2018 JCO, Inc. May not be distributed without permission.
|
|
|
- Barnard Marshall
- 5 years ago
- Views:
Transcription




1 2018 JCO, Inc. May not be distributed without permission. CASE REPORT Treatment of Skeletal Class II Open Bite with the Triple Intrusion System HATİCE GÖKALP, DDS, PhD RUHENGİZ EFENDİYEVA, DDS, PhD ÖZLEM BİLGİLİ, DDS, PhD ECEM EFE, DDS Treatment of patients with skeletal open bite usually characterized by downward and backward rotation of the mandible and vertical overgrowth of the maxilla has always been challenging for orthodontists. 1 In adolescents, treatment has traditionally been aimed at inhibiting vertical maxillary growth by means of appliances such as posterior bite blocks, active vertical correctors with magnets, high-pull headgear, and vertical-pull chin cups. 2-4 In nongrowing patients, however, treatment of severe skeletal anterior open bite has usually required maxillary or mandibular surgery or a combination of the two with Le Fort I posterior maxillary impaction. 5 Dr. Gökalp Dr. Efendiyeva Dr. Bilgili Dr. Efe Dr. Gökalp is a Professor and Dr. Efe is a postgraduate student, School of Dentistry, University of Ankara, Ankara, Turkey. Dr. Efendiyeva is in the private practice of orthodontics in Mersin, Turkey, and Dr. Bilgili is in private practice in Bursa, Turkey. Dr. Gökalp at haticegokalp@yahoo.com. VOLUME LII NUMBER JCO, Inc. 427









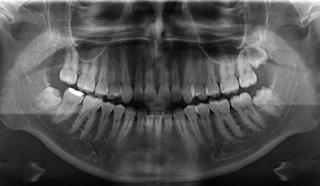

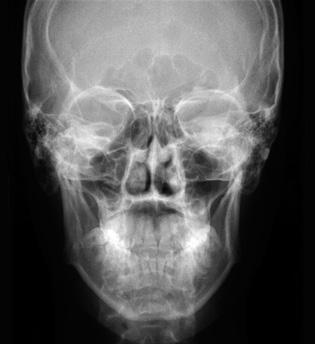
2 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM Fig year-old female patient with skeletal Class II relationship, 6mm overjet, and 1mm anterior open bite before treatment. 428 JCO/August 2018
3 GÖKALP, EFENDİYEVA, BİLGİLİ, EFE If the patient declines surgery because of its potential risks and costs, 1 alternative procedures include extraction therapy, 2 the multiple loop edgewise archwire (MEAW) technique, 6 or the application of nickel titanium archwires with short intermaxillary elastics. 7 Although these methods can increase overbite and provide acceptable interincisal relationships, their soft-tissue results are often unsatisfactory because the skeletal components remain unchanged. Moreover, it is inadvisable to elongate anterior teeth that are already beyond the limits of eruption. 3,4 In recent years, miniscrews 6,8 and miniplates 9,10 have been shown to be effective in providing skeletal anchorage for correction of skeletal open bite by molar intrusion. This case report describes en-masse intrusion of the upper posterior teeth and anterior rotation of the mandible using a triple intrusion system consisting of multipurpose implants* (MPIs), posterior maxillary cap splints, and palatal miniscrews. Diagnosis and Treatment Plan An 18-year-old female with the chief complaint of ineffective chewing was referred to the Department of Orthodontics, Ankara University (Fig. 1). Clinical examination found a symmetrical face, a convex profile, a retrusive contour-deficient chin, and both mentalis and lip strain upon lip closure. The patient had a tonguethrust swallowing pattern and breathed mainly through the nose. Cast analysis revealed 2.5mm of lower crowding, a 6mm overjet, and a 1mm anterior open bite, with a lack of occlusal contact from canine to canine. The curve of Spee was accentuated, and the upper occlusal plane was markedly inclined in an upward direction. Canine and molar relationships were Class II; the dental midlines were nearly coincident with each other and with the facial midline. The patient exhibited 100% incisor display but no gingival exposure on smiling. *Asset Medical Design Co., Istanbul, Turkey; com. A panoramic radiograph showed one missing upper right third molar. Crown-root ratios were normal, with good alveolar bone levels in the buccal segments. Cephalometric analysis indicated a severe skeletal Class II relationship due to a retrognathic mandible (Table 1). The facial pattern was hyperdivergent, as evidenced by a high FMA (28 ), and lower anterior facial height (ANS-Me) was excessive, with a steep mandibular plane. Soft-tissue profile analysis showed protrusive upper and lower lips according to the Ricketts E-line, with a poor chin-throat angle. Functional assessment evidenced no discrepancy between centric relation and centric occlusion. The treatment objectives were to intrude the maxillary posterior segments, reduce the anterior open bite by means of anterior mandibular rotation without extruding the anterior teeth, obtain ideal overbite and overjet, establish Class I canine and molar relationships, modify the tongue habit with anterior guidance, and provide a satisfactory chin projection. Because the underlying malocclusion involved mandibular deficiency and vertical excess of the maxillary posterior dentoalveolar structures, and because redirection of growth and dentoalveolar eruption was impossible in this adult patient, a Le Fort I intrusion osteotomy was recommended for superior repositioning of the posterior maxillary region and a mandibular ramus osteotomy for further advancement of the mandible. 5,14 The patient refused this surgical approach. Nonsurgical alternatives included a combination of intermaxillary elastics with the MEAW 6 technique or nickel titanium archwires, 7 or premolar extractions following retraction of the anterior teeth, with the overbite maintained by a drawbridge effect. 2,15 Camouflage open-bite treatment in an adult patient is indicated only with a normal craniofacial pattern and limited upper incisor exposure at rest. 2,3 Our patient had severe mandibular retrusion, however, so that conventional edgewise treatment would have caused extrusion of the molars and incisors and resulted in posterior and backward rotation of the mandible and worsening of the chin projection. 16 For these reasons, we considered posterior intrusion with skeletal anchorage to be the best nonsurgical VOLUME LII NUMBER 8 429
4 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM treatment plan, allowing the mandible to be repositioned upward and forward and promoting better facial esthetics and joint health. 6,8-13,17 Several authors have described successful intrusion of the maxillary posterior segments in open-bite patients using anchorage from the inferior border of the zygomatic buttress. 6,8-13,17 Transpalatal arches can prevent buccal flaring of the upper posterior teeth, 11 but are not rigid enough to prevent anterior buccal flaring and may lead to TABLE 1 CEPHALOMETRIC ANALYSIS Pre- After Six Post- One Year after Four Years treatment Months Treatment Treatment after Treatment SNA SNB ANB S-Go 81.0mm 82.0mm 81.0mm 82.0mm 80.0mm N-Me 125.0mm 124.0mm 122.0mm 124.0mm 122.5mm Co-Go 51.0mm 57.0mm 59.0mm 59.0mm 55.0mm Gonial angle ANS-Me 78.5mm 76.0mm 74.0mm 75.0mm 74.0mm Facial axis angle SN-MP SN-Occlusal plane U1-NA U1-SN 85.0mm 85.0mm 81.5m 83.0mm 84.0m L1-NB L1-SN 84.5mm 83.5mm 78.5mm 80.5mm 79.0mm L1-MP U1-L U6-SN 76.0mm 71.0mm 70.0mm 72.0mm 71.5mm L6-SN 76.0mm 76.0mm 72.0mm 74.0mm 73.0mm Overjet 6.0mm 3.0mm 2.0mm 2.0mm 3.0mm Overbite 0.0mm 0.5mm 3.0mm 2.5mm 3.0mm Upper lip to E-line 1.5mm 0.0mm 2.0mm 1.0mm 1.0mm Lower lip to E-line 4.5mm 2.5mm 0.0mm 1.0mm 0.0mm Nasolabial angle Labiomental angle JCO/August 2018

 under local anesthesia.")

.")


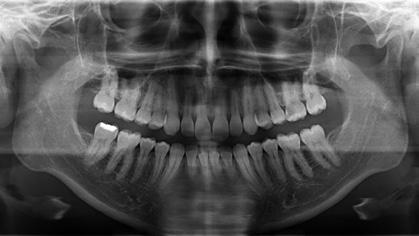
5 GÖKALP, EFENDİYEVA, BİLGİLİ, EFE occlusal interferences. An open Hyrax** screw has been proposed for use with the MPI system, 12 but the palatal mucosa could be injured during intrusion. Therefore, to create a balancing and absolute vertical force of intrusion, we planned to insert miniscrews in the palate. Treatment Progress The three impacted third molars were removed to provide space for molar intrusion. An MPI was adjusted to fit the contour of each zygomatic process and fixed by two bone screws (7mm long) under local anesthesia. The long arm of the miniplate was extended into the oral cavity and exposed to allow attachment of a nickel titanium closed-coil spring.*** One week later, the bilateral occlusal cap splints were fabricated. These shallow acrylic bite blocks should be thicker than the posterior freeway space and long enough to cover all the posterior *Asset Medical Design Co., Istanbul, Turkey; com. **Registered trademark of Dentaurum, Inc., Newtown, PA; www. dentaurum.com. ***Ortho Technology, Inc., Lutz, FL; teeth (Fig. 2). Anterior and posterior hooks were embedded into the buccal and palatal sides of the acrylic blocks for attachment of the coil springs. After the splints were tried in the mouth and primary occlusal contact points were removed, the appliances were attached with glass ionomer cement. Two miniscrews were inserted into the sides of the palate, 5mm apical to the gingival margins of the first molars. When the coil springs were attached from the MPIs and miniscrews to the anterior and posterior hooks on the occlusal cap splints, they applied a total intrusive force of 750-1,000g. The levels of buccal and palatal force were almost equivalent and were closely monitored to avoid crown tipping. The patient was seen every four weeks, but no fixed appliances were placed while the molars were being intruded. After six months, the posterior occlusal cap splints were removed, and a slight posterior open bite was observed (Fig. 3). Clinical crown shortening of the intruded teeth, inflammation of the surrounding periodontal tissues, and relative extrusion of the upper canines were also seen during the active intrusion phase. Periodontal crown lengthening was performed to restore anatomical tooth dimensions and dentogingival relationships. Fig. 2 Posterior occlusal cap splints with embedded hooks used to connect nickel titanium closed-coil springs*** to multipurpose implants* for delivery of vertical intrusive forces on palatal and buccal sides. VOLUME LII NUMBER 8 431










6 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM Fig. 3 Patient after six months of treatment, showing intrusion of lower molars with triple intrusion system. 432 JCO/August 2018
. The upper canines were intruded with.016\".")


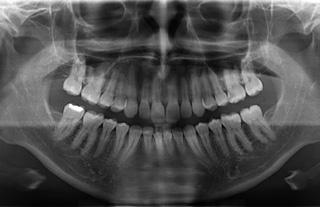
7 GÖKALP, EFENDİYEVA, BİLGİLİ, EFE Fig. 4 Intrusion of upper canines with cantilever springs and of upper incisors with Burstone arch. At this point,.018" preadjusted edgewise appliances were bonded in both arches (Fig. 4). The upper canines were intruded with.016".022" stainless steel cantilever intrusion arches; to allow the insertion of canine intrusion springs, we used brackets with.018" vertical slots. An.016".022" stainless steel Burstone intrusion arch was placed for the upper incisors. Leveling and alignment were completed with.016" stainless steel archwires, followed by.016".022" stainless steel archwires to finish treatment. The lower molar positions were maintained with coil springs throughout the fixed appliance stage, which took 26 months. Total treatment time was 32 months. A removable upper Hawley retainer was delivered to be worn 24 hours per day for one year, and a lower fixed 3-3 retainer was bonded. Both retainers were discontinued one year after treatment. Treatment Results The anterior open bite and retrusive position of the mandible were eliminated through anterior rotation of the mandible, secondary to molar intrusion (Fig. 5). The retrusive chin and poor chinthroat angle were greatly improved, and both mentalis and lip strain disappeared. Functional occlusion with normal interdigitation was achieved, with the canines and molars in a Class I position. The tongue habit was modified, and the periodontal health improved. No root resorption, caries, periodontal bone loss, condylar changes, or flaring of the upper posterior segments occurred. Cephalometric superimpositions showed that the open bite was corrected by intrusion of the posterior maxillary dentoalveolar region with accompanying intrusion of the anterior teeth. This allowed the mandible to be repositioned upward and forward. Favorable soft-tissue profile changes were achieved, and the chin projection was improved. Posterior dentoalveolar intrusion produced a counterclockwise rotation of the mandible, resulting in a 2 increase in SNB and a 2 decrease in ANB (Table 1). Anterior rotation of the mandible was confirmed by a 2.5 increase in the facial axis angle. The flattened mandibular plane angle was primarily caused by reduced posterior maxillary vertical height and increased ramus height. During follow-up observation, the results were seen to remain stable one year (Fig. 6) and four years (Fig. 7) after treatment. Discussion A hyperdivergent facial pattern and retrognathic mandible may result from relatively small amounts of vertical condylar growth and large amounts of vertical alveolar and sutural growth, producing a backward rotation of the mandible. In particular, the vertical height of the upper molars (OP-PP) has been shown to play an important role in this backward rotation. 18 Because our patient had supererupted molars before treatment, our primary objective was to control the vertical dimension. Establishing vertical control in a patient with skeletal open bite and no remaining growth potential is impossible when using conventional fixed appliances such as the MEAW. Such treatment has a minimal effect on the skeletal pattern and bite; closure is achieved mainly by extrusion and uprighting of the incisors, with no molar intrusion. 19,20 VOLUME LII NUMBER 8 433










8 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM Fig. 5 Patient after 32 months of treatment. Lingual buttons on upper first premolars used for attachment of nickel titanium closed-coil springs to maintain vertical control. 434 JCO/August 2018








9 GÖKALP, EFENDİYEVA, BİLGİLİ, EFE Fig. 6 Patient one year after treatment. VOLUME LII NUMBER 8 435









10 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM a Fig. 7 A. Patient four years after treatment (continued on next page). 436 JCO/August 2018
11 GÖKALP, EFENDİYEVA, BİLGİLİ, EFE Pretreatment After six months Post-treatment One year after treatment Four years after treatment b Fig. 7 (cont.) B. Superimposition of cephalometric tracings before treatment, after six months, immediately after treatment, and one and four years after treatment. Skeletal anchorage makes it possible to reduce facial height by absolute intrusion of the molars without extrusion of the adjacent teeth, resulting in an anterior rotation of the mandible and a reduction in facial convexity. 21 We decided to use an MPI system with intraoral attachments that has demonstrated a 92.5% success rate and has been well tolerated by patients. 11,12 The dense cortical bone of the zygomatic buttress is ideal for miniplate anchorage and is relatively safe because of its distance from the dental roots. 9,11-13,17 Posterior bite blocks have been reported to produce a counterclockwise mandibular rotation by transmitting masticatory muscle forces to the buccal alveolar regions and preventing their vertical growth. 22 We made the posterior occlusal cap splints thick enough to exceed the posterior freeway space and thus enable this masticatory muscle force transfer through the acrylic bite blocks. We used segmental mechanics because posterior intrusion with continuous arch mechanics may result in unwanted tooth movement. Intrusion of the posterior dentoalveolar segment with only an apical force on the buccal side would cause adverse buccal tipping, which can impair posterior occlusion, cause interference between the arches, and limit autorotation of the mandible. Although transpalatal arches or constricted overlay archwires are most commonly used to minimize buccal flaring, 11,12 they can impede tongue posture adaptation and should be kept well away from the palate to avoid soft-tissue impingement. The triple intrusion system allows counterbalancing intrusive forces to be applied with no side effects. Although high intrusive forces may play a role in apical root resorption, 21 we observed no significant resorption after intrusion of the first molars with anchorage from zygomatic miniplates and palatal miniscrews. VOLUME LII NUMBER 8 437
12 TREATMENT OF SKELETAL CLASS II WITH TRIPLE INTRUSION SYSTEM Relapse rates after upper molar intrusion reportedly range from 10% to 30%. Sugawara and colleagues observed an average 30% relapse of the posterior teeth after miniscrew-anchored posterior intrusion. 23 Our patient remained stable for at least four years after treatment, with only one year of active retention. Nevertheless, stability might be improved by using strategies such as overcorrection, slow intrusion to allow neuromuscular adaptation, longer retention periods, or more active retention protocols. 24 Conclusion The triple intrusion system is a reliable method for treating an adult open-bite patient with maxillary vertical excess and a retrognathic mandible. In this case, we observed a stable and parallel intrusion of the maxillary posterior dentoalveolar regions without buccal flaring, accompanied by mandibular autorotation. Satisfactory facial esthetics and a functional and stable occlusion were achieved without the need for surgery or unusual patient compliance. REFERENCES 1. Bailey, L.J.; Haltiwanger, L.H.; Blakey, G.H.; and Proffit, W.R.: Who seeks surgical-orthodontic treatment: A current review, Int. J. Adult Orthod. Orthog. Surg. 16: , Beane, R.A.: Nonsurgical management of the anterior open bite: A review of the options, Semin. Orthod. 5: , Sarver, D.M. and Weissman, S.M.: Nonsurgical treatment of open bite in nongrowing patients, Am. J. Orthod. 108: , Subtelny, J.D. and Sakuda, M.: Open-bite: Diagnosis and treatment, Am. J. Orthod. 50: , Epker, B.N. and Fish, L.C.: Surgical-orthodontic correction of open-bite deformity, Am. J. Orthod. 71: , Kuroda, S.; Katayama, A.; and Takano-Yamamoto, T.: Severe anterior open-bite case treated using titanium screw anchorage, Angle Orthod. 74: , Küçükkeleş, N.; Acar, A.; Demirkaya, A.A.; Evrenol, B.; and Enacar, A.: Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics, Am. J. Orthod. 116: , Xun, C.; Zeng, X.; and Wang, X.: Microscrew anchorage in skeletal anterior open-bite treatment, Angle Orthod. 77:47-56, Seres, L. and Kocsis, A.: Closure of severe skeletal anterior open bite with zygomatic anchorage, J. Craniofac. Surg. 20: , Umemori, M.; Sugawara, J.; Mitani, H.; Nagasaka, H.; and Kawamura, H.: Skeletal anchorage system for open-bite correction, Am. J. Orthod. 115: , Erverdi, N.; Tosun, T.; and Keles, A.: A new anchorage site for the treatment of anterior open bite: Zygomatic anchorage: Case report, World J. Orthod. 3: , Erverdi, N.; Keles, A.; and Nanda, R.: The use of skeletal anchorage in open bite treatment: A cephalometric evaluation, Angle Orthod. 74: , Sherwood, K.H.; Burch, J.G.; and Thompson, W.J.: Closing anterior open bites by intruding molars with titanium miniplate anchorage, Am. J. Orthod. 122: , Hoppenreijs, T.J.; Freihofer, H.P.; Stoelinga, P.J.; Tuinzing, D.B.; van t Hof, M.A.; van der Linden, F.P.; and Nottet, S.J.: Skeletal and dento-alveolar stability of Le Fort I intrusion osteotomies and bimaxillary osteotomies in anterior open bite deformities: A retrospective three-centre study, Int. J. Oral Maxillofac. Surg. 26: , Katsaros, C. and Berg, R.: Anterior open bite malocclusion: A follow-up study of orthodontic treatment effects, Eur. J. Orthod. 15: , Endo, T.; Kojima, K.; Kobayashi, Y.; and Shimooka, S.: Cephalometric evaluation of anterior open-bite nonextraction treatment, using multiloop edgewise archwire therapy, Odontol. 94:51-58, De Clerck, H.; Geerinckx, V.; and Siciliano, S.: The zygoma anchorage system, J. Clin. Orthod. 36: , Isaacson, J.R.; Isaacson, R.J.; Speidel, T.M.; and Worms, F.W.: Extreme variation in vertical facial growth and associated variation in skeletal and dental relations, Angle Orthod. 41: , Chang, Y.L. and Moon, S.C.: Cephalometric evaluation of the anterior open bite treatment, Am. J. Orthod. 115:29-38, Ellis, E. III; McNamara, J.A. Jr.; and Lawrence, T.M.: Components of adult Class II open-bite malocclusion, J. Oral Maxillofac. Surg. 43:92-105, Daimaruya, T.; Takahashi, I.; I, Nagasaka, H.; Umemori, M.; Sugawara, J.; and Mitani, H.: Effects of maxillary molar intrusion on the nasal floor and tooth root using the skeletal anchorage system in dogs, Angle Orthod. 73: , Iscan, H.N. and Sarisoy, L.: Comparison of the effects of passive posterior bite-blocks with different construction bites on the craniofacial and dentoalveolar structures, Am. J. Orthod. 112: , Sugawara, J.; Baik, U.B.; Umemori, M.; Takahashi, I.; Nagasaka, H.; Kawamura, H.; and Mitani, H.: Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction, Int. J. Adult Orthod. Orthog. Surg. 17: , Lin, J.C.; Liou, E.J.; and Bowman, S.J.: Simultaneous reduction in vertical dimension and gummy smile using miniscrew anchorage, J. Clin. Orthod. 44: , JCO/August 2018
Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report
 Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Treatment of a malocclusion characterized
 CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
2008 JCO, Inc. May not be distributed without permission. Correction of Asymmetry with a Mandibular Propulsion Appliance
 2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction Treatment?
 TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Anterior open bite due to posterior vertical
 2015 JCO, Inc. May not be distributed without permission. www.jco-online.com Biomechanical Considerations in the Correction of Anterior Open Bite with Maxillary Skeletal Plates S. JACK BURROW III, DDS,
2015 JCO, Inc. May not be distributed without permission. www.jco-online.com Biomechanical Considerations in the Correction of Anterior Open Bite with Maxillary Skeletal Plates S. JACK BURROW III, DDS,
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT. Gupta J*, Makhija P.G.**, Jain V***
 ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT Gupta J*, Makhija P.G.**, Jain V*** Abstract: The inability of orthodontists to change the cant of the maxillary occlusal plane
ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT Gupta J*, Makhija P.G.**, Jain V*** Abstract: The inability of orthodontists to change the cant of the maxillary occlusal plane
2007 JCO, Inc. May not be distributed without permission.
 2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
Intraoral molar-distalization appliances that
 2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment
 The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess
 Case Report 10.5005/jp-journals-10021-1219 Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess 1 Sumit Kumar Yadav, 2 Vikas Sehgal, 3 Sanjay Mittal ABSTRACT Vertical maxillary
Case Report 10.5005/jp-journals-10021-1219 Surgical-Orthodontic Treatment of Gummy Smile with Vertical Maxillary Excess 1 Sumit Kumar Yadav, 2 Vikas Sehgal, 3 Sanjay Mittal ABSTRACT Vertical maxillary
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
Correction of Crowding using Conservative Treatment Approach
 Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Sliding Mechanics with Microscrew Implant Anchorage
 Clinical Report Sliding Mechanics with Microscrew Implant Anchorage Hyo-Sang Park, DDS, MSD, PhD a ; Tae-Geon Kwon, DDS, MSD, PhD b Abstract: Three cases are illustrated. One was treated with maxillary
Clinical Report Sliding Mechanics with Microscrew Implant Anchorage Hyo-Sang Park, DDS, MSD, PhD a ; Tae-Geon Kwon, DDS, MSD, PhD b Abstract: Three cases are illustrated. One was treated with maxillary
Angle Class II, division 2 malocclusion with deep overbite
 BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
Correction of Class II Division 2 Malocclusion by Fixed Functional Class II Corrector Appliance: Case Report
 Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Microscrew Anchorage in Skeletal Anterior Open-bite Treatment
 Original Article Microscrew Anchorage in Skeletal Anterior Open-bite Treatment Chunlei Xun a ; Xianglong Zeng b ; Xing Wang c ABSTRACT Objective: To evaluate the effectiveness of miniscrew anchorage for
Original Article Microscrew Anchorage in Skeletal Anterior Open-bite Treatment Chunlei Xun a ; Xianglong Zeng b ; Xing Wang c ABSTRACT Objective: To evaluate the effectiveness of miniscrew anchorage for
The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding
 B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Case Report. profile relaxed relaxed smiling. How would you treat this malocclusion?
 Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
The etiology of anterior open
 2017 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Nonsurgical Treatment of a Severe Skeletal Anterior Open Bite CHADI KASSIR, DDS, DESO ANTOINE SAADE, CES, CECSMO
2017 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Nonsurgical Treatment of a Severe Skeletal Anterior Open Bite CHADI KASSIR, DDS, DESO ANTOINE SAADE, CES, CECSMO
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth
 Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Severe Anterior Open-Bite Case Treated Using Titanium Screw Anchorage
 Case Report Severe Anterior Open-Bite Case Treated Using Titanium Screw Anchorage Shingo Kuroda, DDS, PhD a ; Akira Katayama, DDS b ; Teruko Takano-Yamamoto, DDS, PhD c Abstract: Anterior open bite is
Case Report Severe Anterior Open-Bite Case Treated Using Titanium Screw Anchorage Shingo Kuroda, DDS, PhD a ; Akira Katayama, DDS b ; Teruko Takano-Yamamoto, DDS, PhD c Abstract: Anterior open bite is
Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient
 Case Report Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient Shingo Kuroda a ; Yasuko Kuroda b Abstract: This article reports the successful treatment of a unilateral
Case Report Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient Shingo Kuroda a ; Yasuko Kuroda b Abstract: This article reports the successful treatment of a unilateral
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Lever-arm and Mini-implant System for Anterior Torque Control during Retraction in Lingual Orthodontic Treatment
 Clinical Report Lever-arm and Mini-implant System for Anterior Torque Control during Retraction in Lingual Orthodontic Treatment Ryoon-Ki Hong, DDS, PHD a ; Jung-Min Heo, DDS b ; Young-Ki Ha, DDS b Abstract:
Clinical Report Lever-arm and Mini-implant System for Anterior Torque Control during Retraction in Lingual Orthodontic Treatment Ryoon-Ki Hong, DDS, PHD a ; Jung-Min Heo, DDS b ; Young-Ki Ha, DDS b Abstract:
Early Mixed Dentition Period
 REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1*
 UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
Orthodontic mini-implants have revolutionized
 CASE REPORT Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient Tae-Woo Kim, a Hyewon Kim, b and Shin-Jae Lee c Seoul, South
CASE REPORT Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient Tae-Woo Kim, a Hyewon Kim, b and Shin-Jae Lee c Seoul, South
Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report
 Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
The treatment options for nongrowing skeletal Class
 CASE REPORT Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion Yoon Jeong Choi, a Jong-Suk Lee, b Jung-Yul Cha, c and Young-Chel Park d Seoul, Korea In nongrowing
CASE REPORT Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion Yoon Jeong Choi, a Jong-Suk Lee, b Jung-Yul Cha, c and Young-Chel Park d Seoul, Korea In nongrowing
An estimated 25-30% of all orthodontic patients can benefit from maxillary
 2017 JCO, Inc. May not be distributed without permission. www.jco-online.com A New Appliance for Efficient Molar Distalization VAIBHAV GANDHI, BDS, MDS FALGUNI MEHTA, BDS, MDS HARSHIK PAREKH, BDS, MDS
2017 JCO, Inc. May not be distributed without permission. www.jco-online.com A New Appliance for Efficient Molar Distalization VAIBHAV GANDHI, BDS, MDS FALGUNI MEHTA, BDS, MDS HARSHIK PAREKH, BDS, MDS
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
Surgically assisted rapid palatal expansion (SARPE) prior to combined Le Fort I and sagittal osteotomies: A case report
 prior to combined Le Fort I and sagittal osteotomies: A case report") 200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion
 Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
Dental Medicine Research 30 2) 161 166, 2010 161 Case Report Orthodontic and Orthognathic Surgical Correction of a Skeletal Class III Malocclusion Tetsutaro Yamaguchi, Yoko Tomoyasu, Tatsuo Shirota*, Masashi
The practice of orthodontics is faced with new
 CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
An Effectiv Rapid Molar Derotation: Keles K
 An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION
 Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Treatment of a severe class II division 1 malocclusion with twin-block appliance
 2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
ISW for the treatment of moderate crowding dentition with unilateral second molar impaction
 International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
A New Fixed Interarch Device for Class II Correction
 A New Fixed Interarch Device for Class II Correction WILLIAM VOGT, DDS Fixed devices are increasingly being used for molar distalization in Class II treatment because they eliminate the need for special
A New Fixed Interarch Device for Class II Correction WILLIAM VOGT, DDS Fixed devices are increasingly being used for molar distalization in Class II treatment because they eliminate the need for special
Introduction Subjects and methods
 European Journal of Orthodontics 33 (2011) 126 131 doi:10.1093/ejo/cjq047 Advance Access Publication 8 November 2010 The Author 2010. Published by Oxford University Press on behalf of the European Orthodontic
European Journal of Orthodontics 33 (2011) 126 131 doi:10.1093/ejo/cjq047 Advance Access Publication 8 November 2010 The Author 2010. Published by Oxford University Press on behalf of the European Orthodontic
ISW for the treatment of adult anterior crossbite with severe crowding combined facial asymmetry case
 International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
Effective and efficient orthodontic management of
 CASE REPORT Interdisciplinary approach for increasing the vertical dimension of occlusion in an adult patient with several missing teeth Flavio Uribe, a Nandakumar Janakiraman, b and Ravindra Nanda c Farmington,
CASE REPORT Interdisciplinary approach for increasing the vertical dimension of occlusion in an adult patient with several missing teeth Flavio Uribe, a Nandakumar Janakiraman, b and Ravindra Nanda c Farmington,
Correction of a maxillary canine-first premolar transposition using mini-implant anchorage
 CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique
 Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Non Extraction philosophy: Distalization using Jone s Jig appliance- a case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars*
 B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S.
 THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
Angle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy*
 O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case
 10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
Case Report Unilateral Molar Distalization: A Nonextraction Therapy
 Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Keeping all these knowledge in mind I will show you 3 cases treated with the Forsus appliance.
 Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile. Background:
 S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
Long-term stability of anterior open bite closure corrected by surgical-orthodontic treatment
 The European Journal of Orthodontics Advance Access published January 17, 2011 European Journal of Orthodontics 1 of 6 doi:10.1093/ejo/cjq194 The Author 2011. Published by Oxford University Press on behalf
The European Journal of Orthodontics Advance Access published January 17, 2011 European Journal of Orthodontics 1 of 6 doi:10.1093/ejo/cjq194 The Author 2011. Published by Oxford University Press on behalf
Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances
 36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
Skeletal Anchorage for Orthodontic Correction of Maxillary Protrusion with Adult Periodontitis
 Case Report Skeletal Anchorage for Orthodontic Correction of Maxillary Protrusion with Adult Periodontitis Tomohiro Fukunaga a ; Shingo Kuroda a ; Hiroshi Kurosaka b ; Teruko Takano-Yamamoto c Abstract:
Case Report Skeletal Anchorage for Orthodontic Correction of Maxillary Protrusion with Adult Periodontitis Tomohiro Fukunaga a ; Shingo Kuroda a ; Hiroshi Kurosaka b ; Teruko Takano-Yamamoto c Abstract:
Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique
 10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions
 Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews.
 SM 3M Health Care Academy Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews. Dr. J.C. Pérez-Varela MD, DDS, MS, Ph.D. Specialist in Orthodontics. Doctor of Medicine
SM 3M Health Care Academy Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews. Dr. J.C. Pérez-Varela MD, DDS, MS, Ph.D. Specialist in Orthodontics. Doctor of Medicine
Treatment of Long face / Open bite
 In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
Research & Reviews: Journal of Dental Sciences
 Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Adult Class lll Treatment Using a J-Hook Headgear to the Mandibular Arch
 Original Article Adult Class lll Treatment Using a J-Hook Headgear to the Mandibular Arch Yasuko Kuroda a ; Shingo Kuroda b ; Richard G.Alexander c ; Eiji Tanaka d ABSTRACT Objective: To evaluate the treatment
Original Article Adult Class lll Treatment Using a J-Hook Headgear to the Mandibular Arch Yasuko Kuroda a ; Shingo Kuroda b ; Richard G.Alexander c ; Eiji Tanaka d ABSTRACT Objective: To evaluate the treatment
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
Class III malocclusions are complex to MANDIBULAR CERVICAL HEADGEAR IN ORTHOPEDIC AND ORTHODONTIC TREATMENT OF CLASS III CASES
 Diego Rey, DDS, Cert Ortho 1 Juan Fernando Aristizabal, DDS, Cert Ortho 2 Giovanni Oberti, DDS, Cert Ortho 3 David Angel, DDS, Cert Ortho 4 MANDIBULAR CERVICAL HEADGEAR IN ORTHOPEDIC AND ORTHODONTIC TREATMENT
Diego Rey, DDS, Cert Ortho 1 Juan Fernando Aristizabal, DDS, Cert Ortho 2 Giovanni Oberti, DDS, Cert Ortho 3 David Angel, DDS, Cert Ortho 4 MANDIBULAR CERVICAL HEADGEAR IN ORTHOPEDIC AND ORTHODONTIC TREATMENT
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Case Report n 2. Patient. Age: ANB 8 OJ 4.5 OB 5.5
 Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Transverse malocclusion, posterior crossbite and severe discrepancy*
 O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
Experience with Contemporary Tip-Edge plus Technique A Case Report.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider
 Bilater eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider Ahmet Keles, DDS, DMSc 1 /Binnur Pamukcu, DDS 2 /Ebru Cetinkaya Tokmak, DDS 2 Aim: To introduce a new intraoral appliance
Bilater eral Maxillary y Molar Distalization with Sliding Mechanics: Keles Slider Ahmet Keles, DDS, DMSc 1 /Binnur Pamukcu, DDS 2 /Ebru Cetinkaya Tokmak, DDS 2 Aim: To introduce a new intraoral appliance
Skeletal class III and anterior open bite treatment with different retention protocols: a report of three cases
 Journal of Orthodontics, Vol. 39, 2012, 212 223 CLINICAL SECTION Skeletal class III and anterior open bite treatment with different retention protocols: a report of three cases Milton Meri Benitez Farret
Journal of Orthodontics, Vol. 39, 2012, 212 223 CLINICAL SECTION Skeletal class III and anterior open bite treatment with different retention protocols: a report of three cases Milton Meri Benitez Farret
Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports
 Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
Dual Force Cuspid Retractor
 CLINICAL INNOVATION 1 Matrishva B Vyas, 2 Neeraj Alladwar ABSTRACT The most time consuming stage of bicuspid extraction-based treatment is cuspid retraction. Cuspid retraction with both types of conventional
CLINICAL INNOVATION 1 Matrishva B Vyas, 2 Neeraj Alladwar ABSTRACT The most time consuming stage of bicuspid extraction-based treatment is cuspid retraction. Cuspid retraction with both types of conventional
System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi
 A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
Orthodontic Treatment Using The Dental VTO And MBT System
 Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year Follow-Up
 Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Combined Orthodontic And Surgical Correction Of An Adolescent Patient With Thin Palatal Cortex And Vertical Maxillary Excess
 Combined Orthodontic And Surgical Correction Of An Adolescent Patient With Thin Palatal Cortex And Vertical Maxillary Excess Hegde M, 1 Hegde C, 2 Parajuli U, 3 Kamath P, 4 MR D 1 Department of orthodontics
Combined Orthodontic And Surgical Correction Of An Adolescent Patient With Thin Palatal Cortex And Vertical Maxillary Excess Hegde M, 1 Hegde C, 2 Parajuli U, 3 Kamath P, 4 MR D 1 Department of orthodontics