The Individual Dental & Vision Benefit Program
|
|
|
- Reynard Boone
- 5 years ago
- Views:
Transcription

1 The Individual Dental & Vision Benefit Program Please complete the enrollment form(s) and return to: 751 E. Southlake Blvd., Suite 120 Southlake, Tx E. Southlake Blvd. Suite 120, Southlake, Tx *

2
3
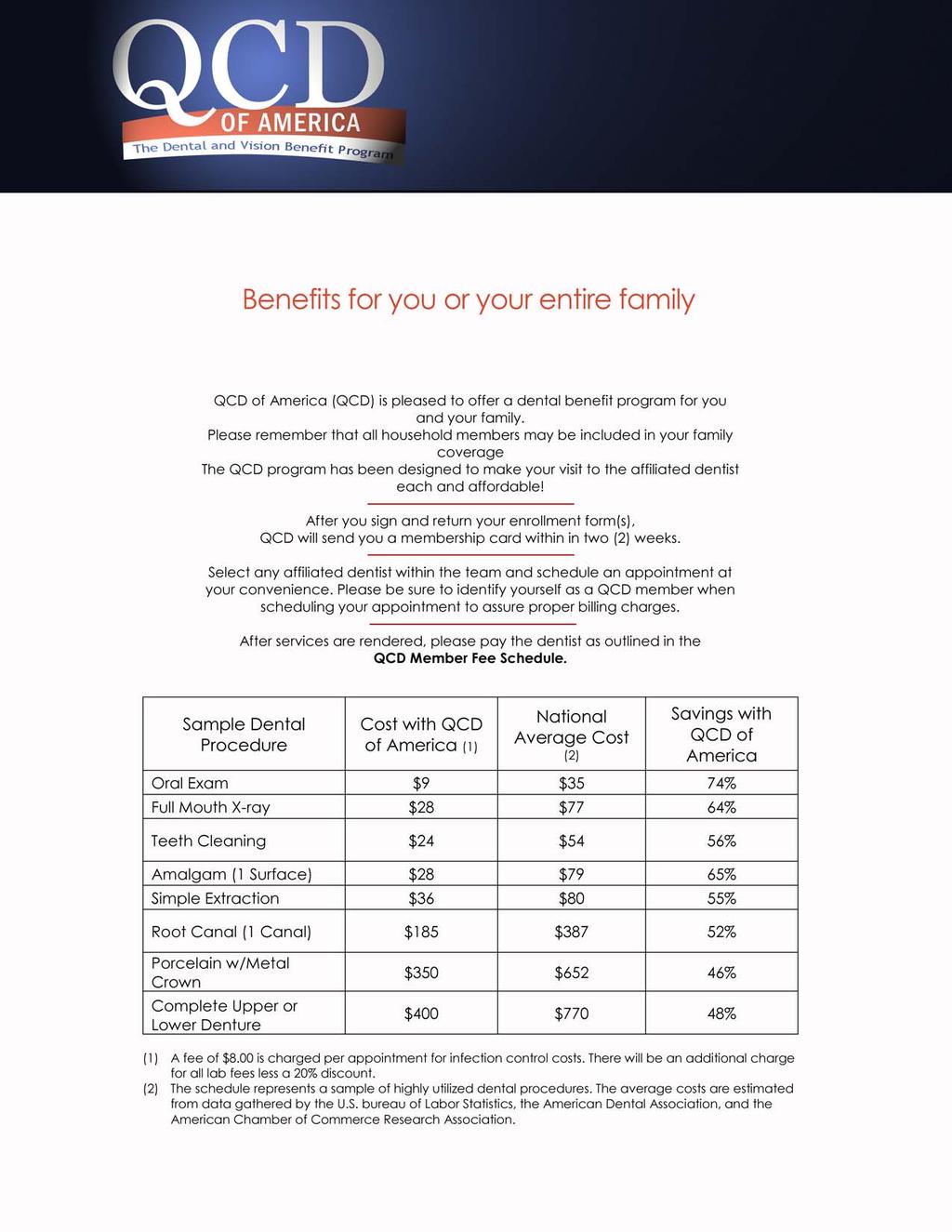
4 Cost Comparison

5 How to enroll QCD of America Individual Enrollment 751 E. Southlake Blvd., Suite 120 Southlake, Tx Phone:
6 Schedule of Programs Fees Procedure Number Member Fee Procedure Number Member Fee DIAGNOSTIC DENTISTRY D0120 PERIODICAL ORAL EXAMINATION... $9.00 D0140 LIMITED ORAL EXAMINATION, PROBLEM FOCUSED... $12.00 D0150 COMPREHENSIVE ORAL EXAMINATION... $18.00 D0210 INTRAORAL X - RAY COMPLETE SERIES... $28.00 D0460 PULP VITALITY TEST... $15.00 D9999 ASEPSIS FEE (INFECTION CONTROL)... $8.00 ALL BITEWING / SINGLE FILM X-RAYS... 20% DISCOUNT PREVENTATIVE DENTISTRY D1110 PROPHYLAXIS ADULT... $24.00 D1120 PROPHYLAXIS CHILD... $24.00 D1203 APPLICATION TOPICAL FLUORIDE CHILD... $5.00 D1204 APPLICATION TOPICAL FLUORIDE ADULT... $5.00 D1351 SEALANT-PER TOOTH... $14.00 D1510 SPACE MAINTAINER - FIXED UNILATERAL... $60.00 D1515 SPACE MAINTAINER - FIXED BILATERAL... $75.00 A specific preventative treatment may present unusual circumstances requiring an additional cost. Please consult the affiliated dentist as to the total procedure cost prior to treatment. COSMETIC ALL COSMETIC DENTISTRY... 20% DISCOUNT RESTORATIVE DENTISTRY D2140 AMALGAM - 1 SURFACE, PRIMARY OR PERMANENT... $28.00 D2150 AMALGAM - 2 SURFACES, PRIMARY OR PERMANENT... $36.00 D2160 AMALGAM - 3 SURFACES, PRIMARY OR PERMANENT... $46.00 D2161 AMALGAM - 4 OR MORE SURFACES, PRIMARY OR PERMANENT... $56.00 D2330 COMPOSITE RESIN - 1 SURFACE, ANTERIOR... $38.00 D2331 COMPOSTIE RESIN - 2 SURFACES, ANTERIOR... $46.00 D2332 COMPOSITE RESIN - 3 SURFACES, ANTERIOR... $56.00 D2335 COMPOSITE RESIN - 4 OR MORE SURFACES OR INVOLVING INCISAL ANGLE, ANTERIOR... $66.00 D2391 COMPOSITE RESIN - 1 SURFACE, POSTERIOR... $50.00 D2392 COMPOSITE RESIN - 2 SURFACES, POSTERIOR... $65.00 D2393 COMPOSTIE RESIN - 3 SURFACES, POSTERIOR... $85.00 D2394 COMPOSITE RESIN - 4 OR MORE SURFACES, POSTERIOR... $95.00 D2750 CROWN - PORCELAIN TO HIGH NOBLE METAL (GOLD AND LAB FEES ADDITIONAL)... $ D2751 CROWN - PORCELAIN TO BASE METAL (LAB FEES ADDITIONAL)... $ D2920 RECEMENT CROWN... $20.00 D2931 PREFABRICATED STAINLESS STEEL CROWN... $48.00 D2940 SEDATIVE FILLING... $16.00 D2950 CORE BUILDUP, (INCLUDING ANY PINS)... $55.00 D2951 PIN RETENTION (PER TOOTH)... $20.00 D2952 CAST POST AND CORE IN ADDITION TO CROWN... $75.00 D2953 EACH ADDITIONAL CAST POST (SAME TOOTH)... $40.00 D2954 PREFAB POST / CORE IN ADDITION TO CROWN... $60.00 D2970 TEMPORARY CROWN (FRACTURED TOOTH)... $40.00 ENDODONTICS D3110 PULP CAP, DIRECT... $19.00 D3120 PULP CAP, INDIRECT... $24.00 D3220 PULPOTOMY... $35.00 D3310 ROOT CANAL, ANTERIOR... $ D3320 ROOT CANAL, BICUSPID... $ D3330 ROOT CANAL, MOLAR.. $ D3920 HEMISECTIO... $65.00 A specific root canal treatment or re-treatment may present unusual circumstances requiring additional cost. Please consult the affiliated dentist as to the total procedure cost prior to treatment. PERIODONTICS D4210 GINGIVECTOMY/GINGIVOPLASTY (PER QUADRANT)..$ D4211 GINGIVECTOMY/GINGIVOPLASTY - (PER TOOTH)... $50.00 D4240 GINGIVAL FLAP PROCEDURE, INCLUDING ROOT PLANING - (PER QUADRANT)... $ D4260 OSSEOUS SURGERY-(PER QUADRANT) (INCLUDING FLAP ENTRY AND CLOSURE)... $ D4341 PERIODONTAL SCALING AND ROOT PLANING - (PER QUADRANT)... $75.00 D4355 FULL MOUTH DEBRIDEMENT... $70.00 D4910 PERIODONTAL MAINTENANCE PROCEDURES FOLLOWING ACTIVE THERAPY... $30.00 A specific periodontal treatment may present unusual circumstances requiring an additional cost. Please consult the affiliated dentist as to the total procedure cost prior to treatment. PROSTHODONTICS REMOVABLE (LAB FEES ADDITIONAL COST) D5110 COMPLETE UPPER DENTURE (INCLUDING SIX MONTHS POST CARE)... $ D5120 COMPLETE LOWER DENTURE (INCLUDING SIX MONTHS POST CARE)... $ D5130 IMMEDIATE UPPER... $ D5140 IMMEDIATE LOWER... $ D5211 UPPER PARTIAL DENTURE RESIN BASE... $ D5212 LOWER PARTIAL DENTURE RESIN BASE... $ D5213 UPPER PARTIAL PREDOMINANTLY CAST BASE... $ D5214 LOWER PARTIAL PERDOMINANTLY CAST BASE... $ D5410 ADJUST COMPLETE DENTURE... $15.00 D5510 REPAIR BROKEN COMPLETE DENTURE BASE... $40.00 D5610 REPAIR RESIN DENTURE BASE... $35.00 D5630 REPAIR OR REPLACE BROKEN CLASP... $45.00 D5640 REPLACE BROKEN TEETH (PER TOOTH)... $30.00 D5650 ADD TOOTH TO EXISTING PARTIAL DENTURE... $45.00 D5660 ADD CLASP TO EXISTING PARTIAL DENTURE... $65.00 D5730 RELINE COMPLETE UPPER (CHAIRSIDE)... $75.00 D5731 RELINE COMPLETE LOWER (CHAIRSIDE)... $75.00 D5740 RELINE UPPER PARTIAL (CHAIRSIDE)... $75.00 D5741 RELINE LOWER PARTIAL (CHAIRSIDE)... $75.00 D5810 TEMPORARY COMPLETE UPPER DENTURE... $ D5811 TEMPORARY COMPLETE LOWER DENTURE... $ D5820 TEMPORARY PARTIAL - STAY PLATE UPPER... $ D5821 TEMPORARY PARTIAL - STAY PLATE LOWER... $180.00
7 Schedule of Programs Fees (Continued) PROSTHODONTICS FIXED BRIDGES D6241 PONTIC-PORCELAIN FUSED TO BASE METAL... $ D6751 CROWN-PORCELAIN FUSED TO BASE METAL... $ D6791 CROWN-FULL CAST FUSED TO BASE METAL... $ D6930 RECEMENT BRIDGE... $20.00 D6940 STRESS BREAKER... $90.00 D6950 PRECISION ATTACHMENT (EACH)... $ A specific prosthodontic treatment may present unusual circumstances requiring an additional cost. If precious metal (gold) is desired, the cost will be additional to the crown cost. Please consult the affiliated dentist as to the total cost prior to treatment. ORAL SURGERY D7110 SINGLE TOOTH EXTRACTION... $36.00 D7120 EACH ADDITIONAL TOOTH... $34.00 D7130 ROOT REMOVAL EXPOSED ROOTS... $48.00 D7210 SURGICAL EXTRACTION-ERUPTED... $68.00 D7220 REMOVAL OF IMPACTED TOOTH - SOFT TISSUE... $78.00 D7230 REMOVAL OF IMPACTED TOOTH - PARTIALLY BONY... $ D7240 REMOVAL OF IMPACTED TOOTH- COMPLETELY BONY... $ D7241 REMOVAL OF IMPACTED TOOTH- COMPLETELY BONY, WITH UNUSUSAL SURGICAL COMPLICATIONS... $ D7250 ROOT RECOVERY... $72.00 D7280 SURGICAL EXPOSURE PER TOOTH... $66.00 D7310 ALVEOLOPLASTY (PER QUADRANT WITH EXTRACTIONS)... $78.00 D7320 ALVEOLOPLASTY (PER QUADRANT WITHOUT EXTRACTIONS)... $84.00 D7960 FRENECTOMY... $99.00 A specific oral surgery procedure may present unusual circumstances requiring an additional cost. Please consult the affiliated dentist as to the total procedure cost prior to ORTHODONTICS (QCD GENERAL DENTIST ONLY) D8999 DIAGNOSTIC WORK UP RADIOGRAPHS, MODEL, RECORDS... $ D8080 CHILD (QCD GENERAL DENTIST) CLASS I OR II FOR 24 MONTH TREATMENT... $2, D8090 ADULT (QCD GENERAL DENTIST) CLASS I OR II FOR 24 MONTH TREATMENT... $2, D8680 ORTHODONTIC RETENTION... $ A special orthodontic treatment may present unusual circumstances requiring an additional cost. During the orthodontic consultation appointment, the affiliated dentist will explain all needed procedures, length of treatment, required fees and payment schedule. D9999 FAILED APPOINTMENT GENERAL SERVICES (WITHOUT 24 HOURS NOTICE)... $30.00 D9999 PALLATIVE (EMERGENCY) TREATMENT OF DENTAL PAIN-MINOR PROCEDURES... $20.00 D9999 OFFICE VISIT-AFTER HOURS... $45.00 IMPORTANT NOTICE THE QCD OF AMERICA DENTAL BENEFIT PROGRAM DOES NO CONSTITUTE DENTAL INSURANCE AND IS NOT A HEALTH MAINTENANCE ORGANIZATION CONTRACT. QCD OF AMERICA DOES NOT REIMBURSE THE AFFILIATED DENTIST OR IMDEMNIFY THE MEMBER FOR THE COST OF DENTAL SERVICES RECEIVED BY THE MEMBER. SPECIALTY CARE SERVICES All scheduled charges listed are for services rendered by a QCD OF AMERICA affiliated general dentist. All treatments provided by a QCD OF AMERICA affiliated specialty dentist (advanced degree) in Endodontics, Periodontics, Prosthodontics, Oral Surgery, Pediatric Dentistry or Orthodontics (Board Certified or Board Eligible only) will be charged at a 20% discount from the affiliated specialty dentist s usual and customary fee for the treatment. OTHER PROCEDURES AND PAYMENT FOR SERVICES Any procedure not listed on the QCD OF AMERICA Schedule of Dental Program Fees is available at the dentist s usual and customary fee less a 20% discount this includes all lab fees. All fees included in the Schedule of Dental Fees are for payment at the time of service. The member may negotiate payment terms with the affiliated dentist, however, an ASEPSIS FEE An asepsis fee of $8.00 per patient appointment is charged by all affiliated dentists to insure proper infection control for all QCD OF AMERICA members. QCD OF AMERICA - EXCLUSIONS AND LIMITATIONS 1) THE FOLLOWING EXCLUSIONS AND LIMITATIONS APPLY: A) SERVICES COVERED UNDER WORKMEN S COMPENSATION OR EMPLOYER S LIABILITY LAWS; B) COST OF ANY DENTAL CARE COVERED BY ANY MEDICAL INSURANCE; C) SERVICES WHICH, IN THE OPIONION OF THE ATTENDING DENTIST, ARE NOT NECESSARY FOR THE PATIENT S DENTAL HEALTH OR CANNOT BE PERFORMED BECAUSE OF THE GENERAL HEALTH OF THE PATIENT; D) GENERAL ANESTHESIA, I.V. SEDATION, HOSPITALIZAITON, AND HOSPITAL OR MEDICAL CHARGES OF ANY TYPE. 2) QCD OF AMERICA MEMBER FEES APPLY TO SERVICES RENDERED BY AFFILIATED DENTAL OFFICES AND ARE SUBJECT TO CHANGE IN THE FUTURE. 3) QCD OF AMERICA MEMBER FEES DO NOT APPLY TO WORK IN PROGRESS OR IF THE PATIENT S MEMBERSHIP IS NO LONGER VALID. 4) QCD OF AMERICA ASSUMES NO RESPONSIBILITY OR LIABILITY FOR SERVICES RENDERED BY AFFILIATED DENTISTS. 5) ANY QCD OF AMERICA MEMBER ACCEPTED FOR ORTHODONTIC TREATMENT MUST REMAIN A MEMBER OF THE PLAN FOR THE COMPLETE DURATION OF THE TREATMENT OR RISK ADDITIONAL CHARGES BY THE AFFILAITED DENTIST. 6) ANY PROCEDURE MAY PRESENT UNUSUAL CIRCUMSTANCES REQUIRING AN ADDITIONAL COST. PLEASE CONSULT THE AFFILIATED DENTIST AS TO THE TOTAL TREATMENT COST PRIOR TO ANY SERVICE BEING RENDERED.



8 Davis Vision is pleased to provide you with a no-cost, traditional vision Discount Program that provides significant discounts on eye exams, lenses, frames and additional eyewear options. For more details, see the Accessing Provider Information section on the reverse side. The Discount Program entitles you to the following discounts off usual and customary fees: Comprehensive Eye Exam Complete Eye Examination 15% Discount off Usual & Customary Contact Lens Examination 15% Discount off Usual & Customary Frame/ 1 Patient Price Average Discount Priced up to $70 Retail $40 40% Priced over $70 Retail $40 plus 10% off the amount over $70 28% Spectacle Lenses (Uncoated Plastic) Single $35 30% Bifocal $55 27% Trifocal $65 28% Lenticular $110 31% Lens Options (Add to Lens Prices Above)/ 2 Standard Progressive $75 50% Premium Progressive $125 35%-60% Glass Lenses $18 40% Polycarbonate Lenses $30 50% Blended Invisible Bifocals $20 60% Intermediate Vision Lenses $30 80% Scratch Resistant Coating $20 33%-66% Standard Anti-Reflective Coating $45 20% Ultraviolet Coating $15 25% Solid Tint $10 30% Gradient Tint $12 20% Photochromic Lenses $35 20%-45% Plastic Photosensitive Lenses $65 35%-55% High Index Lenses $55 40% Polarized Lenses $75 20% Contact Lenses (in lieu of eyeglasses) Conventional 20% off Provider s Usual & Customary 20% Disposable/Planned Replacement 10% off Provider s Usual & Customary 10% Value-Added Features Lens 1-2-3! Membership Free Membership Up to 50% Laser Vision Correction Discount Up to 25% off Provider s U & C /3 Up to 25% 16
9 Clear Vision Discount Program Highlights Vision Plan: Clear Vision Discount Plan Control Code: 2959 Co-payment: N/A, discount plan is 100% member paid at the time of service Eye Examination Members will receive a 15% discount on their comprehensive eye examination including dilation (when professionally indicated). Eyewear (Frames and Spectacle Lenses or Contact Lenses) Members will be entitled to substantial and verifiable savings on all of their eyewear needs. Discounts are uniform nationally and represent pricing well below Average Retail Prices. These discounts are based on published industry standard costs, not markdowns from artificially inflated prices. Significant Savings Client surveys indicate that programs providing discounts off retail prices of eyeglasses are subject to abuse due to the high associated markups of over 300% throughout the optical industry. Consequently, these programs do not result in a true value-add for the beneficiary. The proposed fixed-fee discounted pricing schedule provides both verifiable savings and benefit uniformity for all members from coast to coast. Additional Value-Added Features The Clear Vision Discount Program also offers significant discounts on replacement contact lenses and laser vision correction at no additional cost. Lens 123 is a mail order program that allows you to enjoy the guaranteed lowest prices on replacement contact lenses save up to 60% off retail prices. Members can conveniently call LENS123 with a current prescription for this value-added service. The Lens 123 contact lens replacement program is endorsed by the industry s major manufacturers. Davis Vision s Laser Vision Correction program provides substantial discounts on laser vision correction procedures. Members are entitled to savings of up to 25% off usual and customary fees or a 5% discount off a center s advertised special through a network of preeminent physicians affiliated with Eye Centers of Excellence. (Some centers provide a flat fee equating to these discount levels.) See below for information on finding a participating laser vision provider near you. Accessing a Provider Contact a Davis Vision representative at or simply log on to choose Find a Provider and use your control code 2959 Customer Service -To speak with a customer service representative, call Davis Vision Customer Service at Enter Client Control Number 2959 when prompted. At the main menu, press 0. Our representatives are available to assist you from 8 a.m. to 11 p.m. ET Monday through Friday, 9 a.m. to 4 p.m. ET Saturday and 12 p.m. to 4 p.m. ET Sunday. 17


10 Up to 80% on generic medications Up to 20% on name brand prescriptions Up to 80% on your PET'S medications too! Unlike many other programs and discounts,qcd Wellness This is NOT an insurance program or membership club Your FREE discount drug card simply entitles you to a discount off the purchase price of prescription drugs

11 Dental Referral Form
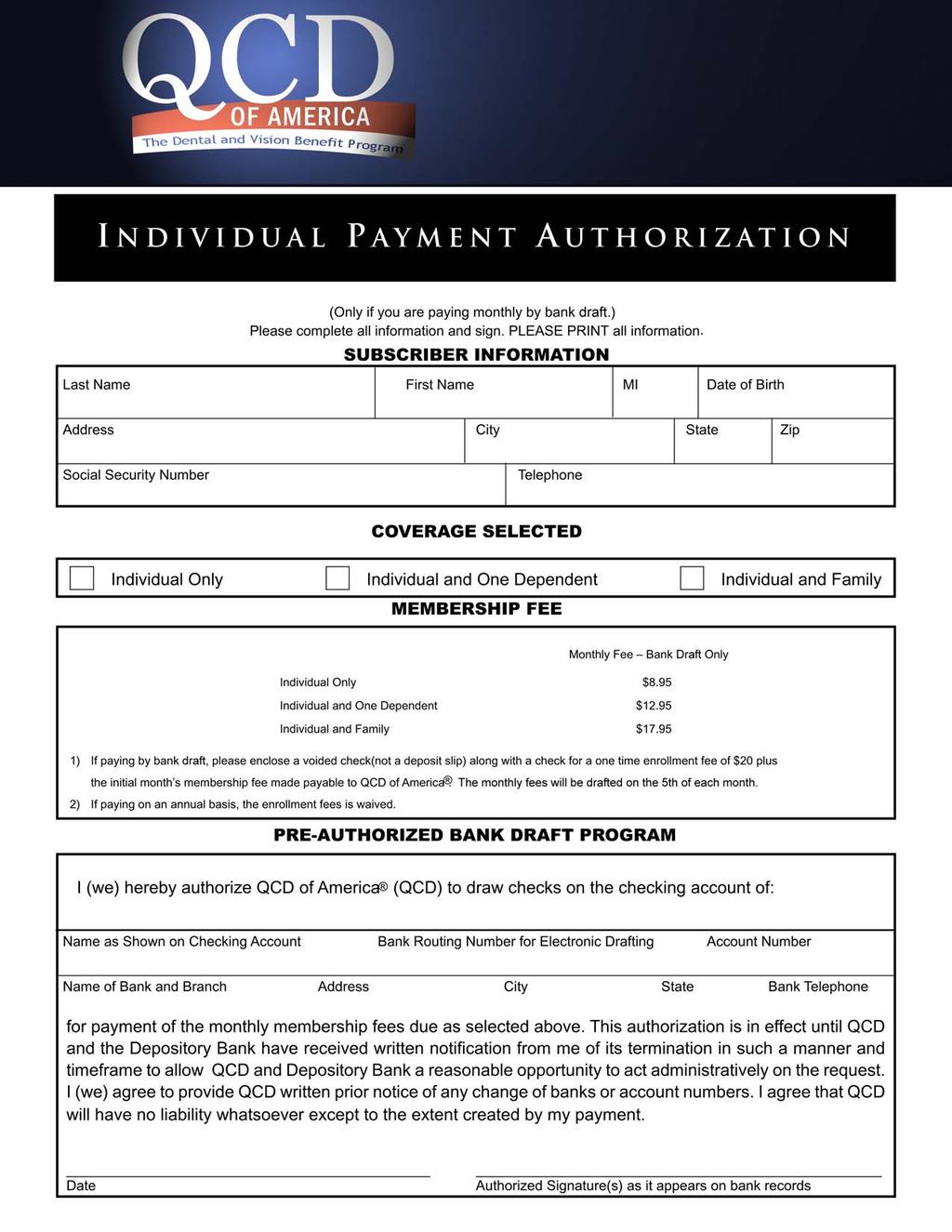
12 The Red Program Please fill out all information and sign at the bottom Last Name First Name MI Date of Birth Address City State Zip Social Security Number Telephone COVERAGE SELECTED Single Member Single Member and One Dependent Single Member and Family $8.95 / Month $12.95 / Month $17.95 / Month DEPENDENT INFORMATION Social Security Number Last Name First Name MI Date of Birth Gender Relationship I hereby make application for membership in QCD of America (QCD). I agree to hold QCD harmless from any liability for negligence on the part of the Affiliated Dentist. I further release QCD from and waive any claims for negligent referral, negligent certification or similar claim. I hereby authorize my employer to make payroll deductions, if required, for the coverage selected. The QCD of America Dental and Vision Benefit Program is not an insurance plan and does not constitute insurance coverage. Date Applicant Signature
13
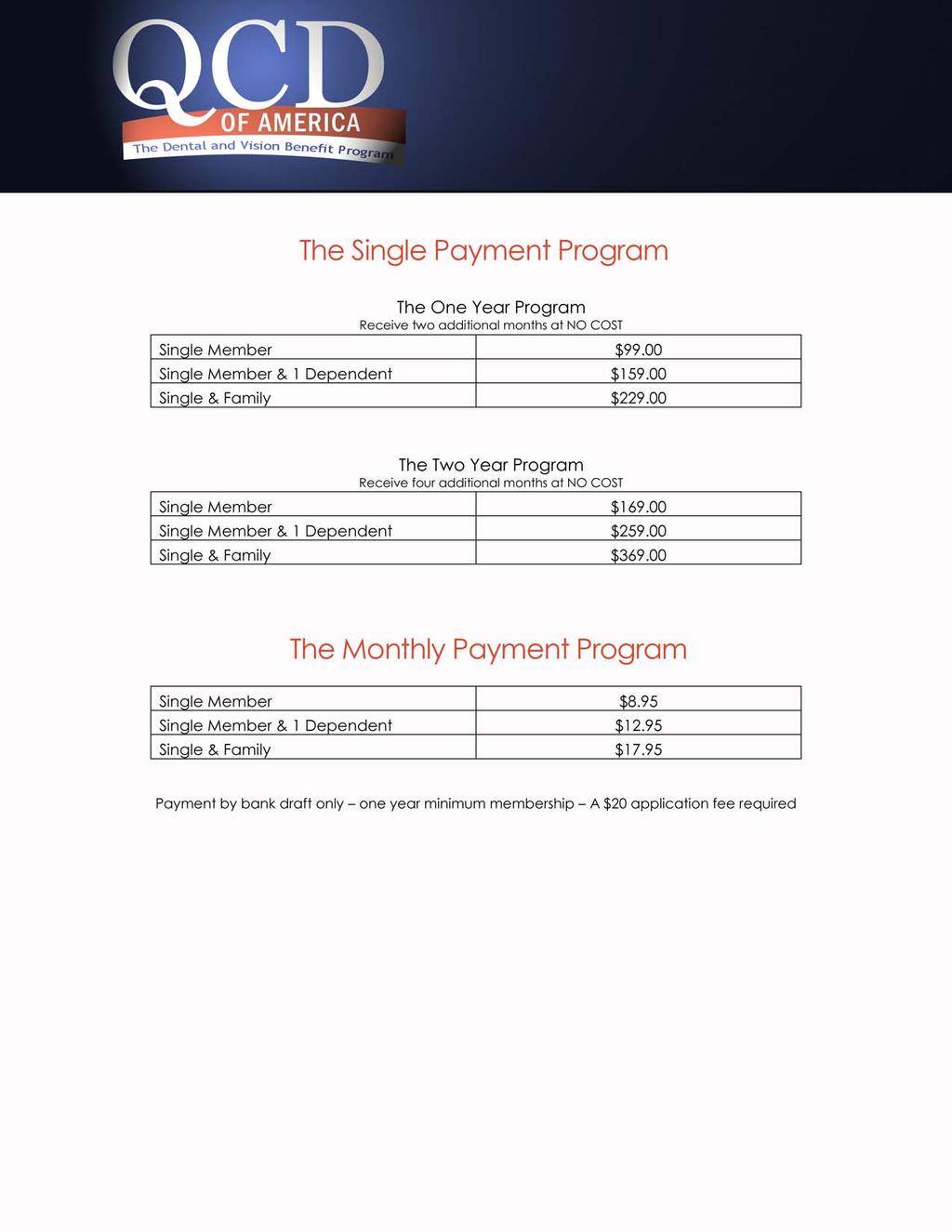
Do not pay high premiums for dental benefits pay for your services when and if used. It just makes good financial sense!
 Houston ISD The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy
Houston ISD The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy
Blackwater Communications Inc.
 Blackwater Communications Inc. Consumer Driven Choices Monthly Employee Rates Employee Only Employee + One Employee + Family RED PLUS Employer Paid $10.00 $20.00 A Limited Reimbursement Program Calendar
Blackwater Communications Inc. Consumer Driven Choices Monthly Employee Rates Employee Only Employee + One Employee + Family RED PLUS Employer Paid $10.00 $20.00 A Limited Reimbursement Program Calendar
Do Not Pay High Premiums for Dental Benefits Pay for Your Services When and If Used. It Just Makes Good Financial Sense!
 The QCD of America Dental & Vision Benefit Program (QCD) is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy QCD
The QCD of America Dental & Vision Benefit Program (QCD) is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy QCD
Aldine ISD. Do not pay high premiums for dental benefits pay for your services when and if used. It just makes good financial sense!
 Aldine ISD The QCD of America Dental & Vision Benefit Program (QCD) is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy
Aldine ISD The QCD of America Dental & Vision Benefit Program (QCD) is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy
Welcome to the Future of Dental & Vision Benefits Today!
 The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy QCD believes
The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The QCD Philosophy QCD believes
Cypress-Fairbanks ISD
 Cypress-Fairbanks ISD The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The
Cypress-Fairbanks ISD The QCD of America Dental & Vision Benefit Program is a managed cost program offering a large selection of highly qualified private practice dental and optical professionals. The
The Individual Dental & Vision Benefit Program
 The Individual Dental & Vision Benefit Program Please complete the enrollment form(s) and return to: 1664 KELLER PKWY. SUITE 101 KELLER, TX 76248 1664 KELLER PKWY. SUITE 101 KELLER, TX 76248 800.229.0304
The Individual Dental & Vision Benefit Program Please complete the enrollment form(s) and return to: 1664 KELLER PKWY. SUITE 101 KELLER, TX 76248 1664 KELLER PKWY. SUITE 101 KELLER, TX 76248 800.229.0304
Anthem Blue Dental PPO Voluntary Option 2V Summary of Benefits
 Anthem Blue Dental PPO Voluntary Option 2V Summary of Benefits Annual Benefit Limit: $1500 Annual Member Deductible: $50 PPO Dentist $50 Non-PPO Dentist Family Coverage Deductible Limit 3 times Annual
Anthem Blue Dental PPO Voluntary Option 2V Summary of Benefits Annual Benefit Limit: $1500 Annual Member Deductible: $50 PPO Dentist $50 Non-PPO Dentist Family Coverage Deductible Limit 3 times Annual
ADA CODE PROCEDURE PATIENT PAYS ADA CODE PROCEDURE PATIENT PAYS APPOINTMENTS
 PRESTIGE 25 Schedule of Benefits and Subscriber Copayments ADA CODE PROCEDURE PATIENT PAYS ADA CODE PROCEDURE PATIENT PAYS APPOINTMENTS 5130 Immediate maxillary (upper)...$300.00 9430 Office visit (normal
PRESTIGE 25 Schedule of Benefits and Subscriber Copayments ADA CODE PROCEDURE PATIENT PAYS ADA CODE PROCEDURE PATIENT PAYS APPOINTMENTS 5130 Immediate maxillary (upper)...$300.00 9430 Office visit (normal
SECURE CHOICE INDIVIDUAL COPAYMENT SCHEDULE
 DentiCare of Alabama, Inc. 3595 Grandview Parkway, Suite 650 Birmingham, AL 35243 SECURE CHOICE INDIVIDUAL COPAYMENT SCHEDULE SECTION I: PLAN DENTIST SERVICES (Subject to Exclusions and Limitations Listed
DentiCare of Alabama, Inc. 3595 Grandview Parkway, Suite 650 Birmingham, AL 35243 SECURE CHOICE INDIVIDUAL COPAYMENT SCHEDULE SECTION I: PLAN DENTIST SERVICES (Subject to Exclusions and Limitations Listed
State of Tennessee. Prepaid Plan. Dental Benefit Option. Sponsored by the. State of Tennessee
 State of Tennessee Prepaid Plan Dental Benefit Option Sponsored by the State of Tennessee 2011 Products and services marketed by Assurant Employee Benefits are underwritten and/or provided by Union Security
State of Tennessee Prepaid Plan Dental Benefit Option Sponsored by the State of Tennessee 2011 Products and services marketed by Assurant Employee Benefits are underwritten and/or provided by Union Security
23XX2293 R3/08 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity Company
 www.bcbsla.com 23XX2293 R3/08 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity Company 1 Blue Cross and Blue Shield of Louisiana and HMO Louisiana, Inc. are
www.bcbsla.com 23XX2293 R3/08 Blue Cross and Blue Shield of Louisiana incorporated as Louisiana Health Service & Indemnity Company 1 Blue Cross and Blue Shield of Louisiana and HMO Louisiana, Inc. are
Schedule of Benefits (GR-9N S )
") Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: BNSF Railway Company GP-727796 Issue Date: January 1, 2016 Effective Date: January 1, 2016 Schedule: 1A Cert Base: 1 For: DMO - All
Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: BNSF Railway Company GP-727796 Issue Date: January 1, 2016 Effective Date: January 1, 2016 Schedule: 1A Cert Base: 1 For: DMO - All
Schedule of Benefits (GR-9N S )
") Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: Roman Catholic Diocese Of Dallas GP-870560-WI Issue Date: February 9, 2015 Effective Date: January 1, 2015 Schedule: 7A Cert Base:
Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: Roman Catholic Diocese Of Dallas GP-870560-WI Issue Date: February 9, 2015 Effective Date: January 1, 2015 Schedule: 7A Cert Base:
Schedule of Benefits (GR-9N S )
") Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: BNSF Railway Company GP-727796 Issue Date: January 1, 2014 Effective Date: January 1, 2014 Schedule: 1A Cert Base: 1 For: DMO - All
Schedule of Benefits (GR-9N S-01-001-01) Employer: Group Policy Number: BNSF Railway Company GP-727796 Issue Date: January 1, 2014 Effective Date: January 1, 2014 Schedule: 1A Cert Base: 1 For: DMO - All
Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #
 a feature of the Delta Dental PPO Denver Public Schools- Group #") Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #6694 7.2011 MAXIMUM BENEFIT Calendar Year Orthodontic Lifetime CALENDAR YEAR DEDUCTIBLE WHO CAN BE COVERED
Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #6694 7.2011 MAXIMUM BENEFIT Calendar Year Orthodontic Lifetime CALENDAR YEAR DEDUCTIBLE WHO CAN BE COVERED
FEE SCHEDULE. Complete Dental Plan is a discount plan offered and administered by our organization at:
 FEE SCHEDULE Complete Dental Plan is a discount plan offered and administered by our organization at: 7801 CORAL WAY SUITE # 106, MIAMI, FL 33144 (786) 326-6873 F (305) 6979785 COMPLETE DENTAL PLAN HIGHLIGHTS
FEE SCHEDULE Complete Dental Plan is a discount plan offered and administered by our organization at: 7801 CORAL WAY SUITE # 106, MIAMI, FL 33144 (786) 326-6873 F (305) 6979785 COMPLETE DENTAL PLAN HIGHLIGHTS
Aetna Dental Inc. One Prudential Circle Sugar Land, TX SUMMARY OF COVERAGE
 Aetna Dental Inc. One Prudential Circle Sugar Land, TX 77478 1-877-238-6200 SUMMARY OF COVERAGE CONTRACT HOLDER: Clear Creek ISD GROUP AGREEMENT: 620318 PLAN EFFECTIVE: September 1, 2014 The benefits shown
Aetna Dental Inc. One Prudential Circle Sugar Land, TX 77478 1-877-238-6200 SUMMARY OF COVERAGE CONTRACT HOLDER: Clear Creek ISD GROUP AGREEMENT: 620318 PLAN EFFECTIVE: September 1, 2014 The benefits shown
Aetna Dental Inc. One Prudential Circle Sugar Land, TX SUMMARY OF COVERAGE
 Aetna Dental Inc. One Prudential Circle Sugar Land, TX 77478 1-877-238-6200 SUMMARY OF COVERAGE CONTRACT HOLDER: BNSF Railway Company GROUP AGREEMENT: 727796 PLAN EFFECTIVE: January 1, 2016 The benefits
Aetna Dental Inc. One Prudential Circle Sugar Land, TX 77478 1-877-238-6200 SUMMARY OF COVERAGE CONTRACT HOLDER: BNSF Railway Company GROUP AGREEMENT: 727796 PLAN EFFECTIVE: January 1, 2016 The benefits
Managed DentalGuard Texas
 Page 1 of 5 0120 0120 0140 0140 0150 0150 0460 0470 0999 9310 9310 9430 9440 0210 0220 0230 0240 0270 0272 0274 0330 1110 1120 1999 1201 1203 1204 1310 1330 1351 9999 1510 1515 1550 2110 2120 2130 2131
Page 1 of 5 0120 0120 0140 0140 0150 0150 0460 0470 0999 9310 9310 9430 9440 0210 0220 0230 0240 0270 0272 0274 0330 1110 1120 1999 1201 1203 1204 1310 1330 1351 9999 1510 1515 1550 2110 2120 2130 2131
GUARANTY ASSURANCE COMPANY - DINA Dental Plan SCHEDULED BENEFITS RIDER
 OSHA Charge for disposables for patients protection, per person, per visit* $5.00 120 Periodic oral exam $5.00 140 Limited oral exam $30.00 150 Comprehensive oral evaluation $20.00 180 Comprehensive Perio
OSHA Charge for disposables for patients protection, per person, per visit* $5.00 120 Periodic oral exam $5.00 140 Limited oral exam $30.00 150 Comprehensive oral evaluation $20.00 180 Comprehensive Perio
COVERED SERVICES DIAGNOSTIC AND PREVENTATIVE SERVICES: CO-PAY
 PLAN DENTAL 1-2 TIJUANA AV PASEO TIJUANA #406 THIRD FLOOR SIMNSA BUILDING TIJUANA B.C. Tel: (664) 231-4739 Monday Friday: 8 A.M. 8 P.M. Saturday: 8 A.M. 4 P.M. Sunday: 10 A.M. 2 P.M. MEXICALI CALLE E #123
PLAN DENTAL 1-2 TIJUANA AV PASEO TIJUANA #406 THIRD FLOOR SIMNSA BUILDING TIJUANA B.C. Tel: (664) 231-4739 Monday Friday: 8 A.M. 8 P.M. Saturday: 8 A.M. 4 P.M. Sunday: 10 A.M. 2 P.M. MEXICALI CALLE E #123
General Dentist Fee Schedule
 General Dentist Fee Schedule ADA Diagnostic D0120 Periodic oral evaluation $0 $72 $72 D0140 Limited oral evaluation problem focused $77 $107 $30 D0150 Comprehensive oral evaluation new or established patient
General Dentist Fee Schedule ADA Diagnostic D0120 Periodic oral evaluation $0 $72 $72 D0140 Limited oral evaluation problem focused $77 $107 $30 D0150 Comprehensive oral evaluation new or established patient
General Dentist Fee Schedule
 General Dentist Fee Schedule Diagnostic D0120 Periodic oral evaluation $0 $59 $59 D0140 Limited oral evaluation problem focused $71 $88 $17 D0150 Comprehensive oral evaluation new or established patient
General Dentist Fee Schedule Diagnostic D0120 Periodic oral evaluation $0 $59 $59 D0140 Limited oral evaluation problem focused $71 $88 $17 D0150 Comprehensive oral evaluation new or established patient
State of Tennessee Prepaid Plan
 State of Tennessee Prepaid Plan Dental Benefit Option Sponsored by the State of Tennessee 2009 Products and services marketed by Assurant Employee Benefits are underwritten and/or provided by Union Security
State of Tennessee Prepaid Plan Dental Benefit Option Sponsored by the State of Tennessee 2009 Products and services marketed by Assurant Employee Benefits are underwritten and/or provided by Union Security
The. Dental Plan. Underwritten by: DENTA-CHEK of Maryland, Inc. A Not-for-Profit Corporation
 The Dental Plan Underwritten by: DENTA-CHEK of Maryland, Inc. A Not-for-Profit Corporation Now you can have comprehensive DENTAL coverage at a cost you can afford! Since 1981, Denta-Chek has been providing
The Dental Plan Underwritten by: DENTA-CHEK of Maryland, Inc. A Not-for-Profit Corporation Now you can have comprehensive DENTAL coverage at a cost you can afford! Since 1981, Denta-Chek has been providing
Delta Dental EPO City & County of Denver Group #6791 EPO
 MAXIMUM BENEFIT - Calendar Year Maximum Delta Dental EPO City & County of Denver Group #6791 EPO Unlimited See copayment schedule for additional details. Orthodontic Lifetime Unlimited See copayment schedule
MAXIMUM BENEFIT - Calendar Year Maximum Delta Dental EPO City & County of Denver Group #6791 EPO Unlimited See copayment schedule for additional details. Orthodontic Lifetime Unlimited See copayment schedule
Delta Dental of Colorado EXCLUSIVE PANEL OPTION (EPO) Schedule EPO 1B List of Patient Co-Payments. * See Special Provisions on Last Page
 Schedule EPO 1B List of Patient Co-Payments. * See Special Provisions on Last Page") List of Co-Payments Code edure Code Definition Co-Pay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
List of Co-Payments Code edure Code Definition Co-Pay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
Fee $20 $30 $60 $35 $65 $55 $45 $15 $30. Fee $55 $75 $85 $105 $60 $80 $115 $80 $105 $140 $170 $875 $135 $155 LENS OPTIONS. Fee $500 $600 $700
 Dental Savings Schedule (General Dentist) *Dentists may add additional lab fees to discounted services with*. DIAGNOSTIC & PREVENTATIVE D0120 Periodic Oral Evaluation D0150 Comprehensive Oral Evaluation
Dental Savings Schedule (General Dentist) *Dentists may add additional lab fees to discounted services with*. DIAGNOSTIC & PREVENTATIVE D0120 Periodic Oral Evaluation D0150 Comprehensive Oral Evaluation
ADA Code Restorative Procedures (Fillings) Member Fee Usual Fee You Save D2951 Pin retention per tooth $ 35.00
 Member Fee Usual Fee You Save D2951 Pin retention per tooth $ 35.00") Northeast General Dentistry Fee Schedule I District of Columbia, Maryland, New Jersey, New York, Pennsylvania, Virginia Please note: This fee schedule applies to procedures performed by a General Dentists
Northeast General Dentistry Fee Schedule I District of Columbia, Maryland, New Jersey, New York, Pennsylvania, Virginia Please note: This fee schedule applies to procedures performed by a General Dentists
Dominion Dental Services
 Dominion Dental Services Plan 603X Presented by Professional Benefit Administrators 1 (800) 578-2082 SUMMARY OF BENEFITS AND COPAYMENTS Enrollee pays DIAGNOSTIC Office Visit/Infectious Disease Control.....$
Dominion Dental Services Plan 603X Presented by Professional Benefit Administrators 1 (800) 578-2082 SUMMARY OF BENEFITS AND COPAYMENTS Enrollee pays DIAGNOSTIC Office Visit/Infectious Disease Control.....$
Newport News Public Schools Summary Schedule of Services Delta Dental PPO EPO Plan
 Newport News Public Schools Summary of Services Delta Dental PPO EPO Plan Services In-Network Out-of-Network PPO Premier All Other Diagnostic & Preventive Oral Exams & Teeth Cleanings Fluoride Applications
Newport News Public Schools Summary of Services Delta Dental PPO EPO Plan Services In-Network Out-of-Network PPO Premier All Other Diagnostic & Preventive Oral Exams & Teeth Cleanings Fluoride Applications
Delta Dental of Colorado DENVER HEALTH AND HOSPITAL AUTHORITY GROUP #587. EXCLUSIVE PANEL OPTION (EPO) List of Patient Copayments
 List of Patient Copayments") List of Copayments Code edure Code Definition Copay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
List of Copayments Code edure Code Definition Copay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
DIAGNOSTIC/PREVENTIVE SERVICES
 DIAGNOSTIC/PREVENTIVE SERVICES Diagnostic Services D0120 Periodic oral evaluation 100% 100% D0140 Limited oral evaluation problem focused 100% 100% D0150 Comprehensive oral evaluation 100% 100% D0160 Detailed
DIAGNOSTIC/PREVENTIVE SERVICES Diagnostic Services D0120 Periodic oral evaluation 100% 100% D0140 Limited oral evaluation problem focused 100% 100% D0150 Comprehensive oral evaluation 100% 100% D0160 Detailed
Delta Dental EPO City & County of Denver Group #6791 EPO
 MAXIMUM BENEFIT - Calendar Year Maximum Delta Dental EPO City & County of Denver Group #6791 EPO Unlimited See copayment schedule for additional details. Orthodontic Lifetime Unlimited See copayment schedule
MAXIMUM BENEFIT - Calendar Year Maximum Delta Dental EPO City & County of Denver Group #6791 EPO Unlimited See copayment schedule for additional details. Orthodontic Lifetime Unlimited See copayment schedule
GUARANTY ASSURANCE COMPANY Dina Dental of Louisiana Pre-Paid Group & Individual
 Effective: January 1, 2016 Eligibility: (866) 436-3093 GUARANTY ASSURANCE COMPANY Dina Dental of Louisiana Pre-Paid Group & Individual Diagnostic D0999 Office Visit Copay - Per Person, Per Visit $9.00
Effective: January 1, 2016 Eligibility: (866) 436-3093 GUARANTY ASSURANCE COMPANY Dina Dental of Louisiana Pre-Paid Group & Individual Diagnostic D0999 Office Visit Copay - Per Person, Per Visit $9.00
HumanaDental PPO 09 (High Option)
") HumanaDental PPO 09 (High Option) FLORIDA ICUBA If you use IN-NETWORK provider If you use OUT-OF-NETWORK provider Plan-year deductible Annual maximum Preventive services Oral examinations X-rays Cleanings
HumanaDental PPO 09 (High Option) FLORIDA ICUBA If you use IN-NETWORK provider If you use OUT-OF-NETWORK provider Plan-year deductible Annual maximum Preventive services Oral examinations X-rays Cleanings
DINA Dental. Prepaid Plan Highlights. Prepaid Plan Bi-weekly Premiums $ 7.00 $10.76 $ Employee Only Employee + One Employee + Family
 DINA Dental Prepaid Plan Highlights NO Claim Forms NO Maximums NO Deductibles NO Waiting Period - Some Preventive and Diagnostic Services Provided at NO CHARGE - Over 180 procedures covered by co-payments
DINA Dental Prepaid Plan Highlights NO Claim Forms NO Maximums NO Deductibles NO Waiting Period - Some Preventive and Diagnostic Services Provided at NO CHARGE - Over 180 procedures covered by co-payments
2018 Presbyterian Health Plan Federal Employee Dental & Vision Options
 2018 Presbyterian Health Plan Federal Employee Dental & Vision Options For more information: 1804 Juan Tabo NE, Suite A, Albuquerque, NM 87112 888 862 8659 505 237 1501 benefitsource.org These benefits
2018 Presbyterian Health Plan Federal Employee Dental & Vision Options For more information: 1804 Juan Tabo NE, Suite A, Albuquerque, NM 87112 888 862 8659 505 237 1501 benefitsource.org These benefits
Adult Dental and Vision Coverage
 Adult Dental and Vision Coverage HMO and HSP Off-Marketplace Health Plans Karen Boyd We are your Health Net. TM Optional Adult Dental and Vision coverage (ages 19 and older) with a Health Net HMO or HSP
Adult Dental and Vision Coverage HMO and HSP Off-Marketplace Health Plans Karen Boyd We are your Health Net. TM Optional Adult Dental and Vision coverage (ages 19 and older) with a Health Net HMO or HSP
Scheduled Dental Benefit Plan Schedule of Dental Allowances
 Diagnostic Scheduled Dental Benefit Plan Schedule of Dental Allowances 0120 Periodic Oral Evaluation (once in 5 months after comprehensive) 20.00 0140 Limited Oral Evaluation 20.00 0150 Comprehensive Oral
Diagnostic Scheduled Dental Benefit Plan Schedule of Dental Allowances 0120 Periodic Oral Evaluation (once in 5 months after comprehensive) 20.00 0140 Limited Oral Evaluation 20.00 0150 Comprehensive Oral
WASHINGTON STATE COUNCIL OF COUNTY AND CITY EMPLOYEES AFSCME AFL-CIO DENTAL PLAN VIII
 WASHINGTON STATE COUNCIL OF COUNTY AND CITY EMPLOYEES AFSCME AFL-CIO DENTAL PLAN VIII HOW TO OBTAIN PLAN BENEFITS To obtain benefits see the Payment of Claims provision. Forward Your completed claim form
WASHINGTON STATE COUNCIL OF COUNTY AND CITY EMPLOYEES AFSCME AFL-CIO DENTAL PLAN VIII HOW TO OBTAIN PLAN BENEFITS To obtain benefits see the Payment of Claims provision. Forward Your completed claim form
ADA Code Cosmetic Procedures Member Fee Usual Fee You Save Bonding (per tooth): D2960 Full face buildup chairside $
: D2960 Full face buildup chairside $") New England General Dentistry Fee Schedule Connecticut, Massachusetts, New Hampshire & Rhode Island Please note: This fee schedule applies to procedures performed by a General Dentists only. Rates are
New England General Dentistry Fee Schedule Connecticut, Massachusetts, New Hampshire & Rhode Island Please note: This fee schedule applies to procedures performed by a General Dentists only. Rates are
LIST OF COVERED DENTAL SERVICES
 LIST OF COVERED DENTAL SERVICES The following is a complete list of those dental Services which will be considered for payment by Constitution Life Insurance Company after the expiration of any applicable
LIST OF COVERED DENTAL SERVICES The following is a complete list of those dental Services which will be considered for payment by Constitution Life Insurance Company after the expiration of any applicable
Kaiser Permanente and Delta Dental
 Kaiser Permanente and Delta Dental Dental Program for Kaiser Permanente FEHBP Enrollees You must be a Kaiser Permanente FEHBP enrollee to participate in the dental plan. Kaiser Permanente and Delta Dental
Kaiser Permanente and Delta Dental Dental Program for Kaiser Permanente FEHBP Enrollees You must be a Kaiser Permanente FEHBP enrollee to participate in the dental plan. Kaiser Permanente and Delta Dental
For a Correction Captains Association Dental Claim Form please follow this link CCA Dental Claim form.pdf
 Correction Captains Association Retiree Security Benefit Fund Group #132 Summary of Benefit for Retired members: Annual maximum $3,500.00 individual Individual Ortho Lifetime max $3,500 Appliance $600,
Correction Captains Association Retiree Security Benefit Fund Group #132 Summary of Benefit for Retired members: Annual maximum $3,500.00 individual Individual Ortho Lifetime max $3,500 Appliance $600,
02130 Cavities involving three surfaces 10.00
 ( ) 02130 Cavities involving three surfaces 10.00 AMALGAM RESTORATIONS, PERMANENT TEETH: 02140 Cavities involving one tooth surface $ 5.00 02150 Cavities involving two tooth surfaces 8.00 02160 Cavities
( ) 02130 Cavities involving three surfaces 10.00 AMALGAM RESTORATIONS, PERMANENT TEETH: 02140 Cavities involving one tooth surface $ 5.00 02150 Cavities involving two tooth surfaces 8.00 02160 Cavities
ASSISTANT SECRETARY PRESIDENT
 Charge Code TYPE I* Benefit Co-Insurance $21.00 0120* Periodic oral exam $21.00 Balance Billing $30.00 0140* Limited oral exam $30.00 Balance Billing $35.00 0150* Comprehensive oral evaluation $35.00 Balance
Charge Code TYPE I* Benefit Co-Insurance $21.00 0120* Periodic oral exam $21.00 Balance Billing $30.00 0140* Limited oral exam $30.00 Balance Billing $35.00 0150* Comprehensive oral evaluation $35.00 Balance
Smile for Health Value Plans
 Smile for Health Value Plans Affordable dental plan solutions ERC-0150-0516 Smile for Health Value Plans Improved PPO plans Whether you need dental and vision benefits to complete your health care package
Smile for Health Value Plans Affordable dental plan solutions ERC-0150-0516 Smile for Health Value Plans Improved PPO plans Whether you need dental and vision benefits to complete your health care package
RETIREE DENTAL PLAN. RETIREE DENTAL PLAN FEE SCHEDULE Page 1 of 8
 D0120 periodic oral evaluation $ 30.50 D0140 limited oral evaluation problem focused $ 30.50 D0150 comprehensive oral evaluation - new or established patient $ 30.50 D0160 detailed and extensive oral evaluation
D0120 periodic oral evaluation $ 30.50 D0140 limited oral evaluation problem focused $ 30.50 D0150 comprehensive oral evaluation - new or established patient $ 30.50 D0160 detailed and extensive oral evaluation
Member Dental Fees Texas
 Dental Discount Plan Member Dental Fees Texas Member s Services Member Pays Member s Services Member Pays Diagnostic and Preventive Dentistry Prosthodontic Dentistry (Dentures)* D0120 Periodic oral evaluation...15
Dental Discount Plan Member Dental Fees Texas Member s Services Member Pays Member s Services Member Pays Diagnostic and Preventive Dentistry Prosthodontic Dentistry (Dentures)* D0120 Periodic oral evaluation...15
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS
 SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental SCHEDULE OF BENEFITS COST-SHARING PEDIATRIC DENTAL CARE ESSENTIAL HEALTH BENEFIT Deductible One (1) Member under age 19 Two (2) or more Members
community Health Plans
 About Us Community Health Plans (CHP) is the fastest growing discounted dental and vision savings program with a national network of participating providers. We are the only free dental and vision savings
About Us Community Health Plans (CHP) is the fastest growing discounted dental and vision savings program with a national network of participating providers. We are the only free dental and vision savings
SHL Dental PPO Plan 29 - SB Adult Only Coverage
 SHL Dental PPO Plan 29 - SB Adult Only Coverage Attachment A Benefit Schedule Please read the definition of Eligible Dental Expenses ( EDE ) and SHL Reimbursement Schedule in the Certificate. When accessing
SHL Dental PPO Plan 29 - SB Adult Only Coverage Attachment A Benefit Schedule Please read the definition of Eligible Dental Expenses ( EDE ) and SHL Reimbursement Schedule in the Certificate. When accessing
Employee Benefit Fund July 2018 ADA Codes and Plan Fees
 CSEA Employee Benefit Fund July 2018 ADA Codes and Plan Fees DIAGNOSTIC D0120 periodic oral examination 40 34 42 45 48 38 30 32 31 D0140 limited oral examination (Does not look at 9110) 40 34 42 45 48
CSEA Employee Benefit Fund July 2018 ADA Codes and Plan Fees DIAGNOSTIC D0120 periodic oral examination 40 34 42 45 48 38 30 32 31 D0140 limited oral examination (Does not look at 9110) 40 34 42 45 48
2018 fee schedule. Georgia. Diagnostic Services (Performed by a General Dentist)
") Diagnostic Services (Performed by a General Dentist) page 1 of 12 IS NOT A REGISTERED INSURANCE PLAN. It is a savings plan offered exclusively by Coast Dental practices to patients who do not have dental
Diagnostic Services (Performed by a General Dentist) page 1 of 12 IS NOT A REGISTERED INSURANCE PLAN. It is a savings plan offered exclusively by Coast Dental practices to patients who do not have dental
SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits
 COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
COST-SHARING SECTION XVI. EssentialSmile Ped 111, ST, INN, Pediatric Dental Schedule of Benefits Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx Member Services:
 This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
 This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
This schedule applies to services provided by a participating General Dentist and is an extensive list of most common procedures. The purpose of this schedule is to establish the maximum fee that a General
ST. CHARLES COMMUNITY SCHOOLS Dental Benefits Plan
 PO Box 610 Southfield, MI 48037 248-901-3705 ST. CHARLES COMMUNITY SCHOOLS Dental Benefits Plan Class 2 - Financial Assistant, Secretaries with Medical The Plan-at-a-Glance PPO Networks: ADN Dental Network,
PO Box 610 Southfield, MI 48037 248-901-3705 ST. CHARLES COMMUNITY SCHOOLS Dental Benefits Plan Class 2 - Financial Assistant, Secretaries with Medical The Plan-at-a-Glance PPO Networks: ADN Dental Network,
STRENGTH. STABILITY. SECURITY.
 GROUP DISCOUNT DENTAL PLAN STRENGTH. STABILITY. SECURITY. Why Purchase a Discount Dental Plan Through the ASCE? With the ASCE Discount Dental Plan, you ll have access to the following benefits: Cost is
GROUP DISCOUNT DENTAL PLAN STRENGTH. STABILITY. SECURITY. Why Purchase a Discount Dental Plan Through the ASCE? With the ASCE Discount Dental Plan, you ll have access to the following benefits: Cost is
Staywell FL Child Medicaid Plan Benefits
 The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
The following is a complete list of dental procedures for which benefits are payable under this Plan. For beneficiaries under age 21, additional coverage may be available with documentation of medical
MDG Dental Plan Comparison
 D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
D0999 Office visit during regular hours, general dentist only Evaluations D0120 Periodic oral examination - established patient D0140 Limited oral evaluation - problem focused D0145 Oral evaluation for
Senior Dental Insurance Scheduled Allowance
 Senior Dental Insurance Scheduled Allowance LIST OF COVERED DENTAL SERVICES The following is a complete list of those dental services which will be considered for payment by The American Progressive Life
Senior Dental Insurance Scheduled Allowance LIST OF COVERED DENTAL SERVICES The following is a complete list of those dental services which will be considered for payment by The American Progressive Life
SECTION 8 DENTAL BENEFITS SCHEDULE OF DENTAL BENEFITS
 SECTION 8 DENTAL BENEFITS The Fund pays up to a maximum of $2,000 per year for Dental expenses incurred by Participants and/or Dependents age 19 or over in accordance with the Schedule of Dental benefits;
SECTION 8 DENTAL BENEFITS The Fund pays up to a maximum of $2,000 per year for Dental expenses incurred by Participants and/or Dependents age 19 or over in accordance with the Schedule of Dental benefits;
Concordia Plus Schedule of Benefits
 Concordia Plus Schedule of Benefits Plan MD/DC 6 IMPORTANT INFORMATION ABOUT YOUR PLAN This schedule of benefits provides a listing of procedures covered by your plan. For procedures that require a copayment,
Concordia Plus Schedule of Benefits Plan MD/DC 6 IMPORTANT INFORMATION ABOUT YOUR PLAN This schedule of benefits provides a listing of procedures covered by your plan. For procedures that require a copayment,
Eligibility and Enrollment
 Eligibility and Enrollment Retirees receiving a monthly age and service or disability benefit may only enroll Legal spouse Must have a valid marriage certificate. Child(ren) This must be a participant
Eligibility and Enrollment Retirees receiving a monthly age and service or disability benefit may only enroll Legal spouse Must have a valid marriage certificate. Child(ren) This must be a participant
DELTA DENTAL PPO EPO PLAN DESIGN CP070
 DELTA DENTAL PPO EPO PLAN DESIGN CP070 SCHEDULE OF BENEFITS AND The benefits shown below are performed as deemed appropriate by the attending Dentist subject to the limitations and exclusions of the program.
DELTA DENTAL PPO EPO PLAN DESIGN CP070 SCHEDULE OF BENEFITS AND The benefits shown below are performed as deemed appropriate by the attending Dentist subject to the limitations and exclusions of the program.
2015 Individual Adult Dental and Vision Care Plan Overview
 2015 Individual Adult Dental and Vision Care Plan Overview Take care of your health with Adult Vision Care and Dental plans Adult Vision Care and Dental plans through Independence Blue Cross (Independence)
2015 Individual Adult Dental and Vision Care Plan Overview Take care of your health with Adult Vision Care and Dental plans Adult Vision Care and Dental plans through Independence Blue Cross (Independence)
Anthem Extras Packages
 Anthem Extras Packages Dental, Vision and more California Benefits that complement your Medicare Supplement plan Packaged benefits better together Healthy teeth and eyes help contribute to your overall
Anthem Extras Packages Dental, Vision and more California Benefits that complement your Medicare Supplement plan Packaged benefits better together Healthy teeth and eyes help contribute to your overall
Summary of Benefits - Dental HMO Deluxe Plan
 Office visit Office visit $5 per visit Diagnostic (exams and x-rays) D0120 Periodic oral evaluation You pay nothing D0140 Limited oral evaluation - problem focused You pay nothing D0145 Oral evaluation
Office visit Office visit $5 per visit Diagnostic (exams and x-rays) D0120 Periodic oral evaluation You pay nothing D0140 Limited oral evaluation - problem focused You pay nothing D0145 Oral evaluation
Delta Dental PPO SM Platinum, Gold and Silver
 Delta Dental PPO SM Platinum, Gold and Silver Plans offered with 2- and 3-tier rate options. Summary of Coverages Platinum Option Gold Option Silver Option Coverage A Diagnostic: Routine exams twice per
Delta Dental PPO SM Platinum, Gold and Silver Plans offered with 2- and 3-tier rate options. Summary of Coverages Platinum Option Gold Option Silver Option Coverage A Diagnostic: Routine exams twice per
APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE
 : EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
: EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
Dental Benefits Summary
 CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 D2510 Inlay - Metallic 1 Surf D6073 Abutment Supported Retainer for Cast Metal FPD (Predominantly Base Metal) D2520 Inlay - Metallic 2 Surf D6074 Abutment
CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 D2510 Inlay - Metallic 1 Surf D6073 Abutment Supported Retainer for Cast Metal FPD (Predominantly Base Metal) D2520 Inlay - Metallic 2 Surf D6074 Abutment
AmeriPlan Lime Fee Zip: 78411
 AmeriPlan Lime Fee Zip: 78411 SPECIALIST FEE SCHEDULE Any AmeriPlan /Dental Plans of America member receiving treatment from a participating specialist provider (advanced degree), shall receive a 15% discount
AmeriPlan Lime Fee Zip: 78411 SPECIALIST FEE SCHEDULE Any AmeriPlan /Dental Plans of America member receiving treatment from a participating specialist provider (advanced degree), shall receive a 15% discount
LOUISIANA MEDICAID PROGRAM ISSUED: 08/18/14 REPLACED: 09/15/13 CHAPTER 16: DENTAL SERVICES APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE PAGE(S) 16
 16") APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE
 : EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
: EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
Summary of Benefits Dental Coverage - New Dental Option
 Summary of Benefits Dental Coverage - New Dental Option Managed Dental Plan MET225 - Texas Code Description Co-Payment Diagnostic Treatment D0120 Periodic Oral Evaluation established patient $0 D0150 Comprehensive
Summary of Benefits Dental Coverage - New Dental Option Managed Dental Plan MET225 - Texas Code Description Co-Payment Diagnostic Treatment D0120 Periodic Oral Evaluation established patient $0 D0150 Comprehensive
Dental Benefits Summary
 CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 CODE DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 CODE DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
LOUISIANA MEDICAID PROGRAM ISSUED: 09/15/13 REPLACED: 03/28/13 CHAPTER 16: DENTAL SERVICES APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE PAGE(S) 16
 16") APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
APPENDIX A: FEE SCHEDULE DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program.
Dental Benefits Summary
 PATIENT PAYS PATIENT PAYS CODE PROCEDURE CODE PROCEDURE Office Visit Copay $0 DIAGNOSTIC D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series Images D0330 Panoramic
PATIENT PAYS PATIENT PAYS CODE PROCEDURE CODE PROCEDURE Office Visit Copay $0 DIAGNOSTIC D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series Images D0330 Panoramic
AIG Group Scheduled Reimbursement Dental SM Insurance
 PRODUCT SPECIFICATIONS AIG Group Scheduled Reimbursement Dental SM Insurance Under the AIG Group Scheduled Reimbursement Dental SM plan, we combine choice and affordability to create long-term satisfaction.
PRODUCT SPECIFICATIONS AIG Group Scheduled Reimbursement Dental SM Insurance Under the AIG Group Scheduled Reimbursement Dental SM plan, we combine choice and affordability to create long-term satisfaction.
DELTA DENTAL PPO sm AGREEMENT SUPPLEMENT TO DELTA DENTAL PREMIER PARTICIPATING DENTIST S AGREEMENT
 DELTA DENTAL PPO sm AGREEMENT SUPPLEMENT TO DELTA DENTAL PREMIER PARTICIPATING DENTIST S AGREEMENT This agreement (the "Supplement") supplements the Delta Dental Premier Participating Dentist s Agreement
DELTA DENTAL PPO sm AGREEMENT SUPPLEMENT TO DELTA DENTAL PREMIER PARTICIPATING DENTIST S AGREEMENT This agreement (the "Supplement") supplements the Delta Dental Premier Participating Dentist s Agreement
DMO Dental Benefits Summary
 CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 CODE DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
CODE PROCEDURE Office Visit Copay PATIENT PAYS $0 CODE DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
APPENDIX A: EPSDT DENTAL PROGRAM FEE SCHEDULE
 : EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
: EPSDT DENTAL PROGRAM FEE SCHEDULE Provided in the table on the following pages are the reimbursable dental procedure codes and fees for the Medicaid of Louisiana, EPSDT Dental Program. All procedures
Aetna Dental presents A Dental Benefit Summary for Michigan Voluntary Option 2; Freedom-of-Choice; No Ortho DMO
 Aetna Dental presents A Dental Benefit Summary for Michigan Voluntary Option 2; Freedom-of-Choice; No Ortho DMO PPO Max Annual Deductible* Individual None $75 Family None $225 Preventive Service Covered
Aetna Dental presents A Dental Benefit Summary for Michigan Voluntary Option 2; Freedom-of-Choice; No Ortho DMO PPO Max Annual Deductible* Individual None $75 Family None $225 Preventive Service Covered
TX Prepaid DHMO Dental
 TX Prepaid DHMO Dental Good news about dental benefits for employees of Pearland Independent School District A Dental Plan Means Healthy Smiles Because you are a valued employee, we are pleased to offer
TX Prepaid DHMO Dental Good news about dental benefits for employees of Pearland Independent School District A Dental Plan Means Healthy Smiles Because you are a valued employee, we are pleased to offer
A Dental Plan Means Healthy Smiles
 Prepaid Dental Good news about dental benefits for employees of Westbury Christian School A Dental Plan Means Healthy Smiles Because you are a valued employee, we are pleased to offer you the opportunity
Prepaid Dental Good news about dental benefits for employees of Westbury Christian School A Dental Plan Means Healthy Smiles Because you are a valued employee, we are pleased to offer you the opportunity
Aetna Dental presents A Dental Benefit Summary for Florida Voluntary Option 2; Freedom-of-Choice; w/ortho DMO
 Aetna Dental presents A Dental Benefit Summary for Florida Voluntary Option 2; Freedom-of-Choice; w/ortho DMO PPO Max Annual Deductible* Individual None $75 Family None $225 Preventive Service Copay/Covered
Aetna Dental presents A Dental Benefit Summary for Florida Voluntary Option 2; Freedom-of-Choice; w/ortho DMO PPO Max Annual Deductible* Individual None $75 Family None $225 Preventive Service Copay/Covered
Aetna Dental presents A Dental Benefit Summary for Florida Option 3; Freedom-of-Choice; w/ortho DMO
 Aetna Dental presents A Dental Benefit Summary for Florida Option 3; Freedom-of-Choice; w/ortho DMO PPO Annual Deductible* Individual None $50 Family None $150 Preventive Service Covered Percent 100% 100%
Aetna Dental presents A Dental Benefit Summary for Florida Option 3; Freedom-of-Choice; w/ortho DMO PPO Annual Deductible* Individual None $50 Family None $150 Preventive Service Covered Percent 100% 100%
SCHEDULE A Description of Benefits and Copayments DHMO-901
 866.650.3660 WWW.PREMIERLIFE.COM SCHEDULE A Description of Benefits and Copayments DHMO-901 The benefits shown below are performed as deemed appropriate by the attending Primary Care Dentist subject to
866.650.3660 WWW.PREMIERLIFE.COM SCHEDULE A Description of Benefits and Copayments DHMO-901 The benefits shown below are performed as deemed appropriate by the attending Primary Care Dentist subject to
KRTA eligible for Delta Dental coverage!
 KRTA eligible for Delta Dental coverage! The oldest and largest dental insurance carrier in Kentucky with the largest dentist networks offers you a choice of three dental programs. You have several different
KRTA eligible for Delta Dental coverage! The oldest and largest dental insurance carrier in Kentucky with the largest dentist networks offers you a choice of three dental programs. You have several different
EssentialSmile Ped 221 Schedule of Benefits
 EssentialSmile Ped 221 Schedule of Benefits P.O. Box 19199 Plantation, FL 33318 Telephone: 877-760-2247 Fax: 954-370-1701 www.mysolstice.net Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx
EssentialSmile Ped 221 Schedule of Benefits P.O. Box 19199 Plantation, FL 33318 Telephone: 877-760-2247 Fax: 954-370-1701 www.mysolstice.net Members can search for a Network Provider at www.solsticecare.com/provider-search.aspx
EssentialSmile Ped 221 Schedule of Benefits
 EssentialSmile Ped 221 Schedule of Benefits P.O. Box 9 Plantation, FL 33318 Telephone: 877 760 2247 Fax: 954 370 1701 www.mysolstice.net Members can search for a Network Provider atwww.solsticecare.com/provider
EssentialSmile Ped 221 Schedule of Benefits P.O. Box 9 Plantation, FL 33318 Telephone: 877 760 2247 Fax: 954 370 1701 www.mysolstice.net Members can search for a Network Provider atwww.solsticecare.com/provider
CHOICES Patients Covered dental services
 CHOICES Patients Covered dental services Important points: There is a $7 co-pay for each covered service visit at the UF College of Dentistry except for some denture therapy services which may require
CHOICES Patients Covered dental services Important points: There is a $7 co-pay for each covered service visit at the UF College of Dentistry except for some denture therapy services which may require
Dental Benefits Summary
 CODE PROCEDURE Office Visit Copay PATIENT PAYS CODE $0 DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
CODE PROCEDURE Office Visit Copay PATIENT PAYS CODE $0 DIAGNOSTIC PROCEDURE PATIENT PAYS D0120-D0180 Oral Evaluations D0277 Vertical Bitewings - 7 to 8 Films D0210 Full mouth series X-rays D0330 Panoramic
Voluntary Dental PPO (Indemnity Plan)
") Voluntary Dental PPO (Indemnity Plan) Good news about your dental benefits Your Dental Plan As a valued employee of Cypress-Fairbanks ISD, you have the opportunity to enroll in a payroll-deduction dental
Voluntary Dental PPO (Indemnity Plan) Good news about your dental benefits Your Dental Plan As a valued employee of Cypress-Fairbanks ISD, you have the opportunity to enroll in a payroll-deduction dental