Comparison of Two methods of Transpalatal Arch and Lingual Arch Activation
|
|
|
- Kerry Lewis
- 5 years ago
- Views:
Transcription

1 Loma Linda University Digital Archive of Research, Scholarship & Creative Works Loma Linda University Electronic Theses, Dissertations & Projects Comparison of Two methods of Transpalatal Arch and Lingual Arch Activation Taoran Zhang Follow this and additional works at: Part of the Orthodontics and Orthodontology Commons Recommended Citation Zhang, Taoran, "Comparison of Two methods of Transpalatal Arch and Lingual Arch Activation" (2016). Loma Linda University Electronic Theses, Dissertations & Projects This Thesis is brought to you for free and open access by Digital Archive of Research, Scholarship & Creative Works. It has been accepted for inclusion in Loma Linda University Electronic Theses, Dissertations & Projects by an authorized administrator of Digital Archive of Research, Scholarship & Creative Works. For more information, please contact
2 LOMA LINDA UNIVERSITY School of Dentistry in conjunction with the Faculty of Graduate Studies Comparison of Two methods of Transpalatal Arch and Lingual Arch Activation by Taoran Zhang A Dissertation submitted in partial satisfaction of the requirements for the degree Master of Science in Orthodontics and Dentofacial Orthopedics September 2016
3 2016 Taoran Zhang All Rights Reserved
4 Each person whose signature appears below certifies that this thesis in his/her opinion is adequate, in scope and quality, as a thesis for the degree of Master of Science., Chairperson Rodrigo Viecilli, Associate Professor of Orthodontics and Dentofacial Orthopedics Joseph Caruso, Professor of Orthodontics and Dentofacial Orthopedics Gregory Olson, Associate Professor of Orthodontics and Dentofacial Orthopedics iii
5 ACKNOWLEDGEMENTS I would like to express my appreciation to the individuals who helped me complete this study: Loma Linda University Department of Orthodontics and the members of my guidance committee; Drs. Rodrigo Viecilli, Joseph Caruso and Greg Olson for their advice and suggestions. iv
6 CONTENT Approval Page... iii Acknowledgements... iv List of Figures... vi List of Tables... xi List of Abbreviations... xiv Abstract...xv Chapter 1. Review of the Literature Comparison of two methods of transpalatal arch and lingual arch activation...20 Abstract...21 Introduction...23 Statement of Problem...23 Hypothesis...24 Materials and Methods...28 Calibration...28 Axis and moment definition...29 Data Collection...32 Comparison 1: PT1 vs. ST1 vs. FT Comparison 2: PT2 vs. ST2 vs. FT Comparison 3: PT3 vs. ST3 vs. FT Comparison 4: PL1 vs. SL1 vs. FL Comparison 5: PL2 vs. SL2 v.s FL Comparison 6: PL3 vs. SL3 vs. FL Statistical Analysis...46 Results...47 Comparison 1: PT1 vs. ST1 vs. FT Comparison 2: PT2 vs. ST2 vs. FT v
7 Comparison 3: PT3 vs. ST3 vs. FT Comparison 4: PL1 vs. SL1 vs. FL Comparison 5: PL2 vs. SL2 v.s FL Comparison 6: PL3 vs. SL3 vs. FL Discussion...88 Conclusion...91 References Extended Discussion...94 References...96 vi
8 FIGURES Figure Title page 1 Axis definition for maxillary right first molar. (Mesial, lingual and buccal views) 30 2 Axis definition for maxillary molars. (Mesial view) 30 3 Axis definition for maxillary dentition Right hand rule for moment axis Passive TPA in first order activation group. Mesial view Passive TPA in first order activation group. Occlusal view Passive TPA in first order activation group. Buccal view TPA with first order shape-driven activation. Mesial view TPA with first order shape-driven activation. Occlusal view TPA with first order shape-driven activation. Buccal view TPA with first order force-driven activation. Mesial view TPA with first order force-driven activation. Occlusal view TPA with first order force-driven activation. Buccal view Passive TPA in second order activation group. Mesial view Passive TPA in second order activation group. Occlusal view Passive TPA in second order activation group. Buccal view TPA with second order shape-driven activation. Mesial view TPA with second order shape-driven activation. Occlusal view TPA with second order shape-driven activation. Buccal view TPA with second order force-driven activation. Mesial view TPA with second order force-driven activation. Occlusal view TPA with second order force-driven activation. Buccal view Passive TPA in third order activation group. Mesial view Passive TPA in third order activation group. Occlusal view Passive TPA in third order activation group. Buccal view TPA with third order shape-driven activation. Mesial view TPA with third order shape-driven activation. Occlusal view. 40 vii
9 28 TPA with third order shape-driven activation. Buccal view TPA with third order force-driven activation. Mesial view TPA with third order force-driven activation. Occlusal view TPA with third order force-driven activation. Buccal view Passive LA in first order activation group. Mesial view Passive LA in first order activation group. Occlusal view Passive LA in first order activation group. Buccal view LA with first order shape-driven activation. Mesial view LA with first order shape-driven activation. Occlusal view LA with first order shape-driven activation. Buccal view LA with first order force-driven activation. Mesial view LA with first order force-driven activation. Occlusal view LA with first order force-driven activation. Buccal view Passive LA in second order activation group. Mesial view Passive LA in second order activation group. Occlusal view Passive LA in second order activation group. Buccal view LA with second order shape-driven activation. Mesial view LA with second order shape-driven activation. Occlusal view LA with second order shape-driven activation. Buccal view LA with second order force-driven activation. Mesial view LA with second order force-driven activation. Occlusal view LA with second order force-driven activation. Buccal view Passive LA in third order activation group. Mesial view Passive LA in third order activation group. Occlusal view Passive LA in third order activation group. Buccal view LA with third order activation. Mesial view LA with third order activation. Occlusal view LA with third order activation. Buccal view D force comparison in TPA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 50 viii
10 57 3D moment comparison in TPA first order activation maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D force comparison in TPA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in TPA first order activation maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D force comparison in TPA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 61 3D moment comparison in TPA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 62 3D force comparison in TPA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in TPA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 64 3D force comparison in TPA third order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in TPA third order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 66 3D force comparison in TPA third order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked ix
11 67 3D moment comparison in TPA third order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 68 3D force comparison in LA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in LA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 70 3D force comparison in LA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in LA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D force comparison in LA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in LA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 74 3D force comparison in LA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked D moment comparison in LA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Means and standard deviations of each group are marked. 76 3D force comparison in LA third order activation for maxillary right first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are marked. 77 3D moment comparison in LA third order activation for maxillary right first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are marked x
12 78 3D force comparison in LA third order activation for maxillary left first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are marked. 79 3D moment comparison in LA third order activation for maxillary left first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are marked xi
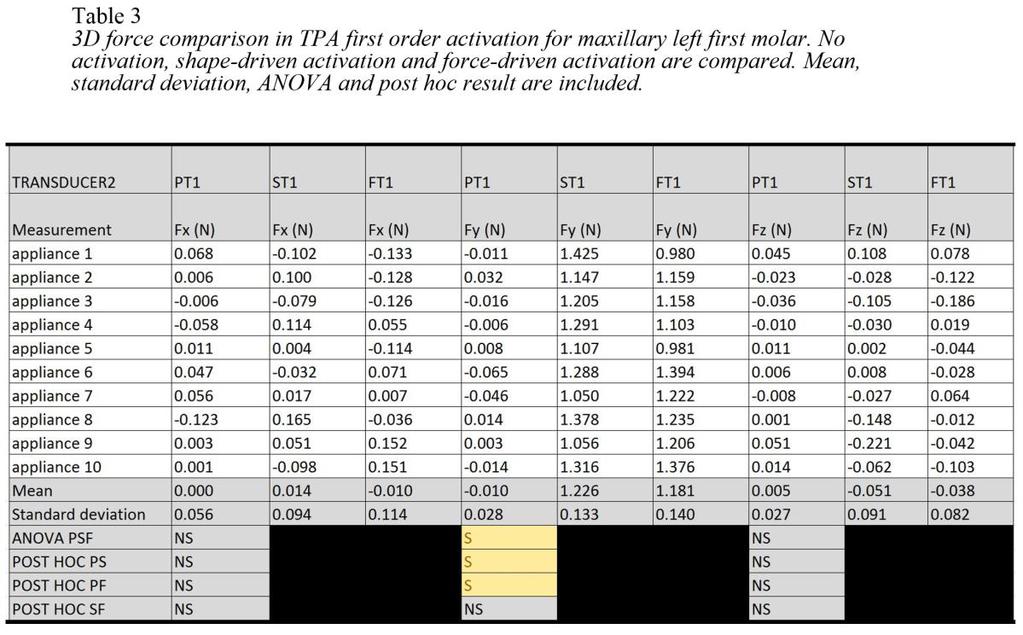
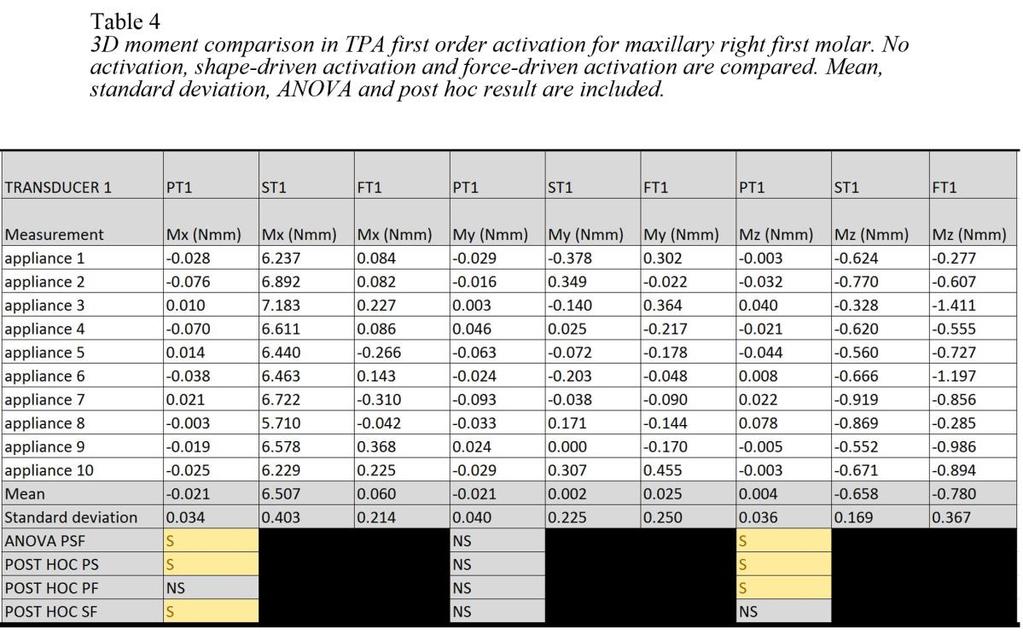
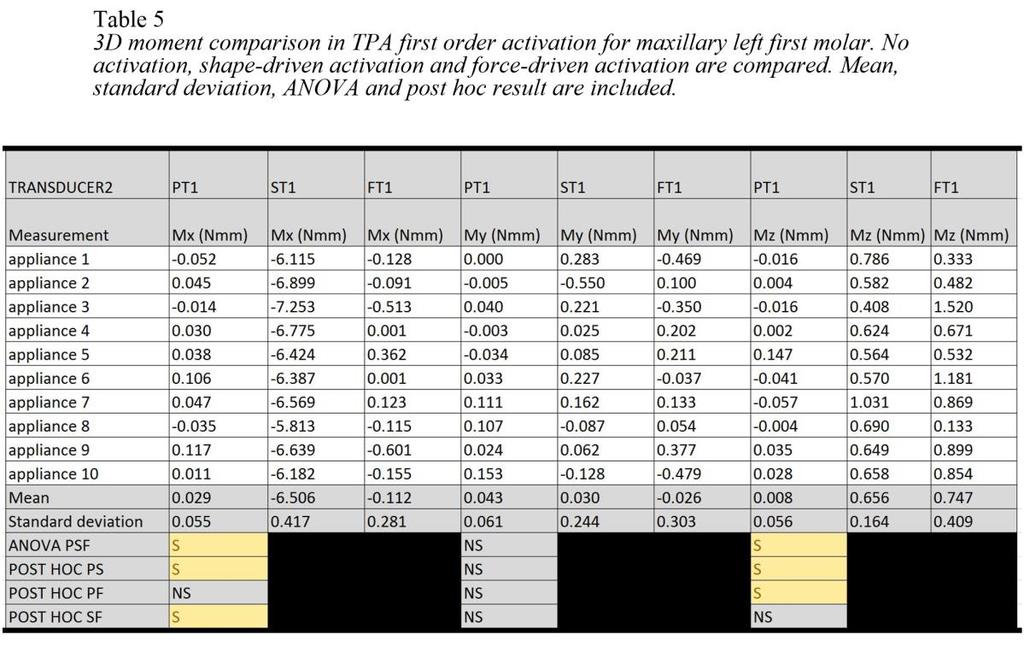
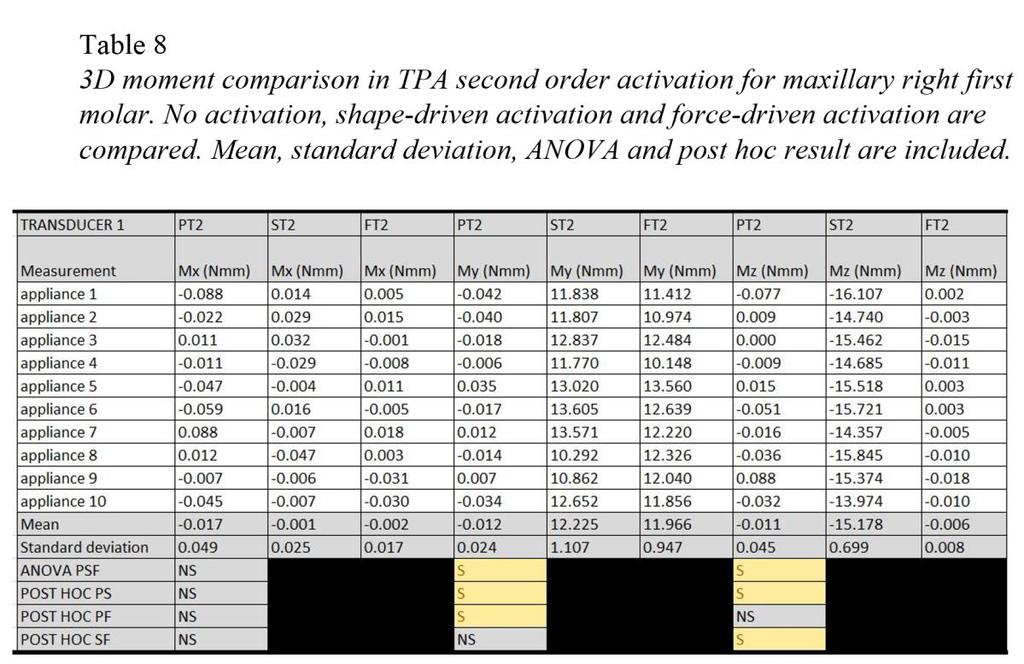
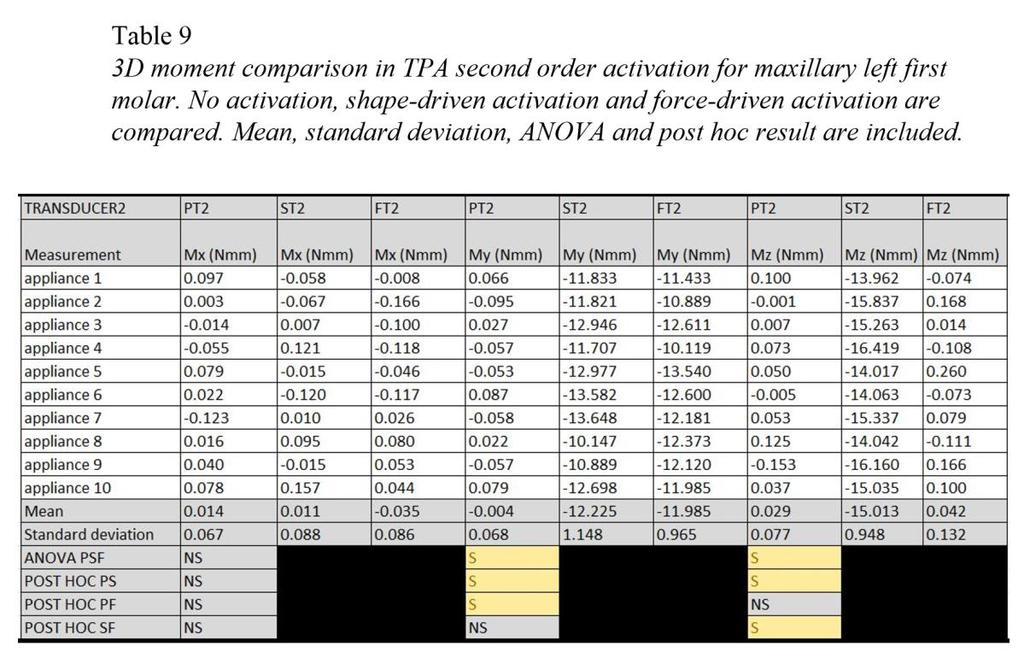
13 TABLES Table Title 1 Grouping table D force comparison in TPA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 3 3D force comparison in TPA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 4 3D moment comparison in TPA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 5 3D moment comparison in TPA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 6 3D force comparison in TPA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 7 3D force comparison in TPA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 8 3D moment comparison in TPA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 9 3D moment comparison in TPA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 10 3D force comparison in TPA third order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. page xii
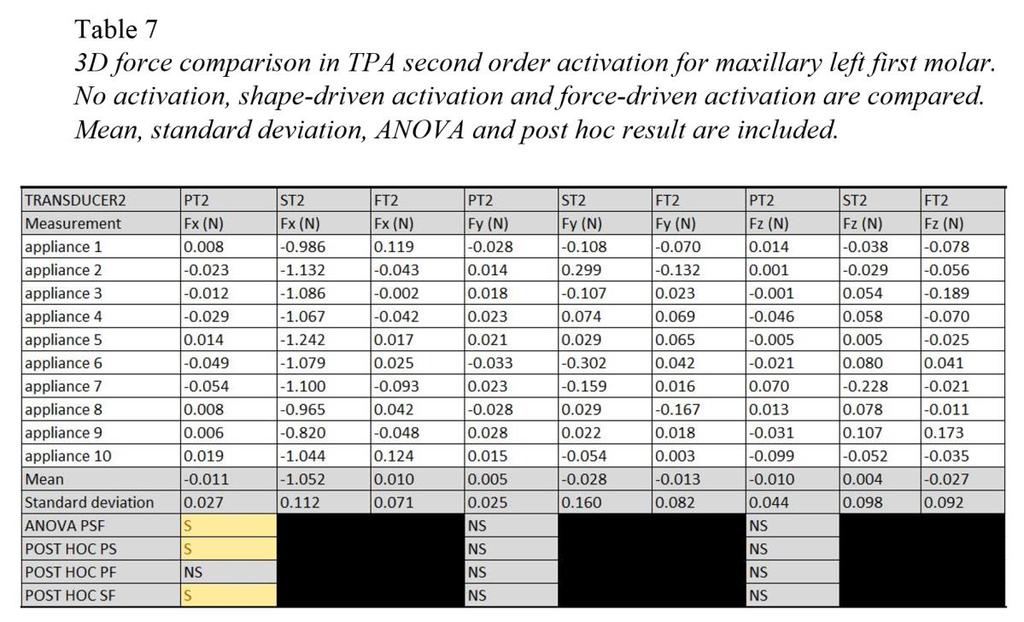
14 11 3D force comparison in TPA third order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 12 3D moment comparison in TPA third order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 13 3D moment comparison in TPA third order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 14 3D force comparison in LA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 15 3D force comparison in LA first order activation for maxillary right left molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 16 3D moment comparison in LA first order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 17 3D moment comparison in LA first order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 18 3D force comparison in LA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 19 3D force comparison in LA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 20 3D moment comparison in LA second order activation for maxillary right first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included. 21 3D moment comparison in LA second order activation for maxillary left first molar. No activation, shape-driven activation and force-driven activation are compared. Mean, standard deviation, ANOVA and post hoc result are included xiii
15 22 3D force comparison in LA third order activation for maxillary right first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are included. 23 3D force comparison in LA third order activation for maxillary left first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are included. 24 3D moment comparison in LA third order activation for maxillary right first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are included. 25 3D moment comparison in LA third order activation for maxillary left first molar. No activation and shape/force-driven activation are compared. Mean and standard deviation are included xiv
16 ABBREVIATIONS TPA LA CRot CRes F Fx Fy Fz M Mx My Mz Transpalatal arch Lingual arch Center of rotation Center of resistance Force Force in x axis Force in y axis Force in z axis Moment Moment in x axis Moment in y axis Moment in z axis xv
17 ABSTRACT OF THE THESIS Comparison of Two methods of Transpalatal Arch and Lingual Arch Activation by Taoran Zhang Master of Science, Graduate Program in Orthodontics and Dentofacial Orthopedics Loma Linda University, September 2016 Dr. Rodrigo Viecilli, Chairperson The TPA and LA can be activated with two methods: the shape-driven method where the appliance is made to match the final tooth position and the force-driven method where the appliance is made to make sure the force system delivered by it at the beginning is consistent with the planned tooth movement. This study compared the two methods in vitro quantitatively with typodont teeth and multi-axis force torque transducers in all three dimensions. Results: In the TPA first order activation, with comparable Fy (force on Y axis) reading, the shape-driven activation group had a significantly higher Mx (moment on X axis) reading than the force-driven activation group. In the TPA second order activation, with comparable My (moment on Y axis) reading, the shape-driven activation group had a significantly higher Fx (Force on X axis) reading than the force-driven activation group. In the TPA third order activation, with comparable Mx (moment on X axis) reading, the shape-driven activation group had a significant higher Fy (force on Y axis) reading than the force-driven activation group. In the LA first order activation, with comparable Fy (force on Y axis) reading, the shapedriven activation group had a significantly higher Mz (moment on Z axis) reading than the force-driven activation group. In the LA second order activation, with comparable My (moment on Y axis) reading, the shape-driven activation group had a significantly higher xvi
18 Fz (force on Z axis) reading than the force-driven activation group. In the LA third order activation, the shape-driven activation method resulted in the exact same shape as the force-driven activation method, no comparison between the two activation methods was needed and both method yielded the same result. Conclusion: Both TPA and LA activated using the force-driven method exhibited lesser unintended side effects in first, second and third order forces and moments than the shape-driven method. As the targeted tooth movements can be helped or hindered by the side effects, clinicians can refer to the results to make the correct activations for the most efficient and effective tooth movements. xvii
19 CHAPTER ONE REVIEW OF THE LITERATURE The transpalatal arch (TPA) is an appliance connects the lingual of contralateral molars horizontally following the contour of the palate.. It is also called transpalatal bar, palatal bar, palatal arch bar or transpalatal lingual arch. The lingual arch (LA) is an appliance going along the alveolar ridge on the tongue side, which is frequently used for mandible, but can also be used for maxillary dentition. Both TPA and LA are commonly used appliances in clinical orthodontics treatment [1-6]. TPA and LA can be used passively to maintain space or anchorage, and they can also be used actively to provide forces and moments for expected tooth movement. However, without careful consideration, the TPA and LA without proper activation can lead to significant clinical side effects of unwanted tipping, torqueing, round tripping and other movements associated with reactive force systems. To maximize the expected effects and to minimize the side effects, TPA and LA activation methods need to be compared and analyzed. Theoretical analysis of the biomechanics has been attempted, but well-designed quantified in vitro comparisons are not yet available. The traditional transpalatal arch (TPA) is fabricated from a heavy gauge stainless wire. The original design consists of a straight bar across the palate, thus it is sometimes called transpalatal bar. This design links the left and right buccal segments together. However, the straight wire limits the possible activation needed, and, depending on the height of placement, it may also invade the natural tongue space in the oral cavity, thus reducing patient comfort. By constantly applying vertical tongue pressure on the appliance, wanted or unwanted molar intrusion can occur. 1
20 Goshgarian type transpalatal bar is the most common TPA design used today. In this design, the straight bar is bent into a curve to fit the palatal vault, thus increasing patient comfort. In addition, in this design, changing the arch form makes expansion, constriction, rotation and torque of the molars possible. Typically, a stainless steel wire is used. The wire can be bent on a stone study model or directly from the mouth to make necessary soft tissue clearance. Prefabricated arches are also available for purchase. After forming the arch, both ends of the arch can be soldered onto the bands or they can be welded to the bands lingual attachments. A single central omega loop can be added to the arch, where the loop can either face forward or backward. This loop setup may make the fabrication and adjustment easier. Added length of the wire also make the appliance more flexible [2, 5]. Zachrisson modified the design of the Goshagarian type transpalatal bar [7, 8]. This type is made from inch Blue Elgiloy wire and has three loops: single big central loop and two symmetrical smaller side loops. The center loop is 9mm and facing medially. The side loops are 5mm and facing distally. Longer end bars are left on both ends. Instead of soldering or welding, the ends are inserted into the lingual sheath of the molar bands. This feature makes the bar removable. As a removable appliance, complete passiveness, precise activation, reactivation and adjustment become easier. The added wire length and side loops design also makes the appliance more flexible, thus insertion/activation and other clinical uses become easier. To get more torque control from TPA, another linking method between the wire and bands can be used. Instead of single wire soldering joint, the wire at the end can be bent back to form a double wire handle. This handle can be inserted into the molar band 2
21 lingual sheath. Because of the rectangular cross section shape of the handle, the end can not rotate freely in the lingual sheath, thus 3rd order torque control from the TPA becomes possible. Again this removable wire handle design also get the benefit of precise control of complete passiveness, activation, reactivation and easier adjustment. In this appliance, an elastic ligature or stainless steel tie ligature can be used to secure the wire into the lingual sheath [9]. Another design, the precision lingual arch, developed by Burstone, also focused on a wire-band attachment. [10, 11] On the lingual of molar band, a bracket which can accomodate an 0.032x0.032 square wire is attached. Compared with a tube, the insertion and removal of TPA wire becomes easier. As in the previous cases, the torque can be added to this design, however in addition, the fit is more precise in this bracket system. To further improve the TPA design and make it user friendly, a bracket with hinge cap attachment is used for linking [12]. Here, when the cap is closed, the bracket automatically becomes a tube. This eliminates the usage of elastic tie or steel tie and make the clinic adjustment much easier. In addition, tie wings are no longer needed thus it is smoother and is more comfortable to patients. A quad helix is an orthodontic appliance for transverse dimension discrepancy correction [13-16]. It is made from stainless steel wire bent into W shape with 4 loops and soldered onto the molar bands. In a broad sense, quad helix appliances are also a variety of TPA. Compared with the common TPA, quad helix has very long wire length with 4 loops built inside to make it very flexible. This gives it a larger range of action and makes it easier to use. The long arms can push the whole buccal segments out during expansion, which is also very useful in clinical situations. In addition, the long straight 3
22 center wire and side wires makes clinical adjustment easier and predictable, and intra-oral adjustment with 3-pronged pliers becomes possible. A hyrax is another common palatal expanding appliance. Prolonged retention phase after the active expansion is usually maintained. TPA is usually used during the retention as it takes less space in the mouth. This can be achieved by removing the Hyrax completely, fabricating a new TPA, then trying it in and cementing it. However, a new method of converting a Hyrax into a TPA has been tested [17]. In this method, two stainless steel wire segments were soldered onto the posterior expansion leg of Hyrax before delivery to the palatal side. After satisfactory expansion is achieved, these two segments are soldered together, the expansion screw is cut off, and the Hyrax is converted to a TPA easily [17]. The Butterfly Arch TPA is a recent variety of TPA design [18]. Although passive TPAs are commonly used as anchorage devices, maximum anchorage is not always achieved with previous designs. One of the weak aspects of traditional TPAs is the inability to resist forces applied perpendicular to the long axis of the teeth, thus a slight force applied on one side of the arch will tend to rotate the other end of the arch with little resistance. Here with a stainless steel wire, the butterfly arch is linked to 4 molar bands of both the first and second molars. In addition to the transitional arch, an x shaped cross framework is added to form a butterfly wing shape. The authors claimed that this kind of framework has a high resistance against distortion by design, and is more resistant to molar dumping and anchorage loss. The bracing element of the framework can resist medial force effectively, and the tongue trapping area can convert the perpendicular tongue pressure into distal tipping force to upper molars. The 3D shape 4
23 of the framework could add resistance to anchorage loss and anterior movement, and reactive pre-activation forces could be added to control the anchorage. With 3 wire soldering points and 4 molar bands soldering points, the framework is divided into short segments, which further increases the total rigidity of the appliance effectively. Overall the authors concluded that this butterfly arch TPA has certain advantages for anchorage preservation in some clinical situations. With the aid of high speed CPUs and calculation software, new designs can be fabricated and tested with a computer using the finite element method. This method can precisely screen the needed force, moment and energy quickly without in vitro experiment and in vivo clinical trial. With the screening of this approach, the possible good designs can be further studied on the models and with the patients. This new method can greatly decrease the time, expense and numbers of patient needed for a large scale clinical trial. In a recent study, [18], 13 different virtual designs of TPAs were tested for the treatment of unilateral molar rotation. All of the 13 designs contain a palatal bar and two tubes, but different number and/or position of U loop and /or helices are added to test the effects. Straight parallel wires, rectangular R loops, and reverse action helices were also tried. In the setup, Model 1 is the traditional continuous TPA and 12 modifications to the traditional TPA are investigated. In Model 2, one U-loop was added at the midline; in Model 3, an additional U-loop was added equidistant between the midline U-loop and molar; in Model 4, two U-loops were added between the midline U- loop and first molar; and in Model 5 only a single U-loop placed near the molar tube was added. In Models 6 and 7, modifications included the addition of either single unilateral or double helices adjacent to the molar tubes to the TPA. In Models 8 and 9, straight 5
24 parallel wires were adapted to the palate, with model 8 wire taking the S shape and model 9 wire, the omega shape. In Models 10 and 11, one or two rectangular R loops were incorporated into the traditional TPA. In Model 12, single helix was used in a reverse action; and Model 13 utilized double helices in a reverse action. Models were meshed with nodes and 6491 elements and analyzed with ANSYS Workbench Ver applying Young s modulus (2e5MPa) and Poisson s ratio (0.3). The mesial part of the left side tube was displaced 0.1, 0.25, 0.5 and 1 mm, successively towards the midline, simulating palatal bar tab engagement in a mesio-palatal rotated maxillary left molar, and the force, moment and energy produced in the normal side (right) molar were recorded in different models. This approach analyzed the characters of the 12 new designs precisely and compared those to the traditional TPA design. Results showed that the associated mesializing force was lower than that seen in the traditional design and the moment showed an increasing pattern when compared with a simple palatal bar. With energy levels, the same increasing pattern was observed in the designs between activations of 0.1 and 1.0 mm. As the best design in this application is thought to have the highest energy, highest moment and the lowest mesializing force, out of the 12 designs, based on all the results, the author concluded that Model 9 with Omega shape straight parallel wires added was the best model for derotating a unilateral maxillary molar tooth. In the future, with further development of faster computer, better software, new interesting materials, longer clinical trials and more clinical experiences, more and better designs of TPA are expected for many different clinical situations. Transpalatal arches have many clinical uses. They can be used either as a passive or an active appliance. When used passively, they provide anchorage, space maintenance, 6
25 etc. When used actively, they provide needed action in first, second, and third orders; correct crossbite, and provide expansion for the whole arch. They can be used symmetrically and asymmetrically, and may also be used together with other appliance or temporary anchorage devices (TAD) for multiple purposes. The most common use of the TPA is anchorage. Here the TPA stays in a passive form without activation. Theoretically, when permanent maxillary molars move anteriorly, they rotate mesiolingually around the large lingual root. The space between the buccal and lingual cortical plates becomes narrow anterior to the first molar roots, preventing the molar from advancing directly and limiting its movement to a rotation [7]. The large lingual root contacts the lingual plate and acts as a pivot, allowing the 2 buccal roots to rotate mesiolingually. The TPA reduces anterior molar movement by coupling the right and left permanent molars together and, thus, preventing any possibility of rotations. For example, in the study of Ziegler, et. al. [19], a Goshgarian type TPA was used together with a standard headgear for anchorage, and this headgear was worn hours per day. With enough anchorage, maxillary canine was retracted with a retraction spring and with a sliding mechanics. In both conditions, satisfactory anchorages were achieved. As maxillary anchorage can also be achieved with Nance palatal arch appliance, many studies have been carried out to compare these two. In a 2007 study [17], Ari Kupietzky, et al. claimed that in mixed dentition, TPA is an alternative to Nance appliance and has certain advantages in pediatric populations. TPA is less likely to irritate the soft tissue and.interfer with speech thus providing greater patient comfort and hygiene. In addition, TPA can control the vertical dimension of the permanent molars 7
26 with constant tongue pressure. If in any condition active forces is required, TPA can also be easily activated for the purpose. For these reasons, the author recommended TPA over Nance appliance for pediatric patient s space maintenance. On the same topic, a randomized clinical trial study was conducted in 2009 by Stivaros, et. al. [20], twenty-nine patients were assigned to the Goshgarian TPA group and 28 patients were assigned to the Nance group. T2 was taken six months later. The amount of upper first permanent molar mesial movement, distal tipping, and mesiopalatal rotation was measured by scanning T1 and T2 study models and then using a software program to calculate molar changes. It is discovered that there were no statistically significant differences in prevention of mesial drift or distal tipping (P > 0.05). There was a statistically significant difference in the amount of molar rotation between the arch types, with both exhibiting some distopalatal rotation even though they were not activated for this movement. The Goshgarian palatal arch produced marginally more disto-palatal rotation than the Nance arch (P = 0.02), although this may not be considered clinically significant. There was also a statistically significant difference in pain scores between the Goshgarian and the Nance arch, with the Nance being associated with more discomfort (P = 0.001). This study did not support any preference in the use of the Goshgarian TPA or Nance palatal arch. As TPA is sometimes criticized to have a negative impact on normal molar eruption and thus vertical control, Wise JB et al did a retrospective patient study [21]. It was discovered that no statistically significant differences were noted between control and test groups form maxillary and mandibular molar vertical eruption per year, maxillary complex vertical growth per year, effective horizontal condylar growth per 8
27 year, ratio of effective horizontal pogonion movement to effective vertical pogonion movement, ratio of effective vertical condylar growth to the summation of maxillary, and mandibular vertical molar eruption plus maxillary complex vertical growth. This study shows that when properly used as a passive appliance, TPA is effective and safe for maintaining anchorage or space without unwanted vertical effects. Maybe the most fascinating part of TPA is its very versatile use as an active appliance with a very simple design. Here, instead of a passive fit, the TPA is activated before cementation or insertion depending on the different designs. First order discrepancies can be corrected effectively with TPA. In Ten Hoeve s patient s study [22], many cases treated successfully with the molars rotated by TPA were reported. In Anders Dahlquist s study in 1996 [23], large scale clinical trial of transpalatal arch for the correction of first molar rotation was conducted. Here, 50 patients (8-13 years of age) first molars were derotated with TPA, then the positions of the molars were compared with those in 34 individuals, aged years, with normal occlusion. Prefabricated (GAC) stainless steel TPA arches were used for days (median time 122 days). The effect was recorded with a measuring microscope on dental casts from before and after the treatment. Molar positions were determined from the tips of the four cusps of the tooth in relation to a coordinate system based on palatal reference points. The centers of rotation of the molars during derotation were calculated from the movement of their cusps. In about two-thirds of the cases the mesiobuccal cusp of the molar moved distally during the derotation. In the remaining cases it moved mesially or remained unchanged. The median distal movement was 0.3 mm on the right and 0.5 mm on the left side. Because many molars moved mesially, on average there was no gain in 9
28 space in the dental arch from the derotation. The location of the centre of derotation varied widely but it was on average located midway between the distobuccal and distopalatal cusps. In most cases the derotation resulted in a small, unintended, expansion. The study showed that mesiopalatally rotated first molars can effectively be derotated with the TPA, but the mesiodistal position of the mesiobuccal cusp is unpredictable. In vitro, first order correction was studied by Bengt Ingervall, et.al. The moments and forces of TPA induced molar rotation in vitro with stainless steel wire and TMA wires were measured [24]. It was found that both steel and TMA TPAs are effective at rotating the molars, however, at full activation, the steel arches delivered relatively large moments which decreased rapidly during deactivation. The TMA arches had a larger working range. It was not possible to achieve full symmetry of the moments at the two ends of the arch. The difference of the two moments resulted in forces acting on the two anchorage teeth in a mesio-distal direction. These forces were generally small but could reach clinically relevant magnitude. The derotation resulted in a contractive force of up to 2.7 N which has to be compensated for by expansion. This in vitro study also showed the effectiveness of activated TPA in rotating molars and its possible side effects. First order molar de-rotation was also studied with Zachrisson-type transpalatal bar (ZTPB) appliance. Elif Gunduz, et. al., [7, 8], studied the ZTPB s derotation character and compared it to Goshgarian-type palatal bar (GTPB) in vitro and in vivo. Moments and forces delivered during symmetrical derotation of upper molars by 10 Goshgariantype (GTPB) and 10 Zachrisson-type transpalatal bars (ZTPB) were measured in laboratory experiments using a computer-based strain gauge. Each end of the 20 passive 10
29 bars was symmetrically activated by 10 mm in the sagittal plane using a template. The activated bars were placed into lingual attachments of the measuring apparatus, and three consecutive measurement steps were taken for each bar. Measurements were taken when the attachments were at 0, 5, and 10 degrees of deactivation. The mesiodistal (sagittal) forces, the horizontal forces, and the moments of rotation at the right and left attachments were measured at each step. The horizontal forces and the moments of rotation of the two designs yielded statistically significant differences. Greater moments of rotation were produced by the GTPB. The ZTPB produced significantly lower contractive horizontal forces than the GTPB did at 5 and 10 degree of deactivation, demonstrating that ZTPB has some clinical relevant advantages to GTPB. Its load deflection rate is lower, thus, there could be lower initial moments at full activation and less or no reactivation during derotation. Also the horizontal contractive forces produced during deactivation were lower thus less compensation is needed. The authors attribute the characters to the different design of the ZTPB as the two small, distal-directed loops of the ZTPB give the bar flexibility, which makes engagement into the attachments easier with less activation loss. Also, at the beginning of derotation, these small loops show less closure; however, during derotation, when the central loop is closing, each loop opens itself at mm. This enables the ZTPB to produce less contractive forces during derotation of molars. These characters are further tested in vivo in two molar rotation cases [8], where the derotations were fully corrected in three months with proper use of the ZTPB. The authors also claimed that ZTPB can be successfully used for different treatment purposes besides upper molar derotation, such as expansion of the upper arch, maintaining arch 11
30 widths, supporting anchorage, improving vertical control, etc. Overall, these studies show ZTPB as a better TPA in certain clinical situations. Second order discrepancy can also be corrected effectively with TPA. However, instead of activation of TPA itself, most of the designs in the literature used TPA as passive anchorage for second order correction. Over-erupted molars can be intruded, and impacted molars can be extruded. Salem, et. al. soldered an additional spring distal to the molar attachment [25], and showed that clinically, this design can effectively intrude the over-erupted maxillary molars. The mechanics is comfortable, cost effective, and can work rapidly. Santoro, et. al. [26] added an additional hook distal to the TPA band joint and run elastics from the hook to the impacted molar, resulting in rapid extrusion and success with minimum side effect. Third order discrepancy can also be corrected effectively with TPA. In Falguni Mehta s study [27], Zachrisson-type transpalatal bars (ZTPB) was used to correct Maxillary second molar buccal crossbite together with E chain successfully. This approach helps to apply an isolated force on the buccally placed maxillary second molars without disturbing the anchorage unit and any undesired movement on the dentition, it also does not interfere with the physiologic eruption of teeth in the opposite arch. In addition, by running E chain crosses over the occlusal surface of Maxillary second molars, possible side effects of tooth extrusion, opening of the mandibular plane angle, and downward and backward rotation of the mandible, worsening of the profile associated with fixed orthodontic appliances and S - elastics are totally avoided. This study shows an interesting way to control third order discrepancy with a modified TPA. 12
31 Crossbite discrepancy can also be managed with a TPA. In Edsard van Steenbergen s study [28], the treatment of a unilateral dental crossbite was recommended to be performed with a lingual arch (0.032 x inch TMA) in the mandible and transpalatal arch (TPA) in the maxilla. In the case of a lingually tipped upper molar, a rigid arch wire is tied to all of the teeth except the molar in crossbite. Buccal root torque is placed in the TPA on the side that is not in crossbite. When the TPA is inserted into the bracket, the horizontal part of the TPA will be occlusal to the bracket on the crossbite side. In addition, expansion activation was built into the transpalatal arch. When this TPA is engaged, the force system created causes the desired buccal tipping of the molar in crossbite. This tipping movement occurs before translation of the molar on the contralateral side. The vertical forces, which act to cause intrusive and extrusive side effects on the two molars, are small and usually are not expressed because occlusal forces are far larger in magnitude. After the crossbite has been corrected, the wire is removed, made passive, and reinserted. This study provides a good protocol for molar crossbite correction with TPA appliance. In Bengt Ingervall s study [29], in vivo results were used to evaluate the activated TPA for crossbite correction. Thirty-five children from 6 years, 8 months to 15 years, 11 months old were studied. Fifteen of the children were treated with an arch activated for expansion only and 20 children with an arch activated in a similar way but with the inclusion of buccal root torque of the anchorage tooth. With both types of activation, the tooth in crossbite was allowed to tip buccally. The movements of the first molars as a result of the treatment were monitored by measurements on dental casts and frontal cephalometric roentgenograms. In the children treated with an arch activated only for expansion, the molars on both sides of the dental arch moved buccally 13
32 during the treatment. In the children treated by torque activation, on the other hand, there was a considerable buccal movement of the molar on the side of the crossbite without any significant buccal movement of the anchorage tooth. With both types of activation, there was only a slight change in inclination of the transverse occlusal plane through the first molars; the plane opened up slightly toward the side of the crossbite. The authors believe the results were satisfactory and recommended this kind of TPA activation for crossbite correction. This study showed that TPA can be properly activated to bring effective crossbite correction. Expansion can also be achieved with TPA. Baldini showed successful palatal expansion with Goshgarian-type palatal bars (GTPB) [30], and Bell, et al. demonstrated effective maxillary expansion during deciduous and mixed dentitions using a quad-helix appliance [13]. This expansion produced orthopedics midpalatal suture separation for early treatment in addition to the orthodontics changes. As quad helix appliance is a variance of TPA in a broad sense, these studies showed the effective expansion function of TPAs. Molar distalization can be done by the TPA as well. Mandurino, et. al. [31] modified the removable TPA slightly to make asymmetric distalization possible. Here the TPA arch is made from TMA wires and double wire ending was bent. By inserting distal to the lingual tube on the anchorage molar side and inserting medial to the tube of the molar needs to be distalized, mesiobuccal rotation of the anchor molar and distal force of the mesialized molar can be formed. Clinical cases proved this setup an effective, simple, hygienic, economic and easy way of molar distalization without anterior anchorage loss. 14
33 Temporary anchoring devices (TAD) including mini- NiTi implants are more and more used in everyday orthodontics practice. TPA can work nicely with the TADs to achieve needed forces. Heiner Wehrbein, et. al. [32], studied the sagittal deflection of TPAs of different dimensions attached to an implant abutment. After comparison of multiple diameter of TPA with multiple forces, the study showed x0.051 stainless steel TPAs can be used when maximum anchorage is needed. Like any other orthodontics appliances, careless use of the TPA can bring problems and side effects. Trauma is one of the problems and side effects TPA may cause. Ng ang'a, et. al. [33], reported cases of possible hazards of TPA use. In an extraction case, maximum anchorage was designed and TPA was used for anchorage together with headgear. This particular TPA is Goshgarian-type palatal bar (GTPB) with mesial central loop. As the anterior segment moved posteriorly, and without headgear compliance, the mesial loop of the GTPB became partially embedded in the palatal mucosa. This could have been prevented with better patient compliance, better parent education and shorter visit intervals. In another case, a removable TPA was used with bent back double wire ends. The ends were ligated into the molar band lingual tube with elastic chains. However, with time, mastication and other oral movements, one end dislodged from the lingual tube and thus the central loop of the GTPB became embedded in the palatal mucosa. This also could have been prevented with shorter visit intervals, frequent check for looseness and palatal clearance, frequent change of elastics, or stainless steel ligature. Another type of side effects come from biomechanical considerations. Yukio Kojima [34] performed a finite element simulation to study the effects of transpalatal arch on molar movement produced by mesial force. The paper claimed passive TPA can prevent both 15
34 rotation and buccolingual tipping of the molars, and also maintains the transverse distance of the molars by mechanical rigidity of the TPA. However, after finite element simulation, it was found that the initial movement produced by elastic deformation of the periodontal ligament, stress magnitude in the periodontal ligament was not changed by the TPA. In the orthodontic movement produced by bone remodeling, the mesial force tipped the anchor teeth irrespective of the TPA. The tipping angles of anchor teeth with and without the TPA were almost the same. The anchor teeth without the TPA were rotated in the occlusal plane and moved transversely. The authors concluded that based on the calculation, The TPA had no effect on the initial movement. Although this conclusion was made, it is only valid when the assumptions used in this calculation are satisfied. In addition, after the theoretical initial movement, maxillary molars large lingual roots will contact the lingual plate and acts as a pivot to make the 2 buccal roots to rotate mesiolingually. Then here the TPA reduces anterior molar movement by coupling the right and left permanent molars together and thus eliminate rotations. As a common clinical observation, buccal root torque to upper molars with Goshgarian-type palatal bar (GTPB) without appropriate adjustments of the arch width can produce, initially, an adverse buccal tipping of the molar crowns. In Baldini G s [35] study, an in vitro experiment was performed on the forces and moments produced by GTPB when symmetrical buccal root torque was applied. The torque moments and expansive lateral forces developed by nine different arch forms of varying height and width were measured and the corresponding moment-to-force ratios were calculated at three different torque levels. It was found that the moment-to-force ratio acting on the upper molars depended mainly on the amount of torque applied and the arch height. This 16
35 indicates that when low palatal bars are used, the application of buccal root torque of clinically relevant amounts leads to an initial buccal crown tipping, whereas the same amounts of torque, when applied by means of high arches, bring about an initial buccal root tipping. This study also claimed that interaction between torque moment and lateral force is not constant but arch form dependent, and the moment to force ratio will change as soon as the teeth move. Aiming to minimize the unwanted side effects, theoretical investigations of TPA have been carried out. However, the biomechanical understanding of the removable TPA is complex because it is a two-bracket system constrained at both ends. In this system, the wire can move neither in nor out of the molar sheaths on either side. Constraining forces that cannot be intuitively predicted are introduced into the system caused by the rigidity and fixed length of the transpalatal wire. The addition of these new forces may affect tooth movement. Accurately account for all of these forces is difficult. To make the analysis easier, Joe Rebellato [9] uses a static approach focused only at time point zero to analysis the force and moment equilibrium system. Multiple scenarios were included in the theoretical analysis. In symmetrical bilateral expansion and constrictions, the opposite force in bilateral molars cancelled out, and the opposite moment also cancelled out. The system can reach balance with no side effect. In symmetrical bilateral first order activations of mesiofacial rotations, bilateral toe ins in the occlusal plane will produce bilateral mesiofacial rotations, and the equal and opposite forces and moments will also cancel each other out, no side effects exists when system reach balance. 17
36 In symmetrical bilateral first order activations of mesiolingual rotations, similarly, bilateral toe outs in the occlusal plane will produce bilateral mesiolingual rotations, and the equal and opposite forces and moments will also cancel each other out, no side effects exists when system reach balance. In bilateral second order activation where mesiodistal tipping is desired, as constraint from TPA wire will prevent second order rotation of molars around their center of resistances, the center of rotation will be more occlusal, thus mesial and distal root torque of the molar roots are expected. In bilateral third order activation where buccal root torques are desired, the symmetrical toe ins in the frontal plane will bring equal and opposite force and moment, However, the system is constrained and the stiffness of the palatal arch will help to maintain the inter-sheath distance. The stiffness of the wire imposes a facially directed force acting at the molar sheaths and the center of resistances of the teeth will move facially because of this force. The instantaneous center-of-rotation in this situation moved occlusally and closer to the molar sheaths. In unilateral first order activations of mesiofacial rotations, as the moment are no longer symmetrical, to keep the moment sum as zero, the rotated molar will have a mesial force and the other molar will have a distal force as side effect. In unilateral first order activations of mesiolingual rotations, as the moment are no longer symmetrical, to keep the moment sum as zero, the rotated molar will have a distal force and the other molar will have a mesial force as side effect. 18
37 In unilateral third order activation of facial root torque, as the moment are no longer symmetrical, to keep the moment sum as zero, the rotated molar creates an intruding force and the other molar will have a extruding force as side effect. To make the clinical insertion of activated TPA end easier for insertion, step bends can be used instead of single bend. Here couples at the brackets that are always in the same direction and the associated equilibrium forces will also be additive. Thus, step bends are an efficient way of increasing the magnitude of the equilibrium forces without greatly increasing the angle of entry at a sheath. Thus the clinical insertion becomes much easier but the biomechanics is still the same as discussed above. As the TPA force system is very shape-sensitive, with the consideration of the undesirable side effects and practical clinical use, Burstone, et. al. [36] theoretically calculated the right arch forms for each clinical situation with a computer. In forming the precise TPA shape, the reactive force approach is compared with the iterative force approach and the iterative force approach is determined to be much more accurate thus was used. This study analyzed common clinical scenarios for using TPA and suggested theoretical solutions to common side effects.. Overall, a TPA and LA are commonly used appliances in clinical orthodontics treatment with many varied design modifications.. Clinically, TPA and LA are versatile, however, side effects are common. Theoretical biomechanics analysis of the appliances were performed to maximize the expected effects and minimize the side effects, however, well designed quantified in vitro comparison have not been available before this study. 19
38 CHAPTER TWO COMPARISON OF TWO METHODS OF TRANSPALATAL ARCH AND LINGUAL ARCH ACTIVATION by Taoran Zhang Master of Science, Graduate Program in Orthodontics Loma Linda University, August 2016 Dr. Rodrigo Viecilli, Chairperson 20
39 Abstract The TPA and LA can be activated with two methods: the shape-driven method where the appliance is made to match the final tooth position and the force-driven method where the appliance is made to make sure the force system delivered by it at the beginning is consistent with the planned tooth movement. This study compared the two methods in vitro quantitatively with typodont teeth and multi-axis force torque transducers in all three dimensions. Results: In the TPA first order activation, with comparable Fy (force on Y axis) reading, the shape-driven activation group had a significantly higher Mx (moment on X axis) reading than the force-driven activation group. In the TPA second order activation, with comparable My (moment on Y axis) reading, the shape-driven activation group had a significantly higher Fx (Force on X axis) reading than the force-driven activation group. In the TPA third order activation, with comparable Mx (moment on X axis) reading, the shape-driven activation group had a significant higher Fy (force on Y axis) reading than the force-driven activation group. In the LA first order activation, with comparable Fy (force on Y axis) reading, the shapedriven activation group had a significantly higher Mz (moment on Z axis) reading than the force-driven activation group. In the LA second order activation, with comparable My (moment on Y axis) reading, the shape-driven activation group had a significantly higher Fz (force on Z axis) reading than the force-driven activation group. In the LA third order activation, the shape-driven activation method resulted in the exact same shape as the force-driven activation method, no comparison between the two activation methods was needed and both method yielded the same result. Conclusion: Both TPA and LA activated using the force-driven method exhibited lesser unintended side effects in first, 21
40 second and third order forces and moments than the shape-driven method. As the targeted tooth movements can be helped or hindered by the side effects, clinicians can refer to the results to make the correct activations for the most efficient and effective tooth movements. 22
41 Introduction Statement of the Problem The transpalatal arch (TPA) is a commonly used appliance in clinical orthodontics treatment [6]. Many different designs have been developed and tested including the Goshgarian type [37], the Zachrisson type [8], the removable type [9], the Precision lingual arch [10, 12], The Butterfly Arch TPA [18], etc. TPA and LA (Lingual arch) can be used passively for anchorage[7, 19] or actively for tooth movement in first order [8, 22, 23], second order [25, 26] and third order[27]. Although TPA and LA are very versatile and can be used to move tooth efficiently in many conditions, unwanted tooth movements can result from less than ideal initial activations. The TPA and lingual arch can be activated with two methods [38]. The first method is shape-driven method, where the appliance wire is fabricated to the ideal arch shape when it is passive. The wire is then elastically bent and placed into the maligned brackets for activation. Although this is straightforward and easy to fabricate, this activation usually brings large unnecessary initial moments to the teeth, thus results the undesirable side effects of round tripping movements of the teeth. The second activation method is force-driven method. To eliminate the unwanted side effects of the shape-driven method, and to give tooth the desired initial force system, a force-driven method has been developed. In this method, correct starting force is prioritized over establishing the ideal final tooth position. This initial force-driven activation can be achieved theoretically with computer calculation based on beam theory and iterative methods, it can also be achieved in five steps at chair side clinically. The first step is to determine the desired force system, the second step is to 23
42 make an appliance arch form passive to the original teeth position, the third step is a simulation shaping of the appliance by the deactivation force system, the fourth step is to permanently deform the appliance to be identical to the simulated deactivated shape, and the fifth step is trial activation in the mouth to make sure no unwanted moments exists. In theory, this force-driven activation method is more efficient than the shape-driven method by delivering the correct force system initially within the optimal force level zone, so the tooth can move directly to the target position without unnecessary wiggling or side effects. The purpose of this study is to compare the shape-driven activation method and force-driven activation method quantitatively in vitro. The forces and moments in all three dimensions were compared. Comparing the force system of both methods at the beginning will establish which one is closer to the ideal, and validate or refute the Burstone method of activation. The clinician will be able to consciously choose the method that better suits the specific case scenario. Hypothesis The central null hypothesis is that there is no difference for the forces in all three dimensions with the two methods of transpalatal arch and lingual arch activation. There is also no difference for the moments in all three dimension created with the two activation methods. This can be divided into sub-hypotheses as follows: 1. The force on the X axis is not different between the two methods of TPA activation for first order. 2. The force on the X axis is not different between the two methods of TPA activation for 24
43 the second order. 3. The force on the X axis is not different between the two methods of TPA activation for the third order. 4. The force on the Y axis is not different between the two methods of TPA activation for the first order. 5. The force on the Y axis is not different between the two methods of TPA activation for the second order. 6. The force on the Y axis is not different between the two methods of TPA activation for the third order. 7. The force on the Z axis is not different between the two methods of TPA activation for the first order. 8. The force on the Z axis is not different between the two methods of TPA activation for the second order. 9. The force on the Z axis is not different between the two methods of TPA activation for the third order. 10. The force on the X axis is not different between the two methods of LA activation for the first order. 11. The force on the X axis is not different between the two methods of LA activation for the second order. 12. The force on the X axis is not different between the two methods of LA activation for the third order. 13. The force on the Y axis is not different between the two methods of LA activation For the first order. 14. The force on the Y axis is not different between the two methods of LA activation 25
44 for the second order. 15. The force on the Y axis is not different between the two methods of LA activation for the third order. 16. The force on the Z axis is not different between the two methods of LA activation for the first order. 17. The force on the Z axis is not different between the two methods of LA activation for the second order. 18. The force on the Z axis is not different between the two methods of LA activation for the third order. 19. The moment on the X axis is not different between the two methods of TPA activation for the first order. 20. The moment on the X axis is not different between the two methods of TPA activation for the second order. 21. The moment on the X axis is not different between the two methods of TPA activation for the third order. 22. The moment on the Y axis is not different between the two methods of TPA activation for the first order. 23. The moment on the Y axis is not different between the two methods of TPA activation for the second order. 24. The moment on the Y axis is not different between the two methods of TPA activation for the third order. 26
45 25. The moment on the Z axis is not different between the two methods of TPA activation for the first order. 26. The moment on the Z axis is not different between the two methods of TPA activation for the second order. 27. The moment on the Z axis is not different between the two methods of TPA activation for the third order. 28. The moment on the X axis is not different between the two methods of LA activation for the first order. 29. The moment on the X axis is not different between the two methods of LA activation for the second order. 30. The moment on the X axis is not different between the two methods of LA activation for the third order. 31. The moment on the Y axis is not different between the two methods of LA activation for the first order. 32. The moment on the Y axis is not different between the two methods of LA activation for the second order. 33. The moment on the Y axis is not different between the two methods of LA activation for the third order. 34. The moment on the Z axis is not different between the two methods of LA activation for the first order. 27
46 35. The moment on the Z axis is not different between the two methods of LA activation for the second order. 36. The moment on the Z axis is not different between the two methods of LA activation for the third order. Materials and Methods In this in vitro study, typodont was used initially for the setup. Anatomically rooted metal teeth from Kilgore TM International Inc. was used for the typodont. The maxillary permanent first molars were cemented with molar bands from Ormco TM, and precision lingual hinge caps from Ormco TM were welded to the molar bands. Removable TPA linked to the molars was made from x0.032 TMA burstone arch form from Ormco TM, and removable LA linked to the molars was made from x0.032 TMA burstone arch form from Ormco TM. After typodont setup, teeth were bonded to steel rods with J-B Weld TM 8280 Steel Reinforced Epoxy, and the steel rods were linked to multiaxis force torque transducers Nano17 from ATI Industrial Automation TM, Apex, NC. The signals were acquired with NI USB-6229 data acquisition device from National Instruments TM, and analyzed in a computer with OFM F/T DAQ TM software. With this setup, the forces and moments can be captured and measured in all three dimension for evaluation. Calibration With TPA or LA appliances attached to the lingual slots, the teeth were removed from the typodont for independent measurements. As the lingual slots positions were 28
47 different from the transducers measuring point, a moment was measured by the transducer when pure force and no moment were applied to the lingual slot point. To make the calculation easier and to make the measurement meaningful, calibration files were generated for each transducer to make sure when forces are applied at the lingual slot, all moments in three dimension were zero. These specific calibration files were loaded into the software for all the following measurements so the data collected below were true forces and moments at the points of the lingual slots. Axis and moment definition As depicted in figure 1, 2, 3, positive or negative forces in X, Y, Z direction are defined as following: X axis is defined as the straight line perpendicular to the coronal plane. The direction toward anterior is defined as positive, and the direction toward posterior is defined as negative. Y axis is defined as the straight line perpendicular to the sagittal plane. The direction toward left is defined as positive, and the direction toward right is defined as negative. Z axis is defined as the straight line perpendicular to the transverse plane. The direction toward upward is defined as positive, and the direction toward downward is defined as negative. Then according to the right hand rule (Figure 4), positive moments direction was defined as the right thumb direction when the right fingers point in the direction of the first vector direction, and then curled towards the second vector. 29
48 30
49 31
50 Data Collection 32

51 The overall grouping is shown in Table 1. 33
52 Comparison 1: PT1 vs. ST1 vs. FT1 For this part, 1st order activation of TPA was compared in 3 groups, and in each group, 10 appliances are tested. In the group PT1 (Passive TPA 1st order activation), the TPA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 5, 6 and Figure 7. In the group ST1 (Shape-driven TPA 1st order activation), the TPA was activated in the first order with the shape-driven method. Specifically, the TPA was bent into the targeted finishing form with 7mm transverse expansion, then the TPA is engaged into the lingual slots without consideration of initial forces and moments. This setup is illustrated in Figure 8, 9 and Figure 10. In the group FT1 (Force-driven TPA 1st order activation), the TPA was activated in the first order with the force-driven method. Similarly, 7mm transverse expansion was placed in the TPA. However, this is done with the simulation activation, copy the activation form and making the activation form passive. Then the new form was engaged into the lingual slots to give optimum initial forces. This setup is illustrated in Figure 11, 12 and Figure 13. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. Fz: force in the Z axis direction. Mx: moment in the X axis direction. 34
53 My: moment in the Y axis direction. Mz: moment in the Z axis direction. 35
54 Comparison 2: PT2 vs. ST2 vs. FT2 Second order activation of TPA was compared among the three groups, and in each group, 10 appliances were tested. In the PT2 group (Passive TPA 2nd order activation), the TPA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 14, 15 and Figure 16. In the ST2 group (Shape-driven TPA 2nd order activation), the TPA was activated in the second order with the shape-driven method. Specifically, the TPA leg engaging to maxillary right first molar was bent 30 degree for distal crown tipping, and the TPA leg engaging to maxillary left first molar was bent 30 degree for mesial crown tipping, then the TPA is engaged into the lingual slots without consideration of initial forces and moments. This setup is illustrated in Figure 17, 18 and Figure 19. In the FT2 group (Force-driven TPA 2nd order activation), the TPA was activated in the second order with the force-driven method. Similarly, 30-degree distal crown tipping for maxillary right first molar and 30-degree mesial crown tipping for maxillary left first molar was placed in the TPA. However, this is done with the simulation activation, copying the activation form, and making the activation form passive. Then the new form was engaged into the lingual slots to give optimum initial forces. This setup is illustrated in Figure 20, 21 and Figure 22. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. 36
55 Fz: force in the Z axis direction. Mx: moment in the X axis direction. My: moment in the Y axis direction. Mz: moment in the Z axis direction. 37
56 38
57 Comparison 3: PT3 vs. ST3 vs. FT3 Third order activation of TPA was compared in 3 groups, and in each group, 10 appliances were tested. In the PT3 group (Passive TPA 3rd order activation), the TPA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 23, 24 and Figure 25. For the ST3 group (Shape-driven TPA 3rd order activation), the TPA was activated in the third order with the shape-driven method. Specifically, the TPA legs engaging to maxillary first molars were bent 30 degrees for buccal crown torque (lingual root torque); then the TPA was engaged into the lingual slots without consideration of initial forces and moments. This setup is illustrated in Figure 26, 27 and Figure 28. In the FT3 group (Force-driven TPA 3rd order activation), the TPA was activated in the third order with the force-driven method. Similarly, 30 degree buccal crown torques (lingual root torques) for maxillary first molars were placed in the TPA. However, this is done with the simulation activation, copy the activation form and making the activation form passive. Then the new form was engaged into the lingual slots to give optimum initial forces. This setup is illustrated in Figure 29, 30 and Figure 31. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. Fz: force in the Z axis direction. Mx: moment in the X axis direction. 39
58 My: moment in the Y axis direction. Mz: moment in the Z axis direction. 40
59 Comparison 4: PL1 vs. SL1 vs. FL1 For this part of the comparison, first order activation of LA was compared in 3 groups, and in each group, 10 appliances were tested. In the PL1 group (Passive LA 1st order activation), the LA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 32, 33 and Figure 34. In the SL1group (Shape-driven LA 1st order activation), the LA was activated in the first order with the shape-driven method. Specifically, the LA was bent into the targeted finishing form with 10mm transverse expansion, then the LA is engaged into the lingual slots without consideration of initial forces and moments. This setup is illustrated in Figure 35, 36 and Figure 37. In the FL1 group (Force-driven LA 1st order activation), the LA was activated in the first order with the force-driven method. Similarly, the LA was bent into the targeted finishing form with 10mm transverse expansion. However, this is done with simulation activation, copying the activation form and making the activation form passive. Then the new form was engaged into the lingual slots to give optimum initial forces. This setup is illustrated in Figure 38, 39 and Figure 40. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. Fz: force in the Z axis direction. Mx: moment in the X axis direction. 41
60 My: moment in the Y axis direction. Mz: moment in the Z axis direction. 42
61 Comparison 5: PL2 vs. SL2 v.s FL2 Second order activation of LA was compared in 3 groups, and in each group, 10 appliances were tested. For the PL2 group (Passive LA 2nd order activation), the LA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 41, 42 and Figure 43. In the SL2 group (Shape-driven LA 2nd order activation), the LA was activated in the second order with the shape-driven method. Specifically, the LA leg engaging to maxillary right first molar was bent 30 degree for distal crown tipping, and the LA leg engaging to maxillary left first molar was bent 30 degree for mesial crown tipping, then the LA was engaged into the lingual slots without consideration of initial forces and moments. This setup is illustrated in Figure 44, 45 and Figure 46. For the FL2 group (Force-driven LA 2nd order activation), the LA was activated in the second order with the force-driven method. Similarly, the LA leg engaged to maxillary right first molar was bent 30 degree for distal crown tipping, and the LA leg engaged to maxillary left first molar was bent 30 degree for mesial crown tipping, however, this is done with the simulation activation, copying the activation form, and making the activation form passive. Then the new form was engaged into the lingual slots to give optimum initial forces. This setup is illustrated in Figure 47, 48 and Figure 49. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. 43
62 Fz: force in the Z axis direction. Mx: moment in the X axis direction. My: moment in the Y axis direction. Mz: moment in the Z axis direction. 44
63 Comparison 6: PL3 vs. SL3 vs. FL3 Third order activation of LA was compared. As in this setup, the shape-driven activation method resulted in the exact same shape as the force-driven activation method. No comparison between the two activation methods is needed; and both methods yielded the same result. So in this setup, 2 groups were compared, and in each group, 10 appliances were tested. In the PL3 group (Passive LA 3rd order activation), the LA was made to be passive to the molar lingual slots. Due to the total passiveness, all forces and moments in three dimensions were expected to be zero or minimum. This setup is illustrated in Figure 50, 51 and Figure 52. For the group SL3 group (Shape-driven LA 3rd order activation), which is also the FL3 group (Force-driven LA 3rd order activation), the LA was activated in the third order with the shape-driven method, which showed the same result as the force-driven method. Specifically, the LA legs engaging to maxillary first molars were bent 30 degree for buccal crown torque (lingual root torque), then the LA was engaged into the lingual slots for measurements. This setup is illustrated in Figure 53, 54 and Figure 55. From all three groups, the following data were collected for both transducers. Fx: force in the X axis direction. Fy: force in the Y axis direction. Fz: force in the Z axis direction. Mx: moment in the X axis direction. My: moment in the Y axis direction. Mz: moment in the Z axis direction. 45
64 Statistical Analysis Statistical analyses were performed using Microsoft Excel with QI MACRO modules. Descriptive statistics was employed as mean ± standard deviation as the data were normally distributed. The results from the 3 groups were compared using ANOVA followed by individual post-hoc tests with Scheffe s procedure. Statistical significance is denoted when p<0.05. The specific comparisons are noted in Table 1. 46

65 Results Comparison 1: PT1 vs. ST1 vs. FT1 Results of comparison in this group are summarized in Tables 2, 3, 4, 5 and Figures 56, 57, 58,
66 48
67 49
68 50
69 51
70 52
71 In this comparison, horizontal expansion forces are given to the lingual slots of maxillary first molars for 7mm expansion. Forces comparisons in x, y, z axis are listed in table 2, 3, they are also drawn in figure 56, 58. The passive group shows minimal activation in all three axes, indicating a low force noise level in the system setup. There were no statistical significant differences in forces in x,y and z axis between shape-driven activation group and force-driven activation group. 53

72 Moment comparisons in x, y, z axis are listed in table 4, 5, they are also drawn in figure 57, 59. The passive group shows minimal moment in all 3 axis, indicating a low moment noise level in the system setup. There are no statistical significant differences in moments in y and z axes between shape-driven activation group and force-driven activation group. There is a statistical significant difference in moments in x axis between shape-driven activation group and force-driven activation group, specifically, the shape-driven activation group has a / Nmm moment on the x axis for transducer 1 and a / Nmm moment on the x axis for transducer 2; in comparison, the forcedriven activation group has a / Nmm moment on the x axis for transducer 1 and a / Nmm moment on the x axis for transducer 2. Comparison 2: PT2 vs. ST2 vs. FT2 Results of comparison in this group are summarized in Tables 6, 7, 8, 9 and Figures 60, 61, 62,
73 55
74 56
75 57
76 58
77 In this comparison, distal crown tipping moments are given to the lingual slots of maxillary right first molar, and mesial crown tipping moments are given to the lingual slots of maxillary left first molar. Forces comparisons in x, y, z axis are listed in Table 6, 7, and they are also drawn in Figure 60, 62. The passive group showed minimal activation in all three axes, indicating a low force noise level in the system setup. There are no statistical significant differences in forces in y and z axis between the shape-driven activation group and force-driven activation group. There is statistical significant difference in forces in x axis between shape-driven activation group and force-driven activation group. 59
78 Moment comparisons in x, y, z axis are listed in Table 8, 9, they are also drawn in Figure 61, 63. The passive group shows minimal moments in all three axes, indicating a low moment noise level in the system setup. There are no statistical significant differences in moments in x and y axis between the shape-driven activation group and force-driven activation group, and there is a negative moment in z axis in the shapedriven activation group due to total moment equilibrium. Comparison 3: PT3 vs. ST3 vs. FT3 Results of comparison in this group are summarized in Tables 10, 11, 12, 13 and Figures 64, 65, 66,
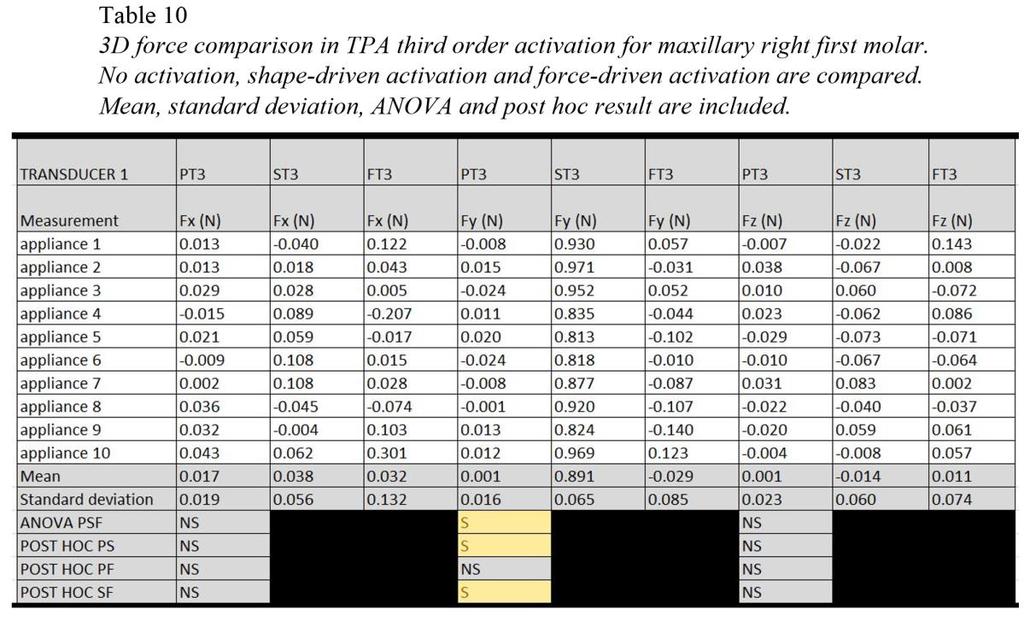
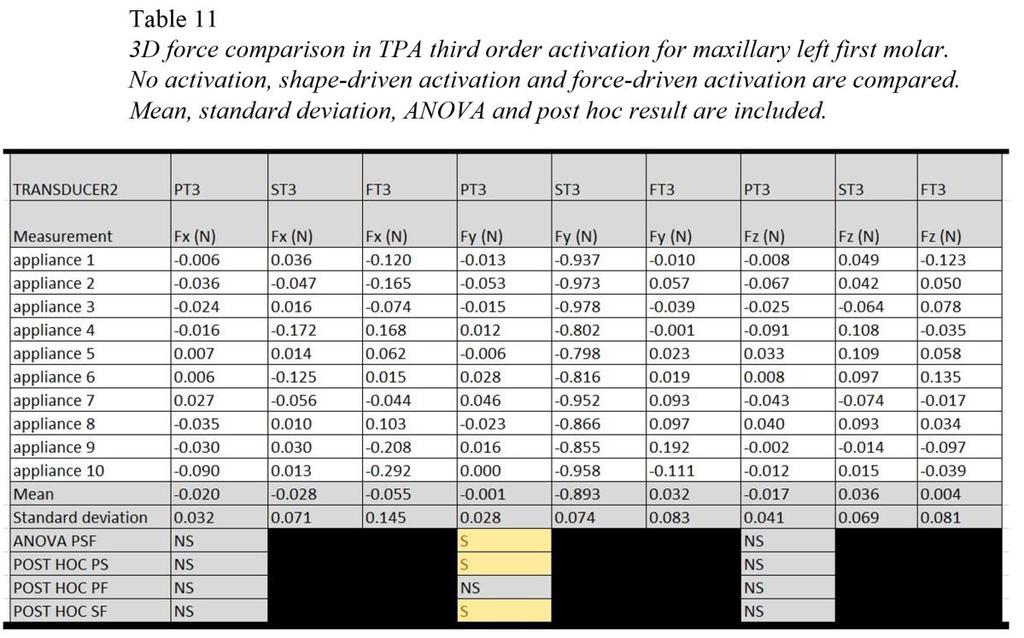
79 61
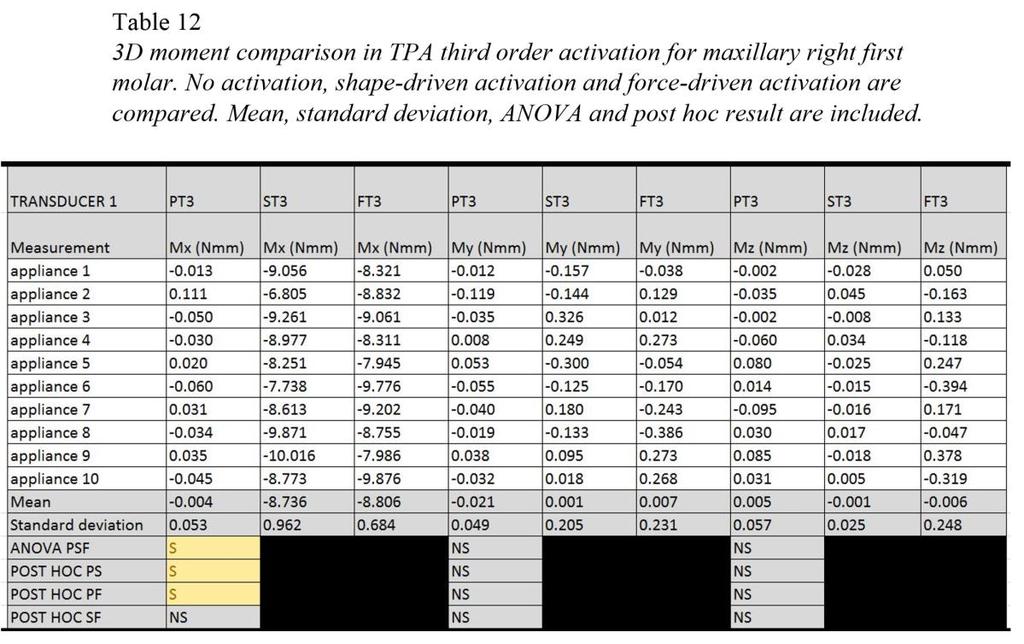
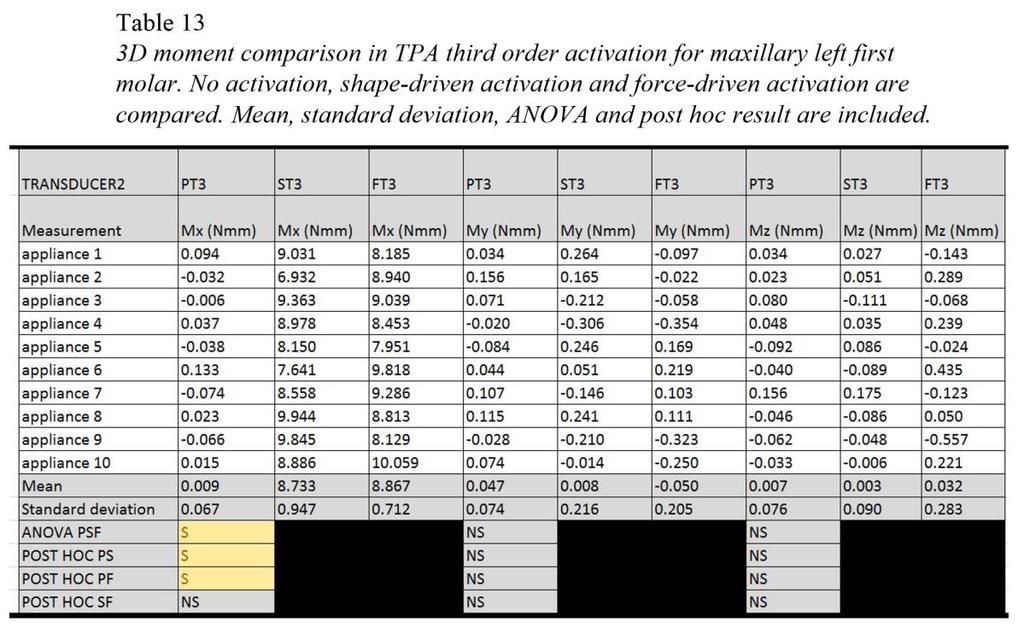
80 62
81 63
82 64
83 65
84 In this comparison, buccal crown torque moments are given to the lingual slots of maxillary first molars for 30 degree activation. Forces comparisons in x, y, z axis are listed in Table 10, 11 and are also drawn in Figure 64, 66. The passive group showed minimal activation in all three axes, indicating a low force noise level in the system setup. There are no statistical significant differences in forces in x and z axis between the shape-driven activation group and the force-driven activation group. There is statistical 66
85 significant difference in forces in y axis between shape-driven activation group and forcedriven activation group; specifically, the shape-driven activation group had a / N force on the y axis for transducer 1, and a / N force on the y axis for transducer 2; while the force-driven activation activation group had a / N force on the y axis for transducer 1, and a / N force on the y axis for transducer 2. Moment comparisons in x, y, z axis are listed in Table 12, 13, and are also drawn in Figure 65, 67. The passive group showed minimal moments in all three axes, indicating a low moment noise level in the system setup. There are no statistical significant differences in moments in y and z axis between the shape-driven activation group and the force-driven activation group. Comparison 4: PL1 vs. SL1 vs. FL1 Results of comparison in this group are summarized in Tables 14, 15, 16, 17 and Figures 68, 69, 70,
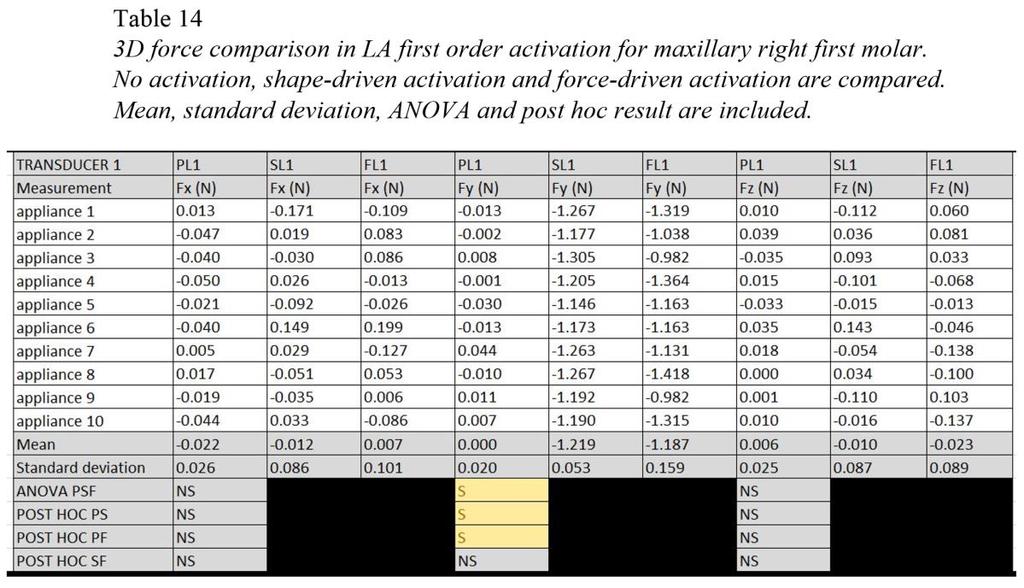
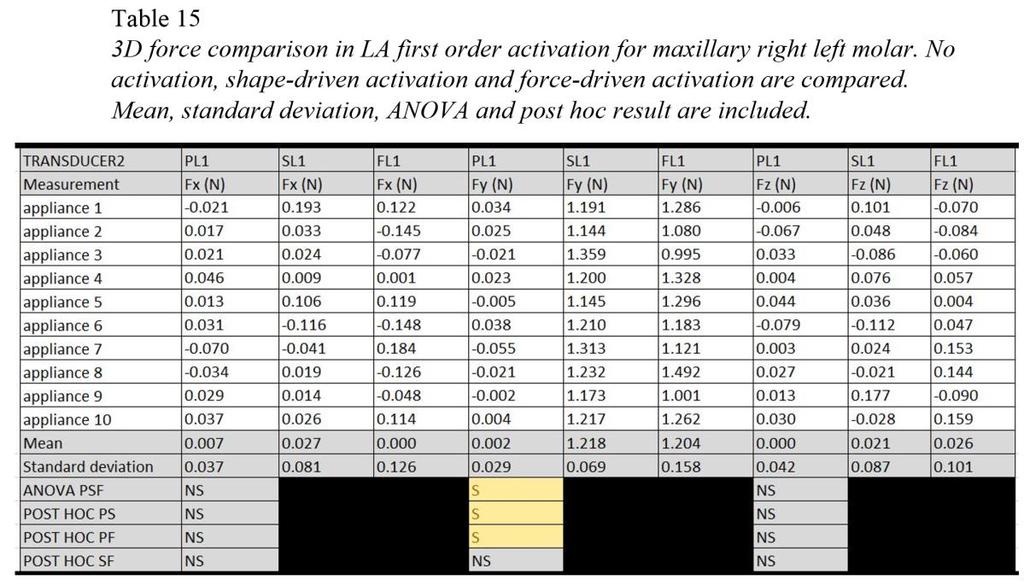
86 68
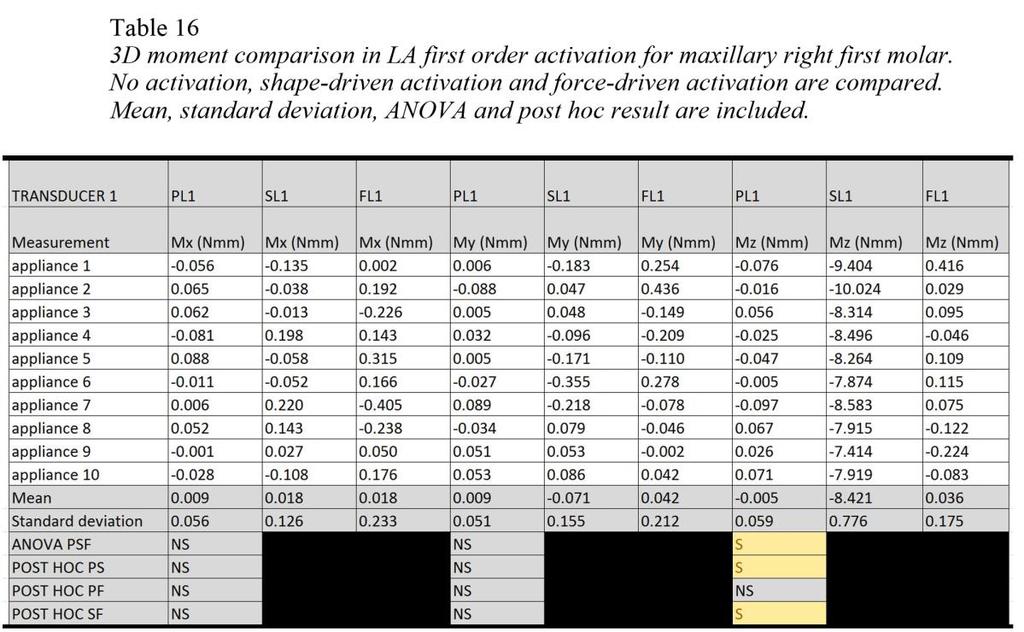
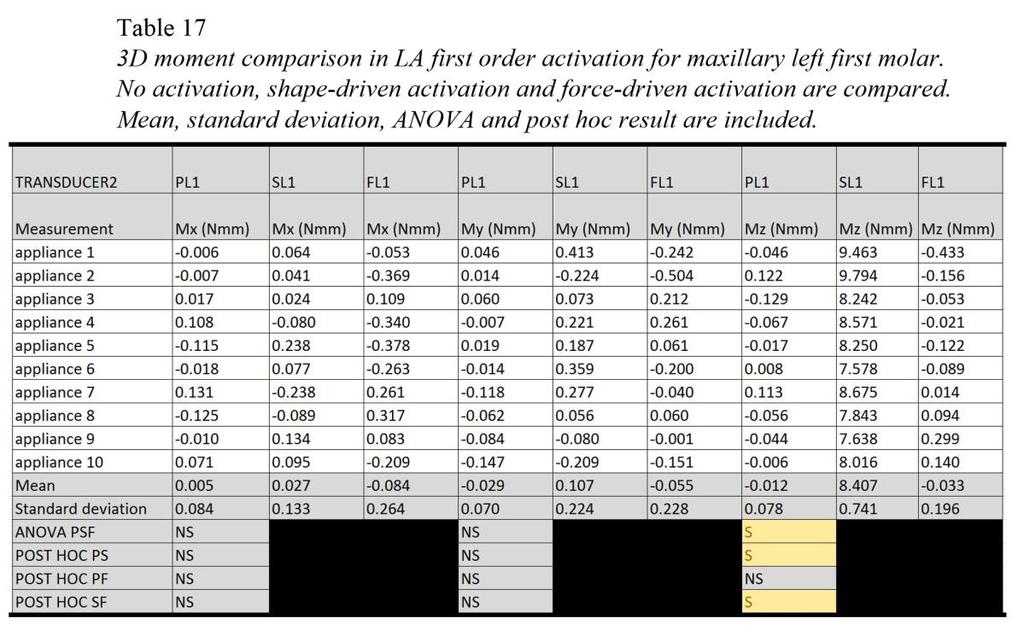
87 69
88 70
89 71
90 72
91 In this comparison, horizontal expansion forces are given to the lingual slots of maxillary first molars for 10mm expansion. Forces comparisons in x, y, z axis are listed in Table 14, 15 and drawn in Figure 68, 70. The passive group showed minimal activation in all three axes, indicating a low force noise level in the system setup. There 73
92 are no statistical significant differences in forces in x, y and z axes between the shapedriven activation group and the force-driven activation group. Moment comparisons in x, y, z axis are listed in Table 16, 17 and drawn in Figure 69, 71. The passive group showed minimal moment in all three axes, indicating a low moment noise level in the system setup. There are no statistical significant differences in moments in x and y axis between the shape-driven activation group and the force-driven activation group. There is a statistical significant difference in moments in z axis between the shape-driven activation group and the force-driven activation group, specifically, the shape-driven activation group had a / Nmm moment on the z axis for transducer 1, and a / Nmm moment on the z axis for transducer 2; and the force-driven activation group had a / Nmm moment on the z axis for transducer 1, and a / Nmm moment on the z axis for transducer 2. Comparison 5: PL2 vs. SL2 vs. FL2 Results of comparison in this group are summarized in Tables 18, 19, 20, 21 and Figures 72, 73, 74,
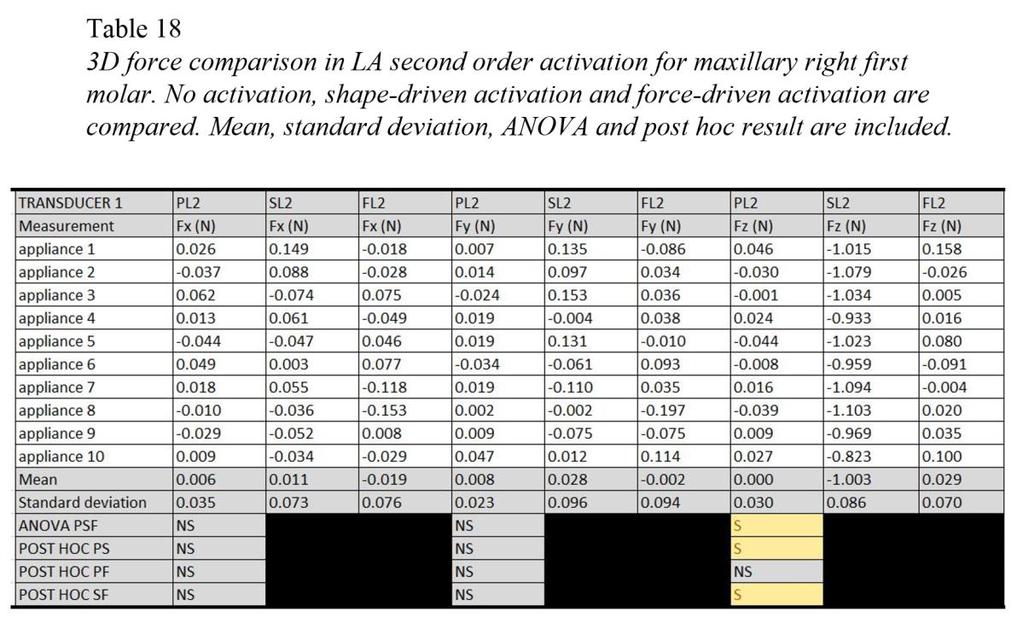
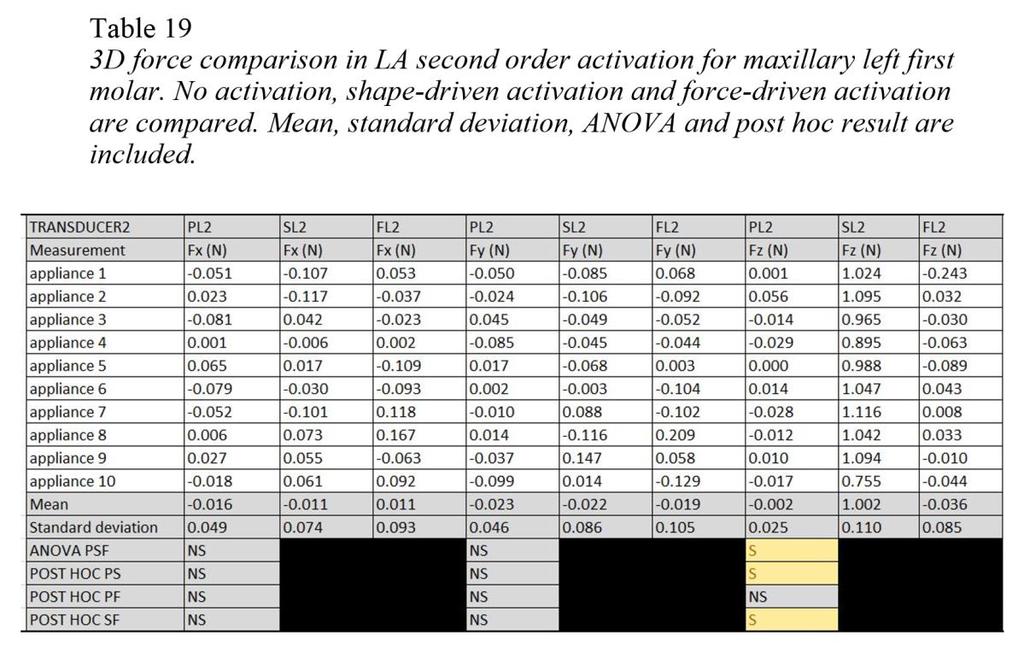
93 75
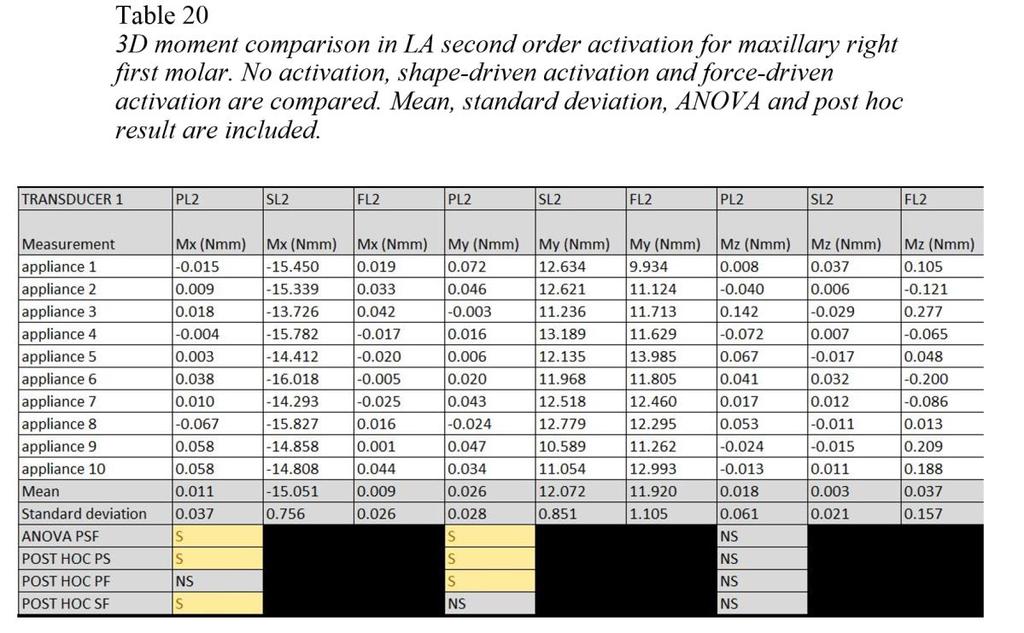
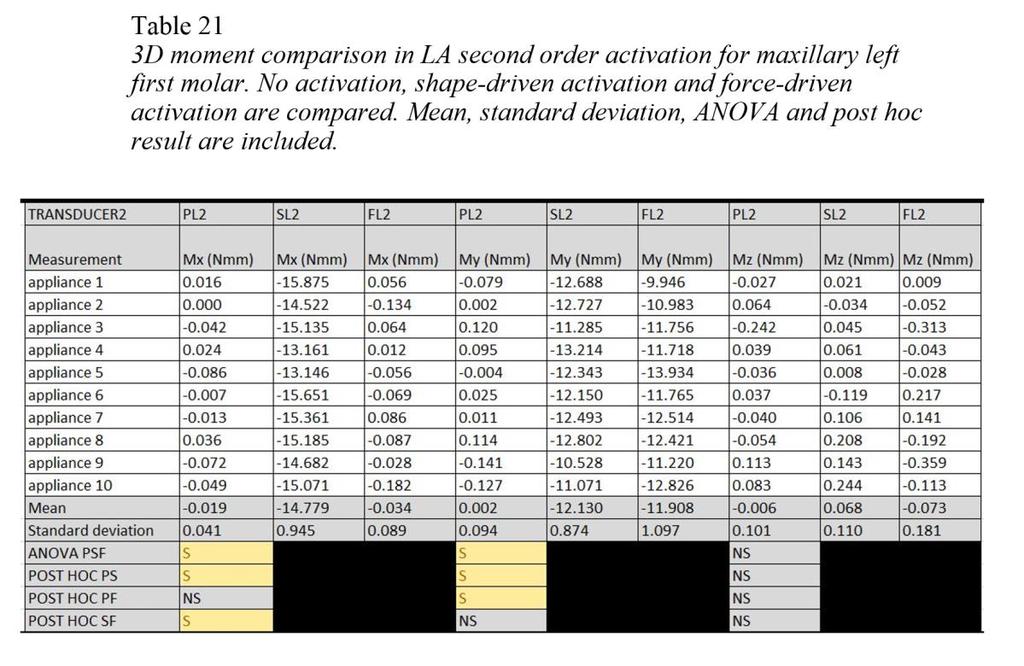
94 76
95 77
96 78
97 79
98 In this comparison, distal crown tipping moments are given to the lingual slots of maxillary right first molar, and mesial crown tipping moments are given to the lingual slots of maxillary left first molar. Forces comparisons in x, y, z axis are listed in Table 18, 19 and drawn in Figure 72, 74. The passive group showed minimal activation in all three axes, indicating a low force noise level in the system setup. There are no statistical significant differences in forces in x and y axis between the shape-driven activation group and the force-driven activation group. There is statistical significant difference in forces in z axis between the shape-driven activation group and the force-driven activation group. 80
99 Moment comparisons in x, y, z axis are listed in table 20, 21, they are also drawn in figure 73, 75. The passive group shows minimal moments in all 3 axis, indicating a low moment noise level in the system setup. There are no statistical significant differences in moments in y and z axis between shape-driven activation group and force-driven activation group, and there is a negative moment in x axis in the shape-driven activation group due to total moment equilibrium. Comparison 6: PL3 vs. SL3 vs. FL3 Results of comparison in this group are summarized in Tables 22, 23, 24, 25 and Figures 76, 77, 78,
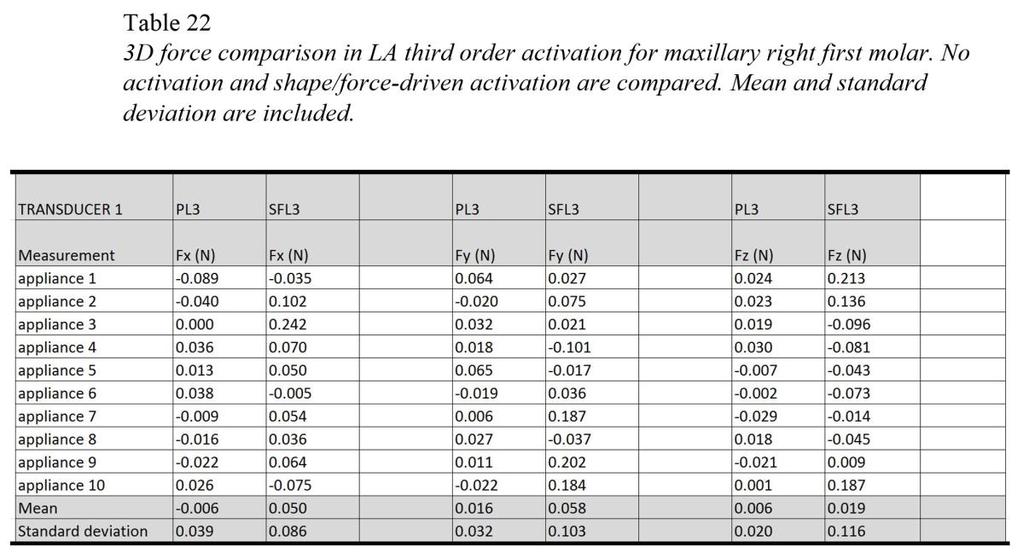
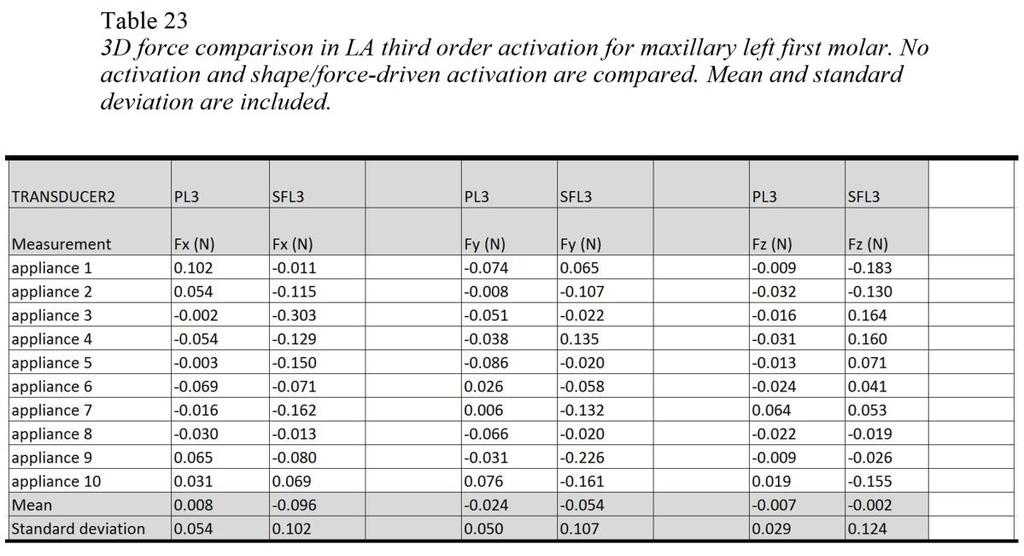
100 82
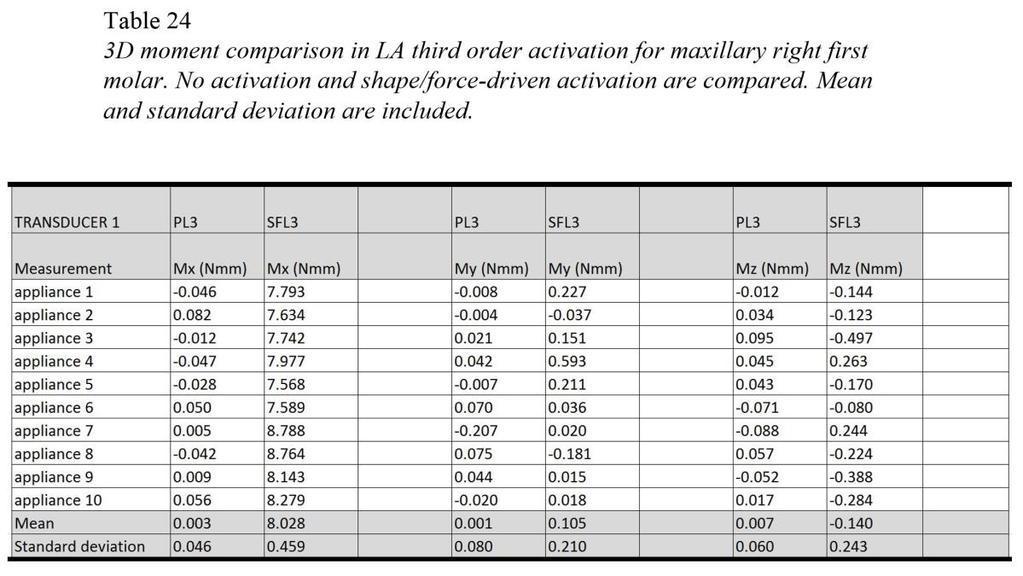
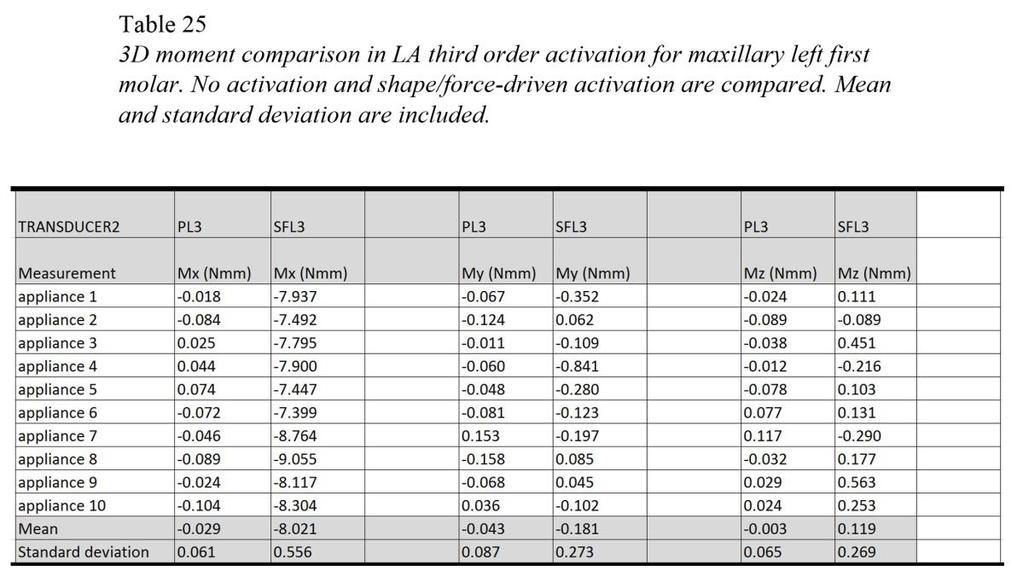
101 83
MemRx Orthodontic Appliances
 MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek
 Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek Dr. Wiezorek studied dental medicine at Kiel University, Germany from 1987 to 1993. He then finished
Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek Dr. Wiezorek studied dental medicine at Kiel University, Germany from 1987 to 1993. He then finished
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
TURN CLASS II INTO SIMPLE CLASS I PATIENTS.
 TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
An Effectiv Rapid Molar Derotation: Keles K
 An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
The management of impacted
 Using a rigid hook and spring auxiliary slid onto the archwire to direct eruption of impacted teeth BY S. JAY BOWMAN, DMD, MSD, AND ALDO CARANO, DR ODONT, MS, SPEC ORTHOD Figure 1: A 12-year-old female
Using a rigid hook and spring auxiliary slid onto the archwire to direct eruption of impacted teeth BY S. JAY BOWMAN, DMD, MSD, AND ALDO CARANO, DR ODONT, MS, SPEC ORTHOD Figure 1: A 12-year-old female
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
rocky mountain orthodontics functionaleducation
 rocky mountain orthodontics 3D 1ST PHASE FIXED/REMOVABLE (WILSON ) Without changing your chosen technique, RMO 3D 1st Phase FIXED/REMOVABLE Modular Orthodontics TM (Wilson ) can help your practice target
rocky mountain orthodontics 3D 1ST PHASE FIXED/REMOVABLE (WILSON ) Without changing your chosen technique, RMO 3D 1st Phase FIXED/REMOVABLE Modular Orthodontics TM (Wilson ) can help your practice target
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
ORTHOdontics SLIDING MECHANICS
 ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
A randomized clinical trial to compare the Goshgarian and Nance palatal arch
 European Journal of Orthodontics 32 (2010) 171 176 doi:10.1093/ejo/cjp075 Advance Access Publication 3 December 2009 The Author 2009. Published by Oxford University Press on behalf of the European Orthodontic
European Journal of Orthodontics 32 (2010) 171 176 doi:10.1093/ejo/cjp075 Advance Access Publication 3 December 2009 The Author 2009. Published by Oxford University Press on behalf of the European Orthodontic
A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR
 Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
With judicious treatment planning, the clinical
 CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
Mixed Dentition Treatment and Habits Therapy
 Interception Mixed Dentition Treatment and Habits Therapy Anterior Crossbites Posterior Crossbites Interference s with Normal Eruption Habit Therapy Tsung-Ju Hsieh, DDS, MSD 1 2 Anterior Crossbites Anterior
Interception Mixed Dentition Treatment and Habits Therapy Anterior Crossbites Posterior Crossbites Interference s with Normal Eruption Habit Therapy Tsung-Ju Hsieh, DDS, MSD 1 2 Anterior Crossbites Anterior
Expansion/Arch Development
 Expansion/Arch Development 9 Expansion and Arch Development is a broad term used to describe appliances designed to treat crowding, the most common type of malocclusion in mixed-dentition patients. These
Expansion/Arch Development 9 Expansion and Arch Development is a broad term used to describe appliances designed to treat crowding, the most common type of malocclusion in mixed-dentition patients. These
Controlled Space Closure with a Statically Determinate Retraction System
 Original Article Controlled Space Closure with a Statically Determinate Retraction System Kwangchul Choy, DDS, MS, PhD a ; Eung-Kwon Pae, DDS, MSc, PhD b ; Kyung-Ho Kim, DDS, MS, PhD c ; Young Chel Park,
Original Article Controlled Space Closure with a Statically Determinate Retraction System Kwangchul Choy, DDS, MS, PhD a ; Eung-Kwon Pae, DDS, MSc, PhD b ; Kyung-Ho Kim, DDS, MS, PhD c ; Young Chel Park,
#39 Ortho-Tain, Inc
 1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
Case Report Unilateral Molar Distalization: A Nonextraction Therapy
 Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Plus Combines Traditional Twin Bracket Treatment With Self-Ligation Convenience
 Lotus Plus Combines Traditional Twin Bracket Treatment With Self-Ligation Convenience Designed by an Orthodontist The initial concept for the Lotus Plus Self-Ligating Bracket System started with a simple
Lotus Plus Combines Traditional Twin Bracket Treatment With Self-Ligation Convenience Designed by an Orthodontist The initial concept for the Lotus Plus Self-Ligating Bracket System started with a simple
Arrangement of posterior artificial teeth Standardized parameters Curve of Wilson Curve of Spee
 . Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
. Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Archwire Insertion and Disengagement Instruments Technique Guide
 Clarity SL and SmartClip SL3 Self-Ligating Brackets Archwire Insertion and Disengagement Instruments Technique Guide Recommended Archwire Insertion Instruments Single point torquing key for tight spots
Clarity SL and SmartClip SL3 Self-Ligating Brackets Archwire Insertion and Disengagement Instruments Technique Guide Recommended Archwire Insertion Instruments Single point torquing key for tight spots
Keeping all these knowledge in mind I will show you 3 cases treated with the Forsus appliance.
 Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
The Inman Aligner. The Inman Aligner,* a versatile removable
 S. JY OWMN, DMD, MSD The Inman ligner,* a versatile removable appliance, is a unique modification of the traditional spring retainer. It uses superelastic opencoil springs to create light and constant
S. JY OWMN, DMD, MSD The Inman ligner,* a versatile removable appliance, is a unique modification of the traditional spring retainer. It uses superelastic opencoil springs to create light and constant
TURN CLASS II INTO SIMPLE CLASS I PATIENTS.
 TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
INCLUDES: OVERVIEW ON CLINICAL SITUATIONS FREQUENTLY ENCOUNTERED IN ORTHODONTIC TREATMENTS MECHANOTHERAPY USED TO RESOLVE THESE SITUATIONS
 ORTHOdontics PGI PROBLEM SOLVING IN ORTHODONTICS INCLUDES: OVERVIEW ON CLINICAL SITUATIONS FREQUENTLY ENCOUNTERED IN ORTHODONTIC TREATMENTS MECHANOTHERAPY USED TO RESOLVE THESE SITUATIONS FACULTY: Fares
ORTHOdontics PGI PROBLEM SOLVING IN ORTHODONTICS INCLUDES: OVERVIEW ON CLINICAL SITUATIONS FREQUENTLY ENCOUNTERED IN ORTHODONTIC TREATMENTS MECHANOTHERAPY USED TO RESOLVE THESE SITUATIONS FACULTY: Fares
INDICATIONS. Fixed Appliances are indicated when precise tooth movements are required
 DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Indian Journal of Basic and Applied Medical Research, March 2015: Vol.-4, Issue- 2, P
 Case report: Intra-arch non-compliant mechanics for maxillary 2 nd molar buccal crossbite: A transpalatal arch with L-Loop 1Dr.Renuka Patel, 2 Dr.Falguni Mehta, 3 Dr.Shivam Mehta, 4 Dr.Swati Khonde 1Assistant
Case report: Intra-arch non-compliant mechanics for maxillary 2 nd molar buccal crossbite: A transpalatal arch with L-Loop 1Dr.Renuka Patel, 2 Dr.Falguni Mehta, 3 Dr.Shivam Mehta, 4 Dr.Swati Khonde 1Assistant
The 20/20 Molar Tube. Ronald M. Roncone, D.D.S., M.S.
 The 20/20 Molar Tube by Ronald M. Roncone, D.D.S., M.S. A) Finish torque STAGE 3: Interactive to Active GOALS 4-6 months B) Finish root uprighting C) Maintain arch form D) Set occlusion with active settling
The 20/20 Molar Tube by Ronald M. Roncone, D.D.S., M.S. A) Finish torque STAGE 3: Interactive to Active GOALS 4-6 months B) Finish root uprighting C) Maintain arch form D) Set occlusion with active settling
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO Dr. Nanda Dr. Marzban Dr. Kuhlberg
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Dr. Nanda Dr. Marzban Dr. Kuhlberg Dr. Nanda is Professor, Head, and Program Director, Dr. Marzban is a thirdyear
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Dr. Nanda Dr. Marzban Dr. Kuhlberg Dr. Nanda is Professor, Head, and Program Director, Dr. Marzban is a thirdyear
System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi
 A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
CLASS II CORRECTION SIMPLIFIED
 C L A S S I I C O R R E C T O R CLASS II CORRECTION SIMPLIFIED PowerScope 2 delivers simple, efficient Class II correction like you ve never seen before. The latest generation of PowerScope features a
C L A S S I I C O R R E C T O R CLASS II CORRECTION SIMPLIFIED PowerScope 2 delivers simple, efficient Class II correction like you ve never seen before. The latest generation of PowerScope features a
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
The main challenge in using the natural dentition
 Use of Osseointegrated Implants for Orthodontic Anchorage DIANA WEBER, DDS, MS STEVEN HANDEL, DMD DANIEL DUNHAM, DDS The main challenge in using the natural dentition for anchorage of minor tooth movements,
Use of Osseointegrated Implants for Orthodontic Anchorage DIANA WEBER, DDS, MS STEVEN HANDEL, DMD DANIEL DUNHAM, DDS The main challenge in using the natural dentition for anchorage of minor tooth movements,
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Anchorage system. tomas / Sets Page 270 tomas / Pins Page 271 Instruments and accessories Page 273 Patient consultation material Page 282
 tomas / Sets Page 270 tomas / Pins Page 271 Instruments and accessories Page 273 Patient consultation material Page 282 266 . innovative comprehensive efficient. Dentaurum Online Shop shop.dentaurum.com
tomas / Sets Page 270 tomas / Pins Page 271 Instruments and accessories Page 273 Patient consultation material Page 282 266 . innovative comprehensive efficient. Dentaurum Online Shop shop.dentaurum.com
ANTERIOR AND CANINE RETRACTION: BIOMECHANIC CONSIDERATIONS. Part One
 In italiano, per favore ANTERIOR AND CANINE RETRACTION: BIOMECHANIC CONSIDERATIONS Part One Gabriele Floria DDS, Lorenzo Franchi DDS, Turi Bassarelli MD English Translation by Dr. Susan Eslambolchi & Dr.
In italiano, per favore ANTERIOR AND CANINE RETRACTION: BIOMECHANIC CONSIDERATIONS Part One Gabriele Floria DDS, Lorenzo Franchi DDS, Turi Bassarelli MD English Translation by Dr. Susan Eslambolchi & Dr.
Canine Extrusion Technique with SmartClip Self-Ligating Brackets
 Canine Extrusion Technique with SmartClip Self-Ligating Brackets Dr. Luis Huanca Ghislanzoni Dr. Luis Huanca received his DDS in 2006 and the MS and Specialist in Orthodontics in 2009 from the University
Canine Extrusion Technique with SmartClip Self-Ligating Brackets Dr. Luis Huanca Ghislanzoni Dr. Luis Huanca received his DDS in 2006 and the MS and Specialist in Orthodontics in 2009 from the University
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Orthodontic Treatment Using The Dental VTO And MBT System
 Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic treatment for jaw defor. Sakamoto, T; Sakamoto, S; Harazaki, Author(s) Yamaguchi, H. Journal Bulletin of Tokyo Dental College, 4
 Yamaguchi, H. Journal Bulletin of Tokyo Dental College, 4") Orthodontic treatment for jaw defor Titlelip and palate patients with the co external-expansion arch and a facia Sakamoto, T; Sakamoto, S; Harazaki, uthor(s) Yamaguchi, H Journal ulletin of Tokyo Dental
Orthodontic treatment for jaw defor Titlelip and palate patients with the co external-expansion arch and a facia Sakamoto, T; Sakamoto, S; Harazaki, uthor(s) Yamaguchi, H Journal ulletin of Tokyo Dental
04 Inserting the HYCON TUBE
 H y c o n D e v i c e f o r s p a c e c l o s u r e hycon HYCON t u b e placement information TUBE placement information 01 The HYCON TUBE block. The teeth of the front block should be laced with a figure
H y c o n D e v i c e f o r s p a c e c l o s u r e hycon HYCON t u b e placement information TUBE placement information 01 The HYCON TUBE block. The teeth of the front block should be laced with a figure
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases
 Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
RETENTION AND RELAPSE
 RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
Delta Force. Bracket System. Putting you in the driver s seat for ultimate control
 Delta Force Bracket System Putting you in the driver s seat for ultimate control Variable Force Orthodontics The Delta Force Bracket System incorporates an advanced design that allows you to control the
Delta Force Bracket System Putting you in the driver s seat for ultimate control Variable Force Orthodontics The Delta Force Bracket System incorporates an advanced design that allows you to control the
Non-osseointegrated. What type of mini-implants? 3/27/2008. Require a tight fit to be effective Stability depends on the quality and.
 Non-osseointegrated What type of mini-implants? Require a tight fit to be effective Stability depends on the quality and quantity of cortical and trabecular bone. Osseointegrated Non-osseointegrated AbsoAnchor
Non-osseointegrated What type of mini-implants? Require a tight fit to be effective Stability depends on the quality and quantity of cortical and trabecular bone. Osseointegrated Non-osseointegrated AbsoAnchor
THE JASPER JUMPER APPLIANCE; USAGE, EFFECTS AND RECENT MODIFICATIONS
 Pakistan Oral & Dent. Jr. 22 (2) Dec 2002 ABSTRACT THE JASPER JUMPER APPLIANCE; USAGE, EFFECTS AND RECENT MODIFICATIONS *HOSHANG RUMI SUKHIA, BDS, BSc, MS Orth The Jasper Jumper is a fixed functional appliance
Pakistan Oral & Dent. Jr. 22 (2) Dec 2002 ABSTRACT THE JASPER JUMPER APPLIANCE; USAGE, EFFECTS AND RECENT MODIFICATIONS *HOSHANG RUMI SUKHIA, BDS, BSc, MS Orth The Jasper Jumper is a fixed functional appliance
Lab Forms and Communications Precise Indirect Bonding Systems.
 Lab Forms and Communications Precise Indirect Bonding Systems. Presented by IN-tendo www.intendo-ortho.com and The Torque Angulation Laboratory www.torque-angulationlab.com The correct information and
Lab Forms and Communications Precise Indirect Bonding Systems. Presented by IN-tendo www.intendo-ortho.com and The Torque Angulation Laboratory www.torque-angulationlab.com The correct information and
From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment
 From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment by Lisa Alvetro, DDS After receiving her DDS summa cum laude from Ohio State University, Dr. Lisa Alvetro completed
From Plan B to Plan A : Using Forsus Class II Correctors as a Regular Mode of Treatment by Lisa Alvetro, DDS After receiving her DDS summa cum laude from Ohio State University, Dr. Lisa Alvetro completed
Indian Journal of Basic and Applied Medical Research; June 2014: Vol.-3, Issue- 3, P
 Case Report: Custom made modified distal jet appliance an effective and economic appliance. Dr.Falguni Mehta 1, Dr.Renuka Patel 2,Dr.Harshik Parekh 3,Dr.Manop Agrawal 4 1Head Of Department, Department
Case Report: Custom made modified distal jet appliance an effective and economic appliance. Dr.Falguni Mehta 1, Dr.Renuka Patel 2,Dr.Harshik Parekh 3,Dr.Manop Agrawal 4 1Head Of Department, Department
DENT Advanced Topics in Removable Prosthodontics, Winter 2008
 University of Michigan Deep Blue deepblue.lib.umich.edu 2008-01 DENT 718 - Advanced Topics in Removable Prosthodontics, Winter 2008 Shotwell, Jeffrey Shotwell, J. (2008, April 23) Advanced Topics in Removable
University of Michigan Deep Blue deepblue.lib.umich.edu 2008-01 DENT 718 - Advanced Topics in Removable Prosthodontics, Winter 2008 Shotwell, Jeffrey Shotwell, J. (2008, April 23) Advanced Topics in Removable
Crowding and protrusion treated by unusual extractions
 SM 3M Health Care Academy Crowding and protrusion treated by unusual extractions Gianluigi Fiorillo, DDS Dr. Gianluigi Fiorillo received his degree in Dentistry from La Sapienza University of Rome in 1992
SM 3M Health Care Academy Crowding and protrusion treated by unusual extractions Gianluigi Fiorillo, DDS Dr. Gianluigi Fiorillo received his degree in Dentistry from La Sapienza University of Rome in 1992
Dual Force Cuspid Retractor
 CLINICAL INNOVATION 1 Matrishva B Vyas, 2 Neeraj Alladwar ABSTRACT The most time consuming stage of bicuspid extraction-based treatment is cuspid retraction. Cuspid retraction with both types of conventional
CLINICAL INNOVATION 1 Matrishva B Vyas, 2 Neeraj Alladwar ABSTRACT The most time consuming stage of bicuspid extraction-based treatment is cuspid retraction. Cuspid retraction with both types of conventional
There is little controversy regarding whether temporary
 CLINICIAN'S CORNER Control of maxillary dentition with 2 midpalatal orthodontic miniscrews Yoon-Goo Kang, a Ji-Young Kim, b and Jong-Hyun Nam c Seoul, Korea The midpalatal area has no critical anatomic
CLINICIAN'S CORNER Control of maxillary dentition with 2 midpalatal orthodontic miniscrews Yoon-Goo Kang, a Ji-Young Kim, b and Jong-Hyun Nam c Seoul, Korea The midpalatal area has no critical anatomic
Mandibular Protraction Appliance IV
 CARLOS M. COELHO FILHO, DDS, MSD Articles published by Pancherz 1,2 on the Herbst* appliance in the last two decades seem to have stimulated the development of several other fixed appliances that work
CARLOS M. COELHO FILHO, DDS, MSD Articles published by Pancherz 1,2 on the Herbst* appliance in the last two decades seem to have stimulated the development of several other fixed appliances that work
Bands Buccal Tubes Lingual Attachments. When only the best will do.
 Bands Buccal Tubes Lingual Attachments When only the best will do. Bands Ortho Organizers, Inc. offers a complete selection of bands to fulfill your every request. Each band has the option to be ordered
Bands Buccal Tubes Lingual Attachments When only the best will do. Bands Ortho Organizers, Inc. offers a complete selection of bands to fulfill your every request. Each band has the option to be ordered
ortho case report Sagittal First international magazine of orthodontics By Dr. Luis Carrière Special Reprint
 Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
Ectopic upper canine associated to ectopic lower second bicuspid. Case report
 Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Table of Contents Section 6 Table of Contents
 Table of Contents Section 6 Table of Contents bands and attachments 6 3M Victory Series First Molar Bands... 6.2 3M Victory Series Second Molar Bands... 6.6 3M Unitek General Purpose Molar Bands... 6.10
Table of Contents Section 6 Table of Contents bands and attachments 6 3M Victory Series First Molar Bands... 6.2 3M Victory Series Second Molar Bands... 6.6 3M Unitek General Purpose Molar Bands... 6.10
ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS
 ORIGINAL ARTICLE ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS ABSTRACT FARHAT AMIN, BDS, MCPS, FCPS Mesial rotation of maxillary
ORIGINAL ARTICLE ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS ABSTRACT FARHAT AMIN, BDS, MCPS, FCPS Mesial rotation of maxillary
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Surveying. 3rd year / College of Dentistry/University of Baghdad ( ) Page 1
 Page 1") د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
(12) Patent Application Publication (10) Pub. No.: US 2005/ A1
 Patent Application Publication (10) Pub. No.: US 2005/ A1") (19) United States US 2005O130094A1 (12) Patent Application Publication (10) Pub. No.: US 2005/0130094A1 Graham (43) Pub. Date: Jun. 16, 2005 (54) ORTHODONTIC ACCESSORY ARCH BAR (52) U.S. Cl.... 433/20
(19) United States US 2005O130094A1 (12) Patent Application Publication (10) Pub. No.: US 2005/0130094A1 Graham (43) Pub. Date: Jun. 16, 2005 (54) ORTHODONTIC ACCESSORY ARCH BAR (52) U.S. Cl.... 433/20
Victory Series Active Self-Ligating Brackets. Reliable. and. Effective
 Victory Series Active Self-Ligating Brackets Reliable and Effective Victory Series Active Self-Ligating Brackets Reliability Victory Series SL Brackets are widely accepted as an industry benchmark for
Victory Series Active Self-Ligating Brackets Reliable and Effective Victory Series Active Self-Ligating Brackets Reliability Victory Series SL Brackets are widely accepted as an industry benchmark for
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Treatment planning of nonskeletal problems. in preadolescent children
 In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports
 Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
THE MBT VERSATILE+ APPLIANCE SYSTEM
 THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
wiirre e a a n n d d w wiirre e ffo orrms ms
 wire and wire forms wire and wire forms wire and wire forms Leone orthodontic wires are available in a range of alloys and different grades of elasticity and hardness to meet any therapeutic requirements.
wire and wire forms wire and wire forms wire and wire forms Leone orthodontic wires are available in a range of alloys and different grades of elasticity and hardness to meet any therapeutic requirements.
SnapLink Re-Convertible Tube
 SnapLink Re-Convertible Tube Background Buccal tubes are attached to the upper and lower molars to anchor the distal ends of archwires, or to attach an auxiliary wire, headgear or lip bumper, or as an
SnapLink Re-Convertible Tube Background Buccal tubes are attached to the upper and lower molars to anchor the distal ends of archwires, or to attach an auxiliary wire, headgear or lip bumper, or as an
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
Intraoral molar-distalization appliances that
 2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion.
 Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS. tportho.com cosmeticbraces.com. POD_TPOC_09_PreFinisher_Retainers_2015, Rev.
 9 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS tportho.com cosmeticbraces.com POD_TPOC_09_PreFinisher_Retainers_2015, Rev. 0 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS Pre-Finisher
9 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS tportho.com cosmeticbraces.com POD_TPOC_09_PreFinisher_Retainers_2015, Rev. 0 PRE-FINISHER APPLIANCE AND BONDABLE LINGUAL RETAINERS Pre-Finisher
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Integrative Orthodontics with the Ribbon Arch By Larry W. White, D.D.S., M.S.D.
 Integrative Orthodontics with the Ribbon Arch By Larry W. White, D.D.S., M.S.D. Abstract The ribbon arch previously had great popularity and utility early in the 20 th century, but lost its appeal as edgewise
Integrative Orthodontics with the Ribbon Arch By Larry W. White, D.D.S., M.S.D. Abstract The ribbon arch previously had great popularity and utility early in the 20 th century, but lost its appeal as edgewise
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique
 10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
10.5005/jp-journals-10021-1012 ORIGINAL ARTICLE Holy Nexus of Variable Wire Cross-section: New Vistas in Begg s Technique 1 Anil Miglani, 2 Ranjit Kumar Reena, 3 Pawanjit Singh Walia, 4 Varun Grover ABSTRACT
AlignEUSummit2015_PPT Template- GEN SESSION_
 Innovations of Invisalign Clear Aligners John Morton Director of Research and Technology 1 2016 Align Technology, Inc. All rights reserved. Legal Disclaimer The statements, views and opinions expressed
Innovations of Invisalign Clear Aligners John Morton Director of Research and Technology 1 2016 Align Technology, Inc. All rights reserved. Legal Disclaimer The statements, views and opinions expressed
It has been proposed that partially edentulous maxillectomy
 CLASSICAL ARTICLE Basic principles of obturator design for partially edentulous patients. Part II: Design principles Mohamed A. Aramany, DMD, MS* Eye and Ear Hospital of Pittsburgh and University of Pittsburgh,
CLASSICAL ARTICLE Basic principles of obturator design for partially edentulous patients. Part II: Design principles Mohamed A. Aramany, DMD, MS* Eye and Ear Hospital of Pittsburgh and University of Pittsburgh,
Indirect retainers. 1 i
 8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
3M Incognito Appliance System extraction case study.
 SM 3M Health Care Academy 3M Incognito Appliance System extraction case study. Toru Inami, DDS, Ph.D. Dr. Toru Inami graduated from the Aichigakuin University School of Dentistry in 1976. From 1977 to
SM 3M Health Care Academy 3M Incognito Appliance System extraction case study. Toru Inami, DDS, Ph.D. Dr. Toru Inami graduated from the Aichigakuin University School of Dentistry in 1976. From 1977 to
Component parts of Chrome Cobalt Removable Partial Denture
 Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Technique Guide. Orthodontic Bone Anchor (OBA) System. Skeletal implants for the orthodontic movement of the teeth.
 System. Skeletal implants for the orthodontic movement of the teeth.") Technique Guide Orthodontic Bone Anchor (OBA) System. Skeletal implants for the orthodontic movement of the teeth. Table of Contents Introduction Orthodontic Bone Anchor (OBA) System 2 Indications and
Technique Guide Orthodontic Bone Anchor (OBA) System. Skeletal implants for the orthodontic movement of the teeth. Table of Contents Introduction Orthodontic Bone Anchor (OBA) System 2 Indications and
Segmental Orthodontics for the Correction of Cross Bites
 10.5005/jp-journals-10005-1080 CASE REPORT IJCPD Segmental Orthodontics for the Correction of Cross Bites 1 Anirudh Agarwal, 2 Rinku Mathur 1 Professor and Head, Department of Orthodontics, Rajasthan Dental
10.5005/jp-journals-10005-1080 CASE REPORT IJCPD Segmental Orthodontics for the Correction of Cross Bites 1 Anirudh Agarwal, 2 Rinku Mathur 1 Professor and Head, Department of Orthodontics, Rajasthan Dental
Principles of. By: Dr. Ahmad Rabah
 Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
Hyrax, quadhelix, headgear,pendulum, Delaire facemask
 Hyrax, quadhelix, headgear,pendulum, Delaire facemask Hyrax Indication: -serious narrowing of the upper arch -bilateral or unilateral cross bite -treatment of cleft palate ( scar-tissue enlargement) hyrax
Hyrax, quadhelix, headgear,pendulum, Delaire facemask Hyrax Indication: -serious narrowing of the upper arch -bilateral or unilateral cross bite -treatment of cleft palate ( scar-tissue enlargement) hyrax
Low-Force Mechanics Nonextraction. Estimated treatment time months (Actual 15 mos 1 week). Low-force mechanics.
. Low-force mechanics.") T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.