Dental Trauma in the Pediatric Population
|
|
|
- Kevin Riley
- 5 years ago
- Views:
Transcription
1 Dental Trauma in the Pediatric Population Juan F. Yepes DDS, MD, MPH, MS, DrPH Associate Professor of Pediatric Dentistry Indiana University School of Dentistry James Whitcomb Hospital for Children


2

3


4

5 Presented with avulsion of # 8 Extra-oral time 20 min

6


7

8

9
10 Disclaimers All clinical pictures were authored by myself unless otherwise listed on the slide. Patients and/or parent consent was received for all photos. All pictures used in the presentation were downloaded from websites with copyrights release on file. Juan F. Yepes DDS, MD, MPH, DrPH
11 Session Objectives 1. To review the classification of dental trauma to the permanent dentition 2. To understand the treatment protocols depending of the type of trauma
12 Vocabulary

13 Requirements of modern splints for stabilization of traumatized teeth Intraoral application No damage to gingival tissues RCT and sensibility testing should be possible Esthetically acceptable Be easy to keep clean Adequate fixation Simple procedure No interference with occlusion No additional trauma to splinted teeth Allowing physiologic tooth mobility

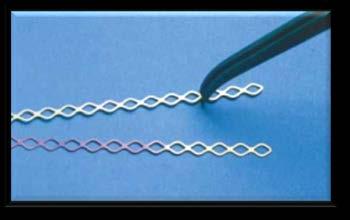


14 Requirements of modern splints for stabilization of traumatized teeth

15 Treatment Guidelines for Trauma to Permanent Dentition Luxated Teeth Avulsed Teeth Tooth and / or Alveolar Fractures

16 Treatment Guidelines for Fractures of Teeth and Alveolar Bone Image Downloaded from

17 Treatment Guidelines for Fractures of Teeth and Alveolar Bone General Considerations Age of the patient Cooperation Parent desires / concerns Dental Development

18 Treatment Guidelines for Fractures of Teeth and Alveolar Bone Treatment Timing Immediate Treatment Avulsion Alveolar fracture Extrusive luxation Lateral luxation
19 Treatment Guidelines for Fractures of Teeth and Alveolar Bone Treatment May be delayed several several hours without compromise Treatment Timing Intrusion Concussion Subluxation Crown fracture with pulp exposure Root Fracture Crown fracture without pulp exposure

20 Infraction Clinical findings An incomplete fracture (crack) of the enamel without loss of tooth structure. Not tender. If tenderness is observed evaluate the tooth for a possible luxation injury or a root fracture. Radiographic Findings No radiographic abnormalities. Radiographs recommended: a periapical view. Additional radiographs are indicated if other signs or symptoms are present. Treatment In case of marked infractions, etching and sealing with resin to prevent discoloration of the infraction lines. Otherwise, no treatment is necessary.
21 Infraction Favorable Outcome Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Unfavorable Outcome Symptomatic Negative response to pulp testing. Signs of apical periodontitis. No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.

22 Enamel Fracture Clinical Findings Radiographic Findings Treatment A complete fracture of the enamel. Loss of enamel. No visible sign of exposed dentin. Not tender. If tenderness is observed evaluate the tooth for a possible luxation or root fracture injury. Normal mobility. Sensibility pulp Enamel loss is visible. Radiographs recommended: periapical, occlusal and eccentric exposures. These are recommended in order to rule out the possible presence of a root fracture or a luxation injury. Radiograph of lip or cheek to search for tooth fragments or foreign materials. If the tooth fragment is available, it can be bonded to the tooth. Contouring or restoration with composite resin depending on the extent and location of the fracture.


23 Enamel Fracture Follow up Favorable Outcome Unfavorable Outcome 6-8 weeks C++ 1 year C++ Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Continue to next evaluation. Symptomatic Negative response to pulp testing. Signs of apical periodontitis No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.


24 9 year old bike wreck

25


26

27

28 9 months later.

29 Enamel -Dentin Fracture Clinical Findings Radiographic Findings Treatment A fracture confined to enamel and dentin with loss of tooth structure, but not exposing the pulp. Percussion test: not tender. If tenderness is observed, evaluate the tooth for possible luxation or root fracture injury. Normal mobility. Sensibility pulp test usually positive Enamel-dentin loss is visible. Radiographs recommended: periapical, occlusal and eccentric exposure to rule out tooth displacement or possible presence of root fracture. Radiograph of lip or cheek lacerations to search for tooth fragments or foreign materials. If a tooth fragment is available, it can be bonded to the tooth. Otherwise perform a provisional treatment by covering the exposed dentin with glass- Ionomer or a more permanent restoration using a bonding agent and composite resin, or other accepted dental restorative materials If the exposed dentin is within 0.5mm of the pulp (pink, no bleeding) place calcium hydroxide base and cover with a material such as a glass ionomer.


30 Enamel -Dentin Fracture 15 years old. Bicycle accident

31 Enamel -Dentin Fracture 15 years old. Bicycle accident

32 Enamel -Dentin Fracture Non-complicated fracture of the crown

33 Enamel -Dentin Fracture band-aid composite

34 Enamel -Dentin Fracture 12 years old

35 Enamel -Dentin Fracture
36 Enamel -Dentin Fracture Age: Gender: Chief complaint: PMH: Dental History: Social History: 8 year old girl hit my face after a bicycle accident Unremarkable Unremarkable Unremarkable

37 Enamel Dentin Fracture

38 Enamel Dentin Fracture

39 Enamel -Dentin Fracture Diagnosis: Extrusion tooth # 8 Crown-fracture uncomplicated teeth # 8 and 9 Treatment (extrusion): 1. Reposition as soon as possible 2. Stabilize the tooth with splint 3. Splint for 2 weeks * American Academy of Pediatric Dentistry. Reference Manual. May Page 220: Acute management of dental trauma

40 Enamel -Dentin Pulp Fracture


41 Enamel -Dentin Pulp Fracture
42 Enamel - Dentin Fracture Follow up Favorable Outcome Unfavorable Outcome 6-8 weeks C++ 1 year C++ Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Continue to next evaluation. Symptomatic Negative response to pulp testing. Signs of apical periodontitis No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.
43 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Clinical Findings Radiographic Findings Treatment A fracture involving enamel and dentin with loss of tooth structure and exposure of the pulp. Normal mobility Percussion test: not tender. If tenderness is observed, evaluate for possible luxation or root fracture injury. Exposed pulp sensitive to stimuli. Enamel dentin loss visible. Radiographs recommended: periapical, occlusal and eccentric exposures, to rule out tooth displacement or possible presence of root fracture. Radiograph of lip or cheek lacerations to search for tooth fragments or foreign materials. In young patients with immature, still developing teeth, it is advantageous to preserve pulp vitality by pulp capping or partial pulpotomy. Also, this treatment is the choice in young patients with completely formed teeth. Calcium hydroxide is a suitable material to be placed on the pulp wound in such procedures. In patients with mature apical development, root canal treatment is usually the treatment of choice, although pulp capping or partial pulpotomy also may be selected. If tooth fragment is available, it can be bonded to the tooth. Future treatment for the fractured crown may be restoration with other accepted dental restorative materials.

44 10 years old Scooter accident 7 hours ago Past medical history: Unremarkable Medications: None Allergies: None
 Click / sounds TMJ IO Soft Tissue exam: Within normal")
45 Extra-oral exam (EOE): (-) Thyromegaly (-) Lymphadenopathy (-) Salivary gland enlargement Clinical Findings I (+) Skin lesions: minor lacerations in the chin and upper lip (-) Click / sounds TMJ IO Soft Tissue exam: Within normal limits
")
46 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture)
")
47 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture)

")

48 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) partially open apex Complicated crown fracture

49 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Fracture involves enamel and dentin and the pulp is exposed. Sensibility testing is usually not indicated. In young patients with immature, still developing teeth, it is advantageous to preserve pulp vitality by pulp capping or partial pulpotomy. Calcium hydroxide or MTA (white) are suitable materials for the procedure. In older patients, root canal treatment can be the treatment of choice, although pulp capping or partial pulpotomy may also be selected.
")

50 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Profuse irrigation with saline solution Direct pulp cap with calcium hydroxide
 Temporary")
51 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Temporary composite
 Temporary composite in")
52 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Temporary composite in place
")
53 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Occlusion check

54 8 year old Yesterday in gym class we had to run laps to warm up and the mean boy on the bus tripped me and my teeth broke on the floor.



55



56
57 Enamel -Dentin Pulp Fracture (Complicated Crown Fracture) Follow up Favorable Outcome Unfavorable Outcome 6-8 weeks C++ 1 year C++ Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Continue to next evaluation. Symptomatic Negative response to pulp testing. Signs of apical periodontitis No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.

58 Crown-Root Fracture without Pulp Exposure Clinical Findings Radiographic Findings Treatment A fracture involving enamel, dentin and cementum with loss of tooth structure, but not exposing the pulp. Crown fracture extending below gingival margin. Percussion test: Tender. Coronal fragment mobile. Sensibility pulp test usually positive for apical fragment. Apical extension of fracture usually not visible. Radiographs recommended: periapical, occlusal and eccentric exposures. They are recommended in order to detect fracture lines in the root. Emergency treatment As an emergency treatment a temporary stabilization of the loose segment to adjacent teeth can be performed until a definitive treatment plan is made. (flexible splint for 3-4 weeks) Non-Emergency Treatment Alternatives Fragment removal only Fragment removal and gingivectomy Orthodontic extrusion of apical fragment Surgical extrusion Root submergence Extraction
59 Crown-Root Fracture without Pulp Exposure Follow up Favorable Outcome Unfavorable Outcome 6-8 weeks C++ 1 year C++ Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Continue to next evaluation. Symptomatic Negative response to pulp testing. Signs of apical periodontitis No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.

 In patients with open apices, it is advantageous to preserve pulp vitality by a partial pulpotomy.")
60 Crown-Root Fracture with Pulp Exposure Clinical Findings Radiographic Findings Treatment A fracture involving enamel, dentin, and cementum and exposing the pulp. Percussion test: tender. Coronal fragment mobile. Apical extension of fracture usually not visible. Radiographs recommended: periapical and occlusal exposure. Emergency treatment Temporary stabilization of the loose segment to adjacent teeth can be performed until a definitive treatment plan is made. (flexible splint for 3-4 weeks) In patients with open apices, it is advantageous to preserve pulp vitality by a partial pulpotomy. This treatment is also the choice in young patients with completely formed teeth. Calcium hydroxide Compounds (or MTA) are suitable pulp capping materials. In patients with mature apical development, root canal treatment can be the treatment of choice. Fragment removal only Fragment removal and gingivectomy Orthodontic extrusion of apical fragment Surgical extrusion Root submergence Extraction
61 Crown-Root Fracture with Pulp Exposure Follow up Favorable Outcome Unfavorable Outcome 6-8 weeks C++ 1 year C++ Asymptomatic Positive response to pulp testing. Continuing root development in immature teeth. Continue to next evaluation. Symptomatic Negative response to pulp testing. Signs of apical periodontitis No continuing root development in immature teeth. Endodontic therapy appropriate for stage of root development is indicated.
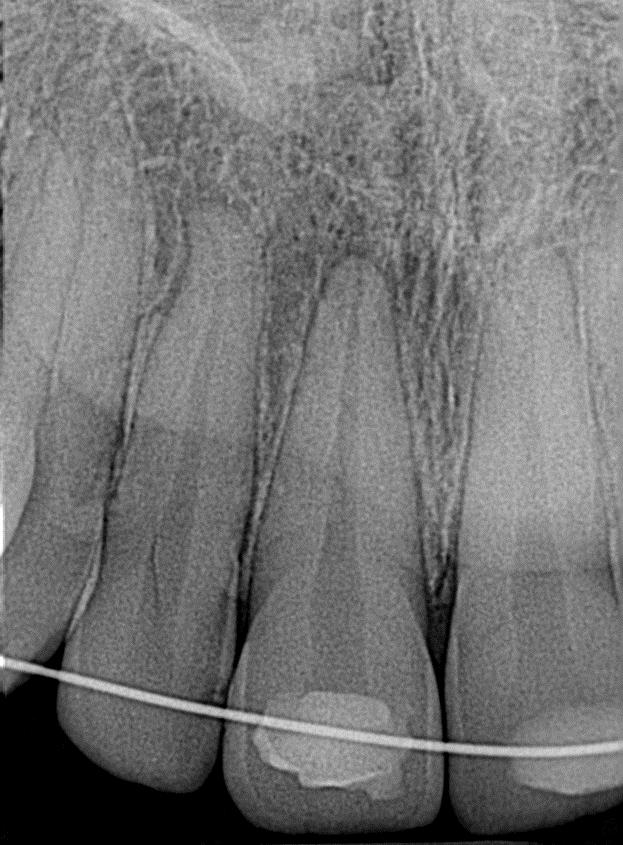
62 Root Fracture Clinical Findings Radiographic Findings Treatment The coronal segment may be mobile and may be displaced. The tooth may be tender to percussion. Bleeding from the gingival sulcus may be noted. Sensibility testing may give negative results initially, indicating transient or permanent neural damage. Monitoring the status of the pulp is recommended. Transient crown discoloration (red or grey) may occur. The fracture involves the root of the tooth and is in a horizontal or oblique plane. Fractures that are in the horizontal plane can usually be detected in the regular periapical 90 angle film with the central beam through the tooth. This is usually the case with fractures in the cervical third of the root. If the plane of fracture is more oblique which is common with apical third fractures, an occlusal view or radiographs with varying horizontal angles are more likely to demonstrate the fracture including those located in the middle third. Reposition, if displaced, the coronal segment of the tooth as soon as possible. Check position radiographically. Stabilize the tooth with a flexible splint for 4 weeks. If the root fracture is near the cervical area of the tooth, stabilization is beneficial for a longer period of time (up to 4 months). It is advisable to monitor healing for at least one year to determine pulpal status. If pulp necrosis develops, root canal treatment of the coronal tooth segment to the fracture line is indicated to preserve the tooth.
. Signs of repair between fractured segments. Continue to next evaluation.")

63 Root Fracture Follow up Favorable Outcome Unfavorable Outcome 4 Weeks S+, C Weeks C++ 4 Months S++*, C++ 6 Months C++ 1 Year C++ 5 Years C++ Positive response to pulp testing (false negative possible up to 3 months). Signs of repair between fractured segments. Continue to next evaluation. Symptomatic Negative response to pulp testing (false negative possible up to 3 months). Extrusion of the coronal segment. Radiolucency at the fracture line. Clinical signs of periodontitis or abscess associated with the fracture line. Endodontic therapy appropriate for stage of root development is indicated. S+ = Splint removal S ++ = Splint removal in cervical fractures

64 Alveolar Fracture Clinical Findings Radiographic Findings Treatment The fracture involves the alveolar bone and may extend to adjacent bone. Segment mobility and dislocation with several teeth moving together are common findings. An occlusal change due to misalignment of the fractured alveolar segment is often noted. Sensibility testing may or may not be positive. Fracture lines may be located at any level, from the marginal bone to the root apex. In addition to the 3 angulations and occlusal film, additional views such as a panoramic radiograph can be helpful in determining the course and position of the fracture Line. Reposition any displaced segment and then splint. Suture gingival laceration if present. Stabilize the segment for 4 weeks.

65 Alveolar Fracture

66 Alveolar Fracture

67 Alveolar Fracture

68 Alveolar Fracture


69


70


71
. Signs of repair between fractured segments. Continue to next evaluation. Symptomatic Negative response to pulp testing (false negative possible up to 3 months).")
72 Alveolar Fracture Follow up Favorable Outcome Unfavorable Outcome 4 Weeks S+, C Weeks C++ 4 Months S++*, C++ 6 Months C++ 1 Year C++ 5 Years C++ Positive response to pulp testing (false negative possible up to 3 months). Signs of repair between fractured segments. Continue to next evaluation. Symptomatic Negative response to pulp testing (false negative possible up to 3 months). Signs of apical periodontitis or external resorption Endodontic therapy appropriate for stage of root development is indicated. S+ = Splint removal S ++ = Splint removal in cervical fractures
73 Treatment Guidelines for Luxation Injuries Concussion Subluxation Extrusive Luxation Lateral Luxation Image Downloaded from
74 Concussion I An injury to the tooth-supporting structures without increased mobility or displacement of the tooth, but with pain to percussion Clinical Findings Radiographic Findings Treatment The tooth is tender to touch or tapping; it has not been displaced and does not have increased mobility. Sensibility tests are likely to give positive results. No radiographic abnormalities No treatment is needed. Monitor pulpal condition for at least one year.
.")
75 Concussion II Follow up Favorable Outcome Unfavorable Outcome 4 Weeks C Weeks C++ 1 Year C++ Asymptomatic Positive response to pulp testing False negative possible up to 3 months. Continuing root development in immature teeth Intact lamina dura Symptomatic Negative response to pulp testing (false negative possible up to 3 months). Signs of apical periodontitis or external resorption Endodontic therapy appropriate for stage of root development is indicated. S+ = Splint removal S ++ = Splint removal in cervical fractures C++= Clinical and radiographic examination


76 Subluxation I An injury to the tooth supporting structures resulting in increased mobility, but without displacement of the tooth. Bleeding from the gingival sulcus confirms the diagnosis Clinical Findings Radiographic Findings Treatment The tooth is tender to touch or tapping and has increased mobility; it has not been displaced. Bleeding from gingival crevice may be noted. Sensibility testing may be negative initially indicating transient pulpal damage. Monitor pulpal response until a definitive pulpal diagnosis can be made. Radiographic abnormalities are usually not found. Normally no treatment is needed, however a flexible splint to stabilize the tooth for patient comfort can be used for up to 2 weeks.
77 Subluxation II Follow up Favorable Outcome Unfavorable Outcome 2 Weeks S+, C++ 4 Weeks C Weeks C++ 6 Months C++ 1 Year C++ Asymptomatic Positive response to pulp testing False negative possible up to 3 months. Continuing root development in immature teeth Intact lamina dura Symptomatic Negative response to pulp testing (false negative possible up to 3 months). Signs of apical periodontitis or external resorption External inflammatory resorption Endodontic therapy appropriate for stage of root development is indicated. S+ = Splint removal S ++ = Splint removal in cervical fractures C++= Clinical and radiographic examination
78 Extrusive Luxation I Partial displacement of the tooth out of its socket The alveolar bone is intact (as oppose to lateral luxation) Clinical Findings Radiographic Findings Treatment The tooth appears elongated and is excessively mobile. Sensibility tests will likely give negative results. Increased periodontal ligament space apically. Reposition the tooth by gently re-inserting It into the tooth socket. Stabilize the tooth for 2 weeks using a flexible splint. In mature teeth where pulp necrosis is anticipated or if several signs and symptoms indicate that the pulp of mature or immature teeth became necrotic, root canal treatment is indicated.
79 Extrusive Luxation II S+ = Splint removal S ++ = Splint removal in cervical fractures C++= Clinical and radiographic examination Follow up Favorable Outcome Unfavorable Outcome 2 Weeks S+, C++ 4 Weeks C Weeks C++ 6 Months C++ 1 Year C++ Yearly 5 years C++ Asymptomatic Clinical and radiographic signs of normal or healed periodontium. Positive response to pulp testing (false negative possible up to 3 months). Marginal bone height corresponds to that seen radiographically after repositioning. Continuing root development in immature teeth Symptoms and radiographic sign consistent with apical periodontitis. Negative response to pulp testing (false negative possible up to 3 months). If breakdown of marginal bone, splint for an additional 3-4 weeks. External inflammatory root resorption. Endodontic therapy appropriate for stage of root development is Indicated
80 Lateral Luxation I Displacement of the tooth (except axially) accompanied by comminution or fracture of either the labial or the palatal / lingual alveolar bone partial or total separation of the periodontal ligament Clinical Findings Radiographic Findings Treatment The tooth is displaced, usually in a palatal/lingual or labial direction. It will be immobile and percussion usually gives a high, metallic (ankylotic) sound. Fracture of the alveolar process present. Sensibility tests will likely give negative results The widened periodontal ligament space is best seen on eccentric or occlusal exposures. Reposition the tooth by gently re-inserting It into the tooth socket. Stabilize the tooth for 4 weeks using a flexible splint. Monitor the pulpal condition. If the pulp becomes necrotic, root canal treatment is indicated to prevent root resorption.
81 Lateral Luxation II Displacement of the tooth (except axially) accompanied by comminution or fracture of either the labial or the palatal / lingual alveolar bone partial or total separation of the periodontal ligament Follow up Favorable Outcome Unfavorable Outcome 2 Weeks S+, C++ 4 Weeks C Weeks C++ 6 Months C++ 1 Year C++ Yearly 5 years C++ Asymptomatic Clinical and radiographic signs of normal or healed periodontium. Positive response to pulp testing (false negative possible up to 3 months). Marginal bone height corresponds to that seen radiographically after repositioning. Continuing root development in immature teeth S+ = Splint removal S ++ = Splint removal in cervical fractures C++= Clinical and radiographic examination Symptoms and radiographic sign consistent with apical periodontitis. Negative response to pulp testing (false negative possible up to 3 months). If breakdown of marginal bone, splint for an additional 3-4 weeks. External inflammatory root resorption. Endodontic therapy appropriate for stage of root development is Indicated
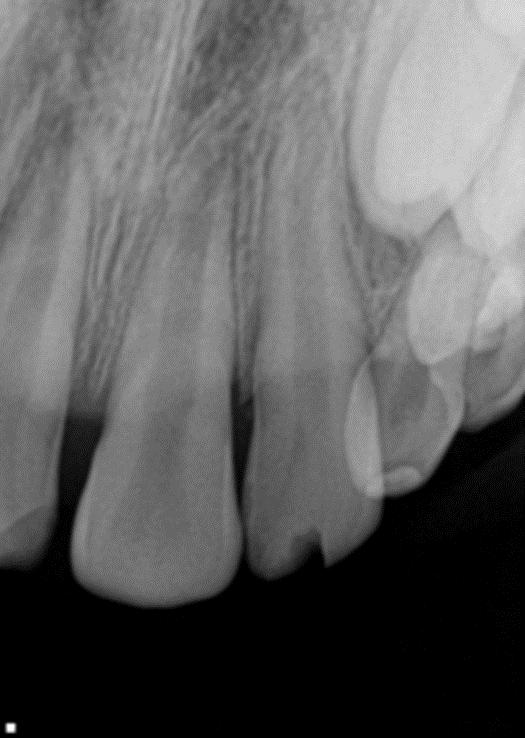
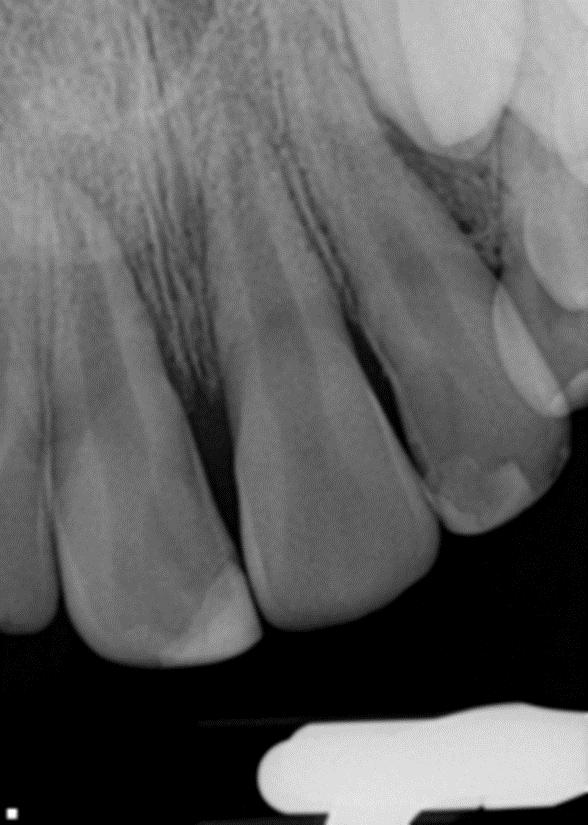
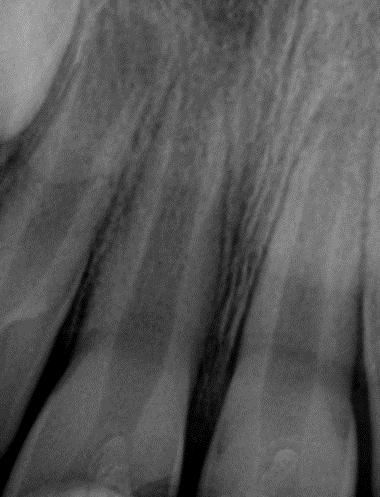
82 Intrusive Luxation I Displacement of the tooth into the alveolar bone Clinical Findings Radiographic Findings Treatment The tooth is displaced axially into the alveolar bone. It is immobile and percussion may give a high, metallic (ankylotic) sound. Sensibility tests will likely give negative results. The periodontal ligament space may be absent from all or part of the root. The cemento-enamel junction is located more apically in the intruded tooth than in adjacent non-injured teeth, at times even apical to the marginal bone level. Teeth with incomplete root formation Allow eruption without intervention If no movement within few weeks, initiate orthodontic repositioning. If tooth is intruded more than 7mm, reposition surgically or orthodontically. Teeth with complete root formation Allow eruption without intervention if tooth intruded less than 3mm. If no movement after 2-4 weeks, reposition surgically or orthodontically before ankylosis can develop. If tooth is intruded beyond 7mm, reposition surgically. The pulp will likely become necrotic in teeth with complete root formation root canal therapy using a temporary filling with calcium hydroxide is recommended and treatment should begin 2-3 w. after surgery. Once an intruded tooth has been repositioned surgically or orthodontically, stabilize with a flexible splint for 4-8 weeks
83 Intrusive Luxation I Age: Gender: Chief complaint: PMH: 9 year old Girl Hit the street Unremarkable Dental History: - Tooth # 9 was traumatic intruded in September of Bracket placed March 2011 Social History: Grandfather is the legal guardian


84 Intrusive Luxation I

85 Intrusive Luxation I

86 Intrusive Luxation I

87 Intrusive Luxation II Displacement of the tooth into the alveolar bone Follow up Favorable Outcome Unfavorable Outcome 2 Weeks S+, C++ 4 Weeks C Weeks C++ 6 Months C++ 1 Year C++ Yearly 5 years C++ Tooth in place or erupting. Intact lamina dura No signs of resorption. Continuing root development in immature teeth. Tooth locked in place/ankylotic tone to percussion. Radiographic signs of apical periodontitis External inflammatory root resorption or replacement resorption. Endodontic therapy appropriate for stage of root development is indicated. S+ = Splint removal S ++ = Splint removal in cervical fractures C++= Clinical and radiographic examination

88 7 year


89


90 4 months later
91 Avulsion A case apart
92 Avulsion Pt. presented to Peds Dentistry on for evaluation of #9. Father states that Pt. wrecked her bike in the drive way and avulsed #9 two weeks prior. Father states that it took aprox. 30 minutes to find the tooth and another 30 minutes to get to the local dentist. Father placed the tooth in milk once he found it. Dentist re-implanted #9.
93 Avulsion

94 Avulsion

95 Avulsion So..what we know? - Avulsion of tooth # 9 - Extraoral time: approximately 60 minutes - 30 minutes dry and 30 minutes in milk - Open apex (more than 1 mm) What we suppose to do?

96 The tooth is completely displaced out of its socket Avulsion Avulsion of a permanent teeth is one of the most serious dental injuries, and a prompt and correct emergency management is very important for the prognosis Extraoral time Maturation stage open vs. close apex
 under cold water and reposition it If this")

97 Avulsion First Aid for Avulsed Teeth Find the tooth and pick it up by the crown If the tooth is dirty, wash it briefly (10 seconds) under cold water and reposition it If this is not possible, place the tooth in a storage medium (milk or Hanks balanced solution) The tooth can also be transported in the mouth Seek emergency dental treatment immediately

98 First Aid for Avulsed Teeth Avulsion
99 Avulsion Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 2 weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) Chlorhexidine rinse for 1 week Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):
100 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Tooth was transported in Hank s Balanced Salt Solution (HBSS) or milk Soak in doxycycline solution for 5 minutes Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 2 weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) Chlorhexidine rinse for 1 week Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days
101 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place Change flexible transport splint for to 2 HBBS weeks or cold milk Prescribe antibiotics (doxycycline or penicillin V for 7 days) Soak Chlorhexidine in doxycycline rinse for solution 1 week for 5 minutes Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):137-
102 Avulsion Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 4weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) Place in 1.23% sodium fluoride Chlorhexidine rinse for 1 week for Assess 5 to tetanus 20 minutes vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days Debride with soft pumice prophylaxis, gentle scaling / root planing, or 3% citric acid for 3 minutes and rinse well to remove the PL
103 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Monitor every 4 weeks + pulp test + radiographs Ideal outcome: Revascularization and / or apexogenesis over the next 12 to 18 months Alternative outcomes: - Initiate apexification with MTA or calcium hydroxide or root canal therapy is signs / symptoms - Consider decoronation procedure if ankylosis Follow up: 1 week, 1 month, 3 months, 6 months, 12 months and annually for 5 years McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):
 Immediately")


104 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Closed Apex (< 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 2 weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) Chlorhexidine rinse for 1 week Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days Initiate pulpectomy / debridement on all teeth within 7 to 10 days
 Immediately replanted Extraoral dry storage <20 min Tooth moist for 20-60 min 20 to 60 minutes of dry extraoral time >60 min extraoral time Tooth was transported in Hank s")
105 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Closed Apex (< 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Tooth was transported in Hank s Balanced Salt Solution (HBSS) or milk Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 2 weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) - Chlorhexidine rinse for 1 week Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days Initiate pulpectomy / debridement on all teeth within 7 to 10 days
106 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Closed Apex (< 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place Change flexible transport splint for to 2 HBBS weeks or cold milk Prescribe antibiotics (doxycycline or penicillin V for 7 days) Chlorhexidine rinse for 1 week Assess tetanus vaccination: if needed, get booster within 48 h Provide post-operative instructions Follow up in 7 to 10 days Initiate pulpectomy / debridement on all teeth within 7 to 10 days McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):137-
107 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Closed Apex (< 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place flexible splint for 4weeks Prescribe antibiotics (doxycycline or penicillin V for 7 days) Chlorhexidine rinse for 1 week Place in 1.23% sodium fluoride Assess tetanus vaccination: if needed, get booster within 48h. for 5 to 20 minutes Provide post-operative instructions Follow up in 7 to 10 days Initiate pulpectomy / debridement on all teeth within 7 to 10 days Debride with soft pumice prophylaxis, gentle scaling / root planing, or 3% citric acid for 3 m. and rinse well to remove the PL
108 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with a Closed Apex (<1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time If root canal therapy was initiated, complete within 1 month or: If patient does not present until > 2 weeks after trauma and / or if radiographic resorption is present: - Pulpectomy / debridement as soon as possible - Long term calcium hydroxide therapy and change every 3 months - Complete root canal therapy when PL is observed healthy Follow up: 1 week, 1 months, 3 months, 12 months, and annually for 5 years McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):

109 Avulsion McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):

110 Avulsion
111 Avulsion Pt. presented to U.K. Peds Dentistry on 05/14/12 for evaluation of #9. Father states that Pt. wrecked her bike in the drive way and avulsed #9 two weeks prior. Father states that it took aprox. 30 minutes to find the tooth and another 30 minutes to get to the local dentist. (Dr. Allen in London, Ky) Father placed the tooth in milk once he found it. Dr. Allen re-implanted #9.
112 Avulsion
113 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Replant / reposition Obtain periapical radiograph to verify position Place Change flexible transport splint for to 2 HBBS weeks or cold milk Prescribe antibiotics (doxycycline or penicillin V for 7 days) Soak Chlorhexidine in doxycycline rinse for solution 1 week for 5 minutes Assess tetanus vaccination: if needed, get booster within 48 h. Provide post-operative instructions Follow up in 7 to 10 days McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):137-
114 Assess medical history and rule out any neurological and non-dental injuries Rule out alveolar fracture 3 radiographic projections Pulp vitality Avulsion Management of an Avulsed Permanent Incisor with an Open Apex (>= 1mm) Immediately replanted Extraoral dry storage <20 min Tooth moist for min 20 to 60 minutes of dry extraoral time >60 min extraoral time Monitor every 4 weeks + pulp test + radiographs Ideal outcome: Revascularization and / or apexogenesis over the next 12 to 18 months Alternative outcomes: - Initiate apexification with MTA or calcium hydroxide or root canal therapy is signs / symptoms - Consider decoronation procedure if ankylosis Follow up: 1 week, 1 month, 3 months, 6 months, 12 months and annually for 5 years McIntyre J, Lee J, Trope M, Vann WJ, Permanent tooth replantation following avulsion: Using a decision tree to achieve the best outcome. Pediatr Dent 2009;31(2):
115 Conclusions Comments? Questions?
FRACTURES AND LUXATIONS OF PERMANENT TEETH
 FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
FRACTURES AND LUXATIONS OF PERMANENT TEETH 1. Treatment guidelines and alveolar bone Followup Procedures INFRACTION Clinical findings Radiographic findings Treatment Follow-Up Favorable Outcome Unfavorable
The Treatment of Traumatic Dental Injuries
 The Recommended Guidelines of the American Association of Endodontists for The Treatment of Traumatic Dental Injuries 2013 American Association of Endodontists Revised 9/13 The Recommended Guidelines of
The Recommended Guidelines of the American Association of Endodontists for The Treatment of Traumatic Dental Injuries 2013 American Association of Endodontists Revised 9/13 The Recommended Guidelines of
DENTAL TRAUMA GUIDELINES
 International Association of Dental Traumatology DENTAL TRAUMA GUIDELINES Revised 2012 CONTENT: Section 1. Fractures and luxations of permanent teeth Section 2. Avulsion of permanent teeth Section 3. Traumatic
International Association of Dental Traumatology DENTAL TRAUMA GUIDELINES Revised 2012 CONTENT: Section 1. Fractures and luxations of permanent teeth Section 2. Avulsion of permanent teeth Section 3. Traumatic
Sports Dentistry: Treating the athletes in your practice.
 Sports Dentistry: Treating the athletes in your practice. November 3, 2011 David P. Croglio, DDS 2503 Kensington Avenue Amherst, New York 14226 716-839-2820 dmdjcro@aol.com Section 1 Introduction to Sports
Sports Dentistry: Treating the athletes in your practice. November 3, 2011 David P. Croglio, DDS 2503 Kensington Avenue Amherst, New York 14226 716-839-2820 dmdjcro@aol.com Section 1 Introduction to Sports
GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS
 GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS Dentists need to understand that the decision to remove or not reimplant an avulsed incisor must be made very carefully. The loss of such a tooth in
GUIDELINES FOR THE MANAGEMENT OF TRAUMATISED INCISORS Dentists need to understand that the decision to remove or not reimplant an avulsed incisor must be made very carefully. The loss of such a tooth in
ADVANCES IN PEDIATRIC DENTISTRY
 TRIAGE TRAUMATIC DENTAL INJURIES: Critical Steps Kaneta R. Lott, DDS LottSeminars.com EDUCATE INSPIRE LEAD GUIDELINES FOR THE MANAGEMENT OF TRAUMATIC DENTAL INJURIES www.iadt dentaltrauma.org DENTAL TRAUMA
TRIAGE TRAUMATIC DENTAL INJURIES: Critical Steps Kaneta R. Lott, DDS LottSeminars.com EDUCATE INSPIRE LEAD GUIDELINES FOR THE MANAGEMENT OF TRAUMATIC DENTAL INJURIES www.iadt dentaltrauma.org DENTAL TRAUMA
Emergency Management of Trauma
 Aims and Objectives Emergency Management of Trauma Susan Parekh/Paul Ashley Unit of Paediatric Dentistry Knowledge and understanding of the following: Epidemiology of traumatic injuries Classification
Aims and Objectives Emergency Management of Trauma Susan Parekh/Paul Ashley Unit of Paediatric Dentistry Knowledge and understanding of the following: Epidemiology of traumatic injuries Classification
Management of Permanent Tooth Dental Trauma in Children and Young Adolescents
 Management of Permanent Tooth Dental Trauma in Children and Young Adolescents Jessica Y. Lee DDS, MPH, PhD Chair and Distinguished Professor Department of Pediatric Dentistry University of North Carolina
Management of Permanent Tooth Dental Trauma in Children and Young Adolescents Jessica Y. Lee DDS, MPH, PhD Chair and Distinguished Professor Department of Pediatric Dentistry University of North Carolina
Trauma to the Central Incisor: The Story So Far
 Cronicon OPEN ACCESS EC DENTAL SCIENCE Review Article Trauma to the Central Incisor: The Story So Far Dania Siddik* Consultant Paediatric Dentist, Guy s & St Thomas NHS Foundation Trust, London, UK *Corresponding
Cronicon OPEN ACCESS EC DENTAL SCIENCE Review Article Trauma to the Central Incisor: The Story So Far Dania Siddik* Consultant Paediatric Dentist, Guy s & St Thomas NHS Foundation Trust, London, UK *Corresponding
SOUTH CALGARY ENDODONTICS
 Spring 2016 SOUTH CALGARY ENDODONTICS ISSUE 1 FALL 2014 www.southcalgaryendo.ca 403-474-1893 Drs. Staniloff, Kolosowski and Smorang are pleased to announce: Mission Endodontics and South Calgary Endodontics
Spring 2016 SOUTH CALGARY ENDODONTICS ISSUE 1 FALL 2014 www.southcalgaryendo.ca 403-474-1893 Drs. Staniloff, Kolosowski and Smorang are pleased to announce: Mission Endodontics and South Calgary Endodontics
Guidelines for the evaluation and management of traumatic dental injuries
 Dental Traumatology 2001; 17: 193 196 Copyright C Munksgaard 2001 Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY ISSN 1600-4469 Editor s note The International Association of Dental Traumatology
Dental Traumatology 2001; 17: 193 196 Copyright C Munksgaard 2001 Printed in Denmark. All rights reserved DENTAL TRAUMATOLOGY ISSN 1600-4469 Editor s note The International Association of Dental Traumatology
Dental Trauma in children I. 5DM PEDO
 Dental Trauma in children I. 5DM PEDO Childhood is a risky period of life considering trauma (high risk and incidence of injuries) Injuries to the teeth can severely harm a child in these aspects: functional
Dental Trauma in children I. 5DM PEDO Childhood is a risky period of life considering trauma (high risk and incidence of injuries) Injuries to the teeth can severely harm a child in these aspects: functional
Intensive care for the immature pulp Maintaining pulp vitality after a traumatic injury
 Nine-year-old Josh is racing down a hill on his mountain bike. The bike hits a rock and Josh lands on the trail. His mouth is bloody. His front tooth feels funny. He gets up, dusts himself off and rides
Nine-year-old Josh is racing down a hill on his mountain bike. The bike hits a rock and Josh lands on the trail. His mouth is bloody. His front tooth feels funny. He gets up, dusts himself off and rides
Paediatric Dentistry Avulsion: Case reports
 Australian Dental Journal 1997;42.(6):361-6 Paediatric Dentistry Avulsion: Case reports J. E. Rutar, BDSc(Qld), GCEd(Qld)* Abstract Children may present at a dental surgery for management of oro-facial
Australian Dental Journal 1997;42.(6):361-6 Paediatric Dentistry Avulsion: Case reports J. E. Rutar, BDSc(Qld), GCEd(Qld)* Abstract Children may present at a dental surgery for management of oro-facial
Management of the avulsed permanent tooth. A review of current guidelines
 Journal of the International Society of Head and Neck Trauma (ISHANT) Original Article Management of the avulsed permanent tooth. A review of current guidelines Hana M Kennedy Royal London Hospital hana.kennedy05@gmail.com
Journal of the International Society of Head and Neck Trauma (ISHANT) Original Article Management of the avulsed permanent tooth. A review of current guidelines Hana M Kennedy Royal London Hospital hana.kennedy05@gmail.com
Orthodontic splints in dental traumatology
 In italiano, per favore Orthodontic splints in dental traumatology Clinical aid Published on 03/09/96 Gabriele Florìa DDS Firenze Italy The pediatric dentist is often involved in the treatment of the maxillary
In italiano, per favore Orthodontic splints in dental traumatology Clinical aid Published on 03/09/96 Gabriele Florìa DDS Firenze Italy The pediatric dentist is often involved in the treatment of the maxillary
Management of Traumatic Injuries to Children s Teeth
 Continuing Education Brought to you by Management of Traumatic Injuries to Children s Teeth Course Author(s): Steven Schwartz, DDS CE Credits: 2 hours Intended Audience: Dentists, Dental Hygienists, Dental
Continuing Education Brought to you by Management of Traumatic Injuries to Children s Teeth Course Author(s): Steven Schwartz, DDS CE Credits: 2 hours Intended Audience: Dentists, Dental Hygienists, Dental
DENTAL TRAUMA IN DECIDUOUS TEETH
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Dental Trauma in Deciduous Teeth must be made in conjunction with
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Dental Trauma in Deciduous Teeth must be made in conjunction with
September 19. Title: In vitro antibacterial activity of different endodontic irrigants. Author: Claudia Poggio et al.
 2012 September 19 Title: In vitro antibacterial activity of different endodontic irrigants. Author: Claudia Poggio et al. Journal: Dental Traumatology 2012; 28: 205-209 Reviewer: Arnav R. Mistry, DMD Purpose:
2012 September 19 Title: In vitro antibacterial activity of different endodontic irrigants. Author: Claudia Poggio et al. Journal: Dental Traumatology 2012; 28: 205-209 Reviewer: Arnav R. Mistry, DMD Purpose:
Protecting All Children s Teeth Oral Injury
 Protecting All Children s Teeth Oral Injury Introduction Dental injuries are very common, and up to 30% of children injure their primary teeth. These injuries occur most often during the toddler years
Protecting All Children s Teeth Oral Injury Introduction Dental injuries are very common, and up to 30% of children injure their primary teeth. These injuries occur most often during the toddler years
Rehabilitation of esthetics after dental avulsion and impossible replantation: A case report
 2018; 4(1): 265-269 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2018; 4(1): 265-269 2018 IJADS www.oraljournal.com Received: 13-11-2017 Accepted: 14-12-2017 Dr. El harram Sara Postgraduate Student,
2018; 4(1): 265-269 ISSN Print: 2394-7489 ISSN Online: 2394-7497 IJADS 2018; 4(1): 265-269 2018 IJADS www.oraljournal.com Received: 13-11-2017 Accepted: 14-12-2017 Dr. El harram Sara Postgraduate Student,
Clinical Guideline on Management of Acute Dental Trauma
 120 Clinical Guidelines American Academy of Pediatric Dentistry Clinical Guideline on Management of Acute Dental Trauma Originating Council Council on Clinical Affairs Review Council Council on Clinical
120 Clinical Guidelines American Academy of Pediatric Dentistry Clinical Guideline on Management of Acute Dental Trauma Originating Council Council on Clinical Affairs Review Council Council on Clinical
Raymond Hinerman, MD, DDS Dental Emergencies in Emergency Medicine. Who am I? Who am I?(cont) 4/15/2014
 4/15/2014") Raymond Hinerman, MD, DDS Dental Emergencies in Emergency Medicine Who am I? Obtained DDS from WVU Dental School 1993 Post graduate General practice residency 1993-94 ( Hospital based dentistry) General
Raymond Hinerman, MD, DDS Dental Emergencies in Emergency Medicine Who am I? Obtained DDS from WVU Dental School 1993 Post graduate General practice residency 1993-94 ( Hospital based dentistry) General
Smiles for Life. Second Edition. Acute Dental Problems. A National Oral Health Curriculum
 A National Oral Health Curriculum Second Edition Module 4 Acute Dental Problems July 2008 Copyright STFM 2005-2008 Steering Committee Alan B. Douglass, M.D. (Editor and Group Co-Chair) Middlesex Hospital,
A National Oral Health Curriculum Second Edition Module 4 Acute Dental Problems July 2008 Copyright STFM 2005-2008 Steering Committee Alan B. Douglass, M.D. (Editor and Group Co-Chair) Middlesex Hospital,
Treatment Options for the Compromised Tooth
 New Edition Treatment Options for the Compromised Tooth A Decision Guide American Association of Endodontists www.aae.org/treatmentoptions TREATMENT PLANNING CONSIDERATIONS The Treatment Options for the
New Edition Treatment Options for the Compromised Tooth A Decision Guide American Association of Endodontists www.aae.org/treatmentoptions TREATMENT PLANNING CONSIDERATIONS The Treatment Options for the
Non-Surgical management of Apical third root fracture with MTA: A Case report
 International Journal Dental and Medical Sciences Research (IJDMSR) ISSN: 2393-073X Volume1, Issue 2 (Jul- 2017), PP 05-09 www.ijdmsr.com Non-Surgical management of Apical third root fracture with MTA:
International Journal Dental and Medical Sciences Research (IJDMSR) ISSN: 2393-073X Volume1, Issue 2 (Jul- 2017), PP 05-09 www.ijdmsr.com Non-Surgical management of Apical third root fracture with MTA:
DENTAL INJURIES IN SPORTS NICHOLAS E. NICOSIA DDS
 DENTAL INJURIES IN SPORTS NICHOLAS E. NICOSIA DDS Academy for Sports Dentistry International Association for Dental Traumatology The Hockey Smile The Role of the Team Dentist Be a licensed dentist in
DENTAL INJURIES IN SPORTS NICHOLAS E. NICOSIA DDS Academy for Sports Dentistry International Association for Dental Traumatology The Hockey Smile The Role of the Team Dentist Be a licensed dentist in
REIMPLANTATION OF AVULSED TOOTH- A CASE REPORT
 Case Report REIMPLANTATION OF AVULSED TOOTH- A CASE REPORT Grover PS 1, Kaur S 2 1 Senior Consultant, 2 Junior Consultant, Dr. Grover s Dental and Implant Center, Ludhiana ABSTRACT This paper describes
Case Report REIMPLANTATION OF AVULSED TOOTH- A CASE REPORT Grover PS 1, Kaur S 2 1 Senior Consultant, 2 Junior Consultant, Dr. Grover s Dental and Implant Center, Ludhiana ABSTRACT This paper describes
22 yo female presented for evaluation and treatment of tooth #24
 Erick Sato Case Report Non-Surgical Root Canal Therapy #24 22 yo female presented for evaluation and treatment of tooth #24 Subjective: Chief Complaint: My tooth is dark, and my dentist referred me for
Erick Sato Case Report Non-Surgical Root Canal Therapy #24 22 yo female presented for evaluation and treatment of tooth #24 Subjective: Chief Complaint: My tooth is dark, and my dentist referred me for
Indication for Intentional Replantation of Teeth
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. V (Dec. 2017), PP 36-42 www.iosrjournals.org Indication for Intentional Replantation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 12 Ver. V (Dec. 2017), PP 36-42 www.iosrjournals.org Indication for Intentional Replantation
IDENTIFYING URGENT DENTAL CARE
 IDENTIFYING URGENT DENTAL CARE Katie Kosten, DMD Director of Community Dentistry Assistant Professor Pediatric and Community Dentistry Southern Illinois University School of Dental Medicine WELCOME! DISCLOSURE
IDENTIFYING URGENT DENTAL CARE Katie Kosten, DMD Director of Community Dentistry Assistant Professor Pediatric and Community Dentistry Southern Illinois University School of Dental Medicine WELCOME! DISCLOSURE
Examination of teeth and gingiva
 Examination of teeth and gingiva Siriporn Chattipakorn, DDS, PhD. SUBJECTIVE HISTORY Chief complaint In patient s own words My tooth hurts when I chew hard foods I can t drink cold drink I have bad breath
Examination of teeth and gingiva Siriporn Chattipakorn, DDS, PhD. SUBJECTIVE HISTORY Chief complaint In patient s own words My tooth hurts when I chew hard foods I can t drink cold drink I have bad breath
DOD MPL, GENERAL DENTISTRY, GENERATED FROM CCQAS FOR AFMS USE, June
 LIST OF CLINICAL PRIVILEGES GENERAL DENTISTRY AUTHORITY: Title 10, U.S.C. Chapter 55, Sections 1094 and 1102. PRINCIPAL PURPOSE: To define the scope and limits of practice for individual providers. Privileges
LIST OF CLINICAL PRIVILEGES GENERAL DENTISTRY AUTHORITY: Title 10, U.S.C. Chapter 55, Sections 1094 and 1102. PRINCIPAL PURPOSE: To define the scope and limits of practice for individual providers. Privileges
Multiple Dentoalveolar Traumatic Lesions: Report of a Case and Proposition of Dental Polytrauma as a New Term
 Multiple Dentoalveolar Traumatic Lesions: Report of a Case and Proposition of Dental Polytrauma as a New Term Abstract Traumatic injuries to permanent teeth are common, and dramatic episodes can occur
Multiple Dentoalveolar Traumatic Lesions: Report of a Case and Proposition of Dental Polytrauma as a New Term Abstract Traumatic injuries to permanent teeth are common, and dramatic episodes can occur
Questions for final state exam
 Questions for final state exam 1. 1. Estetic filling in operative dentistry 2. Pulp-dentin organ, morphology and functions, pulp-periodontal complex 3. The process(es) of tooth eruption, disorders linked
Questions for final state exam 1. 1. Estetic filling in operative dentistry 2. Pulp-dentin organ, morphology and functions, pulp-periodontal complex 3. The process(es) of tooth eruption, disorders linked
5. Injuries to the tooth supporting structures in the permanent dentition
 Research Signpost Trivandrum Kerala, India Dental and Maxillofacial Trauma Challenges in Low and Middle Income Countries, 2018: 79-96 ISBN: 978-81-308-0577-1 Editors: Febronia Kokulengya Kahabuka, Irene
Research Signpost Trivandrum Kerala, India Dental and Maxillofacial Trauma Challenges in Low and Middle Income Countries, 2018: 79-96 ISBN: 978-81-308-0577-1 Editors: Febronia Kokulengya Kahabuka, Irene
This information sheet lists the Cost of Treatment Regulations amounts ACC can pay for dentistry treatments.
 All about Dentists costs Effective 01 December 2018 ACC Information sheet This information sheet lists the Cost of Treatment Regulations amounts ACC can pay for dentistry treatments. DE1 DE2 Dental consultation,
All about Dentists costs Effective 01 December 2018 ACC Information sheet This information sheet lists the Cost of Treatment Regulations amounts ACC can pay for dentistry treatments. DE1 DE2 Dental consultation,
Clinical guideline on management of acute dental trauma
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 Clinical guideline on management Originating Council Council on Clinical Affairs Review Council
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 Clinical guideline on management Originating Council Council on Clinical Affairs Review Council
Autotransplantation and restoration of an avulsed anterior tooth: A multidisciplinary approach
 Autotransplantation and restoration of an avulsed anterior tooth: A multidisciplinary approach Yuli Berlin-Broner 1 Ysidora Torrealba 2 Liran Levin 3 1 Division of Endodontics, Faculty of Medicine and
Autotransplantation and restoration of an avulsed anterior tooth: A multidisciplinary approach Yuli Berlin-Broner 1 Ysidora Torrealba 2 Liran Levin 3 1 Division of Endodontics, Faculty of Medicine and
Diagnosis. overt Examination. Definitive Examination. History. atient interview. Personal History. Clinical Examination.
 Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
Management of Traumatic Dental Injury after Periodontal Surgery in Patient with Hereditary Gingival Fibromatosis: Case Report
 Management of Traumatic Dental Injury after Periodontal Surgery in Patient with Hereditary Gingival Fibromatosis: Case Report Koji Inagaki 1,2, Hidehiko Kamei 2, Akio Mitani 2, Toshihide Noguchi 2 1 Department
Management of Traumatic Dental Injury after Periodontal Surgery in Patient with Hereditary Gingival Fibromatosis: Case Report Koji Inagaki 1,2, Hidehiko Kamei 2, Akio Mitani 2, Toshihide Noguchi 2 1 Department
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy or national coding updates, inclusion of a code on the code tables
Treatment Options for the Compromised Tooth: A Decision Guide
 Treatment Options for the Compromised Tooth: A Decision Guide www.aae.org/treatmentoptions ROOT AMPUTATION, HEMISECTION, BICUSPIDIZATION Case One Hemisection of the distal root of tooth #19. 13 mo. Recall
Treatment Options for the Compromised Tooth: A Decision Guide www.aae.org/treatmentoptions ROOT AMPUTATION, HEMISECTION, BICUSPIDIZATION Case One Hemisection of the distal root of tooth #19. 13 mo. Recall
Pediatric endodontics. Diagnosis, Direct and Indirect pulp capping DR.SHANKAR
 Pediatric endodontics Diagnosis, Direct and Indirect pulp capping DR.SHANKAR WHY TO PRESERVE PRIMARY TEETH? The preservation of the primary dentition until their normal anticipated exfoliation can be justified
Pediatric endodontics Diagnosis, Direct and Indirect pulp capping DR.SHANKAR WHY TO PRESERVE PRIMARY TEETH? The preservation of the primary dentition until their normal anticipated exfoliation can be justified
Minimal Management of Traumatically Luxated Immature Maxillary Permanent Incisors
 imedpub Journals http://journals.imedpub.com Journal of Orthodontics & Endodontics Minimal Management of Traumatically Luxated Immature Maxillary Permanent Incisors Peter M. Di Fiore 1 Diplomate, American
imedpub Journals http://journals.imedpub.com Journal of Orthodontics & Endodontics Minimal Management of Traumatically Luxated Immature Maxillary Permanent Incisors Peter M. Di Fiore 1 Diplomate, American
Healing of external inflammatory root resorption - a case report
 Healing of external inflammatory root resorption - a case report Mithra N. Hegde * Deepak Pardal ** ABSTRACT Case report describes a radiographic follow-up of healing of external inflammatory root resorption
Healing of external inflammatory root resorption - a case report Mithra N. Hegde * Deepak Pardal ** ABSTRACT Case report describes a radiographic follow-up of healing of external inflammatory root resorption
Treatment and orthodontic movement of a root-fractured maxillary central incisor with an immature apex: 10-year follow-up
 doi:10.1111/j.1365-2591.2010.01790.x CASE REPORT Treatment and orthodontic movement of a root-fractured maxillary central incisor with an immature apex: 10-year follow-up A. Mendoza 1, E. Solano 2 & J.
doi:10.1111/j.1365-2591.2010.01790.x CASE REPORT Treatment and orthodontic movement of a root-fractured maxillary central incisor with an immature apex: 10-year follow-up A. Mendoza 1, E. Solano 2 & J.
Treatment of a traumatically intruded maxillary incisor
 A multidisciplinary approach to the treatment of an intruded maxillary permanent incisor complicated by the presence of two mesiodentes Ari Kupietzky, DMD MSc Ilan Rotstein, CD Dov Kischinovsky DMD Dr.
A multidisciplinary approach to the treatment of an intruded maxillary permanent incisor complicated by the presence of two mesiodentes Ari Kupietzky, DMD MSc Ilan Rotstein, CD Dov Kischinovsky DMD Dr.
Reposition of intruded permanent incisor by a combination of surgical and orthodontic approach: a case report
 Reposition of intruded permanent incisor by a combination of surgical and orthodontic approach: a case report Ki-Taeg Jang* / Jung-Wook Kim** / Sang-Hoon Lee*** / Chong-Chul Kim**** / Se-Hyun Hahn*****
Reposition of intruded permanent incisor by a combination of surgical and orthodontic approach: a case report Ki-Taeg Jang* / Jung-Wook Kim** / Sang-Hoon Lee*** / Chong-Chul Kim**** / Se-Hyun Hahn*****
Educational Training Document
 Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Current concepts in the management of dental trauma
 Current concepts in the management of dental trauma S ALBADRI BDS, PHD, MFDS, MPAEDENT, FDS (PAED DENT),FHES READER /HONORARY CONSULTANT IN PAEDIATRIC DENTISTRY Introduction ØAround one in ten children
Current concepts in the management of dental trauma S ALBADRI BDS, PHD, MFDS, MPAEDENT, FDS (PAED DENT),FHES READER /HONORARY CONSULTANT IN PAEDIATRIC DENTISTRY Introduction ØAround one in ten children
Management of Dental Trauma in a Primary Care Setting
 Guidance for the Clinician in Rendering Pediatric Care CLINICAL REPORT Management of Dental Trauma in a Primary Care Setting abstract The American Academy of Pediatrics and its Section on Oral Health have
Guidance for the Clinician in Rendering Pediatric Care CLINICAL REPORT Management of Dental Trauma in a Primary Care Setting abstract The American Academy of Pediatrics and its Section on Oral Health have
ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2018)
") ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2018) I Objectives a. Determine the ability of the candidate to practice as a specialist and provide consultation
ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2018) I Objectives a. Determine the ability of the candidate to practice as a specialist and provide consultation
Pulp Prognosis of Crown-Related Fractures, in Relation to Presence of Luxation Injury and Root Development Stage
 Pulp Prognosis of Crown-Related Fractures, in Relation to Presence of Luxation Injury and Root Development Stage Didem Atabek, Alev Alacam, Itır Aydintug, İlknur Baldag Department of Pedodontics, Faculty
Pulp Prognosis of Crown-Related Fractures, in Relation to Presence of Luxation Injury and Root Development Stage Didem Atabek, Alev Alacam, Itır Aydintug, İlknur Baldag Department of Pedodontics, Faculty
Australian Dental Journal
 Australian Dental Journal The official journal of the Australian Dental Association Australian Dental Journal 2016; 61:(1 Suppl): 120 127 doi: 10.1111/adj.12403 Life cycles of traumatized teeth: long-term
Australian Dental Journal The official journal of the Australian Dental Association Australian Dental Journal 2016; 61:(1 Suppl): 120 127 doi: 10.1111/adj.12403 Life cycles of traumatized teeth: long-term
Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control
 Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
Readings: Fundamentals of Operative Dentistry, 3 nd Edition; Summitt, et al Chapters 5, 6 and 8 Pulpal Protection: bases, liners, sealers, caries control Module D: Pulp capping-caries control REST 528A
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS
 SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
The periodontium attempts to accommodate to the forces exerted to the crown. This adaptive capacity varies in different persons and in the same person
 The periodontium attempts to accommodate to the forces exerted to the crown. This adaptive capacity varies in different persons and in the same person at different times. The effect of occlusal forces
The periodontium attempts to accommodate to the forces exerted to the crown. This adaptive capacity varies in different persons and in the same person at different times. The effect of occlusal forces
Sequelae and prognosis of intruded primary incisors: a retrospective study
 Scientic Article Sequelae and prognosis of intruded primary incisors: a retrospective study Gideon Holan, DMD Diana Ram, Dr. Odontol Dr. Holan is senior lecturer and Dr. Ram is instructor, Department of
Scientic Article Sequelae and prognosis of intruded primary incisors: a retrospective study Gideon Holan, DMD Diana Ram, Dr. Odontol Dr. Holan is senior lecturer and Dr. Ram is instructor, Department of
Case Report Pulp Revascularization in Immature Permanent Tooth with Apical Periodontitis Using Mineral Trioxide Aggregate
 Case Reports in Medicine, Article ID 564908, 5 pages http://dx.doi.org/10.1155/2014/564908 Case Report Pulp Revascularization in Immature Permanent Tooth with Apical Periodontitis Using Mineral Trioxide
Case Reports in Medicine, Article ID 564908, 5 pages http://dx.doi.org/10.1155/2014/564908 Case Report Pulp Revascularization in Immature Permanent Tooth with Apical Periodontitis Using Mineral Trioxide
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology
 QUALITY GUIDELINES Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology Abstract. Quality guidelines for endodontic treatment: consensus report of the.
QUALITY GUIDELINES Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology Abstract. Quality guidelines for endodontic treatment: consensus report of the.
A combined approach with passive and active repositioning of a traumatically intruded immature permanent incisor
 H.-J. Kim*-**, Y.-I. Kim***, K.-S. Min**-**** *Department of Conservative Dentistry, Pusan National University Hospital, Busan, Korea **Department of Conservative Dentistry, School of Dentistry and Institute
H.-J. Kim*-**, Y.-I. Kim***, K.-S. Min**-**** *Department of Conservative Dentistry, Pusan National University Hospital, Busan, Korea **Department of Conservative Dentistry, School of Dentistry and Institute
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits
 COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2017)
") ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2017) I Objectives a. Determine the ability of the candidate to practice as a specialist and provide consultation
ENDODONTICS SAUDI BOARD PROGRAM SAUDI BOARD FINAL CLINICAL EXAMINATION OF ENDODONTICS (2017) I Objectives a. Determine the ability of the candidate to practice as a specialist and provide consultation
Plaque and Occlusion in Periodontal Disease Wednesday, February 25, :54 AM
 Plaque and Occlusion in Periodontal Disease Wednesday, February 25, 2015 9:54 AM 1. The definition of Trauma From Occlusion: Primary TFO, Secondary TFO, and Combined TFO 2. Clinical and Radiographic signs
Plaque and Occlusion in Periodontal Disease Wednesday, February 25, 2015 9:54 AM 1. The definition of Trauma From Occlusion: Primary TFO, Secondary TFO, and Combined TFO 2. Clinical and Radiographic signs
CHAPTER 6 Dental Services
 CHAPTER 6 Dental Services Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 BLOCK 450 Dental examination 97012-00 Periodic oral examination 97013-00 Limited
CHAPTER 6 Dental Services Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 BLOCK 450 Dental examination 97012-00 Periodic oral examination 97013-00 Limited
Intrusive luxation of 60 permanent incisors: a retrospective study of treatment and outcome
 Dental Traumatology 2011; doi: 10.1111/j.1600-9657.2011.01088.x Intrusive luxation of 60 permanent incisors: a retrospective study of treatment and outcome Georgios Tsilingaridis 1, Barbro Malmgren 1,2,
Dental Traumatology 2011; doi: 10.1111/j.1600-9657.2011.01088.x Intrusive luxation of 60 permanent incisors: a retrospective study of treatment and outcome Georgios Tsilingaridis 1, Barbro Malmgren 1,2,
MANAGEMENT OF ROOT RESORPTION- A REBIRTH CASE REPORTS DEPARTMENT OF CONSERVATIVE DENTISTRY AND ENDODONTICS
 MANAGEMENT OF ROOT RESORPTION- A REBIRTH CASE REPORTS AUTHORS Dr. SHALINI.H, PG Student Dr. B. RAMAPRABHA, MDS Professor Dr. M. KAVITHA, MDS Professor and HOD DEPARTMENT OF CONSERVATIVE DENTISTRY AND ENDODONTICS
MANAGEMENT OF ROOT RESORPTION- A REBIRTH CASE REPORTS AUTHORS Dr. SHALINI.H, PG Student Dr. B. RAMAPRABHA, MDS Professor Dr. M. KAVITHA, MDS Professor and HOD DEPARTMENT OF CONSERVATIVE DENTISTRY AND ENDODONTICS
21 NCAC 16G.0101 FUNCTIONS THAT MAY BE DELEGATED
 1 1 1 1 1 1 1 1 0 1 0 1 1 NCAC 1G.01is proposed for amendment as follows: 1 NCAC 1G.01 FUNCTIONS THAT MAY BE DELEGATED A dental hygienist may be delegated functions to be performed under the control and
1 1 1 1 1 1 1 1 0 1 0 1 1 NCAC 1G.01is proposed for amendment as follows: 1 NCAC 1G.01 FUNCTIONS THAT MAY BE DELEGATED A dental hygienist may be delegated functions to be performed under the control and

Staywell FL Child Medicaid Plan Benefits
 The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
FEE SCHEDULE. Complete Dental Plan is a discount plan offered and administered by our organization at:
 FEE SCHEDULE Complete Dental Plan is a discount plan offered and administered by our organization at: 7801 CORAL WAY SUITE # 106, MIAMI, FL 33144 (786) 326-6873 F (305) 6979785 COMPLETE DENTAL PLAN HIGHLIGHTS
FEE SCHEDULE Complete Dental Plan is a discount plan offered and administered by our organization at: 7801 CORAL WAY SUITE # 106, MIAMI, FL 33144 (786) 326-6873 F (305) 6979785 COMPLETE DENTAL PLAN HIGHLIGHTS
Periodontal Disease. Radiology of Periodontal Disease. Periodontal Disease. The Role of Radiology in Assessment of Periodontal Disease
 Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Australian Dental Journal
 Australian Dental Journal The official journal of the Australian Dental Association Australian Dental Journal 2014; 59: 240 244 doi: 10.1111/adj.12164 Management of traumatically intruded young permanent
Australian Dental Journal The official journal of the Australian Dental Association Australian Dental Journal 2014; 59: 240 244 doi: 10.1111/adj.12164 Management of traumatically intruded young permanent
Principles of endodontic surgery
 Principles of endodontic surgery Note: the doctor said that this lecture mainly contain notes, so we should study it from the book for further information (chapter 18) principles of endodontic surgery.
Principles of endodontic surgery Note: the doctor said that this lecture mainly contain notes, so we should study it from the book for further information (chapter 18) principles of endodontic surgery.
The traumatic injury of an immature permanent tooth can lead to the loss of pulp
 Regenerative Treatment of an Immature, Traumatized Tooth With Apical Periodontitis: Report of a Case Elisabetta Cotti, DDS, MS, Manuela Mereu, DDS, and Daniela Lusso, DDS Abstract This case report describes
Regenerative Treatment of an Immature, Traumatized Tooth With Apical Periodontitis: Report of a Case Elisabetta Cotti, DDS, MS, Manuela Mereu, DDS, and Daniela Lusso, DDS Abstract This case report describes
Endodontics Cracked Tooth: How to manage it in daily practice
 Calogero Bugea Endodontics Cracked Tooth: How to manage it in daily practice 5 Feb 2016 Tooth Fractures are not rare, surface cracks, or craze lines, are relatively common in teeth. In most of cases they
Calogero Bugea Endodontics Cracked Tooth: How to manage it in daily practice 5 Feb 2016 Tooth Fractures are not rare, surface cracks, or craze lines, are relatively common in teeth. In most of cases they
An Overview of Your. Dental Benefits. Educators Health Alliance
 An Overview of Your Dental Benefits Educators Health Alliance 2 \ DENTAL BENEFITS OVERVIEW \ 5 A Dental Plan Exclusively for Educators Health Alliance Members Something to Smile About... The EHA makes
An Overview of Your Dental Benefits Educators Health Alliance 2 \ DENTAL BENEFITS OVERVIEW \ 5 A Dental Plan Exclusively for Educators Health Alliance Members Something to Smile About... The EHA makes
Intentional reimplantation - two case reports
 Case Report Intentional reimplantation - two case reports GURPREET SINGH * NIKHIL BAHUGUNA ** PARDEEP MAHAJAN *** ABSTRACT Intentional reimplantation is a procedure in which an intentional tooth extraction
Case Report Intentional reimplantation - two case reports GURPREET SINGH * NIKHIL BAHUGUNA ** PARDEEP MAHAJAN *** ABSTRACT Intentional reimplantation is a procedure in which an intentional tooth extraction
Principles of diagnosis in Endodontics. Pain History. Patient Assessment. Examination. Examination 11/07/2014
 Principles of diagnosis in Endodontics Diagnosis, pulpitis, perio-endo. Treatment planning & case selection Patients assessment Special tests which help us diagnose pulpal disease How reliable are they?
Principles of diagnosis in Endodontics Diagnosis, pulpitis, perio-endo. Treatment planning & case selection Patients assessment Special tests which help us diagnose pulpal disease How reliable are they?
Pulpal changes following trauma. When is it necessary to undertake RCT? Outline. Dentine-pulp complex
 Pulpal changes following trauma. When is it necessary to undertake RCT? Dr Sara Firouzabadi BDSc (Hons) QLD 2003 and DCD (Endo) VIC 2009 sara@northwesternendodontics.com.au Courtesy of Dr Ennio Rebellato
Pulpal changes following trauma. When is it necessary to undertake RCT? Dr Sara Firouzabadi BDSc (Hons) QLD 2003 and DCD (Endo) VIC 2009 sara@northwesternendodontics.com.au Courtesy of Dr Ennio Rebellato
 This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
 This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
Transient Tooth Discoloration After Periodontal Instrumentation of an Aggressive Periodontitis. A Case Report
 Transient Tooth Discoloration After Periodontal Instrumentation of an Aggressive Periodontitis. A Case Report Julio C Rincon A*, Zahida Oakley*, Paul Abbott *Department of Periodontology and Implant Dentistry.
Transient Tooth Discoloration After Periodontal Instrumentation of an Aggressive Periodontitis. A Case Report Julio C Rincon A*, Zahida Oakley*, Paul Abbott *Department of Periodontology and Implant Dentistry.
RAJ M. SAINI, DDS, MSD
 Restoring and Maintaining Periodontal Health with Orthodontic Treatment RAJ M. SAINI, DDS, MSD rajmsaini@yahoo.com Diplomate Of The American Board Of Orthodontics Clinical Professor Of Orthodontics New
Restoring and Maintaining Periodontal Health with Orthodontic Treatment RAJ M. SAINI, DDS, MSD rajmsaini@yahoo.com Diplomate Of The American Board Of Orthodontics Clinical Professor Of Orthodontics New
Clinical Management of Horizontal Mid-Root Fracture in Maxillary Central Incisor - A Case Report
 Clinical Management of Horizontal Mid-Root Fracture in Maxillary Central Incisor - A Case Report Shavina Gupta 1, Anuradha Rani 2, Ritu Mangla 3 1 Assistant Professor, Department of Conservative Dentistry
Clinical Management of Horizontal Mid-Root Fracture in Maxillary Central Incisor - A Case Report Shavina Gupta 1, Anuradha Rani 2, Ritu Mangla 3 1 Assistant Professor, Department of Conservative Dentistry
SCD Case Study. scdlab.com 1
 SCD Case Study Resorption is associated with either a physiologic or a pathologic process resulting in a loss of dentine, cementum and/or bone (www.aae.org/glossary). The aetiology for resorption starts
SCD Case Study Resorption is associated with either a physiologic or a pathologic process resulting in a loss of dentine, cementum and/or bone (www.aae.org/glossary). The aetiology for resorption starts
NON-SURGICAL ENDODONTICS
 NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.02 Effective Date: February 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.02 Effective Date: February 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
NON-SURGICAL ENDODONTICS
 NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
NON-SURGICAL ENDODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG009.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
For Dentists and Other Dental Professionals: Dental Screening Program for Patients Who May Need Hematopoietic Stem Cell Transplantation (HSCT)
") For Dentists and Other Dental Professionals: Dental Screening Program for Patients Who May Need Hematopoietic Stem Cell Transplantation (HSCT) Dear Dental Care Provider, Thank you for your contribution
For Dentists and Other Dental Professionals: Dental Screening Program for Patients Who May Need Hematopoietic Stem Cell Transplantation (HSCT) Dear Dental Care Provider, Thank you for your contribution
Transverse fracture of a tooth root as a consequence of long-term traumatic occlusionda case report
 Journal of Dental Sciences (2010) 5, 237e241 available at www.sciencedirect.com journal homepage: www.e-jds.com Case Report Transverse fracture of a tooth root as a consequence of long-term traumatic occlusionda
Journal of Dental Sciences (2010) 5, 237e241 available at www.sciencedirect.com journal homepage: www.e-jds.com Case Report Transverse fracture of a tooth root as a consequence of long-term traumatic occlusionda
Treatment of Extrusive Luxation in Permanent Teeth: Literature Review with Systematic Criteria
 REVIEW ARTICLE Treatment of Extrusive Luxation in Permanent Teeth: Literature 10.5005/jp-journals-10024-2024 Review with Systematic Criteria Treatment of Extrusive Luxation in Permanent Teeth: Literature
REVIEW ARTICLE Treatment of Extrusive Luxation in Permanent Teeth: Literature 10.5005/jp-journals-10024-2024 Review with Systematic Criteria Treatment of Extrusive Luxation in Permanent Teeth: Literature
Surgical Therapy. Tuesday, April 2, 13. Alessan"o Geminiani, DDS, MS
 Surgical Therapy Alessan"o Geminiani, DDS, MS Periodontal Flap: a surgical procedure in which incisions are made in the gingiva or mucosa to allow for separation of the epithelium and connective tissues
Surgical Therapy Alessan"o Geminiani, DDS, MS Periodontal Flap: a surgical procedure in which incisions are made in the gingiva or mucosa to allow for separation of the epithelium and connective tissues
Fee Schedule Detail Procedure Procedure Description Code Fee
 Fee Schedule Detail Procedure Procedure Description Code Fee D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT $ 32.29 D0140 LIMITED ORAL EVALUATION-PROBLEM FOCUSED $ 53.02 D0150 COMPREHENSIVE ORAL
Fee Schedule Detail Procedure Procedure Description Code Fee D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT $ 32.29 D0140 LIMITED ORAL EVALUATION-PROBLEM FOCUSED $ 53.02 D0150 COMPREHENSIVE ORAL
Endodontic Treatment After Autotransplantation of Tooth with Complete Root Formation
 Endodontic Treatment After Autotransplantation of Tooth with Complete Root Formation Caio Cesar Souza 1, Carlos Eduardo da Silveria Bueno 1, Augusto Shogi Kato 1, Rina Andrea Pelegrine 1 Ana Paula Simezo
Endodontic Treatment After Autotransplantation of Tooth with Complete Root Formation Caio Cesar Souza 1, Carlos Eduardo da Silveria Bueno 1, Augusto Shogi Kato 1, Rina Andrea Pelegrine 1 Ana Paula Simezo
Course Syllabus Wayne County Community College District DA 120 Dental Specialties
 Course Syllabus Wayne County Community College District DA 120 Dental Specialties CREDIT HOURS: 2.00 CONTACT HOURS:.00 COURSE DESCRIPTION: This is a lecture course designed to expose the dental assisting
Course Syllabus Wayne County Community College District DA 120 Dental Specialties CREDIT HOURS: 2.00 CONTACT HOURS:.00 COURSE DESCRIPTION: This is a lecture course designed to expose the dental assisting
Dental materials and cements, and its use in children
 Dental materials and cements, and its use in children Study objective Discuss the role and importance of cements in paediatric dentistry Calcium hydroxide This is a colourless crystal or white powder prepared
Dental materials and cements, and its use in children Study objective Discuss the role and importance of cements in paediatric dentistry Calcium hydroxide This is a colourless crystal or white powder prepared
14/09/15. Assessment of Periodontal Disease. Outline. Why is Periodontal assessment needed? The Basics of Periodontal assessment
 Assessment of Periodontal Disease Dr Wendy Turner Outline Why is Periodontal assessment needed? The Basics of Periodontal assessment Probing: Basic Periodontal Examination for adults and children. Detailed
Assessment of Periodontal Disease Dr Wendy Turner Outline Why is Periodontal assessment needed? The Basics of Periodontal assessment Probing: Basic Periodontal Examination for adults and children. Detailed