! BioCoat Featuring SmartCap Technology The only bioactive pit and fissure sealant that provides relentless protection through daily release of fluoride, calcium and phosphate ions. Bioactive
OliNano Seal Professional prophylaxis for long-term protection
 Professional prophylaxis for long-term protection NEW The patented formula of silicone polymer NANO Technology General information Dental health is one of the main factors to maintain overall health, and
Professional prophylaxis for long-term protection NEW The patented formula of silicone polymer NANO Technology General information Dental health is one of the main factors to maintain overall health, and
EQUIA. Self-Adhesive, Bulk Fill, Rapid Restorative System
 EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
EQUIA EQUIA Fil EQUIA Coat + Self-Adhesive, Bulk Fill, Rapid Restorative System From the World Leader in Glass Ionomer Technology - A Complete Glass Ionomer Based Bulk Fill Rapid Restorative System Class
Active Care - Silver Members Minimally invasive treatment of enamel fluorosis white spot lesions
 Marie Clement Active Care - Silver Members Minimally invasive treatment of enamel fluorosis white spot lesions 31 Aug 2017 A young woman presented in the dental office with a primary complaint of the presence
Marie Clement Active Care - Silver Members Minimally invasive treatment of enamel fluorosis white spot lesions 31 Aug 2017 A young woman presented in the dental office with a primary complaint of the presence
how to technique Issue How to improve the longevity of porcelain veneers.
 Issue 4 2013 How to improve the longevity of porcelain veneers. 1. Avoid finishing on a resin composite restoration. longer term weak spot Although tempting in the interests of minimal tooth removal, finishing
Issue 4 2013 How to improve the longevity of porcelain veneers. 1. Avoid finishing on a resin composite restoration. longer term weak spot Although tempting in the interests of minimal tooth removal, finishing
RelyX Unicem Self-Adhesive Universal Resin Cement Frequently Asked Questions
 RelyX Unicem Self-Adhesive Universal Resin Cement Frequently Asked Questions Q1. What about the clinical history of The first restorations were cemented with RelyX Unicem cement in 2001. The excellent
RelyX Unicem Self-Adhesive Universal Resin Cement Frequently Asked Questions Q1. What about the clinical history of The first restorations were cemented with RelyX Unicem cement in 2001. The excellent
3M Fast Release Varnish
 3M Fast Release Varnish 5% Sodium Fluoride Varnish Fast Release Formula Technical Data Sheet 2 3M Fast Release Varnish 3M Fast Release Varnish is a fluoride-containing varnish. It can be applied to enamel
3M Fast Release Varnish 5% Sodium Fluoride Varnish Fast Release Formula Technical Data Sheet 2 3M Fast Release Varnish 3M Fast Release Varnish is a fluoride-containing varnish. It can be applied to enamel
Bond strengths between composite resin and auto cure glass ionomer cement using the co-cure technique
 SCIENTIFIC ARTICLE Australian Dental Journal 2006;51:(2):175-179 Bond strengths between composite resin and auto cure glass ionomer cement using the co-cure technique GM Knight,* JM McIntyre,* Mulyani*
SCIENTIFIC ARTICLE Australian Dental Journal 2006;51:(2):175-179 Bond strengths between composite resin and auto cure glass ionomer cement using the co-cure technique GM Knight,* JM McIntyre,* Mulyani*
Treatment of Post-Orthodontic whitespot Lesions By Resin Infiltration
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. I (Nov. 2017), PP 80-84 www.iosrjournals.org Treatment of Post-Orthodontic whitespot
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. I (Nov. 2017), PP 80-84 www.iosrjournals.org Treatment of Post-Orthodontic whitespot
values is of great interest.
 User Report Dr. Ralph Schönemann, May 21, 2008 There are numerous self-etchbonding systems on the market that sometimes differ very much from one another with regards to their chemical composition. It
User Report Dr. Ralph Schönemann, May 21, 2008 There are numerous self-etchbonding systems on the market that sometimes differ very much from one another with regards to their chemical composition. It
Ketac Universal Aplicap
 Ketac Universal Aplicap Technical Data Sheet 2 Introduction Ketac Universal Aplicap is the latest development in a long history of proven glass ionomer technology from 3M. It s designed to save steps for
Ketac Universal Aplicap Technical Data Sheet 2 Introduction Ketac Universal Aplicap is the latest development in a long history of proven glass ionomer technology from 3M. It s designed to save steps for
lec: Dental material dr. Aseel Mohammed Filling material
 Filling material Filling material: the material that is used to replace a missing part of the tooth which may result from dental caries, trauma or abrasion. It can be divided in to: 1. Direct filling materials:
Filling material Filling material: the material that is used to replace a missing part of the tooth which may result from dental caries, trauma or abrasion. It can be divided in to: 1. Direct filling materials:
A Step-by-Step Approach to
 A Step-by-Step Approach to a Diastema Closure A Dual-Purpose Technique that Manages Black Triangles Marcos Vargas, DDS, MS Figure 1: Preoperative view of a patient who presented with a diastema between
A Step-by-Step Approach to a Diastema Closure A Dual-Purpose Technique that Manages Black Triangles Marcos Vargas, DDS, MS Figure 1: Preoperative view of a patient who presented with a diastema between
Clinical report. Drs Paul and Alexandre MIARA and F. CONNOLLY COMPOSITE POSTERIOR FILLINGS. How to control. layering? 8 - Dentoscope n 124
 COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
COMPOSITE POSTERIOR FILLINGS How to control layering? 8 - Dentoscope n 124 CV FLASH Dr Paul MIARA Dental surgeon Dr Alexandre MIARA Dental surgeon Dr F. CONNOLLY Dental surgeon Thanks to continuous improvements
PREVALENCE OF WHITE SPOT LESIONS DURING THE PROCEDURE OF FIXED ORTHODONTIC TREATMENT
 Original Article Received : 18 04 15 Review completed : 24 05 15 Accepted : 30 05 15 PREVALENCE OF WHITE SPOT LESIONS DURING THE PROCEDURE OF FIXED ORTHODONTIC TREATMENT Saibel Farishta, * Saurabh Sharma,
Original Article Received : 18 04 15 Review completed : 24 05 15 Accepted : 30 05 15 PREVALENCE OF WHITE SPOT LESIONS DURING THE PROCEDURE OF FIXED ORTHODONTIC TREATMENT Saibel Farishta, * Saurabh Sharma,
5,6 Significant improvements of the dentin bond
 Porcelain Jacket Crowns: Back to the Future Through Bonding Pascal Magne, PhD, DMD 1 Michel Magne, MDT, BS 2 Inge Magne, CDT 2 More than 50 years before bonding to tooth structure (and especially to dentin)
Porcelain Jacket Crowns: Back to the Future Through Bonding Pascal Magne, PhD, DMD 1 Michel Magne, MDT, BS 2 Inge Magne, CDT 2 More than 50 years before bonding to tooth structure (and especially to dentin)
Occlusal Surface Management
 Occlusal Surface Management Sealant With Fluoride? Preventive Class I Resin Restoration Class I Glass Ionomer Primary Teeth Class I Composite Class I Amalgam PIT and FISSURE SEALANTS Contraindications
Occlusal Surface Management Sealant With Fluoride? Preventive Class I Resin Restoration Class I Glass Ionomer Primary Teeth Class I Composite Class I Amalgam PIT and FISSURE SEALANTS Contraindications
QuickPro. Instructions for use
 QuickPro Instructions for use Step 1 Step 2 Step 3 Step 4 Step 5 2 Step 6 Step 7 Step 8 Step 9 Step 10 3 Symbols used in labeling Irritant Irritant Consult instruction manual for use Batch code REF Catalog
QuickPro Instructions for use Step 1 Step 2 Step 3 Step 4 Step 5 2 Step 6 Step 7 Step 8 Step 9 Step 10 3 Symbols used in labeling Irritant Irritant Consult instruction manual for use Batch code REF Catalog
TOOTH DISCOLORATION. Multimedia Health Education. Disclaimer
 Disclaimer This movie is an educational resource only and should not be used to manage dental health. All decisions about the management of tooth discoloration must be made in conjunction with your dentist
Disclaimer This movie is an educational resource only and should not be used to manage dental health. All decisions about the management of tooth discoloration must be made in conjunction with your dentist
Management of ECC and Minimally Invasive Dentistry
 Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Management of ECC and Minimally Invasive Dentistry Ranbir Singh DMD MPH NYU-Lutheran Phoenix Pgy1 Pediatric Dental Resident Phoenix ECC Management Management of dental caries includes identification of
Near-UV light detection
 C L I N I C A L Near-UV light detection Javier Tapia Guadix 1 Near-UV light induced fluorescence has already proven to be very useful as an alternative to classic caries-detector dyes. However its potential
C L I N I C A L Near-UV light detection Javier Tapia Guadix 1 Near-UV light induced fluorescence has already proven to be very useful as an alternative to classic caries-detector dyes. However its potential
Restorative Resin Cement for Bonding and Masking Tetracycline and Dark Stained Teeth for All Veneers
 Restorative Resin Cement for Bonding and Masking Tetracycline and Dark Stained Teeth for All Veneers Store Under Refrigeration Block-Out by Ultra-Bond is a multi-purpose, photo-initiated, dual-cure, restorative
Restorative Resin Cement for Bonding and Masking Tetracycline and Dark Stained Teeth for All Veneers Store Under Refrigeration Block-Out by Ultra-Bond is a multi-purpose, photo-initiated, dual-cure, restorative
riva helping you help your patients
 riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
riva helping you help your patients what is a glass ionomer? how will a dentist benefit from using glass ionomers? how will a patient benefit from their glass ionomer? Glass ionomer is the generic name
Breakthrough Performance
 Technique Guide How to get Breakthrough Performance using TM Adper TM Prompt Self-Etch Adhesive ILLUSTRATED INSIDE: How to properly activate the L-Pop Applicator Direct light-cure restoration Sealing pits
Technique Guide How to get Breakthrough Performance using TM Adper TM Prompt Self-Etch Adhesive ILLUSTRATED INSIDE: How to properly activate the L-Pop Applicator Direct light-cure restoration Sealing pits
For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Matrix
 Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
Cronicon OPEN ACCESS EC DENTAL SCIENCE Case Report For the Perfect Class V and All Cervical Area Gingival Margins when Placing Direct Composites, Create an Injection Molding Paul C Belvedere* Adjunct Professor,
Dental erosion: In vitro model of wine assessor s erosion
 ADRF REPORT Australian Dental Journal 21;46:(4):263-268 Dental erosion: In vitro model of wine assessor s erosion Tong Bee Mok,* J McIntyre,* D Hunt* Abstract Background: Wine makers and assessors frequently
ADRF REPORT Australian Dental Journal 21;46:(4):263-268 Dental erosion: In vitro model of wine assessor s erosion Tong Bee Mok,* J McIntyre,* D Hunt* Abstract Background: Wine makers and assessors frequently
Shadeguides Ceramic Veneers: Tooth Preparation for Enamel Preservation
 Ajay Juneja Shadeguides Ceramic Veneers: Tooth Preparation for Enamel Preservation 1 Feb 2016 The rationale of having minimal preparation and having ceramic veneers cemented to enamel in order for the
Ajay Juneja Shadeguides Ceramic Veneers: Tooth Preparation for Enamel Preservation 1 Feb 2016 The rationale of having minimal preparation and having ceramic veneers cemented to enamel in order for the
Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease
 Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease Dental Caries The current understanding of the caries process supports the shift in caries management from a restorative-only
Examination and Treatment Protocols for Dental Caries and Inflammatory Periodontal Disease Dental Caries The current understanding of the caries process supports the shift in caries management from a restorative-only
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS
 FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS FIVE THINGS YOU NEED TO KNOW ABOUT GLASS IONOMERS Glass Ionomers Solve Clinicians Quandaries Amalgam fillings have been around for almost two centuries,
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations The outline form
 Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Adhesive performance of a caries infiltrant on sound and demineralised enamel
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2011 Adhesive performance of a caries infiltrant on sound and demineralised
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2011 Adhesive performance of a caries infiltrant on sound and demineralised
SCIENTIFIC. Effects of various acids on the buccal surface of human permanent teeth: a study using scanning electron microscopy*
 PEDIATRIC DENTISTRY/Copyright 1979 by The American Academy o! Pedodontics/VoL 1, No. 3/Printed in U.S.A. SCIENTIFIC Effects of various acids on the buccal surface of human permanent teeth: a study using
PEDIATRIC DENTISTRY/Copyright 1979 by The American Academy o! Pedodontics/VoL 1, No. 3/Printed in U.S.A. SCIENTIFIC Effects of various acids on the buccal surface of human permanent teeth: a study using
EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY : A RANDOMIZED CLINICAL TRIAL
 Original Article International Journal of Dental and Health Sciences Volume 01,Issue 02 EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY
Original Article International Journal of Dental and Health Sciences Volume 01,Issue 02 EFFICACY OF AMORPHOUS CALCIUM PHOSPHATE, G.C. TOOTH MOUSSE AND GLUMA DESENSITIZER IN TREATING DENTIN HYPERSENSITIVITY
Patient demand for esthetic dentistry
 PROFILE Masters of Esthetic Dentistry Keys to Success in Creating Esthetic Class IV Restorations Robert C. Margeas, DDS Current occupation Private Practice Adjunct Professor, Department of Operative Dentistry,
PROFILE Masters of Esthetic Dentistry Keys to Success in Creating Esthetic Class IV Restorations Robert C. Margeas, DDS Current occupation Private Practice Adjunct Professor, Department of Operative Dentistry,
Pulpal Protection: bases, liners, sealers, caries control Module C: Clinical applications
 Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module C: Clinical applications REST 528A Operative
Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module C: Clinical applications REST 528A Operative
Colourf low. light cured dental flowable composite
 Colourf low light cured dental flowable composite DENTAL LIFE SCIENCES (mfg) Ltd. Unit A3, Wigan Enterprise Court, Wigan Enterprise Park, WN2 2LE United Kingdom www.dentallifesciences.com Colourf low flowable
Colourf low light cured dental flowable composite DENTAL LIFE SCIENCES (mfg) Ltd. Unit A3, Wigan Enterprise Court, Wigan Enterprise Park, WN2 2LE United Kingdom www.dentallifesciences.com Colourf low flowable
Anisotropy of Tensile Strengths of Bovine Dentin Regarding Dentinal Tubule Orientation and Location
 Original paper Dental Materials Journal 21 (1): 32-43, 2002 Anisotropy of Tensile Strengths of Bovine Dentin Regarding Dentinal Tubule Orientation and Location Toshiko INOUE, Hidekazu TAKAHASHI and Fumio
Original paper Dental Materials Journal 21 (1): 32-43, 2002 Anisotropy of Tensile Strengths of Bovine Dentin Regarding Dentinal Tubule Orientation and Location Toshiko INOUE, Hidekazu TAKAHASHI and Fumio
Influence of Bioactive Materials on Whitened Human Enamel Surface in vitro study
 Influence of Bioactive Materials on Whitened Human Enamel Surface Influence of Bioactive Materials on Whitened Human Enamel Surface in vitro study Pinheiro HB, Cardoso PEC, Universidade de São Paulo, São
Influence of Bioactive Materials on Whitened Human Enamel Surface Influence of Bioactive Materials on Whitened Human Enamel Surface in vitro study Pinheiro HB, Cardoso PEC, Universidade de São Paulo, São
The Effect of Mineralizing Fluorine Varnish on the Progression of Initial Caries of Enamel in Temporary Dentition by Laser Fluorescence
 American Journal of Engineering Research (AJER) e-issn: 2320-0847 p-issn : 2320-0936 Volume-6, Issue-9, pp-39-43 www.ajer.org Research Paper Open Access The Effect of Mineralizing Fluorine Varnish on the
American Journal of Engineering Research (AJER) e-issn: 2320-0847 p-issn : 2320-0936 Volume-6, Issue-9, pp-39-43 www.ajer.org Research Paper Open Access The Effect of Mineralizing Fluorine Varnish on the
Continually Fluoride Releasing Aesthetic Dental Restorative Material
 Continually Fluoride Releasing Aesthetic Dental Restorative Material Research is our best product Image provided by Dr. Sushil Koirala BEAUTIFIL II More than just filling BEAUTIFIL II stands out for its
Continually Fluoride Releasing Aesthetic Dental Restorative Material Research is our best product Image provided by Dr. Sushil Koirala BEAUTIFIL II More than just filling BEAUTIFIL II stands out for its
Metal-Free Restorations PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS D I D I E R D I E T S C H I. For.
 PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS Metal-Free Restorations D I D I E R D I E T S C H I The Geneva Smile Center D.M.D, PhD, Privat-Docent 2, Quai Gustave Ador 1207 Geneva
PROCEDURES FOR POSTERIOR DIRECT & SEMI-DIRECT COMPOSITE RESTORATIONS Metal-Free Restorations D I D I E R D I E T S C H I The Geneva Smile Center D.M.D, PhD, Privat-Docent 2, Quai Gustave Ador 1207 Geneva
General dentists in private practice place numerous
 PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
PROACTIVE INTERVENTION DENTISTRY Incorporating Glass Ionomers into Everyday Dental Practice Todd Snyder, DDS, FAACD, FIADFE Introduction General dentists in private practice place numerous direct tooth
Chapter 14 Outline. Chapter 14: Hygiene-Related Oral Disorders. Dental Caries. Dental Caries. Prevention. Hygiene-Related Oral Disorders
 Chapter 14 Outline Chapter 14: Hygiene-Related Oral Disorders Hygiene-Related Oral Disorders Dental caries Prevention Gingivitis Prevention Tooth hypersensitivity Pathophysiology Treatment 2 Hygiene-Related
Chapter 14 Outline Chapter 14: Hygiene-Related Oral Disorders Hygiene-Related Oral Disorders Dental caries Prevention Gingivitis Prevention Tooth hypersensitivity Pathophysiology Treatment 2 Hygiene-Related
Color Masking of Developmental Enamel Defects: A Case Series
 Ó Operative Dentistry, 2015, 40-1, 25-33 Color Masking of Developmental Enamel Defects: A Case Series CRG Torres AB Borges Clinical Relevance White developmental enamel lesions can be successfully masked
Ó Operative Dentistry, 2015, 40-1, 25-33 Color Masking of Developmental Enamel Defects: A Case Series CRG Torres AB Borges Clinical Relevance White developmental enamel lesions can be successfully masked
Essentials of. Dental Assisting. Edition 6. Debbie S. Robinson Doni L. Bird
 Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
Essentials of Dental Assisting Edition 6 Debbie S. Robinson Doni L. Bird CHAPTER21 Restorative Procedures http://evolve.elsevier.com/robinson/essentials/ LEARNING OBJECTIVES KEY TERMS 1. Pronounce, define,
SDR has proven reliability in high C-factor cavities 2
 R R SDR has proven reliability in high C-factor cavities 2 SDR was introduced by DENTSPLY DETREY, Konstanz, Germany in 200 and has since been used in over 20 million restorations across the globe. SDR
R R SDR has proven reliability in high C-factor cavities 2 SDR was introduced by DENTSPLY DETREY, Konstanz, Germany in 200 and has since been used in over 20 million restorations across the globe. SDR
F i l t e k Z550. Nano Hybrid Universal Restorative. Technical Data Sheet
 F i l t e k Z550 Nano Hybrid Universal Restorative Technical Data Sheet Product Description Filtek Z550 Nano Hybrid Universal Restorative is a visible light-activated nanohybrid composite designed for
F i l t e k Z550 Nano Hybrid Universal Restorative Technical Data Sheet Product Description Filtek Z550 Nano Hybrid Universal Restorative is a visible light-activated nanohybrid composite designed for
Contactless Dentistry. Cleans, Cuts, Prepares - Gently
 Contactless Dentistry Cleans, Cuts, Prepares - Gently Contactless Dentistry Unlike conventional rotary cutting instruments, the AquaCare handpiece is not in direct contact with the tooth structure, removing
Contactless Dentistry Cleans, Cuts, Prepares - Gently Contactless Dentistry Unlike conventional rotary cutting instruments, the AquaCare handpiece is not in direct contact with the tooth structure, removing
Detailed Step-by Step Instruction for Chairside Splinting
 Dentapreg TM Splint - Procedures Basic Procedures in Short Splinting with Dentapreg TM strip always includes several basic procedures repeated in all particular clinical situations: (A) Clean the bonding
Dentapreg TM Splint - Procedures Basic Procedures in Short Splinting with Dentapreg TM strip always includes several basic procedures repeated in all particular clinical situations: (A) Clean the bonding
No Prep And Minimal Prep Veneers
 Ajay Juneja No Prep And Minimal Prep Veneers 12 Apr 2016 It has been now an established entity for more then two decades since No Preparation Ceramic Veneers are being used. The very ideology of preserving
Ajay Juneja No Prep And Minimal Prep Veneers 12 Apr 2016 It has been now an established entity for more then two decades since No Preparation Ceramic Veneers are being used. The very ideology of preserving
CERASMART. The new leader in hybrid ceramic blocks
 The new leader in hybrid ceramic blocks Introducing, a new force absorbing hybrid ceramic block 20 µm Contains high density of ultra fine homogeneously-dispersed fillers in a highly cross-linked resin
The new leader in hybrid ceramic blocks Introducing, a new force absorbing hybrid ceramic block 20 µm Contains high density of ultra fine homogeneously-dispersed fillers in a highly cross-linked resin
Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces
 Journal of Physics: Conference Series PAPER OPEN ACCESS Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces To cite this article: F Dianti et
Journal of Physics: Conference Series PAPER OPEN ACCESS Effects of miswak and nano calcium carbonate toothpastes on the hardness of demineralized human tooth surfaces To cite this article: F Dianti et
Take-Home Whitening. in vitro study. Benefits of ACP TAKE-HOME WHITENING
 Fluoride and Potassium Nitrate-Fluoride Whitening Agents: in vitro Caries Study Fluoride and Potassium Nitrate-Fluoride Whitening Agents: in vitro Caries Study in vitro study Hicks J and Flaitz C. Effects
Fluoride and Potassium Nitrate-Fluoride Whitening Agents: in vitro Caries Study Fluoride and Potassium Nitrate-Fluoride Whitening Agents: in vitro Caries Study in vitro study Hicks J and Flaitz C. Effects
Effect of Three Different Remineralizing Agents on White Spot Lesions; AnIn Vitro Comparative Study
 Original Article Effect of Three Different Remineralizing Agents on White Spot Lesions; AnIn Vitro Comparative Study S. Tahmasbi 1, M. Adhami 2, A. Valian 3, R. Hamedi 4. 1 Assistant Professor, Department
Original Article Effect of Three Different Remineralizing Agents on White Spot Lesions; AnIn Vitro Comparative Study S. Tahmasbi 1, M. Adhami 2, A. Valian 3, R. Hamedi 4. 1 Assistant Professor, Department
The Sof-Lex Finishing and Polishing System 3ESPE
 The Sof-Lex Finishing and Polishing System 3ESPE 3M ESPE is a recognized leader in dental innovation. Introduced in the mid-1970s, the Sof-Lex Finishing and Polishing System was a revolutionary breakthrough
The Sof-Lex Finishing and Polishing System 3ESPE 3M ESPE is a recognized leader in dental innovation. Introduced in the mid-1970s, the Sof-Lex Finishing and Polishing System was a revolutionary breakthrough
Three-dimensional measurement of enamel loss caused by bonding and debonding of orthodontic brackets. VAN WAES, H, MATTER, T, KREJCI, Ivo.
 Article Three-dimensional measurement of enamel loss caused by bonding and debonding of orthodontic brackets VAN WAES, H, MATTER, T, KREJCI, Ivo Abstract A mechanical computerized three-dimensional scanner
Article Three-dimensional measurement of enamel loss caused by bonding and debonding of orthodontic brackets VAN WAES, H, MATTER, T, KREJCI, Ivo Abstract A mechanical computerized three-dimensional scanner
Operative dentistry. Lec: 10. Zinc oxide eugenol (ZOE):
:") Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
Operative dentistry Lec: 10 د.عبذالمنعم الخفاجي Zinc oxide eugenol (ZOE): There are 2 types: 1) Unreinforced ZOE (ordinary type): supplied as powder (zinc oxide + some additives like zinc acetate, white
The Fluoride Recharging Capability of an Orthodontic Primer: an in vitro study
 Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2014 The Fluoride Recharging Capability of an Orthodontic Primer: an in vitro study Samuel Allen Virginia
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2014 The Fluoride Recharging Capability of an Orthodontic Primer: an in vitro study Samuel Allen Virginia
Various composite resins are used in orthodontic
 CLINICIAN S CORNER Four applications of reinforced polyethylene fiber material in orthodontic practice Ali Ihya Karaman, DDS, PhD, a Nihal Kir, DDS, b and Sema Belli, DDS, PhD c Konya, Turkey Four different
CLINICIAN S CORNER Four applications of reinforced polyethylene fiber material in orthodontic practice Ali Ihya Karaman, DDS, PhD, a Nihal Kir, DDS, b and Sema Belli, DDS, PhD c Konya, Turkey Four different
Molar Incisor Hypomineralisation (MIH)
") Molar Incisor Hypomineralisation (MIH) Patient Information Leaflet This leaflet explains more about Molar Incisor Hypomineralisation (MIH). If you have any further questions, please speak to the dentist
Molar Incisor Hypomineralisation (MIH) Patient Information Leaflet This leaflet explains more about Molar Incisor Hypomineralisation (MIH). If you have any further questions, please speak to the dentist
RESINOMER Dual- Bisco. Instructions for Use. Cured Amalgam Bonding/Luting System
 Bisco RESINOMER Dual- Cured Amalgam Bonding/Luting System 0459 Instructions for Use IN-029R9 Rev. 10/17 BISCO, Inc. 1100 W. Irving Park Road Schaumburg, IL 60193 U.S.A. 1-847-534-6000 1-800-247-3368 Caution:
Bisco RESINOMER Dual- Cured Amalgam Bonding/Luting System 0459 Instructions for Use IN-029R9 Rev. 10/17 BISCO, Inc. 1100 W. Irving Park Road Schaumburg, IL 60193 U.S.A. 1-847-534-6000 1-800-247-3368 Caution:
ProphyCare. ProphyCare. By DIRECTA
 ProphyCare By DIRECTA Directa s products are developed, tested and evaluated by our selected team of highly-qualified and renowned Swedish and international dental professionals with the aim of making
ProphyCare By DIRECTA Directa s products are developed, tested and evaluated by our selected team of highly-qualified and renowned Swedish and international dental professionals with the aim of making
CONTINUING EDUCATION 2 INDIRECT COMPOSITE RESIN RESTORATIONS. Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature Review
 CONTINUING EDUCATION 2 INDIRECT COMPOSITE RESIN RESTORATIONS Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature Review Camillo D Arcangelo, DDS; Lorenzo Vanini, MD, DDS; Matteo
CONTINUING EDUCATION 2 INDIRECT COMPOSITE RESIN RESTORATIONS Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature Review Camillo D Arcangelo, DDS; Lorenzo Vanini, MD, DDS; Matteo
***Handout*** Adhesive Dentistry Harald O. Heymann, DDS MEd Dentin Bonding Rewetting/Desensitization
 ***Handout*** Adhesive Dentistry Harald O. Heymann, DDS MEd Dentin Bonding * Regardless of the type dentinal adhesive used, the primary mechanism for dentin adhesion is still establishment of the hybrid
***Handout*** Adhesive Dentistry Harald O. Heymann, DDS MEd Dentin Bonding * Regardless of the type dentinal adhesive used, the primary mechanism for dentin adhesion is still establishment of the hybrid
Tooth wear prevention: A quantitative and qualitative in vitro study
 ADRF RESEARCH REPORT Australian Dental Journal 2003;48:(1):15-19 Tooth wear prevention: A quantitative and qualitative in vitro study JA Kaidonis,* J Gratiaen,* N Bhatia,* LC Richards,* GC Townsend* Abstract
ADRF RESEARCH REPORT Australian Dental Journal 2003;48:(1):15-19 Tooth wear prevention: A quantitative and qualitative in vitro study JA Kaidonis,* J Gratiaen,* N Bhatia,* LC Richards,* GC Townsend* Abstract
Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic Appliances
 BALKAN JOURNAL OF STOMATOLOGY ISSN 1107-1141 STOMATOLOGICAL SOCIETY Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic
BALKAN JOURNAL OF STOMATOLOGY ISSN 1107-1141 STOMATOLOGICAL SOCIETY Remineralisation of Enamel Subsurface Lesions with Casein Phosphopeptide - Amorphous Calcium Phosphate in Patients with Fixed Orthodontic
Get in front of the 8 ball with the new Fuji VIII GP. The first auto-cure, resin reinforced glass ionomer restorative
 Get in front of the 8 ball with the new Fuji VIII GP The first auto-cure, resin reinforced glass ionomer restorative 8 reasons to choose Fuji VIII GP Auto-cure, resin reinforced glass ionomer restorative
Get in front of the 8 ball with the new Fuji VIII GP The first auto-cure, resin reinforced glass ionomer restorative 8 reasons to choose Fuji VIII GP Auto-cure, resin reinforced glass ionomer restorative
Practice Impact Questionnaire
 Practice Impact Questionnaire Your practitioner identifier is: XXXXXXXX It is very important that ONLY YOU complete this questionnaire because your responses will be compared to responses that you provided
Practice Impact Questionnaire Your practitioner identifier is: XXXXXXXX It is very important that ONLY YOU complete this questionnaire because your responses will be compared to responses that you provided
Root Surface Protection Simple. Effective. Important.
 GC Fuji VII / Fuji VII EP Root Surface Protection Simple. Effective. Important. Brush up your painting skills and help your patients Q&A Prof. Laurie Walsh University of Queensland lifestyle factors (frequency
GC Fuji VII / Fuji VII EP Root Surface Protection Simple. Effective. Important. Brush up your painting skills and help your patients Q&A Prof. Laurie Walsh University of Queensland lifestyle factors (frequency
CARIES STABILIZATION AND TEMPORARY RESTORATION
 CARIES STABILIZATION AND TEMPORARY RESTORATION LEARNING OUTCOMES Justify the importance of caries stabilisation procedure in operative care. List and discuss the methods to stabilise caries ( include preventive
CARIES STABILIZATION AND TEMPORARY RESTORATION LEARNING OUTCOMES Justify the importance of caries stabilisation procedure in operative care. List and discuss the methods to stabilise caries ( include preventive
Measurement of surface hardness of primary carious lesions in extracted human enamel Measurement of Knoop hardness using Cariotester
 Dental Materials Journal 2015; 34(2): 252 256 Measurement of surface hardness of primary carious lesions in extracted human enamel Measurement of Knoop hardness using Cariotester Akihiko SHIMIZU 1, Takatsugu
Dental Materials Journal 2015; 34(2): 252 256 Measurement of surface hardness of primary carious lesions in extracted human enamel Measurement of Knoop hardness using Cariotester Akihiko SHIMIZU 1, Takatsugu
DiaDent Group International DIA.DENT DiaRoot BioAggregate. Root Canal Repair Material
 DiaDent Group International 1.877.DIA.DENT www.diadent.com DiaRoot BioAggregate Root Canal Repair Material PRECISION. PURITY. RESULTS ABOUT DIAROOT... DiaRoot BioAggregate Root Canal Repair Material is
DiaDent Group International 1.877.DIA.DENT www.diadent.com DiaRoot BioAggregate Root Canal Repair Material PRECISION. PURITY. RESULTS ABOUT DIAROOT... DiaRoot BioAggregate Root Canal Repair Material is
Preparation and making fillings Class V., III., IV.
 Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
Preparation and making fillings Class V., III., IV. Class V. Cervical defects - Dental caries - Non carious lesions (erosion, abrasion, V shaped defects) Types of defects Caries Erosion Abrasion V shaped
illustrated technique guide
 DENTSPLY Caulk 38 West Clarke Avenue Milford, DE 9963 www.dentsply.com www.caulk.com -302-422-45 In Canada call -800-263-437 illustrated technique guide Complete Luting System for: 2006 DENTSPLY International.
DENTSPLY Caulk 38 West Clarke Avenue Milford, DE 9963 www.dentsply.com www.caulk.com -302-422-45 In Canada call -800-263-437 illustrated technique guide Complete Luting System for: 2006 DENTSPLY International.
Title. Citation 北海道歯学雑誌, 38(Special issue): Issue Date Doc URL. Type. File Information.
: Issue Date Doc URL. Type. File Information.") Title The ICDAS (International Caries Detection & Assessme Author(s)Kanehira, Takashi; Takehara, Junji; Nakamura, Kimiya Citation 北海道歯学雑誌, 38(Special issue): 180-183 Issue Date 2017-09 Doc URL http://hdl.handle.net/2115/67359
Title The ICDAS (International Caries Detection & Assessme Author(s)Kanehira, Takashi; Takehara, Junji; Nakamura, Kimiya Citation 北海道歯学雑誌, 38(Special issue): 180-183 Issue Date 2017-09 Doc URL http://hdl.handle.net/2115/67359
Etching with EDTA- An in vitro study
 ISSN 0970-4388 Etching with EDTA- An in vitro study BOGRA P a, KASWAN S b ABSTRACT: In the present study, 25% EDTA, in gel form, was used to analyse its micromorphological effects on tooth surfaces with
ISSN 0970-4388 Etching with EDTA- An in vitro study BOGRA P a, KASWAN S b ABSTRACT: In the present study, 25% EDTA, in gel form, was used to analyse its micromorphological effects on tooth surfaces with
Glass ionomer cements in complex oral rehabilitations. A case report.
 Università degli Studi di Milano - Department of Technologies for the Health I.R.C.C.S Istituto Ortopedico Galeazzi Department of Odontology Director: Prof. Roberto Weinstein Glass ionomer cements in complex
Università degli Studi di Milano - Department of Technologies for the Health I.R.C.C.S Istituto Ortopedico Galeazzi Department of Odontology Director: Prof. Roberto Weinstein Glass ionomer cements in complex
From the office of: Nahidh D. Andrews, DMD 3332 Portage Ave South Bend, IN (574) Are Your Teeth a Sensitive Subject?
 Are Your Teeth a Sensitive Subject?") From the office of: Nahidh D. Andrews, DMD 3332 Portage Ave South Bend, IN 46628-3656 (574) 273-3900 Are Your Teeth a Sensitive Subject? A patient s guide to sensitive teeth and better oral care ARE YOUR
From the office of: Nahidh D. Andrews, DMD 3332 Portage Ave South Bend, IN 46628-3656 (574) 273-3900 Are Your Teeth a Sensitive Subject? A patient s guide to sensitive teeth and better oral care ARE YOUR
PUBLISHED VERSION. This document has been archived with permission from the Australian Dental Association, received 18th January, 2007.
 PUBLISHED VERSION Saunders, J. G. C.; McIntyre, John Malcolm The ability of 1.23% acidulated phosphate fluoride gel to inhibit simulated endogenous erosion in tooth roots Australian Dental Journal, 2005;
PUBLISHED VERSION Saunders, J. G. C.; McIntyre, John Malcolm The ability of 1.23% acidulated phosphate fluoride gel to inhibit simulated endogenous erosion in tooth roots Australian Dental Journal, 2005;
Enamel surface alterations after repeated conditioning with HCl
 Arnold et al. Head & Face Medicine (2015) 11:32 DOI 10.1186/s13005-015-0089-2 HEAD & FACE MEDICINE RESEARCH Open Access Enamel surface alterations after repeated conditioning with HCl W H Arnold 1*, B.
Arnold et al. Head & Face Medicine (2015) 11:32 DOI 10.1186/s13005-015-0089-2 HEAD & FACE MEDICINE RESEARCH Open Access Enamel surface alterations after repeated conditioning with HCl W H Arnold 1*, B.